

PDF (656384K)
PDF (656384K)
PDF (656384K)

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
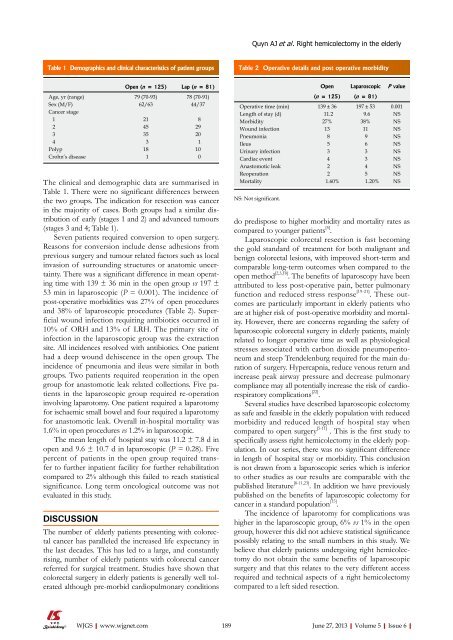
Quyn AJ et al . Right hemicolectomy in the elderlyTable 1 Demographics and clinical characteristics of patient groupsTable 2 Operative details and post operative morbidityThe clinical and demographic data are summarised inTable 1. There were no significant differences betweenthe two groups. The indication for resection was cancerin the majority of cases. Both groups had a similar distributionof early (stages 1 and 2) and advanced tumours(stages 3 and 4; Table 1).Seven patients required conversion to open surgery.Reasons for conversion include dense adhesions fromprevious surgery and tumour related factors such as localinvasion of surrounding structures or anatomic uncertainty.There was a significant difference in mean operatingtime with 139 ± 36 min in the open group vs 197 ±53 min in laparoscopic (P = 0.001). The incidence ofpost-operative morbidities was 27% of open proceduresand 38% of laparoscopic procedures (Table 2). Superficialwound infection requiring antibiotics occurred in10% of ORH and 13% of LRH. The primary site ofinfection in the laparoscopic group was the extractionsite. All incidences resolved with antibiotics. One patienthad a deep wound dehiscence in the open group. Theincidence of pneumonia and ileus were similar in bothgroups. Two patients required reoperation in the opengroup for anastomotic leak related collections. Five patientsin the laparoscopic group required re-operationinvolving laparotomy. One patient required a laparotomyfor ischaemic small bowel and four required a laparotomyfor anastomotic leak. Overall in-hospital mortality was1.6% in open procedures vs 1.2% in laparoscopic.The mean length of hospital stay was 11.2 ± 7.8 d inopen and 9.6 ± 10.7 d in laparoscopic (P = 0.28). Fivepercent of patients in the open group required transferto further inpatient facility for further rehabilitationcompared to 2% although this failed to reach statisticalsignificance. Long term oncological outcome was notevaluated in this study.DISCUSSIONOpen (n = 125) Lap (n = 81)Age, yr (range) 79 (70-93) 78 (70-91)Sex (M/F) 62/63 44/37Cancer stage1 21 82 45 293 35 204 3 1Polyp 18 10Crohn’s disease 1 0The number of elderly patients presenting with colorectalcancer has paralleled the increased life expectancy inthe last decades. This has led to a large, and constantlyrising, number of elderly patients with colorectal cancerreferred for surgical treatment. Studies have shown thatcolorectal surgery in elderly patients is generally well toleratedalthough pre-morbid cardiopulmonary conditionsOpen Laparoscopic P value(n = 125) (n = 81)Operative time (min) 139 ± 36 197 ± 53 0.001Length of stay (d) 11.2 9.6 NSMorbidity 27% 38% NSWound infection 13 11 NSPneumonia 8 9 NSIleus 5 6 NSUrinary infection 3 3 NSCardiac event 4 3 NSAnastomotic leak 2 4 NSReoperation 2 5 NSMortality 1.60% 1.20% NSNS: Not significant.do predispose to higher morbidity and mortality rates ascompared to younger patients [5] .Laparoscopic colorectal resection is fast becomingthe gold standard of treatment for both malignant andbenign colorectal lesions, with improved short-term andcomparable long-term outcomes when compared to theopen method [2,3,18] . The benefits of laparoscopy have beenattributed to less post-operative pain, better pulmonaryfunction and reduced stress response [19-21] . These outcomesare particularly important in elderly patients whoare at higher risk of post-operative morbidity and mortality.However, there are concerns regarding the safety oflaparoscopic colorectal surgery in elderly patients, mainlyrelated to longer operative time as well as physiologicalstresses associated with carbon dioxide pneumoperitoneumand steep Trendelenburg required for the main durationof surgery. Hypercapnia, reduce venous return andincrease peak airway pressure and decrease pulmonarycompliance may all potentially increase the risk of cardiorespiratorycomplications [22] .Several studies have described laparoscopic colectomyas safe and feasible in the elderly population with reducedmorbidity and reduced length of hospital stay whencompared to open surgery [5-11] . This is the first study tospecifically assess right hemicolectomy in the elderly population.In our series, there was no significant differencein length of hospital stay or morbidity. This conclusionis not drawn from a laparoscopic series which is inferiorto other studies as our results are comparable with thepublished literature [8-11,23] . In addition we have previouslypublished on the benefits of laparoscopic colectomy forcancer in a standard population [15] .The incidence of laparotomy for complications washigher in the laparoscopic group, 6% vs 1% in the opengroup, however this did not achieve statistical significancepossibly relating to the small numbers in this study. Webelieve that elderly patients undergoing right hemicolectomydo not obtain the same benefits of laparoscopicsurgery and that this relates to the very different accessrequired and technical aspects of a right hemicolectomycompared to a left sided resection.WJGS|www.wjgnet.com189 June 27, 2013|Volume 5|Issue 6|













