

GUIDELINES - The Endocrine Society
GUIDELINES - The Endocrine Society
GUIDELINES - The Endocrine Society

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
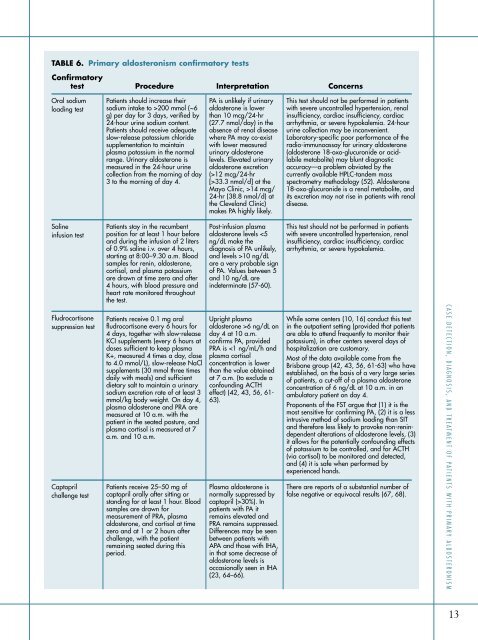
TABLE 6. Primary aldosteronism confirmatory testsConfirmatorytest Procedure Interpretation ConcernsOral sodiumloading testPatients should increase theirsodium intake to >200 mmol (~6g) per day for 3 days, verified by24-hour urine sodium content.Patients should receive adequateslow-release potassium chloridesupplementation to maintainplasma potassium in the normalrange. Urinary aldosterone ismeasured in the 24-hour urinecollection from the morning of day3 to the morning of day 4.PA is unlikely if urinaryaldosterone is lowerthan 10 mcg/24-hr(27.7 nmol/day) in theabsence of renal diseasewhere PA may co-existwith lower measuredurinary aldosteronelevels. Elevated urinaryaldosterone excretion(>12 mcg/24-hr[>33.3 nmol/d] at theMayo Clinic, >14 mcg/24-hr (38.8 nmol/d) atthe Cleveland Clinic)makes PA highly likely.This test should not be performed in patientswith severe uncontrolled hypertension, renalinsufficiency, cardiac insufficiency, cardiacarrhythmia, or severe hypokalemia. 24-hoururine collection may be inconvenient.Laboratory-specific poor performance of theradio-immunoassay for urinary aldosterone(aldosterone 18-oxo-glucuronide or acidlabilemetabolite) may blunt diagnosticaccuracy—a problem obviated by thecurrently available HPLC-tandem massspectrometry methodology (52). Aldosterone18-oxo-glucuronide is a renal metabolite, andits excretion may not rise in patients with renaldisease.Salineinfusion testPatients stay in the recumbentposition for at least 1 hour beforeand during the infusion of 2 litersof 0.9% saline i.v. over 4 hours,starting at 8:00–9.30 a.m. Bloodsamples for renin, aldosterone,cortisol, and plasma potassiumare drawn at time zero and after4 hours, with blood pressure andheart rate monitored throughoutthe test.Post-infusion plasmaaldosterone levels 10 ng/dLare a very probable signof PA. Values between 5and 10 ng/dL areindeterminate (57-60).This test should not be performed in patientswith severe uncontrolled hypertension, renalinsufficiency, cardiac insufficiency, cardiacarrhythmia, or severe hypokalemia.Fludrocortisonesuppression testCaptoprilchallenge testPatients receive 0.1 mg oralfludrocortisone every 6 hours for4 days, together with slow-releaseKCI supplements (every 6 hours atdoses sufficient to keep plasmaK+, measured 4 times a day, closeto 4.0 mmol/L), slow-release NaClsupplements (30 mmol three timesdaily with meals) and sufficientdietary salt to maintain a urinarysodium excretion rate of at least 3mmol/kg body weight. On day 4,plasma aldosterone and PRA aremeasured at 10 a.m. with thepatient in the seated posture, andplasma cortisol is measured at 7a.m. and 10 a.m.Patients receive 25–50 mg ofcaptopril orally after sitting orstanding for at least 1 hour. Bloodsamples are drawn formeasurement of PRA, plasmaaldosterone, and cortisol at timezero and at 1 or 2 hours afterchallenge, with the patientremaining seated during thisperiod.Upright plasmaaldosterone >6 ng/dL onday 4 at 10 a.m.confirms PA, providedPRA is 30%). Inpatients with PA itremains elevated andPRA remains suppressed.Differences may be seenbetween patients withAPA and those with IHA,in that some decrease ofaldosterone levels isoccasionally seen in IHA(23, 64–66).While some centers (10, 16) conduct this testin the outpatient setting (provided that patientsare able to attend frequently to monitor theirpotassium), in other centers several days ofhospitalization are customary.Most of the data available come from theBrisbane group (42, 43, 56, 61-63) who haveestablished, on the basis of a very large seriesof patients, a cut-off of a plasma aldosteroneconcentration of 6 ng/dL at 10 a.m. in anambulatory patient on day 4.Proponents of the FST argue that (1) it is themost sensitive for confirming PA, (2) it is a lessintrusive method of sodium loading than SITand therefore less likely to provoke non-renindependentalterations of aldosterone levels, (3)it allows for the potentially confounding effectsof potassium to be controlled, and for ACTH(via cortisol) to be monitored and detected,and (4) it is safe when performed byexperienced hands.<strong>The</strong>re are reports of a substantial number offalse negative or equivocal results (67, 68).CASE DETECTION, DIAGNOSIS, AND TREATMENT OF PA TIENTS WITH PRIMARY ALDOSTERONISM13