

BULLOUS PEMPHIGOID - IMMCO Diagnostics
BULLOUS PEMPHIGOID - IMMCO Diagnostics
BULLOUS PEMPHIGOID - IMMCO Diagnostics

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
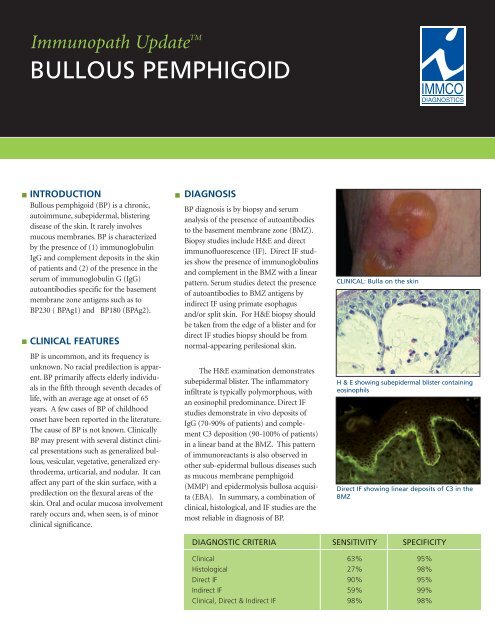
Immunopath Update TM<strong>IMMCO</strong> <strong>Diagnostics</strong>, Inc.<strong>BULLOUS</strong> <strong>PEMPHIGOID</strong>The Total Solution in Autoimmunity ■■INTRODUCTIONBullous pemphigoid (BP) is a chronic,autoimmune, subepidermal, blisteringdisease of the skin. It rarely involvesmucous membranes. BP is characterizedby the presence of (1) immunoglobulinIgG and complement deposits in the skinof patients and (2) of the presence in theserum of immunoglobulin G (IgG)autoantibodies specific for the basementmembrane zone antigens such as toBP230 ( BPAg1) and BP180 (BPAg2).CLINICAL FEATURESBP is uncommon, and its frequency isunknown. No racial predilection is apparent.BP primarily affects elderly individualsin the fifth through seventh decades oflife, with an average age at onset of 65years. A few cases of BP of childhoodonset have been reported in the literature.The cause of BP is not known. ClinicallyBP may present with several distinct clinicalpresentations such as generalized bullous,vesicular, vegetative, generalized erythroderma,urticarial, and nodular. It canaffect any part of the skin surface, with apredilection on the flexural areas of theskin. Oral and ocular mucosa involvementrarely occurs and, when seen, is of minorclinical significance.■DIAGNOSISBP diagnosis is by biopsy and serumanalysis of the presence of autoantibodiesto the basement membrane zone (BMZ).Biopsy studies include H&E and directimmunofluorescence (IF). Direct IF studiesshow the presence of immunoglobulinsand complement in the BMZ with a linearpattern. Serum studies detect the presenceof autoantibodies to BMZ antigens byindirect IF using primate esophagusand/or split skin. For H&E biopsy shouldbe taken from the edge of a blister and fordirect IF studies biopsy should be fromnormal-appearing perilesional skin.The H&E examination demonstratessubepidermal blister. The inflammatoryinfiltrate is typically polymorphous, withan eosinophil predominance. Direct IFstudies demonstrate in vivo deposits ofIgG (70-90% of patients) and complementC3 deposition (90-100% of patients)in a linear band at the BMZ. This patternof immunoreactants is also observed inother sub-epidermal bullous diseases suchas mucous membrane pemphigoid(MMP) and epidermolysis bullosa acquisita(EBA). In summary, a combination ofclinical, histological, and IF studies are themost reliable in diagnosis of BP.CLINICAL: Bulla on the skinH & E showing subepidermal blister containingeosinophilsDirect IF showing linear deposits of C3 in theBMZDIAGNOSTIC CRITERIA SENSITIVITY SPECIFICITYClinical 63% 95%Histological 27% 98%Direct IF 90% 95%Indirect IF 59% 99%Clinical, Direct & Indirect IF 98% 98%
<strong>BULLOUS</strong> <strong>PEMPHIGOID</strong>■BP can be differentiated from EBA bylocalizing the site of immunedeposits onthe peri-lesional biopsy split at the laminalucida junction by incubating the patient'sskin biopsy in high salt. These antigenlocalization studies can be performedon specimens that have been submittedfor routine IF studies. Similar studies ofantigen localization can also be performedon serum. Based on the site of localizationof immune deposits differentaiton betweenBP and EBA can reliably be made assummarized to the right.TREATMENTTopical steroids are effective howevertheir use in extensive disease may belimited by side effects and practicalfactors. The effectiveness of the additionof plasma exchange or azathioprine tocorticosteroids has not been fullyestablished. Combination treatment withtetracycline and nicotinamide may beuseful.■METHODS OF DIFFERENTIATION BP EBASerum tests for BMZ antibodies on Roof Floorsalt split skinRoof & FloorDirect IF on normal salt split skin (may be Roof Floorperformed on same specimen submittedRoof & Floorfor DIF)“Antigen Mapping” for Type IV collagen Floor Roofand Laminin on lesional biopsySUGGESTED READINGLiu Z. Diaz LA. Bullous pemphigoid: end of the centuryoverview. J Dermatol. 2001;28:647-50.Fleming TE, Korman NJ: Cicatricial pemphigoid. JAm Acad Dermatol. 2000;43:571-91;Walsh SR. Hogg D. Mydlarski PR. Bullous pemphigoid:from bench to bedside. Drugs.2005; 65:905-26.Khumalo N. Kirtschig G. Middleton P. Hollis S.Wojnarowska F. Murrell D. Interventions for bullouspemphigoid. Cochrane Database Syst Rev.2005;(3):CD002292.SPECIMEN SUBMISSIONSpecimen collection kits are available free of charge. Please call (800) 537-8378 for animmediate shipment. Use appropriate tube(s) as follows:<strong>IMMCO</strong> <strong>Diagnostics</strong>, Inc. | 60 Pineview DriveBuffalo, NY 14228 USA | www.immco.comtoll free North America: 1-800-537-8378phone: 1-716-691-0091 | fax: 1-716-691-0466Immunofluorescence:Lesional biopsy: Red tubeNormal biopsy: Purple tubeH&E biopsy: Green tubeSerology: Orange tubeSpecimens can be shipped by courier services, U.S. Postal Service and overnight carriers free ofcharge. Results are reported in two business days of specimen receipt via mail, fax and through<strong>IMMCO</strong> Online, a HIPAA-compliant web tool at www.immco.com.