Does taping influence electromyographic muscle activity in the ...
Does taping influence electromyographic muscle activity in the ...
Does taping influence electromyographic muscle activity in the ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Manual Therapy (2002) 7(3), 154–162# 2002 Elsevier Science Ltd. All rights reserved.doi:10.1054/math.2002.0464, available onl<strong>in</strong>e at http://www.idealibrary.com onOrig<strong>in</strong>al article<strong>Does</strong> <strong>tap<strong>in</strong>g</strong> <strong><strong>in</strong>fluence</strong> <strong>electromyographic</strong> <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> <strong>the</strong> scapular rotators<strong>in</strong> healthy shoulders?A. M. Cools, E. E. Witvrouw, L. A. Danneels, D. C. CambierDepartment of Rehabilitation Sciences and Physio<strong>the</strong>rapy & Postgraduate Education <strong>in</strong> Manual Therapy, Facultyof Medic<strong>in</strong>e and Health Sciences, University Hospital, Ghent, BelgiumSUMMARY. Although <strong>tap<strong>in</strong>g</strong> techniques are commonly used <strong>in</strong> addition to exercise programmes <strong>in</strong> <strong>the</strong>rehabilitation of shoulder <strong>in</strong>stability and secondary subacromial or <strong>in</strong>ternal imp<strong>in</strong>gement, few studies exist on <strong>the</strong>effect of <strong>tap<strong>in</strong>g</strong> on <strong>the</strong> <strong>muscle</strong> <strong>activity</strong> of <strong>the</strong> scapular rotators. The purpose of our study was to exam<strong>in</strong>e <strong>the</strong><strong><strong>in</strong>fluence</strong> of one particular tape on muscular <strong>activity</strong> <strong>in</strong> scapular <strong>muscle</strong>s. Twenty healthy shoulders were exam<strong>in</strong>edwith surface EMG record<strong>in</strong>gs on <strong>the</strong> three parts of trapezius and serratus anterior <strong>muscle</strong> dur<strong>in</strong>g dynamic full rangeof motion abduction and forward flexion. The movement direction, and tape and no-tape conditions wererandomized. The statistical analyses with ANOVA repeated Measures (GLM model) showed significant differencesamong <strong>the</strong> means between <strong>the</strong> four <strong>muscle</strong>s (Po0.05), two movement directions (Po0.05), applied resistance(Po0.01), and movement period (Po0.01). However, no significant difference was observed based on <strong>the</strong>application of tape. The results of our <strong>in</strong>vestigation revealed no significant <strong><strong>in</strong>fluence</strong> of tape application on EMG<strong>activity</strong> <strong>in</strong> <strong>the</strong> scapular <strong>muscle</strong>s <strong>in</strong> healthy subjects. Future research will be necessary to exam<strong>in</strong>e o<strong>the</strong>r parametersof neuromuscular control <strong>in</strong> order to determ<strong>in</strong>e possible proprioceptive changes <strong>in</strong> <strong>muscle</strong> recruitment with tapeapplication. r 2002 Elsevier Science Ltd. All rights reserved.INTRODUCTIONThe application of <strong>tap<strong>in</strong>g</strong> is widely used amongathletes both <strong>in</strong> <strong>the</strong> rehabilitation and <strong>in</strong> <strong>the</strong>prevention of sports <strong>in</strong>juries (Engstro¨ m & Renstro¨ m1998; Robb<strong>in</strong>s & Waked 1998). The basic rationalefor <strong>tap<strong>in</strong>g</strong> is to provide protection and support for ajo<strong>in</strong>t while permitt<strong>in</strong>g optimal functional movement.It is assumed that external support <strong>in</strong>creases jo<strong>in</strong>tstability by re<strong>in</strong>forc<strong>in</strong>g <strong>the</strong> ligaments and restrict<strong>in</strong>gmotions. However, various authors mention that <strong>the</strong>support function of <strong>tap<strong>in</strong>g</strong> is lost with<strong>in</strong> a relativelyshort time after application (Greene & Wight 1990;Gross et al. 1994; Lohrer et al. 1999).Received: 28 January 2002Revised: 13 May 2002Accepted: 5 June 2002Ann M. Cools, PT, candidate for a doctoral degree, Erik E.Witvrouw, PT, PhD, Lieven A. Danneels, PT, PhD, Dirk C.Cambier, PT, PhD, Director, Department of RehabilitationSciences and Physio<strong>the</strong>rapy, Ghent University, Ghent, Belgium.Correspondence to: AC, Department of Rehabilitation Sciencesand Physio<strong>the</strong>rapy & Postgraduate Education <strong>in</strong> Manual Therapy,University Hospital Ghent, De P<strong>in</strong>telaan 185, 1B3, B9000 Ghent,Belgium. Tel.: +32/240 26 32; Fax: +32/240 38 11E-mail: ann.cools@rug.ac.beMost authors agree that <strong>the</strong> effect of tape can onlypartially be expla<strong>in</strong>ed by <strong>in</strong>creased mechanicalstability (Wilkerson 1991; Bockrath et al. 1993;Bennell & Goldie 1994, Larsen et al. 1995; Kowallet al. 1996; Somes et al. 1997; Gilleard et al. 1998;Lohrer et al. 1999; McCaw & Cerullo 1999). It issuggested, however, that <strong>tap<strong>in</strong>g</strong> may have someproprioceptive <strong><strong>in</strong>fluence</strong>s. Therefore, if <strong>tap<strong>in</strong>g</strong> techniquesdo give jo<strong>in</strong>t protection, it is now thought that<strong>the</strong>y act by improv<strong>in</strong>g proprioception ra<strong>the</strong>r than byrestrict<strong>in</strong>g movement (Karllson & Andreasson 1992;Heit et al. 1996; Robb<strong>in</strong>s & Waked 1998).The effectiveness of various <strong>tap<strong>in</strong>g</strong> techniques wasstudied extensively <strong>in</strong> <strong>the</strong> knee (Anderson et al. 1992;Bockrath et al. 1993; Larsen et al. 1995; Kowall et al.1996; Gilleard et al. 1998), and <strong>the</strong> ankle (Wilkerson1991; Karlsson & Andreasson 1992; Lohrer et al.1999; McCaw & Cerullo 1999).Although <strong>the</strong> <strong><strong>in</strong>fluence</strong> of <strong>tap<strong>in</strong>g</strong> on neuromuscularfunction is often suggested, <strong>the</strong> underly<strong>in</strong>g mechanismis still unclear. Some authors found changes <strong>in</strong><strong>the</strong> onset of <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> <strong>the</strong> knee with tape(Karlsson & Andreasson 1992; Gilleard et al. 1998).They assumed that changes <strong>in</strong> latency times mightbe <strong>the</strong> result of cutaneous stimulation effected by <strong>the</strong>154
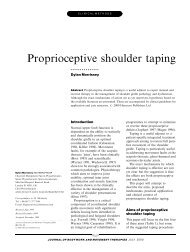
156 Manual TherapyFig. 2Fig. 1<strong>in</strong>ferior border of <strong>the</strong> scapula and <strong>the</strong> <strong>in</strong>sertion of <strong>the</strong><strong>muscle</strong> on <strong>the</strong> anterio-lateral side of <strong>the</strong> thorax. Areference electrode was placed over <strong>the</strong> clavicle. Eachset of bipolar record<strong>in</strong>g electrodes on each of <strong>the</strong> four<strong>muscle</strong>s was connected to a Noraxon Myosystem2000 <strong>electromyographic</strong> receiver (Noraxon USA,Inc., Scottsdale, AZ). The sampl<strong>in</strong>g rate was1000 Hz. All raw myo-electric signals were preamplified(overall ga<strong>in</strong> = 1000, common rate rejectionratio 115 dB, signal-to-noise ratio o1 mV RMSbasel<strong>in</strong>e noise, filtered to produce a bandwidth of10–1000 Hz).A strip of Fixomull stretch (Beiersdorf s ) wasapplied over <strong>the</strong> <strong>muscle</strong> belly of <strong>the</strong> upper trapezius,start<strong>in</strong>g anterior just proximal to <strong>the</strong> clavicle. Thetape was firmly pulled over <strong>the</strong> belly of <strong>the</strong> uppertrapezius, meanwhile giv<strong>in</strong>g a sk<strong>in</strong> traction on <strong>the</strong>soft tissue towards <strong>the</strong> cervical sp<strong>in</strong>e. On <strong>the</strong> posteriorside of <strong>the</strong> trunk, <strong>the</strong> tape was attached towards<strong>the</strong> thoracic sp<strong>in</strong>e, follow<strong>in</strong>g <strong>the</strong> <strong>muscle</strong> fibres of <strong>the</strong>lower trapezius. The same procedure was repeatedwith a leukotape P strip (Beiersdorf s ) (McConnell1999). All <strong>the</strong> <strong>tap<strong>in</strong>g</strong> applications were performed by<strong>the</strong> same researcher, who is experienced <strong>in</strong> <strong>the</strong>procedure (Fig. 2).Manual Therapy (2002) 7(3), 154–162Test<strong>in</strong>g procedureThe test<strong>in</strong>g session started with a warm-up procedure,consist<strong>in</strong>g of shoulder movements <strong>in</strong> alldirections, push-up-exercises aga<strong>in</strong>st <strong>the</strong> wall andstretch<strong>in</strong>g exercises for <strong>the</strong> rotator cuff and scapular<strong>muscle</strong>s. Then verification of EMG signal quality wascompleted for each <strong>muscle</strong> by hav<strong>in</strong>g <strong>the</strong> subjectperform isometric contractions <strong>in</strong> manual <strong>muscle</strong> testpositions specific to each <strong>muscle</strong> of <strong>in</strong>terest (Kendall& Kendall 1983). Subjects performed three 5-smaximum voluntary isometric <strong>muscle</strong> contractionsaga<strong>in</strong>st manual resistance by <strong>the</strong> pr<strong>in</strong>cipal <strong>in</strong>vestigator.A 5-s pause occurred between <strong>muscle</strong> contractions(Hancock & Hawk<strong>in</strong>s 1996, De Luca 1997). Asa normalization reference, EMG data were collecteddur<strong>in</strong>g maximal voluntary contraction (MVC) foreach <strong>muscle</strong>. After signal filter<strong>in</strong>g with a low-passfilter (s<strong>in</strong>gle pass, Butterworth, 6 Hz low-pass filter of<strong>the</strong> 6th order) and visual <strong>in</strong>spection for artefacts, <strong>the</strong>peak average EMG value over a w<strong>in</strong>dow of 1 s wascalculated for each trial. Fur<strong>the</strong>r calculations wereperformed with <strong>the</strong> mean of <strong>the</strong> repeated trials as anormalization value (100%) (Danneels et al. 2001).To avoid alterations <strong>in</strong> <strong>muscle</strong> <strong>activity</strong> of <strong>the</strong> uppertrapezius caused by head position or movement, <strong>the</strong>subjects were <strong>in</strong>structed to look <strong>in</strong> front of <strong>the</strong>m whiletest<strong>in</strong>g. Two movements were performed dur<strong>in</strong>g <strong>the</strong>test: abduction <strong>in</strong> <strong>the</strong> frontal plane, and forwardflexion <strong>in</strong> <strong>the</strong> sagittal plane. Each movement wasperformed over <strong>the</strong> whole range of motion <strong>in</strong> arhythm of 4 s:2 s of concentric contraction andupward movement, and 2 s of eccentric contractionand downward movement, with 4 s of rest betweentrials. The rhythm was set by a metronome andcontrolled by <strong>the</strong> exam<strong>in</strong>er’s count<strong>in</strong>g. Prior tostart<strong>in</strong>g collect<strong>in</strong>g data, subjects were allowed fivepractice trials to ensure <strong>the</strong>y completed <strong>the</strong> armmovement <strong>in</strong> a 4 s rhythm, as set by <strong>the</strong> metronome.Follow<strong>in</strong>g <strong>the</strong> practice trials, <strong>the</strong> subject completedthree trials of each movement. The second movementwas used for fur<strong>the</strong>r analysis.Each movement was performed with and withoutan external resistance, and <strong>in</strong> a tape and a no-tapecondition. The weight resistance was set at 2 kg for abody weight between 50 and 60 kg, 2.5 kg for a bodyweight between 70 and 80 kg, and 3 kg if <strong>the</strong> personweighed more than 80 kg. The test conditions tape/no-tape and abduction/forward flexion were randomized.Signal process<strong>in</strong>gAll raw EMG signals were analogue/digital (A/D)converted (12-bit resolution) at 1000 Hz. Signals <strong>the</strong>n# 2002 Elsevier Science Ltd. All rights reserved.
Tap<strong>in</strong>g and <strong>electromyographic</strong> <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> shoulders 157were digitally full-wave rectified and low-pass filtered(s<strong>in</strong>gle pass, Butterworth, 6 Hz low pass filter of sixthorder). Results were normalized to <strong>the</strong> maximum<strong>activity</strong> observed dur<strong>in</strong>g <strong>the</strong> maximal voluntary trials.After rectify<strong>in</strong>g, filter<strong>in</strong>g and normalization, fur<strong>the</strong>ranalysis was performed on four periods dur<strong>in</strong>g armmovement, each of 1-s duration. Periods were def<strong>in</strong>edby markers, automatically placed on <strong>the</strong> EMG signalwith every metronome signal. The mean amplitudeEMG signal, expressed as a percentage of maximalvoluntary contraction, was used to assess <strong>the</strong> <strong>activity</strong>of <strong>the</strong> three trapezius parts and serratus anterior<strong>muscle</strong> <strong>in</strong> each condition and each period.Statistical analysisDifferences <strong>in</strong> EMG <strong>activity</strong> among <strong>the</strong> severalconditions were analysed with an univariate approachto repeated measures analysis of variance(General L<strong>in</strong>ear Model), <strong>in</strong> which <strong>the</strong> with<strong>in</strong>-subjectfactors were: (1) <strong>muscle</strong>, (2) movement direction (3)resistance, (4) tape, and (5) period. The alpha-levelfor <strong>the</strong> ANOVA was set as 0.05. In case of significantdifferences, paired t-tests with Bonferroni correctionwere used for post-hoc multiple pairwise comparisons.All statistical analysis was performed with<strong>the</strong> Statistical Package for Social Sciences (SPSS),version 9.0.RESULTSThe results of <strong>the</strong> descriptive statistical analyses aresummarized <strong>in</strong> Table 1 for <strong>the</strong> abduction movementwith and without external resistance, and Table 2 for<strong>the</strong> forward flexion movement, with and withoutexternal resistance.The statistical analysis with ANOVA repeatedmeasures General L<strong>in</strong>ear and Model (GLM) showedsignificant differences <strong>in</strong> EMG <strong>activity</strong> based on <strong>the</strong>factors <strong>muscle</strong> (Po0.01), movement direction(Po0.01), resistance (Po0.01), and period (Po0.01), but no significant difference based on <strong>the</strong>application of tape (P = 0.578). The analysis of<strong>in</strong>teraction effects for <strong>the</strong> <strong>muscle</strong> factor revealedsignificant <strong>muscle</strong> movement direction <strong>in</strong>teractioneffect (Po0.05), and no significant <strong>in</strong>teraction for<strong>muscle</strong> period (P = 0.126) and <strong>muscle</strong> resistance(P = 0.720). There was no significant <strong>in</strong>teractionbetween <strong>the</strong> tape factor and any o<strong>the</strong>r factor <strong>in</strong> <strong>the</strong>GLM. The results show that <strong>the</strong> application of tapehas no <strong><strong>in</strong>fluence</strong> on EMG <strong>activity</strong> <strong>in</strong> all conditions,and differences <strong>in</strong> EMG <strong>activity</strong> based on all o<strong>the</strong>rfactors are <strong>in</strong>dependent of tape application (notape o<strong>the</strong>r factor <strong>in</strong>teraction).S<strong>in</strong>ce <strong>the</strong> <strong><strong>in</strong>fluence</strong> of tape on EMG <strong>activity</strong> for <strong>the</strong>four <strong>muscle</strong>s was of particular <strong>in</strong>terest, and <strong>the</strong>ANOVA showed no significant differences based on<strong>the</strong> application of tape, fur<strong>the</strong>r post-hoc analyses on<strong>the</strong> factor tape were not performed.DISCUSSIONNormal <strong>muscle</strong> <strong>activity</strong> of <strong>the</strong> scapular rotatorsallows for normal k<strong>in</strong>ematics of <strong>the</strong> scapular movement.The role of <strong>the</strong> scapular <strong>muscle</strong>s is to promoteglenohumeral stability, to provide a stable basis fromwhich o<strong>the</strong>r <strong>muscle</strong>s can operate <strong>in</strong> an optimallength–tension relationship, and to elevate <strong>the</strong>acromion dur<strong>in</strong>g arm elevation <strong>in</strong> order to preventimp<strong>in</strong>gement (Wilk & Arrigo 1993; Mottram 1997).In addition, <strong>the</strong> scapula plays an important role ofbe<strong>in</strong>g a l<strong>in</strong>k <strong>in</strong> <strong>the</strong> k<strong>in</strong>etic cha<strong>in</strong> of proximal to distalsequenc<strong>in</strong>g of velocity, energy and forces <strong>in</strong> manyshoulder activities such as throw<strong>in</strong>g (Kibler 1998).Anatomic and histochemical studies regard<strong>in</strong>gtrapezius <strong>muscle</strong> composition found some functionalsubdivisions with<strong>in</strong> <strong>the</strong> trapezius <strong>muscle</strong>. L<strong>in</strong>dmanet al. (1990, 1991) found that <strong>the</strong> ascend<strong>in</strong>g portion of<strong>the</strong> trapezius <strong>muscle</strong> (aris<strong>in</strong>g from <strong>the</strong> sp<strong>in</strong>ousprocesses and <strong>in</strong>tersp<strong>in</strong>ous ligaments of approximately<strong>the</strong> T 4 –T 12 vertebrae, and attach<strong>in</strong>g <strong>in</strong> <strong>the</strong>region of <strong>the</strong> tubercle at <strong>the</strong> medial end of <strong>the</strong> sp<strong>in</strong>e of<strong>the</strong> scapula) had a predom<strong>in</strong>ance of type I fibres,whereas <strong>the</strong> most superior parts of pars descendens(from <strong>the</strong> medial third of <strong>the</strong> superior nuchal l<strong>in</strong>e and<strong>the</strong> ligamentum nuchae to <strong>the</strong> posterior border of <strong>the</strong>lateral third of <strong>the</strong> clavicle) had a higher frequency oftype II fibres. These differences <strong>in</strong> fibre type mightreflect different functional demands on <strong>the</strong> trapezius<strong>muscle</strong> parts <strong>in</strong> various head, neck, and shouldermovements. The author concluded that <strong>the</strong> lowertrapezius seems best suited for postural and stabiliz<strong>in</strong>gfunctions <strong>in</strong> <strong>the</strong> shoulder and arm movements,whereas <strong>the</strong> upper trapezius seems best suited forphasic activities. Similar conclusions can be drawnfrom a dissection study reveal<strong>in</strong>g <strong>the</strong> fascicularanatomy of <strong>the</strong> trapezius (Johnson et al. 1994). Basedon <strong>the</strong> orientation of <strong>the</strong> fibres of <strong>the</strong> lower trapezius,it was suggested that <strong>the</strong> role of <strong>the</strong> lower part of <strong>the</strong>trapezius is more consistent with ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g horizontaland vertical equilibrium of <strong>the</strong> scapula ra<strong>the</strong>rthan generat<strong>in</strong>g net torque. In addition, Johnsonet al. (1994) hypo<strong>the</strong>sized that <strong>the</strong> thoracic fibres of<strong>the</strong> trapezius <strong>muscle</strong> do not appreciably changelength throughout <strong>the</strong> entire range of upwardrotation of <strong>the</strong> scapula. Hence, <strong>the</strong> contribution of<strong>the</strong> lower trapezius to net torque about <strong>the</strong> axis ofrotation of <strong>the</strong> scapula was thought to be limited. Theupper fibres of trapezius exert an upward rotationmoment about this axis, complement<strong>in</strong>g that of <strong>the</strong>serratus anterior. Wadsworth and Bullock-Saxton(1997) exam<strong>in</strong>ed <strong>the</strong> temporal recruitment patternsof <strong>the</strong> scapular rotator <strong>muscle</strong>s dur<strong>in</strong>g controlledvoluntary abduction <strong>in</strong> <strong>the</strong> scapular plane. Their# 2002 Elsevier Science Ltd. All rights reserved. Manual Therapy (2002) 7(3), 154–162
Manual Therapy (2002) 7(3), 154–162 # 2002 Elsevier Science Ltd. All rights reserved.Table 1 Mean (7 Standard Deviation) for <strong>the</strong> <strong>electromyographic</strong> <strong>activity</strong> of upper trapezius (UT), middle trapezius (MT), lower trapezius (LT), and serratus anterior (SA), expressed as percentage ofMaximal Voluntary Contraction dur<strong>in</strong>g dynamic abduction movements <strong>in</strong> a tape and no-tape condition, with and without external resistance, analysed for four periods of movement (period 1: concentricfrom 01 to 901 of abduction, period 2: concentric from 901 to 1801 of abduction, period 3: eccentric from 1801 to 901 of abduction, period 4: eccentric from 901 to 01 of abduction)Upper trapezius Middle trapezius Lower trapezius Serratus anteriorP1 P2 P3 P4 P1 P2 P3 P4 P1 P2 P3 P4 P1 P2 P3 P4No resistance, no tape 9.8(74.3)28.8(710.5)21.9(710.9)12.2(75.5)5.7(73.7)18.6(712.3)13.5(77.9)6.4(74.1)3.8(72.7)25.6(712.7)25.7(715.1)8.5(76.4)3.9(71.7)26.0(713.5)25.6(710.7)7.1(72.7)No resistance, tape 10.9(76.4)29.6(711.3)22.7(78.6)14.2(76.3)5.3(73.2)16.4(78.3)13.6(77.6)6.9(73.4)3.8(72.7)22.5(713.1)25.8(718.7)8.1(74.6)3.6(72.0)22.8(713.8)23.5(712.1)7.3(72.6)Resistance, no tape 19.8 51.7 32.1 24.7 11.0 35.2 23.6 17.6 8.5 41.8 40.6 20.6 8.0 42.2 36.7 17.3(711.1)Resistance, tape 22.3(711.2)Table 2 Mean (7 Standard Deviation) for <strong>the</strong> <strong>electromyographic</strong> <strong>activity</strong> of upper trapezius (UT), middle trapezius (MT), lower trapezius (LT), and serratus anterior (SA), expressed as percentage ofMaximal Voluntary Contraction dur<strong>in</strong>g dynamic forward flexion movements <strong>in</strong> a tape and no-tape condition, with and without external resistance, analysed for four periods of movement (period 1:concentric from 01 to 901 of abduction, period 2: concentric from 901 to 1801 of abduction, period 3: eccentric from 1801 to 901 of abduction, period 4: eccentric from 901 to 01 of abduction)Upper trapezius Middle trapezius Lower trapezius Serratus anteriorP1 P2 P3 P4 P1 P2 P3 P4 P1 P2 P3 P4 P1 P2 P3 P4No resistance, no tape 11.2(76.1)26.7(713.4)21.0(79.2)10.2(74.4)2.9(72.3)8.5(77.1)6.3(74.9)2.8(72.1)4.9(72.8)25.7(712.8)29.0(726.3)8.7(78.1)5.5(72.9)27.8(712.3)26.0(711.1)7.3(73.9)No resistance, tape 10.5(76.0)25.4(712.7)22.2(712.9)12.2(77.0)2.3(71.8)5.7(74.0)5.2(73.2)2.9(72.3)4.8(72.7)21.8(712.9)23.3(717.6)9.7(78.7)5.2(73.3)25.8(710.7)26.4(714.4)7.9(73.8)Resistance, no tape 18.2 42.5 29.3 20.6 5.7 17.4 10.4 8.5 11.4 38.1 33.6 22.8 10.7 43.8 35.8 19.6(78.1)Resistance, tape 15.6(76.8)(716.6)51.7(717.9)(714.3)44.1(716.7)(711.7)34.7(713.3)(711.8)30.6(712.2)(77.9)27.7(711.2)(79.2)23.3(711.4)(78.0)13.6(712.2)(74.3)5.4(74.5)(720.7)27.6(713.8)(712.2)16.2(711.6)(712.5)21.3(79.1)(76.9)10.2(78.0)(710.7)15.9(79.5)(76.4)8.4(76.7)(76.6)10.9(713.1)(79.5)10.8(76.8)(716.0)36.6(721.1)(715.8)37.5(720.8)(722.1)39.1(724.8)(726.4)26.9(718.5)(713.9)20.3(710.7)(715.5)25.9(718.2)(75.1)10.2(710.0)(78.6)8.8(75.6)(715.6)41.7(718.2)(716.9)42.1(716.4)(715.3)35.7(715.4)(717.2)36.1(714.3)(78.7)16.4(75.7)(711.9)19.7(78.5)158 Manual Therapy
Tap<strong>in</strong>g and <strong>electromyographic</strong> <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> shoulders 159results <strong>in</strong>dicated that <strong>in</strong> non-<strong>in</strong>jured shoulders, <strong>the</strong>upper trapezius was activated prior to <strong>the</strong> movement,whereas <strong>the</strong> lower trapezius was not recruited untilafter <strong>the</strong> start of <strong>the</strong> shoulder movement. However, <strong>in</strong>a recent study, we exam<strong>in</strong>ed <strong>muscle</strong> latency times of<strong>the</strong> different trapezius parts <strong>in</strong> response to a suddenunexpected arm movement (Cools et al. 2001). Ourresults showed no significant differences among <strong>the</strong>trapezius parts <strong>in</strong> relation to deltoid onset, thussuggest<strong>in</strong>g that <strong>the</strong> trapezius reacted as a unit <strong>in</strong>response to a sudden unexpected arm movement(Cools et al. 2001).Although <strong>the</strong> trapezius <strong>muscle</strong> is often considered amajor stabiliz<strong>in</strong>g <strong>muscle</strong> for <strong>the</strong> scapula (Johnson etal. 1994; Kibler 1998; Cools et al. 2001), o<strong>the</strong>rscapular <strong>muscle</strong>s also contribute to <strong>the</strong> stability andmovement quality of <strong>the</strong> scapula (P<strong>in</strong>k & Tibone2000; Sahrmann 2002). Impaired control of <strong>the</strong>scapula by <strong>the</strong> serratus anterior <strong>muscle</strong> is common<strong>in</strong> patients with shoulder problems (P<strong>in</strong>k & Tibone2000). The levator scapulae and rhomboid <strong>muscle</strong>sare both synergists and antagonists of <strong>the</strong> trapezius<strong>muscle</strong>. Their function is to adduct and <strong>in</strong>ternallyrotate <strong>the</strong> scapula. Shortness of <strong>the</strong>se <strong>muscle</strong>s mayrestrict upward rotation of <strong>the</strong> acromial region,necessary for normal shoulder function (Sahrmann2002). Scapulohumeral <strong>muscle</strong>s such as latissimusdorsi and pectoralis major also contribute to shoulderfunction. These <strong>muscle</strong>s essentially bypass <strong>the</strong> scapulaand are attached directly to <strong>the</strong> humerus, and cancontribute to disruption of scapulohumeral rhythm(Sahrmann 2002).Summariz<strong>in</strong>g, it is clear that <strong>the</strong>re are many diverseroles <strong>the</strong> scapula must play to achieve appropriateshoulder function. These roles are <strong>in</strong>terrelated anddepend on <strong>the</strong> quality of <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> <strong>the</strong>scapular <strong>muscle</strong>s. Therefore, restoration of normalscapular <strong>muscle</strong> <strong>activity</strong> is one of <strong>the</strong> priorities <strong>in</strong> <strong>the</strong>early phase of rehabilitation of <strong>the</strong> athlete withfunctional shoulder <strong>in</strong>stability.The purpose of our study was to determ<strong>in</strong>e if EMG<strong>activity</strong> <strong>in</strong> <strong>the</strong> scapular <strong>muscle</strong>s was <strong><strong>in</strong>fluence</strong>d by <strong>the</strong>application of tape over <strong>the</strong> <strong>muscle</strong> belly of <strong>the</strong> uppertrapezius and parallel to <strong>the</strong> direction of <strong>the</strong> lowertrapezius <strong>muscle</strong>. Based on previous <strong>in</strong>vestigationsand cl<strong>in</strong>ical assumptions (Mor<strong>in</strong> et al. 1997; McConnell1999), we hypo<strong>the</strong>sized that with tape <strong>the</strong> uppertrapezius <strong>activity</strong> would decrease, and <strong>the</strong> lowertrapezius <strong>activity</strong> would <strong>in</strong>crease. In addition, weassumed that <strong>the</strong> <strong>tap<strong>in</strong>g</strong> would change <strong>the</strong> overallrecruitment pattern of all scapular rotators, and<strong>the</strong>refore hypo<strong>the</strong>sized changes <strong>in</strong> <strong>muscle</strong> <strong>activity</strong> of<strong>the</strong> serratus anterior and middle trapezius.Confirm<strong>in</strong>g this hypo<strong>the</strong>sis would be cl<strong>in</strong>icallyrelevant, s<strong>in</strong>ce scapulothoracic dysfunction is oftenseen <strong>in</strong> patients with shoulder problems orcervicobrachial pathologies. In this muscular imbalance,an over<strong>activity</strong> of <strong>the</strong> upper trapezius part isassumed (P<strong>in</strong>k 1991; Kelley 1995). The purpose ofthis tape was to <strong>in</strong>hibit <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> <strong>the</strong> uppertrapezius part, and to enhance <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> <strong>the</strong>lower trapezius, thus correct<strong>in</strong>g <strong>muscle</strong> <strong>activity</strong>around <strong>the</strong> scapula.In contrast to <strong>the</strong> expectations, <strong>the</strong> results of our<strong>in</strong>vestigation revealed no significant changes <strong>in</strong> EMG<strong>activity</strong> <strong>in</strong> <strong>the</strong> scapular <strong>muscle</strong>s based on <strong>the</strong>application of tape. Mor<strong>in</strong> et al. (1997) exam<strong>in</strong>ed<strong>the</strong> <strong><strong>in</strong>fluence</strong> of <strong>tap<strong>in</strong>g</strong> on upper and middle trapezius<strong>muscle</strong> <strong>activity</strong> dur<strong>in</strong>g an isometric contraction <strong>in</strong> <strong>the</strong>shoulder. Contrary to <strong>the</strong> results of our study, hefound a significant decrease <strong>in</strong> <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> <strong>the</strong>upper trapezius <strong>muscle</strong> with tape application, and an<strong>in</strong>crease <strong>in</strong> EMG <strong>activity</strong> of <strong>the</strong> middle trapezius part.However, look<strong>in</strong>g at <strong>the</strong> results of both studies, itmust be mentioned that <strong>in</strong> <strong>the</strong> study of Mor<strong>in</strong> et al.(1997) EMG measurements were performed dur<strong>in</strong>gisometric <strong>muscle</strong> contractions, which usually give amore stable EMG signal than dynamic contractions.The dynamic character of <strong>the</strong> movements performed<strong>in</strong> our study might give a less steady EMG signal.However, <strong>in</strong> view of <strong>the</strong> nature of <strong>in</strong>stabilityproblems and related <strong>in</strong>juries, dynamic movementsover a large range of motions are more functional,and hence more cl<strong>in</strong>ically relevant than isometriccontractions. In addition, <strong>in</strong> Mor<strong>in</strong>’s <strong>in</strong>vestigation,<strong>the</strong> serratus anterior and lower fibres of <strong>the</strong> trapezius,known to play an important role <strong>in</strong> <strong>the</strong> scapulothoracicstability and movement, were not <strong>in</strong>cluded. Twoissues regard<strong>in</strong>g our methods should be discussed: <strong>the</strong>use of surface electrodes to evaluate <strong>muscle</strong> <strong>activity</strong>and <strong>the</strong> use of maximal voluntary contraction as anormalization reference.The current state of surface electromyography isenigmatic. Although it provides many important anduseful applications, it has many limitations that mustbe considered (De Luca 1997). A major problemis <strong>the</strong> issue of <strong>the</strong> cross-talk when us<strong>in</strong>g surfaceelectrode <strong>in</strong> <strong>the</strong> shoulder region. However, <strong>in</strong> view of<strong>the</strong> nature of our <strong>in</strong>vestigation, <strong>in</strong> which <strong>the</strong> same<strong>muscle</strong> was exam<strong>in</strong>ed dur<strong>in</strong>g <strong>the</strong> same movementunder different circumstances, possible cross-talkrema<strong>in</strong>ed unchanged over <strong>the</strong> conditions, and <strong>the</strong>reforeprobably did not <strong><strong>in</strong>fluence</strong> our results. Moreover,<strong>in</strong>vestigat<strong>in</strong>g large <strong>muscle</strong> groups such as <strong>the</strong>trapezius <strong>muscle</strong>, surface electrodes do give a moreglobal evaluation of <strong>muscle</strong> <strong>activity</strong> than f<strong>in</strong>e wireelectrodes, which measure a ra<strong>the</strong>r small selection of<strong>muscle</strong> fibres. In addition, cross-talk is not likely <strong>in</strong>our sett<strong>in</strong>g s<strong>in</strong>ce W<strong>in</strong>ter et al. (1994) estimated that90% of a surface EMG signal has its orig<strong>in</strong> with<strong>in</strong>12-mm distance from an electrode pair. Accord<strong>in</strong>gto Jensen and Westgaard (1997), <strong>the</strong> depth of <strong>the</strong>suprasp<strong>in</strong>atus and levator scapulae <strong>muscle</strong>s suggeststhat cross-talk contributes a relative small fraction to<strong>the</strong> total EMG signal us<strong>in</strong>g surface electrodes on <strong>the</strong>upper trapezius <strong>muscle</strong>.# 2002 Elsevier Science Ltd. All rights reserved. Manual Therapy (2002) 7(3), 154–162
160 Manual TherapyAlthough normalization of EMG signal to MVCvalues is common <strong>in</strong> EMG studies, its reproducibilityand stability is often questioned (Yang & W<strong>in</strong>ter1983; Jensen et al. 1993; Aaras et al. 1996; Araujoet al. 2000). Some authors state that MVC is anunreliable measurement (Yang & W<strong>in</strong>ter 1983;Araujo et al. 2000), while o<strong>the</strong>rs concluded thatunder certa<strong>in</strong> conditions, <strong>in</strong> which methodologicalerrors <strong>in</strong>fluenc<strong>in</strong>g <strong>the</strong> recorded EMG signal from <strong>the</strong><strong>muscle</strong> are kept to a m<strong>in</strong>imum, normalization toMVC values gives reproducible results (Aaras et al.1996; Danneels et al. 2001a,b). In our <strong>in</strong>vestigation,we used guidel<strong>in</strong>es for EMG record<strong>in</strong>g dur<strong>in</strong>gmaximal voluntary contraction proposed by De Luca(1997).Conclud<strong>in</strong>g on <strong>the</strong> basis of our data that <strong>tap<strong>in</strong>g</strong> hasno effect on <strong>the</strong> scapulothoracic <strong>muscle</strong> <strong>activity</strong>would be premature. Possibly, <strong>tap<strong>in</strong>g</strong> may affecto<strong>the</strong>r parameters of neuromuscular control, such as<strong>the</strong> <strong>muscle</strong> reaction times. In recent literature, tim<strong>in</strong>gof <strong>muscle</strong> <strong>activity</strong> is often mentioned <strong>in</strong> a neuromuscularcontext. Lohrer et al. (1999) <strong>in</strong>vestigated <strong>the</strong>neuromuscular properties and functional aspects oftaped ankles. He found <strong>tap<strong>in</strong>g</strong> caused changes <strong>in</strong><strong>muscle</strong> latency times, <strong>in</strong> addition to mechanicalrestriction of movement. This was <strong>in</strong>terpreted as aproprioceptively activated effect of tape. In addition,<strong>the</strong> <strong><strong>in</strong>fluence</strong> of this tape on <strong>the</strong> biomechanicalbehaviour of <strong>the</strong> scapular position was not considered<strong>in</strong> this study.We must take <strong>in</strong>to account that <strong>the</strong> use of healthysubjects is a limitation to our study, and fur<strong>the</strong>rresearch should emphasize <strong>muscle</strong> recruitment patterns<strong>in</strong> patients with abnormal scapular k<strong>in</strong>ematics.O<strong>the</strong>r proprioceptive <strong><strong>in</strong>fluence</strong>s, such as cutaneousstimulation due to tape application, enhanced awarenessof shoulder girdle and upper trunk position, andsubjective parameters of comfort after tape application,may possibly expla<strong>in</strong> a positive effect of <strong>the</strong> tapeon functional shoulder performance.CONCLUSIONSTape is often used <strong>in</strong> functional rehabilitation of <strong>the</strong>shoulder patient. Although various <strong>tap<strong>in</strong>g</strong> techniquesare used <strong>in</strong> cl<strong>in</strong>ical practice, description of <strong>the</strong>seapplication methods and cl<strong>in</strong>ical studies evaluat<strong>in</strong>g<strong>the</strong> effects of tape are scarce.The purpose of our study was to <strong>in</strong>vestigate <strong>the</strong>effect of tape application over <strong>the</strong> trapezius <strong>muscle</strong> on<strong>the</strong> amount of <strong>electromyographic</strong> <strong>muscle</strong> <strong>activity</strong> <strong>in</strong><strong>the</strong> scapular <strong>muscle</strong>s <strong>in</strong> healthy, pa<strong>in</strong>-free shoulders.We hypo<strong>the</strong>sized that application of this particulartape would have a proprioceptive effect on <strong>muscle</strong>activation around <strong>the</strong> scapula, result<strong>in</strong>g <strong>in</strong> a change<strong>in</strong> <strong>in</strong>tensity of <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> <strong>the</strong> scapular <strong>muscle</strong>s.We found no significant differences <strong>in</strong> <strong>muscle</strong> <strong>activity</strong>Manual Therapy (2002) 7(3), 154–162<strong>in</strong> <strong>the</strong> trapezius and serratus anterior <strong>muscle</strong>, basedon <strong>the</strong> application of tape. This scapular techniqueapparently does not affect <strong>muscle</strong> function <strong>in</strong> normalpa<strong>in</strong>-free shoulders. The question arises if <strong>the</strong><strong>in</strong>tensity of EMG <strong>activity</strong>, is a representative parameterfor proprioceptive qualities of a <strong>muscle</strong>.Fur<strong>the</strong>r research is necessary to measure differentaspects of neuromuscular control, <strong>in</strong> order todeterm<strong>in</strong>e proprioceptive changes after <strong>the</strong> applicationof tape. Although we were unable to revealsignificant changes <strong>in</strong> <strong>muscle</strong> <strong>activity</strong> with <strong>the</strong>application of this tape, <strong>the</strong> use of <strong>the</strong> <strong>tap<strong>in</strong>g</strong>techniques <strong>in</strong> <strong>the</strong> cl<strong>in</strong>ical practice often results <strong>in</strong>enhanced subjective functional scapular stability.Future research is also needed to determ<strong>in</strong>e <strong>the</strong>neuromuscular mechanism of <strong>the</strong>se functional improvements<strong>in</strong> patients with scapular <strong>in</strong>stability.AcknowledgementsThe authors would like to thank Ms Sara Vandevelde and MsChristel Vangestel for <strong>the</strong>ir assistance <strong>in</strong> collect<strong>in</strong>g <strong>the</strong> data.ReferencesAaras A, Veierod MB, Larsen S, Ostergren R, Ro O 1996Reproducibility and stability of normalized EMGmeasurements on musculus trapezius. Ergonomics 39(2):171–185Anderson DL, Sanderson DJ, Hennig EM 1995 The role ofexternal non-rigid ankle brac<strong>in</strong>g <strong>in</strong> limit<strong>in</strong>g ankle <strong>in</strong>version.Cl<strong>in</strong>ical Journal of Sports Medic<strong>in</strong>e 5: 18–24Anderson K, Woitys EM, Loubert PV, Miller RE 1992 Abiomechanical evaluation of <strong>tap<strong>in</strong>g</strong> and brac<strong>in</strong>g <strong>in</strong> reduc<strong>in</strong>gknee jo<strong>in</strong>t translation and rotation. The American Journal ofSports Medic<strong>in</strong>e 20(4): 416–421Araujo RC, Duarte M, Amadio AC 2000 On <strong>the</strong> <strong>in</strong>ter- and <strong>in</strong>trasubjectsvariability of <strong>the</strong> <strong>electromyographic</strong> signal <strong>in</strong> isometriccontractions. Electromyography and Cl<strong>in</strong>ical Neurophysiology40(4): 225–229Arrayo JS, Hershon SJ, Bigliani LU 1997 Special considerations <strong>in</strong><strong>the</strong> athletic throw<strong>in</strong>g shoulder. Orthopedic Cl<strong>in</strong>ics of NorthAmerica 28(1): 69–78Basmajian JV, De Luca CJ 1985 Muscles Alive: Their FunctionsRevealed by Electromyography, 5th edn. Williams and Wilk<strong>in</strong>s,BaltimoreBennell KL, Goldie PA 1994 The differential effects of externalankle support on postural control. Journal of Orthopedic andSports Physical Therapy 20(6): 287–295Blev<strong>in</strong>s FT 1997 Rotator cuff pathology <strong>in</strong> athletes. SportsMedic<strong>in</strong>e 24(3): 205–220Bockrath K, Wooden C, Worrell T, Ingersoll CD, Farr J 1993Effects of patella <strong>tap<strong>in</strong>g</strong> on patella position and perceived pa<strong>in</strong>.Medic<strong>in</strong>e and Science <strong>in</strong> Sports and Exercise 25(9): 989–992Cools AM, Witvrouw EE, Declercq GA, Danneels LA, WillemsTM, Cambier DC, Voight ML 2002 Scapular <strong>muscle</strong>recruitment pattern: <strong>electromyographic</strong> response of <strong>the</strong>trapezius <strong>muscle</strong> to sudden arm movement before and after afatigu<strong>in</strong>g exercise. J Orthop Sports Phys Ther 32(5):221–229Danneels LA, Cagnie BJ, Cools AM, Vanderstraeten GG, CambierDC, Witvrouw EE, De Cuyper HJ 2001a Intra-operator and<strong>in</strong>ter-operator reliability of surface electromyography <strong>in</strong> <strong>the</strong>cl<strong>in</strong>ical evaluation of back <strong>muscle</strong>s. Manual Therapy 6(3):145–153Danneels LA, Vanderstraeten GG, Cambier DC, Witvrouw EE,Stevens VK, De Cuyper HJ 2001b A functional subdivision ofhip, abdom<strong>in</strong>al and back <strong>muscle</strong>s dur<strong>in</strong>g asymmetric lift<strong>in</strong>g.Sp<strong>in</strong>e 26(6): E114–E121# 2002 Elsevier Science Ltd. All rights reserved.
Tap<strong>in</strong>g and <strong>electromyographic</strong> <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> shoulders 161Davies GL, Dockoff-Hoffman S 1993 Neuromuscular test<strong>in</strong>g andrehabilitation of <strong>the</strong> shoulder complex. Journal of OrthopedicSports Physical <strong>the</strong>rapy 18(2): 210–219De Luca CJ 1997 The use of surface electromyography <strong>in</strong>biomechanics. Journal of Applied Biomechanics 13: 135–163Engström BK, Renström PA 1998 How can <strong>in</strong>juries be prevented<strong>in</strong> <strong>the</strong> world cup soccer athlete? Cl<strong>in</strong>ics <strong>in</strong> Sports Medic<strong>in</strong>e17(4): 755–768Feuerbach JW, Grab<strong>in</strong>er MD, Koh TJ, Weiker GG 1994 Effect ofan ankle orthosis and ankle ligament anaes<strong>the</strong>sia on ankle jo<strong>in</strong>tproprioception. The American Journal of Sports Medic<strong>in</strong>e22(2): 223–261Gilleard W, McConnell J, Parsons D 1998 The effect of patellar<strong>tap<strong>in</strong>g</strong> on <strong>the</strong> onset of vastus medialis obliquus and vastuslateralis <strong>muscle</strong> <strong>activity</strong> <strong>in</strong> persons with patellofemoral pa<strong>in</strong>.Physical Therapy 78(1): 25–31Glousman R, Jobe F, Tibone J, Moynes D, Antonelli D, Perry J1988 Dynamic <strong>electromyographic</strong> analysis of <strong>the</strong> throw<strong>in</strong>gshoulder with glenohumeral <strong>in</strong>stability. The Journal of Boneand Jo<strong>in</strong>t Surgery 70A(2): 220–226Greene TA, Wight CR 1990 A comparative support evaluationof three ankle orthoses before, dur<strong>in</strong>g and after exercise.Journal of Orthopedic and Sports Physical Therapy 11:453–466Gross MT, Batten AL, Lamm AL 1994 Comparison of Donjoyankle ligament protector and subtalar sl<strong>in</strong>g ankle <strong>tap<strong>in</strong>g</strong> <strong>in</strong>restrict<strong>in</strong>g foot and ankle motion before and after exercise.Journal of Orthopedic and Sports Physical Therapy 19(1):33–41Hancock RE, Hawk<strong>in</strong>s RJ 1996 Applications of electromyography<strong>in</strong> <strong>the</strong> throw<strong>in</strong>g shoulder. Cl<strong>in</strong>ical Orthopaedics and RelatedResearch 330: 84–97.Hall CM 1999 The shoulder girdle. In: Hall CM, Brody LT (eds)Therapeutic Exercise: Mov<strong>in</strong>g Toward Function. Lipp<strong>in</strong>cottWilliams and Wilk<strong>in</strong>s, PhiladelphiaHeit EJ, Lephart SM, Rozzi SL 1996 The effect of ankle brac<strong>in</strong>gand <strong>tap<strong>in</strong>g</strong> on jo<strong>in</strong>t position sense <strong>in</strong> <strong>the</strong> stable ankle. Journal ofSports Rehabilitation 5: 206–213Host HH 1995 Scapular <strong>tap<strong>in</strong>g</strong> <strong>in</strong> <strong>the</strong> treatment of anteriorshoulder imp<strong>in</strong>gement. Physical Therapy 75(9): 803–812Jensen C, Vasseljen O, Westgaard RH 1993 <strong>the</strong> <strong><strong>in</strong>fluence</strong> ofelectrode position on bipolar surface electromyogramrecord<strong>in</strong>gs of <strong>the</strong> upper trapezius <strong>muscle</strong>. European Journal ofApplied Physiology 67: 266–273Jensen C, Westgaard R 1997 Functional subdivision of <strong>the</strong> uppertrapezius <strong>muscle</strong> dur<strong>in</strong>g low-level activation. European Journalof Applied Physiology 76: 335–339Johnson G, Bogduk N, Nowitzke A, House D 1994 Anatomy andactions of <strong>the</strong> trapezius <strong>muscle</strong>. Cl<strong>in</strong>ical Biomechanics 9: 44–50Kamkar A, Irrgang JI, Whitney SL 1993 Non-operativemanagement of secondary imp<strong>in</strong>gement syndrome. Journal ofOrthopedic and Sports Physical Therapy 17(5): 212–224Karlsson J, Andreasson GO 1992 The effect of external anklesupport <strong>in</strong> chronic lateral ankle jo<strong>in</strong>t <strong>in</strong>stability: An<strong>electromyographic</strong> study. The American Journal of SportsMedic<strong>in</strong>e 20(3): 257–261Kelley MJ 1995 Anatomic and biomechanical rationale forrehabilitation of <strong>the</strong> athlete’s shoulder. Journal of SportsRehabilitation 4: 122–154Kelly BT, Kadrmas WR, Speer KP 1996 The manual <strong>muscle</strong>exam<strong>in</strong>ation for rotator cuff strength: An <strong>electromyographic</strong><strong>in</strong>vestigation. Journal of Orthopedic and Sports PhysicalTherapy 24(5): 581–588Kendall FP, Kendall EK 1983 Muscles, Test<strong>in</strong>g and Function.Williams and Wilk<strong>in</strong>s, BaltimoreKibler WB 1998 The role of <strong>the</strong> scapula <strong>in</strong> athletic shoulderfunction. The American Journal of Sports Medic<strong>in</strong>e 26(2):325–337Konradson L, Voight M, Hojsgaard C 1997 Ankle <strong>in</strong>version<strong>in</strong>juries: <strong>the</strong> role of <strong>the</strong> dynamic defence mechanism. TheAmerican Journal of Sports Medic<strong>in</strong>e 25(1): 54–58Kowall MG, Kolk G, Nuber GW, Cassisi JE, Stern SH 1996Patellar <strong>tap<strong>in</strong>g</strong> <strong>in</strong> <strong>the</strong> treatment of patellofemoral pa<strong>in</strong>:A prospective randomized study. The American Journal ofSports Medic<strong>in</strong>e 24(1): 61–65Larsen B, Andreansen E, Urfer A, Mickeslon MR, Newhouse KE1995 Patellar <strong>tap<strong>in</strong>g</strong>: A radiographic exam<strong>in</strong>ation of <strong>the</strong> medialglide technique. The American Journal of Sports Medic<strong>in</strong>e23(4): 465–470L<strong>in</strong>dman R, Eriksson A, Thornell L-E 1990 Fiber typecomposition of <strong>the</strong> human male trapezius <strong>muscle</strong>: Enzymehistochemicalcharacteristics. American Journal of Anatomy189: 236–244.L<strong>in</strong>dman R, Eriksson A, Thornell L-E 1991 Fiber typecomposition of <strong>the</strong> human female trapezius <strong>muscle</strong>: Enzymehistochemicalcharacteristics. American Journal of Anatomy190: 385–392.Lohrer H, Alt W, Gollhofer A 1999 Neuromuscular properties andfunctional aspects of taped ankles. The American Journal ofSports Medic<strong>in</strong>e 27(1): 69–75Ludewig PM, Cook TM, Nawocsenski DA 1996 Threedimensionalscapular orientation and <strong>muscle</strong> <strong>activity</strong> at selectedpositions of humeral elevation. Journal of Orthopedic andSports Physical Therapy 24(2): 57–65Lukasiewicz AC, McClure P, Mich<strong>in</strong>er L, Pratt N, Sennett B 1999Comparison of three dimensional scapular position andorientation between subjects with and without shoulderimp<strong>in</strong>gement. Journal of Orthopedic and Sports PhysicalTherapy 29(10): 574–586McCann PD, Wootten ME, Kadaba MP, Bigliani LU 1993A k<strong>in</strong>ematic and <strong>electromyographic</strong> study of shoulderrehabilitation exercises. Cl<strong>in</strong>ical Orthopedics and RelatedResearches 288: 179–188McConnell J. The Mc Connell approach to <strong>the</strong> problem shoulder.Tap<strong>in</strong>g: Inhibition of <strong>the</strong> upper trapezius <strong>muscle</strong>. 1999 CourseNotes, p 34.McCaw ST, Cerullo JF 1999 Prophylactic ankle stabilizers affectankle jo<strong>in</strong>t k<strong>in</strong>ematics dur<strong>in</strong>g drop land<strong>in</strong>gs. Medic<strong>in</strong>e andScience <strong>in</strong> Sports and Exercise 31(5): 702–707McMahon PJ, Jobe FW, P<strong>in</strong>k MM, Brault JR, Perry J 1996Comparative <strong>electromyographic</strong> analysis of shoulder <strong>muscle</strong>sdur<strong>in</strong>g planar motions: Anterior glenohumeral <strong>in</strong>stabilityversus normal. Journal of Shoulder and Elbow Surgery 5:118–123McQuade KJ, Dawson J, Smidt GL 1998 Scapulothoracic <strong>muscle</strong>fatigue associated with alterations <strong>in</strong> scapulohumeral rhythmk<strong>in</strong>ematics dur<strong>in</strong>g maximum resistive shoulder elevation.Journal of Orthopedic and Sports Physical Therapy 28(2):74–80Mor<strong>in</strong> GE, Tiberio D, Aust<strong>in</strong> G 1997 The effect of upper trapezius<strong>tap<strong>in</strong>g</strong> on <strong>electromyographic</strong> <strong>activity</strong> <strong>in</strong> <strong>the</strong> upper and middletrapezius region. Journal of Sports Rehabilitation 6: 309–319Mottram SL 1997 Dynamic stability of <strong>the</strong> scapula. ManualTherapy 2(3): 123–131P<strong>in</strong>k M, Perry J, Browne A, Scovacco ML, Kerrigan J 1991The normal shoulder dur<strong>in</strong>g free style swimm<strong>in</strong>g: An<strong>electromyographic</strong> and c<strong>in</strong>ematographic analysis oftwelve <strong>muscle</strong>s. The American Journal of Sports Medic<strong>in</strong>e 19:569–576P<strong>in</strong>k MM, Tibone JE 2000 The pa<strong>in</strong>ful shoulder <strong>in</strong> <strong>the</strong> swimm<strong>in</strong>gathlete. Orthopedic Cl<strong>in</strong>ics of North America 31(2): 247–261Robb<strong>in</strong>s S, Waked E 1998 Factors associated with ankle <strong>in</strong>juries:Preventive measures. Sports Medic<strong>in</strong>e 25(1): 63–72Rupp S, Bern<strong>in</strong>ger K, Hopf T 1995 Shoulder problems <strong>in</strong> high levelswimmersFimp<strong>in</strong>gement, anterior <strong>in</strong>stability, muscularimbalance? International Journal of Sports Medic<strong>in</strong>e 16:557–562Sahrmann SA 2002 Diagnosis and treatment of MovementImpairment Syndromes, 1st edn., chapter 5, pp 193–245,Mosby, St.LouisSchmitt L, Snyder-Mackler L 1999 Role of scapular stabilizers <strong>in</strong>etiology and treatment of imp<strong>in</strong>gement syndrome. Journal ofOrthopedic and Sports Physical Therapy 29(1): 31–38Shamus JL, Shamus EC 1997 A <strong>tap<strong>in</strong>g</strong> technique for <strong>the</strong> treatmentof acromioclavicular jo<strong>in</strong>t spra<strong>in</strong>s: A case study. Journal ofOrthopedic and Sports Physical Therapy 25(6): 390–394Somes S, Worrell TW, Corey B, Ingersol CD 1997 Effects ofpatellar <strong>tap<strong>in</strong>g</strong> on patellar position <strong>in</strong> <strong>the</strong> open and closedk<strong>in</strong>etic cha<strong>in</strong>: A prelim<strong>in</strong>ary study. Journal of SportsRehabilitation 6: 299–308Wadsworth DJ, Bullock-Saxton JE 1997 Recruitment patterns of<strong>the</strong> scapular rotator <strong>muscle</strong>s <strong>in</strong> freestyle swimmers withsubacromial imp<strong>in</strong>gement. International Journal of SportsMedic<strong>in</strong>e 18: 618–624# 2002 Elsevier Science Ltd. All rights reserved. Manual Therapy (2002) 7(3), 154–162
162 Manual TherapyWeiser WM, Lee TQ, McMaster WC 1999 Effects of simulatedscapular protraction on anterior glenohumeral stability. TheAmerican Journal of Sports Medic<strong>in</strong>e 27(6): 801–805Wilk KE, Arrigo C 1993 Current concepts <strong>in</strong> <strong>the</strong> rehabilitation of<strong>the</strong> athletic shoulder. Journal of Orthopedic and SportsPhysical Therapy 18(1): 365–378Wilkerson GB 1991 Comparative biomechanical effects of <strong>the</strong>standard method of ankle <strong>tap<strong>in</strong>g</strong> and a <strong>tap<strong>in</strong>g</strong> method designedto enhance subtalar stability. The American Journal of SportsMedic<strong>in</strong>e 19(6): 588–595W<strong>in</strong>ter DA, Fuglevand AJ, Archer SE 1994 Crosstalk <strong>in</strong> surfaceelectromyography: Theoretical and practical estimates. Journalof Electromyography and K<strong>in</strong>esiology 4: 15–26Yang JF, W<strong>in</strong>ter DA 1983 Electromyography reliability <strong>in</strong>maximal and submaximal isometric contractions. Archives ofPhysical Medic<strong>in</strong>e and Rehabilitation 64: 417–420Manual Therapy (2002) 7(3), 154–162# 2002 Elsevier Science Ltd. All rights reserved.