KAN Be Healthy (EPSDT) Screening Form
KAN Be Healthy (EPSDT) Screening Form
KAN Be Healthy (EPSDT) Screening Form

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
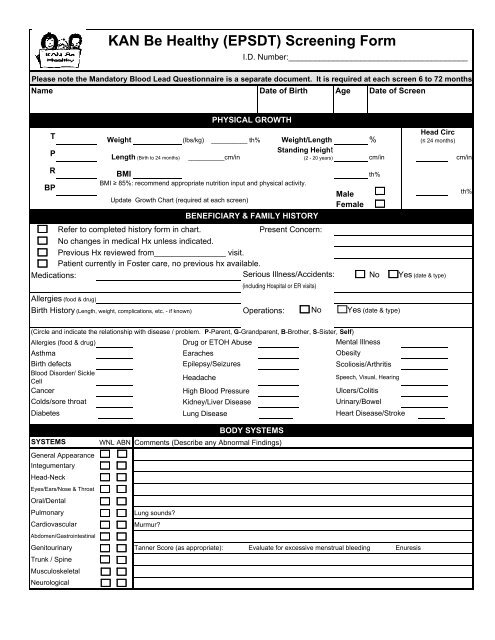
<strong>KAN</strong> <strong>Be</strong> <strong>Healthy</strong> (<strong>EPSDT</strong>) <strong>Screening</strong> <strong>Form</strong>I.D. Number:________________________________________Please note the Mandatory Blood Lead Questionnaire is a separate document. It is required at each screen 6 to 72 monthsName Date of Birth Age Date of ScreenTPPHYSICAL GROWTHHead CircWeight (lbs/kg) __________ th% Weight/Length %(≤ 24 months)Standing HeightLength (Birth to 24 months) __________cm/in(2 - 20 years) cm/in cm/inRBMIth%BMI ≥ 85%: recommend appropriate nutrition input and physical activity.BPMaleUpdate Growth Chart (required at each screen)FemaleBENEFICIARY & FAMILY HISTORYRefer to completed history form in chart.Present Concern:No changes in medical Hx unless indicated.Previous Hx reviewed from________________ visit.Patient currently in Foster care, no previous hx available.Medications: Serious Illness/Accidents: No Yes (date & type)(including Hospital or ER visits)Allergies (food & drug)Birth History (Length, weight, complications, etc. - if known) Operations: No Yes (date & type)th%(Circle and indicate the relationship with disease / problem. P-Parent, G-Grandparent, B-Brother, S-Sister, Self)Allergies (food & drug) Drug or ETOH Abuse Mental IllnessAsthma Earaches ObesityBirth defects Epilepsy/Seizures Scoliosis/ArthritisBlood Disorder/ SickleCellHeadacheSpeech, Visual, HearingCancer High Blood Pressure Ulcers/ColitisColds/sore throat Kidney/Liver Disease Urinary/BowelDiabetes Lung Disease Heart Disease/StrokeSYSTEMSGeneral AppearanceIntegumentaryHead-NeckEyes/Ears/Nose & ThroatOral/DentalPulmonaryCardiovascularAbdomen/GastrointestinalBODY SYSTEMSWNL ABN Comments (Describe any Abnormal Findings)Lung sounds?Murmur?Genitourinary Tanner Score (as appropriate): Evaluate for excessive menstrual bleeding EnuresisTrunk / SpineMusculoskeletalNeurological
Vision ScreenAges 0 to 3 yr - Corneal Light Reflex Present: Yes No Ages 3 thru 20:Ages 3 yr thru 20 - Bruckner Exam: Pass Refer.Distance Acuity - Near Acuity -All ages - Outer Inspection: Normal AbnormalTool used:___________________Tool used: ___________________Eye Tracking: Pass Refer ; PERRLA: Pass ReferScore: L____ R____ Both_______Score: L____ R____ Both_______Ocular Motility(strabismus/cross cover test):Pass Refer Last exam:_________ Further comments (see below)NUTRITIONPHYSICAL ACTIVITYWIC participant Biking Basketball play outsideReferred to WIC Skating Walking other sportsBreast Feeding <strong>Form</strong>ula How many hours screen time/Day? (i.e. TV, Games, PC)Amount & how often: 0-1 hr 1-2hr 3-5hrs 5+hrsNumber of Servings per dayBread/Cereal Dairy KBH participant currently pregnant? Yes NoFat/Sweet/Sugar Fruit If "yes", then complete following :Meat/<strong>Be</strong>an/Egg Vegetable 1. Prenatal Record initiated? Yes NoFluid Intake: water oz. Soda 2. On prenatal vitamins? Yes NoMilk oz. Juice 3. Referred for OB/GYN cares? Yes NoReferred to:LABORATORYIMMUNIZATIONSObtain CBC with automated differential in infants between 9-12 months. Obtain CBC with Copy of record in chart Needs (circle): Rotaautomated differential in males at age 15 and in females at menarche. Annual CBC's withCurrent HepB DTaP Fludiff are required depending on lifestyle/ health needs, please see Provider Manual. WasCBC obtained? Yes No Indicate further follow-up in Plan of Care.<strong>Be</strong>hind Hib IPV MMRDEVELOPMENTAL / EMOTIONAL Unknown MCV4 MPSV4 PCVPlease refer to KMAP Provider Manual for AAP recommended Developmental Tools. Requested from Parent Varicella HepA HPVChildren < 6 yrs. A completed developmental screening tool to include the screener'sReferred to VFC provider Other:interpretation and report regarding meeting developmental milestones. If furthertesting/intervention is required, please include in Plan of Care.DENTALChildren 6-21 yrs. A completed developmental screening tool to include the screener's Sees Dentist? Yes Nointerpretation and report or document all developmental/emotional observations foundbelow. Include further testing/intervention needs in Plan of Care.Last dental exam date: ____/_____/______# times brushes/day:Developmental Tool used:__________________________________________ Dental Referral (annually at a minimum 1-20yr)Sleep Habits Tired / overactive? Yes No ~ Fluoride Varnish? Yes NoDiscipline: Vocational concerns? HEARING SCREENPeer Interaction: Exercise Maintain in record completed paper hearing screens &Grade LevelAverage Marksreport or qualifying hearing screen procedure & report.Special Education: Special Needs: Age birth to 4, perform Risk Indicators for Hearing Loss andAny emotional or behavioral problems?Hearing Developmental Scales Pass ReferEmotional Observations:_________________________________________________ Hearing Health History >4: Pass Refer__________________________________________________________ Or Screen Procedure:_____________________HEALTH EDUCATION AND ANTICIPATORY GUIDANCECircle Those Reviewed/ Handouts Given1. <strong>Be</strong>havior/Discipline 5. Family Planning 9. Parenting 13. Self Breast Exam2. Oral /Dental 6. Immunizations 10. Safety/Poisons 14. Sexuality3. Development 7. Lifestyle 11. Substance Abuse 15. Exercise4. Physical Activity 8. Nutrition 12. Self Testicular Exam 16. Weapon Safety17. Other:_____________________________ _<strong>Screening</strong> Results:RESULTS/PLAN OF CARERecommended Return Date:Parent/Caregiver and/or PatientPlan/Referrals (dental, vision, hearing, dietary, etc):____________________ informed of KBH Screen findings andverbalizes understanding of findingsand recommendations. Yes NoParent/Caregiver and/or PatientSignature:_____________________<strong>Screening</strong> Providers Signature:Date: ________________________(Licensed Physician, ARNP, PA, or Registered Nurse credentialed to perform <strong>KAN</strong> <strong>Be</strong> <strong>Healthy</strong> screens) form revised 12/6/07
Mandatory Blood Lead <strong>Screening</strong> QuestionnaireTo be completed at each KBH Screen from 6 to 72 monthsDoes your child: (circle response received) DATE: (MM/DD/YYYY)1) Live in or visit a house or apartment built before 1960? (This couldinclude a day care center, preschool, the home of a baby-sitter or relative, etc.)YesNoYesNoYesNoYesNoYesNoYesNo2) Live in or regularly visit a house or apartment built before 1960with previous, ongoing or planned renovation or remodeling?YesNoYesNoYesNoYesNoYesNoYesNo3) Have a family member with an elevated blood lead level?YesNoYesNoYesNoYesNoYesNoYesNo4) Interact with an adult whose job or hobby involves exposure tolead? (Furniture refinishing, making stained glass, electronics, soldering, automotive repair,making fishing weights and lures, reloading shotgun shells and bullets, firing guns at a shootingrange, doing home repairs and remodeling, painting/stripping paint, antique/imported toys, and/ormaking pottery).YesNoYesNoYesNoYesNoYesNoYesNo5) Live near a lead smelter, battery plant or other lead industry?(Ammunition/explosives, auto repair/auto body, cable/wiring striping, splicing or production,ceramics, firing range, leaded glass factory, industrial machinery/equipment, jewelry manufactureror repair, lead mine, paint/pigment manufacturer, plumbing, radiator repair, salvage metal orbatteries, steel metalwork, or molten (foundry work).YesNoYesNoYesNoYesNoYesNoYesNo6) Use pottery, ceramic, or crystal wear for cooking, eating, ordrinking?YesNoYesNoYesNoYesNoYesNoYesNoOne positive response to the above questions requires a blood lead level test. Please,remember blood lead level tests are required at 12 and 24 months, regardless of thescore. Was blood drawn for a blood lead level test?YesNoYesNoYesNoYesNoYesNoYesNoInterviewing Staff InitialsStaff Signature:Patient Name: I.D. Number: :Revised 12/2007
Cuestionario Obligatorio para Examen de Plomo en la SangreDebe ser completado en cada examen de KBH de 6 a 72 mesesSu hijo: (circule la respuesta recibida) FECHA: (MM/DD/YYYY)1) ¿A vivido en o visitado una casa o apartamento construido antes del 1960? (Esto puede incluir una guardería,preschool, la casa de su niñera o un pariente, etc.)SíNoSíNoSíNoSíNoSíNoSíNo2) ¿A vivido en o visitado regularmente una casa o apartamento construido antes del 1960 que este, aya estado, ovaya estar bajo renovación o remodelación?SíNoSíNoSíNoSíNoSíNoSíNo3) ¿Tiene un pariente con un alto nivel de plomo en la sangre? SíSíSíSíSíSíNoNoNoNoNoNo4) ¿Tiene comunicación con un adulto que trabaje o que tenga un pasatiempo que involucre la exposición aplomo? (acabado de muebles, haciendo vidrio manchado, electrónicos, soldando, reparación automotriz, haciendopesas o señuelos para pescar, cargando casquillos o balas en una escopeta, disparando armas, haciendo reparos oremodelaciones, pintando/desmontando pintura, juguetes antiguos o importados, y/o haciendo cerámica).SíNoSíNoSíNoSíNoSíNoSíNo5) ¿A vivido cerca de un fundidor de plomo, planta de baterías u otra industria de plomo? (parque/explosivos,reparación de auto/exterior de auto, quitando o juntando cable/alambre, produciendo cables, cerámica, rango dedisparos, fabrica de vidrio plomado, maquinaria/equipo industrial, maquinaria o reparación de joyas, mina de plomo,fabricante de pintura/pigmento, plomería, reparación de radiador, yunque de metal o baterías, hierro o metal, o fundidorderretidoSíNoSíNoSíNoSíNoSíNoSíNo6) ¿Usa trastes cristalinos o de cerámica para cocinar, comer o beber? SíSíSíSíSíSíNoNoNoNoNoNoUna respuesta positiva a estas preguntas exige obtener el nivel de plomo en la sangre. Por favor, recuerde que elnivel de plomo en la sangre es obligatorio a los 12 y 24 meses, aunque las respuestas no sean positivas. ¿Seobtuvo el nivel de sangre?SíNoSíNoSíNoSíNoSíNoSíNoIniciales de Personal que dio la entrevistaFirma de Personal:PLEASE NOTE PROVIDERS ARE REQUIRED TO INTERPRET AND INITIATE CARE AS INDICATEDNombre del Paciente: Numero de ID: :Revisado 12/2007