

23 Lower Eyelid Blepharoplasty - Facial plastic surgeon in San Diego
23 Lower Eyelid Blepharoplasty - Facial plastic surgeon in San Diego
23 Lower Eyelid Blepharoplasty - Facial plastic surgeon in San Diego

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
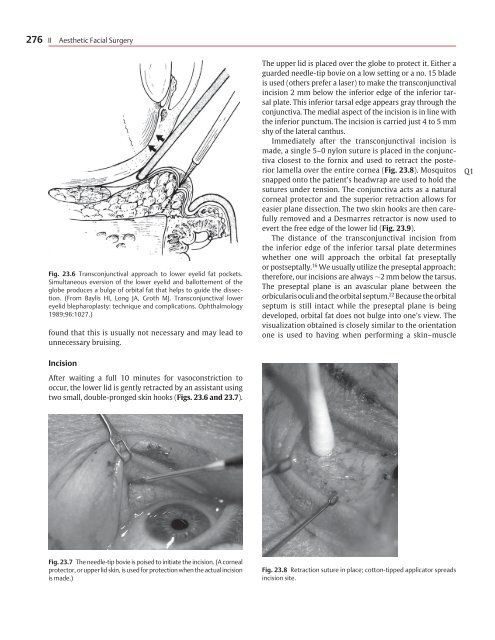
276 II Aesthetic <strong>Facial</strong> SurgeryFig. <strong>23</strong>.6 Transconjunctival approach to lower eyelid fat pockets.Simultaneous eversion of the lower eyelid and ballottement of theglobe produces a bulge of orbital fat that helps to guide the dissection.(From Baylis HI, Long JA, Groth MJ. Transconjunctival lowereyelid blepharoplasty: technique and complications. Ophthalmology1989;96:1027.)found that this is usually not necessary and may lead tounnecessary bruis<strong>in</strong>g.The upper lid is placed over the globe to protect it. Either aguarded needle-tip bovie on a low sett<strong>in</strong>g or a no. 15 bladeis used (others prefer a laser) to make the transconjunctival<strong>in</strong>cision 2 mm below the <strong>in</strong>ferior edge of the <strong>in</strong>ferior tarsalplate. This <strong>in</strong>ferior tarsal edge appears gray through theconjunctiva. The medial aspect of the <strong>in</strong>cision is <strong>in</strong> l<strong>in</strong>e withthe <strong>in</strong>ferior punctum. The <strong>in</strong>cision is carried just 4 to 5 mmshy of the lateral canthus.Immediately after the transconjunctival <strong>in</strong>cision ismade, a s<strong>in</strong>gle 5–0 nylon suture is placed <strong>in</strong> the conjunctivaclosest to the fornix and used to retract the posteriorlamella over the entire cornea (Fig. <strong>23</strong>.8). Mosquitossnapped onto the patient’s headwrap are used to hold thesutures under tension. The conjunctiva acts as a naturalcorneal protector and the superior retraction allows foreasier plane dissection. The two sk<strong>in</strong> hooks are then carefullyremoved and a Desmarres retractor is now used toevert the free edge of the lower lid (Fig. <strong>23</strong>.9).The distance of the transconjunctival <strong>in</strong>cision fromthe <strong>in</strong>ferior edge of the <strong>in</strong>ferior tarsal plate determ<strong>in</strong>eswhether one will approach the orbital fat preseptallyor postseptally. 16 We usually utilize the preseptal approach;therefore, our <strong>in</strong>cisions are always 2 mm below the tarsus.The preseptal plane is an avascular plane between theorbicularis oculi and the orbital septum. 22 Because the orbitalseptum is still <strong>in</strong>tact while the preseptal plane is be<strong>in</strong>gdeveloped, orbital fat does not bulge <strong>in</strong>to one’s view. Thevisualization obta<strong>in</strong>ed is closely similar to the orientationone is used to hav<strong>in</strong>g when perform<strong>in</strong>g a sk<strong>in</strong>–muscleQ1IncisionAfter wait<strong>in</strong>g a full 10 m<strong>in</strong>utes for vasoconstriction tooccur, the lower lid is gently retracted by an assistant us<strong>in</strong>gtwo small, double-pronged sk<strong>in</strong> hooks (Figs. <strong>23</strong>.6 and <strong>23</strong>.7).Fig. <strong>23</strong>.7 The needle-tip bovie is poised to <strong>in</strong>itiate the <strong>in</strong>cision. (A cornealprotector, or upper lid sk<strong>in</strong>, is used for protection when the actual <strong>in</strong>cisionis made.)Fig. <strong>23</strong>.8 Retraction suture <strong>in</strong> place; cotton-tipped applicator spreads<strong>in</strong>cision site.