- Page 1 and 2:
Credibility and Evidence Based Natu
- Page 3 and 4:
Aim of presentation • How far the
- Page 5 and 6:
The relationship between exposure t
- Page 7 and 8:
Conflict of interest (COI) The trad
- Page 9 and 10:
Candidate List of Categories of Fin
- Page 11 and 12:
Actual or reasonably perceived conf
- Page 13 and 14:
Physician relationships with the in
- Page 15 and 16:
Physician Relationships With The In
- Page 17 and 18:
Physician Relationships With The In
- Page 19 and 20:
Concerns Regarding Physician Relati
- Page 21 and 22:
Ethics And Compliance Payments to
- Page 23 and 24:
Ethics And Compliance Biopharmaceut
- Page 25 and 26:
Guidelines For Physician-Pharmaceut
- Page 27 and 28:
Financial Conflicts of Interest Che
- Page 29 and 30:
Financial Conflicts of Interest Che
- Page 31 and 32:
Financial Conflicts of Interest Che
- Page 33 and 34:
Drug surveillance and a real world
- Page 35 and 36:
Systems for assessment of postmarke
- Page 37 and 38:
Systems for assessment of postmarke
- Page 39 and 40:
Exposures to information from pharm
- Page 41 and 42:
Why we as prescribers still meet ph
- Page 43 and 44:
This is how each of the companies l
- Page 45 and 46:
After two decades of decimation, on
- Page 47 and 48:
Incretin Drugs Contribute Heavily t
- Page 49 and 50:
A Clouded Future For Big Pharma's B
- Page 51 and 52:
The largest health fraud settlement
- Page 53 and 54:
Use of drugs and its budgetary impl
- Page 55 and 56:
Key functions of drug regulatory ag
- Page 57 and 58:
Relationships Between Authors of Cl
- Page 59 and 60:
Conflicts (Dualities) of interest i
- Page 61 and 62:
Conflicts (Dualities) of interest a
- Page 63 and 64:
Cross-sectional survey of 192 autho
- Page 65 and 66:
Clinical practice guidelines for di
- Page 67 and 68:
Hierarchy of evidence-based medicin
- Page 69 and 70:
Criteria for assigning levels of ev
- Page 71 and 72:
Criteria for assigning grades of re
- Page 73 and 74:
Criteria for assigning levels of ev
- Page 75 and 76:
Meta-analysis may not consider COI
- Page 77 and 78: Financial disclosures in RCT’s* 5
- Page 79 and 80: Large trials that compared clinical
- Page 81 and 82: HBA1C targets suggested by differen
- Page 83 and 84: The goal for A1c may not be safely
- Page 85 and 86: A Patient- Centered Approach to Typ
- Page 87 and 88: According to subset analyses from a
- Page 89 and 90: Approach to management of hyperglyc
- Page 91 and 92: VA/DoD Clinical Practice Guideline
- Page 93 and 94: What is Algorithm (in guidelines)?
- Page 95 and 96: Types of medical practice setting
- Page 97 and 98: In summary why we need clinical pra
- Page 99 and 100: Dissemination and implementation an
- Page 101 and 102: Clinical Practice Guidelines (CPGs)
- Page 103 and 104: Clinical Practice Guidelines (CPGs)
- Page 105 and 106: Clinical Practice Guidelines (CPGs)
- Page 107 and 108: Personalized medicine Using a pers
- Page 109 and 110: Delaying the Onset of Type 2 Diabet
- Page 111 and 112: Intervention studies on the prevent
- Page 113 and 114: Management of hyperglycaemia in typ
- Page 115 and 116: General recommendations for managem
- Page 117 and 118: ADA-EASD Position Statement: Manage
- Page 119 and 120: Management of Hyperglycemia in T2DM
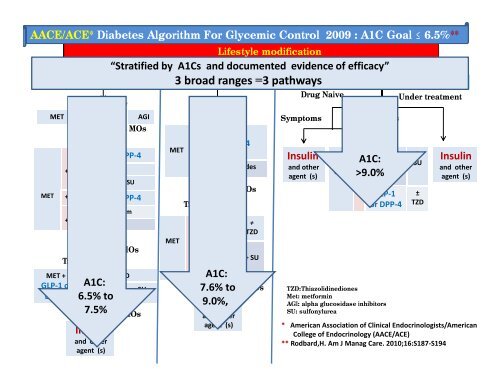
- Page 121 and 122: AACE/ACE* Diabetes Algorithm For Gl
- Page 123 and 124: Dr. Alashbal’ s observation regar
- Page 125 and 126: AACE/ACE* Diabetes Algorithm For Gl
- Page 127: AACE/ACE* Diabetes Algorithm For Gl
- Page 131 and 132: AACE/ACE* Diabetes Algorithm For Gl
- Page 133 and 134: Management of hyperglycemia in type
- Page 135 and 136: Relevant comments on ADA/EASD algor
- Page 137 and 138: ADA-EASD Position Statement: Manage
- Page 139 and 140: ADA-EASD Position Statement: Manage
- Page 141 and 142: ADA-EASD Position Statement: Manage
- Page 144 and 145: Sequential insulin strategies in ty
- Page 146 and 147: ADA/EASD position statement 2012 In
- Page 148 and 149: ADA/EASD position statement 2012 L
- Page 150 and 151: Individualization of therapy ADA/EA
- Page 152 and 153: NICE Type 2 diabetes algorithm for
- Page 154 and 155: Relevant comments on NICE algorithm
- Page 156 and 157: Relevant comments on SIGN algorithm
- Page 158 and 159: Relevant comments on DoD/VA algorit
- Page 160 and 161: Comparison of the ADA/EASD algorith
- Page 162 and 163: Comparison of the ADA/EASD algorith
- Page 164 and 165: Pharmacotherapy of Type 2 Diabetes
- Page 166 and 167: Maximum blood glucose lowering effe
- Page 168 and 169: Dose-response relationships of sulp
- Page 170 and 171: Hazard ratios (95% CI) for differen
- Page 172 and 173: "metformin, sulfonylureas, • •
- Page 174 and 175: Efficacy of monotherapy Drug Thiazo
- Page 176 and 177: Insulin is the most effective diabe
- Page 178 and 179:
Burdens of insulin therapy as a fir
- Page 180 and 181:
Why health care providers and patie
- Page 182 and 183:
ADA-EASD Position Statement: Manage
- Page 184 and 185:
The maximum period after which we m
- Page 186 and 187:
Doctor, patient, and system barrier
- Page 188 and 189:
Painful truth and big question why
- Page 190 and 191:
Report of Institute for Quality and
- Page 192 and 193:
Report of Institute for Quality and
- Page 194 and 195:
Insulin glargine vs. NPH insulin In
- Page 196 and 197:
Safety of Incretin-Based Therapies
- Page 198 and 199:
The use of incretin-based glucose-l
- Page 200 and 201:
Dr. Alashbal’ s observation regar
- Page 202 and 203:
Conclusions The pendulum is swingin
- Page 204 and 205:
Suggested seven deadly sins of drug
- Page 206 and 207:
Never be And the first, this sin is
- Page 208:
hank you Dr. Abdulameer Abdullah Al