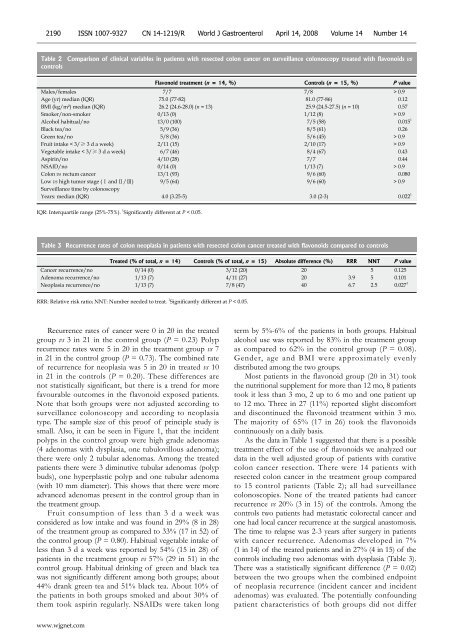
2190 ISSN 1007-9327 CN 14-1219/R World J Gastroenterol April 14, 2008 Volume 14 Number 14Table 2 Comparison <strong>of</strong> cl<strong>in</strong>ical variables <strong>in</strong> <strong>patients</strong> with resected colon cancer on surveillance colonoscopy treated with <strong>flavonoid</strong>s vscontrolsFlavonoid <strong>treatment</strong> (n = 14, %) Controls (n = 15, %) P valueMales/females 7/7 7/8 > 0.9Age (yr) median (IQR) 75.0 (77-82) 81.0 (77-86) 0.12BMI (kg/m²) median (IQR) 26.2 (24.6-28.0) (n = 13) 25.9 (24.5-27.5) (n = 10) 0.57Smoker/non-smoker 0/13 (0) 1/12 (8) > 0.9Alcohol habitual/no 13/0 (100) 7/5 (58) 0.015 1Black tea/no 5/9 (36) 8/5 (61) 0.26Green tea/no 5/8 (36) 5/6 (45) > 0.9Fruit <strong>in</strong>take < 3/≥ 3 d a week) 2/11 (15) 2/10 (17) > 0.9Vegetable <strong>in</strong>take < 3/≥ 3 d a week) 6/7 (46) 8/4 (67) 0.43Aspir<strong>in</strong>/no 4/10 (28) 7/7 0.44NSAID/no 0/14 (0) 1/13 (7) > 0.9Colon vs rectum cancer 13/1 (93) 9/6 (60) 0.080Low vs high tumor stage (Ⅰ and Ⅱ/Ⅲ) 9/5 (64) 9/6 (60) > 0.9Surveillance time by colonoscopyYears: median (IQR) 4.0 (3.25-5) 3.0 (2-3) 0.022 1IQR: Interquartile range (25%-75%). 1 Significantly different at P < 0.05.Table 3 Recurrence rates <strong>of</strong> colon neoplasia <strong>in</strong> <strong>patients</strong> with resected colon cancer treated with <strong>flavonoid</strong>s compared to controlsTreated (% <strong>of</strong> total, n = 14) Controls (% <strong>of</strong> total, n = 15) Absolute difference (%) RRR NNT P valueCancer recurrence/no 0/14 (0) 3/12 (20) 20 5 0.125Adenoma recurrence/no 1/13 (7) 4/11 (27) 20 3.9 5 0.101Neoplasia recurrence/no 1/13 (7) 7/8 (47) 40 6.7 2.5 0.027 1RRR: Relative risk ratio; NNT: Number needed to treat. 1 Significantly different at P < 0.05.Recurrence rates <strong>of</strong> cancer were 0 <strong>in</strong> 20 <strong>in</strong> the treatedgroup vs 3 <strong>in</strong> 21 <strong>in</strong> the control group (P = 0.23) Polyprecurrence rates were 5 <strong>in</strong> 20 <strong>in</strong> the <strong>treatment</strong> group vs 7<strong>in</strong> 21 <strong>in</strong> the control group (P = 0.73). The comb<strong>in</strong>ed rate<strong>of</strong> recurrence for neoplasia was 5 <strong>in</strong> 20 <strong>in</strong> treated vs 10<strong>in</strong> 21 <strong>in</strong> the controls (P = 0.20). These differences arenot statistically significant, but there is a trend for morefavourable outcomes <strong>in</strong> the <strong>flavonoid</strong> exposed <strong>patients</strong>.Note that both groups were not adjusted accord<strong>in</strong>g tosurveillance colonoscopy and accord<strong>in</strong>g to neoplasiatype. The sample size <strong>of</strong> this pro<strong>of</strong> <strong>of</strong> pr<strong>in</strong>ciple study issmall. Also, it can be seen <strong>in</strong> Figure 1, that the <strong>in</strong>cidentpolyps <strong>in</strong> the control group were high grade adenomas(4 adenomas with dysplasia, one tubulovillous adenoma);there were only 2 tubular adenomas. Among the treated<strong>patients</strong> there were 3 dim<strong>in</strong>utive tubular adenomas (polypbuds), one hyperplastic polyp and one tubular adenoma(with 10 mm diameter). This shows that there were moreadvanced adenomas present <strong>in</strong> the control group than <strong>in</strong>the <strong>treatment</strong> group.Fruit consumption <strong>of</strong> less than 3 d a week wasconsidered as low <strong>in</strong>take and was found <strong>in</strong> 29% (8 <strong>in</strong> 28)<strong>of</strong> the <strong>treatment</strong> group as compared to 33% (17 <strong>in</strong> 52) <strong>of</strong>the control group (P = 0.80). Habitual vegetable <strong>in</strong>take <strong>of</strong>less than 3 d a week was reported by 54% (15 <strong>in</strong> 28) <strong>of</strong><strong>patients</strong> <strong>in</strong> the <strong>treatment</strong> group vs 57% (29 <strong>in</strong> 51) <strong>in</strong> thecontrol group. Habitual dr<strong>in</strong>k<strong>in</strong>g <strong>of</strong> green and black teawas not significantly different among both groups; about44% drank green tea and 51% black tea. About 10% <strong>of</strong>the <strong>patients</strong> <strong>in</strong> both groups smoked and about 30% <strong>of</strong>them took aspir<strong>in</strong> regularly. NSAIDs were taken longterm by 5%-6% <strong>of</strong> the <strong>patients</strong> <strong>in</strong> both groups. Habitualalcohol use was reported by 83% <strong>in</strong> the <strong>treatment</strong> groupas compared to 62% <strong>in</strong> the control group (P = 0.08).Gender, age and BMI were approximately evenlydistributed among the two groups.Most <strong>patients</strong> <strong>in</strong> the <strong>flavonoid</strong> group (20 <strong>in</strong> 31) tookthe nutritional supplement for more than 12 mo, 8 <strong>patients</strong>took it less than 3 mo, 2 up to 6 mo and one patient upto 12 mo. Three <strong>in</strong> 27 (11%) reported slight discomfortand discont<strong>in</strong>ued the <strong>flavonoid</strong> <strong>treatment</strong> with<strong>in</strong> 3 mo.The majority <strong>of</strong> 65% (17 <strong>in</strong> 26) took the <strong>flavonoid</strong>scont<strong>in</strong>uously on a daily basis.As the data <strong>in</strong> Table 1 suggested that there is a possible<strong>treatment</strong> effect <strong>of</strong> the use <strong>of</strong> <strong>flavonoid</strong>s we analyzed ourdata <strong>in</strong> the well adjusted group <strong>of</strong> <strong>patients</strong> with curativecolon cancer resection. There were 14 <strong>patients</strong> withresected colon cancer <strong>in</strong> the <strong>treatment</strong> group comparedto 15 control <strong>patients</strong> (Table 2); all had surveillancecolonoscopies. None <strong>of</strong> the treated <strong>patients</strong> had cancerrecurrence vs 20% (3 <strong>in</strong> 15) <strong>of</strong> the controls. Among thecontrols two <strong>patients</strong> had metastatic colorectal cancer andone had local cancer recurrence at the surgical anastomosis.The time to relapse was 2-3 years after surgery <strong>in</strong> <strong>patients</strong>with cancer recurrence. Adenomas developed <strong>in</strong> 7%(1 <strong>in</strong> 14) <strong>of</strong> the treated <strong>patients</strong> and <strong>in</strong> 27% (4 <strong>in</strong> 15) <strong>of</strong> thecontrols <strong>in</strong>clud<strong>in</strong>g two adenomas with dysplasia (Table 3).There was a statistically significant difference (P = 0.02)between the two groups when the comb<strong>in</strong>ed endpo<strong>in</strong>t<strong>of</strong> neoplasia recurrence (<strong>in</strong>cident cancer and <strong>in</strong>cidentadenomas) was evaluated. The potentially confound<strong>in</strong>gpatient characteristics <strong>of</strong> both groups did not differwww.wjgnet.com
Hoensch H et al . Flavonoids and recurrence <strong>of</strong> neoplasia 2191significantly except for habitual alcohol consumption, whichwas significantly more prevalent <strong>in</strong> the treated <strong>patients</strong> than<strong>in</strong> controls. For neoplasia recurrence the prognostically mostimportant factor is the previous tumor stage, which was notsignificantly different between the two groups.DISCUSSIONRecurrence risk is the ma<strong>in</strong> concern <strong>of</strong> <strong>patients</strong> withprevious resected colorectal cancer [1-4] . On follow-up about40% <strong>of</strong> surgically curable colorectal cancers with stageⅡ and stage Ⅲ (accord<strong>in</strong>g to the UICC stag<strong>in</strong>g system)will suffer recurrent cancers with<strong>in</strong> 3-4 years. The bestoutcomes were reported for stage Ⅰ and stage Ⅱ tumors(around 90% survival without recurrences). The prognosis<strong>of</strong> stage Ⅲ cancer (with cancerous regional lymph nodes)is less favourable, but can be improved by adjuvantchemotherapy. Treated cases and controls <strong>in</strong> our studydid not differ regard<strong>in</strong>g the <strong>in</strong>itial tumor stage at surgery;about 40% <strong>in</strong> both groups were stage Ⅲ tumors, only 2<strong>of</strong> them (controls) had adjuvant chemotherapy becausethe surgeon felt confident that most <strong>of</strong> these <strong>patients</strong>would not be suitable for adjuvant chemotherapy. Thetumor recurrence <strong>in</strong> the controls was not observed <strong>in</strong> the<strong>patients</strong> on chemotherapy, but there were too few <strong>patients</strong>to judge whether this could <strong>in</strong>fluence outcomes. We foundthe expected recurrence rate <strong>in</strong> the controls (Table 3),but no <strong>in</strong>cident cancers and only one <strong>in</strong>cident adenoma<strong>in</strong> the <strong>flavonoid</strong> exposed <strong>patients</strong>. Eighty-seven <strong>of</strong> the160 <strong>patients</strong> from the registry were enrolled because wedetected only 56 controls that could be properly adjustedto the 31 treated <strong>patients</strong>. The match<strong>in</strong>g ratio <strong>of</strong> about oneto two (31 treated vs 56 controls) seems to be appropriate.In this real world study 76% <strong>of</strong> the treated and 43% <strong>of</strong>the controls had surveillance colonoscopies; among theresected <strong>patients</strong> 80% had surveillance by colonoscopy butonly 33% <strong>of</strong> the polypectomized <strong>patients</strong>. This fact might<strong>in</strong>fluence the reliability <strong>of</strong> the conclusions regard<strong>in</strong>g theadenoma recurrence.Our controlled cl<strong>in</strong>ical trial was a prospective andobservational <strong>cohort</strong> study performed with the aim <strong>of</strong>f<strong>in</strong>d<strong>in</strong>g out whether long-term <strong>flavonoid</strong> exposure <strong>of</strong><strong>patients</strong> from a tumor registry alters the outcome comparedto untreated control <strong>patients</strong>. This pro<strong>of</strong> <strong>of</strong> pr<strong>in</strong>ciplestudy suggests that <strong>flavonoid</strong>s can be used to reduce therecurrence rate <strong>in</strong> <strong>patients</strong> with resected colorectal cancers.Flavonoids are good candidates for primary and secondaryprevention <strong>of</strong> colorectal cancer, s<strong>in</strong>ce numerous <strong>in</strong> vitrostudies and animal work report on their beneficial activities<strong>in</strong> terms <strong>of</strong> suppression <strong>of</strong> cancer proliferation, antioxidativeand antiangiogenetic properties [24] . Epidemiological<strong>in</strong>vestigations [22,25,26] , <strong>in</strong> vivo and <strong>in</strong> vitro experiments [31-35] andone cl<strong>in</strong>ical <strong>in</strong>tervention study [29] support this concept. Otherauthors could not f<strong>in</strong>d protective effects <strong>of</strong> <strong>flavonoid</strong>son colorectal cancer <strong>in</strong>cidence [21,27,36] . Flavonoids derivedfrom tea plants can be used as a mean <strong>of</strong> biopreventionand have been manufactured and marketed as nutritionalsupplements [24] . Other methods <strong>of</strong> prevention are noteffective (e.g. vitam<strong>in</strong>s except folic acid), show only marg<strong>in</strong>alefficacy (e.g. calcium, selenium) or cannot be used <strong>in</strong> generalbecause <strong>of</strong> their unwanted side effects and complications(aspir<strong>in</strong>, NSAIDs) [20] .We tested the efficacy <strong>of</strong> <strong>flavonoid</strong> supplementation<strong>in</strong> a high risk population (resected colorectal cancer) toexam<strong>in</strong>e its effect <strong>in</strong> a relatively small number <strong>of</strong> <strong>patients</strong>,which were carefully adjusted for various cl<strong>in</strong>ical variableswith prognostic relevance. However, there are prognosticcl<strong>in</strong>ical factors which were not taken <strong>in</strong>to account such aspenetration depth <strong>in</strong>to the colonic wall and histologicalgrad<strong>in</strong>g. Cl<strong>in</strong>ical studies with a larger sample size anda higher statistical power are necessary to show that<strong>flavonoid</strong> exposure alters the outcome <strong>in</strong> terms <strong>of</strong> tumorrecurrence. Flavonoids could prevent recurrences <strong>of</strong>neoplasia by protect<strong>in</strong>g the genome <strong>of</strong> colonocytes fromgenotoxic <strong>in</strong>sults such as oxidative damage, free radicalattacks and adduct formation [37] . Flavonoids are secondaryplant products which could be responsible for some<strong>of</strong> the healthy effects <strong>of</strong> fruits and vegetables. It is stillunknown which components <strong>of</strong> vegetables and fruits areeffective for tumor prevention; ballast, fibres and secondaryplant products play a major role [6,10,38] . Flavonoids, <strong>in</strong>dols,isothiocyanates, curcum<strong>in</strong>, resveratrol, glucos<strong>in</strong>olates andother plant products affect carc<strong>in</strong>ogenic, mutagenic andneoplastic mechanisms [24] , but could also <strong>in</strong>duce protectiveenzymes <strong>of</strong> the <strong>in</strong>test<strong>in</strong>al mucosa [39] . Beside the type <strong>of</strong>chemical and biological prevention lifestyle factors, typeand amount <strong>of</strong> tea consumption, genetic factors, aspir<strong>in</strong>and NSAID medication could <strong>in</strong>fluence the outcome.These variables have to be considered when evaluat<strong>in</strong>g theeffects <strong>of</strong> <strong>flavonoid</strong> <strong>in</strong>tervention. As shown <strong>in</strong> Tables 1and 2 these variables were well balanced among cases andcontrols. However, alcohol use was more prevalent <strong>in</strong>the treated <strong>patients</strong> with resected colorectal cancer than<strong>in</strong> controls. We do not th<strong>in</strong>k that differences <strong>of</strong> habitualalcohol dr<strong>in</strong>k<strong>in</strong>g can expla<strong>in</strong> the difference <strong>of</strong> recurrences<strong>in</strong>ce ethanol is thought <strong>of</strong> as a carc<strong>in</strong>ogenic risk factor andwould rather <strong>in</strong>crease the recurrence risk <strong>of</strong> the <strong>flavonoid</strong>exposed <strong>patients</strong>.Patient compliance with the <strong>flavonoid</strong> <strong>treatment</strong> wasevaluated us<strong>in</strong>g <strong>in</strong>formation derived from a questionnairegiven to 31 treated <strong>patients</strong> <strong>in</strong> the <strong>treatment</strong> group. 67%<strong>of</strong> these treated <strong>patients</strong> took the nutritional supplementlonger than 12 mo, only 10% discont<strong>in</strong>ued the <strong>in</strong>takewith<strong>in</strong> the first 3 mo. No side effects or unwantedsymptoms were reported.The habitual vegetable <strong>in</strong>take <strong>of</strong> the <strong>patients</strong> <strong>in</strong> both<strong>treatment</strong> and control groups (Tables 1 and 2) was ratherlow (< 3 d a week ) and only about 40%-50% <strong>of</strong> the<strong>patients</strong> consumed vegetables ≥ 3 d a week, which still isnot sufficient for tumor prevention. About 16%-30% <strong>of</strong>the <strong>patients</strong> (cases and controls, Tables 1 and 2) reportedlow fruit content <strong>in</strong> their diet (< 3 d a week). Thus, nosignificant differences <strong>of</strong> the dietary habits were observedamong treated and untreated <strong>patients</strong>. The self-adm<strong>in</strong>isteredquestionnaire which was used to assess dietary habitsprovided only a crude estimate and was not validated; it ishowever a simple and practical tool that was well acceptedand understood by the <strong>patients</strong>.Flavonoids are part <strong>of</strong> human nutrition and areconta<strong>in</strong>ed <strong>in</strong> vegetables and fruits, especially <strong>in</strong> apples,onions, berries, citrus fruits and teas but also <strong>in</strong> chocolate.Tea consumption <strong>of</strong> the <strong>patients</strong> was moderate and waswww.wjgnet.com