

A Practical Approach to Panniculitis - Dermatology Rounds Canada
A Practical Approach to Panniculitis - Dermatology Rounds Canada
A Practical Approach to Panniculitis - Dermatology Rounds Canada

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
www.derma<strong>to</strong>logyrounds.ca<br />
DERMATOLOGY<br />
<strong>Rounds</strong>®<br />
A <strong>Practical</strong> <strong>Approach</strong> <strong>to</strong> <strong>Panniculitis</strong><br />
By SUSAN M POELMAN, MD, DENIS SASSEVILLE, MD<br />
<strong>Panniculitis</strong> has always been a difficult <strong>to</strong>pic in derma<strong>to</strong>logy, mainly due <strong>to</strong> the diverse<br />
spectrum of disorders that may present as inflammation of subcutaneous fat. Traditionally,<br />
most textbooks classify the panniculitides based on his<strong>to</strong>logic features (Figure 1) because<br />
they are difficult <strong>to</strong> differentiate clinically (most present with deep-seated tender nodules with<br />
surrounding erythema and edema); however, the his<strong>to</strong>logic approach is not helpful in the clinic.<br />
This issue of Derma<strong>to</strong>logy <strong>Rounds</strong> presents a practical approach <strong>to</strong> panniculitis that will<br />
allow clinicians <strong>to</strong> develop a differential diagnosis in the office and direct the investigation<br />
and management of patients with panniculitis. A brief commentary on diagnostic his<strong>to</strong>pathological<br />
features and treatment of each entity is also given. For a comprehensive review of<br />
the his<strong>to</strong>pathologic features of panniculitis, the reader is referred <strong>to</strong> an excellent article by<br />
1, 2<br />
Requena et al.<br />
The clinical approach <strong>to</strong> panniculitis<br />
The first thing <strong>to</strong> consider when panniculitis is suspected is whether it is caused by an<br />
exogenous or endogenous source (Table 1). After exogenous causes have been ruled-out,<br />
endogenous causes may be expanded by carefully eliciting the medical his<strong>to</strong>ry and reviewing<br />
body systems (Table 2). On physical examination, the appearance and location of the nodules<br />
may narrow the differential diagnosis as indicated in Table 2. The skin biopsy should be a deep<br />
excisional or incisional biopsy <strong>to</strong> the level of subcutaneous fat. A portion of the biopsy should<br />
be sent <strong>to</strong> microbiology for special stains and culture. The features listed in Table 3 should be<br />
included in the pathology report. Once a clinical entity is suspected and the biopsy performed,<br />
labora<strong>to</strong>ry or radiologic investigations may be indicated <strong>to</strong> confirm the diagnosis. These<br />
include, but are not limited <strong>to</strong>, the tests outlined in Table 3. Basic supportive care for patients<br />
with panniculitis includes rest, leg elevation, elastic compression s<strong>to</strong>ckings (Comprilan ® or<br />
ACE ® bandages), and salicylates or nonsteroidal anti-inflamma<strong>to</strong>ry drugs (NSAIDs) for pain.<br />
Noninfectious granuloma<strong>to</strong>us panniculitis<br />
Erythema nodosum (EN): EN, the most common type of panniculitis, is recognized as a reactive<br />
disorder <strong>to</strong> a variety of stimuli. Strep<strong>to</strong>coccal infection is the most common precipitant of<br />
EN in children while, in adults, sarcoidosis, drugs, and inflamma<strong>to</strong>ry bowel disease are the most<br />
common causes. EN typically presents in young women with tender warm nodules and plaques<br />
on the shins that change <strong>to</strong> a colour that is similar <strong>to</strong> deep bruises and resolve without ulceration,<br />
atrophy, or scarring. Commonly associated symp<strong>to</strong>ms include fever, fatigue, malaise,<br />
arthralgias, headache, cough, abdominal pain, vomiting, and diarrhea. A characteristic change<br />
on his<strong>to</strong>logy are Miescher’s radial granulomas, small collections of macrophages surrounding a<br />
stellate-shaped cleft. The clinical course of EN lasts 3 <strong>to</strong> 6 weeks, but lesions may persist and<br />
frequently recur. Treatment involves supportive care3-5 and potassium iodide 400 <strong>to</strong> 900 mg<br />
6, 7<br />
daily or 2 <strong>to</strong> 10 drops in water or orange juice TID may be used adjunctively.<br />
<strong>Panniculitis</strong> involving vessels<br />
Elastin stains are useful in cases of panniculitis with vasculitis because arteries have elastic<br />
lamina and will stain positively, whereas veins do not.<br />
Nodular vasculitis: Nodular vasculitis typically occurs in obese, middle-aged women with<br />
venous insufficiency who present with ulcerating nodules on the posterior legs that are aggravated<br />
by cold weather. When tuberculosis (TB), the most common cause of nodular vasculitis,<br />
is present, the nodules are renamed erythema induratum of Bazin. Nodular vasculitis has also<br />
2 0 0 7 V o l u m e 6 , I s s u e 5<br />
TM<br />
AS PRESENTED IN THE ROUNDS OF<br />
THE DIVISION OF DERMATOLOGY,<br />
MCGILL UNIVERSITY HEALTH CENTRE<br />
Members of the<br />
Division of Derma<strong>to</strong>logy<br />
Denis Sasseville, MD, Direc<strong>to</strong>r<br />
Edi<strong>to</strong>r, Derma<strong>to</strong>logy <strong>Rounds</strong><br />
Alfred Balbul, MD<br />
Alain Brassard, MD<br />
Judith Cameron, MD<br />
Wayne D. Carey, MD<br />
Ari Demirjian, MD<br />
Anna Doellinger, MD<br />
Odette Fournier-Blake, MD<br />
Roy R. Forsey, MD<br />
William Gerstein, MD<br />
David Grat<strong>to</strong>n, MD<br />
Manish Khanna, MD<br />
Raynald Molinari, MD<br />
Linda Moreau, MD<br />
Brenda Moroz, MD<br />
Khue Huu Nguyen, MD<br />
Elizabeth A. O’Brien, MD<br />
Wendy R. Sissons, MD<br />
Beatrice Wang, MD<br />
Ralph D. Wilkinson, MD<br />
Centre universitaire<br />
de santé McGill<br />
McGill University<br />
Health Centre<br />
McGill University Health Centre<br />
Division of Derma<strong>to</strong>logy<br />
Royal Vic<strong>to</strong>ria Hospital<br />
687 Pine Avenue West<br />
Room A 4.17<br />
Montreal, Quebec H3A 1A1<br />
Tel.: (514) 934-1934, local 34648<br />
Fax: (514) 843-1570<br />
The edi<strong>to</strong>rial content of<br />
Derma<strong>to</strong>logy <strong>Rounds</strong> is determined<br />
solely by the Division of Derma<strong>to</strong>logy,<br />
McGill University Health Centre.
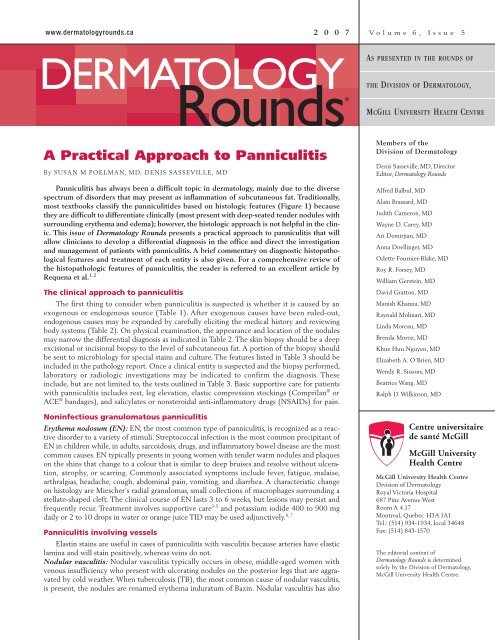
Figure 1: His<strong>to</strong>logic classification of panniculitis 1,2<br />
been associated with hepatitis C8 and treatment with<br />
propylthiouracil. 9 Lesions commonly turn bluish-red,<br />
break down in<strong>to</strong> ulcers with violaceous borders and,<br />
after many years, eventually heal with atrophic scars.<br />
They frequently recur. In cases associated with TB,<br />
caseating necrosis and multinucleated giant cells may be<br />
seen on his<strong>to</strong>logy. Chest x-ray and a Man<strong>to</strong>ux test are<br />
recommended <strong>to</strong> rule-out TB, followed by triple therapy<br />
if indicated. Oral corticosteroids, tetracycline, and potassium<br />
iodide are occasionally indicated as adjuncts <strong>to</strong><br />
supportive care. 10<br />
Superficial migra<strong>to</strong>ry thrombophlebitis (SMT): Patients<br />
with SMT often have a his<strong>to</strong>ry of venous insufficiency<br />
and present with linear, tender, cord-like, erythema<strong>to</strong>us<br />
nodules along an involved vein. SMT has been associated<br />
with malignancy 11-14 and/or a hypercoagulable state;<br />
Septal Lobular<br />
With vasculitis Without vasculitis With vasculitis<br />
Without vasculitis<br />
• Leukocy<strong>to</strong>clastic<br />
vasculitis (small vessels)<br />
• Cutaneous PAN<br />
(medium-sized arteries)<br />
• Superficial migra<strong>to</strong>ry<br />
thrombophlebitis<br />
(large veins)<br />
• Erythema nodosum<br />
• Scleroderma/deep<br />
morphea/eosinophilic<br />
fasciitis<br />
15, 16<br />
therefore, a full coagulation and malignancy work-up is<br />
indicated. Treatment is supportive.<br />
Cutaneous polyarteritis nodosa (PAN): What separates<br />
cutaneous PAN from other panniculitides is the livedo<br />
reticularis and ulceration that accompanies the bilateral<br />
Table 1: Exogenous vs. endogenous causes of panniculitis<br />
• Erythema induratum<br />
• Erythema nodosum<br />
leprosum<br />
• Lucio’s phenomenon<br />
PAN = polyarteritis nodosa; CTD = connective tissue disease; DM = derma<strong>to</strong>myositis; SLE = systemic lupus erythema<strong>to</strong>sus.<br />
Exogenous<br />
• Infection: erythema nodosum,<br />
erythema induratum of Bazin,<br />
viral/fungal/bacterial<br />
• Medications: penicillin, sulfonamides,<br />
bromides/iodides, oral contraceptive<br />
pills, post-steroid panniculitis<br />
• Trauma: blunt trauma, cold trauma,<br />
injection granuloma, paraffin<br />
Endogenous<br />
• Trauma (cold, blunt<br />
trauma, injection)<br />
• Infection<br />
• Pancreatic<br />
• Childhood/neonatal<br />
• Cy<strong>to</strong>phagic histiocytic<br />
• CTD (DM, SLE)<br />
• Lipoderma<strong>to</strong>sclerosis<br />
• Calciphylaxis,<br />
• α1-antitrypsin deficiency<br />
tender red nodules on the lower legs. The medium-sized<br />
arteries of the septa are involved and the process is more<br />
inflamma<strong>to</strong>ry than thrombotic, as in SMT. Patients with<br />
cutaneous PAN frequently have low-grade fever, arthralgias,<br />
malaise, myalgias, and fatigue. 17 If there is no systemic<br />
vasculitis, the prognosis is good and patients respond well<br />
<strong>to</strong> NSAIDs, and low-dose prednisone (20 mg daily).<br />
Erythema nodosum leprosum and Lucio’s phenomenon:<br />
Patients with leproma<strong>to</strong>us leprosy may present<br />
with painful erythema<strong>to</strong>us <strong>to</strong> violaceous nodules on the<br />
extremities that are associated with severe systemic<br />
symp<strong>to</strong>ms. Erythema nodosum leprosum is an immune<br />
complex-mediated vasculitis that involves the dermis<br />
and occasionally extends in<strong>to</strong> the subcutaneous fat.<br />
Treatment with thalidomide 400 mg nightly or clofazimine<br />
300 mg daily and prednisone 30 mg daily is<br />
recommended. 1 Lucio’s phenomenon is an uncommon<br />
diffuse form of leproma<strong>to</strong>us leprosy characterized by<br />
painful hemorrhagic ulcers and severe systemic symp<strong>to</strong>ms;<br />
it occasionally leads <strong>to</strong> death. The treatment of<br />
choice for this necrotizing vasculitis is thalidomide. 18<br />
• Self antigens/au<strong>to</strong>antibodies: lupus panniculitis, derma<strong>to</strong>myositis,<br />
scleroderma/morphea<br />
• Immune complex: superficial migra<strong>to</strong>ry thrombophlebitis, polyarteritis<br />
nodosa<br />
• Venous insufficiency: lipoderma<strong>to</strong>sclerosis, nodular vasculitis<br />
• Malignancies: Pancreatic carcinoma<br />
• Abnormal histiocytes: cy<strong>to</strong>phagic<br />
• Humoral fac<strong>to</strong>rs: α1-antitrypsin deficiency, calciphylaxis<br />
• Hormonal fac<strong>to</strong>rs: pregnancy (erythema nodosum)<br />
• Neonatal abnormal fatty acid ratio with increased propensity <strong>to</strong><br />
crystallize with exposure <strong>to</strong> cold temperatures: sclerema neona<strong>to</strong>rum,<br />
subcutaneous fat necrosis of newborn<br />
• Associated with other diseases: sarcoidosis, inflamma<strong>to</strong>ry bowel disease,<br />
Behcet's disease (erythema nodosum)
Table 2: Clues <strong>to</strong> the etiology of panniculitis on<br />
his<strong>to</strong>ry and physical examination<br />
His<strong>to</strong>ry<br />
• No systemic symp<strong>to</strong>ms (trauma-induced: chemical,<br />
thermal, physical)<br />
• Fever, arthritis, abdominal pain, or his<strong>to</strong>ry of<br />
pancreatic disease (pancreatic panniculitis)<br />
• Immunosuppressed (infectious etiology)<br />
• Pancreatitis, glomerulonephritis, emphysema,<br />
cirrhosis, cutaneous vasculitis, rheuma<strong>to</strong>id arthritis<br />
(α1-antitrypsin deficiency)<br />
• Arthritis, pho<strong>to</strong>sensitivity, Raynaud’s, dysphagia,<br />
and oral ulcers (connective tissue disease)<br />
• Fever, sore throat, arthralgias, malaise, bowel<br />
symp<strong>to</strong>ms, his<strong>to</strong>ry of oral contraceptives,<br />
sulfonamides, bromides/iodides (erythema<br />
nodosum)<br />
• Fever, weight loss (CHP)<br />
Physical Examination<br />
Nodules:<br />
• Fluctuant, ulcerating, draining<br />
– Pancreatic<br />
– Traumatic<br />
– α1-antitrypsin deficiency<br />
– Infection<br />
• Bilateral, tender on posterior legs of middle-aged<br />
obese female with venous insufficiency<br />
– E. induratum/nodular vasculitis,<br />
Lipoderma<strong>to</strong>sclerosis (acute form)<br />
• Hemorrhagic/purpuric<br />
– α1-antitrypsin deficiency, CHP<br />
• Linear configuration (with his<strong>to</strong>ry of varicose veins<br />
and/or hypercoagulable state)<br />
– Superficial migra<strong>to</strong>ry thrombophlebitis<br />
Other observations:<br />
• Venous stasis<br />
– Lipoderma<strong>to</strong>sclerosis, nodular vasculitis<br />
• Livedo reticularis, small nodules in distribution of<br />
superficial arteries<br />
– Polyarteritis nodosa<br />
• Hepa<strong>to</strong>splenomegaly<br />
– CHP<br />
E. induratum = erythema induratum of Bazin,<br />
CHP = cy<strong>to</strong>phagic histiocytic panniculitis<br />
Vascular disorders<br />
Sclerosing panniculitis (lipoderma<strong>to</strong>sclerosis): Similar<br />
<strong>to</strong> nodular vasculitis, lipoderma<strong>to</strong>sclerosis is common in<br />
middle-aged obese women with venous insufficiency.<br />
Patients with lipoderma<strong>to</strong>sclerosis present with woody<br />
indurated plaques on “inverted champagne bottle”shaped<br />
lower legs. Treatment is supportive. Stanozolol<br />
2 <strong>to</strong> 5 mg twice daily 19 or pen<strong>to</strong>xifylline 20 have been<br />
effective in pain control.<br />
Calciphylaxis: Approximately 4% of all patients on<br />
hemodialysis present with calciphylaxis due <strong>to</strong> calcification<br />
of vessel walls and occlusion of small arterioles.<br />
Although the most common cause of calciphylaxis is<br />
end-stage renal failure, it is also associated with secondary<br />
hyperparathyroidism and, rarely, malignancy 21-23<br />
and end-stage liver cirrhosis. 24 Clinically, patients present<br />
with symmetrical violaceous <strong>to</strong> black livedo reticularis-<br />
Table 3: Investigations for panniculitis<br />
Skin biopsy: what <strong>to</strong> look for on the pathology report<br />
• Pattern: lobular, septal, or mixed<br />
• Vasculitis or no vasculitis<br />
• Characteristic his<strong>to</strong>logic findings<br />
(ie, needle-shaped clefts, ghost cells, etc.)<br />
Labora<strong>to</strong>ry tests<br />
• Pancreatic enzymes (amylase, lipase)<br />
• SPEP, CBC, LDH, peripheral blood smear<br />
• Calcium, phosphate, creatinine, PTH<br />
• ANA, ENA, ANCA’s, dsDNA, rheuma<strong>to</strong>id fac<strong>to</strong>r<br />
• α1-antitrypsin levels<br />
• Fasting glucose, HbA1c<br />
Radiologic tests<br />
• Chest x-ray<br />
• CT chest, abdomen, and pelvis<br />
• Lower leg venous Doppler studies<br />
like patches and plaques, most often on the legs, but also<br />
on the upper extremities, trunk, and penis. With time,<br />
lesions enlarge in<strong>to</strong> ulcers and become painful and<br />
necrotic with black eschars. On his<strong>to</strong>logy, fat necrosis<br />
with calcification of vessel walls is characteristic. Mortality<br />
rates of 60% <strong>to</strong> 70% have been reported, mainly due<br />
<strong>to</strong> sepsis from secondarily-infected ulcers. Treatment<br />
options are limited, but include parathyroidec<strong>to</strong>my and<br />
hyperbaric oxygen with subcutaneous low-molecular<br />
weight heparin. 25-27<br />
Connective tissue disorders<br />
Lupus panniculitis: Approximately 1% <strong>to</strong> 3% of<br />
patients with lupus erythema<strong>to</strong>sus (LE) will develop<br />
lupus panniculitis. It is more common in patients with<br />
discoid LE than systemic LE (SLE), and usually precedes<br />
(but may occur synchronously or after) the onset of LE.<br />
Patients with SLE who present with lupus panniculitis<br />
usually have a milder disease course. Clinically, multiple<br />
symmetric painful nodules or plaques are localized <strong>to</strong><br />
the proximal extremities, face, and trunk. When lesions<br />
regress, they result in lipoatrophy (commonly seen on<br />
the shoulders and upper arms).<br />
On his<strong>to</strong>logy, epidermal changes of discoid LE such<br />
as follicular plugging, atrophy, dyspigmentation, telangiectasias,<br />
and ulceration are characteristic. 28, 29 The clinical<br />
course is chronic and recurrent. Avoidance of trauma<br />
and sun protection is important. Potent <strong>to</strong>pical or<br />
intralesional corticosteroids and antimalarials have been<br />
successfully used. 30-32 Alternatively, dapsone, cyclophosphamide,<br />
and thalidomide are reported <strong>to</strong> be successful,<br />
with a second antimalarial added if there is no response<br />
with a single agent.<br />
Deep morphea “scleroderma panniculitis”: Patients with<br />
deep morphea present with bound down plaques or<br />
nodules that heal with atrophy and hyperpigmentation<br />
and respond poorly <strong>to</strong> treatment. Intralesional and oral<br />
corticosteroids, antimalarials, penicillamine, and methotrexate33<br />
have been used unsuccessfully.<br />
Other: In case reports, derma<strong>to</strong>myositis, Sjögren’s<br />
disease, and mixed connective tissue disease have been<br />
described as being associated with panniculitis. 34-36
<strong>Panniculitis</strong> associated with<br />
other systemic disorders<br />
Pancreatic panniculitis: <strong>Panniculitis</strong> in patients with<br />
pancreatic disorders is rare (~2%) 1 and may precede<br />
the onset of pancreatic disease. 37 Pancreatic panniculitis<br />
may be associated with acute or chronic pancreatitis,<br />
pancreatic carcinomas, or rarely ana<strong>to</strong>mic<br />
ductal anomalies, 38 pseudocysts, 39 and vasculopancreatic<br />
fistulas. 40 Clinically, painful erythema<strong>to</strong>us<br />
nodules that ulcerate and discharge a brownish oily<br />
exudate (if fat necrosis is severe) are typically seen<br />
on the lower legs. Patients may also present with<br />
abdominal pain or acute arthritis if peri<strong>to</strong>neal or<br />
periarticular fat is involved, respectively. His<strong>to</strong>logically,<br />
fat necrosis with saponification and “ghost<br />
cells” (adipocytes with absent nuclei) is pathognomonic.<br />
41 The pathogenesis of pancreatic panniculitis<br />
is thought <strong>to</strong> be related <strong>to</strong> a combination of fat<br />
necrosis by pancreatic enzymes and immunologic<br />
fac<strong>to</strong>rs. 42 In pancreatic cancer patients, panniculitis<br />
may herald the development of metastatic disease<br />
and predict a poor clinical outcome. 37 Treatment of<br />
patients with pancreatic panniculitis is based on surgical<br />
repair of the underlying pancreatic abnormality<br />
and supportive care (which is often minimally<br />
effective). For patients with pancreatic tumours,<br />
octreotide, a synthetic soma<strong>to</strong>statin analog that<br />
inhibits secretion of pancreatic enzymes, has been<br />
reported <strong>to</strong> be of some benefit in a few cases. 43<br />
αα 1-antitrypsin deficiency-associated panniculitis:<br />
α1-antitrypsin is an important enzyme produced by<br />
the liver that prevents the au<strong>to</strong>digestion of tissues in<br />
the body by proteases. A deficiency in this enzyme<br />
may result in fat necrosis and panniculitis, cirrhosis,<br />
emphysema, pancreatitis, glomerulonephritis, rheu -<br />
ma<strong>to</strong>id arthritis, cutaneous vasculitis, or angioedema.<br />
Clinically, patients present with erythema<strong>to</strong>us <strong>to</strong><br />
purpuric painful plaques and nodules that may<br />
ulcerate and drain a brownish oily fluid. After a<br />
prolonged course, plaques heal with atrophy and<br />
scarring. His<strong>to</strong>logically, fat necrosis with splaying of<br />
neutrophils between collagen bundles in the deep<br />
dermis is a characteristic finding. Lesions are often<br />
resistant <strong>to</strong> treatment; however, oral corticosteroids,<br />
antimalarials, doxycycline, dapsone, colchicine,<br />
intravenous infusions of exogenous α1-antitrypsin inhibi<strong>to</strong>r, and plasma exchange have been found <strong>to</strong><br />
be effective. 44-46<br />
Cy<strong>to</strong>phagic histiocytic panniculitis and subcutaneous<br />
panniculitis-like T-cell lymphoma: Cy<strong>to</strong> -<br />
phagic histiocytic panniculitis (CHP) is so-named<br />
because of histiocyte phagocy<strong>to</strong>sis of various cells<br />
and debris, resulting in “bean bag cells” his<strong>to</strong>logically.<br />
It is thought <strong>to</strong> represent the early stage of a lymphoproliferative<br />
disorder because, after a prolonged<br />
course, patients may develop T-cell, B-cell, and NK<br />
cell lymphomas, grouped <strong>to</strong>gether as subcutaneous<br />
panniculitis-like T-cell lymphoma (SPTL). Clinically,<br />
deep-seated erythema<strong>to</strong>us nodules with overly-<br />
DERMATOLOGY<br />
<strong>Rounds</strong><br />
ing ecchymoses, symp<strong>to</strong>ms of fever and weight loss,<br />
and findings of lymphadenopathy and hepa <strong>to</strong> splen -<br />
omegaly are found.<br />
Patients with the benign variant of CHP , which<br />
does not transform in<strong>to</strong> lymphoma, tend <strong>to</strong> respond<br />
well <strong>to</strong> prednisone or cyclosporine. 1 Unlike SPTL,<br />
this nonfatal form is not associated with Epstein-<br />
Barr virus (EBV) and is most commonly seen in<br />
patients without systemic symp<strong>to</strong>ms. Patients with<br />
CHP that transforms <strong>to</strong> SPTL have a poor prognosis<br />
and, although therapies such as prednisone, cyclo -<br />
sporine, dapsone, and high-dose chemotherapy<br />
alone or in combination with peripheral stem cell<br />
rescue have been reportedly effective, prolonged<br />
remissions are uncommon.<br />
Infectious panniculitides<br />
Infectious panniculitis is commonly found in,<br />
but is not exclusive <strong>to</strong>, immunosuppressed patients.<br />
It is most often due <strong>to</strong> the hema<strong>to</strong>genous spread of<br />
bacteria, mycobacteria, or fungi, but may also result<br />
from direct inoculation of these infectious agents.<br />
Patients with diabetes mellitus, malignancy, connective<br />
tissue disease, acquired immune deficiency syndrome<br />
(AIDS), or a his<strong>to</strong>ry of organ transplant have<br />
been reported with infectious panniculitis 1 and<br />
typically present with ulcerating fluctuant nodules<br />
similar <strong>to</strong> those of pancreatic or α1-antitrypsin deficiency<br />
panniculitis. The his<strong>to</strong>logy is nondescript.<br />
Diagnosis is made on special stains for organisms<br />
and culture, and patients usually respond <strong>to</strong> anti -<br />
biotics or surgery in selected cases.<br />
Traumatic panniculitis<br />
Traumatic panniculitis results from accidental,<br />
intentional, or iatrogenic injury. Typical scenarios<br />
include children who suck on popsicles, ice cubes,<br />
or ice packs and develop firm nodules on the cheeks<br />
and chin, women who wear tight pants and go<br />
horseback riding who develop erythema<strong>to</strong>us <strong>to</strong> violaceous<br />
plaques on their inner thighs, and women<br />
with large breasts who develop indurated nodules<br />
that mimic inflamma<strong>to</strong>ry breast cancer. Traumatic<br />
panniculitis from injections most commonly occurs<br />
with substances such as mineral oil, silicones,<br />
camphor, cot<strong>to</strong>nseed, and sesame oil. On his<strong>to</strong>logy,<br />
fat necrosis and a characteristic “swiss cheese”<br />
appearance is seen. Treatment requires removal of<br />
the inciting agent and oral or intralesional cortico -<br />
steroids <strong>to</strong> control the inflammation.<br />
Childhood panniculitis<br />
Children are uniquely susceptible <strong>to</strong> panniculitis<br />
due <strong>to</strong> the increased ratio of saturated <strong>to</strong> unsaturated<br />
fatty acids, resulting in a higher melting point<br />
and increased propensity <strong>to</strong>wards crystallization<br />
upon exposure <strong>to</strong> cold.<br />
Sclerema neona<strong>to</strong>rum: The typical patient with<br />
sclerema neona<strong>to</strong>rum is a premature baby with congestive<br />
heart failure (CHF) who presents in the first<br />
T
week of life with a generalized distribution of cold,<br />
rigid, wooden board-like skin. This child may have<br />
underlying hypothermia, lung abnormalities, CHF,<br />
diarrhea, or intestinal blockage, and commonly dies<br />
of septicemia. There is sparing of the palms, soles,<br />
and genitalia and common precipitants include<br />
exposure <strong>to</strong> cold, defective complement, and<br />
dehydration. Needle-shaped clefts in lipocytes are<br />
characteristic on his<strong>to</strong>logy. There is no effective<br />
treatment and supportive measures <strong>to</strong> control sepsis<br />
are indicated.<br />
Subcutaneous fat necrosis of the newborn (SFN):<br />
In contrast <strong>to</strong> sclerema neona<strong>to</strong>rum, SFN is a localized<br />
self-limited disorder that is much less severe.<br />
Newborns between 2 <strong>to</strong> 3 weeks old present with<br />
red <strong>to</strong> violaceous plaques or nodules on the cheeks,<br />
shoulders, trunk, but<strong>to</strong>cks, and thighs that often<br />
resolve within a few days. Predisposing fac<strong>to</strong>rs<br />
include hypothermia, gestational diabetes, hypoglycemia,<br />
meconium aspiration, placenta previa,<br />
seizures, and preeclampsia. 47,48 Common complications<br />
of SFN are hypercalcemia and thrombocy<strong>to</strong>penia;<br />
therefore, moni<strong>to</strong>ring of serum calcium is<br />
recommended and dietary restriction of calcium<br />
and vitamin D, hydration, and furosemide may be<br />
indicated <strong>to</strong> control calcium levels. On his<strong>to</strong>logy,<br />
needle-shaped clefts in both adipocytes and giant<br />
cells are characteristic. Treatment involves supportive<br />
care. Patients recover quickly, but corticosteroids<br />
may occasionally be indicated.<br />
Post-steroid panniculitis: Post-steroid panniculitis<br />
presents in children aged 2 <strong>to</strong> 14 years who have<br />
recently (within the last 1 <strong>to</strong> 40 days) undergone<br />
rapid withdrawal of corticosteroids. Firm red plaques<br />
on the cheeks, arms, and trunk are typically seen.<br />
The his<strong>to</strong>logic appearance is identical <strong>to</strong> subcutaneous<br />
fat necrosis of the newborn. There is no treatment<br />
as lesions spontaneously resolve after months<br />
<strong>to</strong> one year or after corticosteroids are restarted.<br />
References:<br />
1. Requena L, Sanchez Yus E. <strong>Panniculitis</strong>. Part II. Mostly lobular<br />
panniculitis. J Am Acad Derma<strong>to</strong>l 2001;45(3):325-361.<br />
2. Requena L, Yus ES. <strong>Panniculitis</strong>. Part I. Mostly septal panniculitis.<br />
J Am Acad Derma<strong>to</strong>l. Aug 2001;45(2):163-183.<br />
3. Marshall JK, Irvine EJ. Successful therapy of refrac<strong>to</strong>ry erythema<br />
nodosum associated with Crohn’s disease using potassium<br />
iodide. Can J Gastroenterol 1997;11(6):501-502.<br />
4. Hanauer SB. How do I treat erythema nodosum, aphthous<br />
ulcerations, and pyoderma gangrenosum? Inflamm Bowel Dis<br />
1998;4(1):70; discussion 73.<br />
5. Cohen PR, Holder WR, Rapini RP. Concurrent Sweet’s<br />
syndrome and erythema nodosum: a report, world literature<br />
review and mechanism of pathogenesis. J Rheuma<strong>to</strong>l 1992;<br />
19(5):814-820.<br />
6. Horio T, Imamura S, Danno K, Ofuji S. Potassium iodide in<br />
the treatment of erythema nodosum and nodular vasculitis.<br />
Arch Derma<strong>to</strong>l 1981;117(1):29-31.<br />
7. Schulz EJ, Whiting DA. Treatment of erythema nodosum and<br />
nodular vasculitis with potassium iodide. Br J Derma<strong>to</strong>l 1976;<br />
94(1):75-78.<br />
8. Cardinali C, Gerlini G, Caproni M, Pimpinelli N, Fabbri P.<br />
Hepatitis C virus: a common triggering fac<strong>to</strong>r for both nodular<br />
vasculitis and Sjögren’s syndrome? Br J Derma<strong>to</strong>l 2000;<br />
142(1):187-189.<br />
DERMATOLOGY<br />
<strong>Rounds</strong><br />
9. Wolf D, Ben-Yehuda A, Okon E, Naparstek Y. Nodular<br />
vasculitis associated with propylthiouracil therapy. Cutis<br />
1992;49:253-255.<br />
10. Shaffer N, Kerdel FA. Nodular vasculitis (erythema induratum):<br />
treatment with auranofin. J Am Acad Derma<strong>to</strong>l 1991;<br />
25(2 Pt 2):426-429.<br />
11. Bazin E. Lecons theoriques et cliniques sur la scrofule. Paris:<br />
A. Delahaye 1861;2nd edition:146.<br />
12. New<strong>to</strong>n J WF. Pustular panniculitis in rheuma<strong>to</strong>id arthritis.<br />
Br J Derma<strong>to</strong>l 1988;119:97-98.<br />
13. Tran TA, DuPree M, Carlson JA. Neutrophilic lobular (pustular)<br />
panniculitis associated with rheuma<strong>to</strong>id arthritis: a case<br />
report and review of the literature. Am J Derma<strong>to</strong>pathol<br />
1999;21(3):247-252.<br />
14. Cribier B, Grosshans E. [Bazin’s erythema induratum: obsolete<br />
concept and terminology]. Ann Derma<strong>to</strong>l Venereol 1990;<br />
117(12):937-943.<br />
15. Rea TH, Ridley DS. Lucio’s phenomenon: a comparative<br />
his<strong>to</strong>logical study. Int J Lepr Other Mycobact Dis 1979;47(2):<br />
161-166.<br />
16. Anstey A, Wilkinson JD, Wojnarowska F, Kirk A, Gowers L.<br />
Pustular panniculitis in rheuma<strong>to</strong>id arthritis. J R Soc Med<br />
1991;84(5):307-308.<br />
17. Siberry GK, Cohen BA, Johnson B. Cutaneous polyarteritis<br />
nodosa. Reports of two cases in children and review of the<br />
literature. Arch Derma<strong>to</strong>l 1994;130(7):884-889.<br />
18. Walters M. An internationally controlled double blind trial of<br />
thalidomide in severe erythema nodosum leprosum. Lepr Rev<br />
1971;42:26-42.<br />
19. Kirsner RS, Pardes JB, Eaglstein WH, Falanga V. The clinical<br />
spectrum of lipoderma<strong>to</strong>sclerosis. J Am Acad Derma<strong>to</strong>l 1993;<br />
28(4):623-627.<br />
20. Segal S, Cooper J, Bolognia J. Treatment of lipoderma<strong>to</strong>sclerosis<br />
with oxandrolone in a patient with stanozolol-induced<br />
hepa<strong>to</strong><strong>to</strong>xicity. J Am Acad Derma<strong>to</strong>l 2000;43(3):558-559.<br />
21. Raper RF, Ibels LS. Osteosclerotic myeloma complicated by<br />
diffuse arteritis, vascular calcification and extensive cutaneous<br />
necrosis. Nephron 1985;39(4):389-392.<br />
22. Mastruserio DN, Nguyen EQ, Nielsen T, Hessel A, Pellegrini<br />
AE. Calciphylaxis associated with metastatic breast carcinoma.<br />
J Am Acad Derma<strong>to</strong>l 1999;41(2 Pt 2):295-298.<br />
23. Riegert-Johnson DL, Kaur JS, Pfeifer EA. Calciphylaxis associated<br />
with cholangiocarcinoma treated with low-molecularweight<br />
heparin and vitamin K. Mayo Clin Proc 2001;76(7):<br />
749-752.<br />
24. Fader DJ, Kang S. Calciphylaxis without renal failure. Arch<br />
Derma<strong>to</strong>l 1996;132(7):837-838.<br />
25. Mathur RV, Shortland JR, el-Nahas AM. Calciphylaxis.<br />
Postgrad Med J 2001;77(911):557-561.<br />
26. Hafner J, Keusch G, Wahl C, et al. Uremic small-artery disease<br />
with medial calcification and intimal hyperplasia (so-called<br />
calciphylaxis): a complication of chronic renal failure and<br />
benefit from parathyroidec<strong>to</strong>my. J Am Acad Derma<strong>to</strong>l 1995;<br />
33(6):954-962.<br />
27. Podymow T, Wherrett C, Burns KD. Hyperbaric oxygen in the<br />
treatment of calciphylaxis: a case series. Nephrol Dial Transplant<br />
2001;16(11):2176-2180.<br />
28. Blaustein A, Moreno A, Noguera J, de Moragas JM. Septal<br />
granuloma<strong>to</strong>us panniculitis in Sweet’s syndrome. Report of<br />
two cases. Arch Derma<strong>to</strong>l 1985;121(6):785-788.<br />
29. McMillan A. Reiter’s disease in a female, presenting as erythema<br />
nodosum. Br J Vener Dis 1975;51(5):345-347.<br />
30. Miescher G. Zur His<strong>to</strong>logie des Erythema nodosum. Acta<br />
Derm Venereol 1947;27:447-468.<br />
31. Miescher G. Zur Frage der Radiarknotchen beim Erythema<br />
nodosum. Arch Derma<strong>to</strong>l Syphil 1951;193:251-256.<br />
32. Kim B, LeBoit PE. His<strong>to</strong>pathologic features of erythema<br />
nodosum—like lesions in Behcet disease: a comparison with<br />
erythema nodosum focusing on the role of vasculitis. Am J<br />
Derma<strong>to</strong>pathol 2000;22(5):379-390.<br />
33. Peterson LS, Nelson AM, Su WP. Classification of morphea<br />
(localized scleroderma). Mayo Clin Proc 1995;70(11):1068-<br />
1076.<br />
34. Chao YY, Yang LJ. Derma<strong>to</strong>myositis presenting as panniculitis.<br />
Int J Derma<strong>to</strong>l 2000;39(2):141-144.<br />
T
35. Tait CP, Yu LL, Rohr J. Sjogren’s syndrome and granuloma<strong>to</strong>us<br />
panniculitis. Australas J Derma<strong>to</strong>l 2000;41(3):187-189.<br />
36. I<strong>to</strong>h O, Nishimaki T, I<strong>to</strong>h M, et al. Mixed connective tissue disease<br />
with severe pulmonary hypertension and extensive subcutaneous<br />
calcification. Intern Med 1998;37(4):421-425.<br />
37. Heykarts B, Anseeuw M, Degreef H. <strong>Panniculitis</strong> caused by acinous<br />
pancreatic carcinoma. Derma<strong>to</strong>logy 1999;198(2):182-183.<br />
38. Haber RM, Assaad DM. <strong>Panniculitis</strong> associated with a pancreas<br />
divisum. J Am Acad Derma<strong>to</strong>l 1986;14(2 Pt 2):331-334.<br />
39. Kobayashi H, I<strong>to</strong>h T, Shima N, et al. Periduodenal panniculitis due<br />
<strong>to</strong> spontaneous rupture of a pancreatic pseudocyst in<strong>to</strong> the duodenum.<br />
Abdom Imaging 1995;20(2):106-108.<br />
40. Reynaud D AL, Escourrou J, et al. Traitment endoscopique d’une<br />
cy<strong>to</strong>stea<strong>to</strong>necrose secondaire a une fistule pancreaticovasculaire:<br />
a propos d’un cas. Rev Med Interne 1998;19:123-127.<br />
41. Syzmanski FJ. Nodular fat necrosis and pancreatic diseases. Arch<br />
Derma<strong>to</strong>l 1961;83:224-229.<br />
42. Dhawan SS, Jimenez-Acosta F, Poppiti RJ, Jr., Barkin JS. Subcutaneous<br />
fat necrosis associated with pancreatitis: his<strong>to</strong>chemical and<br />
electron microscopic findings. Am J Gastroenterol 1990;85(8):1025-<br />
1028.<br />
43. Hudson-Peacock MJ, Regnard CF, Farr PM. Liquefying panniculitis<br />
associated with acinous carcinoma of the pancreas responding <strong>to</strong><br />
octreotide. J R Soc Med 1994;87(6):361-362.<br />
44. Smith KC, Pittelkow MR, Su WP. <strong>Panniculitis</strong> associated with severe<br />
alpha 1-antitrypsin deficiency. Treatment and review of the literature.<br />
Arch Derma<strong>to</strong>l 1987;123(12):1655-1661.<br />
45. Humbert P, Faivre B, Gibey R, Agache P. Use of anti-collagenase<br />
properties of doxycycline in treatment of alpha 1-antitrypsin deficiency<br />
panniculitis. Acta Derm Venereol 1991;71(3):189-194.<br />
46. O’Riordan K, Blei A, Rao MS, Abecassis M. alpha 1-antitrypsin deficiency-associated<br />
panniculitis: resolution with intravenous alpha 1antitrypsin<br />
administration and liver transplantation. Transplantation<br />
1997;63(3):480-482.<br />
47. Fretzin DF, Arias AM. Sclerema neona<strong>to</strong>rum and subcutaneous fat<br />
necrosis of the newborn. Pediatr Derma<strong>to</strong>l 1987;4(2):112-122.<br />
48. Burden AD, Krafchik BR. Subcutaneous fat necrosis of the newborn:<br />
a review of 11 cases. Pediatr Derma<strong>to</strong>l 1999;16(5):384-387.<br />
Abstract of Interest<br />
Normal subcutaneous fat, necrosis of adipocytes<br />
and classification of the panniculitides<br />
R E Q U E N A L, M A D R I D, S PA I N.<br />
The panniculitides represent a group of heterogeneous inflamma<strong>to</strong>ry<br />
diseases that involve the subcutaneous fat. The specific<br />
diagnosis of these diseases requires his<strong>to</strong>pathologic study<br />
because different panniculitides usually show the same clinical<br />
appearance, which consists of erythema<strong>to</strong>us nodules on the<br />
lower extremities. However, the his<strong>to</strong>pathologic study of panniculitis<br />
is difficult because of an inadequate clinicopathologic<br />
correlation and the changing evolutive nature of the lesions. In<br />
addition, large scalpel incisional biopsies are required. From<br />
his<strong>to</strong>pathologic point of view, all panniculitides are somewhat<br />
mixed because the inflamma<strong>to</strong>ry infiltrate involves both the<br />
septa and lobules. However, nearly always the differential diagnosis<br />
between a mostly septal and a mostly lobular panniculitis<br />
is straightforward at scanning magnification on the basis of the<br />
structures more intensely involved by the inflamma<strong>to</strong>ry infiltrate.<br />
Mostly septal panniculitides with vasculitis are actually<br />
more vasculitis than panniculitis and include superficial thrombophlebitis<br />
and cutaneous polyarteritis nodosa. Mostly septal<br />
panniculitides with no vasculitis include erythema nodosum,<br />
necrobiosis lipoidica, deep morphea, subcutaneous granuloma<br />
annulare, rheuma<strong>to</strong>id nodule, and necrobiotic xanthogranuloma.<br />
Mostly lobular panniculitis with vasculitis is only represented<br />
by erythema induratum of Bazin. In contrast, mostly lobular<br />
panniculitides without vasculitis comprise a large series of disparate<br />
disorders, including sclerosing panniculitis, calciphylaxis,<br />
sclerema neona<strong>to</strong>rum, subcutaneous fat necrosis of the newborn,<br />
poststeroid panniculitis, lupus erythema<strong>to</strong>sus profundus,<br />
pancreatic panniculitis, alpha(1)-antitrypsin deficiency panniculitis,<br />
subcutaneous Sweet syndrome, infective panniculitis,<br />
factitial panniculitis, lipodystrophy, traumatic panniculitis,<br />
subcutaneous sarcoidosis, and sclerosing postirradiation panniculitis.<br />
Finally, some cutaneous lymphomas may simulate<br />
panniculitis, both from clinical and his<strong>to</strong>pathologic points of<br />
view and, for that reason, they will be included in this review,<br />
although they are not inflamma<strong>to</strong>ry processes, but authentic<br />
lymphocytic neoplasms involving subcutaneous tissue.<br />
Semin Cutan Med Surg 2007;26(2):66-70.<br />
Upcoming Scientific Meetings<br />
17-20 January 2008<br />
American Academy of Cosmetic Surgery<br />
24 th Annual Scientific Meeting<br />
Orlando, Florida<br />
Contact: meeting@cosmeticsurgery.org<br />
or www.cosmeticsurgery.org<br />
1-6 February 2008<br />
American Academy of Derma<strong>to</strong>logy<br />
66 th Annual Meeting<br />
Henry B. Gonzalez Convention Center<br />
San An<strong>to</strong>nio, Texas<br />
Contact: registration@aad.org<br />
or: www.aad.org<br />
This publication is made possible by an unrestricted educational grant from<br />
Astellas Pharma <strong>Canada</strong>, Inc.<br />
© 2007 Division of Derma<strong>to</strong>logy, McGill University Health Centre, Montreal, which is solely responsible for the contents. The opinions expressed in this publication do not necessarily<br />
reflect those of the publisher or sponsor, but rather are those of the authoring institution based on the available scientific literature. Publisher: SNELL Medical Communication Inc.<br />
in cooperation with the Division of Derma<strong>to</strong>logy, McGill University Health Centre. ® Derma<strong>to</strong>logy <strong>Rounds</strong> is a registered trade mark of SNELL Medical Communication Inc. All<br />
rights reserved. The administration of any therapies discussed or referred <strong>to</strong> in Derma<strong>to</strong>logy <strong>Rounds</strong> should always be consistent with the recognized prescribing information in <strong>Canada</strong>.<br />
SNELL Medical Communication Inc. is committed <strong>to</strong> the development of superior Continuing Medical Education.<br />
SNELL<br />
Disclosure statement: Dr. Poelman and Dr. Sasseville have<br />
stated that they have no disclosures <strong>to</strong> announce in association with<br />
the contents of this issue.<br />
Change of address notices and requests for subscriptions<br />
for Derma<strong>to</strong>logy <strong>Rounds</strong> are <strong>to</strong> be sent by mail <strong>to</strong> P.O. Box<br />
310, Station H, Montreal, Quebec H3G 2K8 or by fax <strong>to</strong><br />
(514) 932-5114 or by e-mail <strong>to</strong> info@snellmedical.com.<br />
Please reference Derma<strong>to</strong>logy <strong>Rounds</strong> in your correspondence.<br />
Undeliverable copies are <strong>to</strong> be sent <strong>to</strong> the address above.<br />
Publications Post #40032303<br />
124-033




