

Front Panel Painting “LIFE” By William T Chua MD
FREE download - Stroke Society of the Philippines
FREE download - Stroke Society of the Philippines

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
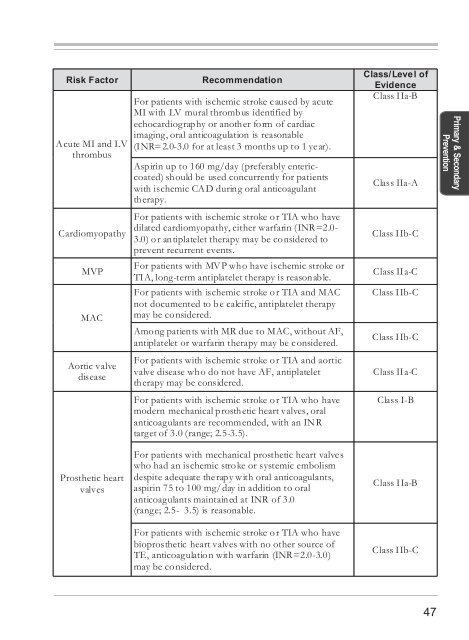
Risk Factor<br />
Acute MI and LV<br />
thrombus<br />
Cardiomyopathy<br />
MVP<br />
MAC<br />
Aortic valve<br />
disease<br />
Recommendation<br />
For patients with ischemic stroke caused by acute<br />
MI with LV mural thrombus identified by<br />
echocardiography or another form of cardiac<br />
imaging, oral anticoagulation is reasonable<br />
(INR=2.0-3.0 for at least 3 months up to 1 year).<br />
Aspirin up to 160 mg/day (preferably entericcoated)<br />
should be used concurrently for patients<br />
with ischemic CAD during oral anticoagulant<br />
therapy.<br />
For patients with ischemic stroke or TIA who have<br />
dilated cardiomyopathy, either warfarin (INR=2.0-<br />
3.0) or antiplatelet therapy may be considered to<br />
prevent recurrent events.<br />
For patients with MVP who have ischemic stroke or<br />
TIA, long-term antiplatelet therapy is reasonable.<br />
For patients with ischemic stroke or TIA and MAC<br />
not documented to be calcific, antiplatelet therapy<br />
may be considered.<br />
Among patients with MR due to MAC, without AF,<br />
antiplatelet or warfarin therapy may be considered.<br />
For patients with ischemic stroke or TIA and aortic<br />
valve disease who do not have AF, antiplatelet<br />
therapy may be considered.<br />
For patients with ischemic stroke or TIA who have<br />
modern mechanical prosthetic heart valves, oral<br />
anticoagulants are recommended, with an INR<br />
target of 3.0 (range; 2.5-3.5).<br />
Class/Level of<br />
Evidence<br />
Class IIa-B<br />
Class IIa-A<br />
Class IIb-C<br />
Class IIa-C<br />
Class IIb-C<br />
Class IIb-C<br />
Class IIa-C<br />
Class I-B<br />
Primary & Secondary<br />
Prevention<br />
Prosthetic heart<br />
valves<br />
For patients with mechanical prosthetic heart valves<br />
who had an ischemic stroke or systemic embolism<br />
despite adequate therapy with oral anticoagulants,<br />
aspirin 75 to 100 mg/day in addition to oral<br />
anticoagulants maintained at INR of 3.0<br />
(range; 2.5- 3.5) is reasonable.<br />
For patients with ischemic stroke or TIA who have<br />
bioprosthetic heart valves with no other source of<br />
TE, anticoagulation with warfarin (INR=2.0-3.0)<br />
may be considered.<br />
Class IIa-B<br />
Class IIb-C<br />
47
