Bilateral Optic Disc Drusen in Hypermetropic Children of a Family
Bilateral Optic Disc Drusen in Hypermetropic Children of a Family
Bilateral Optic Disc Drusen in Hypermetropic Children of a Family

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Case Report<strong>Bilateral</strong> <strong>Optic</strong> <strong>Disc</strong> <strong>Drusen</strong> <strong>in</strong> <strong>Hypermetropic</strong><strong>Children</strong> <strong>of</strong> a <strong>Family</strong>Ghulam Mustafa Memon, Shakir Zafar, Munira Shakir, Zeeshan Kamil, Syeda Aisha BokhariPak J Ophthalmol 2012, Vol. 28 No. 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . .. . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .See end <strong>of</strong> article forauthors affiliations…..………………………..Correspondence to:Ghulam Mustafa MemonLRBT, Free base EyeHospitalKorangi-2 1/2, Karachi-74900…..………………………..<strong>Optic</strong> disc drusen are calcified, round, yellow nodules, with various sizes tend tobe located with<strong>in</strong> any part <strong>of</strong> the optic nerve head. Accord<strong>in</strong>g to most theoriesthey are caused by impaired ganglion cell axonal transport, probably related to asmall sclera canal and mechanical obstruction. We report a case <strong>of</strong> 12 year oldmale child and his 13 year old sister, both presented with decrease vision <strong>in</strong> ouroutpatient department. Fundus exam<strong>in</strong>ation <strong>of</strong> both patients revealed bilateraloptic disc swell<strong>in</strong>gs with no hyperemia. After <strong>in</strong>vestigations, it was proved thatboth patients suffered from bilateral buried optic disc drusen. Decrease vision wasbecause <strong>of</strong> hypermetropia <strong>in</strong> both children.<strong>Optic</strong> disc drusen, also known as hyal<strong>in</strong>e orcolloid bodies, are hyal<strong>in</strong>e, calcified,microbodies situated <strong>in</strong> the prelam<strong>in</strong>ar part<strong>of</strong> the optic nerve head 1 . The processes <strong>of</strong>development <strong>of</strong> drusen <strong>of</strong> the optic nerve head isproposed as abnormal axonal metabolism lead<strong>in</strong>g to<strong>in</strong>tracellular mitochondrial calcification. Smallcalcified microbodies are formed and calciumcont<strong>in</strong>ues to deposit on the surface <strong>of</strong> thesemicrobodies to form drusen 2 . Axoplasmic transportvariation is the anatomic substrate for creation <strong>of</strong>drusen <strong>of</strong> the optic disk 3 . <strong>Optic</strong> disc drusen areassociated with shorter and hypermetropic eyes, theseanatomical situations and vascular factors may giverise to pathogenesis <strong>of</strong> drusen 4,5 . <strong>Optic</strong> disc drusen ispresent <strong>in</strong> 3.4 to 24 per 1,000 populations and arebilateral <strong>in</strong> about 75% 6 . <strong>Optic</strong> disc drusen haveirregular autosomal dom<strong>in</strong>ant <strong>in</strong>heritance 7 . Because <strong>of</strong>cont<strong>in</strong>uous calcium deposition, optic disc drusen will<strong>in</strong>crease <strong>in</strong> size and will become more visible with age.A correct diagnosis <strong>of</strong> optic disc drusen is compulsory,though effective treatment is not yet present but it ismost important to differentiate optic disc drusen frompapilledema <strong>in</strong> order to evade unnecessaryneurological exam<strong>in</strong>ations 6,8 . Cl<strong>in</strong>ical <strong>in</strong>terpretationsprove that the optic nerve head drusen are widelyasymptomatic and that visual acuity rema<strong>in</strong>sunaffected 9 but discrete papillary calcifications orhyal<strong>in</strong>e bodies commonly emerge and visual fielddeficits are commonly noticeable <strong>in</strong> the second decade<strong>of</strong> life <strong>in</strong> patients with pseudopapilledema due to opticdisc drusen 10 . This case is presented to emphasize theimportance <strong>of</strong> optic disc drusen and its associationwith hypermetropia and <strong>in</strong>heritance.CASE REPORT12 year old male child and his 13 year old sisterpresented <strong>in</strong> our eye outpatient department withdecrease vision <strong>in</strong> both eyes s<strong>in</strong>ce last 5 year. Bothwere student and had no systemic illness. Generalphysical exam<strong>in</strong>ation and systemic exam<strong>in</strong>ation wereunremarkable.Ophthalmologic exam<strong>in</strong>ation <strong>of</strong> male childrevealed best corrected visual acuity with correction <strong>of</strong>+19.5 DS <strong>in</strong> both eyes to be 6/60 (us<strong>in</strong>g Snellen’svisual acuity chart) with no p<strong>in</strong> hole improvement.Best corrected visual acuity <strong>of</strong> female patient withcorrection <strong>of</strong> +19.0DS <strong>in</strong> both eyes was 6/36 (us<strong>in</strong>gSnellen’s visual acuity chart) with no p<strong>in</strong> holeimprovement. There was no deviation <strong>in</strong> any eye andextra ocular muscle movements were full <strong>in</strong> both eyes<strong>of</strong> both patients. Both pupils were round, regular andreact<strong>in</strong>g to light and no relative afferent pupillarydefect was noted. Biomicroscopic exam<strong>in</strong>ation <strong>of</strong> boththe anterior segments was unremarkable. Fundoscopicexam<strong>in</strong>ation showed bilateral blurred and swollenoptic discs marg<strong>in</strong>s with no hyperemia and withobliteration <strong>of</strong> the physiological optic disc cupp<strong>in</strong>g(Fig 1A, 2A). Venous pulsations were present <strong>in</strong> botheyes <strong>in</strong> both patients. Visual field exam<strong>in</strong>ation byconfrontation showed grossly restricted peripheralPakistan Journal <strong>of</strong> Ophthalmology Vol. 28, No. 3, Jul – Sep, 2012 163
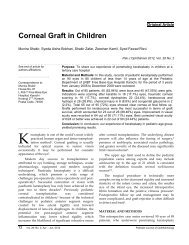
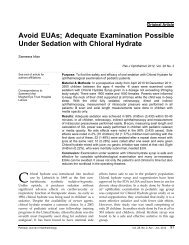
GHULAM MUSTAFA MEMON, et alAdditionally CT scan bra<strong>in</strong> and orbit was done to seethe optic nerve head calcification and to exclude anycentral nervous system pathology. Patients and theirparents were <strong>in</strong>formed about the condition and cause<strong>of</strong> decrease vision, which was hypermetropia and theirparents were also <strong>in</strong>formed that they and their other<strong>of</strong>fspr<strong>in</strong>g should have an ophthalmic exam<strong>in</strong>ation toexclude optic disc drusens.Fig. 1AFig. 2A: Fundus photographs <strong>of</strong> patient show<strong>in</strong>gbilateral optic disc swell<strong>in</strong>g and blurred marg<strong>in</strong>s andobliteration <strong>of</strong> the physiological optic disc cupp<strong>in</strong>g.Fig. C: <strong>Optic</strong>al Coherence Tomography show<strong>in</strong>gtypically elevated optic nerve head and opticallyempty cavity and perceptible reflection from posteriorsurface.Fig. B: B-scan ultrasonograph show<strong>in</strong>g focal highacoustic reflectivity because <strong>of</strong> calcific deposition.visual fields <strong>in</strong> both eyes but it was not possible toperform automatic Humphery perimetry as thepatients were young <strong>in</strong> age so were uncooperative andunable to understand commands for automatichumphery perimetry. A diagnosis <strong>of</strong> bilateral opticnerve head drusen was made, which wassubsequently confirmed by B scan ocular ultrasonography(Fig B) and <strong>Optic</strong>al Coherence Tomography(Fig C) <strong>in</strong> our ophthalmic outpatient department.DISSCUSION<strong>Optic</strong> disc drusen are congenital and developmentalanomalies <strong>of</strong> the optic nerve head seen frequently <strong>in</strong>cl<strong>in</strong>ical practice, <strong>of</strong>ten as an <strong>in</strong>cidental f<strong>in</strong>d<strong>in</strong>g dur<strong>in</strong>grout<strong>in</strong>e ophthalmic exam<strong>in</strong>ation. <strong>Optic</strong> disc drusencan affect children as well as adults. It is important toconsider optic nerve head drusen <strong>in</strong> the differentialdiagnosis <strong>of</strong> papilledema or optic nerve swell<strong>in</strong>g <strong>in</strong>any age group 11 . The primary pathology <strong>of</strong> optic discdrusen is an <strong>in</strong>herited dysplasia <strong>of</strong> the optic disc andits blood supply, which <strong>in</strong>fluence the formation <strong>of</strong>optic disc drusen 4,12 . <strong>Optic</strong> disc drusen has a greatertendency to form <strong>in</strong> eyes with a small scleral canal;therefore hypermetropic eyes would have a higherrate <strong>of</strong> optic disc drusen relative to myopic eyes 5 . Thediagnosis <strong>of</strong> optic disc drusen can be made with164 Vol. 28, No. 3, Jul – Sep, 2012 Pakistan Journal <strong>of</strong> Ophthalmology
BILATERAL OPTIC DISC DRUSEN IN HYPERMETROPIC CHILDREN OF A FAMILYcl<strong>in</strong>ical f<strong>in</strong>d<strong>in</strong>gs comb<strong>in</strong>ed with B scan ultrasound,Fundus fluoresce<strong>in</strong> angiography, Ocular computedtomography and newer modalities us<strong>in</strong>g opticalcoherence tomography <strong>of</strong> optic nerve head, 11 butocular B-Scan ultrasonography, a non-<strong>in</strong>vasive andcost-effective technique is the most sensitive andmethod <strong>of</strong> choice <strong>in</strong> the recognition <strong>of</strong> optic discdrusen 8,13,15 . <strong>Optic</strong> disc drusen shows aut<strong>of</strong>luorescence(ability <strong>of</strong> substance to emit yellow-greenlight when stimulated by blue light <strong>in</strong> the absence <strong>of</strong>fluoresce<strong>in</strong> dye) <strong>in</strong> Fundus fluoresce<strong>in</strong> angiography.Incidental asymptomatic orbital calcifications arefrequently encountered on modern high-resolution CTscan images <strong>of</strong> the bra<strong>in</strong> and orbit 14 . <strong>Optic</strong>al coherencetomography can differentiate optic disc drusen frompapilledema and small optic disc without disc drusenas optic nerve head drusen typically elevate the discsurface and appear as an optically empty cavity,sometimes with a perceptible reflection from theposterior surface. The disc surface is also elevated <strong>in</strong>cases <strong>of</strong> papilledema, but has a strong anteriorreflection beh<strong>in</strong>d which, there is no visible structure.The surface <strong>of</strong> the small optic nerves was slightlyelevated, but with less anterior reflectance, 16 thereforeOCT <strong>of</strong> optic nerve head exposed unique andcl<strong>in</strong>ically helpful views <strong>of</strong> optic nerve drusen 17 .The aim <strong>of</strong> present<strong>in</strong>g this case is that we shouldconsider optic disc drusen <strong>in</strong> any patient who presentswith bilateral optic disc swell<strong>in</strong>g, particularly whenthe patient is hypermetropic and asymptomatic.CONCLUSIONIn our case the unique feature is presence <strong>of</strong> bilateraloptic disc drusen <strong>in</strong> hypermetropic two children <strong>of</strong> thesame family. <strong>Optic</strong> disc drusen may be hereditary andhave close association with small scleral canal.Author’s affiliationDr. Ghulam Mustafa MemonResident Medical OfficerLRBT, Free base Eye HospitalKorangi-2 1/2, Karachi-74900Dr. Shakir ZafarConsultant OphthalmologistLRBT, Free base Eye HospitalKorangi-2 1/2, Karachi-74900Dr. Munira ShakirConsultant Ophthalmologist &Head <strong>of</strong> Pediatric Ophthalmology DepartmentLRBT, Free base Eye HospitalKorangi-2 1/2, Karachi-74900Dr. Zeeshan KamilOphthalmologistLRBT, Free base Eye HospitalKorangi-2 1/2, Karachi-74900Dr. Syeda Aisha BokhariAssociate OpthalmologistLRBT, Free base Eye HospitalKorangi-2 1/2, Karachi-74900REFERENCE1. Wilk<strong>in</strong>s JM, Pomeranz HD. Visual manifestations <strong>of</strong> visibleand buried optic disc drusen. J Neuro-ophthalmol. 2004; 24:125-9.2. Tso MO. Pathology and pathogenesis <strong>of</strong> drusen <strong>of</strong> the opticnervehead. Ophthalmology. 1981; 88: 1066-80.3. Spencer WH. <strong>Drusen</strong> <strong>of</strong> the optic disk and aberrant axoplasmictransport. The XXXIV Edward Jackson memorial lecture. Am JOphthalmol. 1978; 85: 1-12.4. Obuchowska I, Mariak Z. Refraction and the axial length <strong>of</strong>the eyeball <strong>in</strong> patients with the optic disc drusen. Kl<strong>in</strong> Oczna.2009; 111: 33-6.5. Strassman I, Silverston B, Seelenfreund M. <strong>Optic</strong> disc drusenand hypermetropia. Metab Pediatr Syst Ophthalmol. 1991; 14:59-61.6. Auw-Haedrich C, Staubach F, Witschel H. <strong>Optic</strong> disk drusen.Surv Ophthalmol. 2002; 47: 515-32.7. Lorentzen SE. <strong>Drusen</strong> <strong>of</strong> the optic disk, an irregularlydom<strong>in</strong>ant hereditary affection. Acta Ophthalmol (Copenh).1961; 39: 626-43.8. Arbabi EM, Fearnley TE, Carrim ZI. <strong>Drusen</strong> and themislead<strong>in</strong>g optic disc. Pract Neurol. Feb; 10: 27-30.9. Giarelli L, Ravalico G, Saviano S, et al. <strong>Optic</strong> nerve headdrusen: histopathological considerations cl<strong>in</strong>ical features.Metab Pediatr Syst Ophthalmol. 1990; 13: 88-91.10. Hoover DL, Robb RM, Petersen RA. <strong>Optic</strong> disc drusen <strong>in</strong>children. J Pediatr Ophthalmol Strabismus. 1988; 25: 191-5.11. Davis PL, Jay WM. <strong>Optic</strong> nerve head drusen. Sem<strong>in</strong>Ophthalmol. 2003; 18: 222-42.12. Antcliff RJ, Spalton DJ. Are optic disc drusen <strong>in</strong>herited?Ophthalmology. 1999; 106: 1278-81.13. Kheterpal S, Good PA, Beale DJ, et al. Imag<strong>in</strong>g <strong>of</strong> optic discdrusen: a comparative study. Eye (Lond). 1995; 9: 67-9.14. Murray JL, Hayman LA, Tang RA, et al. Incidentalasymptomatic orbital calcifications. J Neuroophthalmol. 1995;15: 203-8.15. Kurz-Lev<strong>in</strong> MM, Landau K. A comparison <strong>of</strong> imag<strong>in</strong>gtechniques for diagnos<strong>in</strong>g drusen <strong>of</strong> the optic nerve head. ArchOphthalmol. 1999 ; 117: 1045-9.16. Wester ST, Fantes FE, Lam BL, et al. Characteristics <strong>of</strong> opticnerve head drusen on optical coherence tomography images.Ophthalmic Surg Lasers Imag<strong>in</strong>g. 41: 83-90.17. Patel NN, Shulman JP, Ch<strong>in</strong> KJ, et al. <strong>Optic</strong>al coherence tomography/scann<strong>in</strong>glaser ophthalmoscopy imag<strong>in</strong>g <strong>of</strong> optic nervehead drusen. Ophthalmic Surg Lasers Imag<strong>in</strong>g. 41: 614-2.Pakistan Journal <strong>of</strong> Ophthalmology Vol. 28, No. 3, Jul – Sep, 2012 165