

Lecture Notes Dermatology - Graham-Brown, Robin, Burns, Tony

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
88 Benign and malignant skin tumours<br />
Treatment<br />
Excision, biopsy and radiotherapy or, for superficial<br />
tumours, curettage, cryotherapy or photodynamic<br />
therapy; careful assessment of morphoeic<br />
tumours is needed — a technique known as ‘ microscopically<br />
controlled surgery ’ (Mohs’ surgery)<br />
may be helpful because it allows prospective<br />
delineation of tumour extent. It is particularly<br />
important to deal adequately with lesions around<br />
the eyes, nose and ears. The use of topical therapies<br />
for superficial types, notably imiquimod (a<br />
promoter of interferon - α ), has been pioneered<br />
more recently.<br />
Actinic or s olar k eratoses<br />
These are areas of dysplastic squamous epithelium<br />
without invasion, but actinic keratoses do<br />
have low - grade malignant potential and their<br />
presence indicates unstable epithelium.<br />
Clinical f eatures<br />
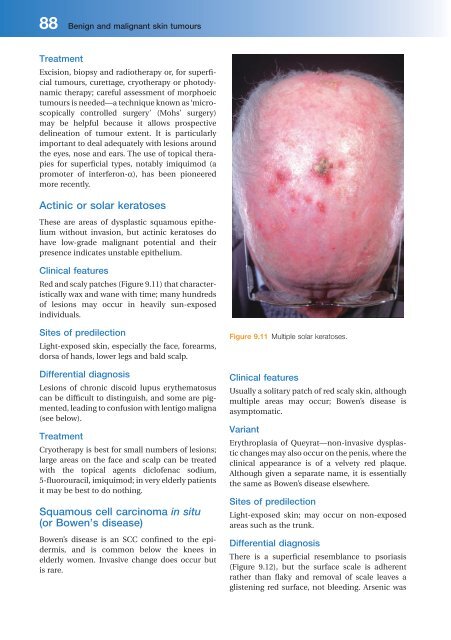
Red and scaly patches (Figure 9.11 ) that characteristically<br />
wax and wane with time; many hundreds<br />
of lesions may occur in heavily sun - exposed<br />
individuals.<br />
Sites of p redilection<br />
Light - exposed skin, especially the face, forearms,<br />
dorsa of hands, lower legs and bald scalp.<br />
Differential d iagnosis<br />
Lesions of chronic discoid lupus erythematosus<br />
can be difficult to distinguish, and some are pigmented,<br />
leading to confusion with lentigo maligna<br />
(see below).<br />
Treatment<br />
Cryotherapy is best for small numbers of lesions;<br />
large areas on the face and scalp can be treated<br />
with the topical agents diclofenac sodium,<br />
5 - fluorouracil, imiquimod; in very elderly patients<br />
it may be best to do nothing.<br />
Squamous c ell c arcinoma in situ<br />
(or Bowen ’ s d isease)<br />
Bowen ’ s disease is an SCC confined to the epidermis,<br />
and is common below the knees in<br />
elderly women. Invasive change does occur but<br />
is rare.<br />
Figure 9.11 Multiple solar keratoses.<br />
Clinical f eatures<br />
Usually a solitary patch of red scaly skin, although<br />
multiple areas may occur; Bowen ’ s disease is<br />
asymptomatic.<br />
Variant<br />
Erythroplasia of Queyrat —non-invasive dysplastic<br />
changes may also occur on the penis, where the<br />
clinical appearance is of a velvety red plaque.<br />
Although given a separate name, it is essentially<br />
the same as Bowen ’ s disease elsewhere.<br />
Sites of p redilection<br />
Light - exposed skin; may occur on non - exposed<br />
areas such as the trunk.<br />
Differential d iagnosis<br />
There is a superficial resemblance to psoriasis<br />
(Figure 9.12 ), but the surface scale is adherent<br />
rather than flaky and removal of scale leaves a<br />
glistening red surface, not bleeding. Arsenic was