

2012 New Drug Updates: Implications for ... - Dcpa.us
2012 New Drug Updates: Implications for ... - Dcpa.us
2012 New Drug Updates: Implications for ... - Dcpa.us

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
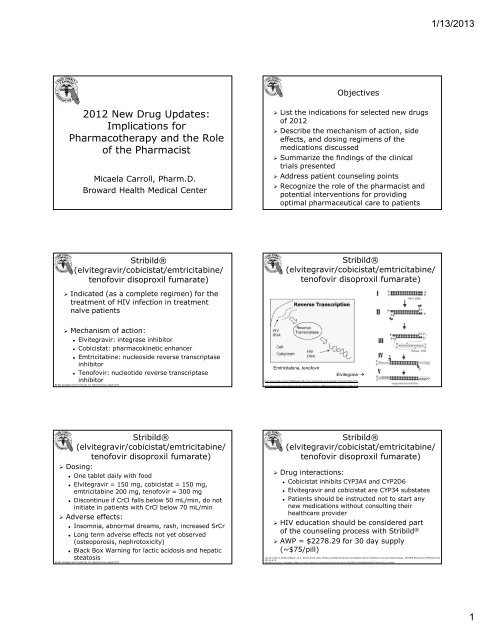
1/13/2013Objectives<strong>2012</strong> <strong>New</strong> <strong>Drug</strong> <strong>Updates</strong>:<strong>Implications</strong> <strong>for</strong>Pharmacotherapy and the Roleof the PharmacistMicaela Carroll, Pharm.D.Broward Health Medical Center List the indications <strong>for</strong> selected new drugsof <strong>2012</strong> Describe the mechanism of action, sideeffects, and dosing regimens of themedications disc<strong>us</strong>sed Summarize the findings of the clinicaltrials presented Address patient counseling points Recognize the role of the pharmacist andpotential interventions <strong>for</strong> providingoptimal pharmaceutical care to patientsStribild®(elvitegravir/cobicistat/emtricitabine/tenofovir disoproxil fumarate)Stribild®(elvitegravir/cobicistat/emtricitabine/tenofovir disoproxil fumarate) Indicated (as a complete regimen) <strong>for</strong> thetreatment of HIV infection in treatmentnaïve patients Mechanism of action: Elvitegravir: integrase inhibitor Cobicistat: pharmacokinetic enhancer Emtricitabine: nucleoside reverse transcriptaseinhibitor Tenofovir: nucleotide reverse transcriptaseinhibitorStribild. [package insert]. Foster City, CA: Gilead Sciences; Aug<strong>us</strong>t <strong>2012</strong>.Emtricitabine, tenofovirElvitegravir http://www.google.comiw=1366&bgrefurl=http://www.retrovirology.com/content/4/1/21/figure/f1&docid=Mwww.retrovirology.com/content/4/1/21/figure/f1&docid=Mtbnw=138&start=0&ndsp=20&ved=1t:429,r:3,s:0Stribild®(elvitegravir/cobicistat/emtricitabine/tenofovir disoproxil fumarate) Dosing: One tablet daily with food Elvitegravir = 150 mg, cobicistat = 150 mg,emtricitabine 200 mg, tenofovir = 300 mg Discontinue if CrCl falls below 50 mL/min, do notinitiate in patients with CrCl below 70 mL/min Adverse effects: Insomnia, abnormal dreams, rash, increased SrCr Long term adverse effects not yet observed(osteoporosis, nephrotoxicity) Black Box Warning <strong>for</strong> lactic acidosis and hepaticsteatosisStribild. [package insert]. Foster City, CA: Gilead Sciences; Aug<strong>us</strong>t <strong>2012</strong>.Stribild®(elvitegravir/cobicistat/emtricitabine/tenofovir disoproxil fumarate) <strong>Drug</strong> interactions: Cobicistat inhibits CYP3A4 and CYP2D6 Elvitegravir and cobicistat are CYP34 substates Patients should be instructed not to start anynew medications without consulting theirhealthcare provider HIV education should be considered partof the counseling process with Stribild ® AWP = $2278.29 <strong>for</strong> 30 day supply(~$75/pill)Lee JS, Calmy A, Andrieux-Meyer I, et al. Review of the safety, efficacy, and pharmacokinetics of elvitegravir with an emphasis on resource-limited settings. HIV/AIDS Research and Palliative Care.<strong>2012</strong>:4;5-15.McKesson Connect. Available at https://connect.mckesson.com/portal/site/smo/menuitem.e282395f5c1594abb9a999d65740d0a0/?query=stribild1
1/13/2013Fycompa ® (Perampanel) Indicated as adjunctive therapy in patientswith partial onset seizures (Proposed) mechanism of action: Noncompetivie antagonism of AMPA glutamatereceptors Dosing: 2-12 mg PO HS M<strong>us</strong>t start at 2 mg PO HS and titrate by 2mg/day once weeklyFycompa. [package insert]. Woodcliff Lake, NJ: Eisai; October <strong>2012</strong>.Fycompa ® (Perampanel) Adverse effects: Anxiety, conf<strong>us</strong>ion, diplopia, imbalance (falls),weight gain Efficacy findings in clinical trials: Patients ages 12 and older randomized to 8mg, 12 mg, or placebo and treated <strong>for</strong> 19weeks Percent change in seizure frequency:• -21% (placebo)• -26.3% (8 mg)• -34.5% (12 mg)French JA, Kra<strong>us</strong>s GL, Biton V, et al. Adjunctive parempanel <strong>for</strong> refractory partial-onset seizures: randomized phase III study 304. Neurology. <strong>2012</strong>;79(6):589-96.Fycompa ® (Perampanel) Safety findings in clinical trials: Up to 43% of patients experienced dizzinessand 10% experienced falls Patients gained 2.5 lbs over 19 weeks vs. 0.7lbs with placebo Additional safety concerns: Black Box Warning <strong>for</strong> psychiatric andbehavioral adverse reactions When taken with alcohol, Fycompa ® mayworsen mood and increase anger Fycompa ® can ca<strong>us</strong>e euphoria in somepatients and will be a controlled substanceFrench JA, Kra<strong>us</strong>s GL, Biton V, et al. Adjunctive parempanel <strong>for</strong> refractory partial-onset seizures: randomized phase III study 304. Neurology. <strong>2012</strong>;79(6):589-96. <strong>Drug</strong> interactions:Fycompa ® (Perampanel)Fycompa ® is a CYP3A4 substrateCarbamazepine and phenytoin have all beenshown to increase clearanceHormonal contraceptives: Fycompa ® has beenshown to decrease levonorgestrel levels by40% and ethynyl estradiol by 18%Myrbetriq ® (Mirabegron)Myrbetriq ® (Mirabegron) Indicated <strong>for</strong> the treatment of overactivebladder (OAB) with symptoms of urgeurinary incontinence, urgency, and urinaryfrequency Mechanism of action: Agonism at beta-3 adrenergic receptors –increases bladder capacity by relaxing thedetr<strong>us</strong>or m<strong>us</strong>cleMyrbetriq. [package insert]. Northbrook, IL: Astellas Pharma; June <strong>2012</strong>hvurology.comivy-rose.co.uk2
1/13/2013 Dosing: 25 mg once dailyMyrbetriq ® (Mirabegron) Can increase to 50 mg once daily after 8weeks Dose adj<strong>us</strong>tments in renal impairment: CrCl < 30 mL/min = max dose 25 mg CrCl < 15 mL/min = not recommended Dose adj<strong>us</strong>tments in hepatic impairment: Child-Pugh Class B = max dose 25 mg Child-Pugh Class C = not recommendedMyrbetriq. [package insert]. Northbrook, IL: Astellas Pharma; June <strong>2012</strong>Myrbetriq ® (Mirabegron) Adverse effects: Urinary tract infections, headache,nasopharyngitis Shown to decrease number ofincontinence episodes per day and numberof micturitions per day Hypertension observed in early, dosefindingstudies Increased incidences of neoplasms seen inphase III trials with 100 mg dose (did notoccur with 50 mg dose)Chapple C., Kaplan S., Mitcheson H., Klecka J., Cummings J., Drogendijk T., et al. (<strong>2012</strong>)Randomised, double-blind, active-controlled phase III study to assess the long-term safety and efficacy of mirabegronin overactive bladder (OAB). Eur Urol Suppl 11: e683–e683Myrbetriq ® (Mirabegron) <strong>Drug</strong> interactions:Myrbetriq ® is a CYP2D6 inhibitorOmontys ® (Peginesatide) Indicated <strong>for</strong> the treatment of anemia dueto chronic kidney disease in adult patientson dialysisContraindicated with thioridazine (QT cprolongation)Increase in digoxin levels shown (mechanismunknown) AWP = $250.20 <strong>for</strong> 30 day supply ($6.76/pill) Mechanism of action: Binds to and activates the humanerythropoetin receptor and stimulateserythropoiesis in human red cell precursors Structurally dissimilar to epoetin alfa anddarbepoetin alfaFDA (<strong>2012</strong>) Summary of safety and efficacy as basis <strong>for</strong> Advisory Committee briefing document <strong>for</strong> mirabegron, Office of <strong>New</strong> <strong>Drug</strong>s Center <strong>for</strong> <strong>Drug</strong> Evaluation and Research of Food and <strong>Drug</strong>Administration; Availablet:http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/<strong>Drug</strong>s/ReproductiveHealth<strong>Drug</strong>sAdvisoryCommittee/UCM298284.pdfOmontys. [package insert]. Deerfield, IL: Takeda; November <strong>2012</strong> Dosing:Omontys ® (Peginesatide)0.04 mg/kg IV or SC once monthly“Pegylation” allows <strong>for</strong> longer duration ofactionInitiate when hemoglobin is less than 10 g/dLPrefilled syringes available from 1 - 6 mgDoses above 6 mg available through multiple<strong>us</strong>e vials Converting from epoetin alfa ordarbepoetin alfa to Omontys ®Previo<strong>us</strong> Total Weekly EpoetinAlfa Dose (U/week)Omontys ® (Peginesatide)Previo<strong>us</strong> Weekly DarbepoetinAlfa Dose (mcg/week)OMONTYS Dose Once Monthly(mg/month)Less than 2,500 Less than 12 22,500 to less than 4,300 12 to less than 18 34,300 to less than 6,500 18 to less than 25 46,500 to less than 8,900 25 to less than 35 58,900 to less than 13,000 35 to less than 45 613,000 to less than 19,000 45 to less than 60 819,000 to less than 33,000 60 to less than 95 1033,000 to less than 68,000 95 to less than 175 15greater than or equal to 68,000 greater than or equal to 175 20Omontys. [package insert]. Deerfield, IL: Takeda; November <strong>2012</strong>Omontys. [package insert]. Deerfield, IL: Takeda; November <strong>2012</strong>3
1/13/2013Omontys ® (Peginesatide) Theoretically less immunogenic thanepoetin alfa or darbepoetin alfa, withless capability to ca<strong>us</strong>e pure red cellaplasia (PRCA) 1.2% of patients tested duringclinical trials had peginesatidespecificbinding antibodiesOmontys ® (Peginesatide) Adverse effects: GI upset, AV fistula site complications, m<strong>us</strong>clespasms, seizures, hypertension Black Box Warning <strong>for</strong> increased risk of death,MI, stroke, and other cardiovascular eventswhen targeting hemoglobin levels of 11 g/dLor higher Contraindications: Uncontrolled hypertensionMikhail A. Profile of peginesatide and its potential <strong>for</strong> the treatment of anemia in adults with chronic kidney disease who are on dialysis. J Blood Med. <strong>2012</strong>;3:25-31.Mikhail A. Profile of peginesatide and its potential <strong>for</strong> the treatment of anemia in adults with chronic kidney disease who are on dialysis. J Blood Med. <strong>2012</strong>;3:25-31.Belviq ® (Lorcaserin) Indicated to treat obesity (as adjunct to dietand exercise) in patients with BMI of 30 kg/m 2or greater OR 27 kg/m 2 or greater in thepresence of at least one weight-relatedcomorbidity Mechanism of action Selective serotonin 2C (5-HT 2C ) receptor agonist Dosing: 10 mg PO BID (discontinue at week 12 if 5% weightloss has not been achieved)Belviq. [package insert]. Woodcliff Lake, NJ: Eisai; September <strong>2012</strong>Belviq ® (Lorcaserin) Adverse effects: Hypoglycemia, priapism, bone marrowsuppression, serotonin syndrome Efficacy findings in clinical trials: Patients with BMI of 27 to 45 withoutdiabetes lost an average of 5.8% bodyweight Patients with a BMI of 27 or higher withinadequately controlled DM lost anaverage of 4.5% body weightBelviq. [package insert]. Woodcliff Lake, NJ: Eisai; September <strong>2012</strong>Belviq ® (Lorcaserin) Safety findings in clinical trials: Numerically higher incidence ofvalvulopathy (moderate or worse mitralvalve regurgitation or mild or worseaortic valve regurgitation)• Not statistically significant 1997 fenfluramine anddexfenfluramine removed from marketdue to association with cardiacvalvulopathy Contraindications:Belviq ® (Lorcaserin) Pregnancy (Category X) <strong>Drug</strong> interactions: Selective serotonin reuptake inhibitors(SSRIs), serotonin-norepinephrinereuptake inhibitors (SNRIs), monoamineoxidase inhibitors (MAOIs), bupropion,St. John’s Wort, triptansColman E, Golden J, Roberts M. The FDA’s assessment of two drugs <strong>for</strong> chronic weight management. NEJM. <strong>2012</strong>:367;1577-79.Belviq. [package insert]. Woodcliff Lake, NJ: Eisai; September <strong>2012</strong>4
1/13/2013Qsymia ® (Phentermine/ExtendedRelease Topiramate) Indicated to treat obesity (as adjunct todiet and exercise) in patients with BMI of30 kg/m 2 or greater OR 27 kg/m 2 orgreater in the presence of at least oneweight-related comorbidity Mechanism of action Phentermine: sympathomimetic amine Topiramate: antiepilepticQsymia. [package insert]. Mountainview, CA: Viv<strong>us</strong>; July <strong>2012</strong>Qsymia ® (Phentermine/ExtendedRelease Topiramate) Dosing: 3.75 mg/23 mg (phentermine/topiramate) POdaily x 14 days, then 7.5 mg/46 mg PO daily Dose escalation (if weight loss is not atleast 3% of baseline after 12 weeks) 11.25 mg/69 mg PO daily x 14 days, then 15 mg/92 mg PO daily If weight loss is not 5% of baseline after 12weeks after dose escalation, GRADUALLYdiscontinue the dose (seizure risk)Qsymia. [package insert]. Mountainview, CA: Viv<strong>us</strong>; July <strong>2012</strong>Qsymia ® (Phentermine/ExtendedRelease Topiramate) Adverse effects: Suicidal thoughts, insomnia, hypokalemia,metabolic acidosis Qsymia ® can also increase HR at certaindoses (7.5 mg/46 mg and higher) butthese doses have also been shown tolower blood pressure <strong>Drug</strong> not recommended in patients withunstable cardiac or cerebrovascular diseaseQsymia ® (Phentermine/ExtendedRelease Topiramate) Contraindications Pregnancy (Category X)• Topiramate associated with infants bornwith orofacial cleft Hyperthyroidism Glaucoma Concomitant <strong>us</strong>e of monoamine oxidaseinhibitors (MAOIs)Qsymia. [package insert]. Mountainview, CA: Viv<strong>us</strong>; July <strong>2012</strong>Margulis AV, Mitchell AA, Gilboa SM. Use of topiramate in pregnancy and risk of oral clefts. Am J Obstet Gynecol. <strong>2012</strong>;Epub ahead of print.Qsymia ® (Phentermine/ExtendedRelease Topiramate) Requires a Risk Evaluatoin and MitigationStrategy (REMS) Prescribers need to undergo a <strong>for</strong>maltraining program Only specially certified pharmacies will beable to dispense the drugColman E, Golden J, Roberts M. The FDA’s assessment of two drugs <strong>for</strong> chronic weight management. NEJM. <strong>2012</strong>:367;1577-79.Case Study 35 y/o F would like to lose weight and asksyou about Qsymia. ® Her BMI is 26 kg/m 2 PMH: Type 2 DM Hyperthyroidism Depression Medications: Met<strong>for</strong>min 500 mg PO BID Methimazole 5 mg PO TID Tranylcypromine 15 mg PO BID Is Qsymia ® a good option <strong>for</strong> this patient?5
1/13/2013Eliquis® (Apixaban) Indicated to reduce the risk of stroke andsystemic embolism in patients withnonvalvular atrial fibrillation Mechanism of action: Directly inhibits factor Xa Dosing: 5 mg PO BID 2.5 mg PO BID in patients with any TWO of thefollowing characteristics:• Age ≥ 80 years• Body weight ≤60 kg• SrCr ≥1.5 mg/dLEliquis. [package insert]. <strong>New</strong> York, NY: Bristol Meyers Squibb and Pfizer; December <strong>2012</strong> Apixaban <strong>for</strong> Reduction in Stroke andOther Thromboembolic Events in AtrialFibrillation (ARISTOTLE)Eliquis® (Apixaban)Randomized double-blind, double-dummy trialto study Eliquis ® vs. warfarinStudied ~18,000 patients with atrial fibrillationand a CHADS 2 score of at least 1Granger CB, Alexander JH, McMurray JJV, et al. Apixaban vers<strong>us</strong> warfarin in patients with atrial fibrillation. NEJM. 2011;365:981-92. ARISTOTLE findings showed thatcompared to warfarin, Eliquis ® reducedrisk of: Stroke or systemic embolism by 21% Major bleeding by 31% Death by 11%Eliquis® (Apixaban) Adverse effects all related to bleedingEliquis. [package insert]. <strong>New</strong> York, NY: Bristol Meyers Squibb and Pfizer; December <strong>2012</strong>Eliquis® (Apixaban) Converting from warfarin to Eliquis ® : Discontinue warfarin and start Eliquis ® when INRfalls below 2 Converting from Eliquis ® to warfarin: Discontinue Eliquis ® and begin both a parenteralanticoagulant and warfarin at the time the next doseof Eliquis ® would have been taken. Stop parenteralagent when INR reaches desired range Switching between Eliquis ® and anticoagulantsother than warfarin: Discontinue one and begin taking the other at thenext scheduled doseEliquis. [package insert]. <strong>New</strong> York, NY: Bristol Meyers Squibb and Pfizer; December <strong>2012</strong> <strong>Drug</strong> interactions: Eliquis ® is a substrate of both CYP3A4 and P-gp Patients should be reminded not to takeany new medications (including OTCs)without consulting their healthcare provider Patients m<strong>us</strong>t stop taking Eliquis ® 24-48hours be<strong>for</strong>e elective proceduresEliquis. [package insert]. <strong>New</strong> York, NY: Bristol Meyers Squibb and Pfizer; December <strong>2012</strong>Eliquis® (Apixaban)True or False Assessment Questions In the ARISTOTLE study, apixaban met thenoninferiority criteria but did not show amortality benefit over warfarin Locaserin differs from previo<strong>us</strong> serotonintargetingweight loss drugs in that it is selective<strong>for</strong> the 5-HT(2C) receptor subtype Unlike other ESAs, peginesatide does not carrythe black box warning of risk of death,myocardial infarction, stroke, and other serio<strong>us</strong>cardiovascular events6
1/13/2013<strong>Drug</strong> Shortages:strive to survive; <strong>Implications</strong><strong>for</strong> Pharmacotherapy and theRole of the PharmacistMina AbdallaPGY1 Pharmacy ResidentMercy HospitalObjectives Understand the scope and severity of drugshortages Understand how drug shortages affectseveryday treatment Recognize what the government is doingabout drug shortages Identify drugs which suffer shortages andwhat alternatives are there Practice how to handle a shortageBackground• Shortages tripled between 2005 and 2010 (1)• 44% reported shortages of more than 21drugs (2)• 63% of the hospitals reported that in somecases, patients didn't receive therecommended treatment (2)• Substitutions are not always as effective• 2-year event-free survival 75% withcyclophosphamide vs 88% with mechlorethamine(Stand<strong>for</strong>d V regimen <strong>for</strong> Hodgkin’s lymphoma) (3)1. http://www.whiteho<strong>us</strong>e.gov/the-press-office/2011/10/31/we-can-t-wait-obama-administration-takes-action-reduce-prescription-drug2. http://www.aarp.org/health/drugs-supplements/info-08-2011/prescription-drug-shortage-hits-doctors-hospitals.html3. http://www.nejm.org.ezproxylocal.library.nova.edu/doi/full/10.1056/NEJMp1212468http://www.aha.org/content/11/drugshortagesurvey.pdfWhy is there a shortage?1. 2. 3.Raw and Bulk MaterialUnavailability Worst kind of shortage Multiple manufacturers make a drugproduct with material available from onlyone source Effects the whole chain of supply Examples: Metoclopramide (Reglan) and PhenobarbitalInjectionshttp://www.fda.gov/<strong>Drug</strong>s/<strong>Drug</strong>Safety/<strong>Drug</strong>Shortages/ucm277626.htmhttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdf1
1/13/2013Manufacturing Difficulties Most common type of shortage Occurs when the primary or onlymanufacturer of a drug stops productiondue to a FDA sanction/regulatoryproblems i.e. Poor manufacturing practices Examples: Naloxone (Narcan), tetan<strong>us</strong> toxoid and IVIG(Flebogamma, Octagam)Recalls Voluntary and non-voluntary drug recallscan ca<strong>us</strong>e a shortage Could be short or long term shortage Shortage depends on whether othermanufacturers are producing the productExample:• Atorvastatin (Lipitor) recall due to possiblecontamination with very small glass particleshttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfhttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfManufacturer Production Decisions Manufacturers can decide, without publicnotification, to: Shift production or reallocate resources toother products Halt production of a product all together dueto financial reasons Examples: Diptheria, tetan<strong>us</strong> toxoids and acellularpert<strong>us</strong>sis (DTaP) vaccineRestricted <strong>Drug</strong> ProductDistribution Some drug products could only come fromcertain approved distribution centerswhich limits supply Creates an artificial shortage Examples: Cisapride (Propulsid) and Dofetilide (Tikosyn)http://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfhttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfInd<strong>us</strong>try Consolidations Manufacturer mergers often result indecisions to narrow the foc<strong>us</strong> of productlines Instead of 2 companies making a product,now streamlined to one More vulnerable to drug shortages Example Ondansetron (zofran) InjectionUnexpected Increases in Demand Occurs when a manufacturer can not handlean increase of drug demand This may occur as a result of a product’spopularity <strong>for</strong> new unlabeled <strong>us</strong>es, asubstantial disease outbreak, orunpredictable factors of demand Can be worse when raw materials are limitedor manufacturing processes are complex Examples: Succinylcholine (Quelicin)http://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfhttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdf2
1/13/2013Natural Disasters Natural disasters ca<strong>us</strong>e drug productshortages when they affect manufacturingfacilities Example: Hurricane damage to manufacturing facilitiesin the Caribbean in 1997 ca<strong>us</strong>ed shortages ofseveral drugs, including gentamicin and thecombination of piperacillin and tazobactamGovernment Actions President Obama signed an executiveorder directing the FDA to: Prevent and reduce prescription drugshortages Protect consumers Prevent price gouging DOJ will examine illegal price gouging orstockpiling of mediations (gray market) Markup average of 650%http://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfhttp://www.whiteho<strong>us</strong>e.gov/the-press-office/2011/10/31/we-can-t-wait-obama-administration-takes-action-reduce-prescription-drugGovernment Actions• FDA established the CDER <strong>Drug</strong> ShortageProgram (DSP)– There is a DSP representative in each FDA center• i.e. Office of <strong>New</strong> <strong>Drug</strong>s & Office of Generic <strong>Drug</strong>s• All potential or actual shortage situations anddiscontinuations of CDER drugs should bereported to the DSP as soon as they areknown– Mandatory <strong>for</strong> single manufacturers– Voluntary <strong>for</strong> multiple manufacturersFDA <strong>Drug</strong> Shortage Manual of Policies and ProceduresGovernment Actions• The CDER <strong>Drug</strong> Shortage Program will:– Communicate in<strong>for</strong>mation to different offices ofthe FDA– Work with FDA offices, ind<strong>us</strong>try, and outsideentities as needed to develop a shortagemanagement plan– Assist in identification of non-U.S. drug sources<strong>for</strong> drugs in shortage– Facilitate resolution of regulatory and scientificissues related to generic drugs in shortageFDA <strong>Drug</strong> Shortage Manual of Policies and ProceduresExecutiveOrderWhat Should We Do?1. Confirm the shortage2. Inventory what is on hand3. Determine <strong>us</strong>age history4. Identify therapeutic alternatives (if any)5. Communicate6. Prioritize patientshttps://blogs.fda.gov/fdavoice/wp-content/uploads/<strong>2012</strong>/05/slide-six.gifhttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdf3
1/13/2013What Should We Do? Confirm The Shortage Product manufacturers, distributors, FDA, andother sources can be contacted to determinethe reason <strong>for</strong> the shortage and its expectedduration• http://www.fda.gov/<strong>Drug</strong>s/<strong>Drug</strong>Safety/<strong>Drug</strong>Shortages/default.htm• http://www.ashp.org/menu/<strong>Drug</strong>Shortages/CurrentShortages.aspx Determine the expected time frame of theshortageWhat Should We Do? Inventory what is on hand Inventory all available stock on hand In and out of the pharmacy (Pyxis, Kirby) Every strength and <strong>for</strong>mulation Determine Usage History Run a <strong>us</strong>age report of the medication Determine if possible inventory can endurethe shortagehttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfhttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfWhat Should We Do? Identify therapeutic alternatives Identify therapeutic alternatives in stock or onthe market (if any)• i.e. Thyrogen Alternative medications should be decided incollaboration with medical, nursing, andpharmacy representatives and approved by P&T• Shortage Committee Set up automatic substitution protocols andprocessWhat Should We Do? Communicate Communicate with all medical and nursingstaff Provide in<strong>for</strong>mation on drug product shortage,alternative therapies, temporary therapeuticguidelines, and implementation plans Pharmacist should be responsible in assistingmedical staff in ordering and administratingtherapeutic alternativeshttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfhttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfWhat Should We Do? Prioritize patients Prioritize patients in the event of severe shortageof a medication with no alternatives Multi-disciplinary team should develop criteria <strong>for</strong>the <strong>us</strong>e of the product Prescribing could be limited to select patients orservices within the healthcare organization Written guidelines should be provided to assistpharmacists to respond to medication orders <strong>for</strong>drug products under a patient priority limitationWhat Should We Not Do? Stockpile Despite pressure to stockpile, as good citizensand professionals, we should not orderquantities in excess of normal <strong>us</strong>e Stockpiling creates artificial shortages Stockpiling also increases inventory whichmight not be <strong>us</strong>ed there<strong>for</strong>e leads toincreased inventory costhttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdfhttp://www.ashp.org/s_ashp/docs/files/BP07/Procure_Gdl_Shortages.pdf4
1/13/2013Sample Current <strong>Drug</strong> Shortages Acetylcysteine (Mucomyst) Vials Acyclovir (Zovirax )Tablets/Capsules/Injections Bupivacaine (Marcaine) Injection Epinephrine (Adrenaline) Syringes Mebendazole (Vermox) Tablets Methotrexate (Rheumatrex) Injection Sodium Bicarb Syringe/Vials Tetracycline (Sumycin) CapsulesAcetylcysteine (Mucomyst) Vials Reason: increased demand <strong>for</strong> the drug,manufacturing delays Estimated resupply date: ~ January 2013 Alternatives: We are only <strong>us</strong>ing Acetylcysteine <strong>for</strong> APAP overdose Acetylcysteine as a mucolytic At Mercy, pharmacists are rejecting those prescriptions andcalling the doctors to in<strong>for</strong>m of shortage and discontinuingthe prescription Acetylcysteine <strong>for</strong> renal protection At Mercy, pharmacists are calling the doctors to switch toNS hydration or sodium bicarb drip (also in shortage)http://www.ashp.org/menu/<strong>Drug</strong>Shortages/CurrentShortages.aspxhttp://www.ashp.org/menu/<strong>Drug</strong>Shortages/CurrentShortages.aspxAcyclovir (Zovirax )Tablets/Capsules/Injections Reason: FDA audits, raw materials shortageand product discontinuation Estimated resupply date: Early 2013 Alternatives: Preserve inj <strong>for</strong> herpes simplex encephalitis• Foscavir or ganciclovir possible alternatives Dispensing a different oral strength to get a totaldosage Call MD to change to PO Valacyclovir Dispensing the s<strong>us</strong>pension insteadBupivacaine (Marcaine) Injection Reason: increased demand <strong>for</strong> the drugand manufacturer delays Estimated resupply date: Early 2013 Alternatives: Communicate the problem to all ORpersonnel, including anesthesiologists Ask to switch to ropivacaine (Naropin)• More costlyhttp://www.ashp.org/menu/<strong>Drug</strong>Shortages/CurrentShortages.aspxhttp://www.ashp.org/menu/<strong>Drug</strong>Shortages/CurrentShortages.aspxEpinephrine (Adrenaline) Injection Reason: increased demand <strong>for</strong> the drugand manufacturer delays Estimated resupply date: Early 2013 Alternatives: Use the 1 mg epinephrine ampule and salinefl<strong>us</strong>h together in the crash carts Pharmacists/nurses are educated on thedifference and how to <strong>us</strong>eMebendazole (Vermox) Tablets Reason: Product has been discontinued byTeva, the sole manufacturer Estimated resupply date: None Alternatives: Call MD to in<strong>for</strong>m of product discontinuation Recommend Albendazole (Albenza)http://www.ashp.org/menu/<strong>Drug</strong>Shortages/CurrentShortages.aspxhttp://www.ashp.org/menu/<strong>Drug</strong>Shortages/CurrentShortages.aspx5
1/13/2013Methotrexate (Rheumatrex)Injection Reason: Manufacturer delays, productdiscontinuation and increase demand <strong>for</strong>product Estimated resupply date: Early 2013 Alternatives: Reserve methotrexate injection <strong>for</strong> oncologypatients Every case is different• Pharmacists and Hem/Onc doctors should disc<strong>us</strong>s eachcase and come up with alternativesReserve preservative-free methotrexate <strong>for</strong>intrathecal dosesSodium Bicarbonate Injection Reason: Manufacturer delays, increaseddemand <strong>for</strong> product and productdiscontinuations Estimated resupply date: Early 2013 Alternatives: We are <strong>us</strong>ing what we have• Vials with vented spike in crash carts Sodium acetate <strong>for</strong> metabolic acidosis (shortage) Some hospitals are making their own sodiumbicarbonate• USP 797 High Risk categoryhttp://www.ashp.org/menu/<strong>Drug</strong>Shortages/CurrentShortages.aspxhttp://www.ashp.org/menu/<strong>Drug</strong>Shortages/CurrentShortages.aspxTetracycline (Sumycin) Capsules Reason: Raw material shortage Estimated resupply date: No date Alternatives: Call MD to in<strong>for</strong>m of shortage Try to change to another tetracycline drug• Minocycline (Minocin)• Doxycycline (Vibramycin)True or False As soon as we find out there is a shortageof a product but our wareho<strong>us</strong>e has a lotin stock, we should order everything theyhave! STAT! DEA quota restrictions is one reason <strong>for</strong>shortages Hospitals and pharmacies are alwaysin<strong>for</strong>med of shortageshttp://www.ashp.org/menu/<strong>Drug</strong>Shortages/CurrentShortages.aspxCase Study Your buyer j<strong>us</strong>t told you that they cannot orderKetorolac (Toradol) injections due to “shortage”.They also tell you that they only have 1 box of 25vials of the 15mg, 25 vials of the 30mg and a lot of10mg tablets. How do you handle this potentialshortage?1. Confirm the shortage2. Inventory what is on hand3. Determine <strong>us</strong>age history4. Identify therapeutic alternatives (if any)5. Communicate6. Prioritize patients7. Hope <strong>for</strong> the best!Concl<strong>us</strong>ion <strong>Drug</strong> shortages are not a new problem facingpharmacists yet it’s not going anywhere The FDA may have prevented someshortages but the fact remains that there aremany shortages affecting practice today As pharmacists, we m<strong>us</strong>t <strong>us</strong>e our knowledgeas drug experts to salvage a shortage crisisand come up with alternatives6
1/12/2013<strong>New</strong> Vaccines to beAdministered by Pharmacists:<strong>Implications</strong> <strong>for</strong> Pharmacotherapyand the Role of the PharmacistKristina Lee, PharmDPharmacy Resident PGY-1South Miami HospitalGoals/Objectives1. Review the legislature authorizing pharmaciststo administer vaccines.2. List the additional vaccines that pharmacistsmay administer as a result of legislativechanges.3. Disc<strong>us</strong>s CDC recommendations and guidelines<strong>for</strong> vaccines administered by pharmacists.4. Identify continuing education requirements <strong>for</strong>pharmacists to qualify as immunizers.5. Recognize the role of the pharmacist andpotential interventions <strong>for</strong> providing optimalpharmaceutical care to patients.Legislative History Pharmacist’s authority to administervaccines is determined by each state Currently – all 50 US states authorize 2007 – Florida 2009 – Maine In Florida: Florida Statute 465.003 (13) Florida Statute 465.189 Florida Statute 465.009 (6)• All revised due to Ho<strong>us</strong>e Bill 509 (Vaccine Access Act)Florida Statute 465.003Definitions(13) …The practice of the profession ofpharmacy also includes theadministration of vaccines to adultspursuant to s. 465.189.Terrie YC 2010Immunization Action Coalition 2009The Florida Legislature <strong>2012</strong>The Florida Legislature <strong>2012</strong>Florida Statute 465.189 (1-3)Administration of vaccines and epinephrine autoinjection(1) In accordance with guidelines of the Centers <strong>for</strong> Disease Controland Prevention <strong>for</strong> each recommended immunization or vaccine, apharmacist may administer the following vaccines to an adult withinthe framework of an established protocol under a supervisingphysician licensed under chapter 458 or chapter 459:(a) Influenza vaccine.(b) Pneumococcal vaccine.(2) In accordance with guidelines of the Centers <strong>for</strong> Disease Controland Prevention, a pharmacist may administer the shingles vaccinewithin the framework of an established protocol and pursuant to awritten or electronic prescription issued to the patient by a physicianlicensed under chapter 458 or chapter 459.(3) In order to address any un<strong>for</strong>eseen allergic reaction, a pharmacistmay administer epinephrine <strong>us</strong>ing an autoinjector delivery systemwithin the framework of an established protocol under a supervisingphysician licensed under chapter 458 or chapter 459Florida Statute 465.009Continuing professional pharmacy education(6) Notwithstanding subsections (1)-(5):(a) Each pharmacist certified to administer a vaccine orepinephrine autoinjection under s. 465.189 m<strong>us</strong>t complete a3-hour continuing education course, which shall be offered bya statewide professional association of physicians in this stateaccredited to provide educational activities designated <strong>for</strong> theAmerican Medical Association Physician’s Recognition Award(AMA PRA) Category I credit, on the safe and effectiveadministration of vaccines and epinephrine autoinjection aspart of biennial relicensure or recertification. This course maybe offered in a distance-learning <strong>for</strong>mat and m<strong>us</strong>t be includedin the 30 hours of continuing professional pharmaceuticaleducation specified in subsection (1).The Florida Legislature <strong>2012</strong>The Florida Legislature <strong>2012</strong>1
1/12/2013Florida Statute 465.009(cont’d.)(b) Each pharmacist m<strong>us</strong>t submitconfirmation of having completed thecourse specified in paragraph (a) on a <strong>for</strong>mprovided by the board when submitting fees<strong>for</strong> license renewal.(c) Failure to comply with paragraphs (a)and (b) results in the revocation of theauthorization <strong>for</strong> a pharmacist to administera vaccine or epinephrine autoinjectionunder s. 465.189. Such authorization maybe restored upon completion of suchrequirements.Summary of Legislature2011 <strong>2012</strong>Patient Population Adult AdultAdministration ofVaccinesAdministration ofEpinephrineWritten Protocol withPhysicianInfluenzaNoRequiredInfluenza, pneumococcal,shingles*YesRequiredLiability Insurance $200,000 $200,000Record-Keeping 5 years 5 yearsCertification Program 20 hours 20 hoursCE Requirements None 3 hours biennially*A prescription is required <strong>for</strong> a pharmacist to administer the shingles vaccine.The Florida Legislature <strong>2012</strong>The Florida Legislature <strong>2012</strong>Additional VaccinationLegislatureFlorida statute 381.005(2) Between 10/1, or earlier if the vaccination is available,and 2/1, hospitals m<strong>us</strong>t offer influenza andpneumococcal vaccinations to patients > 65 years oldFlorida statute 409.912(34)(d) Any health care provider serving Medicaid recipientsm<strong>us</strong>t make immunizations availableFlorida statute 400.141(1)(s-t) Nursing home facilities m<strong>us</strong>t provide influenzaimmunization to all consenting residents be<strong>for</strong>e 11/30 Nursing home facilities m<strong>us</strong>t assess all residents <strong>for</strong>eligibility <strong>for</strong> pneumococcal polysaccharide vaccinationand vaccinate residents when indicatedHospital inpatientAdditional VaccinationLegislaturePatient Type Vaccine RequirementAmbulatory care facility patientLong-term care facility residentInfluenzaPneumococcalInfluenzaPneumococcalInfluenzaPneumococcalOffer*Offer*Offer^Offer^MandateºMandateºCorrectional inmate or resident Any NoDevelopmentally disabled facilityresident* Florida statute 381.005(2)^ Florida statute 409.912(34)(d)º Florida statute 400.141(1)(s-t)AnyNoThe Florida Legislature <strong>2012</strong>The Florida Legislature <strong>2012</strong>Influenza Vaccine Protects against the influenza vir<strong>us</strong>, whichca<strong>us</strong>es a contagio<strong>us</strong> respiratory illness Fever/chills, cough, sore throat, runny or stuffynose, m<strong>us</strong>cle or body aches, headaches, fatigue Older people, young children, pregnant women,people with certain chronic health conditions andpeople who live in facilities like nursing homes areat increased risk of complications CDC Recommendations Routine annual influenza vaccination <strong>for</strong> all > 6months Offer vaccination as soon as vaccine available andthroughout influenza season (October to May)<strong>2012</strong>-2013Influenza Vaccines Types available: Trivalent inactivated vaccine (TIV)• High-dose trivalent inactivated vaccine• Intradermal trivalent inactivated vaccine Live attenuated influenza vaccine (LAIV) All protect against: A/Cali<strong>for</strong>nia/7/2009 (H1N1)-like A/Victoria/361/2011 (H3N2)-like B/Wisconsin/1/2010-like (Yamagatalineage)CDC.gov <strong>2012</strong>MMWR. <strong>2012</strong>; 61(32):613-8MMWR. <strong>2012</strong>; 61(32):613-82
1/12/2013<strong>2012</strong>-2013 InfluenzaVaccinesTIV(e.g. Fluvirin ® )TIV high-dose(Fluzone ®High-Dose)TIVintradermal(Fluzone ®Intradermal)LAIV(FluMist ® )Administration IM IM intradermal intranasalDose 45 mcg/0.5 ml 180 mcg/0.5 ml 27 mcg/0.1 mlHow SuppliedAge GroupSpecialConsiderationsPre-filledsyringe,single-<strong>us</strong>e vial,multi-<strong>us</strong>e vial> 6 months,depending onproductPrefilled syringePrefilledmicroinjectionsystem> 65 years 18-64 yearsTIV <strong>for</strong>mulations are preferred if:• egg allergy (hives only, can eat lightly cookedeggs)• care provider <strong>for</strong> immunosuppressed patients whorequire a protective environment0.2 ml dividedbetween naresPrefilledintranasalsprayer2-49 yearsAnd healthy,not pregnant---Fluzone ® IntradermalMMWR. <strong>2012</strong>; 61(32):613-8Sanofi Pasteur <strong>2012</strong>Fluzone ® IntradermalFuture Influenza Vaccines For the 2013-2014 flu season:FluMist ® Quadrivalent, approved in February<strong>2012</strong>, is expected to replace the currentFluMist ®Inactivated quadrivalent vaccines are currentlyin developmentQuadrivalent influenza vaccines provideprotection against an additional B vir<strong>us</strong> strainSanofi Pasteur <strong>2012</strong>MMWR. <strong>2012</strong>; 61(32):613-8Pneumococcal VaccinePneumococcal Vaccines Protects against infections ca<strong>us</strong>ed byStreptococc<strong>us</strong> pneumoniae(pneumococc<strong>us</strong>) Pneumococcal disease includes pneumonia,bacteremia, meningitis, and otitis media Symptoms vary based on site of infection Bacteria lives in many and is spread bycoughing, sneezing or contact with respiratorysecretionsCDC.gov <strong>2012</strong>Image from: http://inst.bact.wisc.edu/inst/index.php?module=book&func=displayarticle&art_id=137Type of VaccineAdministrationCDCRecommendationsPPSV 23(Pneumovax ® 23)23-valent pneumococcalpolysaccharideIM or SQ• Individuals 2 to 64 yearsold with certainunderlying medicalconditions or otherindication• Individuals 19 to 64 yearsold who smoke or haveasthma• All adults > 65 years old• Residents of nursing homesor long-term care facilitiesPCV 13(Prevnar ® 13)13-valent pneumococcalconjugateIMNote: Shake vigoro<strong>us</strong>ly to make ahomogeno<strong>us</strong>, white s<strong>us</strong>pension.• Adults > 19 years old withcertain medical conditionswho have not previo<strong>us</strong>lyreceived PCV 13, even ifhave previo<strong>us</strong>ly receivedPPSV 23CDC.gov <strong>2012</strong>MMWR. 2010; 59(34):1102-1106MMWR. <strong>2012</strong>; 61(40):816-819Pneumovax ® 23 PIPrevnar ® 13 PI3
1/12/2013Specific Risk Groups/Indications<strong>for</strong> Pneumococcal VaccinesImmunocompetentPersons• Chronic heart disease,excluding HTN• Chronic lung disease• Diabetes mellit<strong>us</strong>• Cerebrospinal fluid leaks*• Cochlear implant*• Alcoholism• Chronic liver disease,including cirrhosis•Cigarette smokingPersons with Functionalor Anatomic Asplenia*• Sickle cell disease andotherhemoglobinopathies• Congenital or acquiredasplenia, splenicdysfunction orsplenectomyPPSV 23 is recommended <strong>for</strong> all.For starred (*) indications,PCV 13 should be given first,followed by PPSV 23 eight weeks later.ImmunocompromisedPersons*• Congenital or acquiredimmunideficiencies• HIV infection• Chronic renal failure• Nephrotic syndrome• Leukemias• Lymphomas• Hodgkin disease• Generalized malignancy• Diseases requiringtreatment withimmunosuppressivedrugs, including longtermsystemiccorticosteroids orradiation therapy• Solid organtransplantation• Multiple myelomaPneumococcal RevaccinationRecommendations For adults aged > 19 years with functional oranatomic asplenia or immunocompromisingconditions: Second dose of PPSV 23 five years after first dose For adults aged > 19 years with functional oranatomic asplenia, immunocompromisingconditions, CSF leaks or cochlear implants whohave received PPSV 23: PCV 13 greater than one year after previo<strong>us</strong> PPSV23 For all 65 years or older: Additional PPSV 23 once five years have passedsince previo<strong>us</strong> doseMMWR. 2010; 59(34):1102-1106MMWR. <strong>2012</strong>; 61(40):816-819MMWR. <strong>2012</strong>; 61(40):816-819Shingles Vaccine Shingles is ca<strong>us</strong>ed byreactivation of the varicellazoster vir<strong>us</strong> Vir<strong>us</strong> stays dormant in the bodyafter recovery from chickenpox Risk of shingles increases withage or with immunosuppression Ca<strong>us</strong>es pain, itching and tingling,and then a painful rash, <strong>us</strong>uallyon one side of the face or bodyZostavax ® Live attenuated vaccine Subcutaneo<strong>us</strong> administration Supplied as single-dose vial Approved <strong>for</strong> the prevention ofshingles in individuals > 50 years old Recommended to administer fourweeks apart from Pneumovax ® 23CDC.gov <strong>2012</strong>Image from: http://www.cdc.gov/shingles/about/photos.htmlZostavax ® PIRecommendations <strong>for</strong>Zostavax ®Indications Routine vaccination asone-time dose <strong>for</strong>adults > 60 year Not routinelyrecommended <strong>for</strong>adults 50-59 yearsContraindications Life-threatening orsevere allergicreaction to gelatin, theantibiotic neomycin,or any othercomponent of shinglesvaccine Immunocompromisedstate Women who are ormight be pregnantZostavax ® Administration1. Withdraw entire contents of supplieddiluent into a syringe.2. Inject diluent slowly into vial oflyophilized vaccine.3. Gently agitate to mix thoroughly.4. Withdraw entire contents ofreconstituted vaccine (0.65ml).5. Administer subcutaneo<strong>us</strong>lyimmediately after reconstitution.Discard if not <strong>us</strong>ed within 30 minutes.CDC.gov <strong>2012</strong>Zostavax ® PI4
1/12/2013Screening Checklist1. Are you sick today?2. Do you have allergies to medications, food, a vaccinecomponent or latex?3. Have you ever had a serio<strong>us</strong> reaction after receiving avaccination?4. Do you have a long-term health problem with heartdisease, lung disease, asthma, kidney disease,metabolic disease (e.g., diabetes), anemia, or otherblood disorders?5. Do you have cancer, leukemia, HIV/AIDS, or any otherimmune system problem?Screening Checklist6. In the past 3 months, have you taken medications thatweaken your immune system, such as cortisone,prednisone, other steroids, or anticancer drugs, orhave you had radiation treatments?7. Have you had a seizure or a brain or other nervo<strong>us</strong>system problem?8. During the past year, have you received a transf<strong>us</strong>ionof blood or blood products, or been given immune(gamma) globulin or an antiviral drug?9. For women: Are you pregnant or is there a chance youcould become pregnant during the next month?10. Have you received any vaccinations in the past 4weeks?Immunization Action Coalition <strong>2012</strong>Immunization Action Coalition <strong>2012</strong>Storage RequirementsEpiPen ® Administration Refrigerator: influenza, pneumococcal Freezer: shingles (diluent in refrigerator or at roomtemperature) Interim Vaccine Storage and Handling Guidance Use of digital data loggers with detachable probes thatrecord and store temperature in<strong>for</strong>mation at frequentprogrammable intervals <strong>for</strong> 24 hour temperaturemonitoring Use of stand-alone refrigerator and stand-alone freezerunits suitable <strong>for</strong> vaccine storage Discontinuing <strong>us</strong>e of dorm-style or bar-stylerefrigerator/freezers <strong>for</strong> ANY vaccine storage, eventemporary storage Weekly review of vaccine expiration dates and rotationof vaccine stockCDC.gov <strong>2012</strong>FluMist ® PIEpipen ® patient insertEpiPen ® Administration1 2 3 41. Grasp unit in a fist with orange tip pointing downward. With other hand,pull off blue safety release .2. Hold orange tip near outer thigh.3. Swing and firmly p<strong>us</strong>h against outer thigh until it clicks so that unit isperpendicular (at a 90º angle) to the thigh. Hold firmly against thigh <strong>for</strong>ten seconds to deliver drug.4. Remove unit from thigh and massage injection area <strong>for</strong> 10 seconds.5. Call 911 and seek immediate medical attention. Take the <strong>us</strong>ed EpiPen®with you.Continuing EducationRequirements Updated by Ho<strong>us</strong>e Bill 509 (Vaccine Access Act)in <strong>2012</strong> 3-hour CE course biennially• M<strong>us</strong>t be offered by statewide professional association ofphysicians accredited to provide AMA PRA Category Icredit• May be offered in a distance-learning <strong>for</strong>mat M<strong>us</strong>t be included in 30 hours of CE Submit confirmation of completion to the board ofpharmacy on a <strong>for</strong>m provided by the board Failure to comply:• Revocation of authorization to administer a vaccine orepinephrine autoinjection• Authorization may be restored once requirementscompletedEpipen ® patient insertThe Florida Statute <strong>2012</strong>5
1/12/2013Continuing EducationCourse http://www.pharmacistonlinece.com/ Provided by the Florida Medical Association Online course Cost $75 Fulfills biennial CE requirement and meetss. 465.009, F.S requirements Reviews vaccine administration andimmunization essentials, specific to Florida(flu, pneumococcal, shingles vaccines)Pharmacist Role Increase awareness Educate patients and providers Identify and screen patients <strong>for</strong>vaccines Recommend appropriate vaccines For patients For <strong>for</strong>mulary Vaccinate!Terrie YC 2010Case StudyCase Study AnswersJL is a 68 year old woman who comesto your pharmacy <strong>for</strong> herimmunizations. She is allergic topenicillin and peanuts and has HTN,COPD, diabetes and generalizedanxiety disorder. She cannotremember if she had the chickenpox.Which vaccines would you administer?Influenza?Pneumococcal?Shingles?TIV (e.g. Fluvirin ® ) orTIV high-dose(Fluzone ® high-dose)PPSV 23(Pneumovax ® )Zostavax ®(4 weeks apart fromPneumovax ® )Test Questions1. [True or False] A pharmacist may administerthe influenza, pneumococcal and shinglesvaccines.True2. [True or False] The shingles vaccine isrecommended every five years <strong>for</strong> adults 60years of age and older.False3.[True or False] Pharmacists certified toimmunize m<strong>us</strong>t complete a 3-hour continuingeducation course every two years on the safeand effective administration of vaccines.TrueReferencesCenters <strong>for</strong> Disease Control and Prevention. CDC – seasonal influenza (flu) – key facts about influenza (flu) & fluvaccine. 28 Mar <strong>2012</strong>. Accessed 20 Dec <strong>2012</strong>. Available at: http://www.cdc.gov/flu/protect/keyfacts.htm.Centers <strong>for</strong> Disease Control and Prevention. CDC – shingles – about shingles – herpes zoster. 10 Jan 2011. Accessed20 Dec <strong>2012</strong>. Available at: http://www.cdc.gov/shingles/about/index.html.Centers <strong>for</strong> Disease Control and Prevention. Prevention and control of influenza with vaccines: recommendations of theAdvisory Committee on Immunization Practices (ACIP) – United States, <strong>2012</strong>-13 influenza season. MMWR. <strong>2012</strong>;61(32):613-8.Centers <strong>for</strong> Disease Control and Prevention. Updated recommendations <strong>for</strong> prevention of invasive pneumococcaldisease among adults <strong>us</strong>ing the 23-valent pneumococcal polysaccharide vaccine (PPSV23). MMWR. 2010;59(34):1102-1106.Centers <strong>for</strong> Disease Control and Prevention. Use of 13-valent pneumococcal conjugate vaccine and 23-valentpneumococcal polysaccharide vaccine <strong>for</strong> adults with immunocompromising conditions: recommendations of theAdvisory Committee on Immunization Practices (ACIP). MMWR. <strong>2012</strong>; 61(40):816-819.Centers <strong>for</strong> Disease Control and Prevention. Vaccines: Recs/Interim vaccine storage and handling guidance. 27 Nov<strong>2012</strong>. Accessed 20 Dec <strong>2012</strong>. Available at: http://www.cdc.gov/vaccines/recs/storage/interim.htm. Centers <strong>for</strong> Disease Control and Prevention. Vaccines: VPD-VAC/VPD menu page. 14 Mar <strong>2012</strong>. Accessed 20 Dec <strong>2012</strong>.Available at: http://www.cdc.gov/vaccines/vpd-vac/. Epipen ® [patient insert]. Meridian Medical Technologies. Napa, CA. Jul 2011. FluMist ® [package insert]. MedImmune, LLC. Gaithersburg, MD. Jul <strong>2012</strong>. Immunization Action Coalition. Screening checklist <strong>for</strong> contraindications to vaccines <strong>for</strong> adults. <strong>2012</strong> Oct. Accessed Dec<strong>2012</strong>. Available at: http://www.immunize.org/catg.d/p4065.pdf.Immunization Action Coalition. State mandates on immunization and vaccine-preventable diseases: state mandates.21 Jul 2009. Accessed 16 Dec <strong>2012</strong>. Available at: http://www.immunize.org/laws/. Pneumovax ® 23 [package insert].Merck & Co, Inc. Whiteho<strong>us</strong>e Station, NJ. Oct 2011. Prevnar ® 13 [package insert]. Wyeth Pharmaceuticals Inc. Philadelphia, PA. Aug <strong>2012</strong>. Sanofi Pasteur. Administration guide: Fluzone® intradermal. Jul <strong>2012</strong>. Accessed 02 Jan 2013. Available at:http://www.fluzone.com/health-care-professionals/pdf/Fluzone_Intradermal_AdminGuide.pdf. The Florida Legislature. Statutes & constitution: view statutes: online sunshine. 1995-<strong>2012</strong>. Accessed 16 Dec <strong>2012</strong>.Available at http://www.leg.state.fl.<strong>us</strong>/Statutes/. Terrie YC. Vaccinations: the expanding role of pharmacists. Pharmacy Times. 15 Jan 2010. Accessed 16 Dec <strong>2012</strong>.Available at: http://www.pharmacytimes.com/publications/issue/2010/January2010/FeatureFoc<strong>us</strong>Vaccinations-0110. Zostavax ® PI. [package insert].Merck & Co, Inc. Whiteho<strong>us</strong>e Station, NJ. Jun 2011.6
1/12/2013<strong>New</strong> Treatment Options in AdultCancer Pain: <strong>Implications</strong> <strong>for</strong>Pharmacotherapy and the Roleof the PharmacistMoe ShwinPGY-1 ResidentBaptist Hospital of Miami Define different types of painGoals & Objectives Describe etiology of adult cancer pain Identify barriers to pain management and the impact ofinadequate pain relief Compare and contrast available treatment options, includingnew agents, re<strong>for</strong>mulated agents and other treatment methods<strong>for</strong> acute and chronic pain Describe current strategies to prevent opioid ab<strong>us</strong>e and mis<strong>us</strong>e Address patient counseling points Recognize the role of the pharmacist and potential interventions<strong>for</strong> providing optimal pharmaceutical care in effective painmanagementEpidemiologyMcGill Pain Index ~ 1.6 million new cancer cases in <strong>2012</strong> ~ 12 million people are living with cancer Cancer pain occurs in: Advanced disease: ~ 75% Undergoing treatment: ~ 33% <strong>New</strong>ly diagnosed malignancies: ~ 25%Pain Scores454035302520151050American Cancer Society. Cancer facts & figures <strong>2012</strong>National Cancer Institute. Surveillance epidemiology and end results. Cancer statistics. Accessed December 27, <strong>2012</strong>.Adapted from: Melzack R. The McGill pain questionnaire: major properties and scoring mehtods. Pain. 1975 September; 1 (3): 277-99Etiology of Cancer PainEtiology of Cancer PainCancer ortumorInjury to somaticstructureNociceptive painChemotherapyCancerpainSurgicaltreatmentsCancer PainInjury to visceralstructureNeuropathic painInjury to theperipheral or centralnervo<strong>us</strong> system (CNS)Procedures1
1/12/2013Etiology of Cancer Pain Nociceptive pain: Activation of nociceptors Occurs often after surgical procedures or from bonemetastasisEtiology of Cancer Pain Neuropathic pain: Injury to the peripheral or central nervo<strong>us</strong> system(CNS)Somatic pain: (Skin, bone, joint, tissue)• Sharp, well localized, throbbing, and pressure-like painVisceral pain: (Internal organ)• More diff<strong>us</strong>e, aching , and cramping• Secondary to compression, infiltrationTingling, burning, sharp, or shooting• Pain due to spinal stenosis• Postherpetic pain• Adverse effect of chemotherapy:Vinca alkaloidsRadiationAmerican Pain Society. Guideline <strong>for</strong> the management of cancer pain in adults and children. 2004American Pharmacist Association. A pharmacist’s guide to the clinical assessment and management of pain. 2004American Pain Society. Guideline <strong>for</strong> the management of cancer pain in adults and children. 2004American Pharmacist Association. A pharmacist’s guide to the clinical assessment and management of pain. 2004Barriers to Pain ManagementProviderPatient & FamilySystem• Lack of awareness of patient’s pain• Lack of time• Inadequate training• Concern about legal or regulatory sanctions• Fear of addiction and dependence• Failure to mention pain to providers• Lack of adherence• Cost of medications• Lack of communication & coordination of care• Local laws & regulations• Availability of analgesicsAmerican Pain Society. Guideline <strong>for</strong> the management of cancer pain in adults and children. 2004Inadequate Pain Control Financial consequences ~ $100 billion each year Physiological consequences Endocrine/metabolic Cardiovascular Respiratory Gastrointestinal M<strong>us</strong>culoskeletal Immune Psychological consequences Quality of lifeAmerican Pharmacist Association. A pharmacist’s guide to the clinical assessment and management of pain. 2004.National Pharmaceutical Council. Pain: Current Understanding of Assessment,Management, and Treatments. Reston,VANon-opioids- Acetaminophen- NSAIDS- AspirinAdjuvants- Corticosteroids- Anticonvulsants- TCA’s- SNRIs- BisphosphonatesPharmacologic AgentsPhenanthrenes:- Morphine- Codeine- Hydrocodone- Hydromorphone- Oxycodone- Oxymorphone- NalbuphineOpioidsPhenylheptylamines:- MethadonePhenylpiperidines:- Meperidine- FentanylAmerican Pain Society. Guideline <strong>for</strong> the management of cancer pain in adults and children. 2004American Pharmacist Association. A pharmacist’s guide to the clinical assessment and management of pain. 2004Management of PainStep Severity of pain Recommended treatmentOneTwoThreeMild Pain(1-3)The World Health Organization (WHO) analgesic ladderMild- Moderate Pain(4-6)Moderate – Severe Pain(7-10)Non-opioid analgesics:NSAIDs, acetaminophen, aspirinOpioids:Codeine, hydrocodone, tramadol,morphine+/- Non-opioid+/- AdjuvantOpioids:Morphine ER, hydromorphone,oxycodone, fentanyl, methadone+/- Non-opioid+/- AdjuvantWorld Health Organization. Cancer. Palliative care: WHO’s pain relief ladder. Accessed December 27, <strong>2012</strong>.2
1/12/2013Acetaminophen (APAP) MOA: Inhibits the synthesis of prostagladins Blocks pain impulse generation Analgesic and antipyretic properties Lacks anti-inflammatory Dose: 325 – 650 mg PO Q4 – 6h Maximum daily dose: 2.5 g - 4 g Side effects: HepatotoxicityL<strong>us</strong>sier D. Adjuvant analgesics in cancer pain management. The Oncologist 2004; 9: 571-591NCCN: Clinical practice guidelines in oncology. Adult cancer pain. Version I.<strong>2012</strong>NSAIDs MOA: Binds to cyclooxygenase (COX) enzymes Inhibits the synthesis of prostaglandin Analgesic, antipyretic, anti-inflammatory Most <strong>us</strong>eful in bone pain Side effects: Cardiovascular Renal failure GI complications BleedingL<strong>us</strong>sier D. Adjuvant analgesics in cancer pain management. The Oncologist 2004; 9: 571-591NSAIDsAdjuvants<strong>Drug</strong> Dosing Maximum Daily Dose CommentsIbuprofen(Motrin®,Advil®)Ketorolac(Toradol®)Celecoxib(Celebrex®)400 mg Q6h 3,200 mg GI, renal, cardiactoxicities,ThrombocytopeniaBleeding15-30 mg IV Q6h(≤ 5 days)IM, IV: 120 mgIM, IV: 60 mg (age >65 years, weight < 50kg, renally impaired)100-200 mg Q12-24h 400 mg (hepaticimpairment, poorCYP2C9 metabolizers↓dosage by 50%)GI problemsBleedingRenal toxicityCardiac toxicitiesHeadacheUpper respiratoryinfectionAntman EM, Bennett JS, Daugherty A, et al. Use of nonsteroidal antiinflammatory drugs: an update <strong>for</strong> clinicians. A scientific statementfrom the American Heart Association. Circulation 2007; 115: 1634-42.<strong>Drug</strong> Dosing CommentsNeuropathic painTricyclic antidepressants(TCAs):Nortriptyline (Pamelor®),Desipramine (Norpramin®)Serotonin norepinephrinereuptake inhibitors(SNRIs):Duloxetine (Cymbalta®)Venlafaxine (Effexor®)Anticonvulsants:Gabapentin (Neurontin®)Pregabalin (Lyrica®)Start: 10 – 25 mg nightlyStart: 30 – 60 mg/dailyStart: 50 – 75 mg/d dailyStart: 100 – 300 mg nightlyStart: 150 mg daily individed doses- Cardiac side effects- Anticholinergic effects- Orthostatic hypotension- Serotonin syndrome- ↓tamoxifen (Nolvadex®)efficacy- Dose adj<strong>us</strong>tment requiredin renal impairmentNational comprehensive cancer network: Clinical practice guidelines in oncology. Adult cancer pain. Version I.<strong>2012</strong>Adjuvants<strong>Drug</strong> Dose CommentsBone PainCorticosteroids:DexamethasoneBisphosphanates:Pamidronate (Aredia®)Zoledronic acid (Zometa®)- 16 - 24 mg daily in divideddoses- 90 mg IV over 2h Q month- 4 mg IV over 15 min Qmonth-- C<strong>us</strong>hing’s syndrome- Osteoporosis- Infection- Edema- Neurologic effects- Electrolytes disturbance- Dose adj<strong>us</strong>tment in renaldysfunction- Osteonecrosis of jawNational comprehensive cancer network: Clinical practice guidelines in oncology. Adult cancer pain. Version I.<strong>2012</strong>General Principles of OpioidTherapy Goal is prevention of painIn chronic pain:• Around the clock + as-needed <strong>for</strong> breakthrough pain Appropriate dose: Relieves pain throughout the dosing interval withoutca<strong>us</strong>ing unmanageable side effects Full opioid agonists:• No analgesic ceiling or maximal recommended dose Oral route is preferred Cost effectiveness & ease of <strong>us</strong>eNational comprehensive cancer network: Clinical practice guidelines in oncology. Adult cancer pain. Version I.<strong>2012</strong>3
1/12/2013Opioid Terminology Opioid tolerant: Patients taking at least one week or longer:• 60 mg oral morphine/day,• 25 mcg transdermal fentanyl/hour,• 30 mg oral oxycodone/day,• 8 mg oral hydromorphone/day,• 25 mg oral oxymorphone/day, or• An equianalgesic dose of another opioid Addiction: Impaired control over drug <strong>us</strong>e Craving Physical dependence: Withdrawal syndrome Pseudoaddiction: “Clock watch” Pseudoaddiction vs addictionNCCN: Clinical practice guidelines in oncology. Adult cancer pain. Version I.<strong>2012</strong>Opioids MOA: Bind to receptors in the CNS Stimulate inhibitory descending pathways Opiate receptors: Mu, kappa, deltaMu receptors- Analgesia- Euphoria- Respiratory depression- Vomiting- Physical dependence- SedationKappa receptor- Analgesia- Sedation- MiosisDelta receptor- AnalgesiaAmerican Pain Society. Guideline <strong>for</strong> the management of cancer pain in adults and children. 2004American Pharmacist Association. A pharmacist’s guide to the clinical assessment and management of pain. 2004.PhenanthrenesPhenanthrenes<strong>Drug</strong> Parenteral Oral CommentsMorphine 10 30 - Starting dose: 5 – 30 mg PO Q 3 – 4 h- Long acting <strong>for</strong>mulations:- MS Contin® 15 – 30 mg PO Q 12 h- Kadian® 20 mg PO Q 24 h- Avinza® 30 mg PO Q 24 h- 90% metabolized hepatically to morphine-3-glucuronide (M3G) and morphine-6-glucuronide(M6G)- Can stimulate histamine release- Caution in renal dysfunctionCodeine 120 200 - Starting dose: 15 – 60 mg PO Q 3 – 4 h- Metabolized by CYP 2D6 into morphine- May ca<strong>us</strong>e more na<strong>us</strong>ea and constipation- Doses > 1.5 mg/kg are not recommended- Caution in renal dysfunction- Avoid <strong>us</strong>e in hepatic dysfunctionJohnson, S. Opioid safety in patients with renal or hepatic dysfunction. Pain-Topics. November 2007National Laboratory Certification Program. <strong>Drug</strong> testing matters. Opiates history and chemical structures. December 2011<strong>Drug</strong> Parenteral Oral CommentsHydrocodone(Lorcet®,Lortab®,Vicodin®,Vicoprofen®)Hydromorphone(Dilaudid®,Exalgo®)N/A 30 - Starting dose: 5 – 10 mg PO Q 3 – 4 h- Weak binding capacity <strong>for</strong> the mu receptor- Metabolized to hydromorphone by CYP 2D6- Only available in combination with non-opioids- Used with caution in hepatic dysfunction1.5 7.5 - Starting dose:- 2 – 4 mg PO Q 3 – 6 hr- 0.2—1 mg IV Q 2—3 hours- Long acting <strong>for</strong>mulation:- Exalgo® 8 – 64 mg PO Q 24 h- Metabolized in the liver, excreted in the urine- Used with caution in renal / hepatic dysfunctionJohnson, S. Opioid safety in patients with renal or hepatic dysfunction. Pain-Topics. November 2007National Laboratory Certification Program. <strong>Drug</strong> testing matters. Opiates history and chemical structures. December 2011PhenanthrenesPhenylpiperidines<strong>Drug</strong> Parenteral Oral CommentsOxycodone(Oxenta®,Oxycontin OP®)Oxymorphone(Opana®, OpanaER®)N/A 20 - Starting dose: 5 – 15 mg PO Q 3 – 4 h- Long acting <strong>for</strong>mulation:- Oxycontin® 10 mg PO Q 12 h- Metabolized by CYP 2D6- Good alternative to morphine- Used with caution in renal / hepatic dysfunction1 10 - Starting dose: 5 – 10 mg PO Q 4 – 6 h- Long acting <strong>for</strong>mulation:- Opana ER® 5 mg PO Q 12 h- Active metabolite of oxycodone- No significant histamine release- Used with caution in renal / hepatic dysfunction<strong>Drug</strong>Fentanyl(Sublimaze®)(Duragesic®)Meperidine(Demerol®)CommentsIV fentanyl 0.1 – 0.25 mg = 10 mg IV MorphineTD fentanyl 25 mcg/h = 20 mg/d IV Morphine; 60 mg PO Morphine- Patches are not recommended <strong>for</strong> acute and unstable pain- Frequency of the patch is <strong>us</strong>ually Q 48 - 72 h- Onset: 5 min <strong>for</strong> IV, 12 h <strong>for</strong> TD- Metabolized by CYP 3A4 to non-active metabolitesSwitching from TD fentanyl→ another opioid:- Wait ≥ 24 h <strong>for</strong> the full replacement doseIV fentanyl to TD fentanyl: 1:1Contraindications <strong>for</strong> TD fentanyl:- Fever, topical application of heat, or extreme exertion- Not recommended in chronic pain- High incidence of neurotoxicity due to metabolite nor-meperidine- Adverse effects of nor-meperidine are not reversible by naloxoneJohnson, S. Opioid safety in patients with renal or hepatic dysfunction. Pain-Topics. November 2007National Laboratory Certification Program. <strong>Drug</strong> testing matters. Opiates history and chemical structures. December 2011National Laboratory Certification Program. <strong>Drug</strong> testing matters. Opiates history and chemical structures. December 20114
1/12/2013PhenylheptylamineOpioid Conversion<strong>Drug</strong>Methadone(Dolophine®)CommentsMOA:- Binds to Mu, kappa, delta- Inhibits re-uptake of serotonin and norepinephrine- N-methyl-D-aspartate (NMDA) receptor- Half-life (~ 5 - 130 h)- Metabolized by liver into inactive metabolitesDose:- 2.5 – 10 mg PO Q 8 – 12 hConversion ratio:- Varies with the amount of opioid a patient has taking- Higher doses of opioids require lower doses of methadone Determine the total amount of opioid(s) taken in a 24 h period Calculate the equianalgesic dose of new opioid Effectively controlled pain: Reduce the dose by 25 – 50% Uncontrolled pain:Initiate new opioid with 100 – 125% of dose Breakthrough pain: 10 – 20% of total 24 h dose every 1 h as neededSide Effects:- QTc prolongation- <strong>Drug</strong> interaction with CYP 450 enzymes inducers/ inhibitorsNational Laboratory Certification Program. <strong>Drug</strong> testing matters. Opiates history and chemical structures. December 2011NCCN: Clinical practice guidelines in oncology. Adult cancer pain. Version I.<strong>2012</strong>Management of Opioid Side EffectsManagement of Opioid Side EffectsSide EffectPrevention & ManagementSide EffectPrevention & ManagementConstipationRespiratory depressionProphylaxis:- Stimulant laxative +/- stool softener- ↑Dietary fiber, ↑fluid intake- ExerciseIf constipation persists:- Lactulose, sorbitol, magnesium hydroxide,Prokinetic agent:- Metoclopramide (Reglan®) 10 – 20 mg PO four times/dayAfter failing 2 laxatives:- Methylnaltrexone (Relistor®) 0.15 mg/kg sub-Q x 1/ day- Higher risk in opioid naïve patients and limitedcardiopulmonary reserve- Titrate dosages gradually- Dilute naloxone (0.4 mg/mL) into 9 mL NS, give 1- 2 mLevery 30 – 60 seconds until symptoms improvedNa<strong>us</strong>eaPruritis- Metoclopramide (Reglan®) 10 – 20 mg PO Q 6 h PRN- Prochlorperazine (Compazine®) 10 mg PO Q 6 h PRN- Haloperidol (Haldol®) 0.5 – 1 mg PO Q 6 – 8 h PRNIf na<strong>us</strong>ea persists:- Administer around the clock <strong>for</strong> 1 week, then as needed- +/- serotonin antagonist or dexamethasoneIf na<strong>us</strong>ea persists <strong>for</strong> > 1 week:- Reassess ca<strong>us</strong>e and consider opioid rotation- Rash or hives:- Consider true allergy, change to another opiod- Diphenhydramine 25 – 50 mg IV or PO Q 6 hIf pruritis persists:- May change to another opiod- Nalbuphine (Nubain®) 0.5 – 1 mg IV Q 6 h- Naloxone (Narcan®) 0.25 - 1 mcg/kg/h continuo<strong>us</strong> inf<strong>us</strong>ionNCCN: Clinical practice guidelines in oncology. Adult cancer pain. Version I.<strong>2012</strong>NCCN: Clinical practice guidelines in oncology. Adult cancer pain. Version I.<strong>2012</strong>Pharmacist’s Role Provide medication recommendations to ensureadequate pain control Monitor and manage side effects Educate patient and family Prevent mis<strong>us</strong>e and ab<strong>us</strong>e Assist patients in overcoming legal, regulatory, andcost barriersCraig D. Introduction: Pharmacist role in pain management. Journal of Pharmacy Practice <strong>2012</strong>. 25: 496Prevention of Mis<strong>us</strong>e and Ab<strong>us</strong>eStrategies: Risk evaluation and mitigation strategy (REMS) Educational programs <strong>for</strong> prescribers Patient counseling documents Ab<strong>us</strong>e deterrent <strong>for</strong>mulations (ADFs) Exalgo® (hydromorphone ER), Oxycontin®(oxycodoneER),Remoxy®(oxycodone CR),Embeda®(morphine sulfate +naltrexone) Prescription drug monitoring program (PDMP) Electronic- Florida Online Reporting of ControlledSubstances Evaluation (E-FORCSE)5
1/12/2013E-FORCSEPer<strong>for</strong>mance MeasureResultsClinical decision- making 2.3 million timesDeaths ca<strong>us</strong>ed by oxycodone ↓ ~18% in 2011Overall drug deaths ↓ 6.3%C-II drugs from ≥ 5 PRESCRIBERS ↓ 58% (from 567 to 239)Patient CaseRH is a 67 y/o woman hospice patient with end-stage breast cancer. Shehas been receiving 20 mg/day of IV hydromorphone. Her pain has beencontrolled and the attending physician decides to switch RH fromhydromorphone to morphine extended-release, to be given Q 12h andmorphine immediate release Q 4h as needed <strong>for</strong> breakthrough pain. Thehospice policy <strong>for</strong> opioid conversion in effectively controlled pain is toreduce the new dose by 50%. Recommend appropriate doses <strong>for</strong> morphine.(Conversion factor: hydromorphone IV 1.5 mg = 30 mg PO morphine)Reduce dose by 50% = 200 mg PO MorphineMorphine ER 100 mg PO Q 12hBreakthrough dose = (15%) x 200 mg = 30 mg PO MorphineMorphine IR 30 mg PO Q 4h PRN= 400 mg PO MorphineFlorida Department of Health. Prescription drug monitoring program annual report. 2011 – <strong>2012</strong>. December <strong>2012</strong>.True/False Questions:ReferencesConstipation <strong>us</strong>ually occurs with opioid treatment, there<strong>for</strong>e administrationof prophylactic bowel regimen with a stimulant laxative with or without astool softener is recommended. (T/F) TRUEAccording to the U.S Food and <strong>Drug</strong> Administration (FDA), “patients takingat least 60 mg oral morphine per day or an equianalgesic dose of anotheropioid <strong>for</strong> one week or longer are considered as opioid tolerant. (T/F) TRUEBone pain, connective tissue pain, and neuropathic pain generally requireadjuvant therapies with NSAIDS, anti-inflammatories, or anticonvulsants.(T/F) TRUEAntman EM, Bennett JS, Daugherty A, et al. Use of nonsteroidal antiinflammatorydrugs: an update <strong>for</strong> clinicians. A scientific statement from the American HeartAssociation. Circulation 2007; 115: 1634-42. American Cancer Society. Cancer facts & figures <strong>2012</strong>American Pain Society. Guideline <strong>for</strong> the management of cancer pain in adults andchildren. 2004American Pharmacist Association. A pharmacist’s guide to the clinical assessmentand management of pain. 2004.Craig D. Introduction: Pharmacist role in pain management. Journal of PharmacyPractice <strong>2012</strong>. 25: 496Johnson, S. Opioid safety in patients with renal or hepatic dysfunction. Pain-Topics.November 2007 L<strong>us</strong>sier D. Adjuvant analgesics in cancer pain management. The Oncologist 2004; 9:571-591References Marc<strong>us</strong> D.; Epidemiology of cancer pain. Curr Pain Headache Rep (2011) 15:231 –234Melzack R. The McGill pain questionnaire: major properties and scoring mehtods.Pain. 1975 September; 1 (3): 277-99National Cancer Institute. Surveillance epidemiology and end results. Cancerstatistics. Accessed December 27, <strong>2012</strong>http://seer.cancer.gov/statfacts/html/all.htmlNational comprehensive cancer network: Clinical practice guidelines in oncology.Adult cancer pain. Version I.<strong>2012</strong>National Laboratory Certification Program. <strong>Drug</strong> testing matters. Opiates history andchemical structures. December 2011World Health Organization. Cancer. Palliative care: WHO’s pain relief ladder.Accessed December 27, <strong>2012</strong><strong>New</strong> Treatment Options inAdult Cancer PainMoe ShwinPGY-1 ResidentBaptist Hospital of Miami6
1/13/2013Learning ObjectivesCOPD: <strong>New</strong> Treatment Update<strong>Updates</strong> in the GOLD Practice GuidelinesPoe Aunggyi, PharmDPGY-1 Pharmacy ResidentCleveland Clinic Florida By the end of this presentation, participants shouldbe able toRecognize changes in the updated GOLD guidelinesIdentify acute exacerbations and optimize treatmentsRecognize and recommend new treatment options inappropriate patient populationAddress patient counseling pointsRecognize the role of the pharmacist and potentialinterventions <strong>for</strong> providing optimal care in COPDBurden of COPD Fourth leading ca<strong>us</strong>e of death (Global & U.S.) 24 million individuals in U.S. alone Economic burden Direct cost: 29 billion Indirect cost: 20 billionCOPD Definition1. Global Initiative <strong>for</strong> chronic obstructive lung disease: Global strategy <strong>for</strong> the diagnosis, management, and prevention of COPD. 2011. www.goldcopd.org.2. www.per<strong>for</strong>omist.comGlobal Initiative <strong>for</strong> chronic obstructive lung disease: Global strategy <strong>for</strong> the diagnosis, management, and prevention of COPD. 2011. www.goldcopd.orgInflammatory ProcessCigarette smoke and irritants Tobacco smokingRisk FactorsEpithelial cellsMacrophages Age greater than 40Inflammation Men > womenEmphysema(Inflammation of air sacs (alveoli))Chronic bronchitis(Inflammation of large airways) Alpha-1 antitrypsindeficiency1. healthline.com 2. bodybuilding.comGlobal Initiative <strong>for</strong> chronic obstructive lung disease: Global strategy <strong>for</strong> the diagnosis, management, and prevention of COPD. 2011. www.goldcopd.org.healthtap.com1
1/13/2013Key Indicators <strong>for</strong> Diagnosis Clinical Symptoms Dyspnea, chronic cough and sputum production,wheezing and chest tightnessSpirometry: Gold Standard! Post-bronchodilator FEV 1 /FVC ratio < 70% is required <strong>for</strong>diagnosis Staging and disease progression per FEV 1 History of exposure Tobacco smoke Occupational d<strong>us</strong>ts and chemicals Family history of COPD Physical examination Not present until lung function has significantlyimpairedGlobal Initiative <strong>for</strong> chronic obstructive lung disease: Global strategy <strong>for</strong> the diagnosis, management, and prevention of COPD. 2011. www.goldcopd.org.FEV 1 ≥80%predictedI: MildStaging of Airflow Limitation50% ≤ FEV 1 < 80%PredictedII: Moderate30% ≤ FEV 1 < 50%PredictedIII: SevereFEV 1 < 30%PredictedIV: Very SevereGlobal Initiative <strong>for</strong> chronic obstructive lung disease: Global strategy <strong>for</strong> the diagnosis, management, and prevention of COPD. 2011. www.goldcopd.org.GOLD ClassificationSymptom AssessmentRiskGold Classification of Airflow Limitation4321(C)(A)mMRC 0-1CAT
1/13/2013GOLD Pharmacologic OptionsCOPD Available AgentsBronchodilators• Beta-agonists• Anticholinergics• MethylxanthinesCorticosteroids• Inhaled• OralPhosphodiesterase-4 inhibitors• Roflumilast (Daliresp)Global Initiative <strong>for</strong> chronic obstructive lung disease: Global strategy <strong>for</strong> the diagnosis, management, and prevention of COPD. 2011. www.goldcopd.org.SABAsSAMAsLABAsLAMAsICSSCSCombinationsPDE 4 -I• Albuterol (Ventolin®, Proventil®, Airet®), albuterol sulfate (ProAir HFA®)• Levalbuterol (Xopenex®), pirbuterol acetate (Maxair®)• Ipratropium bromide (Atrovent®)• Salmeterol inhalation powder (Serevent®), <strong>for</strong>moterol (Foradil®)• Indacaterol (Arcapta Neohaler®)• Tiotropium bromide (Spiriva Handihaler®)• Refer to combination products• Methylprednisolone• Prednisone• Albuterol and ipratropium (Combivent®) (Duoneb®)• Salmeterol and fluticasone (ADVAIR DISKUS ® 250/50)• Formeterol and budesonide (Symbicort®)• Formoterol and mometasone.(Dulera®)• Roflumilast (Daliresp®)Therapies in Stable COPDGold RecommendationsGroup DGroup ASABAorSAMAAs PRN+Group BLABAorLAMA+Group CICSSame as C2 nd ChoicesICS+LAMA+LABA(Or)ICS+LABA+PDE 4 -I(or)LAMA+PDE 4 -IBronchodilators• LA > SA• Inhaled > oral• Theophylline aslast lineCorticosteroids• ICS in Grade C&D• Long-termmonotherapy NOTrecommended(Combination withLABA is more effective)PDE 4 -I• Roflumilast inGrade C & D• FEV1
1/13/2013Monitoring and Follow UpSpirometry Testing• Per<strong>for</strong>med at least once a yearChanges in symptoms• Cough and sputum, breathlessness, fatigue,activity limitation and sleep disturbances<strong>New</strong>er Options in COPDExacerbation history• Frequency, severity, and likely ca<strong>us</strong>es• Increased rescue inhaler <strong>us</strong>e• Antibiotic treatment or hospitalization1. nlm.nih.gov 2.soundcare.comProphylactic Antibiotic TherapyMacrolide prophylaxis (1yr) to reduce exacerbations?Azithromycin250mg dailyPlacebo FDA approved <strong>for</strong>severe COPDassociated with chronicbronchitis(GOLD: Grade C & D)Roflumilast (Daliresp ® )Exacerbation frequency (1.48 vs 1.83 per patient year)Time to first exacerbation (266 vs 174 days)GOLD guideline currently does not recommend this <strong>us</strong>e due tonegative benefit/risk ratioAzithromycin <strong>us</strong>e increased hearing impairment and resistance patterncompared to placebo groupAlbert et al. "Azithromycin <strong>for</strong> Prevention of Exacerbations of COPD." The <strong>New</strong> England Journal of Medicine 365 (2011): 689-98N Engl J Med 2011;365:689-98 Once daily oral 500mcg tab/day Contraindications Child-Pugh B or C Side effect profile Weight loss Psychiatric eventsDaliresp (roflumilast) [package insert]. St. Louis, MO:Forest Laboratories, Inc;2011 FebruaryRoflumilast in Symptomatic COPDRoflumilast Trials FindingsSubjects:• >40 yr oldTwo placebo-controlled, double blind, multicentre trials with identical design (ITT)• 20 pack year smoking hx• Clinical dx of COPD(FEV 1 /FVC
1/13/2013Patient Counseling Points How to take 500mcg tab/day orally MonitoringChanges in weight (-2kg during therapy)Psychiatric events (insomnia, anxiety and depression) Contraindications Strong CYP-3A4/1A2 inducers and inhibitors Liver impairmentDaliresp (roflumilast) [package insert]. St. Louis, MO:Forest Laboratories, Inc;2011 FebruaryIndacaterol (Arcapta ® ) Ultra-long-acting beta-2 agonist (LABA) First FDA approved LABA <strong>for</strong> once daily <strong>us</strong>e Only indicated <strong>for</strong> COPD, NOT asthma Place in therapy Moderate to severe COPD Advantage over other LABAs (QD vs BID) Comparable to once-daily tiotropium (Spiriva ® ) Limitation 75 mcg capsule/day FDA approved dose Below doses studied in majority of clinical trialsArcapta [package insert] . East Hanover, NJ: Novartis Corp; 2011Six Confirmatory RCTsTrial 3, 4, 5, 6, 7 & 8Study Findings: Trial 4 & 5Subjects:• > 40 yr old• Hx 10 Pyrs• FEV 1 30-80%• FEV 1/ FVC
1/13/2013Pharmacist Role Accurately classify patients according to GOLDmultidimensional grading system Optimize drug therapy based on patient’s COPDgrade Minimize side effects and drug interactions Apply evidence-based recommendations whenselecting treatment options Educate patients on co-morbidities commonlyassociated with COPDPatient Case JC is a 50 year old male with a smoking history of10 pack years. He has been diagnosed with COPD<strong>for</strong> 3 years. His repeated spirometry shows FEV 1of 50% predicted, his mMRC grading was 2 andhe had 1 exacerbation within last 10 months. What GOLD classification does JC fall under?1. Grade A2. Grade B3. Grade C4. Grade DQuestions (True or False)ReferencesUse of inhaled corticosteroids are appropriatein patients who are in GOLD Grade C.TRUEUse of azithromycin 250mg daily to preventexacerbation is accepted by GOLD 2011.FALSEUse of inhaled corticosteroids as monotherapyis not recommended by GOLD 2011.TRUEGlobal Initiative <strong>for</strong> chronic obstructive lung disease: Global strategy <strong>for</strong> the diagnosis,management, and prevention of COPD. 2011. www.goldcopd.org.Albert et al. "Azithromycin <strong>for</strong> Prevention of Exacerbations of COPD." The <strong>New</strong>England Journal of Medicine 365 (2011): 689-98Daliresp (roflumilast) [package insert]. St. Louis, MO:Forest Laboratories, Inc;2011 February Calverley PMA, Rabe KF, Goehring U-M, Kristiansen S, Fabbri LM, Martinez FJ; <strong>for</strong> the M2-124and M2-125 study groups. Roflumilast in symptomatic chronic obstructive pulmonary disease: tworandomised clinical trials. Lancet. 2009;374:685-694 Arcapta [package insert] . East Hanover, NJ: Novartis Corp; 2011Kerwin EM, Meli J, Peckitt C, et al. Efficacy and safety of indacaterol 75 µg once-daily in patientswith moderate-to-severe COPD. Am J Respir Crit Care Med. 2011;183:A1595.Imageswww.thinkcopdifferently.comhealthline.combodybuilding.comhealthtap.comper<strong>for</strong>omist.comdepositphotos.comazithromicin-rx.netThank You For YourKind Attention!!Poe Aunggyi, PharmDPGY-1 Pharmacy ResidentCleveland Clinic Floridaaungp@ccf.org6
1/13/2013ObjectivesPatient Instruction on the Use ofInhalant Devices and SpacersPursuant to GOLD GuidelinesDaphne Zeilinger, PharmD.PGY-1 Pharmacy ResidentPalmetto General HospitalJanuary 2013 Compare and contrast inhalation devices Disc<strong>us</strong>s the place in therapy of extension devices Review GOLD recommendations <strong>for</strong> the <strong>us</strong>e of devicesand spacers Demonstrate appropriate <strong>us</strong>e of dry powder/ aerosolgeneratingdevices Address patient counseling points Recognize the role of the pharmacist and potentialinterventions <strong>for</strong> providing optimal pharmaceutical carein COPDBackgroundRespiratory disorders Common respiratory disorders Asthma• 3 rd leading ca<strong>us</strong>e of preventable hospitalization• Resulting in more than 470,000 ER visits per year Chronic obstructive pulmonary disease (COPD)• 4 th leading ca<strong>us</strong>e of death in the US• Estimated direct costs in the US are 29.5 billion Inhaled delivery route is the mainstay of treatment <strong>for</strong> respiratorydisorders Numero<strong>us</strong> studies have identified sub-optimal inhaler technique as acommon problem in patients with respiratory diseaseAsthmahwww.nhlbi.nih.gov/health/health-topics/topics/asthma/COPDhttp://en.wikipedia.org/wiki/File:Copd_vers<strong>us</strong>_healthy_lung.jpgDiPiro et al Pharmacotherapy: A Pathophysiologic Approach.; 2011.GOLD guidelines 2011Goals of ManagementBenefits of Inhaled Therapy Maintain normal activity levels Maintain (near) normal pulmonary functions Prevent chronic and troublesome symptoms Prevent recurrent exacerbations Minimize emergency department visits or hospitalizations Improve symptoms while minimizing adverse effects Meet patients’ and families’ expectations of satisfactionwith care Allows a smaller dose to be administered Greater chance of efficacy Faster onset of action Fewer systemic side effectsNIH,. National Asthma Education and Prevention Program. Full Report of the Expert Panel:Guidelines <strong>for</strong> the Diagnosis and Management of Asthma (EPR-3); July 2007.1
1/13/2013Factors Affecting <strong>Drug</strong>DepositionEffects of Particle Size onDeposition of Aerosols Increased particle speed increases impaction in theoropharynx/ large conducting airways Slow aerosol speed allows more particles to penetratethe peripheral bronchial tree Holding breath increases gravitational sedimentation Particle size and speed are important• Ideal particle size <strong>for</strong> aerosols is 2- 5 micronshttp://www.cdc.gov/cancer/hpv/basic_info/cancers.htmBell J. Why optimise inhaler technique in asthma and COPD? Br. J. Prim Care Nurs 2,37-39 (2008).Pharmacologic Categories:Respiratory Inhalers Short-acting bronchodilators Long-acting bronchodilators Anticholinergics Inhaled corticosteroids Combination medications Long acting bronchodilator + InhaledcorticosteroidMethods of delivery Pressurized metered-dose inhaler(pMDI) Dry powdered inhaler (DPI) Breath-actuated metered-dose Soft mist inhalers NebulizerAssess all inhaler types a patientreceives and review instructions <strong>for</strong> allMetered Dose Inhalers (MDI)Instructions <strong>for</strong> <strong>us</strong>e of a MDIhttp://www.health.utah.gov/asthma/pdf_files/pharmacy/inhaler_techniques_hanouts.pdf2
1/13/2013Patient Mistakes When Using MDIs Failure to check <strong>for</strong> <strong>for</strong>eign objects in mouthpiece Not shaken well Not exhaling first Breathing in through their nose and not their mouth Poor timing and coordination <strong>for</strong> inhalation No ef<strong>for</strong>t to inhale slowly and <strong>for</strong> several seconds Pressing down more than one time Quick, fast inhalation vers<strong>us</strong> desired slow, deepinhalationExtension Devices Spacers/ Valved Holding Chambers (VHC) Produces a reservoir into which the drug aerosol isgenerated Can increase deposition within the lung Reduces particle velocity and size Decreases oropharyngeal deposition Reduces local adverse effects from ICS Vario<strong>us</strong> types available Diminishes need <strong>for</strong> patient to coordinate inhalation withinhaler actuationInstructions <strong>for</strong> Use of anAdult VHCBreath-actuated Metered-dose Inhalers Similar to traditional pMDIs but do not require the samecoordination between actuation and inhalation These devices do not allow the <strong>us</strong>e of a spacer device Aerosol is released from the canister with a minimum levelof inspiratory flow rate Inspiratory flow triggers device Consideration Patient ability to generate sufficientinspiratory flowhttp://www.health.utah.gov/asthma/pdf_files/pharmacy/inhaler_techniques_hanouts.pdfhttp://www.empr.com/maxair-autohaler/drug/2916/Dry Powder Inhalers Available in single or multi-dose inhalers Generation of the drug aerosol is driven by patientsinhalation A <strong>for</strong>ceful inspiration is required to ensure good lungdeposition Most frequently reported errors include: Failure to exhale first Failure to breath-hold after inhalation Incorrect positioning of the device Swallowing capsules Failure to generate enoughinspiratory flowInstructions <strong>for</strong> <strong>us</strong>e of a DPI1. Check that the mechanism is clean and the mouthpiece is free of obstruction2. Load and prepare the medication <strong>for</strong> inhalation3. Exhale slowly and completely without straining or breathing into your DPI(moisture from your breath can interfere with your DPI's function)4. Place your teeth over the mouthpiece and seal your lips around it5. Take a fast deep full inhalation to activate the flow of medication6. Try to hold the medication in your lungs <strong>for</strong> 10 seconds7. Let your breath out—but not into the inhaler8. For single-dose inhalers, open the inhaler, take out the <strong>us</strong>ed pill, and throw it awayhttp://rxmedicament.com/en/60-spiriva-18mcg-capsules-handihaler-rx-required.html3
1/13/2013Soft Mist InhalerCombivent Respimat ® http://www.respimat.com/ Combivent Respimat ® (ipratropium bromide/albuterol) Does not require a propellant or the patient’s inspiratory flowto generate an aerosol Combivent CFC MDI will be discontinued as of July 2013. High fine particles coupled with lowvelocity Longer duration of spray Not dependent on inspiratory flow rate Coordination of inhalation and actuationis simplifiedhttp://www.respimat.com/Nebulizers Include a battery/electrically operated device and amask or mouthpiece Each nebulizer has specific instructions <strong>for</strong> <strong>us</strong>e andcare Prime population Children Elderly Patients of any age who cannot <strong>us</strong>e an MDI withVHC and a face mask “Little randomized trial evidence <strong>for</strong> their benefit overother devices and <strong>us</strong>e will depend on preference,availibility, and price” – GOLD guidelinesInstructions <strong>for</strong> <strong>us</strong>e of aNebulizerhttp://www.health.utah.gov/asthma/pdf_files/pharmacy/inhaler_techniques_hanouts.pdfGOLD Guidelines on Inhalersand SpacersPharmacist-led Intervention Study to ImproveInhalation Technique in Asthma and COPD patients When patients require inhaled treatment, training ininhaler technique is essential Choice of inhaler device will depend on availability, cost,the prescribing physician, and the specific skills/ability ofthe patient Inhaler technique is important and should be re-checkedat EVERY visit For the MDI, addition of a large or small volume spaceroften overcomes coordination problems, improves lowerairway deposition and clinical benefit• 55 community pharmacists• 757 study participants• At baseline, 597 patients (78.9%)made at least one error inper<strong>for</strong>ming their inhalation• Number dropped to 214 (28.3%)from the first to the secondappointment (P < 0.001)• Average number of errors droppedfrom 2.5 to 0.5 per patient(P < 0.001)4
1/13/2013Short-acting bronchodilatorsLong-acting BronchodilatorsBrandMaxair®Autohaler®ProAir® Proventil® Ventolin® Xopenex®Generic pirbuterol acetate albuterol sulfate albuterol sulfate albuterol sulfate levalbuterol tartrateType of Inhaler breath actuated MDI HFA MDI HFA MDI HFA MDI HFA MDIDose Counter no no no yes no64 or 204 sprays; or 12 200 sprays; or 18Discard after 400 sprays 200 sprays or 24 months 200 sprays or 24 monthsmonthsmonthsAge approved age 12 and up age 4 and up age 4 and up age 4 and up age 4 and up1-2 inhalations every 4-6 1-2 inhalations every 4-6 1-2 inhalations every 4-6Dosing and 1-2 inhalations every 4-61-2 inhalations every 4-6hours or 15-30 minutes hours or 15-30 minutes hours or 15-30 minutesAdministrationhourshoursbe<strong>for</strong>e exercise be<strong>for</strong>e exercise be<strong>for</strong>e exerciseShake and spray 4 timesShake and spray 2 times Shake and spray 3 times Shake and spray 4 timesShake and spray 4 timesbe<strong>for</strong>e first <strong>us</strong>e, afterShaking and priming be<strong>for</strong>e first <strong>us</strong>e or after be<strong>for</strong>e first <strong>us</strong>e or after be<strong>for</strong>e first <strong>us</strong>e or afterbe<strong>for</strong>e first <strong>us</strong>e or afterdropping, or after 248 hours non-<strong>us</strong>e 2 weeks non-<strong>us</strong>e 2 weeks non-<strong>us</strong>e3 days non-<strong>us</strong>eweeks non-<strong>us</strong>eOnce a week or asrequired wipe Once a week remove Once a week remove Once a week remove Once a week removemouthpiece and inside canister and rinse plastic canister and rinse plastic canister and rinse plastic canister and rinse plasticCleaning Instructionssurface of protective actuator with warm actuator with warm actuator with warm actuator with warmflap with dry cloth or water; air dry water; air dry water; air dry water; air dryswabhttp://www.aanma.orgBrand Foradil® Aerolizer Serevent® Disk<strong>us</strong>Generic <strong>for</strong>moterol fumarate salmeterol xinafoateType of Inhaler DPI DPIDose Counter n/a yesDiscard after 60 capsules or 4 months 60 inhalations or 6 weeksAge approved age 5 and up age 4 and upDosing and Administration1 inhalation twice a day or 15minutesbe<strong>for</strong>e exercise; do not<strong>us</strong>e more frequently than every12 hours1 inhalation twice a day or 30minutes be<strong>for</strong>e exercise; do not<strong>us</strong>e more frequently than every12 hoursShaking and priming Do not shake or prime Do not shake or primeCleaning InstructionsDo not wash or take apart; keepdryDo not wash or take apart; keepdryhttp://www.aanma.orgAnticholinergicsInhaled CorticosteroidsBrand Atrovent® Combivent® Spiriva® HandiHalerGenericipratropium bromideipratropium bromide andalbuterol sulfatetiotropium bromideType of Inhaler HFA MDI CFC MDI DPIDose Counter no no n/aDiscard after 200 sprays 200 sprays 30 or 90 capsulesAge approved not specified not specified not specifiedDosing andAdministrationShaking and primingCleaning Instructions2 inhalations, 4 times a day 3 inhalations, 4 times a day 1 inhalation, once a dayDo not shake spray 2 times be<strong>for</strong>efirst <strong>us</strong>e or after 3 days non-<strong>us</strong>eOnce a week remove canister andrinse plastic actuator with warmwater; air dryShake (10 seconds) and spray 3times be<strong>for</strong>e first <strong>us</strong>e of after 24hours of non-<strong>us</strong>ewash mouthpiece with hot water;dry thoroughlyDo not shake or primeClean mouthpiece with moisttissue; once a month open devicefully and rinse with warm water; airdry <strong>for</strong> 24 hourshttp://www.aanma.orgAsmanex® Flovent®Pulmicort®Brand AeroBid® Alvesco®Flovent® HFAQVAR®Twisthaler Disk<strong>us</strong>Flexihalermometosone fluticasonebeclomethasonGeneric flunisolide ciclesonidefluticasone propionate budesonidefuroate propionatee dipropionateType of Inhaler CFC MDI HFA MDI DPI DPI HFA MDI DPI HFA MDIDose Counter no yes yes yes yes yes no30, 60, or 120 60 inhalations or60 or 120 100 or 120Discard after 100 sprays 60 sprays inhalations or 45 6 weeks or 2 120 spraysinhalations spraysdays monthsAge approved age 6 and up age 12 and up age 4 and up age 4 and up age 4 and up age 6 and up age 5 and upDosing andAdministration2 inhalations twicea day1 - 2 inhalationstwice a day1 - 2 inhalationstwice a day1 - 2 inhalationstwice a day2 inhalations twice aday1 - 2 inhalationstwice a day1 - 2 inhalationstwice a dayDo not shake;Shake and spray 4 timesDo not shake;spray 3 timesbe<strong>for</strong>e first <strong>us</strong>e; shakeDo not shake;spray 2 timesShaking and Shake be<strong>for</strong>e eachDo not shake or Do not shake ortwist and click 2be<strong>for</strong>e first <strong>us</strong>e orand spray once afterbe<strong>for</strong>e first <strong>us</strong>epriming<strong>us</strong>eprimeprimetimes be<strong>for</strong>e firstafter 10 days non<strong>us</strong>edropping or after 7 daysor after 10 days<strong>us</strong>eof non-<strong>us</strong>enon-<strong>us</strong>eEvery few daysOnce a week clean exitOnce a weekremove canister Once a week wipeOnce a weekAfter each <strong>us</strong>e Do not wash or port with damp cottonwip mouthpieceCleaning and rinse plastic mouthpiece withwipe mouthpiecewipe mouthpiece take apart; keep swab; wipe mouthpiecewith dry cloth;Instructions actuator with dray cloth; do notwith dry cloth;with dry cloth dry with damp tissue; airdo not <strong>us</strong>ewarm water; dry <strong>us</strong>e waterdo not <strong>us</strong>e waterdry overnightwaterthoroughlyhttp://www.aanma.orgCombination MedicationsBrand Advair Disk<strong>us</strong> ® Advair HFA® Dulera® Symbicort®mometasone furoate and budesonide andfluticasone propionate and fluticasone propionate andGeneric<strong>for</strong>moterol fumarate <strong>for</strong>moterol fumaratesalmeterol salmeterol xinafoatedihydratedihydrateType of Inhaler DPI HFA MDI HFA MDI HFA MDIDose Counter yes yes yes yesDiscard after 60 inhalations or 1 month 120 sprays 120 sprays 120 sprays or 3 monthsAge approved age 4 and up age 12 and up age 12 and up age 12 and up1 inhalation twice a day; 2 inhalations twice a day; 2 inhalations twice a day; 2 inhalations twice a day;do not <strong>us</strong>e more do not <strong>us</strong>e more do not <strong>us</strong>e more do not <strong>us</strong>e moreDosing and Administrationfrequently than every 12 frequently than every 12 frequently than every 12 frequently than every 12hourshourshourshoursShake and spray 4 times Shake and spray 4 timesShake and spray 2 timesShaking and priming Do not shake or prime be<strong>for</strong>e first <strong>us</strong>e or after 5 be<strong>for</strong>e first <strong>us</strong>e or after 5be<strong>for</strong>e first <strong>us</strong>e, afterdays non-<strong>us</strong>edays non-<strong>us</strong>edropping or after 7 daysnon-<strong>us</strong>eOnce weekly clean exit Once a week wipeOnce a week wipeDo not wash or take apart; port with dry cotton swab; mouthpiece with dry cloth;Cleaning Instructionsmouthpiece with dry cloth;keep dry wipe mouthpiece with do not remove canisterdo not <strong>us</strong>e waterdamp tissue; air dry from actuatorPharmacist's Impact Basic facts about Asthma/COPD Contrast between normal and restricted airways Roles of medications How medications work Long term control: reducing inflammation Quick Relief: short acting to relax m<strong>us</strong>cles aroundairways Skills Inhaler/Spacer <strong>us</strong>e (have them demonstrate) Symptom monitoring Environmental control measureshttp://www.aanma.org5
1/13/2013Rein<strong>for</strong>cement Phrases Stress the importance of <strong>us</strong>ing anti-inflammatorymedication every day Emphasize that anti-inflammatory medication will notprovide quick relief Show pictures of normal airways vs. inflamed airways Remind patients that there are two main types of inhalermedications- preventers and quick relievers “Your Rx today is ________” Stress that DPIs require deep, quick inhalation and MDIsrequire slow, coordinated inhalationSelection of Delivery Device Patient’s ability to <strong>us</strong>e the device correctly Preferences of the patient <strong>for</strong> the device Availability of the drug/device combination Uni<strong>for</strong>mity of all patients’ inhaled therapy via the sametype of device Compatibility between the drug and delivery device Time or skills to properly instruct the patient in the <strong>us</strong>e ofthe device or monitoring Cost of therapy/ reimbursementSummary COPD and Asthma are both common conditions with anincreasing prevalence Inhaled delivery of drugs is an essential component <strong>for</strong>the management of respiratory disease There are a wide variety of inhalers available and patientpreference should be considered Inhaler education is lacking and patients should beconstantly assessed <strong>for</strong> technique Inhaler technique training and education has beendemonstrated to be successful Pharmacists are in a key position to significantly impactpatients respiratory therapyT/F Questions Patients <strong>us</strong>ing a metered dose inhaler (MDI) should<strong>us</strong>e a slower inhalation compared with a dry powderinhaler (DPI), which requires a faster inhalation rate True /False When <strong>us</strong>ing a valved holding chamber (VHC), patientsshould be advised to inhale faster if a whistle is heard. True /False A dry powder inhaler (DPI) should be shaken <strong>for</strong> atleast 5 seconds prior to first <strong>us</strong>e True /FalseReferences Global Inititiative <strong>for</strong> Asthma. Global strategy <strong>for</strong> asthma management and prevention. http://www.ginasthma.com/ Global Initiative <strong>for</strong> Chronic Obstructive Disease. Global strategy <strong>for</strong> the diagnosis, management and prevention of chronic obstructive pulmonarydisease. http://www.goldcopd.org/ Device selection and outcomes of aerosol therapy: evidence-based guidelines*: american college of chest physicians/american college of asthma,allergy, and immunology Dolovich MB, Ahrens RC, Hess DR, et al. CHEST. 2005;127(1):335-371. Chronic Obstructive Pulmonary Disease:Data Fact Sheet. US Department of Health and Human Services, National Institutes of Health, NHLBI, NIHpublication 03-5529, March 2003 Bell J. Why optimise inhaler technique in asthma and COPD? Br. J. Prim Care Nurs 2,37-39 (2008). Kelly HW, Sorkness CA. Chapter 33. Asthma. In: Talbert RL, DiPiro JT, Matzke GR, Posey LM, Wells BG, Yee GC, eds. Pharmacotherapy: APathophysiologic Approach. 8th ed. <strong>New</strong> York: McGraw-Hill; 2011. http://www.accesspharmacy.com.lp.hscl.ufl.edu/content.aspx?aID=7975293.Accessed January 2, 2013. WILLIAMS DM, Bourdet SV. Chapter 34. Chronic Obstructive Pulmonary Disease. In: Talbert RL, DiPiro JT, Matzke GR, Posey LM, Wells BG, Yee GC,eds. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. <strong>New</strong> York: McGraw-Hill; 2011.http://www.accesspharmacy.com.lp.hscl.ufl.edu/content.aspx?aID=7975888. Accessed January 8, 2013. National Institutes of Health, National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program. Full Report of the ExpertPanel: Guidelines <strong>for</strong> the Diagnosis and Management of Asthma (EPR-3); July 2007. http://www.nhlbi.nih.gov.lp.hscl.ufl.edu/guidelines/asthma . Dolovich MA, MacIntyre NR, Dhand R, et al. Consens<strong>us</strong> conference on aerosols and delivery devices. Respir Care 2000;45:589–596. [PMID:10894452] Kelly HW. Comparison of inhaled corticosteroids: an update. Ann Pharmacother 2009; 43:519–527. [PMID: 19261959] Global Initiative <strong>for</strong> Chronic Obstructive Lung Disease. Global Strategy <strong>for</strong> the Diagnosis, Management, and Prevention of Chronic ObstructivePulmonary Disease. NHLBI/WHO workshop report. Bethesda, MD: National Heart, Lung, and Blood Institute; Updated November2011, http://www.goldcopd.com/ . National Institutes of Health, National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program. Full Report of theExpert Panel: Guidelines <strong>for</strong> the Diagnosis and Management of Asthma (EPR-3); July2007. http://www.nhlbi.nih.gov.lp.hscl.ufl.edu/guidelines/asthma . http://aaac.duhs.duke.edu/modules/aaac_ptrsrc/index.php?id=31#Valved www.respimat.com Pharmacist-led intervention study to improve inhalation technique in asthma and COPD patients. J Eval Clin Pract. 2011 Feb ;17(1):61-70. doi:10.1111/j.1365-2753.2010.01369.x. Epub 2010 Aug 30 . Dolovich MA, MacIntyre NR, Dhand R, et al. Consens<strong>us</strong> conference on aerosols and delivery devices. Respir Care 2000;45:589–596. [PMID:10894452] National Institutes of Health, National Heart, Lung and Blood Institute. NAEPP Expert Panel Report Managing Asthma During Pregnancy:Recommendations <strong>for</strong> Pharmacologic Treatment—Update 2004. NIH Publication No. 04–5246, March 2004. Chronic obstructive pulmonary disease (COPD) Fact sheet. American Lung Association. Feb 2010. Washington DC, available atwww.lung<strong>us</strong>a.org/lung-disease/COPD/resources/fact-figures/COPD-Fact-Sheet.html.6
1/11/2013National PracticeGuidelines on Issues inCritical Care:Shock, Nutrition, andthe Pharmacist’s RoleWho puts out theguidelines? The main source of guidelinesSociety of Critical Care Medicine (SCCM) Others American College of Cardiology (ACC) American College of CHEST Physicians (ACCP) American Society <strong>for</strong> Parenteral and EnteralNutrition (ASPEN) Infectio<strong>us</strong> Diseases Society of America (IDSA) National Institute <strong>for</strong> Health and ClinicalExcellence (NICE) Neurocritical Care Society (NCS)ObjectivesBy the end of this presentation you will be able to Identify the common symptoms and primarydiagnoses of patients in critical care Recognize the role of the critical carepharmacist and potential interventions <strong>for</strong>providing optimal pharmaceutical care in aninterdisciplinary team Differentiate between the vario<strong>us</strong>vasoconstrictors <strong>us</strong>ed <strong>for</strong> a patient in shock Distinguish the types of patients who mayrequire total parenteral nutrition from thosewho require enteral feedingWhat defines a criticalcare patient? A critical care patient is a patient with alife-threatening injury or illness Patient issues that may require criticalcare treatment include: Complications from surgery Accidents Infections Respiratory problems Functional declinePre-presentation Quiz1. Phenylephrine isthe preferredagent overnorepinephrine<strong>for</strong> a patient withhypotension andbradyarrythmiaTrue or False:2. Total parenteralnutrition is theideal source ofnutrients in thecritically illpatient3. Critical carepharmacists playan integral role inthe ICU settingWhat defines a criticalcare patient?Concerns to pay close attention towhile treating critical care patients Sepsis Shock Respiratory distress Nutritional stat<strong>us</strong>1
1/11/2013Role of the Critical CarePharmacistRole of thePharmacist Strive to educate other healthcarepractitioners when the needarises Emphasize the need <strong>for</strong> evidencebasedmedicine while followinghospital protocolsRole of the Critical CarePharmacistThe following encompasses the role of thecritical care pharmacist: To guarantee the safe and effective <strong>us</strong>eof medications in patients who arecritically ill To identify potential medication-relatedca<strong>us</strong>es of the patient’s current illness Understand the diagnostic criteria <strong>for</strong>vario<strong>us</strong> life-threatening illnesseswhich impact how a patient is treatedTreating CriticalCare Patients inShockRole of the Critical CarePharmacist Possess the ability to work as part ofan integrated team A rapid response to in<strong>for</strong>mation suchas the following <strong>for</strong> medicationmanagement: Electrolyte changes Culture results Changes inrenal function The patient’s vitalsigns Procedure resultsWhat is shock? Hypotension that cannot be correcteddespite proper res<strong>us</strong>citationtechniques Some other common features seenwith shock include: Tachycardia Diminished organ perf<strong>us</strong>ion Which may lead to the following: Hypoxemia Cardiac arrest2
1/11/2013What is shock? Hypovolemic shock Loss of plasma volume secondaryto hemorrhage or fluid loss Cardiogenic shock Ventricular failure that leads todiminished oxygen and nutrients to therest of the body Septic shock Severe infection that has led to acuteorgan dysfunction + shockNorepinephrine(Levophed ® )α > β Known as the most potent vasoconstrictor Works to stimulate alpha and beta-1receptors Effects alpha slightly more than beta Increases blood pressure, heart rate, andcoronary blood flow Dosage given as continuo<strong>us</strong> IV inf<strong>us</strong>ion 0.5-1 mcg/min Up to 30 mcg/min <strong>for</strong> response Mean arterialpressure (MAP)≥ 65 mmHgGoals <strong>for</strong> a patient inshock Central veno<strong>us</strong>pressure (CVP) ≥ 8 mmHg ≥ 12 mmHg ifpatient ismechanicallyventilated Urine output≥ 0.5 mL/kg/hrDopamine (Intropin ® )α β Dose-specific receptor stimulation and effects Dosage given as continuo<strong>us</strong> IV inf<strong>us</strong>ion Low dose: 0.5-2 mcg/kg/min• Primarily effects dopamine receptors leading torenal and mesenteric dilation Intermediate dose: 2-10 mcg/kg/min• Effects dopamine and beta-1 receptors withincreased renal dilation and heart rate High dose: 10-20 mcg/kg/min (or greaterup to 50 mcg/kg/min)• Primarily effects alpha receptorsincreasing blood pressureChoices <strong>for</strong> a patient inshock Norepinephrine*(Levophed ® ) Dopamine*(Intropin ® ) Dobutamine(Dobutrex ® ) Epinephrine(Adrenalin ® ) Midodrine(ProAmatine ® ) Phenylephrine(Neo-Synephrine ® ) Inamrinone(Inocor ® ) Milrinone(Primacor ® ) Vasopressin(Pitressin ® )*First-line choicesper the guidelinesDopamine (Intropin ® )α β Controversy among somepractitioners with dopamine <strong>us</strong>e Incidence of tachyarrythmias, especiallyatrial fibrillation is much greater withdopamine than norepinephrine This has led to a decrease indopamine’s <strong>us</strong>e despite currentguideline recommendations3
1/11/2013Dobutamine(Dobutrex ® )α < β Primarily stimulates beta-1 receptors Some effects on beta-2 and alphareceptors Increases contractility and heart rate Has minor effect on blood pressure Dosage given as continuo<strong>us</strong> IV inf<strong>us</strong>ion 2.5-20 mcg/kg/min Up to 40 mcg/kg/min <strong>for</strong> responsePhenylephrine (Neo-Synephrine ® ) Potent stimulator of alpha receptors Very weak stimulation of beta receptorsmay be seenα Reduces cardiac output while increasingblood pressure Has minimal to no effects on heart rate Dosage may be given IM, SQ, IV bol<strong>us</strong>,or via continuo<strong>us</strong> IV inf<strong>us</strong>ion Bol<strong>us</strong>: 0.1-0.5 mg/dose q 10-15 min Inf<strong>us</strong>ion: 100-180 mcg/minEpinephrine(Adrenalin ® )α β Stimulates alpha, beta-1, and beta-2receptors Noted as the most potent alpha stimulator Relaxes smooth m<strong>us</strong>cle in the bronchialtree Increases blood pressure and heart rate Dosage given as continuo<strong>us</strong> IV inf<strong>us</strong>ion 1-10 mcg/min Up to 20 mcg/min <strong>for</strong> responseInamrinone (Inocor ® ) A phosphodiesterase inhibitor that increasescellular levels of cAMP Increases cardiac output Acts a positive inotrope Reduces pre- and afterload Dosage given as IV bol<strong>us</strong> followed bycontinuo<strong>us</strong> IV inf<strong>us</strong>ion Bol<strong>us</strong>: 0.75 mg/kg bol<strong>us</strong> over 2-3 min (mayrepeat 30 minutes later) Inf<strong>us</strong>ion: 5-10 mcg/kg/min Max: 10 mg/kg in a 24-hour periodMidodrine(ProAmatine ® ) Active metabolite stimulates alpha-1receptors Result is an increase in bloodpressure with primary <strong>us</strong>e inorthostasis Dosage given orally Usual dose is 10 mg PO TID Max: 40 mg/day Dose needs to be renally adj<strong>us</strong>tedαMilrinone (Primacor ® ) Selective phosphodiesterase inhibitorof cardiac and vascular tissue Results in vasodilation and acts as apositive inotrope Dosage given as a continuo<strong>us</strong> IVinf<strong>us</strong>ion Loading dose of 50 mcg/kg over 10 min Maintenance: 0.375 to 0.75 mcg/kg/min4
1/11/2013Vasopressin (Pitressin ® ) Is an antidiuretic hormone analog Acts as a direct vasoconstrictor thatincreases cAMP levels Results in decreased urine volume andincreased osmolality Increases blood pressure with littleeffect on the heart rate Dosage given as a continuo<strong>us</strong> IVinf<strong>us</strong>ion 0.01-0.04 units/minEnteral Nutrition vs.Total Parenteral Nutrition Enteral Nutrition (EN) AKA “Tube feeding” Liquid nutrition consisting of proteins,carbohydrates, fats, vitamins, andminerals given through a tube insertedinto the stomach or small intestine Total Parenteral Nutrition (TPN) Fluid mixture given IV containingamino acids, sugars, lipids, vitamins,minerals, and other nutrientsShock: To sum it allup… Shock is a true emergency situationthat should be treated immediately Goals are to increase the MAP, CVP,and urine output Norepinephrine and dopamine arestill the preferred vasopressors Controversy over dopamine’s <strong>us</strong>e existsamong practitioners Other agents may be better <strong>for</strong> aparticular scenarioWhat the guidelines say EN is preferred over TPN in most cases EN should be started in critically illpatients who cannot satisfy theirnutritional requirements Nutrition should be withheld <strong>for</strong>patients in shock until res<strong>us</strong>citated EN in the small intestine is preferred ifThere is high risk <strong>for</strong> aspirationPatient has high gastric residualvolumesWhat the guidelines sayPatient NutritionStat<strong>us</strong> Minimize the amount of time apatient is NPO and get them on ENto prevent nutritional deficiency Monitor <strong>for</strong> tolerance of EN including Signs of pain Bowel sounds Passage of stool Electrolyte and lab changes5
1/11/2013What the guidelines say If EN is not <strong>us</strong>ed within 7 days of admission Preferable to go without nutritional supportthan to <strong>us</strong>e TPN• Risk <strong>for</strong> infection or even death increases withTPN <strong>us</strong>e TPN may be <strong>us</strong>ed in certain scenarios In patients who were not malnourished priorto admission but will be NPO <strong>for</strong> ≥ 7 days Can be <strong>us</strong>ed immediately in patients whoare malnourished upon admission if EN isunavailableA Patient Case Despite IV fluid, HR increased to 200 in atrialfibrillation and BP decreased to 60/40 After multiple cardioversion attempts andaddition of amiodarone drip, patient’s BPdropped to 140s in sin<strong>us</strong> tachycardia Vasopressin drip started at 0.03 units/min <strong>for</strong> BP Determined that patient had septic shock Patient was started on EN at 40 mL/hr After 6 days patient stable with normal BP andHR, as well as afebrile and tolerating ENNutrition: To sum it allup… If an ICU patient requires nutritionalsupport, EN is generally preferredover TPN Monitor <strong>for</strong> signs of improvement orworsening while receiving nutritionalsupport TPN is noted to increase the risk <strong>for</strong>infection and deathPost-presentation QuizTrue or False:1. Phenylephrine is the preferredagent over norepinephrine <strong>for</strong> apatient with hypotension andbradyarrythmia2. Total parenteral nutrition is theideal source of nutrients in thecritically ill patient3. Critical care pharmacists play anintegral role in the ICU settingA Patient Case 67 yo Caucasian male comes to ER withweakness, fatigue, decreased appetite, coughingblood x 5 days, and difficulty swallowing PMH: HTN, hyperlipidemia, COPD, arthralgia,lung and tonsilar cancer, agent orangeexposure, cataracts, GERD SH: (+)Tob, (+)EtOH, (-)IVDU FH: Father - pancreatic cancer; Mother/brother -head and neck cancer VS: BP - 81/52, HR - 156, Temp - 102.6°F(39.2°C)References Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign:international guidelines <strong>for</strong> management of severe sepsis and septic shock:2008. Crit Care Med. 2008 Jan;36(1):296-327. De Backer D, Biston P, Devriendt J, et al. Comparison of dopamine andnorepinephrine in the treatment of shock. N Engl J Med. 2010 Mar4;362(9):779-789. Martindale RG, McClave SA, Vanek VW, et al. Guidelines <strong>for</strong> the provision andassessment of nutrition support therapy in the adult critically ill patient:Society of Critical Care Medicine and American Society <strong>for</strong> Parenteral andEnteral Nutrition. Crit Care Med. 2009 May;37(5):1-30.Medline Pl<strong>us</strong>: Critical Care http://www.nlm.nih.gov/medlinepl<strong>us</strong>/criticalcare.htmlSociety of Critical Care Medicine Homepage http://www.sccm.org/Pages/default.aspxLearnICU.org Guidelines Page http://www.learnicu.org/Pages/Guidelines.aspxGlobalRPh: Vasopressors and Inotropes http://www.globalrph.com/icu-agents.htmAmerican Society <strong>for</strong> Parenteral and Enteral Nutrition Homepage http://www.nutritioncare.org/6
1/14/2013ObjectivesIDSA Practice Guidelines <strong>for</strong>Antimicrobial StewardshipProgramsDr. Joy A. Awoniyi, PharmD.PGY1 Clinical Pharmacy Practice ResidentMiami VA Healthcare System17 th Annual South Florida Residency SeminarSaturday, January 26, 2013 To provide a background on the implementation andutilization of Antimicrobial Stewardship Programs (ASPs) To disc<strong>us</strong>s the role of antimicrobial stewardship in thehealthcare setting To recognize the IDSA Guideline recommendations andtheir impact on pharmacy To describe the role of pharmacists in antimicrobialstewardship To recognize the role of the pharmacist and potentialinterventions <strong>for</strong> providing optimal pharmaceutical carewhile shepherding antimicrobial stewardship <strong>for</strong> theinstitution12“The microbes are educated to resist penicillin and ahost of penicillin-fast organisms is bred out…In suchcases the thoughtless person playing with penicillin ismorally responsible <strong>for</strong> the death of the man whofinally succumbs to infection with the penicillinresistantorganism. I hope this evil can be averted.”Sir Alexander Fleming<strong>New</strong> York TimesJune 26, 19453Timeline leading to AntimicrobialStewardship1990s1930s• Sulfonamides,penicillin andstreptomycinbecameavailable• Harnessing ofantibacterialagents <strong>for</strong>clinical <strong>us</strong>ebegins1940s• Penicillinresistance toStaph aure<strong>us</strong>is detected1960s• Staph aure<strong>us</strong>resistance tomethicillinemerges• MRSA isobserved inover 53% ofisolatesobtained fromICU patients ina USsurveillancesystem• IDSA/SHEApublished“Guidelines<strong>for</strong>AntimicrobialResistance inHospitals”4Present-day Issues Multi-drug resistance is a significant issueresulting increased morbidity, mortality,and healthcare costs In 2010, the World Health Organizationrecognized antimicrobial resistance as 1 ofthe 3 greatest threats to human health 50% of antimicrobial <strong>us</strong>e is inappropriate Recent decline in the development andapproval of newer antibacterial agents Increase incidence of Clostridium difficileassociated diarrhea and emergence ofresistance to treatment“Antimicrobial resistance is aglobal problem,and antimicrobial stewardshipprograms are the global solution.”Pharmacy Practice <strong>New</strong>sAug<strong>us</strong>t <strong>2012</strong>5 61
1/14/2013What is Antimicrobial Stewardship?“Coordinated interventions designed to improve andmeasure the appropriate <strong>us</strong>e of antimicrobial agentsby promoting the selection of the optimal antimicrobialdrug regimen including dosing, duration of therapy,and route of administration”The Society <strong>for</strong> Healthcare Epidemiology of America (SHEA), The Infectio<strong>us</strong> Diseases Society ofAmerica (IDSA) and the Pediatric Infectio<strong>us</strong> Diseases Society (PIDS)7IDSA/SHEA GUIDELINES FOR DEVELOPING ANINSTITUTIONAL PROGRAM TO ENHANCEANTIMICROBIAL STEWARDSHIPBACKGROUND Published in 2007 Developed and issued onbehalf of the IDSA andSHEAThe developmentof effective hospital basedstewardship programsAllpatients in acute carehospitalsCONTENTS Executive Summary Introduction including thepurpose and methods ofguideline development Evidence- basedRecommendations Members of ASP Team Elements of ASPs Research and FutureDirections8Purpose of AntimicrobialStewardship ProgramsSix Essential Elements Goals of Antimicrobial Stewardship Programs (ASPs)To optimize clinical outcomes whileminimizing unintended consequences of antimicrobial<strong>us</strong>eTo reduce health-care costs withoutadversely impacting quality of care Benefits of ASPs Financially self-supporting Improve patient care Increases appropriateness of antimicrobial <strong>us</strong>e Increased clinical cureSupplementalStrategiesActiveStrategiesIn<strong>for</strong>mationTechnologyEffectiveAntimicrobialStewardshipMicrobiologyLabMonitoring ofProcess andOutcomeMeasurementComprehensiveMultidisciplinaryTeam Approach9101. Active Strategies2. Supplemental StrategiesProspective audit ofantimicrobial <strong>us</strong>eShould include directinteraction and verbal orwritten feedback to providersMay be facilitated throughcomputer surveillanceShown beneficial in both largeand small hospitalsFormulary restriction andpreauthorization requirements<strong>for</strong> specific agentsReduces antimicrobial <strong>us</strong>e andcostEffectiveness ofpreauthorization depends onthe authorizing individualUtilize the Pharmacy andTherapeutics Committee orequivalent group Most frequently employedintervention Essential to improvingprescribing behavior Will enhance and increaseacceptance of stewardshipstrategies Development of evidencebasedpractice guidelinesthat incorporate localmicrobiology andresistance patterns Facilitation of guidelinesthrough education andfeedback11122
1/14/20132. Supplemental Strategies2. Supplemental Strategies Cycling refers to scheduledremoval and substitutionof a specific antibiotic orantibiotic class to preventor reverse resistance Insufficient data torecommend routine <strong>us</strong>e ofcycling <strong>for</strong> this purpose Decrease antimicrobialconsumption Aid in utilization of developedguidelines Example <strong>for</strong>ms available onCDC website at:http://www.cdc.gov/getsmart/healthcare/improveef<strong>for</strong>ts/tools.html Insufficient data torecommend routine <strong>us</strong>e ofcombination therapy toprevent resistance Recommended Use Empirical therapy <strong>for</strong>critically ill patients withMDR pathogens Increase breadth ofcoverage Increase likelihood ofadequate initial therapy Continuing broad therapycontributes to selection ofresistant pathogens Recommended to <strong>us</strong>e onthe basis of culture results Decreases antimicrobialexposure Substantial cost savings13142. Supplemental Strategies3. In<strong>for</strong>mation Technology Account <strong>for</strong> patientcharacteristics, ca<strong>us</strong>ativeorganism, infection site,and pharmacokinetic andpharmacodynamiccharacteristics of the drug Important component toantimicrobial stewardship Benefits Reduced length of hospitalstay Decreased healthcare cost Reduced incident ofcomplications related to IVaccess May be facilitated by thedevelopment of clinicalcriteria and guidelinesallowing conversion Options Computer Physician OrderEntry (CPOE) Use of electronic medicalrecords Incorporate data basedcomputer-identified values Microbiology C&S Hepatic and renal function <strong>Drug</strong>-drug interactions Allergies Cost Efficient targeting ofantimicrobial interventions Tracking of resistancepatterns Identification of NosocomialInfections Identification of adverse drugevents15164. Microbiology Laboratory5. Monitoring of Process andOutcome Measurements Critical role played in antimicrobialstewardship Timely identification of pathogens Per<strong>for</strong>mance of s<strong>us</strong>ceptibility testing Assists infection control ef<strong>for</strong>ts inresistance surveillanceProcessMeasures• Did the interventionresult in the desiredchange inantimicrobial <strong>us</strong>e? Useful in determiningimpact of theprogram onantimicrobial <strong>us</strong>e andresistance patterns Recommended Responsibilities Routine S<strong>us</strong>ceptibility testing Resistance surveillance involvement• Local antibiograms updated at leastannually Partner with infection control toinvestigate local outbreaks of infectionOutcomeMeasures• Did the processimplemented reduceor prevent unintendedconsequences? Investment in datasystems to allow <strong>for</strong>evaluation as aroutine measure ofquality improvement17183
1/14/20136. Comprehensive MultidisciplinaryAntimicrobial Management Programs Antimicrobial stewardship requires a team approachthat incorporates each element simultaneo<strong>us</strong>ly Hospital administrative support is essential Consens<strong>us</strong> building between administration andproviders should foc<strong>us</strong> on patient safety and carerather than policing These programs consistently demonstrate decrease inantimicrobial <strong>us</strong>e and hospital cost which pays <strong>for</strong> theprogram19The Stewardship Team Infectio<strong>us</strong> Diseases Physician Clinical Pharmacist with IDTraining Clinical Microbiologist In<strong>for</strong>mation System Specialist Infection Control Professional Hospital Epidemiologist20Recommended <strong>for</strong> InvestigationRecommended <strong>for</strong> InvestigationAntimicrobial CyclingEvaluation ofApproaches thatIncorporate Many ofthe Most EffectiveStrategiesRole of AntimicrobialStewardshipCombined withInfection ControlPracticesValidation thatHeterogeneo<strong>us</strong>Antimicrobial UseSlows ResistanceSpreadExamination ofStrategy Efficacy inSubpopulations ofHospitalized PatientsDetermination of theRelative Impact ofASPs on SpecificResistant BacteriaLong-term Impact ofFormulary Restrictionand PreauthorizationThe Ability ofAntimicrobials toCa<strong>us</strong>e “CollateralDamage” orEcological ResistanceDevelopment andValidation ofAutomatedSurveillance Strategies<strong>for</strong> NosocomialInfectionsDecision SupportSystems IncorporationAntimicrobialStewardship into CPOEEducation and Trainingof Infectio<strong>us</strong> DiseasesFellows and Pharmacistsin AntimicrobialStewardshipDevelopment and Costeffectivenessof morerapid and sensitivediagnostic testsInfluence ofPharmaceutical Ind<strong>us</strong>tryand Representatives onAntimicrobial PrescribingStrategies to StimulateResearch andDevelopment of NovelAntimicrobials2122Recent RecommendationsSHEA, IDSA, PIDS April <strong>2012</strong>1. Antimicrobial stewardship programs should berequired through regulatory mechanisms Recommended that Centers <strong>for</strong> Medicare and MedicaidServices require participating healthcare institutionsdevelop and implement ASPs CMS should improve programs by requiring additionalactivities2. Antimicrobial stewardship should be monitored inambulatory healthcare settings3. Education about antimicrobial resistance andantimicrobial stewardship m<strong>us</strong>t be accomplished23Recent RecommendationsSHEA, IDSA, PIDS April <strong>2012</strong>4. Antimicrobial <strong>us</strong>e data shouldbe collected and readilyavailable <strong>for</strong> both inpatientand outpatient settings5. Research on antimicrobialstewardship is needed andshould be funded by theappropriate federal agencies244
1/14/2013Recent RecommendationsSHEA, IDSA, PIDS April <strong>2012</strong>Recommended Minimum Requirements <strong>for</strong> ASPs Multidisciplinary teamincluding A physician A pharmacist A clinical microbiologist An infectionpreventionist Limited <strong>for</strong>mulary Institutional guidelines<strong>for</strong> managing commoninfection syndromes Additional interventionsto improve <strong>us</strong>e ofantimicrobials Processes to measureand monitoringantimicrobial <strong>us</strong>e at theinstitutional level Periodic distribution of afacility-specificantibiogram25Pharmacist Role in AntimicrobialStewardship“Pharmacists have a responsibility to take prominentroles in antimicrobial stewardship programs andparticipate in the infection prevention and controlprograms of health systems”American Society of Health-System PharmacistsPosition Statement, 201026Responsibilities of PharmacistsResponsibility to PromoteOptimal Use of AntimicrobialsPromoting Optimal Use ofAntimicrobial AgentsReducing Transmission of InfectionsEducating Health Professionals,Patients, and the Public Encourage multidisciplinarycollaboration Work within the P&TCommittee, or equivalentstructure, to ensure theappropriate agents areavailable Operate an ASP that utilizespatient outcomes to assesseffectiveness of policies Generate and analyzequantitative data onantimicrobial drug <strong>us</strong>e toper<strong>for</strong>m outcome analysis Work with laboratorypersonnel to ensureappropriate s<strong>us</strong>ceptibilitytests are reported in a timelymanner Work to compile anddistribute s<strong>us</strong>ceptibilityreports at least annually Utilize in<strong>for</strong>mationtechnology to enhancestewardship throughsurveillance Facilitate safe medicationmanagement practices2728Responsibility to ReduceTransmission of InfectionsResponsibility to Educate Others Participate in the infectionprevention and controlcommittee Establish internal pharmacypolicies, procedures andquality-control programs toprevent contamination ofpharmacy products Encourage <strong>us</strong>e of single-dosepackages rather thanmultiple-dose containers Recommend proper labeling,dating, and storage of sterileproducts and their containersEncourage routine immunizationof staff and those who mayimpact the patient careenvironmentPromote adherence to standardprecautions by those whoimpact the patient careenvironmentCollaborate in the developmentof guidelines <strong>for</strong> risk assessment,treatment, and monitoring ofindividuals in contact with atransmissible infectio<strong>us</strong> diseaseStrive <strong>for</strong> zero-tolerance ofhealth-care associated infections Provide educational <strong>for</strong>ums<strong>for</strong> healthcare professionalson stewardship-related topics Antimicrobial <strong>us</strong>e andresistance Decontaminating agents Aseptic technique andprocedures Sterilization methods Educate and counsel patientsregarding adherence toprescribed directions, storageand handling, proper disposal,and other infection controlproceduresParticipate in public healtheducation and awarenessprograms aimed and controllingspread of infectio<strong>us</strong> disease Prudent <strong>us</strong>e of antimicrobials Immunization access <strong>for</strong>children and adults Appropriate infectionprevention and controlmeasuresProvide exposure toantimicrobial stewardship andinfection prevention and controlpractices through training <strong>for</strong>pharmacists, students, residentsand research fellows29305
1/14/2013Review CaseJM is an active 15 year old girl who enjoys playingsoftball, swimming and running track. She was initiallypresented by her mother to the ER with a temperatureof 103 and complaining of fatigue x 1 week and pain inher hip.During the admission her WBC countswere normal and doctors stated therewere no signs of infection. She wassent home with a prescription <strong>for</strong>ibuprofen and told to follow-up in 3days.31Review CaseWithin 2 days she was brought backed to the ER as her symptomsseemed to worsen. She was admitted and blood cultures returnedpositive <strong>for</strong> Staphylococc<strong>us</strong> Aure<strong>us</strong>. JM was diagnosed with sepsis thathad begun as an abscess growing in her hip.The infection was accompanied by manycomplications including a DVT leading to PE,and pneumonia requiring intubation.Eventually, JM developed infections ca<strong>us</strong>ed bymultiple MDR organisms including ESBLproducingE. coli, S. Maltophilia, andEnterobacter aerogenesThe only antibiotic available to treat her infections was colistin. 5months later, after a lung transplant, suffering a stroke, and losing 30lbs, JM was discharged home. Her entire stay totaled 6 million dollarsin healthcare costs32Questions to Consider What roles could antimicrobial stewardship haveplayed in this case...To prepare <strong>for</strong> such a situation prior to admission?To preventing nosocomial infections during admission? What future changes could be made to thehospital’s policy? What role did or could have pharmacists playedin this case?InterventionsPatient, family, or provider education33True or False Questions1. Audits of restrictions and<strong>for</strong>mularies arerecommended by the IDSAas key antimicrobialstewardship activity2. Antimicrobial stewardship isthe practice of <strong>us</strong>ingantimicrobials appropriately3. Antimicrobial stewardshipdoes not need to bemonitored in ambulatoryhealthcare settingsTrueFalse34ReferencesASHP Statement on the Pharmacist’s Role in Antimicrobial Stewardship andInfection Prevention and Control. Am J Health-Sys Pharm.2010;67:575-7.Dellit TH, Owens RC, McGowan JE, et al. Infectio<strong>us</strong> Diseases Society of Americaand the Society <strong>for</strong> Healthcare Epidemiology of America Guidelines <strong>for</strong> Developingand Institutional Program to Enhance Antimicrobial Stewardship. ClinicalInfectio<strong>us</strong> Diseases, 2007;44:159-177.Infectio<strong>us</strong> Diseases Society of America. The 10x20 Initiative: pursuing a globalcommitment to develop 10 new antibacterial drugs by 2020. Clin Infect Dis2010;50;1081-1083.Goff DA, Bauer KA, Mangino JE. “Antimicrobial Stewardship Management ofInfections: Beyond the Cost of Antimicrobials”. Pharmacy Practice <strong>New</strong>s.McMahon Publishing, Aug<strong>us</strong>t <strong>2012</strong>.Society <strong>for</strong> Healthcare Epidemiology of America; Infectio<strong>us</strong> Diseases Society ofAmerica; Pediatric Infectio<strong>us</strong> Diseases Society. “Antimicrobial Stewardship PolicyStatement”. Infection Control and Hospital Epidemiology, April <strong>2012</strong>; 33(4):322-327.356
1/13/2013ObjectivesADA/EASD TreatmentGuidelines and Issues inDiabetesMarylee Worley, PharmDPGY-1 ResidentPalmetto General Hospital Describe the new ADA/EASD treatment guidelines Disc<strong>us</strong>s long term ACCORD trial results and how those canbe interpreted into clinical practice Describe the risks/benefits of each of the regimen optionslisted in the ADA/EASD treatment guidelines Address patient counseling points Recognize the role of the pharmacist and potentialinterventions <strong>for</strong> providing optimal pharmaceutical care inthe treatment of diabetesBackground Type 1 diabetes Accounts <strong>for</strong> about 5% of all diagnosed casesof diabetes Type 2 diabetes Accounts <strong>for</strong> about 95% of diagnosed diabetesin adults Gestational diabetes Develops in 2%–10% of pregnant womenAssociated Health Risks Diabetes remains a leading ca<strong>us</strong>e ofcardiovascular disorders, blindness, endstagerenal failure, amputations, andhospitalizations. It is also associated with increased risk ofcancer, serio<strong>us</strong> psychiatric illness, cognitivedecline, chronic liver disease, acceleratedarthritis, and other disabling or deadlyconditions.Centers <strong>for</strong> Disease Control and Prevention. Diabetes Report Card <strong>2012</strong>.Patient-Centered Care An approach to “providing care thatis respectful of and responsive toindividual patient preferences,needs, and values and ensuring thatpatient values guide all clinicaldecisions”Glycemic Measures <strong>for</strong> AdultsA1C
1/13/2013ADA/EASD HbA1c GoalsPatient-Centered Approach A1C goal <strong>for</strong> many adults is
1/13/2013Summary of Microvascular Results:ACCORD (Through the end of study)Now we know ourgoals…What are therecommendations on how toget there?ADA Recommendations on TherapySelection Type 1 DMAntihyperglycemic Therapy in Type 2Diabetes: General Recommendations Should be treated with MDI injections orcontinuo<strong>us</strong> subcutaneo<strong>us</strong> insulin inf<strong>us</strong>ion (A) Educate patients to match prandial insulin dose tocarbohydrate intake, premeal blood glucose, andanticipated activity (E) Should <strong>us</strong>e insulin analogs to reducehypoglycemia risk (A) Consider screening autoimmune diseases (B)Inzucchi S E et al. Dia Care <strong>2012</strong>;35:1364-1379ADA Recommendations onTherapy Selection Type 2 DM Met<strong>for</strong>min preferred initial agent (A) Add second oral agent or injectable (A)If noninsulin monotherapy at maximal tolerated dose doesnot achieve or maintain the A1C target over 3–6 monthsA GLP-1 receptor agonist, or insulin Insulin therapy, with or without additionalagents, from the outset (E)<strong>New</strong>ly diagnosed patients with markedly elevated bloodglucose levels or elevated A1COralTherapeutic optionsBiguanides- met<strong>for</strong>min (Glucophage)Sulfonylureas-glyburide (Diabeta), glipizide(Glucotrol), glimepiride (Amyl), Glyburidemicronized (Glynase)Thiazolidinediones- pioglitazone (Actos),rosiglitazone (Avandia)DPP-4 inhibitors- sitagliptin (Januvia), saxagliptin(Onglyza), linagliptin (Tradjenta)Meglitinides- nateglinide (Starlix) repaglinide(Prandin)α-glucosidase inhibitors- acarbose (Precose)miglitol (Glyset)Bile acid sequestrants- colesevelam (Welchol)InjectablesInsulinGLP-1 receptor agonists- exenatide(Byetta), exenatide extendedrelease, liraglutide (Victoza)Amylin mimetics- pramlintide(Symlin)Dopamine-2 agonists- bromocriptine (Cycloset)3
1/13/2013Comparison between agentsClass Mechanism Advantages Disadvantages CostBiguanides(Met<strong>for</strong>min)*1 st Line*Sulfonylureas/MeglitinidesThiazolidinedionesα-glucosidaseinhibitors• Activates AMPkinase• ↓ Hepatic glucoseproduction• Closes KATPchannels• ↑ Insulinsecretion• Activates PPAR-g• ↑ Insulinsensitivity• Inhibits a-glucosidase• Slowscarbohydrateabsorption• Extensive experience• No hypoglycemia• Weight neutral• ↓ CVD events (RecentSPREAD-DIMCADStudy)• Extensive experience• ↓ Microvascular risk• No hypoglycemia• Durability• ↓ TGs, ↑ HDL-C• ? ↓ CVD events (pio,NOT rosi)• No hypoglycemia• Nonsystemic• ↓ Post-prandialglucose• ? ↓ CVD events• Gastrointestinal AEs• Lactic acidosis• B-12 deficiency• Contraindications• Hypoglycemia• Weight gain• Low durability• Weight gain• Edema /HF• Bone fractures• May↑ MI (rosi)• May↑ Risk Bladderca (pio)• Gastrointestinal AEs• Dosing frequency• Modest ↓ A1cLowLowHighMod.Comparison between agentsClass Mechanism Advantages Disadvantages CostDPP-4inhibitorsGLP-1receptoragonistsAmylinmimeticsBile acidsequestrantsDopamine-2agonists• Inhibits DPP-4• Increases GLP-1, GIP• Activates GLP-1 receptor• ↑ Insulin, ↓ glucagon• ↓ gastric emptying• ↑ satiety• Activates amylinreceptor• ↓ glucagon• ↓ gastric emptying• ↑ satiety• Binds bile acids• ↓ Hepatic glucoseproduction• Activates DA receptor• Modulates hypothalamiccontrol of metabolism• ↑ Insulin sensitivity• No hypoglycemia• Well tolerated• Weight loss• No hypoglycemia• ? ↑Beta cell mass• ? CV protection• Weight loss• ↓ Post-prandialglucose• No hypoglycemia• Nonsystemic• ↓ LDL-C• No hypoglycemia• ? ↓ CVD events• Modest ↓ A1c• May ↑ RiskPancreatitis• Urticaria/angioedema• GI• ? Pancreatitis• Medullary ca• Injectable• GI SEs (N/V)• Modest ↓ A1c• Injectable• Hypoglycemia w/insulin• Dosing frequency• GI (mainlyconstipation)• Modest ↓ A1c• ↑ TGs• Dosing frequency• <strong>Drug</strong> Interactions• Modest ↓ A1c• Dizziness/syncope• Na<strong>us</strong>ea• FatigueHighHighHighHighHighADA/EASD SpecificRegimensADA/EASD SpecificRegimensBestRegimen:When Goal isto AvoidHypoglycemiaBestRegimen:When Goal isto AvoidWeight GainAntiplatelet regimens Consider aspirin therapy (75–162 mg/day) (C) As a primary prevention strategy in those with type 1 or type 2 diabetes atincreased cardiovascular risk (10-year risk >10%) Aspirin should not be recommended <strong>for</strong> CVD prevention <strong>for</strong> adultswith diabetes at low CVD risk, since potential adverse effects frombleeding likely offset potential benefits (C) 10-year CVD risk
1/13/2013Counseling PointsSulfonylureas Do not double dose, don't skip meals Take glipizide IR tab 30 min be<strong>for</strong>e mealsto enhance absorption Can ca<strong>us</strong>e hypoglycemia, so make surepatient is aware of signs/symptoms ofhypoglycemiaCounseling Points exenatide(Byetta) and liraglutide (Victoza) Increased risk <strong>for</strong> na<strong>us</strong>ea Usually mild and declines with continued treatment Injection technique 5 seconds hold (Byetta) or 6 seconds hold (Victoza) Byetta Doses should be administered anytime within 60 minutesbe<strong>for</strong>e the morning and evening meals, if missed dose, donot double up. J<strong>us</strong>t wait until the next meal and resumenormal dosing. Victoza Once daily dosing, regardless of meal timeCounseling Pointsα-glucosidase inhibitors MUST be taken with meals In<strong>for</strong>m physician when surgery orprocedure with contrast in needed Most effective when taken with complexcarbs ADR: Diarrhea, bloating, stomach gas(common) Actos ≠ AvandiaCounseling PointsTZDs Actos- Take without regard to meals, takemissed dose ASAP; do not double dose AVANDIA is available only through arestricted distribution program called theAVANDIA-Rosiglitazone Medicines AccessProgram.Counseling PointsDPP-4 inhibitors Taken once daily with or without food If a dose is missed, patients should be instructednot to double their next dose Patients should also be counseled on thesymptoms of hypoglycemia (e.g., sweating,weakness, conf<strong>us</strong>ion) Risk of pancreatitis- Patients should be in<strong>for</strong>medof signs or symptoms of pancreatitisCounseling Points BileAcid Sequestrant Welchol is contraindicated in patients w/: A history of bowel obstruction Serum TG concentrations >500 mg/dL A history of hypertriglyceridemia-inducedpancreatitis Give other medications 1 hour be<strong>for</strong>e or 4-6hours after taking Welchol5
1/13/2013Counseling PointsBromocriptine QR It should be taken once a day, within 2 hours afterwaking in the morning, with food The starting dose is 0.8 mg, which is increasedonce a week to an eventual tolerated dose of 2 – 6tablets per day (1.6 mg to 4.8 mg) Contraindications: taking ergot medications women who are breastfeeding those with history of fainting and migraine headaches Is weight neutral and does not increase the risk ofsevere hypoglycemiaTake Home Points Individualized glycemic targets and BG-lowering goals! Diet, exercise, and education Met<strong>for</strong>min = 1st-line drug (Unless contraindicated) After met<strong>for</strong>min, data are limited (<strong>for</strong> second line)Combination therapy with 1-2 other oral/injectable agentsis reasonable; minimize side effects All treatment decisions should be made in conjunction withthe patient (foc<strong>us</strong> on preferences, needs and values) Comprehensive CV risk reduction - a major foc<strong>us</strong> of therapy Think lipid lowering agents, antihypertensives andantiplatelets if indicatedCase Example MP is a 45 year old F who has type 2 DM and has been onmet<strong>for</strong>min <strong>for</strong> 2 years. She is overweight, and worriedabout weight gain. She has good insurance coverage. Shecomes in today <strong>for</strong> evaluation. Her labs are as follows: HbA1c= 8 % (1/26/13) HbA1c= 7.2% (4/3/<strong>2012</strong>) Fasting glucose in the clinic today= 160 mg/dL Home Meds:• Met<strong>for</strong>min 1000 mg bid• Lisinopril 10 mg daily• ASA 81 mg daily• Crestor 5 mg qhs What drug class/agent would you recommend?Role of the pharmacist Patient counseling Recognizing hypoglycemia symptoms Aware of SEs, timing of medication administration Glucose monitoring and BG goals Nutrition Appropriate injection technique Smoking Cessation Medication Compliance Identify barriers to self-managementT/F Question and AnswerAccording to ACCORD, intensive blood sugar control (HbA1c
1/14/2013ObjectivesAmerican College of Chest Physicians<strong>2012</strong> Guideline <strong>Updates</strong> Identify aspects of the Chest Guidelines 9thedition Be familiar with two new medications included inthe updated recommendations Address patient counseling points Recognize the role of the pharmacist andpotential interventions <strong>for</strong> providing optimalpharmaceutical care as outlined in the ChestGuidelinesKristin Morabito, PharmD, CPhPGY 1 ResidentCleveland Clinic FloridaACCP Guidelines 9 th ed. First evidence-based guidelines>25 years ago 18,400 members Released February <strong>2012</strong> Literature review• Jan 1, 2005 – October 2009 Minimized intellectual and financialconflict Patient’s values and preferences wereconsidered Accessibility Financial Impact 80% of panelists required to make astrong recommendationDefining RecommendationGrades Numbers: Strength of recommendation Benefits vs. Risk Letters: Quality of evidence A: High quality research Confidence B: More research could lead to moreconfidenceGuideline Year# of Grade 1ARecommendations2004 1232008 182<strong>2012</strong> 29 More room <strong>for</strong> interpretation compared toprevio<strong>us</strong> editionIntroduction to the Ninth Edition. Gordon Guyatt, etal.CHEST. <strong>2012</strong>;141(2_suppl):48S-52SDefining RecommendationGradesGrade Benefit vs. Risk Strength of SupportingEvidence1A2A2B2CBenefit clearly outweighsriskBenefit closely balancedwith risk (weakrecommendation)Benefit closely balancedwith risk (weakrecommendation)Benefit closely balancedwith risk (weakrecommendation)RCTs• Consistent evidence• Without importantlimitationsObservational studies• Exceptionally strongRCTs• Consistent evidence• Without importantlimitationsObservational studies• Exceptionally strongRCTs with limitationsHigher quality research may berequiredEvidence <strong>for</strong> at least one criticaloutcome from observationalstudy, case series, or RCT, withserio<strong>us</strong> flaws or indirectevidence.<strong>Implications</strong>Application to mostpatients in mostcircumstancesFurther research isvery unlikely to changeour confidence in therecommendationsBest action may differdepending oncircumstancesBest action may differdepending oncircumstanceAlternatives may beequally reasonable.Higher-quality researchlikely to have animportant impact onour confidence3.5 AnticoagulationManagement Services <strong>for</strong> VKAs Best Practices Statement We suggest that health-care providerswho manage oral anticoagulationtherapy should do so in a: systematic and coordinated fashionincorporating patient educationsystematic INR• testing• tracking• follow-upgood patient communication of results anddosing decisionsAntithrombotic Therapy and Prevention of Thrombosis, 9th Ed: American College of Chest Physician Evidence-Based Clinical Practice Guidelines.Walter Ageno, etal. CHEST. <strong>2012</strong>;141(2_suppl):e44S-e88S1
1/14/20132.1 Loading Dose <strong>for</strong> Initiation ofVitamin K Antagonist (VKA)Therapy “For patients sufficiently healthy to be treated asoutpatients, we suggest initiating VKA therapywith warfarin 10 mg daily <strong>for</strong> the first 2 daysfollowed by dosing based on internationalnormalized ratio (INR) measurements rather thanstarting with the estimated maintenance dose(2C).”2.1 Loading Dose <strong>for</strong> Initiation ofVitamin K Antagonist Therapy No additional dosing recommendations made Average half-life of clotting factors are about42 hours Does not take into consideration patientcharacteristics• Elderly• Hypoalbuminemia• CHF• Renal dysfunction• Liver disease• Interacting MedicationsAntithrombotic Therapy and Prevention of Thrombosis, 9th Ed: American College of Chest Physician Evidence-Based Clinical Practice Guidelines.Walter Ageno, etal. CHEST. <strong>2012</strong>;141(2_suppl):e44S-e88SAntithrombotic Therapy and Prevention of Thrombosis, 9th Ed: American College of Chest Physician Evidence-Based Clinical Practice Guidelines.Walter Ageno, etal. CHEST. <strong>2012</strong>;141(2_suppl):e44S-e88S3.1 Monitoring Frequencyand Management <strong>for</strong> VKAs For patients taking VKA therapy with consistentlystable INRs, we suggest an INR testing frequencyof up to 12 weeks rather than every 4 weeks (2B). May be <strong>us</strong>eful in well educated, stable, compliant, youngpatients INR home monitors may be another option For patients taking VKAs with previo<strong>us</strong>ly stabletherapeutic INRs who present with a single out-ofrangeINR of ≤ 0.5 below or above therapeutic,we suggest continuing the current dose andtesting the INR within 1 to 2 weeks (2C).Evaluating the Risk <strong>for</strong>StrokeCHADS 2 ScoreC Congestive heart failure 1 pointH Hypertension 1 pointA Age ≥ 75 years 1 pointD Diabetes 1 pointSStroke orTransient ischemic attackRisk Stratification0 points Low risk2 points1 point Moderate risk≥ 2 pointsHigh riskAntithrombotic Therapy and Prevention of Thrombosis, 9th Ed: American College of Chest Physician Evidence-Based Clinical Practice Guidelines.Walter Ageno, etal. CHEST. <strong>2012</strong>;141(2_suppl):e44S-e88SAntithrombotic Therapy and Prevention of Thrombosis, 9th Ed: American College of Chest Physician Evidence-Based ClinicalPractice Guidelines.Walter Ageno, etal. CHEST. <strong>2012</strong>;141(2_suppl):e44S-e88S2.1.8; 9; 10 Patients With NonvalvularAtrial Fibrillation (AF)CHEST 2008 1.1.2-1.1.4 CHEST <strong>2012</strong> 2.1.8-2.1.10Low RiskLong term aspirin therapy (1B)Intermediate RiskWarfarin (1A) or aspirin (1B)therapyHigh riskLong term warfarin therapy(1A)CHADS2 = 0No medication therapy (2B)CHADS2 = 1Oral anticoagulation therapy (1B)CHADS2 = 2 or
1/14/2013Dabigatran / Pradaxa®Mechanism of ActionRE-LY StudyRandomized Single Blind Study. n = 18,113Warfarintitrated toan INR2-3Dabigatran110mgorallytwice dailyDabigatran150mgorallytwice dailyPrimary End Point: Stroke or Systemic Embolism(non-inferiority, then superiority)CHADS 2 mean = 2.1TTR = 64% (mean)Micromedex <strong>Drug</strong> In<strong>for</strong>mation: Pradaxa. http://www.thomsonhc.com/micromedex2/librarian/. 15 Aug<strong>us</strong>t <strong>2012</strong>The <strong>New</strong> England Journal of Medicine. Re-ly Trial. 361; 12. 17 September 2009.RE-LY Trial ResultsDabigatran Etexilate / Pradaxa ®Dose / FrequencyHepatic dysfunction•CrCl >30ml/min: 150mg PO BID•CrCl 15-30ml/min: 75mg PO BIDDo not <strong>us</strong>e in Child-Pugh score C or D1.69%Half-life12-17 hoursWarfarin 1.69%Dabigatran 100mg dose 1.51%Dabigatran 150mg dose 1.11%1.53%1.11%Routing lab monitoringAntidote availableNone needed(Ecarin clotting time)aPTT and TT can be <strong>us</strong>ed to determineanticoagualtion, but not the extentNo•The rate of the primary outcome•Warfarin 1.69% vs Dabigatran 150 mg 1.11% (P < 0.001 <strong>for</strong> superiority•The rate of major bleeding•Warfarin 3.36% vs Dabigatran 150 mg 3.11% (P = 0.31)<strong>Drug</strong> InteractionsP-glycoproteinsRifampin (p-gp inducer)(dronederone or ketoconazole p-gp inhibitors)The <strong>New</strong> England Journal of Medicine. Re-ly Trial. 361; 12. 17 September 2009Micromedex <strong>Drug</strong> In<strong>for</strong>mation: Pradaxa. http://www.thomsonhc.com/micromedex2/librarian/. 15 Aug<strong>us</strong>t <strong>2012</strong>Dabigatran / PradaxaCapsule•Requires acidic environment <strong>for</strong> absorption•Most common side effect of dabigatran is dyspepsia; 6.1%•Tartaric acid makes up <strong>for</strong> some of the tartness in wine.•Rapid onset:•Time to maximum clot inhibition: 1 hr•No need <strong>for</strong> bridging•Store in original container not a medication organizer•60 day expiration after opening bottle•Moisture degrades medicationMicromedex <strong>Drug</strong> In<strong>for</strong>mation: Pradaxa. http://www.thomsonhc.com/micromedex2/librarian/. 15 Aug<strong>us</strong>t <strong>2012</strong>Transitioning fromDabigatran to WarfarinMedicationand doseWarfarinvario<strong>us</strong> tabletstrengthsDabigatran150mg tabletCost of a 30 daysupply +monitoring ifnecessary$ 70.00Including INRmonitoringInsurance coverage?• Likely$250.00 • May be in a different tier• Possibly a higher co-payConverting From WarfarinDabigatranDiscontinue warfarin and start dabigatran when INR
1/14/20132.0 Primary Prevention ofCardiovascular DiseaseFor persons aged 50 years or older withoutsymptomatic cardiovascular disease, we suggestlow-dose aspirin 75 to 100 mg daily over no aspirintherapy (2B). Remarks: Aspirin slightly reduces total mortality regardlessof cardiovascular risk profile if taken over 10 years. Moderate to high risk of CV events, the reduction inmyocardial infarction (MI) is closely balanced with an increasein major bleeds. People who are averse to taking medication over a prolongedtime period <strong>for</strong> very small benefits will be disinclined to <strong>us</strong>easpirin <strong>for</strong> primary prophylaxis. Individuals who value preventing an MI substantially higherthan avoiding a GI bleed will be, if they are in the moderate orhigh cardiovascular risk group, more likely to choose aspirin. Recent findings also demonstrate a cancer fighting benefit3.2 Choice of Antithrombotic TherapyFollowing ACS1 st year after ACSwithout PCI We recommend dualantiplatelet therapy ticagrelor 90 mg twice dailypl<strong>us</strong> low-dose aspirin 75-100mg daily, or clopidogrel 75 mg daily pl<strong>us</strong>low-dose aspirin 75-100 mgdailyover single antiplatelettherapy (1B).We suggest ticagrelor 90 mgdaily pl<strong>us</strong> low-dose aspirinover clopidogrel 75 mg dailypl<strong>us</strong> low-dose aspirin (2B).1 st year after ACSwith PCI We recommend dual antiplatelettherapy ticagrelor 90 mg twice daily pl<strong>us</strong>low-dose aspirin 75-100 mgdaily clopidogrel 75 mg daily pl<strong>us</strong>low-dose aspirin, or prasugrel 10 mg daily pl<strong>us</strong> lowdoseaspirinover single antiplatelettherapy) (1B). • We suggest ticagrelor 90 mgtwice daily pl<strong>us</strong> low-doseaspirin over clopidogrel 75 mgdaily pl<strong>us</strong> low-dose aspirin (2B).Primary and Secondary Prevention of Cardiovascular Disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed.Per Olav Vandivik. CHEST. <strong>2012</strong>;141(2_suppl):e637S-e668SRemarks: Evidence suggests that prasugrel results in no benefit net harm in patients with abody weight of < 60 kg, age > 75 years, or with a previo<strong>us</strong> stroke/transient ischemic attack.Primary and Secondary Prevention of Cardiovascular Disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed.Per Olav Vandivik. CHEST. <strong>2012</strong>;141(2_suppl):e637S-e668STicagrelor / Brilinta®Mechanism of ActionTicagrelor / Brilinta ®Dose / Frequency • Loading dose 180mg + ASA 325mg• Maintenance dose 90mg BID + ASA 99% protein bound; Vd: 88LMetabolism • Primarily Liver via CYP3A4Contraindications • Severe hepatic impairment (increased drugexposure and increased risk of bleeding)• History of intracranial hemorrhage• Active pathological bleeding• Ticagrelor and it’s active metabolite reversibly bind to the ADPreceptor site, P2Y12, on platelets preventing ADP from binding toplatelets, th<strong>us</strong> preventing platelet activation and aggregationMicromedex <strong>Drug</strong> In<strong>for</strong>mation: TIcagrelor. http://www.thomsonhc.com/micromedex2/librarian/. 15 December <strong>2012</strong>Micromedex <strong>Drug</strong> In<strong>for</strong>mation: TIcagrelor. http://www.thomsonhc.com/micromedex2/librarian/. 15 December <strong>2012</strong>Adverse EffectsTicagrelor / Brilinta ®Common• Bleeding, major and minor (8.7%)• Headache (6.5%)• Increase in serum creatinine (7.4%)• Dyspnea (13.8%)Serio<strong>us</strong>• Atrial fibrillation (4.2%)• Major bleeding (4.5%)<strong>Drug</strong> Interactions • Avoid strong CYP3A4/5 inhibitors• Avoid strong CYP3A4/5 inducersCounseling Points • ≤100 mg of aspirin• Discontinue at least 5 days prior to surgery• If possible, manage bleeding withoutdiscontinuing ticagerlorBlack Box WarningDo not <strong>us</strong>e in patients with active pathological bleeding.Do not start in patients planned to undergo urgent CABG.Ticagrelor / Brilinta®Counseling Advise patient to immediately reportsigns/symptoms of unanticipated, prolonged, orexcessive bleeding Hematuria Hematemesis Blood in the stool Nosebleeds Advise against early discontinuation ofmedication Advise patient not to take more than 100mg ofaspirin, or aspirin containing products.Micromedex <strong>Drug</strong> In<strong>for</strong>mation: Pradaxa. http://www.thomsonhc.com/micromedex2/librarian/. 15 Aug<strong>us</strong>t <strong>2012</strong>Micromedex <strong>Drug</strong> In<strong>for</strong>mation: TIcagrelor. http://www.thomsonhc.com/micromedex2/librarian/. 15 December <strong>2012</strong>4
1/14/2013PLATO TrialMulticenter, randomized, double-blind, double-dummy study. n = 18,624Aspirin 75 – 100 mg once daily(higher doses were permitted)Ticagrelor180mg,followed by90mgtwice dailyClopidogrel300-600mg,followed by75mg dailyPrimary End Point: Time to first occurrence of nonfatal MI,nonfatal stroke, or death from vascular ca<strong>us</strong>esPatients were treated up to 12 monthsIntent to treat analysis•The rate of the primary endpoint•Clopidogrel 11.7% vs Ticagrelor 9.8% (P < 0.001 <strong>for</strong> superiority)•The rate of major bleeding•Clopidogrel 11.2% vs Ticagrelor 11.6% (P = 0.43)The <strong>New</strong> England Journal of Medicine 361; 12. 17 September 2009.The <strong>New</strong> England Journal of Medicine 361; 12. 17 September 2009Transitioning fromClopidogrel to Ticagrelor4.1.1-4 Choice of AntithromboticTherapy following elective PCIMedication anddoseClopidogrel75mg tabletTicagrelor90mg tabletCost of a 30 daysupplyConverting From Clopidogrel$11.00 • LikelyInsurancecoverage?$252.00 • Possibly• Could be ahigher co-payTicagrelorStop Clopidogrel, and start Ticagrelor 24 hours later•Issues to consider: Clopidogrel resistance Patient compliance CostElective PCI with BMSstent placementFor the first month Aspirin 75-325 mg daily + Clopidogrel 75 mg daily Over single antiplatelettherapy(1A)For the subsequent 11 months Low-dose aspirin 75 – 100 mgdaily + Clopidogrel 75 mg daily Over single antiplatelet therapy(2C)After 12 months Single antiplatelet therapy isrecommended over dualantiplatelet therapy (1B)Elective PCI with DESstent placementFor the first 3 – 6 months3 months <strong>for</strong> sirolim<strong>us</strong> stents6 months <strong>for</strong> paclitaxel stents Aspirin 75 – 325 mg daily + Clopidogrel 75 mg daily Over single antiplatelet therapy(1A)For next 9 – 6 months respectively Aspirin 75 – 100 mg daily + Clopidogrel 75 mg daily (2C)After 12 months Single antiplatelet therapy isrecommended over dualantiplatelet therapy (1B)Micromedex <strong>Drug</strong> In<strong>for</strong>mation: TIcagrelor. http://www.thomsonhc.com/micromedex2/librarian/. 15 December <strong>2012</strong>Primary and Secondary Prevention of Cardiovascular Disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed.Per Olav Vandivik. CHEST. <strong>2012</strong>;141(2_suppl):e637S-e668S4.1.1-4 Choice of AntithromboticTherapy following elective PCIElective PCI with no stent placement For the first month Aspirin 75 – 325 mg daily + Clopidogrel 75 mg daily Over single antiplatelet therapy (2C) Single antiplatelet therapy is recommendedthereafter per the “established coronary arterydisease” guidelinesPrimary and Secondary Prevention of Cardiovascular Disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed.Per Olav Vandivik. CHEST. <strong>2012</strong>;141(2_suppl):e637S-e668S3.1 Choice of AntithromboticTherapy <strong>for</strong> Patients withEstablished CAD Established coronary artery disease1 year post ACS with• Prior revascularation• Coronary stenosis >50% by coronary angiogram +/-• Evidence <strong>for</strong> cardiac ischemia ischemia on diagnostictestingLong-term single antiplatelet therapy with• Aspirin 75 – 100 mg daily OR• Clopidogrel 75 mg daily• Over no antiplatelet therapy (1A)Single over dual antiplatelet therapy withaspirin pl<strong>us</strong> clopidogrel (2B)• No benefit and possible harm <strong>for</strong> continuing dualantiplatelet therapy beyond 1 yearPrimary and Secondary Prevention of Cardiovascular Disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed.Per Olav Vandivik. CHEST. <strong>2012</strong>;141(2_suppl):e637S-e668S5
1/14/2013What is the Pharmacist’sRole? Educate prescribers on guidelinerecommendations Assist in selection of therapeutic agents: Patient specific risk factors Cost Tolerability Patient preference or values Potential drug interactions Educate our patients Indication Proper administration The potential <strong>for</strong> drug interactionsWE CAN IMPROVE OUTCOMES!QuestionsDr. Smith orders pradaxa/ dabigatran 150mg BID <strong>for</strong> a patient.The patient is a 64 year old patient with paroxysmal atrialfibrillation. The patients CrCl = 27.0 ml/min. This is anappropriate dose <strong>for</strong> this patient? True or False?It is important to tell patients to store Pradaxa in it’s originalpackage.True or False?Ticagrelor can be taken with one aspirin 325mg tablet daily? True or False?Every patient over the age of 50 without symptomaticcardiovascular disease should be taking low dose aspirin? True or False?Any Questions?Thank You !6



