collagen vascular disordersjuvenile idiopathic arthritisRecently, inflamed joints in patients who have JIAhave been shown to have high levels of IL-17–producingT cells; IL-17 induces the production of other interleukinsand matrix metalloproteinases that are all involvedin joint damage. The role of humoral immunity in JIApathogenesis is supported by the increased level of autoantibodies,such as antinuclear antibodies (ANAs) andimmunoglobulins, by complement activation, and by thepresence of circulating immune complexes. (5)Other possible factors that have been implicated in thepathogenesis of JIA include immunologic dysregulation,psychological stress, trauma, hormonal abnormalities, andinfectious triggers.Clinical FeaturesJIA is divided into seven subtypes defined by clinical featuresduring the first 6 months of disease. The InternationalLeague of Associations for Rheumatology classification ofJIA includes the following subtypes: (1) Systemic-onsetarthritis, (2) oligoarticular arthritis, (3) polyarticular RFpositivearthritis, (4) polyarticular RF-negative arthritis,(5) psoriatic arthritis, (6) Enthesitis-related arthritis, and(7) undifferentiated arthritis, or “other.” Each subtypevaries with respect to clinical presentation, pathogenesis,treatment outcomes, and prognosis. All subtypes of JIA,however, share common symptoms, such as morningstiffness or “gelling phenomenon” (stiffness after a jointremains in one position for a prolonged period) thatimproves throughout the day, limp, swollen joints, limitationof activities because of pain, and periods characterizedby disease remission interspersed with disease flares.There is no diagnostic test for JIA; therefore, othercauses of arthritis must be excluded carefully before thediagnosis is made.The rash in systemic JIA is described typically as an evanescent,salmon-colored macular rash that accompaniesfebrile periods (Fig 1). The rash generally is nonpruriticand occurs most commonly on the trunk and proximalextremities, including the axilla and inguinal areas. (2)Other extra-articular manifestations that can be seen insystemic JIA include hepatosplenomegaly, lymphadenopathy,pulmonary disease, such as interstitial fibrosis,and serositis, such as pericarditis. The febrile period andother systemic features may precede the onset of arthritisby weeks to months. A definite diagnosis of JIA, however,cannot be made until arthritis is detected on physical examination.(6)Laboratory abnormalities typically observed in systemicJIA include anemia, leukocytosis, thrombocytosis,elevated liver enzymes, and acute-phase reactants, such aserythrocyte sedimentation rate, C-reactive protein, andferritin. ANA titer is usually negative and is not helpfulin making the diagnosis.Complications of systemic JIA include infection fromimmunosuppressive therapy, growth disturbances, osteoporosis,cardiac disease, amyloidosis (rare in NorthAmerica compared with other parts of the world), andmacrophage-activation syndrome (MAS) (Table 3). MASoccurs in about 5% to 8% of children who have systemicJIA and is characterized by persistent fever, pancytopenia,hepatosplenomegaly, liver dysfunction, coagulopathy,and neurologic symptoms. Bone marrow examinationSystemic-Onset JIASystemic-onset JIA is distinct compared with the othersubtypes in that it is characterized by the presence ofhigh-spiking fevers of at least 2 weeks’ duration in additionto arthritis. The disease affects 10% to 15% ofchildren who have JIA, and tends to affect boys andgirls equally, with a peak age of onset between 1and 5 <strong>year</strong>s. Early in the disease course, patients canpresent with fatigue and anemia. The fever in systemicJIA is characterized by temperatures >39°C that occurdaily or twice daily, with a rapid return to baseline or belowbaseline (quotidian pattern). Fever spikes usually occur inthe late afternoon or evening. Children often appear illduring febrile periods and look well when the feversubsides.Figure 1. Salmon-colored rash in systemic juvenile idiopathicarthritis. (Courtesy of Charles H. Spencer [http://www.rheumatlas.org].)306 Pediatrics in Review Vol.33 No.7 July 2012Downloaded from http://pedsinreview.aappublications.org/ by Enrique Mendoza-Lopez on July 2, 2012
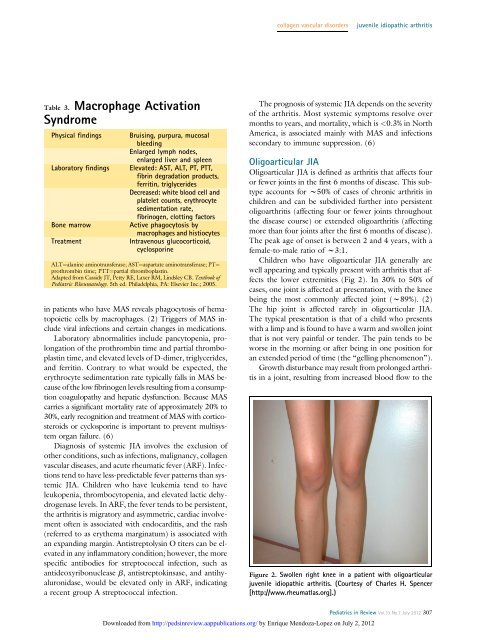
collagen vascular disordersjuvenile idiopathic arthritisTable 3. Macrophage ActivationSyndromePhysical findingsLaboratory findingsBone marrowTreatmentBruising, purpura, mucosalbleedingEnlarged lymph nodes,enlarged liver and spleenElevated: AST, ALT, PT, PTT,fibrin degradation products,ferritin, triglyceridesDecreased: white blood cell andplatelet counts, erythrocytesedimentation rate,fibrinogen, clotting factorsActive phagocytosis bymacrophages and histiocytesIntravenous glucocorticoid,cyclosporineALT¼alanine aminotransferase; AST¼aspartate aminotransferase; PT¼prothrombin time; PTT¼partial thromboplastin.Adapted from Cassidy JT, Petty RE, Laxer RM, Lindsley CB. Textbook ofPediatric Rheumatology. 5th ed. Philadelphia, PA: Elsevier Inc.; 2005.in patients who have MAS reveals phagocytosis of hematopoieticcells by macrophages. (2) Triggers of MAS includeviral infections and certain changes in medications.Laboratory abnormalities include pancytopenia, prolongationof the prothrombin time and partial thromboplastintime, and elevated levels of D-dimer, triglycerides,and ferritin. Contrary to what would be expected, theerythrocyte sedimentation rate typically falls in MAS becauseof the low fibrinogen levels resulting from a consumptioncoagulopathy and hepatic dysfunction. Because MAScarries a significant mortality rate of approximately 20% to30%, early recognition and treatment of MAS with corticosteroidsor cyclosporine is important to prevent multisystemorgan failure. (6)Diagnosis of systemic JIA involves the exclusion ofother conditions, such as infections, malignancy, collagenvascular diseases, and acute rheumatic fever (ARF). Infectionstend to have less-predictable fever patterns than systemicJIA. Children who have leukemia tend to haveleukopenia, thrombocytopenia, and elevated lactic dehydrogenaselevels. In ARF, the fever tends to be persistent,the arthritis is migratory and asymmetric, cardiac involvementoften is associated with endocarditis, and the rash(referred to as erythema marginatum) is associated withan expanding margin. <strong>An</strong>tistreptolysin O titers can be elevatedin any inflammatory condition; however, the morespecific antibodies for streptococcal infection, such asantideoxyribonuclease b, antistreptokinsase, and antihyaluronidase,would be elevated only in ARF, indicatinga recent group A streptococcal infection.The prognosis of systemic JIA depends on the severityof the arthritis. Most systemic symptoms resolve overmonths to <strong>year</strong>s, and mortality, which is