application form
application form
application form

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
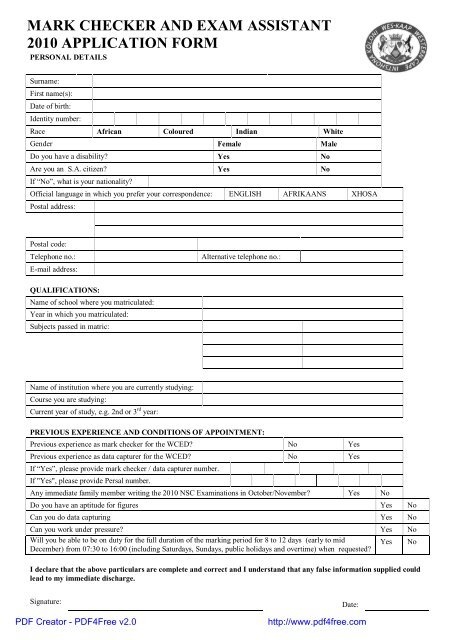
MARK CHECKER AND EXAM ASSISTANT2010 APPLICATION FORMPERSONAL DETAILSSurname:First name(s):Date of birth:Identity number:Race African Coloured Indian WhiteGender Female MaleDo you have a disability? Yes NoAre you an S.A. citizen? Yes NoIf “No”, what is your nationality?Official language in which you prefer your correspondence: ENGLISH AFRIKAANS XHOSAPostal address:Postal code:Telephone no.:E-mail address:Alternative telephone no.:QUALIFICATIONS:Name of school where you matriculated:Year in which you matriculated:Subjects passed in matric:Name of institution where you are currently studying:Course you are studying:Current year of study, e.g. 2nd or 3 rd year:PREVIOUS EXPERIENCE AND CONDITIONS OF APPOINTMENT:Previous experience as mark checker for the WCED? No YesPrevious experience as data capturer for the WCED? No YesIf “Yes”, please provide mark checker / data capturer number.If "Yes", please provide Persal number.Any immediate family member writing the 2010 NSC Examinations in October/November? Yes NoDo you have an aptitude for figures Yes NoCan you do data capturing Yes NoCan you work under pressure? Yes NoWill you be able to be on duty for the full duration of the marking period for 8 to 12 days (early to midDecember) from 07:30 to 16:00 (including Saturdays, Sundays, public holidays and overtime) when requested?Yes NoI declare that the above particulars are complete and correct and I understand that any false in<strong>form</strong>ation supplied couldlead to my immediate discharge.Signature:PDF Creator - PDF4Free v2.0Date:http://www.pdf4free.com
THIS SECTION MUST BE SIGNED BY THE DIRECTOR / REGISTRAR / RECTOR / HEADOF DEPARTMENTThis is to certify that (applicant’s name in full)_______________________________________________________________is a registered full-time student at (name of institution)_________________________________________________________and is registered for the following course: _______________________________________________________________(e.g. B.A. I, N.D. Comm II)I, _____________________________________, as __________________________, hereby recommend his/her appointment.(full name)(rank)INSTITUTION’S STAMPSignature:…………………………………..………….Date: ……….…………………………The documents listed below must accompany each completed <strong>application</strong> <strong>form</strong>. Late <strong>application</strong>sand faxes will not be accepted.1. Certified copy of identity document2. Certified copy of Senior Certificate3. Proof of current registration at a tertiary institution4. Proof of subjects registered for this year5. Proof of subjects already passedN.B.If this completed <strong>application</strong> <strong>form</strong> does not contain your institution’s official stamp andthe signature of the Director/Registrar/Rector/Head of Department, your <strong>application</strong>will not be considered.PDF Creator - PDF4Free v2.0http://www.pdf4free.com