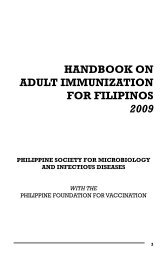
138 Card<strong>in</strong>o MJ T <strong>and</strong> Lantion-Ang FLdisorder <strong>and</strong> was started with Carbamazep<strong>in</strong>e withescalat<strong>in</strong>g doses. Bra<strong>in</strong> computed tomography scan<strong>and</strong> electroencephalogram were normal. Topiramatewas added to the anti-seizure regimen howeverpatient still had 4-6 seizure episodes per year. Therewere episodes of true hypoglycemia precipitat<strong>in</strong>gthe seizure attacks thus a computed tomographyscan of the abdomen was done <strong>and</strong> showed a 2 x1.8cm pancreatic mass thus she was referred toEndocr<strong>in</strong>ology for evaluation.Fig 1.MRI of the Abdomen Show<strong>in</strong>g A 2 x 1.8cmPancreatic Nodule Enhanced By ContrastOn review, our patient started to have symptomsof generalized weakness associated with palpitations,hunger pangs <strong>and</strong> dizz<strong>in</strong>ess resolved with food <strong>in</strong>takefor 5 years. These symptoms usually occurredon wak<strong>in</strong>g up. Because of this pattern, she beganga<strong>in</strong><strong>in</strong>g weight until 6 months later, she had onsetof generalized tonic seizures. Everytime she wasbrought to the emergency room, her blood sugarwas low. After giv<strong>in</strong>g <strong>in</strong>travenous glucose, patientrega<strong>in</strong>ed consciousness. She ga<strong>in</strong>ed 18 kg <strong>in</strong> 4months prior to referral to our service.Menarche was at 11 years old. Menstrual flowwas regular until a year prior to consult she hadamenorrhea. She had no dysmenorrheal, abnormaldischarges <strong>and</strong> history of contraceptive <strong>in</strong>take.Developmental history was at par with age. Shehad good school performance <strong>and</strong> even graduatedcollege. She had no history of blurr<strong>in</strong>g of vision, <strong>and</strong>chronic headaches. She had no family history oftumors, diabetes <strong>and</strong> hypertension.On exam<strong>in</strong>ation, she had normal vital signs.She was obese with a BMI of 32 kg/m, 2 waistcircumference of 95 cm, hip circumference of 99cm, <strong>and</strong> waist to hip ratio was 0.95. There was noacanthosis nigricans, thyromegaly, <strong>and</strong> xanthomas.Silver striae were noted <strong>in</strong> the <strong>in</strong>ner thighs. She hadno visual field cuts on confrontation test.Fig 2.Photograph of the Patient Dur<strong>in</strong>g Her Admission atPGHIn the approach to hypoglycemic patients, wehave to classify the etiology of the hypoglycemia.Our patient had fast<strong>in</strong>g hypoglycemia. Differentialdiagnoses for fast<strong>in</strong>g hypoglycemia <strong>in</strong>cludeddrugs e.g. sulfonylurea, critical illness, adrenal<strong>and</strong> pituitary <strong>in</strong>sufficiency <strong>and</strong> <strong>in</strong>sul<strong>in</strong>oma. Shewas not hypotensive, lethargic <strong>and</strong> weak mak<strong>in</strong>gthe consideration of adrenal <strong>in</strong>sufficiency unlikely.Patient had no <strong>in</strong>take of sulfonylurea.The signs <strong>and</strong> symptoms of patients weresuggestive of <strong>in</strong>sul<strong>in</strong>oma, thus serum <strong>in</strong>sul<strong>in</strong>, C-peptide <strong>and</strong> r<strong>and</strong>om blood sugar were taken aftera 72-hour fast test. Basel<strong>in</strong>e counter-regulatoryhormone levels were taken <strong>and</strong> then blood sugarwas monitored every 2 hours while patient fasted.Basel<strong>in</strong>e 8 oÊclock morn<strong>in</strong>g serum cortisol (880nmol/L) was normal. A 72 hour fast test was done. Onthe 18th hour, she manifested with neuroglycopenicsymptoms. Capillary blood sugar was 38 mg/dl.A low r<strong>and</strong>om blood sugar at 18mg/dl with an<strong>in</strong>appropriately high serum <strong>in</strong>sul<strong>in</strong> levels at 41.08uU/ml (normal: 2.6-24 uU/ml) were documented.C peptide was elevated at 25.6 ng/ml (normal: 1-5ng.ml) <strong>in</strong>dicative of endogenous hyper<strong>in</strong>sul<strong>in</strong>emia.Serum <strong>in</strong>sul<strong>in</strong> <strong>and</strong> C-peptide are secreted <strong>in</strong>equimolar amounts. In our patient, the serum <strong>in</strong>sul<strong>in</strong>to C-peptide was 1.6 reflective of degradation of theC-peptide. The catheps<strong>in</strong> B degrades the C term<strong>in</strong>alam<strong>in</strong>o acids of C-peptide which is be<strong>in</strong>g determ<strong>in</strong>ed<strong>in</strong> the assay, result<strong>in</strong>g to higher <strong>in</strong>sul<strong>in</strong> to C-peptideratio. 4
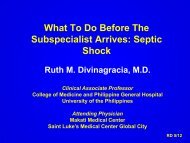
<strong>Insul<strong>in</strong>oma</strong> <strong>and</strong> <strong>Prolact<strong>in</strong>oma</strong> <strong>in</strong> A <strong>Young</strong> <strong>Female</strong> 139Table I. Review of Cases with Insul<strong>in</strong> to C-peptide Ratio <strong>in</strong><strong>Insul<strong>in</strong>oma</strong> Patients 4AuthorLevels <strong>in</strong> <strong>Insul<strong>in</strong>oma</strong>Katabami 7.2G<strong>in</strong> 6.3Sakai 6.1Scarlet 5.9Saudek 5Lebowitz 4.9Kondo 4.2Service 3.6Ciavarella 2.9Turner 2Fujikura 2Our Case 1.6Intraoperative ultrasound showed a 2 x 1.8 cmsolid nodule at the antero-<strong>in</strong>ferior portion of the bodyof the pancreas <strong>and</strong> subsequently an enucleation ofthe nodule was done. Post-operatively, blood sugarrose to 208 mg/dl with<strong>in</strong> 30 m<strong>in</strong>utes from enucleationof the tumor. No symptoms of acute pancreatitis weredocumented <strong>and</strong> serum amylase was slightly elevatedonly at 178 U/ml (normal 83-110 U/ml). There wereno calcifications noted. Post-operative biopsy revealedan <strong>in</strong>sul<strong>in</strong>oma. Cells were arranged <strong>in</strong> anastomos<strong>in</strong>gcords separated by a vascular stroma, <strong>in</strong>terspersedwith sparse collagenous stroma. Chromogran<strong>in</strong>-A<strong>and</strong> synaptophys<strong>in</strong> sta<strong>in</strong><strong>in</strong>g of the tumor were positive(see figure 3). These sta<strong>in</strong><strong>in</strong>g results confirmed thatthe tumor was an <strong>in</strong>sul<strong>in</strong>oma.Fig 3.A) 2x2 cm Pancreatic Nodule Post-Pancreatic Enucleation. B) Hematoxyl<strong>in</strong> <strong>and</strong> Eos<strong>in</strong> Sta<strong>in</strong><strong>in</strong>g Show<strong>in</strong>g Uniform Cells<strong>in</strong> Anastomos<strong>in</strong>g Cords. C) Panoramic View of the Tumor Cells <strong>in</strong> Clumps with Sparse Collagenous Stroma. D) PositiveSynaptophys<strong>in</strong> Sta<strong>in</strong><strong>in</strong>g of the Pancreatic Nodule. E) Positive Chromogran<strong>in</strong> Sta<strong>in</strong><strong>in</strong>g of the Pancreatic Nodule.