

BULLETIN
CSQ-Bulletin92
CSQ-Bulletin92

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Page 36 | Bulletin 92 | July 2015<br />
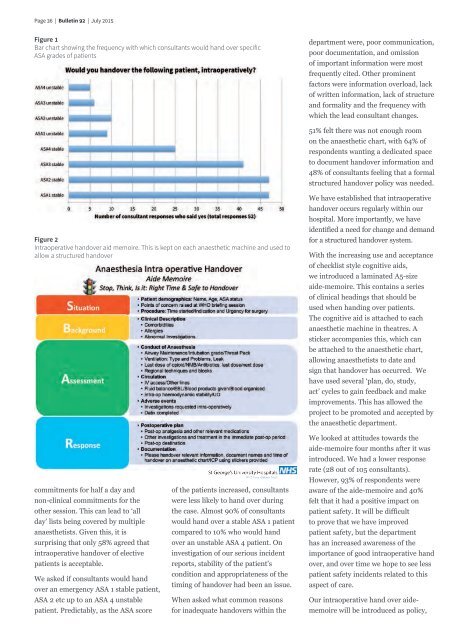
Figure 1<br />
Bar chart showing the frequency with which consultants would hand over specific<br />
ASA grades of patients<br />
department were, poor communication,<br />
poor documentation, and omission<br />
of important information were most<br />
frequently cited. Other prominent<br />
factors were information overload, lack<br />
of written information, lack of structure<br />
and formality and the frequency with<br />
which the lead consultant changes.<br />
51% felt there was not enough room<br />
on the anaesthetic chart, with 64% of<br />
respondents wanting a dedicated space<br />
to document handover information and<br />
48% of consultants feeling that a formal<br />
structured handover policy was needed.<br />
Figure 2<br />
Intraoperative handover aid memoire. This is kept on each anaesthetic machine and used to<br />
allow a structured handover<br />
We have established that intraoperative<br />
handover occurs regularly within our<br />
hospital. More importantly, we have<br />
identified a need for change and demand<br />
for a structured handover system.<br />
With the increasing use and acceptance<br />
of checklist style cognitive aids,<br />
we introduced a laminated A5-size<br />
aide-memoire. This contains a series<br />
of clinical headings that should be<br />
used when handing over patients.<br />
The cognitive aid is attached to each<br />
anaesthetic machine in theatres. A<br />
sticker accompanies this, which can<br />
be attached to the anaesthetic chart,<br />
allowing anaesthetists to date and<br />
sign that handover has occurred. We<br />
have used several ‘plan, do, study,<br />
act’ cycles to gain feedback and make<br />
improvements. This has allowed the<br />
project to be promoted and accepted by<br />
the anaesthetic department.<br />
commitments for half a day and<br />
non-clinical commitments for the<br />
other session. This can lead to ‘all<br />
day’ lists being covered by multiple<br />
anaesthetists. Given this, it is<br />
surprising that only 58% agreed that<br />
intraoperative handover of elective<br />
patients is acceptable.<br />
We asked if consultants would hand<br />
over an emergency ASA 1 stable patient,<br />
ASA 2 etc up to an ASA 4 unstable<br />
patient. Predictably, as the ASA score<br />
of the patients increased, consultants<br />
were less likely to hand over during<br />
the case. Almost 90% of consultants<br />
would hand over a stable ASA 1 patient<br />
compared to 10% who would hand<br />
over an unstable ASA 4 patient. On<br />
investigation of our serious incident<br />
reports, stability of the patient’s<br />
condition and appropriateness of the<br />
timing of handover had been an issue.<br />
When asked what common reasons<br />
for inadequate handovers within the<br />
We looked at attitudes towards the<br />
aide-memoire four months after it was<br />
introduced. We had a lower response<br />
rate (28 out of 105 consultants).<br />
However, 93% of respondents were<br />
aware of the aide-memoire and 40%<br />
felt that it had a positive impact on<br />
patient safety. It will be difficult<br />
to prove that we have improved<br />
patient safety, but the department<br />
has an increased awareness of the<br />
importance of good intraoperative hand<br />
over, and over time we hope to see less<br />
patient safety incidents related to this<br />
aspect of care.<br />
Our intraoperative hand over aidememoire<br />
will be introduced as policy,