

BAA MAGAZINE SUMMER 2017 DRAFT 4

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
FEATURE<br />
Single Sided<br />
Deafness: CROS<br />
Aid or BAHA?<br />
KERRY DOWNES<br />
Advanced Audiologist,<br />
St George’s Hospital<br />
Single Sided Deafness (SSD) affects around 9,000 new people<br />
each year in the UK. For many individuals, the condition can<br />
have a profound and debilitating effect on their lives. Sufferers<br />
experience difficulty picking up sounds from their deaf side,<br />
struggle in crowds and background noise and are unable to<br />
localise sounds. Whilst some losses are congenital or acquired<br />
in early childhood, most occur in adulthood and are of sudden<br />
onset. Adjusting to SSD can cause stress and anxiety, and<br />
impact hugely on a person’s well-being. In particular, individuals<br />
report withdrawal from group activities and feelings of isolation<br />
(Wie et al, 2010).<br />
There is some evidence to support the use of intratympanic<br />
steroids for idiopathic sudden SSD (Ferri et al, 2012), but results<br />
have varied widely and research on success rates are limited.<br />
Consequently, SSD remains a predominantly permanent and<br />
untreatable condition. Rehabilitation options include support<br />
groups and counselling, and provision of either Contralateral<br />
Routing of Sound (CROS) or Bone-Anchored Hearing Aids<br />
(BAHA).<br />
CROS/ BiCROS aids and BAHA can help to alleviate the<br />
difficulties caused by the head-shadow effect and provide relief<br />
to some of the difficulties SSD sufferers face (Faber et al, 2013).<br />
Most of the available research comparing the two amplification<br />
options is in regard to older, more cumbersome and cosmetically<br />
unappealing CROS aids with a wire around the back of the neck,<br />
and percutaneous connected abutments for BAHAs which are<br />
also less cosmetically appealing and can be prone to infection.<br />
With the improved technology and cosmetics of CROS aids, and<br />
the release of subcutaneous Cochlear BAHA attracts, this study<br />
aimed to provide an up to date and relevant insight into patient<br />
choice between the two amplification options.<br />
The research also intended to challenge some common<br />
assumptions; such as congenital SSD sufferers not opting for<br />
amplification and elderly patients avoiding BAHA due to the<br />
surgery involved. Factors which may influence the choice were<br />
also investigated; age, cause of deafness, acoustic neuroma<br />
surgery and high frequency thresholds in the hearing ear.<br />
Methods:<br />
30 individuals with SSD were referred to the BAHA service over<br />
the course of 16 months. All were offered back-to-back trials<br />
of wireless Phonak CROS/BiCROS aids (open-fit BTEs) and<br />
Cochlear BAHAs on soft-bands, for at least 2 weeks each. 27<br />
completed trials with both devices, 3 declined trials with BAHAs<br />
as they had no interest in pursuing this option.<br />
Following the trials, the patients attended follow-up<br />
appointments to give their feedback on the devices. Based on<br />
their experiences, the patients then made the decision whether<br />
to:<br />
- Proceed with BAHA and be added to the surgery<br />
waiting list (Group A)<br />
- Continue with the CROS aids (discharged from BAHA<br />
Service) (Group B)<br />
- Decline both options and return to being unaided<br />
(Group C)<br />
Data was collected retrospectively from patient records and<br />
mean averages were calculated. With the “age of patient”<br />
being the age at the time of data collection rather than at the<br />
time of the trials. The 3 patients who refused BAHA trials were<br />
included in Group B.<br />
Findings:<br />
90% of patients reported some level of benefit from either a<br />
CROS system or BAHA on soft-band, and only 3 people (10%)<br />
chose option C - to pursue neither device and return to being<br />
unaided. Of the 27 patients who reported benefit; 37% opted<br />
to be implanted with a BAHA (Group A), and 63% declined<br />
BAHA and chose to stick with their CROS aids (Group B).<br />
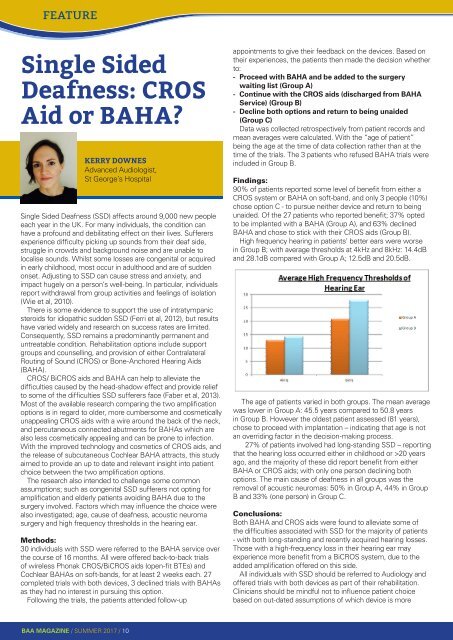
High frequency hearing in patients’ better ears were worse<br />
in Group B; with average thresholds at 4kHz and 8kHz: 14.4dB<br />
and 28.1dB compared with Group A; 12.5dB and 20.5dB.<br />
The age of patients varied in both groups. The mean average<br />
was lower in Group A: 45.5 years compared to 50.8 years<br />
in Group B. However the oldest patient assessed (81 years),<br />
chose to proceed with implantation – indicating that age is not<br />
an overriding factor in the decision-making process.<br />
27% of patients involved had long-standing SSD – reporting<br />
that the hearing loss occurred either in childhood or >20 years<br />
ago, and the majority of these did report benefit from either<br />
BAHA or CROS aids; with only one person declining both<br />
options. The main cause of deafness in all groups was the<br />
removal of acoustic neuromas: 50% in Group A, 44% in Group<br />
B and 33% (one person) in Group C.<br />
Conclusions:<br />
Both BAHA and CROS aids were found to alleviate some of<br />
the difficulties associated with SSD for the majority of patients<br />
- with both long-standing and recently acquired hearing losses.<br />
Those with a high-frequency loss in their hearing ear may<br />
experience more benefit from a BiCROS system, due to the<br />
added amplification offered on this side.<br />
All individuals with SSD should be referred to Audiology and<br />
offered trials with both devices as part of their rehabilitation.<br />
Clinicians should be mindful not to influence patient choice<br />
based on out-dated assumptions of which device is more<br />
<strong>BAA</strong> <strong>MAGAZINE</strong> / <strong>SUMMER</strong> <strong>2017</strong> / 10
