Volume 3, Issue 5 - Midwest Orthopaedics at Rush
Volume 3, Issue 5 - Midwest Orthopaedics at Rush
Volume 3, Issue 5 - Midwest Orthopaedics at Rush

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
of either an open or percutaneous Achilles<br />
lengthening produces more consistent<br />
outcomes, with improved ankle dorsiflexion<br />
and gre<strong>at</strong>er parental s<strong>at</strong>isfaction 11 .<br />
Stricker and Angulo 12 showed th<strong>at</strong> children<br />
tre<strong>at</strong>ed initially with surgical intervention<br />
had better results with respect to restor<strong>at</strong>ion<br />
of ankle dorsiflexion and parental<br />
s<strong>at</strong>isfaction, and th<strong>at</strong> cast and brace tre<strong>at</strong>ment<br />
offered little long-term improvement<br />
compared with untre<strong>at</strong>ed ITW. Hall et. al. 6<br />
performed tendo Achilles lengthenings on<br />
a group of p<strong>at</strong>ients who showed no improvement<br />
after six months to two years<br />
of observ<strong>at</strong>ion. They showed th<strong>at</strong>, when<br />
tre<strong>at</strong>ed surgically, the children exhibited<br />
normal passive and active dorsiflexion<br />
with a heel-toe gait p<strong>at</strong>tern, except for<br />
occasional toe walking in older children.<br />
Both percutaneous and open techniques<br />
have been used for tendo Achilles lengthening.<br />
P<strong>at</strong>ients are placed in below-the-knee<br />
weightbearing casts for four weeks and are<br />
allowed to bear weight immedi<strong>at</strong>ely. During<br />
the four-week period, they particip<strong>at</strong>e in<br />
physical therapy for gait training. Since they<br />
have likely toe walked since ambul<strong>at</strong>ion<br />
began, p<strong>at</strong>ients need to be retrained to walk.<br />
Physical therapy should continue after the<br />
casts are removed, and it is beneficial th<strong>at</strong><br />
Bibliography<br />
1. Brouwer B, davidson LK, Olney SJ. Serial casting in idiop<strong>at</strong>hic<br />
toe-walkers and children with spastic cerebral palsy.<br />
J Pedi<strong>at</strong>r orthop 2000;20:221- .<br />
2. Caselli MA, Rzonca eC, Lue By. habitual toe walking: evalu<strong>at</strong>ion<br />
and approach to tre<strong>at</strong>ment. clin Podi<strong>at</strong>r Med surg<br />
1 ; : - .<br />
. deLuca pA. the musculoskeletal management of children<br />
with cerebral palsy. Pedi<strong>at</strong>r clin north am 1 ; :11 - 0.<br />
. furrer f, deonna t. persistent toe walking in children:<br />
a comprehensive clinical study of 2 cases. Helv Paedi<strong>at</strong>r<br />
acta 1 2; : 01-1 .<br />
. Griffin p, Wheelhouse W, Shiavi R, Bass W. habitual<br />
younger children go to a center th<strong>at</strong> has<br />
pedi<strong>at</strong>ric physical therapists.<br />
Conclusion<br />
ITW is a problem th<strong>at</strong> is seen quite often.<br />
Both oper<strong>at</strong>ive and nonoper<strong>at</strong>ive methods<br />
of tre<strong>at</strong>ment have been recommended,<br />
and each has its pros and cons. Serial<br />
casting is a lengthy process with the child<br />
<strong>at</strong>tending physical therapy once a week<br />
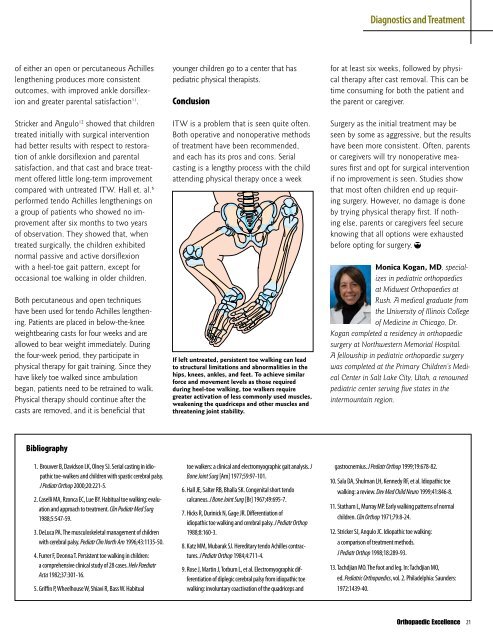
If left untre<strong>at</strong>ed, persistent toe walking can lead<br />
to structural limit<strong>at</strong>ions and abnormalities in the<br />
hips, knees, ankles, and feet. To achieve similar<br />
force and movement levels as those required<br />
during heel-toe walking, toe walkers require<br />
gre<strong>at</strong>er activ<strong>at</strong>ion of less commonly used muscles,<br />
weakening the quadriceps and other muscles and<br />
thre<strong>at</strong>ening joint stability.<br />
toe walkers: a clinical and electromyographic gait analysis. J<br />
Bone Joint surg [Am] 1 ; : -101.<br />
. hall Je, Salter RB, Bhalla SK. Congenital short tendo<br />
calcaneus. J Bone Joint surg [Br] 1 ; : - .<br />
. hicks R, durinick n, Gage JR. differenti<strong>at</strong>ion of<br />
idiop<strong>at</strong>hic toe walking and cerebral palsy. J Pedi<strong>at</strong>r orthop<br />
1 ; :1 0- .<br />
. K<strong>at</strong>z MM, Mubarak SJ. hereditary tendo Achilles contractures.<br />
J Pedi<strong>at</strong>r orthop 1 ; : 11- .<br />
. Rose J, Martin J, torburn L, et al. electromyographic differenti<strong>at</strong>ion<br />
of diplegic cerebral palsy from idiop<strong>at</strong>hic toe<br />
walking: involuntary coactiv<strong>at</strong>ion of the quadriceps and<br />
Diagnostics and Tre<strong>at</strong>ment<br />
for <strong>at</strong> least six weeks, followed by physical<br />
therapy after cast removal. This can be<br />
time consuming for both the p<strong>at</strong>ient and<br />
the parent or caregiver.<br />
Surgery as the initial tre<strong>at</strong>ment may be<br />
seen by some as aggressive, but the results<br />
have been more consistent. Often, parents<br />
or caregivers will try nonoper<strong>at</strong>ive measures<br />
first and opt for surgical intervention<br />
if no improvement is seen. Studies show<br />
th<strong>at</strong> most often children end up requiring<br />
surgery. However, no damage is done<br />
by trying physical therapy first. If nothing<br />
else, parents or caregivers feel secure<br />
knowing th<strong>at</strong> all options were exhausted<br />
before opting for surgery.<br />
Monica Kogan, MD, specializes<br />
in pedi<strong>at</strong>ric orthopaedics<br />
<strong>at</strong> <strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong><br />
<strong>Rush</strong>. A medical gradu<strong>at</strong>e from<br />
the University of Illinois College<br />
of Medicine in Chicago, Dr.<br />
Kogan completed a residency in orthopaedic<br />
surgery <strong>at</strong> Northwestern Memorial Hospital.<br />
A fellowship in pedi<strong>at</strong>ric orthopaedic surgery<br />
was completed <strong>at</strong> the Primary Children’s Medical<br />
Center in Salt Lake City, Utah, a renowned<br />
pedi<strong>at</strong>ric center serving five st<strong>at</strong>es in the<br />
intermountain region.<br />
gastrocnemius. J Pedi<strong>at</strong>r orthop 1 ;1 : - 2.<br />
10. Sala dA, Shulman Lh, Kennedy Rf, et al. Idiop<strong>at</strong>hic toe<br />
walking: a review. dev Med child neuro 1 ; 1: - .<br />
11. St<strong>at</strong>ham L, Murray Mp. early walking p<strong>at</strong>terns of normal<br />
children. clin orthop 1 1; : -2 .<br />
12. Stricker SJ, Angulo JC. Idiop<strong>at</strong>hic toe walking:<br />
a comparison of tre<strong>at</strong>ment methods.<br />
J Pedi<strong>at</strong>r orthop 1 ;1 :2 - .<br />
1 . tachdjian MO. the foot and leg. In: tachdjian MO,<br />
ed. Pedi<strong>at</strong>ric orthopaedics, vol. 2. philadelphia: Saunders:<br />
1 2:1 - 0.<br />
Orthopaedic Excellence<br />
21