

Gourley TCCC and CLS Army May 2010 - Health.mil
Gourley TCCC and CLS Army May 2010 - Health.mil
Gourley TCCC and CLS Army May 2010 - Health.mil

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
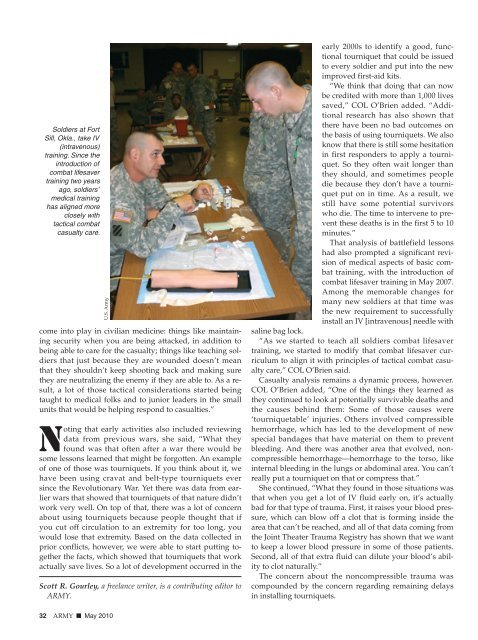
Soldiers at FortSill, Okla., take IV(intravenous)training. Since theintroduction ofcombat lifesavertraining two yearsago, soldiers’medical traininghas aligned moreclosely withtactical combatcasualty care.U.S. <strong>Army</strong>come into play in civilian medicine: things like maintainingsecurity when you are being attacked, in addition tobeing able to care for the casualty; things like teaching soldiersthat just because they are wounded doesn’t meanthat they shouldn’t keep shooting back <strong>and</strong> making surethey are neutralizing the enemy if they are able to. As a result,a lot of those tactical considerations started beingtaught to medical folks <strong>and</strong> to junior leaders in the smallunits that would be helping respond to casualties.”Noting that early activities also included reviewingdata from previous wars, she said, “What theyfound was that often after a war there would besome lessons learned that might be forgotten. An exampleof one of those was tourniquets. If you think about it, wehave been using cravat <strong>and</strong> belt-type tourniquets eversince the Revolutionary War. Yet there was data from earlierwars that showed that tourniquets of that nature didn’twork very well. On top of that, there was a lot of concernabout using tourniquets because people thought that ifyou cut off circulation to an extremity for too long, youwould lose that extremity. Based on the data collected inprior conflicts, however, we were able to start putting togetherthe facts, which showed that tourniquets that workactually save lives. So a lot of development occurred in theScott R. <strong>Gourley</strong>, a freelance writer, is a contributing editor toARMY.early 2000s to identify a good, functionaltourniquet that could be issuedto every soldier <strong>and</strong> put into the newimproved first-aid kits.“We think that doing that can nowbe credited with more than 1,000 livessaved,” COL O’Brien added. “Additionalresearch has also shown thatthere have been no bad outcomes onthe basis of using tourniquets. We alsoknow that there is still some hesitationin first responders to apply a tourniquet.So they often wait longer thanthey should, <strong>and</strong> sometimes peopledie because they don’t have a tourniquetput on in time. As a result, westill have some potential survivorswho die. The time to intervene to preventthese deaths is in the first 5 to 10minutes.”That analysis of battlefield lessonshad also prompted a significant revisionof medical aspects of basic combattraining, with the introduction ofcombat lifesaver training in <strong>May</strong> 2007.Among the memorable changes formany new soldiers at that time wasthe new requirement to successfullyinstall an IV [intravenous] needle withsaline bag lock.“As we started to teach all soldiers combat lifesavertraining, we started to modify that combat lifesaver curriculumto align it with principles of tactical combat casualtycare,” COL O’Brien said.Casualty analysis remains a dynamic process, however.COL O’Brien added, “One of the things they learned asthey continued to look at potentially survivable deaths <strong>and</strong>the causes behind them: Some of those causes were‘tourniquetable’ injuries. Others involved compressiblehemorrhage, which has led to the development of newspecial b<strong>and</strong>ages that have material on them to preventbleeding. And there was another area that evolved, noncompressiblehemorrhage—hemorrhage to the torso, likeinternal bleeding in the lungs or abdominal area. You can’treally put a tourniquet on that or compress that.”She continued, “What they found in those situations wasthat when you get a lot of IV fluid early on, it’s actuallybad for that type of trauma. First, it raises your blood pressure,which can blow off a clot that is forming inside thearea that can’t be reached, <strong>and</strong> all of that data coming fromthe Joint Theater Trauma Registry has shown that we wantto keep a lower blood pressure in some of those patients.Second, all of that extra fluid can dilute your blood’s abilityto clot naturally.”The concern about the noncompressible trauma wascompounded by the concern regarding remaining delaysin installing tourniquets.32 ARMY ■ <strong>May</strong> <strong>2010</strong>
![Eye Injury Prevention Month Fact Sheet [PDF 3.64 MB]](https://img.yumpu.com/28543556/1/190x245/eye-injury-prevention-month-fact-sheet-pdf-364-mb.jpg?quality=85)

