Innovations in mesh kit technology for vaginal wall prolapse - OBG ...
Innovations in mesh kit technology for vaginal wall prolapse - OBG ...
Innovations in mesh kit technology for vaginal wall prolapse - OBG ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Innovations</strong> <strong>in</strong> <strong>mesh</strong> <strong>kit</strong> <strong>technology</strong> <strong>for</strong> vag<strong>in</strong>al <strong>wall</strong> <strong>prolapse</strong><br />
Hydrodissection<br />
aids <strong>in</strong> reduc<strong>in</strong>g<br />
complications.<br />
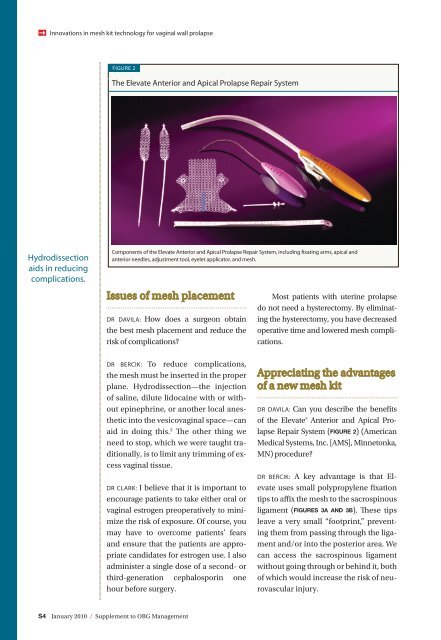
FIGURE 2<br />
The Elevate Anterior and Apical Prolapse Repair System<br />
Components of the Elevate Anterior and Apical Prolapse Repair System, <strong>in</strong>clud<strong>in</strong>g fixat<strong>in</strong>g arms, apical and<br />
anterior needles, adjustment tool, eyelet applicator, and <strong>mesh</strong>.<br />
Issues of <strong>mesh</strong> placement<br />
DR DAVILA: How does a surgeon obta<strong>in</strong><br />
the best <strong>mesh</strong> placement and reduce the<br />
risk of complications?<br />
DR BERCIK: To reduce complications,<br />
the <strong>mesh</strong> must be <strong>in</strong>serted <strong>in</strong> the proper<br />
plane. Hydrodissection—the <strong>in</strong>jection<br />
of sal<strong>in</strong>e, dilute lidoca<strong>in</strong>e with or without<br />
ep<strong>in</strong>ephr<strong>in</strong>e, or another local anesthetic<br />
<strong>in</strong>to the vesicovag<strong>in</strong>al space—can<br />
aid <strong>in</strong> do<strong>in</strong>g this. 3 The other th<strong>in</strong>g we<br />
need to stop, which we were taught traditionally,<br />
is to limit any trimm<strong>in</strong>g of excess<br />
vag<strong>in</strong>al tissue.<br />
DR CLARK: I believe that it is important to<br />
encourage patients to take either oral or<br />
vag<strong>in</strong>al estrogen preoperatively to m<strong>in</strong>imize<br />
the risk of exposure. Of course, you<br />
may have to overcome patients’ fears<br />
and ensure that the patients are appropriate<br />
candidates <strong>for</strong> estrogen use. I also<br />
adm<strong>in</strong>ister a s<strong>in</strong>gle dose of a second- or<br />
third-generation cephalospor<strong>in</strong> one<br />
hour be<strong>for</strong>e surgery.<br />
S4 January 2010 / Supplement to <strong>OBG</strong> Management<br />
Most patients with uter<strong>in</strong>e <strong>prolapse</strong><br />
do not need a hysterectomy. By elim<strong>in</strong>at<strong>in</strong>g<br />
the hysterectomy, you have decreased<br />
operative time and lowered <strong>mesh</strong> complications.<br />
Appreciat<strong>in</strong>g the advantages<br />
of a new <strong>mesh</strong> <strong>kit</strong><br />
DR DAVILA: Can you describe the benefits<br />
of the Elevate® Anterior and Apical Prolapse<br />
Repair System (FIGURE 2) (American<br />
Medical Systems, Inc. [AMS], M<strong>in</strong>netonka,<br />
MN) procedure?<br />
DR BERCIK: A key advantage is that Elevate<br />
uses small polypropylene fixation<br />
tips to affix the <strong>mesh</strong> to the sacrosp<strong>in</strong>ous<br />
ligament (FIGURES 3A AND 3B). These tips<br />
leave a very small “footpr<strong>in</strong>t,” prevent<strong>in</strong>g<br />
them from pass<strong>in</strong>g through the ligament<br />
and/or <strong>in</strong>to the posterior area. We<br />
can access the sacrosp<strong>in</strong>ous ligament<br />
without go<strong>in</strong>g through or beh<strong>in</strong>d it, both<br />
of which would <strong>in</strong>crease the risk of neurovascular<br />
<strong>in</strong>jury.