2010 Associate Medical Plans Comparison Chart - Seton Health Plan
2010 Associate Medical Plans Comparison Chart - Seton Health Plan
2010 Associate Medical Plans Comparison Chart - Seton Health Plan

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
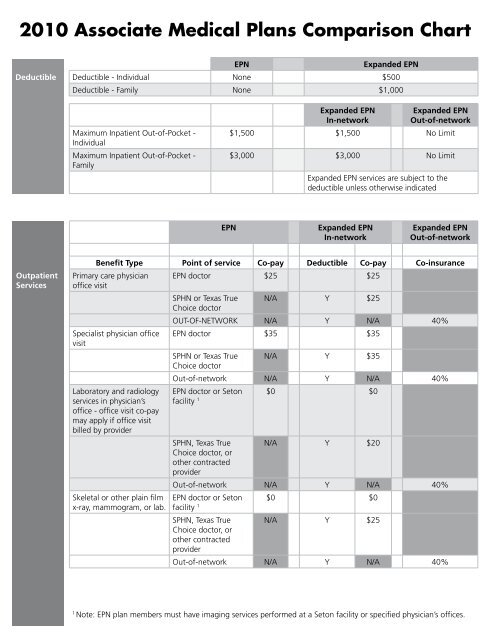
<strong>2010</strong> <strong>Associate</strong> <strong>Medical</strong> <strong><strong>Plan</strong>s</strong> <strong>Comparison</strong> <strong>Chart</strong>EPNExpanded EPNDeductible Deductible - Individual None $500Deductible - Family None $1,000Maximum Inpatient Out-of-Pocket -IndividualMaximum Inpatient Out-of-Pocket -FamilyExpanded EPNIn-networkExpanded EPNOut-of-network$1,500 $1,500 No Limit$3,000 $3,000 No LimitExpanded EPN services are subject to thedeductible unless otherwise indicatedEPNExpanded EPNIn-networkExpanded EPNOut-of-networkOutpatientServicesBenefit Type Point of service Co-pay Deductible Co-pay Co-insurancePrimary care physician EPN doctor $25 $25office visitSPHN or Texas True N/A Y $25Choice doctorOut-of-network N/A Y N/A 40%Specialist physician office EPN doctor $35 $35visitSPHN or Texas True N/A Y $35Choice doctorOut-of-network N/A Y N/A 40%Laboratory and radiologyservices in physician’soffice - office visit co-paymay apply if office visitbilled by providerSkeletal or other plain filmx-ray, mammogram, or lab.EPN doctor or <strong>Seton</strong> $0 $0facility 1SPHN, Texas True N/A Y $20Choice doctor, orother contractedproviderOut-of-network N/A Y N/A 40%EPN doctor or <strong>Seton</strong> $0 $0facility 1SPHN, Texas True N/A Y $25Choice doctor, orother contractedproviderOut-of-network N/A Y N/A 40%1Note: EPN plan members must have imaging services performed at a <strong>Seton</strong> facility or specified physician’s offices.
EPNExpanded EPNIn-networkExpanded EPNOut-of-networkOutpatientServicesBenefit Type Point of service Co-pay Deductible Co-pay Co-insuranceUltrasound, GI Series andother diagnostic servicesper plan guidelines,including contrast studieswith no vascular injectionMajor radiologicalprocedure (e.g., MRI,CT scan) and invasivediagnostic services perplan guidelines. (Listingof applicable servicesavailable upon request)Surgical procedure(s) in aprimary care or specialistphysician office - Pleasenote the physician maycharge for an office visiton the same date of theprocedure. In that case anoffice visit copay wouldapply.Prenatal and postnatalobstetrical care obstetricsphysician only.EPN doctor or <strong>Seton</strong> $0 $0facility 1SPHN, Texas True N/A Y $25Choice doctor, orother contractedproviderOut-of-network N/A Y N/A 40%EPN doctor or <strong>Seton</strong> $0 $0facility 1SPHN, Texas True N/A Y $100Choice doctor, orother contractedproviderOut-of-network N/A Y N/A 40%EPN doctor $0 $0SPHN or Texas True N/A Y $0Choice doctorOut-of-network N/A Y N/A 40%EPN doctor $35 $35SPHN or Texas True N/A Y $35Choice doctorOut-of-network N/A Y N/A 40%1Note: EPN plan members must have imaging services performed at a <strong>Seton</strong> facility or specified physician’s offices.
EPNExpanded EPNIn-networkExpanded EPNOut-of-networkOutpatientServicesBenefit Type Point of service Co-pay Deductible Co-pay Co-insuranceRehabilitation therapies(speech, physical,occupational, cardiac)- When services arerendered at a <strong>Seton</strong> Familyor Joint Venture FacilityAuthorization is requiredafter the first 12 visits pertype of therapy service(i.e., speech, physical,occupational) - Whenservices are rendered via aSPHN, Texas True Choice,or out of network providerauthorization is requiredafter the first 8 visits pertype of therapy service(i.e., speech, physical,occupational)Outpatient surgeryphysician charges(surgeon, anesthesia,pathology, radiology)Outpatient surgeryhospital charges<strong>Medical</strong> or surgicalobservation (scheduled,direct admission) 2<strong>Seton</strong> Family or joint $15 $20venture facility 1SPHN or Texas True N/A Y $20Choice doctorOut-of-network N/A Y N/A 40%EPN doctor $0 $0SPHN or Texas True N/A Y $0Choice doctorOut-of-network N/A Y N/A 40%<strong>Seton</strong> Family or joint $0 $0venture facilityContracted facility $0 Y $0Out-of-network N/A Y N/A 40%<strong>Seton</strong> Family or joint $0 $0venture facilityContracted facility $0 Y $0Out-of-network N/A Y N/A 40%Preventive<strong>Health</strong> CareServicesCheck-ups, well-baby andwell-child careEPN doctor $25 $25SPHN or Texas True N/A Y $25Choice doctorOut-of-network N/A Y N/A 40%1Note: EPN plan members must have imaging services performed at a <strong>Seton</strong> facility or specified physician’s offices.2Note: Must be less than 24 hours or observation will be subject to inpatient per day co-pay.
EPNExpanded EPNIn-networkExpanded EPNOut-of-networkPreventive<strong>Health</strong> CareServicesBenefit Type Point of service Co-pay Deductible Co-pay Co-insuranceOther immunizations EPN doctor $25 $25Well-woman examinationby primary care physicianWell-woman examinationby OB/GYNSPHN or Texas True N/A Y $25Choice doctorOut-of-network N/A Y N/A 40%EPN doctor $25 $25SPHN or Texas True N/A Y $25Choice doctorOut-of-network N/A Y N/A 40%EPN doctor $35 $35SPHN or Texas True N/A Y $35Choice doctorOut-of-network N/A Y N/A 40%In-patienthospitalservices(Must beAuthorized)Facility charges (peradmission)<strong>Seton</strong> Family or jointventure facility$100$100per day 1 per day 1Y $100Contracted facility $100per day 1 per day 1Out-of-network N/A Y N/A 40%Physician charges EPN doctor $0 $0SPHN or Texas True N/A Y $0Choice doctorOut-of-network N/A Y N/A 40%Maternity services -mother (per admission)hospital chargesMaternity services -mother (per admission)physician chargesMaternity servicesnewborn(per admission)hospital charges<strong>Seton</strong> Family or jointventure facility$100$100per day 1 per day 1Y $100Contracted facility $100per day 1 per day 1Out-of-network N/A Y N/A 40%EPN doctor $0 $0SPHN or Texas True N/A Y $0Choice doctorOut-of-network N/A Y N/A 40%<strong>Seton</strong> Family or jointventure facility$100$100per day 1 per day 1Y $100Contracted facility $100per day 1 per day 1Out-of-network N/A Y N/A 40%1$100 per day; $500 maximum per admission
EPNExpanded EPNIn-networkExpanded EPNOut-of-networkIn-patienthospitalservices(Must beAuthorized)Benefit Type Point of service Co-pay Deductible Co-pay Co-insuranceMaternity servicesnewbornEPN doctor $0 $0(per admission)physician chargesSPHN or Texas True N/A Y $0Choice doctorOut-of-network N/A Y N/A 40%Behavioral<strong>Health</strong>ServicesInpatient facility charges<strong>Seton</strong> Family or jointventure facility$100$100per day 1 per day 1Y $100Contracted facility $100per day 1 per day 1Out-of-network N/A Y N/A 40%Inpatient physician charges EPN doctor $0 $0SPHN or Texas True N/A Y $0Choice doctorOut-of-network N/A Y N/A 40%Outpatient EPN provider $35 $35SPHN or Texas True N/A Y $35Choice doctorOut-of-network N/A Y N/A 40%Chemical dependencyinpatient facility chargesChemical dependencyinpatient physician charges<strong>Seton</strong> Family or jointventure facility$100per day 1 $100per day 1Contracted facility $100$100per day 1 per day 1Out-of-network N/A Y N/A 40%EPN provider $0 $0SPHN or Texas True N/A Y $0Choice doctorOut-of-network N/A Y N/A 40%Benefit Type Point of service Co-pay Deductible Co-pay Co-insuranceChemical dependency EPN provider $35 $35outpatient individual orgroup therapy sessionsSPHN or Texas True N/A Y $35Choice doctorOut-of-network N/A Y N/A 40%1$100 per day; $500 maximum per admission
EPNExpanded EPNIn-networkExpanded EPNOut-of-networkOther<strong>Health</strong> CareServicesBenefit Type Point of service Co-pay Deductible Co-pay Co-insuranceOrgan transplantation - <strong>Seton</strong> Family or joint $0 $0transplant event (Note: venture facilityphysician and hospitalservices rendered pre-andpost-transplant are subjectto co-pays based on typeof service rendered)Contracted facility $0 Y $0Out-of-network N/A N/A 40%Home health care (per Contracted $15 Y $20visit)Out-of-network N/A Y N/A 40%Diabetic supplies - insulin, Contracted $10 1 $10 1test strips, lancets andsyringesOut-of-network N/A Y N/A 40%Diabetic equipment - Contracted $0 2 $0 2blood glucose monitorsOut-of-network N/A Y N/A 40%Diabetic self-management <strong>Seton</strong> facility only $15 $20training (covered at <strong>Seton</strong>facilities only)Out-of-network N/A N/A N/ALiving Well with Diabetes <strong>Seton</strong> facility only $0 $0Program: Team approachin managing diabetes;includes diabetic education,nutritional counseling, anddiabetic educator support.Out-of-network N/A N/A N/ALife Style ChangesPrograms (Weightmanagement options):1.<strong>Seton</strong> Create your WeightProgram - 9 week sessions,$20 workbook fee2. <strong>Seton</strong> IndividualNutritional Counseling Visits(maximum 6 visits/plan year)<strong>Seton</strong> Family or jointventure facility$20 $30Out-of-network N/A N/A N/A<strong>Seton</strong> Family or joint $20 $30venture facilityOut-of-network N/A N/A N/A1DME and Pharmacy BenefitsInsulin (any brand) = $10 for 30-day supplyGlucose test strips = $10 for 30-day supplyLancets = $10 for 30-day supplySyringes = $10 for 30-day supply2If additional monitor is required, co-pay = $15
EPNExpanded EPNIn-networkExpanded EPNOut-of-networkOther<strong>Health</strong> CareServicesBenefit Type Point of service Co-pay Deductible Co-pay Co-insurance3. Physician Directed Contracted Provider $35 $35Program: comprehensiveweight loss programOut-of-network N/A N/A N/AAcupuncture (Annual 20 EPN provider $20 $30visit maximum)SPHN or Texas True N/A Y $30Choice providerAcupuncture Intern $10 Y $15ClinicOut-of-network N/A Y N/A 40%Biofeedback (Annual 20 visit EPN provider $20 $30maximum and authorizationrequired for ALL visits)Chiropractic (Annual 20visit maximum and noauthorization required)Allergy testing and shots($500 maximum) - serumonlyDurable medicalequipment ($5,000 planyear maximum)Hospice services (180 dayslifetime maximum)Texas True Choice N/A Y $30providerOut-of-network N/A Y N/A 40%EPN provider $20 $30Texas True Choice N/A Y $30providerOut-of-network N/A Y N/A 40%$15 $20SPHN or Texas True N/A Y $20Choice doctorOut-of-network N/A Y N/A 40%Contracted provider $0 $0Out-of-network N/A Y N/A 40%Contracted provider $0 $0Out-of-network N/A Y N/A 40%Emergencyand UrgentCareEmergency careEmergency care toobservation care (overnightstays for observation careare not considered inpatientadmissions)<strong>Seton</strong> Family or jointventure facility$125 $125Contracted facility $125 Y $125Out-of-network N/A Y N/A 40%<strong>Seton</strong> Family or joint $125 $125venture facilityContracted facility $125 Y $125Out-of-network N/A Y N/A 40%
EPNExpanded EPNIn-networkExpanded EPNOut-of-networkEmergencyand UrgentCareBenefit Type Point of service Co-pay Deductible Co-pay Co-insuranceEmergency care to <strong>Seton</strong> Family or joint $125 $125surgery then observation venture facilitycare (overnight staysfor observation care arenot considered inpatientadmissions).Contracted facility $125 Y $125Out-of-network N/A Y N/A 40%Urgent care <strong>Seton</strong> facility $45 $45Contracted facility $45 $45Texas True Choice $45 Y $45Out-of-network N/A Y N/A 40%Emergency ambulance (if All plans $0 $50transported to a hospitalby the ambulance)PrescriptionDrugsGeneric $15 N/A $15 $15Diabetic SuppliesInsulin (any brand), $10 N/A $10 $1030-day supplyLancets, 30-day $10 N/A $10 $10supplySyringes, 30-day $10 N/A $10 $10supplyGlucose test strips, $10 N/A $10 $1030-day supplyPreferred (see formulary) $30 N/A $30 $30Non-preferred (see$60 N/A $60 $60formulary)Note: Members may receive a three months’ supply of medication for two co-payments either by using one of the<strong>Seton</strong> Network Outpatient Pharmacies or by using the mail order program.Some drugs are subject to authorization and quantity limits. Please refer to the formulary for this information. Ifa generic drug is available and a name brand is filled your co-pay will be the co-pay listed above plus the costdifference between the generic and name brand drug.AdditionalInformation(1) The specified physicians are listed in the directory with a star symbol next to their names.*In-network services must be received from in-network participating providers and accessed according to the rulesof the plan.*Covered services provided under Expanded EPN out-of-network benefits may be received from any licensedprovider*Expanded Out-of-Network - After meeting the annual deductible, the participant is responsible for charges inexcess of usual, customary and reasonable (UCR).*Information regarding your coverage is addressed in the information you receive from <strong>Seton</strong> Human Resources. Ifyou have additional questions after reviewing the information please contact member services at (512) 421-5667 ortoll free (866) 272-2507.
AdditionalInformationExcept when services are received at a <strong>Seton</strong> Family of Hospitals or Joint Venture facility, Expanded annual deductiblemust be satisfied first before payment will be made to a provider by the plan. Once the deductible is satisfied youwill be responsible for the co-pay/co-insurance only.Inpatient out-of-pocket individual and family maximums do not include deductible and co-payments onlycoinsurance is applied to this maximum.Co-pays are applied when an office visit or other service subject to a co-pay is billed by a provider. When more thanone service subject to a co-pay is provided on the same day, same visit and by the same provider, then the plan willapply the highest co-pay to that visit.*Pharmacy and diabetic supplies not subject to deductibleLimitations and exclusions are specified in the Summary <strong>Plan</strong> Description.