Changing the Future
Part of the Cure - American Partnership For Eosinophilic Disorders
Part of the Cure - American Partnership For Eosinophilic Disorders
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
President’s Pen<br />
<strong>Changing</strong> <strong>the</strong> <strong>Future</strong><br />
Wendy Book, MD<br />
APFED President<br />
A new year is upon us—a year full of<br />
hope and potential. With <strong>the</strong> New<br />
Year come opportunities to change<br />
<strong>the</strong> future of people with eosinophilic<br />
diseases. We at APFED have been<br />
working hard on your behalf to educate<br />
<strong>the</strong> public, <strong>the</strong> doctors, families,<br />
educators, industry and legislators on<br />
<strong>the</strong> importance of eosinophil associated<br />
diseases. We now have several<br />
clinical trials for patients with eosinophilic<br />
esophagitis and Hypereosinophilic<br />
syndrome. For a rare disease,<br />
<strong>the</strong>se initial steps are crucial, but<br />
more work needs to be done.<br />
Dedicated researchers, and <strong>the</strong> funding<br />
to support <strong>the</strong>ir ideas, are desperately<br />
needed. Sadly, federally funded<br />
studies of eosinophil associated diseases<br />
can be summarized in a few<br />
pages. That must change. The prevalence<br />
of eosinophil associated gastrointestinal<br />
disorders (EGID) has risen<br />
over <strong>the</strong> past decade, to a combined<br />
estimated prevalence of 1 in 1200<br />
today. Currently, diseases with<br />
prevalence similar to eosinophilic diseases<br />
receive many-fold more annual<br />
research funding, and have dedicated<br />
federal funding through <strong>the</strong> National<br />
Institutes of Health. The National<br />
Institutes of Health (NIH) is <strong>the</strong> primary<br />
federal agency for conducting<br />
and supporting medical research investigating<br />
<strong>the</strong> causes, treatments and<br />
cures for both common and rare diseases<br />
(http://www.nih.gov). The NIH<br />
attracts grant applications from <strong>the</strong><br />
top researchers in <strong>the</strong> country.<br />
What can we do? I am always in awe<br />
of <strong>the</strong> strength and enthusiasm within<br />
our community. That remarkable energy<br />
and drive led to <strong>the</strong> passing of<br />
HR 296 in 2007, declaring <strong>the</strong> 3 rd<br />
week of May National Eosinophil<br />
Awareness Week, followed by <strong>the</strong><br />
passage of four ICD-9-CM codes for<br />
eosinophilic gastrointestinal disorders<br />
in 2008.<br />
HR 296, <strong>the</strong> legislation which established<br />
a National Eosinophilic Awareness<br />
week, has language that specifically<br />
mentions <strong>the</strong> need for funding<br />
for improving methods of diagnosis<br />
and developing effective treatments.<br />
Dedicated<br />
researchers, and<br />
<strong>the</strong> funding to<br />
support <strong>the</strong>ir ideas,<br />
are desperately<br />
needed.<br />
In <strong>the</strong> two years that have passed<br />
since HR 296, <strong>the</strong> estimated prevalence<br />
of this debilitating group of diseases<br />
has dramatically risen, resulting<br />
in an even more pressing need for<br />
research funding.<br />
In recognition of this rapidly rising and<br />
poorly understood group of rare diseases,<br />
we ask that The National Institutes<br />
of Health convene a working<br />
group to develop a research agenda<br />
related to eosinophil associated diseases,<br />
and <strong>the</strong> related morbidity and<br />
mortality due to lack of diagnostic and<br />
treatment options. Funds are being<br />
raised in hopes of creating a partnership<br />
with NIH to fund research based<br />
on <strong>the</strong> working group recommendations.<br />
Our community will benefit from<br />
a NIH partnership with patient associations,<br />
such as APFED, and o<strong>the</strong>r appropriate<br />
health-care agencies, to develop<br />
education and research initiatives targeted<br />
to <strong>the</strong> life-long needs of those<br />
with eosinophil associated diseases.<br />
With our proposed partnership, we<br />
can increase our collective reach and<br />
research dollars.<br />
By increasing funding, we will attract<br />
high-quality researchers, initiate important<br />
research projects that might o<strong>the</strong>rwise<br />
not be funded, and stimulate<br />
much-needed interest in EGID research<br />
at <strong>the</strong> national level. Successful<br />
research projects will also increase<br />
public awareness, which will likely increase<br />
funding fur<strong>the</strong>r. Your contribution<br />
can lead to long-term exponential<br />
benefits to <strong>the</strong> community. Toge<strong>the</strong>r<br />
we can change <strong>the</strong> future for children<br />
and adults with eosinophilic diseases.<br />
To make this research initiative a reality,<br />
we must raise <strong>the</strong> necessary funding.<br />
A generous anonymous donor has<br />
contributed $50,000 and challenged<br />
our community to match those funds.<br />
Contribute today to HOPE on <strong>the</strong> Horizon,<br />
APFED’s dedicated research<br />
fund, and make a difference in <strong>the</strong> lives<br />
of those living with eosinophilic diseases.<br />
3
Medical Education<br />
Genetics<br />
of EE and EGID<br />
Genes are contained in chromosomes in<br />
<strong>the</strong> nucleus of all cells. Even though<br />
cells in different parts of <strong>the</strong> human<br />
body appear different from each o<strong>the</strong>r,<br />
<strong>the</strong>y all contain <strong>the</strong> same genes. The<br />
genes that are very active and important<br />
for cell function in some cell types may<br />
be completely silent in o<strong>the</strong>r cells.<br />
Genes contain <strong>the</strong> information that is<br />
essential for cell growth, development<br />
and function. That information is transcribed,<br />
or copied, from <strong>the</strong> DNA in <strong>the</strong><br />
genes to messenger RNA (mRNA),<br />
which <strong>the</strong>n brings that information<br />
from <strong>the</strong> nucleus into <strong>the</strong> cytoplasm,<br />
where <strong>the</strong> information is translated and<br />
specific proteins that perform specific<br />
functions are syn<strong>the</strong>sized. Knowledge<br />
of <strong>the</strong> genes that are active and also<br />
inactive in disease states is crucial to<br />
develop effective <strong>the</strong>rapies and ultimately<br />
to find cures.<br />
Recently, <strong>the</strong> gene expression profile of<br />
esophageal biopsies from patients with<br />
eosinophilic esophagitis (EE) was compared<br />
to biopsies from patients without<br />
EE. (1) Approximately 1% of all human<br />
genes were expressed more in esophageal<br />
tissue containing numerous<br />
eosinophils compared to tissue with<br />
few or no eosinophils. The gene that<br />
was most overexpressed in <strong>the</strong> inflamed<br />
biopsies was eotaxin-3, a substance that<br />
powerfully attracts eosinophils, from<br />
blood circulating in blood vessels, to<br />
enter tissue. The results concerning<br />
gene expression obtained from chip<br />
analysis were confirmed by detecting<br />
By Margaret Collins, MD<br />
increased amounts of both eotaxin-3<br />
mRNA and protein in EE biopsies. A<br />
particular type of microscopic analysis,<br />
in situ hybridization, demonstrated that<br />
<strong>the</strong> eotaxin-3 mRNA was increased in<br />
<strong>the</strong> epi<strong>the</strong>lial cells of <strong>the</strong> EE biopsies<br />
compared to controls. Additional research<br />
showed that interleukin-13 (IL-<br />
13) mRNA was greatly increased in<br />
biopsies from EE patients, and that<br />
epi<strong>the</strong>lial cells obtained from esophageal<br />
biopsies of EE patients that were<br />
cultured and grown in <strong>the</strong> lab produced<br />
large amounts of eotaxin-3 when stimulated<br />
with IL-13. (2) Those stimulated<br />
esophageal epi<strong>the</strong>lial cells had a gene<br />
expression profile very similar to that<br />
found on microarray analysis of esophageal<br />
biopsies from EE patients,<br />
strongly implicating IL-13 in <strong>the</strong> pathogenesis<br />
of EE. In addition to overexpression,<br />
a variation in a part of <strong>the</strong><br />
eotaxin-3 gene was significantly more<br />
common in EE patients, among those<br />
who had allergies as well as those who<br />
did not. (1) The gene expression profile<br />
identified in EE also did not vary<br />
with patient age or sex. (1) Thus, distinct<br />
gene alterations are present in esophageal<br />
tissue in patients who have EE;<br />
<strong>the</strong> alterations are independent of patient<br />
allergy status, age or sex; and at<br />
least one cytokine associated with<br />
atopy induces increased expression of<br />
genes in EE-derived esophageal epi<strong>the</strong>lial<br />
cells. Therefore, <strong>the</strong>rapy that reduces<br />
IL-13 content and/or interferes<br />
with IL-13 function may be helpful to<br />
treat EE. (2)<br />
In a number of families, more than one<br />
family member has EE. Based on estimates<br />
of <strong>the</strong> prevalence of EE in <strong>the</strong><br />
general population, and in siblings<br />
among EE patients, <strong>the</strong> estimated risk<br />
of a sibling of an EE patient to develop<br />
EE is significantly greater than for<br />
o<strong>the</strong>r common allergic diseases such as<br />
asthma. (3) EE is known to occur in<br />
twins. (4) The incidence in fraternal<br />
compared to identical twins may help to<br />
elucidate <strong>the</strong> genetic transmission of<br />
<strong>the</strong> disease: If <strong>the</strong> incidence of EE is<br />
significantly higher among identical<br />
compared to fraternal twins, that will<br />
even fur<strong>the</strong>r implicate genetics in <strong>the</strong><br />
development of <strong>the</strong> disease. In a recent<br />
study of families with multiple members<br />
who have EE, <strong>the</strong> clinical and histologic<br />
characteristics of 59 members<br />
of 26 families did not vary significantly<br />
from those of age- and sex-matched<br />
patients who were not known to have<br />
o<strong>the</strong>r family members with EE. (4) The<br />
gene expression profile of a subset of<br />
<strong>the</strong> biopsies also did not differ between<br />
familial and sporadic cases. These data<br />
suggest that <strong>the</strong>re is a common final<br />
pathway that results in <strong>the</strong> clinical and<br />
histologic expression of EE that is independent<br />
of family history, allergy, etc.<br />
There should <strong>the</strong>refore be <strong>the</strong>rapies that<br />
are effective for virtually all EE patients.<br />
EE occurs in patients who have diseases<br />
associated with known gene abnormalities,<br />
such as patients who have<br />
Rubinstein-Taybi Syndrome (RTS). (5)<br />
Many patients who have RTS have abnormalities<br />
of <strong>the</strong> CREB Binding Protein,<br />
or CBP, gene. That gene product<br />
interacts with a large number of o<strong>the</strong>r<br />
proteins. There isn’t any evidence currently<br />
that EE is more prevalent among<br />
patients who have a particular syndrome,<br />
including RTS. However, by<br />
analyzing tissue from patients who<br />
have syndromes with known genetic<br />
abnormalities we may fur<strong>the</strong>r advance<br />
our understanding of <strong>the</strong> genetic abnormalities<br />
in EE that directly participate<br />
in disease pathogenesis.<br />
There are virtually no publications<br />
concerning <strong>the</strong> genetics of o<strong>the</strong>r<br />
forms of EGID such as eosinophilic<br />
gastritis, etc. (6)<br />
DNA Continued on page 5<br />
4
Medical Education<br />
Pathology<br />
Pathologists’ evaluation of biopsies is an<br />
essential component of both <strong>the</strong> diagnosis<br />
of eosinophilic gastrointestinal disorders<br />
(EGIDS), and of <strong>the</strong> evaluation for<br />
response to <strong>the</strong>rapy. Pathology reports<br />
communicate pathology diagnoses based<br />
on review of <strong>the</strong> slides made from GI<br />
biopsies. The communication between<br />
pathologists and gastroenterologists may<br />
be supplemented by discussions at conferences,<br />
phone calls and emails. All<br />
pathology reports display <strong>the</strong> pathologist’s<br />
final diagnosis; a description—<br />
called gross description—of <strong>the</strong> number<br />
and size of <strong>the</strong> biopsy pieces from each<br />
part of <strong>the</strong> GI tract that were submitted<br />
to <strong>the</strong> pathology lab; and in some a microscopic<br />
description of <strong>the</strong> features of<br />
<strong>the</strong> tissue on <strong>the</strong> slides made from <strong>the</strong><br />
biopsies.<br />
Consensus concerning <strong>the</strong> diagnosis of<br />
EGIDS is generally lacking. The recommended<br />
diagnosis of eosinophilic<br />
esophagitis (EE), <strong>the</strong> most common form<br />
of EGIDS, is characteristic clinical signs<br />
and symptoms with an abnormal esophageal<br />
biopsy containing at least 15<br />
eosinophils in a high power field, in patients<br />
who have no or incomplete response<br />
to anti-gastroesophageal reflux<br />
disease (GERD) <strong>the</strong>rapy. (1) There are<br />
not currently recommendations for <strong>the</strong><br />
diagnosis of <strong>the</strong> o<strong>the</strong>r forms of EGIDS<br />
such as eosinophilic gastritis, etc. Although<br />
<strong>the</strong> recommendations to diagnose<br />
eosinophil<br />
gitis<br />
Of EGIDs<br />
high power field<br />
EE based on literature review and expert<br />
experience and opinion includes<br />
only an eosinophil count obtained from<br />
biopsy review, in fact most biopsies<br />
that show EE also show architectural<br />
abnormalities. Some pathologists require<br />
architectural abnormalities in<br />
o<strong>the</strong>r sites in <strong>the</strong> GI tract in addition to<br />
increased numbers of eosinophils to<br />
diagnose o<strong>the</strong>r forms of EGIDS such<br />
as eosinophilic gastritis. (2)<br />
Following is a glossary of terms that<br />
patients may find helpful to read pathology<br />
reports and discuss <strong>the</strong>ir disease<br />
with <strong>the</strong>ir clinicians.<br />
High power field: Pathologists see<br />
patterns in every biopsy. Pattern recognition<br />
is essential for proper biopsy<br />
interpretation. Therefore, pathologists<br />
initially evaluate slides under <strong>the</strong> microscope<br />
from afar to determine <strong>the</strong><br />
number of pieces of tissue that are on<br />
<strong>the</strong> slide, <strong>the</strong> pattern among <strong>the</strong> pieces,<br />
within each piece, etc. This degree of<br />
magnification is referred to as low<br />
power, and <strong>the</strong> circular area, or field,<br />
seen by <strong>the</strong> pathologist is referred to as<br />
a low power field. In order to view<br />
more detail in <strong>the</strong> tissue, pathologists<br />
use a different objective lens on <strong>the</strong><br />
microscope and see less of <strong>the</strong> total<br />
area on <strong>the</strong> slide, but greater detail of<br />
<strong>the</strong> smaller amount of tissue that is in<br />
<strong>the</strong> field <strong>the</strong>y see. This is referred to as<br />
high power magnification and <strong>the</strong> cir-<br />
mucosa<br />
epihelium<br />
6<br />
By Margaret Collins, MD<br />
Cincinnati Children’s Hospital Medical Center<br />
crypt<br />
cular area subtended on <strong>the</strong> slide is a<br />
high power field. Typically high power<br />
fields have a standard total magnification<br />
of 400X, although <strong>the</strong> actual area<br />
of <strong>the</strong> field varies among microscopes.<br />
Peak count: This is <strong>the</strong> number of<br />
eosinophils contained within one high<br />
power field. Ano<strong>the</strong>r means to quantitate<br />
eosinophils in biopsies is to count<br />
eosinophils in all <strong>the</strong> high power fields<br />
of all <strong>the</strong> pieces to generate a mean or<br />
average count, but that is not practical<br />
for daily work and is essentially a research<br />
tool. Pathologists survey <strong>the</strong><br />
biopsy pieces at low power magnification,<br />
identify <strong>the</strong> area with <strong>the</strong> densest<br />
inflammation, and generate a peak eosinophil<br />
count by counting esoinophils in<br />
that area. In esophageal biopsies, only<br />
eosinophils in <strong>the</strong> epi<strong>the</strong>lium are<br />
counted.<br />
Epi<strong>the</strong>lium: Epi<strong>the</strong>lium lines <strong>the</strong> inner<br />
surface of <strong>the</strong> tube that is <strong>the</strong> GI tract.<br />
Gastroenterologists see <strong>the</strong> epi<strong>the</strong>lium<br />
during endoscopy but cannot distinguish<br />
individual epi<strong>the</strong>lial cells.<br />
Epi<strong>the</strong>lial cells participate in multiple<br />
processes, including a barrier function<br />
that prevents bacteria and undigested<br />
food or foreign material from entering<br />
<strong>the</strong> body. The epi<strong>the</strong>lium that lines <strong>the</strong><br />
surface of <strong>the</strong> GI tract is called surface<br />
epi<strong>the</strong>lium. In <strong>the</strong> stomach and small<br />
and large intestines <strong>the</strong>re are numerous<br />
hyperplasia<br />
fibrosis<br />
esopha<br />
lamina propria
invaginations from <strong>the</strong> surface that are<br />
lined by epi<strong>the</strong>lial cells. In <strong>the</strong> stomach<br />
<strong>the</strong> invaginations are glands and <strong>the</strong> epi<strong>the</strong>lium<br />
lining <strong>the</strong> glands is glandular epi<strong>the</strong>lium.<br />
In <strong>the</strong> small and large intestines<br />
<strong>the</strong> invaginations form crypts and <strong>the</strong> epi<strong>the</strong>lium<br />
lining <strong>the</strong> crypts is known as<br />
crypt epi<strong>the</strong>lium.<br />
Basal layer: The epi<strong>the</strong>lial lining of <strong>the</strong><br />
esophagus is different from that of <strong>the</strong> rest<br />
of <strong>the</strong> GI tract. The epi<strong>the</strong>lium of <strong>the</strong><br />
esophagus consists of several layers but<br />
<strong>the</strong> surface and crypt epi<strong>the</strong>lium in <strong>the</strong><br />
rest of <strong>the</strong> GI tract mostly consists of one<br />
layer of cells. The esophagus is lined by<br />
squamous epi<strong>the</strong>lium that resembles <strong>the</strong><br />
lining of <strong>the</strong> mouth and also skin. The<br />
basal layer of <strong>the</strong> esophageal squamous<br />
epi<strong>the</strong>lium becomes thickened in EE, described<br />
as basal layer hyperplasia. This is<br />
a reactive and reversible change.<br />
Lamina propria: This is composed of<br />
fibrous tissue, blood vessels, and o<strong>the</strong>r<br />
types of tissue that provide structural support<br />
and perform o<strong>the</strong>r functions for <strong>the</strong><br />
surrounding tissue. Since <strong>the</strong> configuration<br />
of epi<strong>the</strong>lium is different in <strong>the</strong><br />
esophagus from <strong>the</strong> rest of <strong>the</strong> GI tract,<br />
<strong>the</strong> configuration of <strong>the</strong> lamina propria is<br />
also. In <strong>the</strong> esophagus, it forms a distinct<br />
layer below or outside of <strong>the</strong> basal layer<br />
of <strong>the</strong> epi<strong>the</strong>lium. The lamina propria<br />
forms periodic protrusions into <strong>the</strong> epi<strong>the</strong>lium<br />
called papillae that also contain<br />
blood vessels that supply oxygen to <strong>the</strong><br />
epi<strong>the</strong>lium. In <strong>the</strong> rest of <strong>the</strong> GI tract, <strong>the</strong><br />
lamina propria resides immediately below<br />
<strong>the</strong> single layer of surface epi<strong>the</strong>lium and<br />
surrounds <strong>the</strong> crypts. The differing configurations<br />
of epi<strong>the</strong>lium and distribution<br />
of lamina propria explains <strong>the</strong> fact that<br />
lamina propria is not present in some, or<br />
most, esophageal biopsies but is virtually<br />
always present in biopsies from <strong>the</strong> rest of<br />
<strong>the</strong> GI tract.<br />
Parietal cells: These are specialized<br />
epi<strong>the</strong>lial cells found in stomach glands<br />
that secrete acid. Anti-reflux medications<br />
block acid secretion and in response <strong>the</strong>se<br />
cells become enlarged and numerous, a<br />
finding that pathologists report as reactive<br />
change consistent with <strong>the</strong> use of PPIs, or<br />
parietal cell hypertrophy and hyperplasia.<br />
Villi: These are protrusions of <strong>the</strong> surface<br />
into <strong>the</strong> lumen of <strong>the</strong> small intestine and<br />
normally are found only in small intestine.<br />
All parts of <strong>the</strong> small intestine have<br />
<strong>the</strong>se, but villi vary in length and width<br />
somewhat among duodenum, jejunum<br />
and ileum. Villi enormously increase <strong>the</strong><br />
surface of <strong>the</strong> small intestine, increasing<br />
<strong>the</strong> area over which nutrients derived<br />
from food can be absorbed. Villi may<br />
become altered in numerous diseases.<br />
The most common alteration is blunting<br />
or a decrease in length, which is found in<br />
celiac disease but may also be seen with<br />
excessive numbers of eosinophils.<br />
Muscularis mucosa: This is a layer of<br />
muscle that separates <strong>the</strong> mucosa from<br />
<strong>the</strong> underlying submucosa. It may be<br />
present in biopsies from <strong>the</strong> GI tract depending<br />
on how deeply <strong>the</strong> biopsies<br />
were obtained. It is rarely seen in biopsies<br />
from <strong>the</strong> esophagus, but is more<br />
commonly present in biopsies from <strong>the</strong><br />
rest of <strong>the</strong> GI tract. One criterion for<br />
making a histologic diagnosis of EGIDS<br />
in sites o<strong>the</strong>r than <strong>the</strong> esophagus is finding<br />
eosinophils in <strong>the</strong> muscularis mucosa.<br />
Submucosa: This layer of <strong>the</strong> wall of<br />
<strong>the</strong> GI tract is below <strong>the</strong> muscularis mucosa<br />
and contains blood vessels and<br />
o<strong>the</strong>r structures. If any submucosa is<br />
seen in GI biopsies, it generally is only a<br />
small amount. Eosinophilic inflammation<br />
in <strong>the</strong> submucosa is also used as a<br />
criterion to help to diagnose EGIDS.<br />
Fibrosis: Fibrous tissue is a normal<br />
component of all parts of <strong>the</strong> body and<br />
helps to create and maintain <strong>the</strong> structure<br />
of various organs and tissues. Fibrosis<br />
means that <strong>the</strong>re is an excessive amount<br />
of fibrous tissue, equivalent to a scar.<br />
Lamina propria fibrosis is seen in esophageal<br />
biopsies showing EE, and may<br />
be reversible<br />
REFERENCES<br />
1. Furuta GT, Liacouras CA, Collins<br />
MH, Gupta SK, Justinich C, Putnam PE,<br />
Bonis P, Hassall E, Straumann A, Ro<strong>the</strong>nberg<br />
ME: Eosinophilic Esophagitis in<br />
Children and Adults: A Systematic Review<br />
and Consensus Recommendations<br />
for Diagnosis and Treatment. Sponsored<br />
by <strong>the</strong> American Gastroenterological<br />
Association (AGA) Institute and North<br />
American Society of Pediatric Gastroenterology,<br />
Hepatology, and Nutrition.<br />
Gastroenterology 133(4):1342-63, 2007.<br />
Collins MH: Histopathology Associated<br />
with Eosinophilic Gastrointestinal Diseases.<br />
Immunol Allergy Clin NA<br />
29:109-117<br />
7<br />
Medical Education<br />
Genomics of EE<br />
Antonella Cianferoni, MD, PhD<br />
APFED 2009 HOPE Grant Recipient<br />
EE is a global health disease now reported<br />
in all continents except Africa<br />
with an incidence of ~1:10,000. Patients<br />
with EE commonly report symptoms<br />
that include difficulty feeding,<br />
failure to thrive, vomiting, epigastric or<br />
chest pain, dysphagia and food impaction.<br />
EE patients are predominantly<br />
young males with a high rate of atopic<br />
disease and <strong>the</strong> diagnosis is made by<br />
endoscopy and biopsy finding of isolated<br />
eosinophils in <strong>the</strong> esophagus.<br />
Accumulating evidence suggests that<br />
EE has a strong familial association.<br />
Nearly 10% of parents of EE patients<br />
have a history of esophageal strictures<br />
and ~8% have biopsy proven EE and at<br />
least 27 multiplex families have been<br />
described to date. EE also exhibits a<br />
high sibling risk ratio compared with<br />
related atopic diseases such as asthma.<br />
While genetics is likely to have a large<br />
role in EE susceptibility, <strong>the</strong>re has been<br />
only one candidate gene identified to<br />
date, <strong>the</strong> eotaxin-3 gene. Eotaxin-3 is<br />
<strong>the</strong> most overexpressed gene in <strong>the</strong><br />
esophagus, based on genome wide expression<br />
profile analysis. However, <strong>the</strong><br />
disease-associated allele is only present<br />
in 14% of EE patients, suggesting that<br />
additional variants are to be found.<br />
In collaboration with Cincinnati Children’s<br />
Hospital Medical Center, and<br />
The Children’s Hospital of Philadelphia<br />
Center for Applied Genomics we have<br />
conducted a genome wide analysis<br />
study on children with EE aimed at<br />
identifying a gene variation that can<br />
make children susceptible to <strong>the</strong> disease.<br />
We genotyped approximately<br />
550,000 gene variation present in all<br />
<strong>the</strong> genome in 271 EE cases from Cincinnati<br />
Children’s Hospital Medical<br />
Center (CCHMC), and 180 EE patients<br />
and ~3100 controls from Children’s<br />
Hospital of Philadelphia (CHOP). We<br />
detected genome-wide association with<br />
variants on one gene that has been reported<br />
to favor allergic sensitization -<br />
TSLP.<br />
We are in <strong>the</strong> process of doing an extensive<br />
Genotyping/phenotyping analysis<br />
for <strong>the</strong> TSLP gene in <strong>the</strong> Children’s<br />
HOPE Continued on page 9
Eos Connection 2010<br />
2010<br />
Eos Connection<br />
The 8th Annual<br />
Patient Education<br />
Conference<br />
Presented by<br />
American Partnership For<br />
Eosinophilic Disorders<br />
in conjunction with<br />
The Children’s Hospital Denver<br />
and National Jewish Health<br />
July 16-18<br />
Denver, CO<br />
A ga<strong>the</strong>ring of some of <strong>the</strong> foremost<br />
experts in <strong>the</strong> field of EGIDs. Come to<br />
learn, to share, to meet o<strong>the</strong>r families<br />
affected by eosinophilic disorders.<br />
Eos Connection 2010<br />
APFED’s annual Patient Education Conference will take place in Denver,<br />
CO. Join us to learn from <strong>the</strong> experts, to meet o<strong>the</strong>r families affected by<br />
EGID and to make memories that will last a lifetime. More information<br />
and registration at www.apfed.org .<br />
Educational Sessions Include:<br />
Thursday, July 15, 2010 Optional<br />
Family Fun Day<br />
Denver Zoo (Optional, additional fee required)<br />
Friday July 16, 2010 Optional<br />
Fundraising Social at <strong>the</strong> Pavilion (optional, donation required)<br />
What’s New in Eos Research<br />
Entertainment<br />
Saturday July 17th<br />
Session 1-Overview of EGIDs<br />
What are EGIDs?<br />
EE– What it is and how we diagnose<br />
Endoscopy and Pathology of EE<br />
Session 2- Allergies and Treatment of EGIDs<br />
Allergies and EGIDs<br />
Treatment of EGIDs<br />
Session 3- Living Well<br />
Diets, Medications – How do I know which treatment is best?<br />
Six-food elimination diet: Practical tips<br />
Celebrating <strong>the</strong> Holidays<br />
Session 4- Eating, Nutrition and Coping with EGIDs<br />
Concurrent Sessions<br />
A. Feeding difficulties and EGIDs<br />
B. Teens only<br />
C. Nutrition: Living on an Elimination or Elemental Diet<br />
D. Coping with Chronic Illness<br />
Sunday July 18 th<br />
Session 5- Hope for Today<br />
2010 HOPE Grant lecture<br />
Living with chronic illness<br />
Parent-Child Panel<br />
Speakers Include:<br />
Dan Atkins MD<br />
Pediatric Allergist<br />
Nancy Creskoff–Maune<br />
Pediatric Occupational Therapist<br />
David Fleischer MD<br />
Pediatric Allergist<br />
Glenn Furuta MD<br />
Pediatric Gastroenterologist<br />
Angela Haas M.A.C<br />
Pediatric Speech Pathologist, Denver, CO<br />
Michelle L. Henry, MPH, RD<br />
Mary Klinnert PhD<br />
Pediatric Psychologist<br />
Jonathan Markowitz MD<br />
Pediatric Gastroenterologist<br />
Philip Putnam MD<br />
Pediatric Gastroenterologist<br />
Speakers and Sessions are Preliminary and Subject to Change<br />
8
EGID Myths<br />
Fact<br />
versus<br />
Fiction<br />
Eosinophilic Esophagitis: Fact or Fiction?<br />
Philip E Putnam, MD<br />
Pediatric Gastroenterologist, Cincinnati Children’s Hospital Medical Center<br />
The transfer of medical information<br />
from medical professionals to <strong>the</strong>ir patients<br />
is an essential part of patient care.<br />
The translation from medical terminology<br />
into language that is interpretable<br />
by individuals who may not have a<br />
medical background plays an important<br />
role in assuring that <strong>the</strong> patient understands<br />
<strong>the</strong> diagnosis, disease process,<br />
and plan for care. Arguably, <strong>the</strong> presentation,<br />
impact, success, and comprehension<br />
of that translation are variable.<br />
The information that is provided to patients<br />
and <strong>the</strong>ir families may undergo<br />
some transformation when it is repeated<br />
after <strong>the</strong> visit. The process is equivalent<br />
to <strong>the</strong> game of “Telephone”. Each time<br />
it is repeated to family or friends or<br />
over <strong>the</strong> internet, it is modified in some<br />
fa sh i on , such that th e fi nal<br />
‘understanding’ that develops may be<br />
accurate, mostly accurate, mostly inaccurate,<br />
or just plain fiction.<br />
If it’s repeated often enough and loud<br />
enough, fiction becomes perceived<br />
truth, but is fiction never<strong>the</strong>less. Fiction<br />
stated as truth, embellished for<br />
effect, attains mythologic status. In <strong>the</strong><br />
world of eosinophilic esophagitis, mythology<br />
abounds, and <strong>the</strong> following is<br />
an attempt to identify and demystify<br />
some of <strong>the</strong> statements that have attained<br />
mythologic status.<br />
Pathology Myths<br />
Myth: “Pathologists must count<br />
<strong>the</strong> eosinophils.” The reality is that<br />
pathologists look at slides as a profession,<br />
and are extraordinarily adept at<br />
identifying patterns of abnormality.<br />
Well-developed eosinophilic esophagitis<br />
is easy to recognize with little more<br />
than a glance at <strong>the</strong> slide because it is<br />
so different from normal esophagus.<br />
Counting <strong>the</strong> eosinophils to “prove it”<br />
is completely unnecessary. In borderline<br />
cases wherein <strong>the</strong> number of eosinophils<br />
is close to <strong>the</strong> threshold range<br />
(15-20 per high power field that is currently<br />
accepted as <strong>the</strong> minimum number<br />
needed to label <strong>the</strong> inflammatory<br />
process as “eosinophilic,”) it may be<br />
worthwhile to count.<br />
The actual number does not determine<br />
cause, severity, or treatment, so knowing<br />
whe<strong>the</strong>r <strong>the</strong> eosinophil count is 64<br />
or 164/hpf is not worth <strong>the</strong> time it takes<br />
to count. In addition, <strong>the</strong> eosinophil<br />
number varies from area to area within<br />
a biopsy and from biopsy specimen to<br />
biopsy specimen (even if <strong>the</strong>y are taken<br />
millimeters apart in <strong>the</strong> same patient),<br />
so <strong>the</strong> one number that is reported as<br />
<strong>the</strong> peak (highest concentration identified<br />
by inspection of all <strong>the</strong> available<br />
tissue) is seldom representative of <strong>the</strong><br />
entire set of high powered fields that<br />
are available.<br />
Being precise and counting eosinophils<br />
as part of a research project assures that<br />
<strong>the</strong> result is objective and not subjective,<br />
so <strong>the</strong> number of eosinophils/hpf<br />
will always be reported in a research<br />
article, but in clinical practice, <strong>the</strong> actual<br />
number is unimportant once <strong>the</strong><br />
peak has exceeded <strong>the</strong> threshold for<br />
diagnosis.<br />
Myth: “More eosinophils = more<br />
severe disease.” It is true that more<br />
eosinophils makes for a really impressive<br />
biopsy under <strong>the</strong> microscope, but<br />
<strong>the</strong> reality is that <strong>the</strong>re is a poor correlation<br />
between <strong>the</strong> degree of inflammation<br />
and what <strong>the</strong> patient feels (e.g.,<br />
pain or difficulty swallowing). The<br />
number does not determine <strong>the</strong> cause of<br />
<strong>the</strong> esophagitis, nor does it suggest one<br />
particular treatment over ano<strong>the</strong>r.<br />
Myth: “Routine biopsies are not<br />
sufficient to ‘see’ eosinophils, <strong>the</strong>y<br />
must do a special ‘test’ to find<br />
<strong>the</strong>m.” The reality is that eosinophils<br />
are easy to see on biopsy specimens processed<br />
in standard fashion in all pathology<br />
departments. “Eosinophilic” literally<br />
means “eosin-loving,” and <strong>the</strong>y are<br />
named that because <strong>the</strong>y take up a stain<br />
called eosin more than o<strong>the</strong>r cells. All<br />
biopsy specimens are stained with 2<br />
stains, hematoxylin and eosin (referred to<br />
commonly as H & E), because unstained<br />
tissue on a slide is virtually impossible to<br />
analyze. Various tissue and cells take up<br />
<strong>the</strong> hematoxylin (which is dark blue) or<br />
eosin (which is red) in unique patterns<br />
predictably, which <strong>the</strong>n allows <strong>the</strong> pathologist<br />
to identify <strong>the</strong> cell types in <strong>the</strong><br />
specimen. Eosinophils stand out from<br />
surrounding tissue because <strong>the</strong> tiny granules<br />
within <strong>the</strong>m stain intensely red with<br />
eosin.<br />
HOPE Continued from page 7<br />
Hospital of Philadelphia cohort of patients<br />
to see if such association is validated in a<br />
larger group and if it could be used as a<br />
blood biomarker in <strong>the</strong> future.<br />
Noel, R. J., and M. E. Ro<strong>the</strong>nberg. 2005. Eosinophilic<br />
esophagitis. Curr Opin Pediatr 17:690.<br />
Liacouras, C. A., J. M. Spergel, E. Ruchelli, R.<br />
Verma, M. Mascarenhas, E. Semeao, J. Flick, J.<br />
Kelly, T. Brown-Whitehorn, P. Mamula, and J. E.<br />
Markowitz. 2005. Eosinophilic esophagitis: a 10-<br />
year experience in 381 children. Clin Gastroenterol<br />
Hepatol 3:1198.<br />
Orenstein, S. R., T. M. Shalaby, C. Di Lorenzo, P.<br />
E. Putnam, L. Sigurdsson, H. Mousa, and S. A.<br />
Kocoshis. 2000. The spectrum of pediatric eosinophilic<br />
esophagitis beyond infancy: a clinical series<br />
of 30 children. Am J Gastroenterol 95:1422.<br />
Ro<strong>the</strong>nberg, M. E., A. Mishra, E. B. Brandt, and S.<br />
P. Hogan. 2001. Gastrointestinal eosinophils in<br />
health and disease. Adv Immunol 78:291.<br />
Blanchard, C., N. Wang, K. F. Stringer, A. Mishra,<br />
P. C. Fulkerson, J. P. Abonia, S. C. Jameson, C.<br />
Kirby, M. R. Konikoff, M. H. Collins, M. B. Cohen,<br />
R. Akers, S. P. Hogan, A.H. Assa'ad, P. E. Putnam,<br />
B. J. Aronow, and M. E. Ro<strong>the</strong>nberg. 2006. Eotaxin-<br />
3 and a uniquely conserved gene-expression profile<br />
in eosinophilic esophagitis. J Clin Invest 116:536<br />
9
Events<br />
Recent Events<br />
Run for a Cure<br />
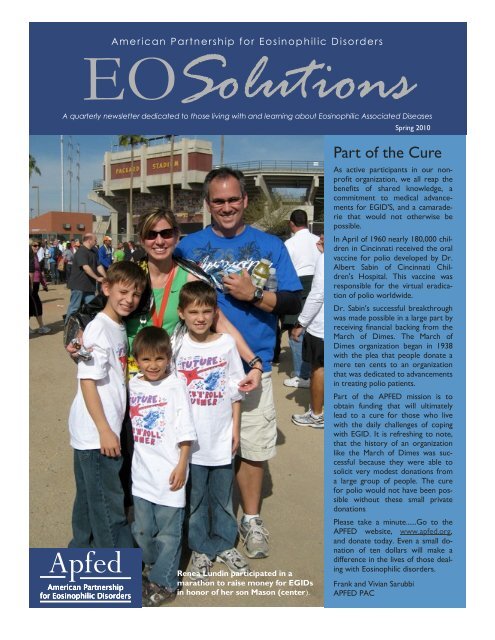
Congratulations to Renea Lundin for<br />
her finish in <strong>the</strong> PF Chang's Rock'n'Roll<br />
Marathon in Arizona on January 17th.<br />
Renea finished in 4 hrs, 55 minutes and<br />
raised over $1900.00 in donations by<br />
participating in this event.<br />
Dance-A-Thon<br />
Special Thanks to Megan Yanos and <strong>the</strong><br />
Mortar Board Honor Society of Findlay<br />
University for hosting a Dance-A-Thon<br />
on January 23rd. The event raised<br />
awareness of EGIDs and a great time<br />
was had by all who attended.<br />
Upcoming Events<br />
Remington Walls Golf Tournament<br />
May 1, 2010<br />
Wesley Chapel, Fl<br />
K.E.'s 2nd Annual Art Show and<br />
Bazaar to Benefit APFED.<br />
May 16, 2010<br />
Woodside, NY<br />
For more info on <strong>the</strong>se events, please<br />
visit APFED Fundraising page.<br />
Awareness Week<br />
National Awareness Walk<br />
May is not too far off. Spring wea<strong>the</strong>r,<br />
trees and flowers blooming, birds singing...and<br />
National Eosinophil Awareness<br />
Week!<br />
The third week of May is National<br />
Eosinophil Awareness Week dedicated<br />
to Eosinophilic Disorders. Get involved<br />
by planning an event in your<br />
area. Here are some great, easy ideas:<br />
• Pass out Dum-Dums or Smarties to<br />
classmates, with information about<br />
Eosinophilic Disorders.<br />
• Deliver DumDum bouquets to your<br />
doctors’ offices, to share with o<strong>the</strong>r<br />
patients.<br />
• Host a lemonade stand, bake sale,<br />
or car wash.<br />
• Do a letter or email campaign, asking<br />
friends and family to support<br />
APFED.<br />
Ano<strong>the</strong>r great way to raise awareness<br />
and support APFED is to participate in<br />
our Virtual National Eosinophil Awareness<br />
Walk. Grab your family, friends<br />
and neighbors and enjoy some quality<br />
time while raising awareness. Get toge<strong>the</strong>r<br />
your support group and meet<br />
up at a local park to Walk and socialize.<br />
Registration information and<br />
pledge forms will be available on <strong>the</strong><br />
website in March. If you are interested<br />
in hosting an event in your area, please<br />
c o n t a c t J u l i e S p r i n g e r a t<br />
julie@apfed.org.<br />
Julie A. Springer<br />
National Fundraising Coordinator<br />
407-340-2412 julie@apfed.org<br />
Fundraising Social<br />
A Fundraising Social will be held in conjunction<br />
with <strong>the</strong> Eos Connection 2010<br />
Patient Education Conference in Denver,<br />
CO, on July 16. An optional fundraising<br />
event, those families raising<br />
$100 or more for eosinophilic research<br />
are invited to attend. Those<br />
families raising $500 or more will receive<br />
a free gift store item.<br />
The whole family is invited to attend<br />
this event, and activities for children as<br />
well as entertainment will be provided.<br />
Fundraising forms will be available at<br />
www.apfed.org. Those interested in<br />
volunteering with organization of <strong>the</strong><br />
event or at <strong>the</strong> fundraiser may contact<br />
Melissa at mtierce@sbcglobal.net.<br />
Rare Disease Day<br />
APFED will partner with The National<br />
Organization for Rare Diseases<br />
(NORD) to celebrate <strong>the</strong> global observance<br />
of Rare Disease Day on<br />
February 28, 2010. We hope to<br />
raise awareness of EGIDs and understanding<br />
of <strong>the</strong> challenges faced by<br />
patients and <strong>the</strong>ir families.<br />
Last year, 39 states issues proclamations<br />
in support of Rare Disease Day.<br />
Requests for proclamations must come<br />
from residents of each state. Please<br />
consider writing a letter or sending an<br />
email to your governor requesting that<br />
he issue a proclamation for 2010. Sample<br />
letters and more information can<br />
be found at www.rarediseaseday.us.<br />
Support APFED<br />
There are three ways you can support<br />
APFED when making online purchases.<br />
Merchants will donate a portion<br />
of your purchase amount to<br />
APFED, with no additional cost to you.<br />
Amazon.com<br />
Use <strong>the</strong> links on <strong>the</strong> APFED website to<br />
shop through Amazon.com and a portion<br />
of all your purchases will benefit<br />
APFED. (You must use <strong>the</strong> links on<br />
<strong>the</strong> APFED website in order for your<br />
purchases to benefit APFED.)<br />
Buy for Charity<br />
Designate APFED as your charity<br />
of choice when shopping through Buy<br />
for Charity and a portion of your proceeds<br />
will benefit APFED. Buy for<br />
Charity provides you with a variety of<br />
s t o r e s , i n c l u d i n g B a r n e s<br />
& Nobles, Target, Toys R Us, Sears,<br />
Bath and Body, and many, many<br />
more. Link is available on <strong>the</strong> APFED<br />
website.<br />
iGive.com<br />
With over 757 merchants to choose<br />
from, you should find exactly what you<br />
are looking for with iGive.com. Register<br />
with iGive and select APFED as<br />
your Charity and a portion of all your<br />
purchases will benefit APFED.<br />
Link is available on <strong>the</strong> APFED website.<br />
eBay Donations<br />
A portion of your eBay sales can be<br />
designated to benefit APFED through<br />
Mission Fish. Sign up when you list<br />
your item for sale.<br />
APFED Merchandise<br />
Visit <strong>the</strong> Gift Store at www.apfed.org<br />
for unique merchandise that spreads<br />
awareness of eosinophilic disorders<br />
and supports research through its proceeds.<br />
A variety of items are available,<br />
including:<br />
Two-Year Eos Calendar<br />
Note Cards<br />
T-Shirts<br />
Restricted Diet Cookbook<br />
Hats<br />
Cooler Bag<br />
Educational Books<br />
10
Donations<br />
Turkey Schnitzel<br />
Donations<br />
Top 6 Allergen Free<br />
Sincere thanks to those making donation to APFED<br />
this quarter.<br />
In Memory of <strong>the</strong>se individuals:<br />
Ed Collins<br />
Emma Egreczky<br />
Ashley Fliger<br />
In honor of <strong>the</strong> following birthdays:<br />
Mat<strong>the</strong>w Markowitz<br />
Shannon O'Farrell<br />
Shmuel Rosenblatt<br />
In honor of:<br />
Maddox Bruening<br />
James DeLano<br />
David Dietz and Jane Kendall<br />
LeRoux Jooste<br />
Andrew Kern<br />
Ari Klosinski<br />
Jessica Lyn Miller<br />
Kyan Mwatha<br />
Meredith Naylor<br />
Ryan Piansky<br />
Oran C. Privett<br />
Gabby Provenzano<br />
Charles Remquest<br />
Edward Sarubbi<br />
Jeremy Sable<br />
Jacob Schwartz<br />
Sadie Sikora<br />
Amanda Smith<br />
Jason and Katrina Wesson<br />
Ryan Williams<br />
The Robby Smith Family<br />
The Family of Paula Eubanks and David Blume<br />
In honor of:<br />
Sarah Wisely through <strong>the</strong> LanConnect Golf Tournament<br />
Renea and Mason Lundin through Running for a Cause<br />
Ricky Springer through Racing for a Cause<br />
Megan Yanos and <strong>the</strong> Findley University Dance-A-Thon<br />
The Birch Wa<strong>the</strong>n Lenox School donation from Dress Down<br />
Day coordinated by APD member Andrew Frischling<br />
IDL Worldwide donation from <strong>the</strong>ir Coffee Cup Fund<br />
Many small people,<br />
who in many small places,<br />
do many small things,<br />
can alter <strong>the</strong> face of <strong>the</strong> world.<br />
-Published in Newsweek,<br />
from <strong>the</strong> Berlin Wall<br />
Thinly sliced turkey<br />
Brown rice flour<br />
Erewhon Crispy Brown rice cereal<br />
California Rice bran oil<br />
Rice milk<br />
Pulverize rice cereal in food processor until fine. Place in a<br />
bowl. Place flour and rice milk in separate bowls. Coat thinly<br />
sliced turkey fillets first with flour, <strong>the</strong>n rice milk, <strong>the</strong>n coat<br />
with rice crumb mixture. Place in a cast iron skillet <strong>the</strong>n coat<br />
with rice bran oil. Sautee for about 10 minutes each side.<br />
Options: substitute o<strong>the</strong>r safe meat<br />
Options: substitute fruit juice for rice milk<br />
Options: substitute o<strong>the</strong>r safe grain for rice<br />
APFED Membership / Donation Form<br />
Mission: American Partnership for Eosinophilic Disorders is a nonprofit<br />
organization dedicated to patients and <strong>the</strong>ir families coping<br />
with eosinophilic disorders. APFED strives to expand education,<br />
create awareness, and support research while promoting advocacy<br />
among its members.<br />
Annual Memberships now being accepted.<br />
Become a member online at www.apfed.org or mail this form.<br />
Name<br />
Personal Membership<br />
US $30<br />
Canadian $45<br />
International $55<br />
Address<br />
Country<br />
Phone<br />
Professional Membership<br />
US $100<br />
Canadian $125<br />
International $150<br />
Email *<br />
∗ Please note that APFED is going Green. In an effort to save money<br />
and <strong>the</strong> environment, <strong>the</strong> APFED newsletter will be delivered via<br />
email unless noted o<strong>the</strong>rwise.<br />
I want to receive email notifications from APFED<br />
I want to receive only newsletters via email from APFED<br />
Name and age of person with eosinophilic disorder:<br />
Donations: I would like to support APFED’s mission with a tax<br />
deductible donation of:<br />
$25 $50 $100 $250 $500 $1000<br />
O<strong>the</strong>r ______________<br />
Submitted by Viv Sarubbi<br />
Online donations welcome at www.apfed.org.<br />
Donations by check should be made payable to APFED at:<br />
APFED<br />
PO Box 29545<br />
Atlanta, GA 30359<br />
11
American Partnership<br />
for Eosinophilic Disorders<br />
PO Box 29545<br />
Atlanta, GA 30359<br />
www.apfed.org<br />
Phone: 713-493-7749<br />
E-mail: mail@apfed.org<br />
PLEASE FORWARD