Annual Conference
Your Clinical - National Association of Clinical Nurse Specialists
Your Clinical - National Association of Clinical Nurse Specialists
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Full Name _____________________________________________<br />
First Name for Badge _____________________________________<br />
Address _______________________________________________<br />
City, State, Zip _ _________________________________________<br />
Daytime Phone __________________________________________<br />
Employer ______________________________________________<br />
Position _______________________________________________<br />
E-mail** _______________________________________________<br />
**Required for registration confirmation<br />
My mailing and e-mail addresses and position can be listed on the<br />
conference participant list.<br />
❏ Yes ❏ No<br />
❏ Yes, I am willing to serve as a session moderator.<br />
Please contact me if my services are needed.<br />
If necessary, a copy of a purchase order<br />
can accompany the registration form.<br />
SCHEDULE SELECTION<br />
Please indicate which Concurrent Sessions you are planning to attend<br />
by checking one checkbox for each session series. You may change<br />
your selection at any time without notifying the conference office:<br />
Thursday, March 10:<br />
Sessions A: ❏ 1 ❏ 2 ❏ 3 ❏ 4 ❏ 5<br />
Sessions B: ❏ 1 ❏ 2 ❏ 3 ❏ 4 ❏ 5<br />
Sessions C: ❏ 1 ❏ 2 ❏ 3 ❏ 4 ❏ 5<br />
Friday, March 11:<br />
Sessions D: ❏ 1 ❏ 2 ❏ 3 ❏ 4 ❏ 5<br />
Sessions E: ❏ 1 ❏ 2 ❏ 3 ❏ 4 ❏ 5<br />
Saturday, March 12:<br />
Sessions F: ❏ 1 ❏ 2 ❏ 3 ❏ 4 ❏ 5<br />
Refund/Cancellation Policy: Requests must be submitted via email to<br />
info@nacns.org A $75 administrative fee will be deducted from the<br />
refund. NACNS reserves the right to cancel this program and return all<br />
fees in the event of insufficient enrollment. In the case of cancellation,<br />
NACNS cannot be responsible for other registrant expenses, including<br />
but not limited to, reimbursement of airline or other transportation<br />
fares, hotel or rental charges, deposits, or penalties. NO REFUND RE-<br />
QUESTS will be accepted after February 28, 2011.<br />
Mail to:<br />
NACNS<br />
100 North 20th Street, Suite 400<br />
Philadelphia, PA 19103<br />
Fax to: 215-564-2175<br />
Email to: info@nacns.org<br />
ONLINE REGISTRATION AVAILABLE<br />
AT WWW.NACNS.ORG<br />
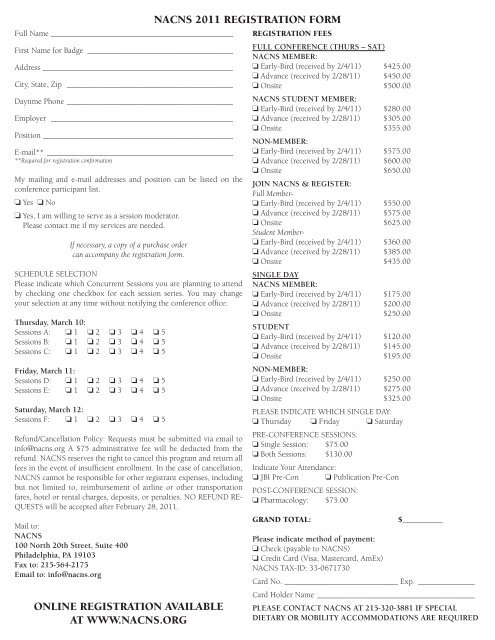
NACNS 2011 REGISTRATION FORM<br />
REGISTRATION FEES<br />
FULL CONFERENCE (THURS – SAT)<br />
NACNS MEMBER:<br />
❏ Early-Bird (received by 2/4/11) $425.00<br />
❏ Advance (received by 2/28/11) $450.00<br />
❏ Onsite $500.00<br />
NACNS STUDENT MEMBER:<br />
❏ Early-Bird (received by 2/4/11) $280.00<br />
❏ Advance (received by 2/28/11) $305.00<br />
❏ Onsite $355.00<br />
NON-MEMBER:<br />
❏ Early-Bird (received by 2/4/11) $575.00<br />
❏ Advance (received by 2/28/11) $600.00<br />
❏ Onsite $650.00<br />
JOIN NACNS & REGISTER:<br />
Full Member-<br />
❏ Early-Bird (received by 2/4/11) $550.00<br />
❏ Advance (received by 2/28/11) $575.00<br />
❏ Onsite $625.00<br />
Student Member-<br />
❏ Early-Bird (received by 2/4/11) $360.00<br />
❏ Advance (received by 2/28/11) $385.00<br />
❏ Onsite $435.00<br />
SINGLE DAY<br />
NACNS MEMBER:<br />
❏ Early-Bird (received by 2/4/11) $175.00<br />
❏ Advance (received by 2/28/11) $200.00<br />
❏ Onsite $250.00<br />
STUDENT<br />
❏ Early-Bird (received by 2/4/11) $120.00<br />
❏ Advance (received by 2/28/11) $145.00<br />
❏ Onsite $195.00<br />
NON-MEMBER:<br />
❏ Early-Bird (received by 2/4/11) $250.00<br />
❏ Advance (received by 2/28/11) $275.00<br />
❏ Onsite $325.00<br />
PLEASE INDICATE WHICH SINGLE DAY:<br />
❏ Thursday ❏ Friday ❏ Saturday<br />
PRE-CONFERENCE SESSIONS:<br />
❏ Single Session: $75.00<br />
❏ Both Sessions: $130.00<br />
Indicate Your Attendance:<br />
❏ JBI Pre-Con ❏ Publication Pre-Con<br />
POST-CONFERENCE SESSION:<br />
❏ Pharmacology: $75.00<br />
GRAND TOTAL:<br />
$__________<br />
Please indicate method of payment:<br />
❏ Check (payable to NACNS)<br />
❏ Credit Card (Visa, Mastercard, AmEx)<br />
NACNS TAX-ID: 33-0671730<br />
Card No._____________________________ Exp._ ______________<br />
Card Holder Name________________________________________<br />
PLEASE CONTACT NACNS AT 215-320-3881 IF SPECIAL<br />
DIETARY OR MOBILITY ACCOMMODATIONS ARE REQUIRED