The Patient-Centered Medical Home - American College of ...
The Patient-Centered Medical Home - American College of ...
The Patient-Centered Medical Home - American College of ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>The</strong> <strong>Patient</strong>-<strong>Centered</strong> <strong>Medical</strong> <strong>Home</strong>:<br />
What, Why, Where, When…and How<br />
<strong>American</strong> <strong>College</strong> <strong>of</strong> Osteopathic Internists<br />
Annual Convention & Scientific Sessions<br />
October 2012<br />
Orlando, FL<br />
Michael S. Barr, MD, MBA, FACP<br />
Senior Vice President<br />
<strong>Medical</strong> Practice, Pr<strong>of</strong>essionalism & Quality<br />
mbarr@acponline.org<br />
202-261-4531
Goals for Presentation<br />
• Building the case for change (What & Why)<br />
• Does the PCMH fit into the future <strong>of</strong> health<br />
care? What about the “neighborhood”?<br />
(Where & When)<br />
• What are the tactics to achieve three-part aim<br />
(aka Triple Aim)? (How)<br />
• How can practices move towards the PCMH?<br />
(How)
↑Access ↑Quality ↓Cost<br />
Desired<br />
Future
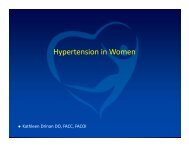
QUALITY: PATIENT-CENTERED, TIMELY CARE<br />
Waiting Time to See Doctor When Sick or Need <strong>Medical</strong> Attention,<br />
Among Sicker Adults, 2008<br />
Percent <strong>of</strong> adults who could get an appointment on the same or next day<br />
when sick or needed medical attention<br />
100<br />
75<br />
50<br />
25<br />
0<br />
80<br />
71<br />
62 61 59<br />
NETH NZ FRA UK GER AUS US CAN<br />
Sicker adults met at least one <strong>of</strong> the following criteria: health is fair or poor; serious illness in past two years; or was hospitalized or<br />
had major surgery in past two years. AUS=Australia; CAN=Canada; FRA=France; GER=Germany; NETH=Netherlands; NZ=New<br />
Zealand; UK=United Kingdom; US=United States.<br />
Data: 2008 Commonwealth Fund International Health Policy Survey.<br />
53<br />
43<br />
EXHIBIT 16<br />
Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011. 6<br />
36
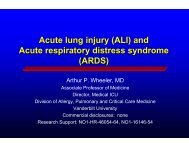
EQUITY: HEALTHY LIVES<br />
144 144<br />
Coronary Heart Disease and Diabetes-Related Mortality,<br />
by Race/Ethnicity and Education Level, 2006<br />
Age-adjusted mortality per 100,000 population<br />
250<br />
200<br />
150<br />
100<br />
50<br />
0<br />
Coronary heart disease mortality<br />
188<br />
114<br />
101<br />
Total White Black Hispanic Less than<br />
high<br />
school<br />
71<br />
High<br />
school<br />
graduate<br />
28<br />
At least<br />
some<br />
college<br />
Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011. 14<br />
250<br />
200<br />
150<br />
100<br />
50<br />
0<br />
74<br />
Diabetes-related mortality<br />
68<br />
130<br />
86<br />
61<br />
Total White Black Hispanic Less than<br />
high<br />
school<br />
Data: National Vital Statistics System—Mortality (retrieved from DATA2010 at http://wonder.cdc.gov/data2010).<br />
41<br />
High<br />
school<br />
graduate<br />
16<br />
At least<br />
some<br />
college
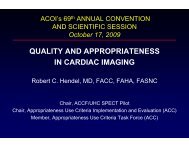
ACCESS: PARTICIPATION<br />
5<br />
6<br />
Access Problems Because <strong>of</strong> Costs, 2010<br />
Percent <strong>of</strong> adults who had any <strong>of</strong> three access problems* in past year because <strong>of</strong> costs<br />
50<br />
25<br />
0<br />
10 10 11<br />
13 14 15<br />
UK NETH SWE SWIZ NOR FRA NZ CAN AUS GER US<br />
* Did not get medical care because <strong>of</strong> cost <strong>of</strong> doctor’s visit; skipped medical test, treatment, or follow-up because <strong>of</strong> cost;<br />
or did not fill Rx or skipped doses because <strong>of</strong> cost.<br />
AUS=Australia; CAN=Canada; FRA=France; GER=Germany; NETH=Netherlands; NZ=New Zealand; NOR=Norway;<br />
SWE=Sweden; SWIZ=Switzerland; UK=United Kingdom; US=United States.<br />
Data: 2010 Commonwealth Fund International Health Policy Survey.<br />
22<br />
25<br />
33<br />
EXHIBIT 16<br />
Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011. 15
ACCESS: PARTICIPATION<br />
CA<br />
OR<br />
WA<br />
NV<br />
ID<br />
AZ<br />
UT<br />
AK<br />
MT ND<br />
WY<br />
NM<br />
CO<br />
Percent <strong>of</strong> Adults Ages 19–64 Uninsured by State<br />
1999–2000 2009–2010<br />
HI<br />
SD<br />
NE<br />
TX<br />
KS<br />
OK<br />
MN<br />
IA<br />
MO<br />
AR<br />
LA<br />
WI<br />
IL<br />
MS<br />
IN<br />
TN<br />
MI<br />
AL<br />
KY<br />
OH<br />
G<br />
A<br />
WV<br />
SC<br />
FL<br />
NC<br />
23% or more<br />
19%–22.9%<br />
14%–18.9%<br />
Less than 14%<br />
Data: U.S. Census Bureau, 2000–01 (revised) and 2010–11 Current Population Survey ASEC Supplement.<br />
PA<br />
VA<br />
VT NH<br />
NY<br />
ME<br />
MA<br />
RI<br />
CT<br />
NJ<br />
DE<br />
MD<br />
DC<br />
Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011. 16<br />
CA<br />
OR<br />
WA<br />
NV<br />
ID<br />
AZ<br />
UT<br />
AK<br />
MT ND<br />
WY<br />
NM<br />
CO<br />
HI<br />
SD<br />
NE<br />
TX<br />
KS<br />
OK<br />
MN<br />
IA<br />
MO<br />
AR<br />
LA<br />
WI<br />
IL<br />
MS<br />
IN<br />
TN<br />
MI<br />
AL<br />
KY<br />
OH<br />
G<br />
A<br />
WV<br />
SC<br />
FL<br />
PA<br />
VA<br />
NC<br />
VT NH<br />
NY<br />
ME<br />
MA<br />
RI<br />
CT<br />
NJ<br />
DE<br />
MD<br />
DC
ACCESS: PARTICIPATION<br />
CA<br />
OR<br />
Post-Reform: Projected Percent <strong>of</strong> Adults Ages 19–64 Uninsured by State<br />
WA<br />
NV<br />
ID<br />
AZ<br />
UT<br />
AK<br />
MT ND<br />
WY<br />
NM<br />
CO<br />
2009–2010 2019 (estimated)<br />
HI<br />
SD<br />
NE<br />
TX<br />
KS<br />
OK<br />
MN<br />
IA<br />
MO<br />
AR<br />
LA<br />
WI<br />
IL<br />
MS<br />
IN<br />
TN<br />
MI<br />
AL<br />
KY<br />
OH<br />
G<br />
A<br />
WV<br />
SC<br />
FL<br />
PA<br />
VA<br />
NC<br />
NY<br />
23% or more<br />
19%–22.9%<br />
14%–18.9%<br />
VT NH<br />
ME<br />
8%–13.9%<br />
Less than 8%<br />
Data: U.S. Census Bureau, 2010–11 Current Population Survey ASEC Supplement; estimates for 2019 by Jonathan Gruber<br />
and Ian Perry <strong>of</strong> MIT using the Gruber Microsimulation Model for <strong>The</strong> Commonwealth Fund.<br />
MA<br />
RI<br />
CT<br />
NJ<br />
DE<br />
MD<br />
DC<br />
Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011. 18<br />
CA<br />
OR<br />
WA<br />
NV<br />
ID<br />
AZ<br />
UT<br />
AK<br />
MT ND<br />
WY<br />
NM<br />
CO<br />
HI<br />
SD<br />
NE<br />
TX<br />
KS<br />
OK<br />
MN<br />
IA<br />
MO<br />
AR<br />
LA<br />
WI<br />
IL<br />
MS<br />
IN<br />
TN<br />
MI<br />
AL<br />
KY<br />
OH<br />
G<br />
A<br />
WV<br />
SC<br />
FL<br />
PA<br />
VA<br />
NC<br />
VT NH<br />
NY<br />
ME<br />
MA<br />
RI<br />
CT<br />
NJ<br />
DE<br />
MD<br />
DC
Florida Data 2011<br />
http://statesnapshots.ahrq.gov/snaps11/
Florida Data 2011
Florida Data 2011
Florida Data 2011
http://www.commonwealthfund.org/Maps-and-Data/State-Data-Center/State-Scorecard.aspx
http://whynotthebest.org
EFFICIENCY<br />
8,000<br />
7,000<br />
6,000<br />
5,000<br />
4,000<br />
3,000<br />
2,000<br />
1,000<br />
0<br />
1980<br />
International Comparison <strong>of</strong> Spending on Health, 1980–2009<br />
1982<br />
Average spending on health<br />
per capita ($US PPP*)<br />
1984<br />
United States<br />
Canada<br />
Germany<br />
France<br />
Australia<br />
United Kingdom<br />
1986<br />
1988<br />
* PPP=Purchasing Power Parity.<br />
Data: OECD Health Data 2011 (database), version 6/2011.<br />
1990<br />
1992<br />
1994<br />
1996<br />
1998<br />
2000<br />
Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.<br />
2002<br />
2004<br />
2006<br />
2008<br />
18<br />
16<br />
14<br />
12<br />
10<br />
8<br />
6<br />
4<br />
2<br />
0<br />
1980<br />
1982<br />
1984<br />
Total expenditures on health<br />
as percent <strong>of</strong> GDP<br />
1986<br />
1988<br />
1990<br />
1992<br />
1994<br />
1996<br />
1998<br />
United States<br />
France<br />
Germany<br />
Canada<br />
United Kingdom<br />
Australia<br />
2000<br />
2002<br />
2004<br />
2006<br />
2008<br />
25
Illness / Wellness Pyramid – 2010 CareFirst Experience<br />
80% <strong>of</strong><br />
admissions<br />
were for<br />
members in<br />
bands 1 and 2<br />
Advanced / Critical<br />
Illness<br />
BAND 1<br />
Multiple Chronic<br />
Illnesses<br />
BAND 2<br />
At Risk<br />
BAND 3<br />
Stable<br />
BAND 4<br />
Healthy<br />
BAND 5<br />
Source: CareFirst Health Care Analytics<br />
Percent <strong>of</strong><br />
Population<br />
Percent <strong>of</strong><br />
Cost<br />
PMPM<br />
Cost<br />
Illness<br />
Burden<br />
Range<br />
3% 37% $4,212 ≥ 5.0<br />
8% 22% $1,106 2.00-4.99<br />
12% 18% $577 1.00-1.99<br />
27% 17% $246 0.25-0.99<br />
50% 6% $57 0-0.24<br />
26
Reasons for Growth in Healthcare<br />
Spending (MedPac, March 2012)<br />
Technology: introduction/diffusion/expansion<br />
Price: lack <strong>of</strong> transparency; lack <strong>of</strong> competition<br />
Competition/Regulation: markets with provider<br />
consolidation/less competition leads to excess<br />
bargaining power<br />
Health Insurance: insulation to cost; lack <strong>of</strong><br />
knowledge about comparative effectiveness<br />
Income/Wealth/Demographics: increase in<br />
national income & wealth lead to more spending<br />
MedPac Report to Congress March 2012
Performance on indicators <strong>of</strong> health system efficiency remains<br />
especially low, with the U.S. scoring 53 out <strong>of</strong> 100 on measures<br />
that gauge the level <strong>of</strong> inappropriate, wasteful, or fragmented<br />
care; avoidable hospitalizations; variation in quality and costs;<br />
administrative costs; and use <strong>of</strong> information technology.<br />
Lowering insurance administrative costs to benchmark country<br />
rates could alone save up to $114 billion a year, or $55 billion if<br />
such costs were lowered to the level in countries with a mixed<br />
private–public insurance system, like the U.S. has.<br />
--Why Not the Best? Results from the National Scorecard on U.S.<br />
Health System Performance, 2011
“We are at a crossroads…<br />
…one road leads to<br />
hopelessness and<br />
despair;<br />
…the other leads to total<br />
extinction.<br />
Let us pray that we<br />
choose wisely.”<br />
-- Woody Allen
Strategy without tactics<br />
is the slowest route to victory.<br />
Sun Tzu – Chinese Military General<br />
Tactics without strategy<br />
is the noise before defeat.
Strategy<br />
Berwick, Nolan & Whittington; Health Affairs 2008<br />
Reduce Per<br />
Capita Costs<br />
Improve<br />
Health <strong>of</strong><br />
Populations<br />
Improve the<br />
Experience<br />
<strong>of</strong> Care<br />
Three Part Aim
National Quality Strategy<br />
March 2011<br />
1. Making care safer by reducing harm.<br />
2. Ensuring that each person and family are engaged.<br />
3. Promoting effective communication & coordination.<br />
4. Promoting the most effective prevention and<br />
treatment practices for the leading causes <strong>of</strong><br />
cardiovascular disease.<br />
5. Working with communities to promote wide use <strong>of</strong><br />
best practices to enable healthy living.<br />
6. Making quality care more affordable for individuals,<br />
families, employers, and government by developing<br />
and spreading new health care delivery models.<br />
http://www.healthcare.gov/law/resources/reports/quality03212011a.html
Tactics PCMH/<br />
PCMH-N<br />
Accountable<br />
Care Models<br />
Culture<br />
Improve<br />
Experience<br />
<strong>of</strong> Care<br />
Improve<br />
Health <strong>of</strong><br />
Populations<br />
Reduce Per<br />
Capita Costs<br />
Payment<br />
Health IT
PCMH Time Line<br />
1967<br />
-AAP Introduces<br />
“medical home”<br />
concept<br />
1992<br />
-AAP publishes<br />
first policy paper<br />
1980<br />
-Dr. Cal Sia, Peds gets<br />
Hawaii to adopt MH<br />
2002<br />
-AAP updates<br />
policy paper<br />
2006<br />
ACP AMH<br />
TRHCA 2006<br />
2004<br />
AAFP<br />
- FFM<br />
2009<br />
Advanced<br />
Primary Care<br />
2008<br />
NCQA-<br />
PCC-<br />
PCMH<br />
2007<br />
Joint<br />
Principles<br />
PCMH<br />
2011 CMS<br />
Comprehensive<br />
Primary Care<br />
2010<br />
Affordable<br />
Care Act
March 2007:<br />
AAFP, AAP, ACP, AOA Release<br />
Joint Principles <strong>of</strong> PCMH
<strong>The</strong> Joint Principles <strong>of</strong> the PCMH<br />
• Personal physician<br />
• Physician directed medical practice<br />
• Whole person orientation<br />
• Care is coordinated<br />
and/or integrated<br />
• Quality and safety<br />
• Enhanced access to care<br />
• Payment to support the PCMH<br />
http://www.acponline.org/running_practice/p<br />
cmh/demonstrations/jointprinc_05_17.pdf<br />
Team-based care:<br />
NP/PA<br />
RN/LPN<br />
<strong>Medical</strong> Assistant<br />
Office Staff<br />
Care Coordinator<br />
Nutritionist/Educator<br />
Pharmacist<br />
Behavioral Health<br />
Case Manager<br />
Social Worker<br />
Community resources<br />
DM companies<br />
Others…
Collaboration Among Societies<br />
March 2009: Guidelines for PCMH Demonstration<br />
Projects<br />
November 2010: Joint Principles for Accountable<br />
Care Organizations<br />
December 2010: Joint Principles for the <strong>Medical</strong><br />
Education <strong>of</strong> Physicians in Preparation for Practicing<br />
in the PCMH<br />
February 2011: Guidelines for PCMH Recognition<br />
and Accreditation Programs<br />
Working On… Joint Guidelines for Integrating<br />
Mental Health/Behavioral Health into Primary Care
2007<br />
<strong>Patient</strong>-<strong>Centered</strong> Primary Care<br />
Collaborative Formed
Six<br />
Collaborative<br />
Centers:<br />
www.pcpcc.net<br />
Overview <strong>of</strong> PCPCC<br />
Activities<br />
• Center for Multi-Stakeholder<br />
Demonstrations<br />
• Center to Promote Public Payer<br />
Implementation<br />
• Center for Employer Engagement<br />
• Center for eHealth<br />
• Center for Consumer Engagement<br />
• Center for Accountable Care
Current Demos<br />
(Per PCPCC Website)<br />
http://pcpcc.net/pcpcc-pilot-projects (as <strong>of</strong> 7/31/12)
Recognition & Accreditation Programs<br />
January 2008: NCQA Releases PPC-PCMH<br />
Recognition Program<br />
2009: Accreditation Association for Ambulatory<br />
Health Care – <strong>Medical</strong> <strong>Home</strong> Program<br />
September 2010: Joint Commission announces<br />
Primary Care <strong>Home</strong> Initiative<br />
December 2010: URAC Releases <strong>Patient</strong>-<strong>Centered</strong><br />
Health Care <strong>Home</strong> Tool Kit<br />
January 2011: NCQA Releases PCMH 2011<br />
May 2011: Joint Commission releases PCH Initiative
http://www.ncqa.org/LinkClick.aspx?fileticket=MYvjUN6K3Ik%3d&tabid=<br />
631&mid=2435&forcedownload=true
NCQA Standard Must Pass Element Meaningful Use Correlate<br />
Identify & Manage<br />
Populations<br />
Use Data for Population<br />
Management<br />
-Use clinical decision<br />
support<br />
-Generate lists <strong>of</strong> patients<br />
Plan & Manage Care Care Management -Medication reconciliation<br />
-Generate reminders<br />
Provide Self-Care Support &<br />
Community Resources<br />
Track & Coordinate Care Referral Tracking & Followup<br />
Measure & Improve<br />
Performances<br />
NCQA vs. Meaningful Use<br />
Support Self-Care Process -View/download/transmit<br />
-Send secure messages<br />
Implement Continuous<br />
Quality Improvement<br />
-Provide summary <strong>of</strong> care<br />
for transitions<br />
-Record team members<br />
-Incorporate imaging<br />
results<br />
-Report on Clinical Quality<br />
Measures (CQMs)
Comprehensive Primary Care Initiative<br />
• CPCi is a multi-payer initiative fostering<br />
collaboration between public and private health<br />
care payers to strengthen primary care.<br />
• Medicare will work with commercial and State<br />
health insurance plans and <strong>of</strong>fer bonus payments<br />
to primary care doctors who better coordinate<br />
care for their patients.<br />
• Primary care practices that choose to participate<br />
in this initiative will be given resources to better<br />
coordinate primary care for their Medicare<br />
patients.
Seven Regions Selected<br />
• Arkansas: Statewide (4 Payers)<br />
• Colorado: Statewide (9 Payers)<br />
• New Jersey: Statewide (5 Payers)<br />
• New York: Capital District-Hudson Valley Region<br />
(6 Payers)<br />
• Ohio and Kentucky: Cincinnati-Dayton Region (10<br />
Payers)<br />
• Oklahoma: Greater Tulsa Region (3 Payers)<br />
• Oregon: Statewide (7 Payers) Read More
CPCi Practice Milestones<br />
1. Create an annual budget<br />
2. Provide care management for high-risk patients<br />
3. Provide 24/7 access to the medical record<br />
4. Assess & improve patient experience <strong>of</strong> care<br />
5. Use data to guide improvement in care at the provider/care team<br />
level<br />
6. Demonstrate active engagement and care coordination across the<br />
medical neighborhood<br />
7. Improve patient shared decision-making capacity<br />
8. Participate in market-based learning community (This would be<br />
unique to the CPCi and organized by them)<br />
9. Attest to the Stage 1 Meaningful Use EHR Incentive Program<br />
requirements
Payment Model for CPCi<br />
• <strong>The</strong> payment model includes a monthly care<br />
management fee paid to the selected primary care<br />
practices on behalf <strong>of</strong> their fee-for-service Medicare<br />
beneficiaries<br />
• In years 2-4 <strong>of</strong> the initiative, the potential to share in<br />
any savings to the Medicare program.<br />
• Practices will also receive compensation from other<br />
payers participating in the initiative, including private<br />
insurance companies and other health plans, which will<br />
allow them to integrate multi-payer funding streams to<br />
strengthen their capacity to implement practice-wide<br />
quality improvement.
100<br />
75<br />
50<br />
25<br />
0<br />
64<br />
Widespread Support for <strong>Medical</strong> <strong>Home</strong>s<br />
Percent reporting importance <strong>of</strong> having one place/doctor<br />
responsible for primary care and coordinating care<br />
93 93 93 92 93 94 94<br />
21<br />
89<br />
29<br />
29 26 24<br />
30<br />
41<br />
30<br />
72<br />
52<br />
64 67 69<br />
Total NE NC South West Dem Rep Ind<br />
NE=Northeast; NC=North–Central; Dem=Democrat; Rep=Republican; Ind=Independent.<br />
Source: Commonwealth Fund Survey <strong>of</strong> Public Views <strong>of</strong> the U.S. Health Care System, 2011.<br />
Important<br />
Very important<br />
U.S. region Political affiliation<br />
59<br />
63<br />
THE<br />
COMMONWEALTH<br />
FUND
Project Hosp ER Visits Quality Pt<br />
Experience<br />
Group Health<br />
Cooperative (WA)<br />
-6% (all)<br />
-13% (ACSC)<br />
Geisinger (PA) -18% (all)<br />
-36% (re-ad)<br />
-29% Improved Improved in<br />
5 / 7 scales<br />
NDP (national) NA NA Improved<br />
Community Care <strong>of</strong><br />
North Carolina*<br />
Colorado <strong>Medical</strong><br />
<strong>Home</strong>s for Children*<br />
Intermountain (UT)* -5% (all)<br />
-19% (c.dz)<br />
Total $ per<br />
patient/yr<br />
-$120<br />
NA NA NA -7% (+5% to -18%)<br />
-40% NA Improved<br />
asthma, DM<br />
Slightly<br />
worse (NS)<br />
NA -$516<br />
(Not Stat Significant)<br />
*Practice Rev<br />
+2% to 12%<br />
-18% -16% NA NA -$169 (all)<br />
-$530 (c. dz)<br />
0% (all)<br />
-7% (c.dz)<br />
NA NA -$640<br />
North Dakota BCBS* -6% -24% NA NA -$530<br />
Vermont Blueprint* -11% -12% NA NA -$215<br />
Slide courtesy <strong>of</strong> Dr. Asaf Bitton. See also:<br />
Bitton A, Martin C, Landon B. “A National Survey <strong>of</strong> PCMH Demonstrations. JGIM. June 2010.<br />
*Not peer reviewed ACS= ambulatory care sensitive conditions c dz = chronic disease<br />
NS = not statistically significant re-ad = readmissions
Horizon Blue Cross Blue Shield (NJ)<br />
• Quality Measures<br />
• 8% higher rate in improved diabetes control (HbA1c)<br />
• 6% higher rate in breast cancer screening<br />
• 6% higher rate in cervical cancer screening<br />
• Cost and Utilization Indicators<br />
• 10% lower cost <strong>of</strong> care (per member per month)<br />
• 26% lower rate in emergency room visits<br />
• 25% lower rate in hospital readmissions<br />
• 21% lower rate in hospital inpatient admissions<br />
• 5% higher rate in the use <strong>of</strong> generic prescriptions<br />
http://www.horizon-bcbsnj.com/news_room/news_releases/article.html?id=33878
Group Health Cooperative<br />
• $10 PMPM reduction in total costs; total PMPM cost $488<br />
for PCMH patients vs. $498 for control patients (p=.076).<br />
• 16% reduction in hospital admissions (p
HealthPartners <strong>Medical</strong> Group<br />
BestCare PCMH Model (MN)<br />
• 39% decrease in emergency department visits<br />
and 24% decrease in hospital admissions per<br />
enrollee between 2004 and 2009.<br />
• Overall costs for enrollees in HealthPartners<br />
<strong>Medical</strong> Group decreased from being equal to<br />
the state average in 2004 to 92% <strong>of</strong> the state<br />
average in 2008, in a state with costs already<br />
well below the national average.
Some Additional Findings To Date…<br />
• Medicaid: Improved access to care, reduced<br />
PMPM/PMPY costs, decreased ER and<br />
inpatient utilization, greater use <strong>of</strong> evidencebased<br />
primary care<br />
• Access to care through visits outside <strong>of</strong> regular<br />
hours and same day access reduced<br />
emergency department use<br />
• Improved patient and clinician satisfaction<br />
Takach, M. 2011. Reinventing Medicaid: State Innovations to Qualify And Pay For<br />
<strong>Patient</strong>-<strong>Centered</strong> <strong>Medical</strong> <strong>Home</strong>s Show Promising Results. Health Affairs. 30(7):1325-1334.<br />
Bodenheimer, T., H. Pham. 2010. Primary Care: Current Problems and Proposed Solutions. Health Affairs. 29(5):799–805.<br />
Reid, R., P. Fishman, O. Yu, T. Ross, J.T. Tufano. 2009. <strong>Patient</strong>-<strong>Centered</strong> <strong>Medical</strong> <strong>Home</strong> Demonstration: A prospective,<br />
quasi-experimental, before and after evaluation. <strong>American</strong> Journal <strong>of</strong> Managed Care. 15(9), e71-e87.
www.pcmh.ahrq.gov
Infrastructure<br />
(Integrated<br />
Network/CI ACO)<br />
Community<br />
Neighbor<br />
PCMH
• First contact<br />
• Comprehensive<br />
• Coordinating<br />
• Integrated with<br />
behavioral<br />
health/mental heath<br />
• Wellness &<br />
Preventative care<br />
PCMH
Care Coordination<br />
“Effective care coordination…requires not<br />
only full access to all the necessary clinical<br />
information…but also a willingness by all the<br />
physicians [and their teams] involved…to<br />
participate in collaborative decision making.”<br />
-Elliott Fisher, NEJM 2008
Gaps in Care Coordination<br />
• Primary care and specialists:<br />
– No information sent to Peds specialist 49% <strong>of</strong> time; no feedback to<br />
primary care 55% <strong>of</strong> time<br />
• Emergency Department<br />
– 30% <strong>of</strong> adults indicated regular physician not informed about visit<br />
• Hospital<br />
– 33% <strong>of</strong> adults with chronic condition did not have follow-up plans<br />
post hospital discharge<br />
– 3% <strong>of</strong> primary care physicians discussed discharge plans with hospital<br />
physicians<br />
– 66% <strong>of</strong> time primary care follow-up post discharge was done without<br />
a hospital discharge summary<br />
Bodenheimer, T: Coordinating Care – A Perilous Journey through the Health Care System. NEJM 2008;358:10
Nearly Half <strong>of</strong> U.S. Adults Report Failures to Coordinate Care<br />
Percent U.S. adults reported in past two years:<br />
Your specialist did not receive basic<br />
medical information from your<br />
primary care doctor<br />
Your primary care doctor did not<br />
receive a report back from a specialist<br />
Test results/medical records were not<br />
available at the time <strong>of</strong> appointment<br />
Doctors failed to provide important<br />
medical information to other doctors<br />
or nurses you think should have it<br />
No one contacted you about<br />
test results, or you had to call<br />
repeatedly to get results<br />
Any <strong>of</strong> the above<br />
13<br />
15<br />
19<br />
21<br />
25<br />
47<br />
0 20 40 60<br />
Source: S. K. H. How, A. Shih, J. Lau, and C. Schoen, Public Views on U.S. Health System Organization:<br />
A Call for New Directions (New York: <strong>The</strong> Commonwealth Fund, Aug. 2008).<br />
THE<br />
COMMONWEALTH<br />
FUND
Fragmentation<br />
• Typical primary care physician relates to<br />
229 other physicians in 117 practices for<br />
Medicare FFS beneficiaries<br />
Pham, H et al: Ann Intern Med February 17, 2009 150:236-242
Teams<br />
• Wikipedia definition: A team comprises a group <strong>of</strong><br />
people linked in a common purpose. Teams are<br />
especially appropriate for conducting tasks that<br />
are high in complexity and have many<br />
interdependent subtasks.<br />
• Interdependent team:<br />
– no significant task can be accomplished without<br />
the help <strong>of</strong> any <strong>of</strong> the members;<br />
– within that team members typically specialize in<br />
different tasks, and<br />
– the success <strong>of</strong> every individual is inextricably bound to the success<br />
<strong>of</strong> the whole team. No football player, no matter how talented,<br />
has ever won a game by playing alone.<br />
Adapted from: http://en.wikipedia.org/wiki/Team
<strong>The</strong> <strong>Patient</strong>-<strong>Centered</strong> <strong>Medical</strong> <strong>Home</strong><br />
Neighbor
Typology <strong>of</strong> Clinical Roles -<br />
Specialists<br />
• Cognitive consultation<br />
– Provide diagnostic or therapeutic advice<br />
• Procedural consultation<br />
– Perform a technical procedure to aid diagnosis, cure a<br />
condition, identify/prevent new conditions, palliate<br />
• Co-manager with shared care<br />
– Long-term management with primary care physician<br />
• Co-manager with principal care<br />
– Assume total responsibility for long-term management<br />
• Primary care physician<br />
– Provides a medical home for a group <strong>of</strong> patients<br />
Forrest, Christopher: Arch Int Med 2009
PCMH Neighbor Attributes<br />
• Provide effective bidirectional communication with a<br />
focus on care coordination and information sharing<br />
with the PCMH<br />
• Engage in timely and appropriate<br />
referrals/consultations<br />
• Support patient-centered care co-management<br />
• Establish care coordination agreements that:<br />
– Define roles/responsibilities/expectations<br />
– Provide specific parameters for secondary referrals,<br />
admissions, emergencies<br />
• Align incentives<br />
• Explore a PCMH-N recognition process
Good Neighbors?
%<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
Percentage <strong>of</strong> Services Obtained at Retail Clinics<br />
48 47<br />
New illness<br />
or symptom<br />
Prescription<br />
renewal<br />
23<br />
Source: Center for Studying Health System Change 2007 Health Tracking Household Survey, April 2007–January 2008<br />
Publication: H. T. Tu and G. R. Cohen, Checking Up on Retail-Based Health Clinics: Is the Boom Ending?,<br />
<strong>The</strong> Commonwealth Fund, December 2008.<br />
18<br />
Vaccination Care for<br />
ongoing<br />
chronic<br />
condition<br />
Notes: Categories are not mutually exclusive; respondents were able to select multiple categories.<br />
14<br />
Physical<br />
exam for school,<br />
camp, or<br />
employment<br />
5<br />
Other<br />
THE<br />
COMMONWEALTH<br />
FUND
%<br />
80<br />
60<br />
40<br />
20<br />
0<br />
Reasons for Choosing Retail Clinics<br />
Over Other Health Providers<br />
64<br />
Clinic hours were<br />
more convenient<br />
than another<br />
source <strong>of</strong> care<br />
62<br />
Location was<br />
more convenient<br />
than another<br />
source <strong>of</strong> care<br />
Source: Center for Studying Health System Change 2007 Health Tracking Household Survey, April 2007–January 2008<br />
Publication: H. T. Tu and G. R. Cohen, Checking Up on Retail-Based Health Clinics: Is the Boom Ending?,<br />
<strong>The</strong> Commonwealth Fund, December 2008.<br />
53<br />
Did not have<br />
to make an<br />
appointment<br />
for a retail clinic<br />
Notes: Categories are not mutually exclusive; respondents were able to select multiple categories.<br />
48<br />
Cost was<br />
lower than<br />
another source <strong>of</strong><br />
care<br />
34<br />
Did not have a<br />
usual source<br />
<strong>of</strong> care<br />
THE<br />
COMMONWEALTH<br />
FUND
Community
<strong>Patient</strong>-<strong>Centered</strong>, Core <strong>of</strong> Team-Based Physician-Guided Care<br />
Care<br />
Practice Family<br />
Team<br />
Physician <strong>Patient</strong><br />
Adapted from:<br />
Defining Primary Care: An Interim Report, Institute <strong>of</strong> Medicine 1994
http://permanent.access.gpo.gov/gpo16811/acsbr10-17.pdf
http://labs.slate.com/articles/food-deserts-in-america/
http://iom.edu/~/media/Files/Activity%20Files/PublicHealth/<br />
PrimCarePublicHealth/PCPH-Report-Release-Presentation-03-28-12.pdf
-Atul Gawande; NCQA Quality Awards 2012
Infrastructure<br />
(Health System,<br />
Integrated<br />
Network/CI/ACM)
Integrated Delivery System<br />
Practice<br />
Team<br />
Physician<br />
Practice<br />
Team<br />
Physician<br />
<strong>Patient</strong><br />
Physician<br />
Practice<br />
Team<br />
Accountable Care Model<br />
Practice<br />
Physician Team<br />
Clinical Integration Independent<br />
Practice Assoc.
Building the Model
Pyramid to Peak Performance<br />
Service<br />
Workflow/Logistics<br />
Organization/Infrastructure<br />
Personnel/Training/Competency<br />
Technology
<strong>The</strong> first rule <strong>of</strong> any technology used in a business<br />
is that automation applied to an efficient operation<br />
will magnify the efficiency. <strong>The</strong> second is that<br />
automation applied to an inefficient operation will<br />
magnify the inefficiency.<br />
Bill Gates<br />
http://www.brainyquote.com/<br />
640K ought to be enough for<br />
anybody.<br />
Bill Gates
Service<br />
Technology<br />
Workflow/Logistics<br />
Organization/Infrastructure<br />
Personnel/Training/Competency
Personnel/Training/Competency<br />
• Right number, skill sets, competencies<br />
– Clinical & administrative<br />
– Cross-trained<br />
• Assessment <strong>of</strong> readiness for change<br />
• Recognize potential “threats” to staff<br />
• Assess satisfaction with job activities<br />
• Remove barriers to working at level <strong>of</strong> training
Organization/Infrastructure<br />
• Identify any cultural issues that impede teamwork<br />
and collaboration<br />
• Review hierarchy and org chart<br />
• Introduce team-huddles<br />
• Improve communication<br />
• Review facility layout and lines <strong>of</strong> sight
Workflow/Logistics<br />
• Evaluate work flow <strong>of</strong> common processes as well as<br />
uncommon yet critical pathways<br />
• Eliminate extraneous steps, layered “solutions” and<br />
misapplied technology<br />
• Consider the functionality <strong>of</strong> well-implemented<br />
technology to assist clinicians, staff, patients &<br />
families
Technology<br />
• Right product(s)<br />
• Right prep & training<br />
• Right implementation<br />
• Right support<br />
• Right optimization<br />
• Right maintenance
Service<br />
• Organized, pro-active, responsive, accountable and<br />
accessible<br />
• Culturally competent<br />
• Addresses health literacy/numeracy<br />
• Focused on quality & safety<br />
• Addresses needs <strong>of</strong> individuals and the population<br />
• Incorporates patient preferences, stated<br />
needs/desires in formulating care strategies and<br />
follow-up<br />
• Uses health information technology to facilitate care
Teambased<br />
practice<br />
Improves<br />
Care<br />
Chart<br />
Organization
<strong>Patient</strong>/Family<br />
Communication<br />
Medication<br />
Management<br />
Chart<br />
Lab/Test<br />
Tracking<br />
Referral Tracking
Labs<br />
Radiology<br />
Referral<br />
Requests<br />
Suppliers<br />
Hospitals<br />
Rx<br />
Clinicians<br />
<strong>Patient</strong>s<br />
Family<br />
Clinicians<br />
Families<br />
/Pts<br />
<strong>Home</strong><br />
Health<br />
Hospitals<br />
Rx<br />
Vendors<br />
&<br />
Suppliers<br />
Payers/<br />
Prior<br />
Auths
Service<br />
Technology<br />
Workflow/Logistics<br />
Organization/Infrastructure<br />
Personnel/Training/Competency
Service<br />
Technology<br />
Workflow/Logistics<br />
Organization/Infrastructure<br />
Personnel/Training/Competency<br />
Service<br />
Technology<br />
Workflow/Logistics<br />
Organization/Infrastructure<br />
Personnel/Training/Competency<br />
Service<br />
Technology<br />
Workflow/Logistics<br />
Organization/Infrastructure<br />
Personnel/Training/Competency<br />
Service<br />
Technology<br />
Workflow/Logistics<br />
Organization/Infrastructure<br />
Personnel/Training/Competency
8 Key Change Concepts<br />
• Engaged leadership;<br />
• Quality improvement strategy;<br />
• Empanelment (linking each patient with a<br />
responsible primary care provider);<br />
• Continuous and team-based healing<br />
relationships;<br />
• Organized, evidence-based care;<br />
• <strong>Patient</strong>-centered interactions;<br />
• Enhanced access; and<br />
• Care coordination.<br />
Wagner , Ed et al.<br />
Guiding Transformation: How <strong>Medical</strong> Practices<br />
Can Become <strong>Patient</strong>-<strong>Centered</strong> <strong>Medical</strong> <strong>Home</strong>s<br />
www.commonwealthfund.org; February 2012
National Academy <strong>of</strong> State Health Policy<br />
Consortia to Advance <strong>Medical</strong> <strong>Home</strong>s for Medicaid & CHIP Participants<br />
1. Strategically engage partners.<br />
2. Set performance expectations and implement a process to<br />
identify practices that meet expectations.<br />
3. Compensate & motivate practices through enhanced payment.<br />
4. Help practices meet expectations & improve performance.<br />
5. Evaluate program performance.<br />
Commonwealth Fund Building <strong>Medical</strong> <strong>Home</strong>s: Lessons from Eight States with<br />
Emerging Programs (Dec. 2011)
National Academy <strong>of</strong> State Health Policy<br />
Common <strong>The</strong>mes<br />
1. Tailor PCMH definition to reflect state needs, priorities & circumstances.<br />
2. Use payment policy to foster collaboration among primary care and specialty<br />
care.<br />
3. Use payment policy to reward more capable and better-performing medical<br />
homes.<br />
4. Help practices improve performance.<br />
5. Provide support for care coordination.<br />
6. Ease the evaluation burden for medical home providers.<br />
7. Base medical home qualification criteria on models established by a national<br />
organization.<br />
8. Balance the desire for improved performance with the cost <strong>of</strong> the<br />
improvements.<br />
9. Address antitrust concerns that arise when multiple payers create a medical<br />
home program.
ACP <strong>Medical</strong> <strong>Home</strong> Builder®<br />
www.medicalhomebuilder.org
Three Categories <strong>of</strong> Modules<br />
(Current as <strong>of</strong> 4/26/12)<br />
• Quick Start: NCQA*<br />
• Organize Your Practice<br />
• Work as a Team<br />
• Communicate with <strong>Patient</strong>s<br />
• Enhance <strong>Patient</strong> Access<br />
• Deliver <strong>Patient</strong>-<strong>Centered</strong> Care<br />
• Coordinate Care<br />
• Facilitate Transitions I & II*<br />
• Use <strong>of</strong> Technology I & II<br />
*Modules (11) added since launch in August 2011<br />
White = PCMH: Green = Clinical; Yellow = Practice Mgt<br />
• Improve Quality<br />
• Manage Populations<br />
• Manage <strong>Patient</strong>s’ Medications*<br />
• Engage <strong>Patient</strong>s*<br />
• Manage Diabetes Mellitus*<br />
• Immunize Adults*<br />
• Depression Screening & Care*<br />
• Manage Chronic Pain*<br />
• Practice Basics*<br />
• Managing People*<br />
• Bloodborne Pathogens/OSHA*<br />
• Manage <strong>Medical</strong> Waste*
Planned Enhancements<br />
Improving Clinical Care<br />
• Arthritis<br />
• Cardiovascular Risk Factors<br />
• Choosing Wisely (High<br />
Value, Cost-Conscious<br />
Care)<br />
• Additional Clinically-<br />
Related modules to follow<br />
Green = Clinical; Yellow = Practice Mgt<br />
Managing Your Practice (For<br />
example only; actual topics<br />
to be determined)<br />
• Financial Management<br />
• Coding<br />
• Billing/Collections<br />
• Working on aligning MHB<br />
modules with<br />
Maintenance <strong>of</strong><br />
Certification requirements<br />
• New data download<br />
capability for users
New Module Landing Page Design
Module Organization
Practice Biopsy Questions
Biopsy Report<br />
• Highlights<br />
critical issues<br />
• Percentage<br />
score<br />
• Guidance<br />
based on<br />
responses<br />
• Links to key<br />
resources &<br />
Resource<br />
Library
Module Resource Library
Virtual Bookshelf / Resource Library
Practice-to-Practice Connections
Reporting Features<br />
• Premium license<br />
permits data<br />
aggregation at level<br />
<strong>of</strong> practice location,<br />
practice group, or<br />
groups <strong>of</strong> practices<br />
• Drill down capability<br />
to individual<br />
• Provides average<br />
score from entire<br />
MHB community for<br />
benchmarking<br />
• Indicates # <strong>of</strong><br />
individuals who have<br />
completed particular<br />
module in<br />
community<br />
• Additional reports on<br />
a customized basis
Current Groups Using MHB<br />
• CareFirst BlueCross BlueShield (MD/VA/DC)<br />
• Independence Blue Cross (PA)<br />
• Connecticut State <strong>Medical</strong> Society IPA (CT)<br />
• Eastern Connecticut PHO (CT)<br />
• Mercy <strong>Medical</strong> Associates (Maine)<br />
• St. Francis Health System (OK)<br />
• Temple University General IM (PA)<br />
• University Medicine (RI)<br />
• West Penn Allegheny Health System (PA)<br />
• Monroe Plan for <strong>Medical</strong> Care (NY)<br />
• University <strong>of</strong> Texas Health Science Center (TX)<br />
• Southern Illinois University (IL)<br />
• Louisiana Health Care Quality Forum (LA)<br />
Groups (exclusive <strong>of</strong> 2,000<br />
practices from CareFirst<br />
BCBS) currently represent:<br />
• >1000 clinicians<br />
• >300 locations<br />
CareFirst:<br />
• 2,000 practice licenses<br />
• Approx. 6,000 clinicians
Map <strong>of</strong> Current Users (7/31/12)
My patients are those who<br />
come to see me<br />
Chief complaint determines<br />
care<br />
Care is determined by today’s<br />
problem and time available<br />
Care varies by time, memory,<br />
and skill <strong>of</strong> doctor<br />
<strong>Patient</strong>s coordinate their own<br />
care<br />
Personal confidence based on<br />
training<br />
Acute care is delivered by next<br />
available appt and walk-in<br />
<strong>Patient</strong> relates interval history<br />
Operations are doctorcentered<br />
Adapted from Malcolm Cox and Richard Stark<br />
U.S. Department <strong>of</strong> Veterans Affairs<br />
My patients are those who are<br />
part <strong>of</strong> our medical home<br />
Systematic assessment <strong>of</strong><br />
patient needs<br />
Care is determined by<br />
proactive plan<br />
Standardized care based on<br />
EBG and CDSS<br />
Prepared team <strong>of</strong> pr<strong>of</strong>essionals<br />
coordinates care with patient<br />
Outcomes are assessed;<br />
continuous improvement<br />
Acute care is delivered by<br />
advanced access/non-visit care<br />
Tracking <strong>of</strong> tests/procedures &<br />
consultations/hospitalizations<br />
Multi-disciplinary team works<br />
at “top <strong>of</strong> license” for patients
What Does a PCMH + Neighbor Look Like<br />
From a <strong>Patient</strong>’s Perspective?<br />
Access/Communication<br />
Between Face-to-face Encounters visit<br />
•Contact via traditional/health IT-enabled<br />
•Planned/prepared<br />
•Online vs. phone<br />
processes<br />
•Coordinated •Open access activities/co-management<br />
vs. delayed visits<br />
•Collaboration with other health care providers<br />
•Team-based •Email effort vs. with snail staff mail & colleagues<br />
•Transparent information sharing<br />
•Use •PHR <strong>of</strong> customized and practice educational portal 24/7/365 materials<br />
•Interactive PHR with lab/test results, etc.<br />
•Clinicians •Information knowledgeable prescription<br />
about specialty care<br />
•Remote monitoring
Defining Success<br />
“Success is falling nine times<br />
and getting up ten.”<br />
-- Jon Bon Jovi
Defining Success<br />
Indicator If FLORIDA improved its performance to the level <strong>of</strong> the bestperforming<br />
state for this indicator, then:<br />
Insured Adults 2,048,106 more adults (18-64) would be covered<br />
Insured Children 601,618 more children (0-17) would be covered<br />
Adult Preventive Care 652,393 more adults (50+) would receive recommended care<br />
Diabetes Care 265,081 more adults (18+) would receive eye exam, foot exam, HbA1c<br />
Childhood Vaccination 35,898 more children (19-35 months) would be UTD<br />
Adults with USOC* 1,750,697 (18+) would have usual source <strong>of</strong> care<br />
Children with MH** 502,788 (0-17) would have medical home<br />
Preventable Admissions 37,917 fewer hospitalizations for ASC*** among Medicare beneficiaries<br />
$145,566,318 dollars would be saved<br />
Hospital Re-admits 7,660 fewer re-admits; $59,254,092 would be saved<br />
Amenable Mortality 3,307 fewer premature deaths (before age 75)<br />
http://www.commonwealthfund.org/Maps-and-Data/State-Data-Center/State-Scorecard/DataByState/State.aspx?state=FL<br />
*USOC = usual source <strong>of</strong> care; **MH = medical home;<br />
***ASC=ambulatory care sensitive conditions
"I put a dollar in a<br />
change machine.<br />
Nothing changed."<br />
— George Carlin
“You must be the change you<br />
want to see in the world.”<br />
-Mahatma Gandhi
Michael S. Barr, MD, MBA, FACP<br />
Senior Vice President<br />
<strong>Medical</strong> Practice, Pr<strong>of</strong>essionalism & Quality<br />
mbarr@acponline.org<br />
202-261-4531