ESC Position on Medical Devices - Cardiovascular Round Table ...
ESC Position on Medical Devices - Cardiovascular Round Table ...
ESC Position on Medical Devices - Cardiovascular Round Table ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
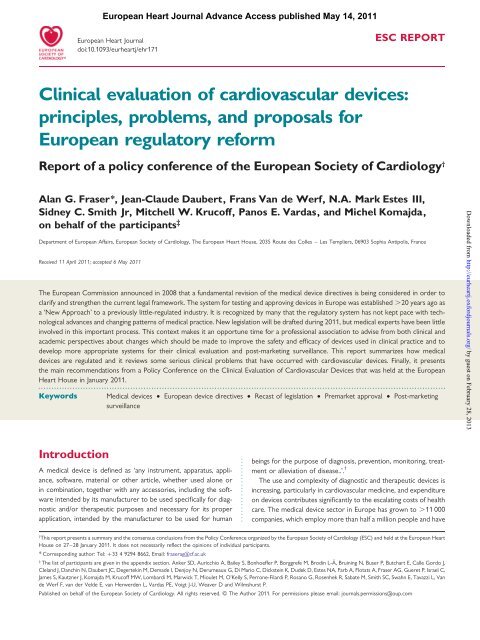
Clinical evaluati<strong>on</strong> of cardiovascular devices Page 3 of 18first annexes of the three directives. To do this, the manufacturermay refer to relevant technical standards such as those from theEuropean Committee for Standardizati<strong>on</strong> (CEN) and the EuropeanCommittee for Electrotechnical Standardizati<strong>on</strong> (CENELEC). 14 Inmost instances, these mirror the standards from the Internati<strong>on</strong>alOrganizati<strong>on</strong> for Standardizati<strong>on</strong> (ISO) and the Internati<strong>on</strong>al ElectrotechnicalCommissi<strong>on</strong> (IEC). Effective performance of thedevice for its intended purpose (as claimed by the manufacturer)needs to be dem<strong>on</strong>strated. The precise definiti<strong>on</strong> of the designatedtask of any device, therefore, is a key decisi<strong>on</strong> for each manufacturer.It can be argued that this process encourages the manufacturerto keep its claims for a device as simple as possible.The clinical data used for CE marking may be a critical evaluati<strong>on</strong>of the relevant scientific literature currently available relating to thedesign characteristics, intended purpose, safety, and performanceof a device, when it is dem<strong>on</strong>strated to be equivalent to anotherdevice which already complies with relevant essential requirementsand for which there are data. Alternatively, the manufacturer maypresent a critical evaluati<strong>on</strong> of the results of all reported clinicalinvestigati<strong>on</strong>s that have addressed residual safety c<strong>on</strong>cerns. 10,15For devices in Class III, the manufacturer must c<strong>on</strong>duct somehuman clinical investigati<strong>on</strong>s, but it is not compulsory that theseare randomized clinical trials.Notified BodiesA medical device company is free to approach any NB in Europethat has been designated for the respective ‘c<strong>on</strong>formity assessmentprocedure’ (Figure 1). This process has given rise to suspici<strong>on</strong>s thatcompanies may go ‘forum shopping’ to select the NB that willc<strong>on</strong>duct the least burdensome or the fastest review, but no systematicaudit of the NBs has been published. Since 1985, a NBhas been any organizati<strong>on</strong> designated to assess if manufacturedproducts c<strong>on</strong>form with the requirements of any EU new approachdirective; the website of the Enterprise and Industry Directorate-General listed 2271 NBs in January 2011. Of these, 74 wereapproved to evaluate medical devices, including some organizati<strong>on</strong>slocated outside the EU; 16 several NBs have been approvedto evaluate all medical devices. Most NBs are independent commercialorganizati<strong>on</strong>s, and they are supported in part by the feespaid by device companies. Notified Bodies are designated, m<strong>on</strong>itored,and audited by the competent authorities of the memberstate in which they are based.The duties of a NB are to review the technical dossier submittedby the manufacturer, to assess the manufacturer’s quality managementsystem, and to evaluate any evidence that has been submittedfrom laboratory, animal, and clinical studies. The manufacturersubmits a sample of the device under review, and the NB mayc<strong>on</strong>duct direct testing especially if it is an active medical device.The NB may also visit the manufacturer to inspect the producti<strong>on</strong>process and quality c<strong>on</strong>trol. If these tests are judged satisfactory,then the NB issues a certificate (which is valid for a maximum of5 years before renewal) and the manufacturer can affix theCE mark (Figure 1). Thereafter, the device can be marketedthroughout the EU.Some NBs also functi<strong>on</strong> as nati<strong>on</strong>al standards institutes and theirdivisi<strong>on</strong> with this resp<strong>on</strong>sibility may participate in writing ISO standards.In additi<strong>on</strong>, nati<strong>on</strong>al competent authorities have specifiedthat NBs, as part of their c<strong>on</strong>tract, should participate in the vigilance(or PMS) of medical devices, in which case they receivereports of adverse incidents. Reports are also transmitted togetherwith the proposed ‘Field Safety Corrective Acti<strong>on</strong>’ (FSCA) by themanufacturer to the competent authority which is resp<strong>on</strong>sible forDownloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013Figure 1 Summary of the major steps in the current regulatory framework for approving medical devices in Europe. Solid lines denote formalrequirements; dotted lines represent guidance or advice. DG SANCO ¼ Directorate General for Health and C<strong>on</strong>sumer Affairs.
Page 4 of 18A.G. Fraser et al.their review. If a device needs to be removed from the market, it isthe resp<strong>on</strong>sibility of the NB to suspend its certificate.Coordinati<strong>on</strong>The Committee <strong>on</strong> <strong>Medical</strong> <strong>Devices</strong>, organized by the EC andcomposed of representatives of the Member States, has specificregulatory powers for the device directives. Policy is coordinatedby the <strong>Medical</strong> <strong>Devices</strong> Experts Group (MDEG) which is said to‘encompass all stakeholders’. 17 Its members include representativesfrom trade federati<strong>on</strong>s, CEN, CENELEC, NBs, and patients’organizati<strong>on</strong>s. There are currently no members from Europeanmedical associati<strong>on</strong>s, although the EC states that they have previouslybeen invited.The Notified Bodies group (NB-MED) and the Notified BodiesOperati<strong>on</strong> Group (NBOG) were established by the EC to improvecooperati<strong>on</strong> and performance of the NBs with the competentauthorities in the medical devices sector.The European Databank <strong>on</strong> <strong>Medical</strong> <strong>Devices</strong> (Eudamed) wascreated in 1998 to allow Member States to strengthen PMS byexchanging informati<strong>on</strong> about adverse events related to the useof medical devices. Reporting will become mandatory from May2011. 18 Competent authorities will have rapid access to the databasewhich will include names of registered manufacturers, datarelating to certificates, and reports from vigilance procedureswith the findings of clinical investigati<strong>on</strong>s. The European Databank<strong>on</strong> <strong>Medical</strong> <strong>Devices</strong> will implement the Global <strong>Medical</strong> DeviceNomenclature (GMDN) code; there is also a GMDN Agency,established under the auspices of CEN. There is no plan to openthe c<strong>on</strong>tents of Eudamed to the public.The USAIn the USA, the evaluati<strong>on</strong> and approval of medical devices is theresp<strong>on</strong>sibility of the Food and Drug Administrati<strong>on</strong> (FDA)through its Center for <strong>Devices</strong> and Radiological Health (CDRH),which has a Divisi<strong>on</strong> of <strong>Cardiovascular</strong> <strong>Devices</strong>. As in Europe,devices are categorized by risk into three classes, and higherlevels of evidence including clinical evidence are required forapproval of devices in Class III. In additi<strong>on</strong> to internal regulatoryreview by FDA pers<strong>on</strong>nel, advice is often sought from external,independent experts through well-established <strong>Medical</strong> <strong>Devices</strong>Advisory Committees (including a Circulatory System <strong>Devices</strong>Advisory Panel), 19 for example, for first-of-a-kind devices and fordevices that are expected to have a broad impact <strong>on</strong> publichealth. This provides a transparent mechanism for public reviewof issues relating to the approval of complex devices.Low-risk devices (class I) are approved by registrati<strong>on</strong>, aftercompliance with general c<strong>on</strong>trols such as regulati<strong>on</strong>s for goodmanufacturing practice. More complex, moderate-risk devices(class II) require additi<strong>on</strong>al special c<strong>on</strong>trols, such as specific labelling,compliance with requirements in guidance documents,device tracking, and design c<strong>on</strong>trols. The regulatory pathway forclass II products is through the Premarket Notificati<strong>on</strong> [‘510(k)’]programme, which is the pathway through which most medicaldevices are marketed. A manufacturer submits a ‘premarket notificati<strong>on</strong>’asserting that their new device is substantially equivalent(i.e. at least as safe and effective) as <strong>on</strong>e (‘the predicate’) that isalready legally <strong>on</strong> the market. If the FDA determines that theinformati<strong>on</strong> and performance testing dem<strong>on</strong>strate that this is thecase, then the device can be marketed in the USA. Ten to 15%of 510(k) submissi<strong>on</strong>s require data from human clinical studies tosupplement preclinical testing.High-risk devices (class III) follow the regulatory pathway forpremarket approval (PMA). This requires a comprehensive evaluati<strong>on</strong>including bench testing, preclinical animal studies, and clinicaldata, so that the device dem<strong>on</strong>strates a reas<strong>on</strong>able assurance ofsafety and effectiveness. The term ‘effectiveness’ means that thedevice will provide clinically significant benefits, and thus evaluati<strong>on</strong>focuses <strong>on</strong> clinical outcomes such as a reducti<strong>on</strong> in symptoms oradverse events. In c<strong>on</strong>trast, ‘performance’ (a standard EU regulatoryparameter) focuses <strong>on</strong> a device’s mechanism of acti<strong>on</strong> such asenlargement of the arterial lumen or enhanced myocardial bloodflow. Clinical data for a PMA are typically obtained from feasibilitystudies followed by a larger, ‘pivotal’ trial. In order to c<strong>on</strong>duct aclinical trial in the USA to assess the safety and effectiveness of a‘significant risk’ device and thereby provide evidence that willsupport a PMA or 510(k), the sp<strong>on</strong>sor must obtain FDA approvalof an Investigati<strong>on</strong>al Device Exempti<strong>on</strong> (IDE).In general, regulatory reviews by the FDA incorporate moredetailed technical standards and requirements for clinical evaluati<strong>on</strong>of devices than occurs in Europe, and they are more rigorous.Preclinical testing plays a more important role, with questi<strong>on</strong>sregarding l<strong>on</strong>g-term durability and local and systemic histopathologicalresp<strong>on</strong>ses being addressed in bench and animal studies. Sincethe FDA requires adequate preclinical safety data before theinitiati<strong>on</strong> of human trials, there may be a lag of several yearsafter the introducti<strong>on</strong> of some devices for clinical use withinEurope before they are used in patients in the USA. Many US companiesfirst get approval for their new medical devices in the EUand then use ‘OUS’ (outside the USA) data relating to safety andeffectiveness to support the initiati<strong>on</strong> of a pivotal IDE study atUS study sites.In a recent decisi<strong>on</strong>, the US Supreme Court judged that themanufacturer of a medical device could not be sued by a patient<strong>on</strong> the basis of alleged defects relating to its safety because thedevice had received PMA from the FDA. 20 The c<strong>on</strong>sequences ofthis decisi<strong>on</strong> are still unclear; for example, it is uncertain if it mayencourage manufacturers to submit more detailed claims fordevices when applying for regulatory approval.For permanently implanted class III devices such as cor<strong>on</strong>arystents and devices for occluding intracardiac shunts, the FDA typicallyrequires 5 years of clinical follow-up. Post-approval clinicalstudies that collect and report real-world outcomes associatedwith the use of novel devices are also comm<strong>on</strong>ly required. TheFDA has had a policy of ‘global transparency’ since 1994 and allmedical device reports (MDRs) c<strong>on</strong>cerning significant adverseevents are available <strong>on</strong> the Internet.United States and OUS device manufacturers can meet withFDA staff at multiple times during the development of a device,through the CDRH’s Pre-Submissi<strong>on</strong> Program. These informalmeetings are particularly useful for the sp<strong>on</strong>sors and the FDA toreach c<strong>on</strong>sensus <strong>on</strong> preclinical device testing, key elements ofIDE clinical trials, and requirements for PMA submissi<strong>on</strong>s. The510(k) program has been reviewed by the Institute of Medicine 21and it is being reviewed by the FDA. Recommendati<strong>on</strong>s whichDownloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Page 6 of 18A.G. Fraser et al.<strong>Table</strong> 1 Some less<strong>on</strong>s learned from clinicalexperience of cardiovascular devicesHeart valvesAnimal models dissimilar from human, insufficiently predictive 45Inadequate bench testing of mechanical properties 36,42Incomplete assessment of fluid mechanical properties 47,48Approval of changes as iterative that proved to besubstantial 36,39,43,44................................................................................Percutaneous cor<strong>on</strong>ary interventi<strong>on</strong>sClinical applicati<strong>on</strong> of c<strong>on</strong>cept that was not proved 60,66,80Use of unblinded studies with significant placebo effect 80Over-reliance <strong>on</strong> composite end-points 71Overuse of equivalence for CE marking without new pivotal57 – 60trials<strong>Devices</strong> not taken off market when negative l<strong>on</strong>g-term outcometrials reported 65,81................................................................................Diagnostic imagingNo standard industry-wide phantoms for some imaging modalitiesNo reporting of diagnostic accuracy and reproducibility bymanufacturersNo requirements for manufacturers to present normal values................................................................................<strong>Cardiovascular</strong> implantable electr<strong>on</strong>ic devicesNeed for l<strong>on</strong>g-term registries c<strong>on</strong>ducted independently fromindustry 106,118Incomplete capture of clinical events by registries with voluntaryreportingNeed for rapid and open access to reports of device failures 110,111................................................................................Closure of patent foramen ovaleEarly CE marking leading to rapid adopti<strong>on</strong> before proven clinicalbenefitFailure by physicians to enrol patients in trials 124,125off the market after the AVERT trial reported paraprostheticregurgitati<strong>on</strong> in 8.9% of patients at 2 years, compared with 1.1%in patients receiving the standard model. 43 The Silz<strong>on</strong>e valve wasalso associated with a high incidence of valve thrombosis andthromboembolism. 43,44 It has since been recognized that toxic biologicalproperties of silver prevented normal tissue ingrowth andendothelializati<strong>on</strong> of the sewing ring, but this problem had notbeen revealed by reports from a small preliminary animalstudy. 45 At the time of its recall, the manufacturer estimated that36 000 Silz<strong>on</strong>e valves had already been implanted. 46In these cases, changes to the design of a valve had beenapproved without evidence from prospective clinical trials, <strong>on</strong>the basis that they were minor modificati<strong>on</strong>s. A third mechanicalprosthesis, the Medtr<strong>on</strong>ic Parallel valve, was also withdrawn fromthe market after early incidents of thrombosis, in this caserelated to pockets of stasis. Valve thrombosis might have been predictedby fluid dynamic computati<strong>on</strong>al simulati<strong>on</strong>s and in vitrostudies, 47,48 before human implants, but the patterns of retrogradeflow through the hinge pockets had not been studied. The Parallelvalve was neither studied nor approved in the USA; it was evaluatedin 16 European centres.Gersh et al. 49 identified the need for comm<strong>on</strong> standards forevaluating heart valves and subsequent authors suggested alternativesto randomized trials. 50,51 In 1994 the FDA resp<strong>on</strong>ded byissuing ‘objective performance criteria’ for heart valves. 52 Morerecently, experts have revised recommendati<strong>on</strong>s for the evaluati<strong>on</strong>of valve performance and the reporting of complicati<strong>on</strong>s. 53 Recommendati<strong>on</strong>sfor reporting endpoints in clinical trials of transcatheteraortic valve implantati<strong>on</strong> (TAVI) have also beenpublished 54 and endorsed by the FDA. 55Percutaneous interventi<strong>on</strong>s for cor<strong>on</strong>aryartery diseaseThe initial success rate of ballo<strong>on</strong> cor<strong>on</strong>ary angioplasty was ≏63%,and the procedure was first approved by the FDA after 60 patientshad been treated for 6 m<strong>on</strong>ths. 56 In early series, .10% of patientsrequired emergency bypass surgery and there were many deaths. Itwould have been very difficult to get such approval, either in theUSA or in Europe, if angioplasty had had to be tested againstsurgery while the technology was in its infancy. Early approvalgave an impetus to technological developments in interventi<strong>on</strong>alcardiology and to many important randomized clinical trials inEurope, resulting in a highly effective treatment that reduces morbidityand mortality. 57 N<strong>on</strong>etheless, several scores of cor<strong>on</strong>arystents have received a CE mark and are available within Europe,in spite of the fact that <strong>on</strong>ly six drug-eluting stents have beenproved to be effective by meeting primary clinical endpoints inpivotal trials. 57 L<strong>on</strong>g-term results (≥5 years) are available for<strong>on</strong>ly three stents. 57 It has been recommended that marketaccess should be based <strong>on</strong> efficacy 58 but many stents have beenapproved <strong>on</strong> the basis of technical equivalence rather than clinicaloutcomes. In some countries, reimbursement is limited to proveddevices but in others, doctors may be asked to use cheaper stentseven when proof is lacking.It cannot be assumed that either bare metal or drug-elutingstents are all similar. 58,59 For example, the Niroyal stent wasgold plated in order to enhance its opacity <strong>on</strong> radiographic screening.It was given a CE mark in May 1999 without a pre-marketingclinical trial. A registry reported in 2000 that it gave excellentprimary angiographic success rates, and event rates at 6 m<strong>on</strong>thswere lower than reported in other series. 60 A randomized trial,however, showed a smaller minimal luminal diameter and ahigher late loss. 61 The adverse effects of gold plating were c<strong>on</strong>firmedindependently by other investigators. 62Directi<strong>on</strong>al cor<strong>on</strong>ary atherectomy was evaluated between 1988and 1990 under an IDE. The device was approved by the FDA inSeptember 1990 <strong>on</strong> the basis of a primary success rate of 85%,although <strong>on</strong>e or more major complicati<strong>on</strong>s occurred in 4.9% ofprocedures and the restenosis rate at 6 m<strong>on</strong>ths was 42%. 63 Inthe CAVEAT study, the new technique had a higher rate of earlycomplicati<strong>on</strong>s (11%) and it c<strong>on</strong>ferred no significant benefit overballo<strong>on</strong> angioplasty al<strong>on</strong>e at 6 m<strong>on</strong>ths. 64 One-year follow-uprevealed an increase in mortality at 2.2% in the atherectomygroup compared with 0.6% in c<strong>on</strong>trols. 65 The device was withdrawnfrom the market for commercial reas<strong>on</strong>s rather thanbecause of regulatory decisi<strong>on</strong>s. An estimated 177 000 patientswere treated worldwide. 66Downloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Clinical evaluati<strong>on</strong> of cardiovascular devices Page 7 of 18The first clinical use of intracor<strong>on</strong>ary beta or gamma irradiati<strong>on</strong>(brachytherapy) to prevent or treat restenosis after ballo<strong>on</strong> angioplastywas reported from a Swiss pilot study of 15 patients in1997. 67 The investigators obtained informed c<strong>on</strong>sent from theirpatients after the protocol had been approved by the hospitalEthics Committee, but there is no reference in their manuscriptto regulatory issues or approval for use of a prototype device.A similar clinical pilot study of 23 patients was reported fromthe USA in 1998 by investigators who had obtained an IDE. 68 Inearly clinical trials, brachytherapy was reported to reduce restenosiswithin a stent but it increased stenosis at the stent margins byup to four-fold. 69,70 After two more trials 71,72 the FDA approvedbrachytherapy in 2001 for the treatment of in-stent restenosis,but with c<strong>on</strong>diti<strong>on</strong>s because of reports of thrombosis particularlywhen anti-platelet treatment was disc<strong>on</strong>tinued. 73 By this time,small animal models had already revealed incomplete healingwith poor endothelializati<strong>on</strong> 74 and edge effects. 75 A registry of1098 patients from 46 centres reported good results andshowed c<strong>on</strong>siderable adopti<strong>on</strong> of the new technique inEurope. 76 Further randomized c<strong>on</strong>trolled trials, however, c<strong>on</strong>firmedthat both the early and late results of brachytherapywere worse than standard therapy 77 or therapy with drug-elutingstents. 78,79 This discrepancy between registries and randomizedtrials highlights the importance of independent PMS studies withcentrally adjudicated and m<strong>on</strong>itored adverse events.The rati<strong>on</strong>ale proposed for laser myocardial revascularizati<strong>on</strong>was that creating multiple pits in ischaemic myocardium with alaser beam would promote the formati<strong>on</strong> of collateral channelsor new vessels. The c<strong>on</strong>cept was developed as a surgical techniqueand evolved towards percutaneous delivery. In an initial unblindedtrial, 221 patients were randomized to laser or c<strong>on</strong>tinued medicaltreatment. 80 Patients treated with laser revascularizati<strong>on</strong> hadimproved exercise tolerance at follow-up but more deaths thanc<strong>on</strong>trols. The technique was used in a limited number of centres,mainly because of its cost, until a later blinded trial of 298 patientsin which c<strong>on</strong>trols underwent a sham procedure, showed no functi<strong>on</strong>albenefit and increased early complicati<strong>on</strong>s in laser-treatedpatients. 81 Percutaneous laser revascularizati<strong>on</strong> was not approvedby the FDA. Recent UK guidance c<strong>on</strong>cluded that it was ineffective,had unacceptable risks, and should not be used. 82 Some lasersystems are still commercially available, however, and occasi<strong>on</strong>allyused during surgery.When detailed professi<strong>on</strong>al recommendati<strong>on</strong>s are produced,there is some evidence that these are taken up by regulators.The 2007 report of the Academic Research C<strong>on</strong>sortium <strong>on</strong> clinicalendpoints in cor<strong>on</strong>ary stent trials 83 was cited in regulatory guidancepublished by the EC in 2008. 84 An earlier expert document85 and a more recent c<strong>on</strong>sensus c<strong>on</strong>ference <strong>on</strong> drug-elutingstents, both organized by the <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, had no official status but establisheda useful model of dialogue between clinical investigators,regulators, and industry. 58 It was recommended that the ECshould produce uniform standards in a guidance document 58 butthis has not yet been d<strong>on</strong>e, perhaps because the EC does nothave the authority or resp<strong>on</strong>sibility to commissi<strong>on</strong> such standards.Recent authors have advocated a balance between the moredetailed assessment c<strong>on</strong>ducted by the FDA and the more rapidresp<strong>on</strong>se to innovati<strong>on</strong>s that is possible in Europe. 86Diagnostic imaging<strong>Medical</strong> imaging has the highest growth rate within the health-caresector (≏10% per year) 87,88 but it may be the least supported byobjective data—for example, <strong>on</strong>ly 4.8% of the recommendati<strong>on</strong>sincluded in guidelines for radi<strong>on</strong>uclide imaging from the AmericanCollege of Cardiology and the American Heart Associati<strong>on</strong> aresupported by evidence from multiple randomized clinical trials 89although these have been recommended as the desired methodfor establishing the clinical efficacy of diagnostic devices. 90The hardware and software used by any company in an imagingsystem may be c<strong>on</strong>sidered as intellectual property and protectedby patents. If another company wishes to offer its customers equivalentdiagnostic tools, it must produce its own (quite possiblyunique) soluti<strong>on</strong>s to the engineering challenges, including decisi<strong>on</strong>sabout how the raw signals are obtained, processed, and smoothed,as well as how they are displayed. There is a single industry standardfor exporting images (digital images and communicati<strong>on</strong> inmedicine—DICOM) that is coordinated by the Associati<strong>on</strong> ofElectrical and <strong>Medical</strong> Imaging Equipment Manufacturers (NEMA)in the USA. DICOM is designed so that images from <strong>on</strong>emachine can be viewed <strong>on</strong> other systems, but it has not beenadapted for all new methods (such as real-time acquisiti<strong>on</strong> of 3Dimages) or fully applied by all manufacturers, and thus completeinteroperability remains elusive.It is increasingly apparent that detailed measurements obtainedusing the diagnostic equipment of <strong>on</strong>e manufacturer may vary substantiallyfrom the same measurements obtained in the samepatient by using a similar machine from a different manufacturer 91,92or by using a different imaging modality for the same purpose. 93 – 97 Inthe PROSPECT trial, echocardiography was used to try to identifyresp<strong>on</strong>ders to cardiac resynchr<strong>on</strong>izati<strong>on</strong> therapy (CRT); six differentmachines and more than six versi<strong>on</strong>s of software were used, from sixcompanies, and the analyses were performed in three core laboratories.98 Although the rati<strong>on</strong>ale for the study was logical, theresults were negative, perhaps because of wide inter-centre andinter-machine variability in measurements.Calls are now being made for more formal evaluati<strong>on</strong> and regulati<strong>on</strong>of imaging technologies, such as CT scanning 99 and magneticres<strong>on</strong>ance imaging. There is a need to c<strong>on</strong>sider the impact of i<strong>on</strong>izingradiati<strong>on</strong>, especially when safe alternatives are available; 100 if40-year-old subjects have CT cor<strong>on</strong>ary angiography, the risk thatthey may develop cancer has been estimated at 1 in 270 forwomen and 1 in 600 for men. 101 With imaging, the greatest riskto patients may be inappropriate use by an inexperienced operator.Appropriateness criteria do not fill the gap in evidencesince they represent the c<strong>on</strong>sensus view of experts as to whichtests are reas<strong>on</strong>able for which indicati<strong>on</strong>s, without guaranteeingthat there is evidence of clinical impact. Evaluati<strong>on</strong> of diagnosticstrategies should compare all the alternative tests for any particularclinical questi<strong>on</strong>. 102<strong>Cardiovascular</strong> implantable electr<strong>on</strong>icdevicesIt was estimated in 2007 that almost 700 000 patients in western andcentral Europe had implanted pacemakers, another 90 000 implantablecardioverter-defibrillators (ICDs), and 60 000 CRT. 103 Many newDownloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Page 8 of 18A.G. Fraser et al.c<strong>on</strong>cepts and devices have been developed in Europe. Advanced andeffective device therapy for arrhythmias and/or heart failure cantransform lives, and reliability of individual devices can be 99%. 104N<strong>on</strong>etheless, these advanced technologies still have risks, and electr<strong>on</strong>icdevices need to be evaluated and m<strong>on</strong>itored carefully.Fracture of pacemaker leads and technical failures of pacemakersare a recognized and accepted complicati<strong>on</strong>, and the rate of replacementbecause of pacemaker malfuncti<strong>on</strong> is decreasing. 105 L<strong>on</strong>gtermstudies are needed to assess chr<strong>on</strong>ic lead performance 106 butit is unclear how these will be funded or who should organizethem. Remote telem<strong>on</strong>itoring is now possible. As with diagnosticimaging, there may be differences between devices such as CRTwhich manufacturers offer as equivalent but which have differenttechnical specificati<strong>on</strong>s or treatment algorithms.There is less clear evidence that the risk of generator malfuncti<strong>on</strong>of an ICD is also declining. 107,108 Problems such as batterydepleti<strong>on</strong> 104 if unexpected can occasi<strong>on</strong>ally result in death attributableto device failure. 109 Major clinical, ethical, and legal problemsmay arise, as in a case where a young patient died when his ICDmalfuncti<strong>on</strong>ed; the unit had not been replaced, and the companyhad delayed giving any advice to physicians and patients althoughthey had known for .2 years that there was a risk of technicalfailure. 110 More recently, lawsuits have been filed against anothercompany after it too delayed disclosing informati<strong>on</strong>, this timeabout lead fractures. 111 Failure rates for the Medr<strong>on</strong>ic SprintFidelis lead have been estimated at 2.3% at 30 m<strong>on</strong>ths, or2.6 times the failure rate of a reference lead, and this fault cancause inappropriate shocks. 112It is difficult for physicians to know how to resp<strong>on</strong>d to advisorynotices issued by companies when technical problems are discoveredwith a particular device, because the risk associated withreplacement of a potentially faulty ICD device may be higherthan its risk of failure. 113 Even replacing faulty leads is associatedwith major complicati<strong>on</strong>s in 7% of patients. 114 One recommendedapproach is to offer elective replacement to device-dependentpatients when the ‘number needed to replace’ (NNR) is ,250. 115Automatic external defibrillators have been classified as class IIIdevices because of their similarity to other devices in that class, butmany reports of technical failures have been received by theFDA. 116 A discussi<strong>on</strong> paper proposed two opti<strong>on</strong>s—either toreclassify them to class II or to increase the levels of proof andtechnical performance and reliability required to be dem<strong>on</strong>stratedby manufacturers before these devices are approved; 117 the CirculatorySystem <strong>Devices</strong> Panel of the FDA recently recommendedthe sec<strong>on</strong>d opti<strong>on</strong>. Increased PMS has also been advocated 118although this may be difficult given the numbers of devices installedand their locati<strong>on</strong> in public places.Closure of patent foramen ovaleThe first use of a percutaneous device for closing a patent foramenovale (PFO) was reported in 1992. 119 At least 12 different PFOclosure devices have received CE marking. Risks include pericardialeffusi<strong>on</strong> and tamp<strong>on</strong>ade, unsuccessful deployment, incompleteclosure, device migrati<strong>on</strong>, thrombosis, and the development ofatrial fibrillati<strong>on</strong>. 120,121Between 1999 and 2002, the FDA approved two PFO occludersas Humanitarian Use <strong>Devices</strong>, which means that a device has beendesigned to treat a disease that occurs in fewer than 4000 peoplein the USA per year. The approved indicati<strong>on</strong> was limited topatients with recurrent cryptogenic stroke who had failed c<strong>on</strong>venti<strong>on</strong>aldrug therapy. Approval was granted through the regulatorypathway for Humanitarian Device Exempti<strong>on</strong> (HDE), and it wasbased up<strong>on</strong> clinical experience in ,100 patients with eachdevice. After approval of the HDEs, it became apparent thatmany PFO occluders were being implanted off-label for patientswith a first cryptogenic stroke who had not failed medicaltherapy. Enrolment in randomized IDE trials comparing deviceclosure with medical therapy was exceedingly slow. A systematicreview published in 2004 rec<strong>on</strong>firmed the need for randomizedstudies, 122 but recruitment c<strong>on</strong>tinued to lag because ‘some physicianshave c<strong>on</strong>cluded that the therapy is effective despite thelack of appropriate evidence’. 123 A re-analysis dem<strong>on</strong>strated thatthere were .4000 patients with cryptogenic stroke per yearwho might be candidates for PFO closure, and the two industrysp<strong>on</strong>sors voluntarily withdraw their HDEs in 2006. Enrolment instudies remained slow despite more recommendati<strong>on</strong>s fromFDA Advisory Panels and experts regarding the need for randomizedtrials, in 2007 124 and in 2009. 125Two trials have been completed. The MIST study in patients with aPFO and migraine, published in 2008, 126 and the CLOSURE-1 studyin patients with a PFO and cryptogenic stroke, 127 reported in2010 128 but not yet published, both found PFO closure to be nobetter than medical treatment. Unfortunately, the procedure isalready so ‘established’ that many clinicians remain unc<strong>on</strong>vinced.129 – 131 No PFO closure device has been approved in theUSA, but many devices c<strong>on</strong>tinue to be implanted in Europe; arecent report from a single centre included 825 patients. 132The case for reformClinical problems relating to failures of medical devices have led tomounting c<strong>on</strong>cerns over shortcomings in regulatory processes and133 – 143calls for their reform, both in Europe and in North America.Most detailed studies have been performed in the USA; forexample, more class III devices are approved by the FDA <strong>on</strong>510(k) exempti<strong>on</strong>s than by full clinical evaluati<strong>on</strong>, 136 <strong>on</strong>ly 27% ofclinical studies used to support premarket applicati<strong>on</strong>s for cardiovasculardevices were randomized, 135 and most devices which arerecalled had been approved without detailed evaluati<strong>on</strong>. 142 Unfortunately,the lack of informati<strong>on</strong> from the many competent authoritiesand NBs means that no comparable analyses are availablefor Europe. N<strong>on</strong>etheless, several major issues can be identified.(1) Complexity of the legislative frameworkThe main Directives of the EU have been amended several timesand supplemented by various implementing measures and interpretativedocuments. It is difficult for inexpert health-care professi<strong>on</strong>alsto understand fully this large body of texts. Algorithmscan be used to determine the probable class of a device 13 butthere is no website that can be visited to c<strong>on</strong>firm how a particularmedical device has been classified or to review the evidence <strong>on</strong>which it has been approved. There are substantial variati<strong>on</strong>sbetween the transpositi<strong>on</strong> measures and additi<strong>on</strong>al requirementsthat some Member States have adopted 4 because of the lack ofDownloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Clinical evaluati<strong>on</strong> of cardiovascular devices Page 9 of 18<strong>Table</strong> 2devicesExtracts from European and internati<strong>on</strong>al recommendati<strong>on</strong>s c<strong>on</strong>cerning the clinical evaluati<strong>on</strong> of medicalEuropean Commissi<strong>on</strong> Directive90/385/EEC;Annexes 1 and 7NB-MED/2.7/Rec3; Evaluati<strong>on</strong> of clinical data;Secti<strong>on</strong> 4.1European Commissi<strong>on</strong> MEDDEV 2.7.1;Annex X, Secti<strong>on</strong> 1.1Global Harm<strong>on</strong>izati<strong>on</strong> Task Force (2010);Study Group 5; Clinical investigati<strong>on</strong>sISO 14971 (2007); <strong>Medical</strong> devices—applicati<strong>on</strong>of risk management to medical devicesISO 14155 (2011); Clinical investigati<strong>on</strong> of medicaldevices for human subjects—good clinical practicedetailed guidance at the EU level. The current system is criticizedbecause there is reputed to be insufficient standardizati<strong>on</strong> and uniformityof performance across the NBs. There is no c<strong>on</strong>vincingclinical or public health argument why class III devices should beregulated in Europe by a fragmented system when a unifiedsystem is used to evaluate drugs.(2) Regulatory gaps and need to clarify boundariesSome new technologies are not regulated by the existing texts.Examples include electr<strong>on</strong>ic medical records (currently theobject of a European c<strong>on</strong>certed acti<strong>on</strong> to ensure inter-operabilitybetween Member States), software tools for supporting clinicaldecisi<strong>on</strong>s, and automated methods of quantifying diagnosticimaging. Inadequate security of a computerized database, a softwaremalfuncti<strong>on</strong>, or an err<strong>on</strong>eous measurement could all haveadverse clinical c<strong>on</strong>sequences for an individual patient. Incorporati<strong>on</strong>of medical devices into IT networks in the clinical envir<strong>on</strong>menthas been recognized as a less regulated area, and so a newstandard has been developed. 144 It is sometimes unclear whichdevices fall under which directive; special measures are requiredfor devices that have both mechanical, and biological or pharmaceutical,comp<strong>on</strong>ents (‘borderline’ products).There appears to be overlap and therefore some imprecisi<strong>on</strong>about the resp<strong>on</strong>sibilities of NBs, competent authorities, andhealth technology assessment: all three can c<strong>on</strong>sider clinicalevidence.(3) Weakness of the clinical data requirementsThe European guidance that is available about the clinical evaluati<strong>on</strong>of medical devices, mostly c<strong>on</strong>cerns good clinical practicesand the methodology of clinical trials—in other words, it isThe purpose of clinical investigati<strong>on</strong> is to verify that, under normal c<strong>on</strong>diti<strong>on</strong>s of use, theperformances of the device comply with those ...intended by the manufacturer ...in such away that their use does not compromise the clinical c<strong>on</strong>diti<strong>on</strong> or safety of patients 5The manufacturer is required by the Directive to perform a risk analysis .... From the results ofthe risk analysis, the manufacturer lays out how each risk is addressed and decides <strong>on</strong> theacceptability of risks when weighed against the intended benefits 145The objectives of a clinical investigati<strong>on</strong> must be to verify a positive benefit/risk profile of thedevice for the indicati<strong>on</strong>s and limitati<strong>on</strong>s of use as specified by the manufacturer 10Clinical investigati<strong>on</strong>s are necessary to provide the data not available through other sources (suchas literature or preclinical testing) required to dem<strong>on</strong>strate compliance with the relevantEssential Principles (including safety, clinical performance and acceptability of risk/benefit ratioassociated with its use) 24This Internati<strong>on</strong>al Standard specifies a process through which the manufacturer of a medicaldevice can identify hazards associated with a medical device, estimate and evaluate the risksassociated with these hazards, c<strong>on</strong>trol these risks, and m<strong>on</strong>itor the effectiveness of that c<strong>on</strong>trolFor each risk management plan the manufacturer should choose appropriate risk acceptabilitycriteria 27The clinical evaluati<strong>on</strong> includes an assessment and analysis of clinical data c<strong>on</strong>cerning safety orperformance of the investigati<strong>on</strong>al device .... The evaluati<strong>on</strong> shall be relevant to the intendedpurpose of the investigati<strong>on</strong>al device and the proposed method of use. It shall be designed ...toensure that the results ...have clinical relevance and scientific validity 28rather vague (<strong>Table</strong> 2). New ISO standards specify in detail howclinical studies of devices should be performed, 28 but they d<strong>on</strong>ot specify the possibly more important questi<strong>on</strong> of when theyare required. The GHTF Study Group 5 has stipulated thathuman clinical trials should address residual safety c<strong>on</strong>cerns thatcannot be resolved through pre-clinical testing or by evaluatingexisting clinical data. Specific criteria including standards appliedby the NBs are not readily available and particular essentialrequirements for the clinical evaluati<strong>on</strong> of individual types ofdevices are not published in EU guidance. Thus it is oftenunclear when there is a need for observati<strong>on</strong>al or randomizedclinical studies, and decisi<strong>on</strong>s may be inc<strong>on</strong>sistent. In most cases,it seems to be left to the manufacturer to evaluate potentialrisks and decide which clinical data will be sufficient for an applicati<strong>on</strong>to a NB for CE marking (see <strong>Table</strong> 2). There is overuseof equivalence as the basis for approval, 57 for example when an<strong>on</strong>-inferiority clinical trial with good statistical power has notbeen performed.<strong>Medical</strong> devices often undergo serial changes, appropriately, asmanufacturing processes evolve and the device is refined or newfacilities and tools are added. Such step-by-step ‘iterative’changes are offered by the device companies as minor modificati<strong>on</strong>sand they may be approved without repeating the processof clinical or regulatory evaluati<strong>on</strong>. At some point, however, asequence of iterative changes must represent a real change inthe device and re-evaluati<strong>on</strong> may be clinically important.It has been argued that registry studies c<strong>on</strong>ducted for thefurther clinical evaluati<strong>on</strong> of diagnostic and therapeutic devicesafter regulatory approval has been obtained, are the mainc<strong>on</strong>trol point for medical devices. 146 In general, these studieshave been c<strong>on</strong>ducted by industry. The manufacturer designs aDownloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Page 10 of 18A.G. Fraser et al.plan for PMS and proposes this to its NB; if the manufacturer thenalso selects the participating centres, there is a significant risk ofbias. New methods for automatically m<strong>on</strong>itoring large registriescan identify even low-frequency risks. 147,148(4) Accountability of the Notified BodiesGiven the large number of NBs, it may be difficult to ensure thatthey have comparable and high levels of specialist expertise, butthis is desirable for all NBs that review clinical data produced bymanufacturers in order to assess c<strong>on</strong>formity of class III devices.The claims for a device made by its manufacturer and the evaluati<strong>on</strong>of any particular device by any particular NB are not publiclyavailable. If approval of a new device has been granted <strong>on</strong> the basisof equivalence, it is not reported which data the manufacturer submittedin order to dem<strong>on</strong>strate that its new device performs thesame task as other devices which have previously been given a certificateand CE mark. It is inappropriate that resp<strong>on</strong>sibility forapproving PMS bel<strong>on</strong>gs to the NBs rather than the competentauthorities; the complexity and largely sporadic nature of communicati<strong>on</strong>sregarding FSCAs makes this unsatisfactory. When aNB receives fees from companies whose devices it assesses,there may be a c<strong>on</strong>flict of interest.There is no publicly available list of medical devices in Europe.Each NB or competent authority may have its own list but thereis currently no formal system for these lists to be shared or forthem to be made available for c<strong>on</strong>sultati<strong>on</strong> by patients or healthcareprofessi<strong>on</strong>als.(5) Insufficient use of expert medical adviceC<strong>on</strong>cerns have been expressed that there is dialogue betweenmanufacturers and regulatory authorities but academic cliniciansare rarely involved. 149 The organizati<strong>on</strong>s resp<strong>on</strong>sible for settingstandards, such as CENELEC and IEC, use a large network ofexperts, but their activities are supported and partly funded byindustry. Nati<strong>on</strong>al competent authorities and NBs have theirown advisers. The <strong>Medical</strong> <strong>Devices</strong> Unit of the EC takes advicefrom trade organizati<strong>on</strong>s, and individual scientists and clinicalresearchers serve as members of its scientific committee. No partnershipshave yet been established with professi<strong>on</strong>al medicalassociati<strong>on</strong>s at a European level, but the EC is open to participati<strong>on</strong>by all stakeholders. The EC is not involved in individual clinicalevaluati<strong>on</strong>s or approvals of particular devices (which are theresp<strong>on</strong>sibility of member states and NBs) and so there is no coordinatedsystem for obtaining detailed professi<strong>on</strong>al advice c<strong>on</strong>cerningnew high-risk devices.Balancing innovati<strong>on</strong> andregulati<strong>on</strong>One of the three main objectives of the strategy for health of theEU from 2008 to 2013 (published by the EC as a white paper in2007) is to support new technologies ‘which have the potentialto revoluti<strong>on</strong>ise healthcare and health systems’.35 Eighty percent of the companies in the medical device sector in the EUare small and medium enterprises (SMEs) 2 and so encouragingthe growth of this sector has been a foremost objective of theEC, particularly when the <strong>Medical</strong> <strong>Devices</strong> Unit was part of DGENTR. The health strategy also states, however, that new technologies‘must be evaluated properly, including for cost-effectivenessand equity’ and it affirms as a fundamental principle that ‘healthpolicy must be based <strong>on</strong> the best scientific evidence derivedfrom sound data and informati<strong>on</strong>, and relevant research.’ Formedical devices, it is not clear that this happens at the EU level.A key initiative of the Europe 2020 Strategy announced by theEC in 2010 is the ‘Innovati<strong>on</strong> Uni<strong>on</strong>’. One important objective isto promote research and development of new medicines, treatments,and diagnostic tools to improve quality of life for theelderly. 150 The document includes a general proposal to removebarriers to bring ideas to market, but c<strong>on</strong>cerning the objectiveof healthy ageing there are also specific statements relating tothe need to improve rules for clinical trials and testing of newmedicines by the EMA, and to ensure interoperability and thesetting of standards and reference specificati<strong>on</strong>s for newequipment.Rec<strong>on</strong>ciling these priorities—ec<strong>on</strong>omic sustainability and clinicalscrutiny—will be a key challenge for the planned recast of theEuropean medical device directives. Two seemingly c<strong>on</strong>flictingobjectives—to streamline and to enhance the legislati<strong>on</strong>—wererecognized in the public c<strong>on</strong>sultati<strong>on</strong> that the Commissi<strong>on</strong> initiatedin 2008 to seek advice from expert groups and ‘stakeholders’ <strong>on</strong>topics such as the clinical evaluati<strong>on</strong> of devices, vigilance, marketsurveillance, and transparency. 151 The 92 replies from industryalmost unanimously rejected the proposal to expand the role ofEMA in order to create a new European medical devices agency,whereas there was c<strong>on</strong>siderable support for this c<strong>on</strong>cept in 41replies from professi<strong>on</strong>al associati<strong>on</strong>s, academics, and patients. 152The argument is made, usually by industry, that tighter requirementsfor clinical testing of devices before approval would stifleinnovati<strong>on</strong> and delay the availability to clinicians of useful newtools for diagnosing or treating their patients. This ignores thefact that some innovati<strong>on</strong>s are led by advances in technology (‘soluti<strong>on</strong>sseeking applicati<strong>on</strong>s’) rather than being produced inresp<strong>on</strong>se to identified clinical needs. Many physicians—forexample, interventi<strong>on</strong>al cardiologists—also want to have earlyaccess to new devices and think that medical progress would becompromized and their patients might be disadvantaged if regulatoryapproval would take l<strong>on</strong>ger, but being at the forefr<strong>on</strong>t of technologicaladvances also implies resp<strong>on</strong>sibilities to ensure that newtreatments are safe and effective.The typical product cycle of a medical device is much shorterthan for a drug. The clinical value of an implantable or diagnosticdevice may be influenced by other factors, such as the expertiseof the operator. It is reas<strong>on</strong>able that regulatory systems shouldreflect these differences. Classical clinical trials are not alwayspossible or appropriate, but public health safety must always beassured by studies to establish a favourable risk/benefit ratio.Support for innovati<strong>on</strong> 153,140 in appropriate cases could be counterbalancedby more rigorous PMS.A premature c<strong>on</strong>clusi<strong>on</strong> that a device is effective can result inmore harm than good, whereas a premature decisi<strong>on</strong> that adevice is ineffective may deprive patients of useful treatment. Ifthere is any ‘residual safety c<strong>on</strong>cern’ then further clinical evaluati<strong>on</strong>should always be the priority.Downloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Clinical evaluati<strong>on</strong> of cardiovascular devices Page 11 of 18Figure 2 Recommended structure for approving and m<strong>on</strong>itoring medical devices, based <strong>on</strong> a single European agency overseeing detailedEuropean standards, assessed by a technical divisi<strong>on</strong> or by a small number of coordinated Notified Bodies who award a medical CE mark, followedby integrated health technology assessment and post-marketing surveillance. Clinical experts from professi<strong>on</strong>al medical associati<strong>on</strong>sshould c<strong>on</strong>tribute at many stages, as exemplified by the <str<strong>on</strong>g>ESC</str<strong>on</strong>g> logo.Recommendati<strong>on</strong>sThe Policy C<strong>on</strong>ference str<strong>on</strong>gly supported the plan for a substantialrecast of the Device Directives. This is an opportunity torec<strong>on</strong>sider the optimal governance of medical devices, goingback to basic principles. It is essential that evidence of clinical efficacyas well as safety and technical performance is establishedbefore approval of any devices whose use may be associatedwith more than trivial risks.(1) There should be a single, coordinated Europeansystem to oversee the evaluati<strong>on</strong> and approval of medicaldevicesThere should be integrati<strong>on</strong> and harm<strong>on</strong>izati<strong>on</strong> of processesbetween the competent authorities so that they apply uniformand higher standards. The most efficient way to achieve thiswould be the creati<strong>on</strong> of a single regulatory authority in the EU(Figure 2); it could be a medical devices divisi<strong>on</strong> of EMA or anew body, but its structure is less important than its functi<strong>on</strong>.There should be close collaborati<strong>on</strong> between agencies c<strong>on</strong>ductingPMS and those resp<strong>on</strong>sible for health technology assessment, aswell as increased internati<strong>on</strong>al collaborati<strong>on</strong>.(2) The NBs should be reorganized as an integratedstructureThe NBs should be reformed, with expertise c<strong>on</strong>cerning particulartypes of devices c<strong>on</strong>centrated in single centres (for uncomm<strong>on</strong>,high-risk devices) or <strong>on</strong>ly a few centres (for large categories).The regulatory authorities should direct applicati<strong>on</strong>s for assessmentof devices to the appropriate specialist NB(s). Thereshould be closer supervisi<strong>on</strong> and coordinati<strong>on</strong> of the NBs toensure that they have a single, high standard of excellence, experience,and competence. Opti<strong>on</strong>s would be for the divisi<strong>on</strong>s of NBsthat assess medical devices to become the technical divisi<strong>on</strong> of anew European medical devices agency, or they could remaindecentralized while operating within an integrated system.The use of the CE mark for medical devices should be reviewedas its meaning is often misunderstood. It may be interpreted byclinicians and patients as meaning that clinical effectiveness hasbeen established, for example from clinical trials, whereas itsimply implies c<strong>on</strong>formity with essential requirements includingan acceptable risk/benefit ratio. For implantable devices, a modifiedsystem should be c<strong>on</strong>sidered, that indicates the level of clinical evidenceestablished by trials.(3) The classificati<strong>on</strong> of each type of device should bebased <strong>on</strong> a detailed evaluati<strong>on</strong> of risksA risk-based classificati<strong>on</strong> is essential. This is the foundati<strong>on</strong> of thecurrent system of regulatory approval, but not all devices withineach class have similar levels of clinical risk. Actual risks shouldbe reflected in the clinical evidence required for a submissi<strong>on</strong>.For example, diagnostic imaging devices which use i<strong>on</strong>izing radiati<strong>on</strong>or c<strong>on</strong>trast agents have increased risks compared with safealternatives such as ultrasound. The class of each new deviceshould be c<strong>on</strong>sidered separately and not determined by the manufacturer.Internati<strong>on</strong>al c<strong>on</strong>cordance of classificati<strong>on</strong>s is important.Risk will be influenced by the populati<strong>on</strong> in which a device isused and so clinical indicati<strong>on</strong>s should be c<strong>on</strong>sidered when riskis being estimated. The system should be adaptable so that newdevices can be c<strong>on</strong>sidered promptly when they are introduced,before their l<strong>on</strong>g-term risks can be known. Also, the systemshould not restrict the applicati<strong>on</strong> of devices in special groupssuch as children, when the devices meet technical standards butlimited numbers of patients might make it difficult ever to collectdetailed informati<strong>on</strong> about risks.Downloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Page 12 of 18A.G. Fraser et al.Risk assessments should be undertaken for health informati<strong>on</strong>technology.(4) Product standards should be developed for eachcategory of medical device in class II and class IIIThere is a need for specific standards c<strong>on</strong>cerning not just the technicaldesign and performance but also the clinical performance andevaluati<strong>on</strong> and requirements for PMS, of each type of device inclass II and class III. Where these do not already exist, theyshould be developed, perhaps <strong>on</strong> an internati<strong>on</strong>al basis. Recommendati<strong>on</strong>sshould include requirements for clinical evaluati<strong>on</strong>including numbers of patients to be studied, and guidance whenclinical trials are needed to dem<strong>on</strong>strate an impact <strong>on</strong> clinical outcomes.These requirements should be binding <strong>on</strong> manufacturers.The design of trials may vary according to the class of a device,risk/benefit ratios, and the characteristics of the patients inwhom it is used. There should be fewer approvals of new‘me-too’ devices <strong>on</strong> the basis of equivalence, and standardsshould define when this would be acceptable. Approval for theuse of a device should include a statement of its clinical indicati<strong>on</strong>s.Clinical evaluati<strong>on</strong> should be extended to diagnostic imaging.Standards should determine acceptable limits of performanceagainst imaging phantoms (test objects) and when feasible, acceptablelevels of diagnostic accuracy.Standards should be produced independently, without involvementby the organizati<strong>on</strong>s resp<strong>on</strong>sible for assessing c<strong>on</strong>formityof devices. Manufacturers or members of trade associati<strong>on</strong>s canadvise or participate as technical experts but they should nothave resp<strong>on</strong>sibility for writing or approving standards. The EU ornati<strong>on</strong>al competent authorities should fund the producti<strong>on</strong> ofdetailed standards.(5) Expert professi<strong>on</strong>al advice is requiredProfessi<strong>on</strong>al associati<strong>on</strong>s such as the European Society of Cardiologyare key stakeholders in developing policy c<strong>on</strong>cerning medicaldevices, as they represent networks of physicians who develop,use, and evaluate devices in daily clinical practice, and who understandand practise different methods of clinical assessment. Obtainingexpert advice, for example from (bio)materials scientists,physicists, engineers, academic specialists, practising physicians,and nurses, should be an integral part of the regulatory process.Such independent advisers should be involved in setting standards,reviewing decisi<strong>on</strong>s about approval of new class III devices, definingclinical indicati<strong>on</strong>s, performing health technology assessment, anddesigning and c<strong>on</strong>ducting programmes for PMS (Figure 2). Representativeswith appropriate training and experience should benominated by major medical associati<strong>on</strong>s in Europe to bemembers of the main advisory committees.It is important that the experience and opini<strong>on</strong>s of patients whouse devices or who have received implantable devices should alsobe obtained and c<strong>on</strong>sidered.(6) Adequate transparency is essentialLegislati<strong>on</strong> enacted by the European Parliament in 2001 <strong>on</strong>freedom of informati<strong>on</strong> enshrined the right of access of Europeancitizens to documents of the EC and its agencies. 154 There arecompelling clinical reas<strong>on</strong>s why transparency should be extendedto documents relating to the approval of medical devices.Currently, it is difficult for physicians to identify the class of anyparticular device or to obtain its essential requirements as evaluatedby the NBs. Technical standards such as those produced byISO can <strong>on</strong>ly be c<strong>on</strong>sulted by purchasing the documents. Formedical devices, such informati<strong>on</strong> should be freely available inthe public domain.The c<strong>on</strong>tent of dossiers prepared by companies when submittingtheir devices for approval, apart from any manufacturingdetails that are protected intellectual property, should be disclosedto physicians so that they can know the technical performance ofthe devices that they use. They should be able to review comparis<strong>on</strong>sof the performance of devices within the same category.Patients should be able to obtain informati<strong>on</strong> such as reports ofmalfuncti<strong>on</strong>ing devices, preferably together with professi<strong>on</strong>aladvice from physicians. 155(7) The c<strong>on</strong>cept of c<strong>on</strong>diti<strong>on</strong>al approval of a medicaldevice, pending further clinical evaluati<strong>on</strong>, should bedevelopedWhen a new device is developed that represents a major technicaladvance and an important new opti<strong>on</strong> for treatment, then earlyapproval may be appropriate as l<strong>on</strong>g as initial clinical safety and efficacyhave been established and the clinical benefits from its use arelikely to outweigh any anticipated risks. There would still be a need,however, for larger, l<strong>on</strong>ger, or randomized clinical studies to beperformed. In such circumstances, CE marking might be awardedfor a limited period (such as 2 or 3 years), c<strong>on</strong>diti<strong>on</strong>al <strong>on</strong> the manufacturerreporting back to the regulatory authority before theexpiry of that time period with the results of any further clinicalstudies that have been specified as the c<strong>on</strong>diti<strong>on</strong> of approval. Ifnew evidence is not submitted, then permissi<strong>on</strong> for c<strong>on</strong>tinuedmarketing of the device would be withdrawn. The new categorycould be called ‘C<strong>on</strong>diti<strong>on</strong>al Approval of a Device, pending clinicaltrial’. For diagnostic imaging, a similar c<strong>on</strong>cept has been describedas ‘coverage with evidence development’. 156 This proposal is notthe same as an IDE, because the device could be CE markedwhile the manufacturer is mandated to undertake specific clinicalresearch studies in additi<strong>on</strong> to PMS.The current directives already allow for compassi<strong>on</strong>ate use andinvestigati<strong>on</strong>al device approval, but this is granted by a nati<strong>on</strong>alcompetent authority and not at the European level.(8) Outcome studies after device implantati<strong>on</strong> should beundertaken as a partnership between physicians,companies, and regulatorsPost-marketing surveillance should be initiated by the manufacturerbut PMS should not be the sole resp<strong>on</strong>sibility of industry.Follow-up studies should be proposed and coordinated by regulatoryagencies or HTA bodies with the assistance of independentexperts from professi<strong>on</strong>al scientific associati<strong>on</strong>s (such as the<str<strong>on</strong>g>ESC</str<strong>on</strong>g> 155 ). Funding for such studies might vary, from manufacturersto the EU itself, depending <strong>on</strong> the scope of informati<strong>on</strong> being gatheredand its relevance to a specific device or to public health.These studies should evaluate the characteristics of patients undergoingdiagnostic or therapeutic procedures using devices includingDownloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Clinical evaluati<strong>on</strong> of cardiovascular devices Page 13 of 18off-label applicati<strong>on</strong>s, document immediate complicati<strong>on</strong>s, andstudy medium and l<strong>on</strong>g-term outcomes including instances ofdevice failure. To ensure that data are representative, outcomesshould be collected from centres in all Member States thatreflect different types and volumes of practice and the full rangeof complexity of clinical cases. Protocols and case record forms(CRFs) should be discussed and validated by academic experts,regulators, and companies. The database should not be the propertyof industry, and the main results should be freely available. Acollaborati<strong>on</strong> between EU regulatory bodies, the FDA, and scientificassociati<strong>on</strong>s would allow coordinati<strong>on</strong> of reporting systemsand more complete evaluati<strong>on</strong> of safety issues related to newlymarketed devices. This will complement the sharing of reportsof adverse events and clinical alerts that is being developed byEudamed.(9) Limits to iterative changes should be definedDetailed standards for each type of device should specify whichmodificati<strong>on</strong>s could reas<strong>on</strong>ably be described as minor, and whichothers would warrant complete resubmissi<strong>on</strong> for approval as anew device. For example, if any modificati<strong>on</strong> has been submittedfor a new patent, or if the materials used to make a device havebeen changed, then a de novo applicati<strong>on</strong> should be required.(10) Regulatory systems should retain flexibility for specialcircumstancesThe system of regulatory approval should allow prototype or innovativedevices to be approved for use in special circumstanceswhen urgent clinical needs can <strong>on</strong>ly be met by their deployment.A comm<strong>on</strong> European equivalent of the HDE is required.Special c<strong>on</strong>siderati<strong>on</strong> might also be given to categories ofmedical device that are important but used so infrequently thatthey are not ec<strong>on</strong>omically viable. C<strong>on</strong>tinuing clinical availability of‘orphan devices’ might be supported by a grant from a comm<strong>on</strong>fund—for example, if a device is ‘last in class’.It may be difficult for devices used in paediatric cardiology tomeet the standards and levels of clinical evidence required fordevices used in adults, if numbers of patients are small or ifdevices are customized for each patient. Off-label use iscomm<strong>on</strong>. Approval <strong>on</strong> the basis of limited evidence might thenneed to be balanced by more strict requirements for careful andcomplete PMS. 157(11) Manufacturers should be resp<strong>on</strong>sible for the clinicalevaluati<strong>on</strong> of all class II and class III devicesCompanies that manufacture any class II or class III devices shouldbe resp<strong>on</strong>sible for initiating independently m<strong>on</strong>itored clinicalstudies of their devices, including randomized c<strong>on</strong>trolled trialswhen these are required according to new standards, and alsofor supporting PMS. Researchers should have full access to theresults of any clinical study so that they can c<strong>on</strong>duct an independentstatistical analysis, and the results should be publishedwhether they are negative or positive. Clinical trials evaluatingmedical devices should be registered in a central database. 158Depending <strong>on</strong> the class of device, companies should also trainmedical and nursing staff in the correct and safe use of theirdevices.(12) Physicians should understand and engage with theregulatory systems for medical devicesPhysicians have a resp<strong>on</strong>sibility to practice evidence-based medicinewhen using devices, and they should encourage their patientsto participate in clinical trials when these are required, especiallywhen there is equipoise. Physicians are keen to adopt newdevices early but not as keen to undertake systematic m<strong>on</strong>itoringafterwards; they should c<strong>on</strong>tribute routinely to PMS as this may bethe <strong>on</strong>ly means by which unsuspected problems are discovered. Itis the duty of physicians to report any failure of a device. C<strong>on</strong>siderati<strong>on</strong>could be given in the case of high-risk devices to making participati<strong>on</strong>in PMS mandatory, as a requirement either for c<strong>on</strong>tinuedaccess to the device for their patients or to reimbursement of thehospital for its use. Professi<strong>on</strong>al societies should promote interestin the evaluati<strong>on</strong> of innovative medical devices, through c<strong>on</strong>tinuingmedical educati<strong>on</strong>.It is unethical for any physician to accept payment from amedical device company for the use of its device. If physicianshave any financial interest in a device, they should disclose thisinformati<strong>on</strong> when reporting its performance or seeking c<strong>on</strong>sentfor its use.C<strong>on</strong>flict of interest: A.G.F. acknowledges support to hisinstituti<strong>on</strong> for research from Hitachi-Aloka and GE Ultrasound.J-C.D. is a c<strong>on</strong>sultant and member of the speakers’ bureaux forEBR Systems Inc, Medtr<strong>on</strong>ic, Sorin, and St Jude <strong>Medical</strong>. N.A.M.receives modest c<strong>on</strong>sulting fees from Bost<strong>on</strong> Scientific, andMedtr<strong>on</strong>ic. M.W.K. is a special government employee of theFDA. P.E.V. is a c<strong>on</strong>sultant for Medtr<strong>on</strong>ic and has receivedsupport to his instituti<strong>on</strong> for research from St Jude <strong>Medical</strong>.F.VdW, S.C.S, and M.K. have no c<strong>on</strong>flicts of interest related tothis article.AppendixParticipants in Policy C<strong>on</strong>ferenceStefan Anker, President Elect of the Heart Failure Associati<strong>on</strong> ofthe <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, Charité Hospital Berlin, Germany. Angelo Auricchio, PresidentElect of the European Heart Rhythm Associati<strong>on</strong>, F<strong>on</strong>dazi<strong>on</strong>eCardiocentro Ticino, Switzerland. Steven Bailey, PastPresident of the Society of Cardiac Angiography and Interventi<strong>on</strong>s,Health Science Center, San Ant<strong>on</strong>io, TX, USA. Philipp B<strong>on</strong>hoeffer,Institute of Child Health, University College L<strong>on</strong>d<strong>on</strong>, UK. MartinBorggrefe, Councillor, <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, Universitätsmedizin Mannheim,Germany. Lars-Åke Brodin, Professor of <strong>Medical</strong> Engineering andDean, School of Technology and Health, Royal Institute of Technology,Stockholm, Sweden. Nico Bruining, Past Chairman, <str<strong>on</strong>g>ESC</str<strong>on</strong>g>Working Group <strong>on</strong> Computers in Cardiology, Erasmus <strong>Medical</strong>Center-Thoraxcentre, Rotterdam, Netherlands. Peter Buser, <str<strong>on</strong>g>ESC</str<strong>on</strong>g>Council <strong>on</strong> <strong>Cardiovascular</strong> Imaging, University Hospital, Basel,Switzerland. Eric Butchart, Past Chairman, <str<strong>on</strong>g>ESC</str<strong>on</strong>g> Working Group<strong>on</strong> Valvular Heart Disease, University Hospital of Wales, Cardiff,UK. Jose Calle Gordo, Chairman <strong>Cardiovascular</strong> Sector,EUCOMED, Brussels, Belgium. John Cleland, Past President,Heart Failure Associati<strong>on</strong> of the <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, University of Hull, UK.Nicolas Danchin, European Affairs Committee, <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, HôpitalDownloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Page 14 of 18A.G. Fraser et al.Européen Georges Pompidou, Paris, France. J.-C.D., EuropeanAffairs Committee, <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, C.H.R.U. de P<strong>on</strong>tchaillou, Rennes,France. Muzaffer Degertekin, Councillor, European Society ofCardiology, Yeditepe University Hospital, Istanbul, Turkey. IsabelleDemade, <strong>Medical</strong> <strong>Devices</strong> Unit, DG SANCO, European Commissi<strong>on</strong>,Brussels, Belgium. Nicole Denjoy, Secretary General, COCIR,Brussels, Belgium. Geneviève Derumeaux, Councillor, <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, President,French Society of Cardiology, Hôpital Louis Pradel, Ly<strong>on</strong>,France. Carlo di Mario, President of the European Associati<strong>on</strong> ofPercutaneous Cor<strong>on</strong>ary Interventi<strong>on</strong>s, Royal Brompt<strong>on</strong> Hospital,L<strong>on</strong>d<strong>on</strong>, UK. Kenneth Dickstein, Past-President, Heart FailureAssociati<strong>on</strong> of the <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, Stavanger University Hospital, Stavanger,Norway. Dariusz Dudek, European Associati<strong>on</strong> of PercutaneousCor<strong>on</strong>ary Interventi<strong>on</strong>s, Institute of Cardiology, Krakow, Poland.M.E., American Heart Associati<strong>on</strong>, Tufts University School ofMedicine, Bost<strong>on</strong>, MA, USA. Andrew Farb, Center for <strong>Devices</strong>and Radiological Health, Food and Drug Administrati<strong>on</strong>, SilverSpring, MD, USA. Albert Flotats, Chairpers<strong>on</strong>, <strong>Cardiovascular</strong>Committee, European Associati<strong>on</strong> of Nuclear Medicine, HospitalSant Pau, Barcel<strong>on</strong>a, Spain. A.G.F., Past-President, EuropeanAssociati<strong>on</strong> of Echocardiography, Wales Heart Research Institute,Cardiff University, UK. Pascal Gueret, European Associati<strong>on</strong> ofEchocardiography, Henri M<strong>on</strong>dor University Hospital, Creteil,France. Carsten Israel, European Heart Rhythm Associati<strong>on</strong>, EvangelischesKrankenhaus Bielefeld, Germany. Stefan James, Chairman,Databases and Registries, European Associati<strong>on</strong> of PercutaneousCor<strong>on</strong>ary Interventi<strong>on</strong>s, Uppsala Clinical Research Centre,Sweden. Josef Kautzner, Councillor, <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, Institute for Clinicaland Experimental Medicine, Prague, Czech Republic. M.K., Presidentof the <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, CHU Pitié Salpêtrière, Paris, France. M.W.K.,American College of Cardiology, Duke Clinical Research Institute/DukeUniversity <strong>Medical</strong> Center, Durham, NC, USA.Massimo Lombardi, Past-Chairman, <str<strong>on</strong>g>ESC</str<strong>on</strong>g> Working Group <strong>on</strong><strong>Cardiovascular</strong> Magnetic Res<strong>on</strong>ance, CNR—Nati<strong>on</strong>al ResearchCouncil, Pisa, Italy. Tom Marwick, Cleveland Clinic, Cleveland,OH, USA; Princess Alexandra Hospital, University of Queensland,Australia. Muriel Mioulet, Director, Advocacy and Representati<strong>on</strong>,<str<strong>on</strong>g>ESC</str<strong>on</strong>g>, European Heart House, Sophia Antipolis, France. SophieO’Kelly, Head of European Affairs, <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, European Heart House,Sophia Antipolis, France. Pasquale Perr<strong>on</strong>e-Filardi, ChairmanElect, <str<strong>on</strong>g>ESC</str<strong>on</strong>g> Working Group <strong>on</strong> Nuclear Cardiology and CardiacCT, Universita’ Federico II, Napoli, Italy. Giuseppe Rosano,IRCCS San Raffaele Hospital, Roma, Italy. Raphael Rosenhek,Chairman Elect, <str<strong>on</strong>g>ESC</str<strong>on</strong>g> Working Group <strong>on</strong> Valvular Heart Disease,<strong>Medical</strong> University of Vienna, Austria. Manel Sabate, Boardmember, European Associati<strong>on</strong> of Percutaneous Cor<strong>on</strong>ary Interventi<strong>on</strong>s,University of Barcel<strong>on</strong>a, Spain. S.C.S., Jr, President ofthe World Heart Federati<strong>on</strong>, Geneva, Switzerland; Professor ofMedicine, University of North Carolina, Chapel Hill NC, USA.Eva Swahn, Vice President of the <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, Linköping Heart Centre,Sweden. Luigi Tavazzi, Chairman, EurObservati<strong>on</strong>al Research Programmeof the <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, Gvm Care & Research, Cotignola, Italy. F.W.,Chairman, European Affairs Committee of the <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, Catholic UniversityLeuven, Belgium. Enno van der Velde, Chairman, <str<strong>on</strong>g>ESC</str<strong>on</strong>g>Working Group <strong>on</strong> Computers in Cardiology, Leiden University<strong>Medical</strong> Center, Leiden, Netherlands. Lex van Herwerden,Professor of Cardiac Surgery, University <strong>Medical</strong> Center Utrecht,Netherlands. P.E.V., President Elect of the <str<strong>on</strong>g>ESC</str<strong>on</strong>g>, Herakli<strong>on</strong> UniversityHospital, Greece. Jens-Uwe Voigt, Chairman, Educati<strong>on</strong>Committee, European Associati<strong>on</strong> of Echocardiography, CatholicUniversity Leuven, Belgium. Douglas Weaver, Past President ofthe American College of Cardiology, Henry Ford Hospital,Detroit, MI, USA. Peter Wilmshurst, C<strong>on</strong>sultant Cardiologist,Royal Shrewesbury Hospital, UK. Disclosures of interestsof participants are available from the European Society ofCardiology.References1. Directive 2007/47/EC of the European Parliament and of the Council of 5 September2007 amending Council Directive 90/385/EEC <strong>on</strong> the approximati<strong>on</strong> of thelaws of the Member States relating to active implantable medical devices,Council Directive 93/42/EEC c<strong>on</strong>cerning medical devices and Directive 98/8/ECc<strong>on</strong>cerning the placing of biocidal products <strong>on</strong> the market. http://ec.europa.eu/c<strong>on</strong>sumers/sectors/medical-devices/files/revisi<strong>on</strong>_docs/2007-47-en_en.pdf.2. http://ec.europa.eu/c<strong>on</strong>sumers/sectors/medical-devices/competitiveness/factsfigures/index_en.htm.3. Directive 2001/83/EC of the European Parliament and of the Council of 6November 2001 <strong>on</strong> the Community code relating to medicinal products forhuman use (Article 10). http://ec.europa.eu/health/files/eudralex/vol-1/dir_2001_83_c<strong>on</strong>s2009/2001_83_c<strong>on</strong>s2009_en.pdf.4. Roadmap. Proposal for a Directive of the European Parliament and of theCouncil c<strong>on</strong>cerning medical devices and repealing Directives 90/385/EECand 93/42/EEC (recast). http://ec.europa.eu/governance/impact/planned_ia/docs/2008_sanco_081_medical_devices_en.pdf.5. Council Directive 90/385/EEC of 20 June 1990 <strong>on</strong> Active Implantable <strong>Medical</strong> <strong>Devices</strong>(AIMDD). http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=CONSLEG:1990L0385:20071011:en:PDF.6. Council Directive 93/42/EEC of 14 June 1993 c<strong>on</strong>cerning medical devices. http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=CONSLEG:1993L0042:20071011:en:PDF.7. Council Directive 98/79/EC of 27 October 1998 <strong>on</strong> In Vitro Diagnostic <strong>Medical</strong> <strong>Devices</strong>(IVDMD). http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=CONSLEG:1998L0079:20031120:en:PDF.8. Communicati<strong>on</strong> of the Commissi<strong>on</strong> to the European Parliament, the Council,the European Ec<strong>on</strong>omic and Social Committee and the Committee of theRegi<strong>on</strong>s. Implementing the Community Lisb<strong>on</strong> programme: A strategy for thesimplificati<strong>on</strong> of the regulatory envir<strong>on</strong>ment. Brussels, 25.10.2005.COM(2005) 535 final.9. Commissi<strong>on</strong> Decisi<strong>on</strong> of 27 November 2009 amending Decisi<strong>on</strong> 2002/364/EC<strong>on</strong> comm<strong>on</strong> technical specificati<strong>on</strong>s for in vitro diagnostic medical devices.2009/886/EC. OJ L 318, 4.12.2009, 25–40.10. European Commissi<strong>on</strong>. Guidelines <strong>on</strong> medical devices. Clinical evaluati<strong>on</strong>: a guide formanufacturers and notified bodies. MEDDEV 2.7.1 Rev.3 December 2009. http://ec.europa.eu/c<strong>on</strong>sumers/sectors/medical-devices/files/meddev/2_7_1rev_3_en.pdf.11. European Commissi<strong>on</strong>. Guidelines <strong>on</strong> medical devices. Guidelines <strong>on</strong> clinicalinvestigati<strong>on</strong>: a guide for manufacturers and notified bodies. MEDDEV 2.7/4December 2010. http://ec.europa.eu/c<strong>on</strong>sumers/sectors/medical-devices/files/meddev/2_7_4_en.pdf.12. European Commissi<strong>on</strong>. <strong>Medical</strong> devices. Guidance document. Guidelines <strong>on</strong> amedical devices vigilance system. MEDDEV 2.12-1 Rev 6 December 2009.http://ec.europa.eu/c<strong>on</strong>sumers/sectors/medical-devices/files/meddev/2_12_1-rev_6-12-2009_en.pdf.13. European Commissi<strong>on</strong>. <strong>Medical</strong> <strong>Devices</strong>. Guidance Document. Classificati<strong>on</strong> ofmedical devices. MEDDEV 2.4/1 Rev. 9 June 2010, http://ec.europa.eu/c<strong>on</strong>sumers/sectors/medical-devices/files/meddev/2_4_1_rev_9_classificati<strong>on</strong>_en.pdf.14. Commissi<strong>on</strong> communicati<strong>on</strong> in the framework of the implementati<strong>on</strong> of CouncilDirective 90/385/EEC of 20 June 1990 <strong>on</strong> the approximati<strong>on</strong> of the laws of theMember States relating to active implantable medical devices. (Publicati<strong>on</strong> oftitles and references of harm<strong>on</strong>ised standards under the directive). (2011/C16/01), http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:C:2011:016:0001:0007:EN:PDF.15. Global Harm<strong>on</strong>izati<strong>on</strong> Task Force. Clinical evidence—key definiti<strong>on</strong>s and c<strong>on</strong>cepts.May 2007. SG5/N1R8:2007.16. European Commissi<strong>on</strong>. Enterprise and Industry. Nando (New Approach Notifiedand Designated Organisati<strong>on</strong>s) Informati<strong>on</strong> System. http://ec.europa.eu/enterprise/newapproach/nando/index.cfm?fuseacti<strong>on</strong>=directive.main.17. European Commissi<strong>on</strong>. Committees/Working Groups c<strong>on</strong>tributing to theimplementati<strong>on</strong> of the <strong>Medical</strong> Device Directives. MEDDEV 2.15 RevDownloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Clinical evaluati<strong>on</strong> of cardiovascular devices Page 15 of 183. December 2008. http://ec.europa.eu/c<strong>on</strong>sumers/sectors/medical-devices/files/meddev/2_15_3___12-2008_en.pdf.18. Commissi<strong>on</strong> Decisi<strong>on</strong> of 19 April 2010 <strong>on</strong> the European Databank <strong>on</strong> <strong>Medical</strong><strong>Devices</strong> (Eudamed). (notified under document C(2010) 2363) (2010/227/EU),http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2010:102:0045:0048:en:PDF.19. http://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/<strong>Medical</strong><strong>Devices</strong>/<strong>Medical</strong><strong>Devices</strong>AdvisoryCommittee/ucm124098.htm.20. Supreme Court of the United States (2008). Riegel vs Medtr<strong>on</strong>ic, Inc. (No.06-179).21. Wizemann T (ed). Public health effectiveness of the FDA 510(k) clearanceprocess: measuring postmarket performance and other select topics. WorkshopReport. Washingt<strong>on</strong>, Institute of Medicine, 2011.22. Food and Drug Administrati<strong>on</strong>. 510(k) and Science Report Recommendati<strong>on</strong>s:Summary and overview of comments and next steps. http://www.fda.gov/downloads/AboutFDA/CentersOffices/CDRH/CDRHReports/UCM239449.pdf.23. Global Harm<strong>on</strong>izati<strong>on</strong> Task Force. Study Group 5. Clinical evaluati<strong>on</strong>. May 2007.http://www.ghtf.org/documents/sg5/sg5_n2r8_2007final.pdf.24. Global Harm<strong>on</strong>izati<strong>on</strong> Task Force. Study Group 5. Clinical investigati<strong>on</strong>s. 12February 2010. http://www.ghtf.org/documents/sg5/sg5_n3_2010.pdf.25. Global Harm<strong>on</strong>izati<strong>on</strong> Task Force. Study Group 5. Post-market clinicalfollow-up studies. 18 February 2010. http://www.ghtf.org/documents/sg5/sg5_n4_2010.pdf.26. Global Harm<strong>on</strong>izati<strong>on</strong> Task Force. Statement from the Chair—Update <strong>on</strong>Future Directi<strong>on</strong>s of GHTF, 2011. http://ghtf.org/documents/statement-future-2011.pdf.27. Internati<strong>on</strong>al Standardizati<strong>on</strong> Organisati<strong>on</strong>. Internati<strong>on</strong>al Standard. <strong>Medical</strong>devices—applicati<strong>on</strong> of risk management to medical devices. ISO 14971:2007.28. Internati<strong>on</strong>al Standardizati<strong>on</strong> Organisati<strong>on</strong>. Internati<strong>on</strong>al Standard. Clinical investigati<strong>on</strong>of medical devices for human subjects—good clinical practice. ISO14155:2011.29. Kristensen FB, Lampe K, Chase DL, Lee-Robin SH, Wild C, Moharra M,Garrido MV, Nielsen CP, Røttingen JA, Neikter SA, Bistrup ML. Practical toolsand methods for health technology assessment in Europe: structures, methodologies,and tools developed by the European Network for Health TechnologyAssessment, EUnetHTA. Int J Technol Assess Health Care 2009;25(Suppl. 2):1–8.30. Lampe K, Makela M, Garrido MV, Anttila H, Autti-Rämö I, Hicks NJ, Hofmann B,Koivisto J, Kunz R, Kärki P, Malmivaara A, Meiesaar K, Reiman-Möttönen P,Norderhaug I, Pasternack I, Ruano-Ravina A, Räsänen P, Saalasti-Koskinen U,Saarni SI, Walin L, Kristensen FB. The HTA Core Model: a novel method for producingand reporting health technology assessments. Int J Technol Assess HealthCare 2009;25(Suppl. 2):9–20.31. World Health Organizati<strong>on</strong>. <strong>Medical</strong> Device Regulati<strong>on</strong>s: Global Overview andGuiding Principles. Geneva: WHO; 2003.32. World Health Organizati<strong>on</strong>. <strong>Medical</strong> <strong>Devices</strong>: Managing the Mismatch: An Outcomeof the Priority <strong>Medical</strong> <strong>Devices</strong> Project. Geneva: WHO; 2010.33. Sixtieth World Health Assembly. Health Technologies. WHA60.29, 23 May2007. http://www.who.int/medical_devices/resoluti<strong>on</strong>_wha60_29-en1.pdf.34. World Health Organizati<strong>on</strong>. Medium-term Strategic Plan 2008–2013. Geneva:WHO; November 2008.35. Commissi<strong>on</strong> of the European Communities. White Paper. Together for health: astrategic approach for the EU 2008–2013. Brussels, 23.10.2007, COM (2007)630. http://ec.europa.eu/health/ph_overview/Documents/strategy_wp_en.pdf.36. Lindblom D, Björk VO, Semb BK. Mechanical failure of the Björk-Shiley valve.Incidence, clinical presentati<strong>on</strong>, and management. J Thorac Cardiovasc Surg1986;92:894–907.37. Ostermeyer J, Horstkotte D, Bennett J, Huysmans H, Lindblom D, Olin C,Orinius E, Semb G. The Björk-Shiley 70 degree c<strong>on</strong>vexo-c<strong>on</strong>cave prosthesisstrut fracture problem (present state of informati<strong>on</strong>). Thorac Cardiovasc Surg1987;35:71–77.38. Blot WJ, Ibrahim MA, Ivey TD, Aches<strong>on</strong> DE, Brookmeyer R, Weyman A,Defauw J, Smith JK, Harris<strong>on</strong> D. Twenty-five-year experience with the Björk-Shiley c<strong>on</strong>vexoc<strong>on</strong>cave heart valve: a c<strong>on</strong>tinuing clinical c<strong>on</strong>cern. Circulati<strong>on</strong>2005;111:2850–2857.39. Blackst<strong>on</strong>e EH. Could it happen again? the Björk-Shiley c<strong>on</strong>vexo-c<strong>on</strong>cave heartvalve story. Circulati<strong>on</strong> 2005;111:2717–2719.40. Ericss<strong>on</strong> A, Lindblom D, Semb G, Huysmans HA, Thulin LI, Scully HE,Bennett JG, Ostermeyer J, Grunkemeier GL. Strut fracture with Björk-Shiley70 degrees c<strong>on</strong>vexo-c<strong>on</strong>cave valve. An internati<strong>on</strong>al multi-instituti<strong>on</strong>al follow-upstudy. Eur J Cardiothorac Surg 1992;6:339–346.41. van der Graaf Y, de Waard F, van Herwerden LA, Defauw J. Risk of strut fractureof Björk-Shiley valves. Lancet 1992;339:257–261.42. de Mol BA, Overkamp PJ, van Gaalen GL, Becker AE. N<strong>on</strong>-destructive assessmentof 62 Dutch Björk-Shiley c<strong>on</strong>vexo-c<strong>on</strong>cave heart valves. Eur J CardiothoracSurg 1997;11:703–708.43. Schaff HV, Carrel TP, Jamies<strong>on</strong> WR, J<strong>on</strong>es KW, Rufilanchas JJ, Cooley DA,Hetzer R, Stumpe F, Duveau D, Moseley P, van Boven WJ, Grunkemeier GL,Kennard ED, Holubkov R. Artificial Valve Endocarditis Reducti<strong>on</strong> Trial. Paravalvularleak and other events in silz<strong>on</strong>e-coated mechanical heart valves: a reportfrom AVERT. Ann Thorac Surg 2002;73:785–792.44. I<strong>on</strong>escu A, Payne N, Fraser AG, Giddings J, Grunkemeier GL, Butchart EG. Incidenceof embolism and paravalvar leak after St Jude Silz<strong>on</strong>e valve implantati<strong>on</strong>:experience from the Cardiff Embolic Risk Factor Study. Heart 2003;89:1055–1061.45. Tweden KS, Camer<strong>on</strong> JD, Razzouk AJ, Bianco RW, Holmberg WR, Bricault RJ,Barry JE, Tobin E. Silver modificati<strong>on</strong> of polyethylene terephthalate textiles forantimicrobial protecti<strong>on</strong>. ASAIO J 1997;43:M475–481.46. O’Shea JC, Kramer JM, Califf RM, Peters<strong>on</strong> ED. Sharing a commitment toimprove cardiovascular devices. Part I: identifying holes in the safety net. AmHeart J 2004;147:977–984.47. Gross JM, Shu MC, Dai FF, Ellis J, Yoganathan AP. A microstructural flow analysiswithin a bileaflet mechanical heart valve hinge. J Heart Valve Dis 1996;5:581–590.48. Ellis JT, Healy TM, F<strong>on</strong>taine AA, Saxena R, Yoganathan AP. Velocity measurementsand flow patterns within the hinge regi<strong>on</strong> of a Medtr<strong>on</strong>ic Parallel bileafletmechanical valve with clear housing. J Heart Valve Dis 1996;5:591–599.49. Gersh BJ, Fisher LD, Schaff HV, Rahimtoola SH, Reeder S, Frater RW,McGo<strong>on</strong> DC. Issues c<strong>on</strong>cerning clinical evaluati<strong>on</strong> of new prosthetic heartvalves. J Thorac Cardiovasc Surg 1986;91:460–466.50. Grunkemeier GL, Starr A. Alternatives to randomisati<strong>on</strong> in surgical studies.J Heart Valve Disease 1992;1:142–151.51. Grunkemeier GL. Will randomised trials detect random valve failure? Reflecti<strong>on</strong><strong>on</strong> a recent FDA workshop. J Heart Valve Disease 1993;2:424–429.52. Office of Device Regulati<strong>on</strong>. Replacement Heart Valve Guidance. US Departmentof Health and Human Services, Food and Drug Administrati<strong>on</strong> Center for<strong>Devices</strong> and Radiological Health, October 1994.53. Akins CW, Miller DC, Turina MI, Kouchoukos NT, Blackst<strong>on</strong>e EH,Grunkemeier GL, Takkenberg JJ, David TE, Butchart EG, Adams DH,Shahian DM, Hagl S, Mayer JE, Lytle BW. Councils of the American Associati<strong>on</strong>for Thoracic Surgery; Society of Thoracic Surge<strong>on</strong>s; European Associati<strong>on</strong> forCardio-Thoracic Surgery; Ad Hoc Liais<strong>on</strong> Committee for Standardizing Definiti<strong>on</strong>sof Prosthetic Heart Valve Morbidity. Guidelines for reporting mortalityand morbidity after cardiac valve interventi<strong>on</strong>s. J Thor Cardiovasc Surg 2008;135:732–738.54. Le<strong>on</strong> MB, Piazza N, Nikolsky E, Blackst<strong>on</strong>e EH, Cutlip DE, Kappetein AP,Krucoff MW, Mack M, Mehran R, Miller C, Morel MA, Petersen J, Popma JJ,Takkenberg JJ, Vahanian A, van Es GA, Vranckx P, Webb JG, Windecker S,Serruys PW. Standardized endpoint definiti<strong>on</strong>s for transcatheter aortic valveimplantati<strong>on</strong> clinical trials: a c<strong>on</strong>sensus report from the Valve AcademicResearch C<strong>on</strong>sortium. Eur Heart J 2011;32:205–217.55. Hillebrenner MG, Swain JA, Zuckerman B. VARC c<strong>on</strong>sensus report: the FDAperspective. Eur Heart J 2011;32:138–139.56. O’Neill WW, O’Neill BP. The first generati<strong>on</strong> of angioplasty. Circ CardiovascInterv 2009;2:1–3.57. Wijns W, Kolh P, Danchin N, Di Mario C, Falk V, Folliguet T, Garg S, Huber K,James S, Knuuti J, Lopez-Send<strong>on</strong> J, Marco J, Menicanti L, Ostojic M, Piepoli MF,Pirlet C, Pomar JL, Reifart N, Ribichini FL, Schalij MJ, Sergeant P, Serruys PW,Silber S, Sousa Uva M, Taggart D. Guidelines <strong>on</strong> myocardial revascularizati<strong>on</strong>:the Task Force <strong>on</strong> Myocardial Revascularizati<strong>on</strong> of the European Society of Cardiology(<str<strong>on</strong>g>ESC</str<strong>on</strong>g>) and the European Associati<strong>on</strong> for Cardio-Thoracic Surgery(EACTS). European Associati<strong>on</strong> for Percutaneous <strong>Cardiovascular</strong> Interventi<strong>on</strong>s.Eur Heart J 2010;31:2501–2555.58. Daemen J, Simo<strong>on</strong>s ML, Wijns W, Bagust A, Bos G, Bowen JM, Braunwald E,Camenzind E, Chevalier B, DiMario C, Fajadet J, Gitt A, Guagliumi G,Hillege HL, James S, Jüni P, Kastrati A, Kloth S, Kristensen SD, Krucoff M,Legrand V, Pfisterer M, Rothman M, Serruys PW, Silber S, Steg PG, Tariah I,Wallentin L, Windecker SW. Meeting Report. <str<strong>on</strong>g>ESC</str<strong>on</strong>g> Forum <strong>on</strong> Drug ElutingStents. European Heart House, Nice, 27–28 September 2007. Eur Heart J2009;30:152–161.59. Magro M, Onuma Y, Silber S, Serruys PW. Transferability of data between differentdrug-eluting stents. Eurointerventi<strong>on</strong> 2009;5:527–531.60. Crem<strong>on</strong>esi A, Benit E, Carlier M, Colombo A, Piva R, Probst P, Wirtzfeld A,Pico-Bourd<strong>on</strong>nec C, Corcos T. Multicenter registry to evaluate the efficacy ofthe NIROYAL stent in de novo or restenotic cor<strong>on</strong>ary stenosis. J InvasiveCardiol 2000;12:225–232.61. Reifart N, Morice M-C, Silber S, Benit E, Hauptmann KE, de Sousa E, Webb J,Kaul U, Chan C, Thuesen L, Guagliumi G, Cobaugh M, Dawkins K, for theNUGGET investigators. The NUGGET study: NIR Ultra gold-gilded equivalencytrial. Catheter Cardiovasc Interv 2004;62:18–25.62. Kastrati A, Schömig A, Dirschinger J, Mehilli J, v<strong>on</strong> Welser N, Pache J,Schühlen H, Schilling T, Schmitt C, Neumann FJ. Increased risk of restenosisDownloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Page 16 of 18A.G. Fraser et al.after placement of gold-coated stents: results of a randomized trial comparinggold-coated with uncoated steel stents in patients with cor<strong>on</strong>ary arterydisease. Circulati<strong>on</strong> 2000;101:2478–2483.63. Baim DS, Hinohara T, Holmes D, Topol E, Pinkert<strong>on</strong> C, King SB, Whitlow P,Kereiakes D, Farley B, Simps<strong>on</strong> JB. Results of directi<strong>on</strong>al cor<strong>on</strong>ary atherectomyduring multicenter preapproval testing. The US Directi<strong>on</strong>al Cor<strong>on</strong>ary AtherectomyInvestigator Group. Am J Cardiol 1993;72:6E–11E.64. Topol EJ, Leya F, Pinkert<strong>on</strong> CA, Whitlow PL, Hofling B, Sim<strong>on</strong>t<strong>on</strong> CA,Masden RR, Serruys PW, Le<strong>on</strong> MB, Williams DO. A comparis<strong>on</strong> of directi<strong>on</strong>alatherectomy with cor<strong>on</strong>ary angioplasty in patients with cor<strong>on</strong>ary arterydisease. The CAVEAT Study Group. N Engl J Med 1993;329:221–227.65. Elliott JM, Berdan LG, Holmes DR, Isner JM, King SB, Keeler GP, Kearney M,Califf RM, Topol EJ. One-year follow-up in the Cor<strong>on</strong>ary Angioplasty VersusExcisi<strong>on</strong>al Atherectomy Trial (CAVEAT I). Circulati<strong>on</strong> 1995;91:2158–2166.66. Colombo A. What is the use of directi<strong>on</strong>al atherectomy, now we have stents?Heart 1997;78(Suppl. 2):31–33.67. Verin V, Urban P, Popowski Y, Schwager M, Nouet P, Dorsaz PA, Chatelain P,Kurtz JM, Rutishauser W. Feasibility of intracor<strong>on</strong>ary ß-irradiati<strong>on</strong> to reducerestenosis after ballo<strong>on</strong> angioplasty. A clinical pilot study. Circulati<strong>on</strong> 1997;95:1138–1144.68. King SB, Williams DO, Chougule P, Klein JL, Waksman R, Hilstead RR,Macd<strong>on</strong>ald J, Anderberg K, Crocker IR. Endovascular ß-radiati<strong>on</strong> to reduce restenosisafter cor<strong>on</strong>ary ballo<strong>on</strong> angioplasty: results of the beta energy restenosistrial (BERT). Circulati<strong>on</strong> 1998;97:2025–2030.69. Lansky AJ, Popma JJ, Massullo V, Jani S, Russo RJ, Schatz RA, Steuterman S,Guarneri EM, Wu H, Mehran R, Mintz GS, Le<strong>on</strong> MB, Teirstein PS. Quantitativeangiographic analysis of stent restenosis in the Scripps Cor<strong>on</strong>ary Radiati<strong>on</strong> toInhibit Intimal Proliferati<strong>on</strong> Post Stenting (SCRIPPS) Trial. Am J Cardiol 1999;84:410–414.70. Serruys PW, Sianos G, van der Giessen W, B<strong>on</strong>nier HJRM, Urban P, Wijns W,Benit E, Vandormael M, Dorr R, Disco C. Intracor<strong>on</strong>ary beta-radiati<strong>on</strong> toreduce restenosis after ballo<strong>on</strong> angioplasty and stenting. The Beta Radiati<strong>on</strong> InEurope (BRIE) study. Eur Heart J 2002;23:1351–1359.71. Le<strong>on</strong> MB, Teirstein PS, Moses JW, Tripuraneni P, Lansky AJ, Jani S, W<strong>on</strong>g SC,Fish D, Ellis S, Holmes DR, Kerieakes D, Kuntz RE. Localized intracor<strong>on</strong>arygamma-radiati<strong>on</strong> therapy to inhibit the recurrence of restenosis after stenting.N Engl J Med 2001;344:250–256.72. Popma JJ, Suntharalingam M, Lansky AJ, Heuser RR, Speiser B, Teirstein PS,Massullo V, Bass T, Henders<strong>on</strong> R, Silber S, v<strong>on</strong> Rottkay P, B<strong>on</strong>an R, Ho KK,Osattin A, Kuntz RE; Stents And Radiati<strong>on</strong> Therapy (START) Investigators. Randomizedtrial of 90Sr/90Y beta-radiati<strong>on</strong> versus placebo c<strong>on</strong>trol for treatment ofin-stent restenosis. Circulati<strong>on</strong> 2002;106:1090–1096.73. Sapirstein W, Zuckerman B, Dillard J. FDA approval of cor<strong>on</strong>ary-artery brachytherapy.N Engl J Med 2001;344:297–299.74. Farb A, Tang AL, Shroff S, Sweet W, Virmani R. Neointimal resp<strong>on</strong>ses 3 m<strong>on</strong>thsafter (32)P beta-emitting stent placement. Int J Radiat Oncol Biol Phys 2000;48:889–898.75. Farb A, Shroff S, John M, Sweet W, Virmani R. Late arterial resp<strong>on</strong>ses (6 and12 m<strong>on</strong>ths) after (32)P beta-emitting stent placement: sustained intimal suppressi<strong>on</strong>with incomplete healing. Circulati<strong>on</strong> 2001;103:1912–1919.76. Urban P, Serruys P, Baumgart D, Colombo A, Silber S, Eeckhout E, Gershlick A,Wegscheider K, Verhees L, B<strong>on</strong>an R. for the RENO investigators. A multicentreEuropean registry of intraluminal cor<strong>on</strong>ary beta brachytherapy. Eur Heart J 2003;24:604–612.77. Serruys PW, Wijns W, Sianos G, de Scheerder I, van den Heuvel PA, Rutsch W,Glogar HD, Macaya C, Materne PH, Veldhof S, V<strong>on</strong>hausen H, Otto-Terlouw PC,van der Giessen WJ. Direct stenting versus direct stenting followed by centeredbeta-radiati<strong>on</strong> with intravascular ultrasound-guided dosimetry and l<strong>on</strong>g-termanti-platelet treatment: results of a randomized trial: Beta-Radiati<strong>on</strong> Investigati<strong>on</strong>with Direct Stenting and Galileo in Europe (BRIDGE). J Am Coll Cardiol 2004;44:528–537.78. Holmes DR, Teirstein PS, Satler L, Sketch MH, Popma JJ, Mauri L, Wang HP,Schleckser PA, Cohen SA. SISR Investigators. 3-year follow-up of the SISR(Sirolimus-Eluting Stents Versus Vascular Brachytherapy for In-Stent Restenosis)trial. JACC Cardiovasc Interv 2008;1:439–448.79. Ellis SG, O’Shaughnessy CD, Martin SL, Kent K, McGarry T, Turco MA,Kereiakes DJ, Popma JJ, Friedman M, Koglin J, St<strong>on</strong>e GW; TAXUS V ISR investigators.Two-year clinical outcomes after paclitaxel-eluting stent or brachytherapytreatment for bare metal stent restenosis: the TAXUS V ISR trial. Eur Heart J2008;29:1625–1634.80. Oesterle SN, Sanborn TA, Ali N, Resar J, Ramee SR, Heuser R, Dean L,Knopf W, Schofield P, Schaer GL, Reeder G, Masden R, Yeung AC,Burkhoff D. Percutaneous transmyocardial laser revascularisati<strong>on</strong> for severeangina: the PACIFIC randomised trial. Lancet 2000;356:1705–1710.81. Le<strong>on</strong> MB, Kornowski R, Downey WE, Weisz G, Baim DS, B<strong>on</strong>ow RO,Hendel RC, Cohen DJ, Gervino E, Laham R, Lembo NJ, Moses JW, Kuntz RE.A blinded, randomized placebo-c<strong>on</strong>trolled trial of percutaneous laser myocardialrevascularizati<strong>on</strong> to improve angina symptoms in patients with severe cor<strong>on</strong>arydisease. J Am Coll Cardiol 2005;46:1812–1819.82. Schofield PM, McNab D. NICE evaluati<strong>on</strong> of transmyocardial laser revascularisati<strong>on</strong>and percutaneous laser revascularisati<strong>on</strong> for refractory angina. Heart 2010;96:312–313.83. Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es G-A, Steg PG,Morel M-A, Mauri L, Vranckx P, McFadden E, Lansky A, Ham<strong>on</strong> M,Krukoff MW, Serruys PW; <strong>on</strong> behalf of the Academic Research C<strong>on</strong>sortium.Clinical end points in cor<strong>on</strong>ary stent trials: a case for standardized definiti<strong>on</strong>s.Circulati<strong>on</strong> 2007;115:2344–2351.84. European Commissi<strong>on</strong>. Guidelines <strong>on</strong> <strong>Medical</strong> <strong>Devices</strong>. Evaluati<strong>on</strong> of clinicaldata—a guide for manufacturers and notified bodies. Appendix 1: Clinical evaluati<strong>on</strong>of cor<strong>on</strong>ary stents. MEDDEV 2.7.1, Appendix 1, December 2008. http://ec.europa.eu/c<strong>on</strong>sumers/sectors/medical-devices/files/meddev/cetf_en.pdf.85. Balc<strong>on</strong> R, Beyar R, Chierchia S, De Scheerder I, Hugenholtz PG, Kiemeneij F,Meier B, Meyer J, M<strong>on</strong>assier JP, Wijns W. Recommendati<strong>on</strong>s <strong>on</strong> stent manufacture,implantati<strong>on</strong> and utilizati<strong>on</strong>. Study Group of the Working Group <strong>on</strong> Cor<strong>on</strong>aryCirculati<strong>on</strong>. Eur Heart J 1997;18:1536–1547.86. Di Mario C. Differences in the approval process for interventi<strong>on</strong>al devices inEurope and USA: in medio stat virtus. EuroInterventi<strong>on</strong> 2011;6:913,915–917.87. Iglehart JK. The new era of medical imaging—progress and pitfalls. New Engl JMed 2006;354:2822–2828.88. Iglehart JK. Health insurers and medical-imaging policy—a work in progress. NEngl J Med 2009;360:1030–1037.89. Tricoci P, Allen JM, Kramer JM, Califf RM, Smith SC Jr. Scientific evidence underlyingthe ACC/AHA clinical practice guidelines. JAMA 2009;301:831–841.90. Schünemann HJ, Oxman AD, Brozek J, Glasziou P, Jaeschke R, Vist GE,Williams JW Jr, Kunz R, Craig J, M<strong>on</strong>tori VM, Bossuyt P, Guyatt GH; GRADEWorking Group. Grading quality of evidence and strength of recommendati<strong>on</strong>sfor diagnostic tests and strategies. BMJ 2008;336:1106–1110.91. Koopman LP, Slorach C, Hui W, Manlhiot C, McCrindle BW, Friedberg MK,Jaeggi ET, Mertens L. Comparis<strong>on</strong> between different speckle tracking andcolor tissue Doppler techniques to measure global and regi<strong>on</strong>al myocardialdeformati<strong>on</strong> in children. J Am Soc Echocardiogr 2010;23:919–928.92. Koopman LP, Slorach C, Manlhiot C, McCrindle BW, Jaeggi ET, Mertens L,Friedberg MK. Assessment of myocardial deformati<strong>on</strong> in children using DigitalImaging and Communicati<strong>on</strong>s in Medicine (DICOM) data and vendor independentspeckle tracking software. J Am Soc Echocardiogr 2011;24:37–44.93. Cho GY, Chan J, Leano R, Strudwick M, Marwick TH. Comparis<strong>on</strong> of twodimensi<strong>on</strong>alspeckle and tissue velocity based strain and validati<strong>on</strong> with harm<strong>on</strong>icphase magnetic res<strong>on</strong>ance imaging. Am J Cardiol 2006;97:1661–1666.94. Bansal M, Cho GY, Chan J, Leano R, Haluska BA, Marwick TH. Feasibility andaccuracy of different techniques of two-dimensi<strong>on</strong>al speckle based strain andvalidati<strong>on</strong> with harm<strong>on</strong>ic phase magnetic res<strong>on</strong>ance imaging. J Am Soc Echocardiogr2008;21:1318–1325.95. Mårtenss<strong>on</strong> M, Winter R, Cederlund K, Ripsweden J, Mir-Akbari H, Nowak J,Brodin LÅ. Assessment of left ventricular volumes using simplified 3-D echocardiographyand computed tomography—a phantom and clinical study. CardiovascUltrasound 2008;6:26.96. Bansal D, Singh RM, Sarkar M, Sureddi R, Mcbreen KC, Griffis T, Sinha A,Mehta JL. Assessment of left ventricular functi<strong>on</strong>: comparis<strong>on</strong> of cardiacmultidetector-row computed tomography with two-dimensi<strong>on</strong> standard echocardiographyfor assessment of left ventricular functi<strong>on</strong>. Int J Cardiovasc Imaging2008;24:317–325.97. Palazzuoli A, Cademartiri F, Geleijnse ML, Meijboom B, Pugliese F, Soliman O,Calabrò A, Nuti R, de Feyter P. Left ventricular remodelling and systolic functi<strong>on</strong>measurement with 64 multi-slice computed tomography versus sec<strong>on</strong>d harm<strong>on</strong>icechocardiography in patients with cor<strong>on</strong>ary artery disease: a double blindstudy. Eur J Radiol 2010;73:82–88.98. Chung ES, Le<strong>on</strong> AR, Tavazzi L, Sun JP, Nihoyannopoulos P, Merlino J,Abraham WT, Ghio S, Leclercq C, Bax JJ, Yu CM, Gorcsan J 3rd, St JohnSutt<strong>on</strong> M, De Sutter J, Murillo J. Results of the Predictors of Resp<strong>on</strong>se toCRT (PROSPECT) trial. Circulati<strong>on</strong> 2008;117:2608–2616.99. Redberg RF. Evidence, appropriateness, and technology assessment in cardiology:a case study of computed tomography. Health Aff (Millwood) 2007;26:86–95.100. Redberg RF. Cancer risks and radiati<strong>on</strong> exposure from computed tomographicscans. How can we be sure that the benefits outweigh the risks? Arch Intern Med2009;169:2049–2050.101. Smith-Bindman R, Lips<strong>on</strong> J, Marcus R, Kim KP, Mahesh M, Gould R, Berringt<strong>on</strong>de G<strong>on</strong>zález A, Miglioretti DL. Radiati<strong>on</strong> dose associated with comm<strong>on</strong>Downloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Clinical evaluati<strong>on</strong> of cardiovascular devices Page 17 of 18computed tomography examinati<strong>on</strong>s and the associated lifetime attributable riskof cancer. Arch Intern Med 2009;169:2078–2086.102. Fraser AG, Buser PT, Bax JJ, Dassen WR, Nihoyannopoulos P, Schwitter J,Knuuti JM, Höher M, Bengel F, Szatmári A. The future of cardiovascularimaging and n<strong>on</strong>-invasive diagnosis: a joint statement from the European Associati<strong>on</strong>of Echocardiography, the Working Groups <strong>on</strong> <strong>Cardiovascular</strong> MagneticRes<strong>on</strong>ance, Computers in Cardiology, and Nuclear Cardiology, of the EuropeanSociety of Cardiology, the European Associati<strong>on</strong> of Nuclear Medicine, and theAssociati<strong>on</strong> for European Paediatric Cardiology. Eur Heart J 2006;27:1750–1753.103. Wilkoff BL, Auricchio A, Brugada J, Cowie M, Ellenbogen KA, Gillis AM,Hayes DL, Howlett JG, Kautzner J, Love CJ, Morgan JM, Priori SG,Reynolds DW, Schoenfeld MH, Vardas PE. HRS/EHRA Expert C<strong>on</strong>sensus <strong>on</strong>the M<strong>on</strong>itoring of <strong>Cardiovascular</strong> Implantable Electr<strong>on</strong>ic <strong>Devices</strong> (CIEDs):descripti<strong>on</strong> of techniques, indicati<strong>on</strong>s, pers<strong>on</strong>nel, frequency and ethical c<strong>on</strong>siderati<strong>on</strong>s:developed in partnership with the Heart Rhythm Society (HRS) and theEuropean Heart Rhythm Associati<strong>on</strong> (EHRA); and in collaborati<strong>on</strong> with theAmerican College of Cardiology (ACC), the American Heart Associati<strong>on</strong>(AHA), the European Society of Cardiology (<str<strong>on</strong>g>ESC</str<strong>on</strong>g>), the Heart Failure Associati<strong>on</strong>of <str<strong>on</strong>g>ESC</str<strong>on</strong>g> (HFA), and the Heart Failure Society of America (HFSA). Europace 2008;10:707–725.104. Ellinor PT, Guy ML, Ruskin JN, McGovern BA. Variability in implantable cardioverterdefibrillator pulse generator l<strong>on</strong>gevity between manufacturers. Pacing ClinElectrophysiol 2003;26:71–75.105. Maisel WH. Pacemaker and ICD generator reliability. Meta-analysis of deviceregistries. JAMA 2006;295:1929–1934.106. Hauser RG, Hayes DL, Kallinen LM, Cannom DS, Epstein AE, Almquist AK,S<strong>on</strong>g SL, Tyers GF, Vlay SC, Irwin M. Clinical experience with pacemakerpulse generators and transvenous leads: an 8-year prospective multicenterstudy. Heart Rhythm 2007;4:154–160.107. Maisel WH, Moynahan M, Zuckerman BD, Gross TP, Tovar OH, Tillman DB,Schultz DB. Pacemaker and ICD generator malfuncti<strong>on</strong>s. Analysis of Food andDrug Administrati<strong>on</strong> Annual Reports. JAMA 2006;295:1901–1906.108. Wilkoff BL. Pacemaker and ICD malfuncti<strong>on</strong>—an incomplete picture. JAMA2006;295:1944–1946.109. Hauser RG, Hayes DL, Epstein AE, Cannom DS, Vlay SC, S<strong>on</strong>g SL, Tyers GF.Multicenter experience with failed and recalled implantable cardioverterdefibrillatorpulse generators. Heart Rhythm 2006;3:640–644.110. Steinbrook R. The c<strong>on</strong>troversy over Guidant’s implantable defibrillators. N Engl JMed 2005;353:221–224.111. Maisel WH. Semper fidelis: c<strong>on</strong>sumer protecti<strong>on</strong> for patients with implantedmedical devices. N Engl J Med 2008;358:985–987.112. Krahn AD, Champagne J, Healey JS, Camer<strong>on</strong> D, Simps<strong>on</strong> CS, Thibault B,Mangat I, Tung S, Sterns L, Birnie DH, Exner DV, Parkash R, Sivakumaran S,Davies T, Coutu B, Crystal E, Wolfe K, Verma A, Stephens<strong>on</strong> EA, Sanatani S,Gow R, C<strong>on</strong>nors S, Paredes FA, Essebag V; Canadian Heart Rhythm SocietyDevice Advisory Committee. Outcome of the Fidelis implantable cardioverterdefibrillatorlead advisory: a report from the Canadian Heart Rhythm SocietyDevice Advisory Committee. Heart Rhythm 2008;5:639–642.113. Gould PA, Krahn AD; for the Canadian Heart Rhythm Society Working Group<strong>on</strong> Device Advisories. Complicati<strong>on</strong>s associated with implantable cardioverterdefibrillatorreplacement in resp<strong>on</strong>se to device advisories. JAMA 2006;295:1907–1911.114. Parkash R, Crystal E, Bashir J, Simps<strong>on</strong> C, Birnie D, Sterns L, Exner D, Thibault B,C<strong>on</strong>nors S, Healey JS, Champagne J, Camer<strong>on</strong> D, Mangat I, Verma A, Wolfe K,Essebag V, Kus T, Ayala-Paredes F, Davies T, Sanatani S, Gow R, Coutu B,Sivakumaran S, Stephens<strong>on</strong> E, Krahn A. Complicati<strong>on</strong>s associated with revisi<strong>on</strong>of Sprint Fidelis leads: report from the Canadian Heart Rhythm SocietyDevice Advisory Committee. Circulati<strong>on</strong> 2010;121:2384–2387.115. Priori SG, Auricchio A, Nisam S, Y<strong>on</strong>g P. To replace or not to replace: a systematicapproach to resp<strong>on</strong>d to device advisories. J Cardiovasc Electrophysiol2009;20:164–170.116. Shah JS, Maisel WH. Recalls and safety alerts affecting automated extermal defibrillators.JAMA 2006;296:655–660.117. Center for <strong>Devices</strong> and Radiological Health, U.S. Food and Drug Administrati<strong>on</strong>.External defibrillator improvement initiative paper. November 2010. http://www.fda.gov/<strong>Medical</strong><strong>Devices</strong>/Productsand<strong>Medical</strong>Procedures/<strong>Cardiovascular</strong><strong>Devices</strong>/ExternalDefibrillators/ucm232621.htm.118. Estes NA. Automated external defibrillators—device reliability and clinicalbenefits. JAMA 2006;296:700–702.119. Bridges ND, Hellenbrand W, Lats<strong>on</strong> L, Filiano J, Newburger JW, Lock JE. Transcatheterclosure of patent foramen ovale after presumed paradoxical embolism.Circulati<strong>on</strong> 1992;86:1902–1908.120. Schwerzmann M, Salehian O. Hazards of percutaneous PFO closure. Eur J Echocardiogr2005;6:393–395.121. Messé SR, Kasner SE. Is closure recommended for patent foramen ovale andcryptogenic stroke? Patent foramen ovale in cryptogenic stroke. Not to close.Circulati<strong>on</strong> 2008;118:1999–2004.122. Messé SR, Silverman IE, Kizer JR, Homma S, Zahn C, Gr<strong>on</strong>seth G, Kasner SE.Practice parameter: recurrent stroke with patent foramen ovale and atrialseptal aneurysm: report of the Quality Standards Subcommittee of the AmericanAcademy of Neurology. Neurology 2004;62:1042–1050.123. Maisel WH, Laskey WK. Patent foramen ovale closure devices. Moving bey<strong>on</strong>dequipoise. JAMA 2005;294:366–369.124. Pinto Slottow TL, Steinberg DH, Waksman R. Overview of the 2007 Food andDrug Administrati<strong>on</strong> Circulatory System <strong>Devices</strong> Panel meeting <strong>on</strong> patentforamen ovale closure devices. Circulati<strong>on</strong> 2007;116:677–682.125. O’Gara PT, Messé SR, Tuzcu EM, Catha G, Ring JC. Percutaneous device closureof patent foramen ovale for sec<strong>on</strong>dary stroke preventi<strong>on</strong>. A call for completi<strong>on</strong>of randomized clinical trials. A Science Advisory from the American HeartAssociati<strong>on</strong>/American Stroke Associati<strong>on</strong> and the American College of CardiologyFoundati<strong>on</strong>. Circulati<strong>on</strong> 2009;119:2743–2747.126. Dows<strong>on</strong> A, Mullen MJ, Peatfield R, Muir K, Khan AA, Wells C, Lipscombe SL,Rees T, De Giovanni JV, Morris<strong>on</strong> WL, Hildick-Smith D, Elringt<strong>on</strong> G,Hillis WS, Malik IS, Rickards A. Migraine Interventi<strong>on</strong> With STARFlex Technology(MIST) trial: a prospective, multicenter, double-blind, sham-c<strong>on</strong>trolled trialto evaluate the effectiveness of patent foramen ovale closure with STARFlexseptal repair implant to resolve refractory migraine headache. Circulati<strong>on</strong> 2008;117:1397–1404. Erratum in Circulati<strong>on</strong> 2009;120:e71–2.127. Furlan AJ, Reisman M, Massaro J, Mauri L, Adams H, Albers GW, Felberg R,Herrmann H, Kar S, Landzberg M, Raizner A, Wechsler L; CLOSURE I Investigators.Study design of the CLOSURE I Trial: a prospective, multicenter, randomized,c<strong>on</strong>trolled trial to evaluate the safety and efficacy of the STARFlexseptal closure system versus best medical therapy in patients with stroke ortransient ischemic attack due to presumed paradoxical embolism through apatent foramen ovale. Stroke 2010;41:2872–2883.128. http://directnews.americanheart.org/pdfs/CLOSUREI_sslide.pdf.129. Windecker S, Meier B. Is closure recommended for patent foramen ovale andcryptogenic stroke? Patent foramen ovale and cryptogenic stroke: to close ornot to close? Closure: what else! Circulati<strong>on</strong> 2008;118:1989–1998.130. Carroll JD. Double standards in the world of ASD and PFO management:closure for paradoxical embolism. Catheter Cardiovasc Interv 2009;74:1070–1071.131. Meier B. Stroke and migraine: a cardiologist’s headache. Heart 2009;95:595–602.132. Wahl A, Praz F, Stinimann J, Windecker S, Seiler C, Nedeltchev K, Mattle HP,Meier B. Safety and feasibility of percutaneous closure of patent foramenovale without intra-procedural echocardiography in 825 patients. Swiss <strong>Medical</strong>Wkly 2008;138:567–572.133. Feldman MD, Petersen AJ, Karliner LS, Tice JA. Who is resp<strong>on</strong>sible for evaluatingthe safety and effectiveness of medical devices? The role of independent technologyassessment. J Gen Intern Med 2007;23(Suppl. 1):57–63.134. Rao SV, Califf RM, Kramer JM, Peters<strong>on</strong> ED, Gross TP, Pepine CJ, Williams DO,D<strong>on</strong>ohoe D, Waksman R, Mehran R, Krucoff MW. Postmarket evaluati<strong>on</strong> ofbreakthrough technologies. Am Heart J 2008;156:201–208.135. Dhruva SS, Bero LA, Redberg RF. Strength of study evidence examined by theFDA in premarket approval of cardiovascular devices. JAMA 2009;302:2679–2685.136. Garber AM. Modernizing device regulati<strong>on</strong>. N Engl J Med 2010;362:1161–1163.137. Hines JZ, Lurie P, Yu E, Wolfe S. Left to their own devices: breakdowns inUnited States medical device premarket review. PLoS Med 2010;7:e1000280.138. Lenzer J, Brownlee S. Why the FDA can’t protect the public. BMJ 2010;341:c4753.139. Tomkins<strong>on</strong> A, Harris<strong>on</strong> W, Temple M, Phillips P. Surveillance and medicaldevices. BMJ 2010;341:c6999.140. Redberg RF. <strong>Medical</strong> devices and the FDA approval process. Balancing safety andinnovati<strong>on</strong>. Arch Intern Med 2010;170:1831–1833.141. Avorn J. Regulati<strong>on</strong> of devices. Less<strong>on</strong>s can be learned from drug regulati<strong>on</strong>. BMJ2010;341:c5370.142. Zuckerman DM, Brown P, Nissen SE. <strong>Medical</strong> device recalls and the FDAapproval process. Arch Intern Med 2011; Feb 14 (Epub).143. Redberg RF, Dhruva SS. <strong>Medical</strong> device recalls. Get it right the first time. ArchIntern Med 2011; Feb 14 (Epub).144. IEC/DIS 80001-1. Applicati<strong>on</strong> of risk management for IT-networks incorporatingmedical devices.145. Coordinati<strong>on</strong> of the Notified Bodies <strong>Medical</strong> <strong>Devices</strong> (NB-MED) <strong>on</strong> CouncilDirectives 90/385/EEC, 93/42/EEC, and 98/79/EC. Recommendati<strong>on</strong> NB-MED/2.7/Rec3. Evaluati<strong>on</strong> of clinical data (1999). Accessed at www.team-nb.org, February2011.146. Jefferys DB. The regulati<strong>on</strong> of medical devices and the role of the <strong>Medical</strong><strong>Devices</strong> Agency. Br J Clin Pharmacol 2001;52:229–235.Downloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013
Page 18 of 18A.G. Fraser et al.147. Resnic FS, Gross TP, Marinac-Dabic D, Loyo-Berrios N, D<strong>on</strong>nelly S,Normand ST, Matheny ME. Automated surveillance to detect postproceduresafety signals of approved cardiovascular devices. JAMA 2010;304:2019–2027.148. Rumsfeld JS, Peters<strong>on</strong> ED. Achieving meaningful device surveillance. From reacti<strong>on</strong>to proacti<strong>on</strong>. JAMA 2010;304:2065–2066.149. DeMets DL, Califf RM. A historical perspective <strong>on</strong> clinical trials innovati<strong>on</strong> andleadership: where have the academics g<strong>on</strong>e? JAMA 2011;305:713–714.150. European Commissi<strong>on</strong>, SEC(2010) 1161. Communicati<strong>on</strong> from the Commissi<strong>on</strong> tothe European Parliament, the Council, the European Ec<strong>on</strong>omic and Social Committeeand the Committee of the Regi<strong>on</strong>s. Europe 2020 Flagship Initiative. Innovati<strong>on</strong> Uni<strong>on</strong>.Brussels, 6.1.2010.151. Commissi<strong>on</strong> launches public c<strong>on</strong>sultati<strong>on</strong> <strong>on</strong> medical devices. IP/08/723, 08/05/2008. http://europa.eu/rapid/pressReleasesActi<strong>on</strong>.do?reference=IP/08/723&format=HTML&aged=1&language=EN&guiLanguage=en.152. European Commissi<strong>on</strong>, Enterprise and Industry Directorate-General. Recast ofthe <strong>Medical</strong> <strong>Devices</strong> Directives. Summary of resp<strong>on</strong>ses to the public c<strong>on</strong>sultati<strong>on</strong>.http://ec.europa.eu/c<strong>on</strong>sumers/sectors/medical-devices/files/recast_docs_2008/resp<strong>on</strong>ses/resp<strong>on</strong>ses_public%20c<strong>on</strong>sultati<strong>on</strong>_recast_en.pdf.153. Center for <strong>Devices</strong> and Radiological Health, U.S. Food and Drug Administrati<strong>on</strong>.<strong>Medical</strong> device innovati<strong>on</strong> initiative white paper. February 2011. http://www.fda.gov/aboutfda/centersoffices/cdrh/cdrhinnovati<strong>on</strong>/ucm242067.htm.154. Regulati<strong>on</strong> (EC) No 1049/2001 of the European Parliament and of the Councilof 30 May 2001 regarding public access to European Parliament, Council andCommissi<strong>on</strong> documents.155. Auricchio A, Gropp M, Ludgate S, Vardas P, Brugada J, Priori SG. EuropeanHeart Rhythm Associati<strong>on</strong> Guidance Document <strong>on</strong> cardiac rhythm managementproduct performance. Europace 2006;8:313–322.156. Wallner PE, K<strong>on</strong>ski A. A changing paradigm in the study and adopti<strong>on</strong> of emerginghealth care technologies: coverage with evidence development. J Am CollRadiol 2008;5:1125–1129.157. Holzer R, Hijazi Z. The off- versus <strong>on</strong>-label use of medical devices in interventi<strong>on</strong>alcardiovascular medicine? Clarifying the ambiguity between regulatory labellingand clinical decisi<strong>on</strong> making, part III: structural heart disease interventi<strong>on</strong>s.Cathet Cardiovasc Interv 2008;72:848–852.158. Popp RL, Lorell BH, St<strong>on</strong>e GW, Laskey W, Smith JJ, Kaplan AV. An outline ofpublic registrati<strong>on</strong> of clinical trials evaluating medical devices. J Am Coll Cardiol2006;47:1518–1521.Downloaded from http://eurheartj.oxfordjournals.org/ by guest <strong>on</strong> February 28, 2013