Bisphosphonate IV (AREDIA/ZOMETA) - Group Health Cooperative
Bisphosphonate IV (AREDIA/ZOMETA) - Group Health Cooperative
Bisphosphonate IV (AREDIA/ZOMETA) - Group Health Cooperative

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
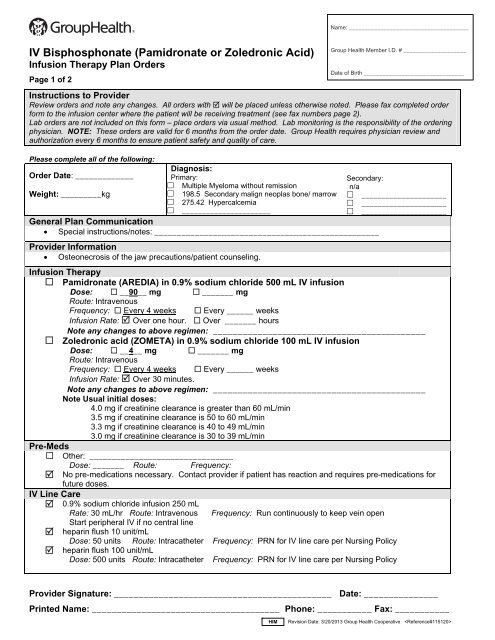
Name: ______________________________________<strong>IV</strong> <strong>Bisphosphonate</strong> (Pamidronate or Zoledronic Acid)Infusion Therapy Plan OrdersPage 1 of 2Instructions to ProviderReview orders and note any changes. All orders with will be placed unless otherwise noted. Please fax completed orderform to the infusion center where the patient will be receiving treatment (see fax numbers page 2).Lab orders are not included on this form – place orders via usual method. Lab monitoring is the responsibility of the orderingphysician. NOTE: These orders are valid for 6 months from the order date. <strong>Group</strong> <strong>Health</strong> requires physician review andauthorization every 6 months to ensure patient safety and quality of care.Please complete all of the following:Diagnosis:Order Date: _____________Primary:Secondary: Multiple Myeloma without remissionn/aWeight: _________kg 198.5 Secondary malign neoplas bone/ marrow _____________________ 275.42 Hypercalcemia _____________________ ______________________ _____________________General Plan Communication Special instructions/notes: __________________________________________________Provider Information Osteonecrosis of the jaw precautions/patient counseling.Infusion Therapy Pamidronate (<strong>AREDIA</strong>) in 0.9% sodium chloride 500 mL <strong>IV</strong> infusionDose: __90__ mg _______ mgRoute: IntravenousFrequency: Every 4 weeks Every ______ weeksInfusion Rate: Over one hour. Over _______ hoursNote any changes to above regimen: ___________________________________________ Zoledronic acid (<strong>ZOMETA</strong>) in 0.9% sodium chloride 100 mL <strong>IV</strong> infusionDose: __4__ mg _______ mgRoute: IntravenousFrequency: Every 4 weeks Every ______ weeksInfusion Rate: Over 30 minutes.Note any changes to above regimen: ___________________________________________Note Usual initial doses:4.0 mg if creatinine clearance is greater than 60 mL/min3.5 mg if creatinine clearance is 50 to 60 mL/min3.3 mg if creatinine clearance is 40 to 49 mL/min3.0 mg if creatinine clearance is 30 to 39 mL/minPre-Meds Other: ________________________________Dose: _______ Route: Frequency: No pre-medications necessary. Contact provider if patient has reaction and requires pre-medications forfuture doses.<strong>IV</strong> Line Care 0.9% sodium chloride infusion 250 mLRate: 30 mL/hr Route: Intravenous Frequency: Run continuously to keep vein openStart peripheral <strong>IV</strong> if no central line heparin flush 10 unit/mLDose: 50 units Route: Intracatheter Frequency: PRN for <strong>IV</strong> line care per Nursing Policy heparin flush 100 unit/mLDose: 500 units Route: IntracatheterFrequency: PRN for <strong>IV</strong> line care per Nursing Policy<strong>Group</strong> <strong>Health</strong> Member I.D. # ____________________Date of Birth ________________________________Provider Signature: ____________________________________________ Date: _______________Printed Name: ______________________________________ Phone: ___________ Fax: ___________HIM Revision Date: 3/20/2013 <strong>Group</strong> <strong>Health</strong> <strong>Cooperative</strong>
Name: ______________________________________<strong>IV</strong> <strong>Bisphosphonate</strong> (Pamidronate or Zoledronic Acid)Infusion Therapy Plan OrdersPage 2 of 2<strong>Group</strong> <strong>Health</strong> Member I.D. # ____________________Date of Birth ________________________________Lab Review for Nursing Baseline labs and labs before each treatment: SCr and CalciumLab Parameters to Assess: CrCl greater than 29 mL/min. For patient with BASELINE SCR LESS THAN 1.4 mg/dL, notify provider if there is an increase in SCr frombaseline of less than or equal to 0.5 mg/dL. For patient with BASELINE SCR GREATER THAN OR EQUAL TO 1.4 mg/dL, notify provider if there is anincrease in SCr from baseline of less than or equal to 1 mg/dL.Nursing Orders Discontinue <strong>IV</strong> line when therapy complete and patient stabilized.References de Lemos M et al. J Oncol Pharm Practice. 2006 Dec;12(4):193-9 Pamidronate information - Daily Med Berenson J, et al. Cancer, 2001;91:1191-1200 Kyle RA et al. JCO 2007;25:2464-2472. Zometa® Prescribing Information. Revised November 2012.<strong>Group</strong> <strong>Health</strong> Infusion LocationsBellevue Medical Center11511 NE 10 th St, Bellevue, WA 98004Fax: 425-502-3512 Phone: 425-502-3510Capitol Hill Medical Center201 16 th Ave E, Seattle WA 98112Fax: 206-326-2104 Phone: 206-326-3109Everett Medical Center2930 Maple St, Everett, WA 98201Fax: 425-261-1659 Phone: 425-261-1681Olympia Medical Center700 Lily Road N.E., Olympia, WA 98506Fax: 360-923-7106 Phone: 360-923-7164Riverfront Medical Center – SpokaneW 322 North River Drive, Spokane, WA 99201Fax: 509-324-7168 Phone: 509-241-2073Silverdale Medical Center10452 Silverdale Way NW, Silverdale, WA 98383Fax: 360-307-7493 Phone: 360-307-7444Tacoma Medical Center209 Martin Luther King Jr Way, Tacoma, WA 98405Fax: 253-383-6262 Phone: 253-596-3666Provider Signature: ____________________________________________ Date: _______________Printed Name: ______________________________________ Phone: ___________ Fax: ___________HIM Revision Date: 3/20/2013 <strong>Group</strong> <strong>Health</strong> <strong>Cooperative</strong>