Notice of Reimbursement Arrangements - Department of Human ...
Notice of Reimbursement Arrangements - Department of Human ...
Notice of Reimbursement Arrangements - Department of Human ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
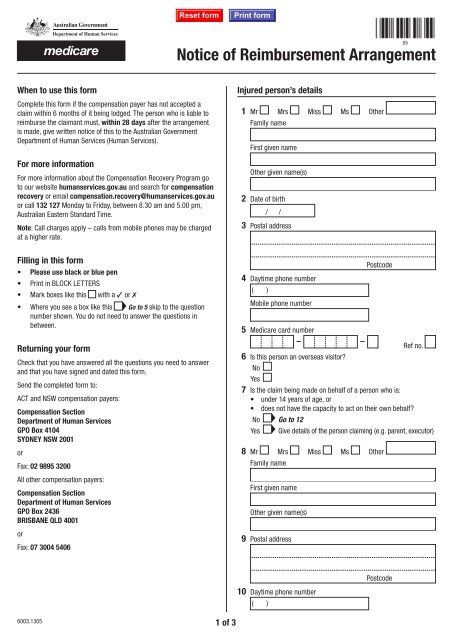
<strong>Notice</strong> <strong>of</strong> <strong>Reimbursement</strong> Arrangement05When to use this formComplete this form if the compensation payer has not accepted aclaim within 6 months <strong>of</strong> it being lodged. The person who is liable toreimburse the claimant must, within 28 days after the arrangementis made, give written notice <strong>of</strong> this to the Australian Government<strong>Department</strong> <strong>of</strong> <strong>Human</strong> Services (<strong>Human</strong> Services).For more informationFor more information about the Compensation Recovery Program goto our website humanservices.gov.au and search for compensationrecovery or email compensation.recovery@humanservices.gov.auor call 132 127 Monday to Friday, between 8.30 am and 5.00 pm,Australian Eastern Standard Time.Note: Call charges apply – calls from mobile phones may be chargedat a higher rate.Injured person’s details1 Mr Mrs Miss Ms OtherFamily nameFirst given nameOther given name(s)2 Date <strong>of</strong> birth/ /3 Postal addressFilling in this form• Please use black or blue pen• Print in BLOCK LETTERS• Mark boxes like this with a ✓ or 7• Where you see a box like this Go to 5 skip to the questionnumber shown. You do not need to answer the questions inbetween.4 Daytime phone number( )Mobile phone number5 Medicare card numberPostcodeReturning your formCheck that you have answered all the questions you need to answerand that you have signed and dated this form.Send the completed form to:ACT and NSW compensation payers:Compensation Section<strong>Department</strong> <strong>of</strong> <strong>Human</strong> ServicesGPO Box 4104SYDNEY NSW 2001orFax: 02 9895 3200All other compensation payers:Compensation Section<strong>Department</strong> <strong>of</strong> <strong>Human</strong> ServicesGPO Box 2436BRISBANE QLD 4001orFax: 07 3004 5406 Ref no.6 Is this person an overseas visitor?NoYes7 Is the claim being made on behalf <strong>of</strong> a person who is:• under 14 years <strong>of</strong> age, or• does not have the capacity to act on their own behalf?No Go to 12Yes Give details <strong>of</strong> the person claiming (e.g. parent, executor)8 Mr Mrs Miss Ms OtherFamily nameFirst given nameOther given name(s)9 Postal address10 Daytime phone number( )Postcode6003.1305 1 <strong>of</strong> 3
Mobile phone numberEmail20 Does this claim involve more than one compensation payer?NoYesnames <strong>of</strong> the other compensation payers@11 Relationship to the injured person (e.g. parent, executor)Injured person's solicitor's details12 Solicitor's reference13 Name <strong>of</strong> firm14 Postal addressClaim details21 Date <strong>of</strong> injury or injuries/ /22 Type <strong>of</strong> Compensation being claimed:Workers CompensationMotor Vehicle AccidentTransport Accident CommissionCommon LawPublic LiabilityOtherProvide details15 Work phone number( )Fax number( )EmailPostcode23 Brief description <strong>of</strong> the injury or injuries@Compensation payer’s details16 Compensation payer's reference17 Name <strong>of</strong> compensation payer18 Postal address19 Work phone number( )Fax number( )Email@Postcode<strong>Reimbursement</strong> arrangement details24 Date claim for compensation was lodged/ /25 Date reimbursement arrangement was made/ /Declaration26 I declare that:• the information provided in this form is complete and correct.I understand that:• giving false or misleading information is a serious <strong>of</strong>fence.Full nameTitle (e.g. claimant, compensation manager, compensationassessor, solicitor)SignatureDate- / /6003.1305 2 <strong>of</strong> 3
Privacy noticeCentrelink, Medicare, Child Support and CRS Australia are serviceswithin the Australian Government <strong>Department</strong> <strong>of</strong> <strong>Human</strong> Services(<strong>Human</strong> Services).Your personal information is protected by law, including thePrivacy Act 1988. Your information is collected for Social Security,Family Assistance, Medicare, Child Support and CRS purposes. Thisinformation may be required by the powers provided within eachservices’ legislation or voluntarily given by you when you apply forservices or payments.Your information will be used for the assessment and administration<strong>of</strong> payments and services. Your information may also be used within<strong>Human</strong> Services, where you have provided consent or it is required orauthorised by law. <strong>Human</strong> Services may disclose your information toCommonwealth <strong>Department</strong>s, other persons, bodies or agencies ONLYwhere you have provided consent or it is required or authorised by law.You can get more information about privacy by going to our websitehumanservices.gov.au/privacy or requesting a copy <strong>of</strong> the fullprivacy policy at any <strong>of</strong> our Service Centres.6003.1305 3 <strong>of</strong> 3