evidence based mouth care policy - Doncaster and Bassetlaw ...
evidence based mouth care policy - Doncaster and Bassetlaw ...
evidence based mouth care policy - Doncaster and Bassetlaw ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
EVIDENCE BASED<br />
MOUTH CARE POLICY<br />
Developed & Written by: Janet Ryles – Macmillan Head <strong>and</strong><br />
Neck Clinical Nurse Specialist<br />
Date: March 2007<br />
Approved by: Clinical Review Group<br />
Date: June 2007<br />
Implementation Date: July 2007<br />
For Review: November 2009<br />
Page 1 of 21<br />
REF: PAT/PA 17 v.1<br />
WARNING: Always ensure that you are using the most up to date <strong>policy</strong> or procedure document. If<br />
you are unsure, you can check that it is the most up to date version by looking on the Trust Website:<br />
www.dbh.nhs.uk under the headings → ‘Freedom of Information’ → ‘Information Classes’ → ‘Policies<br />
<strong>and</strong> Procedures’
CONTENTS<br />
Page 2 of 21<br />
REF: PAT/PA 17 v.1<br />
Page No.<br />
• Introduction 3<br />
• Staff Who May Carry Out the Procedure 4<br />
• Risk Factors 4<br />
• Drugs / Treatments/ The Oral Cavity <strong>and</strong> Oropharynx 5<br />
• Potential Problems / Assessment / Actions 6 - 7<br />
• Flow chart 8<br />
- Flow chart – Additional Information 9<br />
- Supportive Information for Flow Chart 9<br />
• St<strong>and</strong>ard Mouth Care 10<br />
- Patient Requiring Assistance 10<br />
- Ulceration 10<br />
- Coated Tongue, Teeth or Mucosa 11<br />
- Dry Mouth 11<br />
- Painful Mouth 11 - 13<br />
• Information for ‘At Risk’ Groups<br />
- Oncology <strong>and</strong> Haematology 13 - 15<br />
- Older Patients 15<br />
- Other Conditions 16<br />
• References 17<br />
• Background to Research 18<br />
Appendix 1 - Oral Assessment Tool 19<br />
Appendix 2 - Oral Hygiene Record Chart 20<br />
Appendix 3 - The Oral Cavity <strong>and</strong> Oropharynx 21
• INTRODUCTION<br />
Page 3 of 21<br />
REF: PAT/PA 17 v.1<br />
Quality of life issues including oral <strong>care</strong> should be a priority for staff involved in any health<strong>care</strong><br />
setting. Oral health is often affected by medical conditions <strong>and</strong> some cancer treatments. This is<br />
often underreported, undiagnosed as problematic <strong>and</strong> inadequately treated (Adams 1996).<br />
It is the role <strong>and</strong> responsibility of the Registered General Nurse (RGN), also Health Care Assistants<br />
(HCA’s) <strong>and</strong> students, under supervision. The purpose of this <strong>policy</strong> is to avoid <strong>mouth</strong> <strong>care</strong><br />
practices which are often historical rather than research or <strong>evidence</strong> <strong>based</strong>. A <strong>mouth</strong> <strong>care</strong><br />
assessment tool is required in order to make an initial assessment <strong>and</strong> to promote high quality <strong>and</strong><br />
st<strong>and</strong>ardised oral <strong>care</strong> through a co-ordinated team approach. Failure to conduct an adequate oral<br />
assessment <strong>and</strong> documentation of oral <strong>care</strong> management may be interpreted as a poor st<strong>and</strong>ard of<br />
holistic <strong>care</strong>. As nurses we should be mindful of our legal responsibilities to not only ensure high<br />
st<strong>and</strong>ards of <strong>care</strong> for patient/clients but also accurate documentation (NMC 2002).<br />
Principles of <strong>evidence</strong> <strong>based</strong> practice.<br />
There should be a local <strong>policy</strong> consisting of guidelines <strong>and</strong> an assessment tool on which to base<br />
appropriate <strong>care</strong> needs. An agreed st<strong>and</strong>ard of assessing, implementing <strong>and</strong> evaluating <strong>mouth</strong><br />
<strong>care</strong> should be carried out every 12 hours. However, the following content is not exhaustive <strong>and</strong><br />
should be used to enhance the quality of <strong>care</strong> given to all our patients/clients. Staff implementing<br />
<strong>care</strong> should be trained appropriately. Our <strong>policy</strong> <strong>and</strong> guidelines should be used in conjunction with<br />
the Mouth Care Training pack produced by the Oral Heath Working Party 2003 (which can be<br />
obtained from the Training <strong>and</strong> Development Department upon request) <strong>and</strong> the Royal Marsden<br />
NHS Trust Manual of Clinical Procedures – latest version, personal hygiene section (<strong>mouth</strong> <strong>care</strong>).
• STAFF WHO MAY CARRY OUT THE PROCEDURE<br />
The <strong>mouth</strong> <strong>care</strong> needs of patients are identified on an individual basis.<br />
Page 4 of 21<br />
REF: PAT/PA 17 v.1<br />
Student nurses <strong>and</strong> midwives may deliver oral <strong>care</strong> to patients only under the supervision of a<br />
registered nurse or midwife who are competent in this aspect of <strong>care</strong> <strong>and</strong> the supervisory role.<br />
A registered nurse or midwife must carry out the oral assessment whilst health <strong>care</strong> assistants <strong>and</strong><br />
clinical support workers may carry out oral <strong>care</strong>, under supervision.<br />
It is the responsibility of the RGN <strong>and</strong> Registered Midwife to assess, plan, implement <strong>and</strong> evaluate<br />
<strong>care</strong>.<br />
In line with guidelines laid down by the NMC (2002) for records <strong>and</strong> record keeping there must be a<br />
current <strong>and</strong> appropriate plan of <strong>care</strong> for all patients. The plan must incorporate on-going evaluation<br />
<strong>and</strong> reassessment of <strong>care</strong> <strong>and</strong> <strong>evidence</strong> that relevant interventions <strong>and</strong> observations have been<br />
communicated to appropriate members of the multidisciplinary team.<br />
Student nurses/midwives, health <strong>care</strong> assistants <strong>and</strong> clinical support workers should work through<br />
the <strong>mouth</strong> <strong>care</strong> pack produced by the Oral Health Working Party (OHWP 2003). This pack is<br />
available from the Training <strong>and</strong> Development Department upon request.<br />
The following risk factors should be taken into account:<br />
• RISK FACTORS<br />
Illnesses<br />
The literature consistently supports that various illnesses increase an individual’s risk of oral<br />
complications.<br />
* Diabetes * limited/restricted fluids<br />
* thyroid dysfunction * <strong>mouth</strong> breathers<br />
* oral disease/trauma * confusion<br />
* cerebrovascular disease * depression<br />
* debility * terminal illness<br />
* acute/chronic breathing * poor nutritional status<br />
disorders * oxygen therapy<br />
* insufficient saliva production * a general lack of motivation or inability<br />
to undertake oral hygiene<br />
(Thurgood 1994, Regnard et al 1997, Holmes 1997).<br />
• Other patients groups ‘at risk’<br />
i) Patient receiving intensive <strong>care</strong><br />
ii) Patients receiving chemotherapy <strong>and</strong> patients receiving radiotherapy to the head <strong>and</strong><br />
neck.<br />
iii) Patients receiving immunosuppressive therapy, i.e. transplant patients. (White 2000)<br />
iv) Elderly patients – if ill fitting, then dentures should be avoided where possible. If well<br />
fitting then dentures should be cleaned twelve hourly <strong>and</strong> removed at night. They<br />
should be brushed with an unperfumed soap or toothpaste, soaked in a solution of<br />
sodium hypocloride (Milton Sol, Denture Steradent for metal dentures) for 30 minutes<br />
<strong>and</strong> stored dry overnight.
• DRUGS AND TREATMENTS<br />
Page 5 of 21<br />
REF: PAT/PA 17 v.1<br />
There are various drugs <strong>and</strong> treatments that increase the vulnerability of the oral cavity to infection.<br />
Drugs<br />
Cytotoxic/Chemotherapeutic Drugs Reduce the auto-immune response<br />
Corticosteroids Affect the healing properties of tissues<br />
Antibiotics Alter the bacterial balance of commensal<br />
organisms in the <strong>mouth</strong> <strong>and</strong> allow<br />
c<strong>and</strong>idal invasions<br />
Antispasmodics Alters gut mobility <strong>and</strong> reduces salivary<br />
Antihistamines<br />
Anticholinergics<br />
Psychotropics<br />
Antidepressants <strong>and</strong> tranquillisers<br />
production<br />
These groups of drugs reduce salivary<br />
production<br />
Diuretics Potential dry <strong>mouth</strong> due to increased fluid<br />
loss<br />
Morphine Strong association with dryness of the<br />
<strong>mouth</strong><br />
Treatments<br />
Radiotherapy to the Head <strong>and</strong><br />
Neck<br />
Reduced ability to eat/drink normally<br />
Localised inflammation<br />
Oxygen Therapy Unhumidified oxygen administered by<br />
mask can dry the <strong>mouth</strong><br />
Intermittent suction Potential risk of damage to oral<br />
tissues<br />
Restricted oral intake Potential for dehydration<br />
Anaesthesia Reduces oral secretions<br />
• THE ORAL CAVITY AND OROPHARYNX<br />
See Appendix 3, page 21.<br />
Physiology<br />
(Thurgood 1994)<br />
The oral cavity is lined by a layer of rapidly dividing mucosal cells, which generate every 7-14 days<br />
(Madeya 1996). These cells become a focal point for a variety of complications. Minor salivary <strong>and</strong><br />
sebaceous gl<strong>and</strong>s found beneath the epithelium surface are most important for lubrication (Madeya<br />
1996).
• POTENTIAL PROBLEMS<br />
Frequently cited potential oral disorders are listed below (Thurgood 1994)<br />
Xerostomia A dry <strong>mouth</strong><br />
Stomatitis Inflammation <strong>and</strong> infection of the oral<br />
mucosa<br />
C<strong>and</strong>idiasis (oral thrush) Caused by a yeast-like fungus, C<strong>and</strong>ida<br />
albicans, which normally inhabits the<br />
vagina <strong>and</strong> digestive system. It<br />
commonly manifests as soft white<br />
plaques on the mucosa <strong>and</strong> tongue.<br />
Gingivitis Inflammation of the gums leading to<br />
swelling <strong>and</strong> bleeding caused by plaque<br />
attacking the damaging tissue.<br />
Leukoplakia (white/red) A lesion that cannot be scraped off or<br />
attributed to any other cause.<br />
Ulceration Ulcers which are white, small, punched<br />
out lesions of epithelial surfaces of the<br />
<strong>mouth</strong>, probably of viral origin.<br />
Mucositis Inflammation of the lining of the <strong>mouth</strong><br />
The following oral disorders are seen less commonly:-<br />
Dental Caries Decay <strong>and</strong> crumbling of tooth structure caused by the formation of<br />
plaque following the deposit of bacteria onto teeth, gums <strong>and</strong><br />
tongue.<br />
Dysgensia Impairment of the sense of taste.<br />
Parotitis Inflammation of the parotid salivary gl<strong>and</strong>s.<br />
Periodontal<br />
deterioration<br />
Disease of the gums <strong>and</strong> other structures supporting the teeth.<br />
Caused by release of toxins from plaque. These initiate a local<br />
immunological response which attacks teeth <strong>and</strong> gums<br />
(Thurgood 1994).<br />
Page 6 of 21<br />
REF: PAT/PA 17 v.1
• ASSESSMENT AND ACTION REQUIRED TO MAINTAIN ORAL HYGIENE<br />
Equipment Required:<br />
Torch<br />
Toothbrush <strong>and</strong> paste<br />
Tongue depressor<br />
Soft paraffin ointment<br />
Kidney dish<br />
Suction equipment (if appropriate)<br />
Clean procedure gloves<br />
Tissues or wipes<br />
Preparation:<br />
Explain procedure to patient<br />
Wash h<strong>and</strong>s<br />
Examine lips for any sores or cracking<br />
Page 7 of 21<br />
REF: PAT/PA 17 v.1<br />
Use oral assessment tool (appendix 1) <strong>and</strong> flow chart (page 8) to assess, implement <strong>and</strong> evaluate<br />
<strong>care</strong>. All actions <strong>and</strong> outcomes to be documented in patients <strong>care</strong> plan.
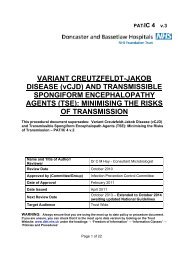
(Chlorhexidene)<br />
START<br />
Is the <strong>mouth</strong> healthy?<br />
(intact mucosa, clean,<br />
moist <strong>and</strong> pain free)<br />
No<br />
Is ulceration<br />
present?<br />
No<br />
Are the tongue,<br />
teeth, or mucosa<br />
coated?<br />
No<br />
Is the<br />
<strong>mouth</strong> dry?<br />
No<br />
Yes<br />
Is the <strong>mouth</strong><br />
painful?<br />
Flow Chart to Guide Oral Assessment <strong>and</strong> Care<br />
Yes<br />
Is c<strong>and</strong>ida<br />
present?<br />
Yes<br />
Yes<br />
St<strong>and</strong>ard Mouth Care<br />
REF: PAT/PA 17 v.1<br />
� 12 hourly teeth brushing, if own teeth, with soft brush<br />
<strong>and</strong> tooth paste – rinse well<br />
� Brush dentures 12 hourly<br />
� Brush off debris <strong>and</strong> soak dentures over night (if<br />
required)<br />
� Reassess every 24 hours<br />
� Soft paraffin to lips if dry<br />
Also if patient is unable to maintain own oral hygiene:<br />
� If <strong>mouth</strong> dry – moisten 1-2 hourly with water soaked<br />
<strong>mouth</strong> swabs<br />
� Oral suction to remove excess oral secretions if<br />
unconscious<br />
(NB refer to special protocols if relevant)<br />
Yes<br />
No<br />
St<strong>and</strong>ard <strong>mouth</strong> <strong>care</strong> plus:<br />
Difflam <strong>mouth</strong> wash every 3 hours if required for 7<br />
days, or Adcortyl in orabase paste apply a thin layer<br />
2-4 times daily for 5 days. refer to medical staff if<br />
persistent longer than 5 days<br />
St<strong>and</strong>ard <strong>mouth</strong> <strong>care</strong> plus:<br />
� Discuss with medical staff regarding antifungal<br />
treatment<br />
� Clean dentures at least four hourly<br />
St<strong>and</strong>ard <strong>mouth</strong> <strong>care</strong> plus<br />
� Brush tongue/teeth with Corsodyl gel<br />
(chlorhexidene)<br />
� If available allow patient to suck pineapple<br />
chunks or dissolve ¼ effervescent vitamin C<br />
tablet on tongue<br />
St<strong>and</strong>ard <strong>mouth</strong> <strong>care</strong> plus<br />
� Treat cause – e.g. dehydration, infection<br />
� Consider artificial saliva<br />
� Provide local comfort – ice cubes, pineapple<br />
chunks, ice lollies<br />
� Soft paraffin to lips<br />
Consider using topical analgesics – Difflam,<br />
Bonjela, Kamillosan Tea Tree Oil, <strong>and</strong> Gelclair<br />
Examine for ill-fitting dentures/dental decay or<br />
Infection. Follow local protocols for patients<br />
undergoing chemotherapy/radiotherapy.<br />
N.B. All medication must be prescribed<br />
Document evaluation <strong>and</strong> <strong>care</strong> in <strong>care</strong> plan <strong>and</strong> on oral hygiene chart<br />
Page 8 of 21
Additional Information<br />
Page 9 of 21<br />
REF: PAT/PA 17 v.1<br />
NB Always give st<strong>and</strong>ard <strong>mouth</strong> <strong>care</strong> plus one of the following, as prescribed by the doctor:-<br />
• Difflam (benzydamine hydrochloride) is effective in alleviating mild to moderate mucositis for<br />
some patients. It should be used prior to meals, also consider the use of Gel Clair, an<br />
analgesic <strong>and</strong> protective solution.<br />
• Gelclair is useful in controlling pain due to mucositis <strong>and</strong>/or ulceration. Used as a paste <strong>and</strong><br />
applied one hour prior to meal times.<br />
• Also a 2% Lignocaine solution <strong>mouth</strong>wash will help, if mucositis is more severe.<br />
• Adcortyl in orabase is useful as pain relief for ulceration.<br />
• Effervescent Vitamin C tablet 1000mg is valuable when treating chemotherapy induced<br />
mucositis caused by fluorecil <strong>and</strong> provides some protection for methotrexate induced<br />
mucositis. (Moisten tongue with water <strong>and</strong> place ¼ of a tablet directly to the tongue <strong>and</strong><br />
allow to fizz <strong>and</strong> dissolve)<br />
All of these treatments should be reviewed every 5-7 days<br />
Supportive Information for Flow Chart<br />
The literature review in relation to <strong>mouth</strong> <strong>care</strong> focuses on the need for an initial nursing assessment<br />
before any action is taken on necessary hygiene needs (Holmes 1993, Turner 1996, Longhurst<br />
1998). However, the literature suggests that nurses lack a tangible knowledge base (Turner 1996,<br />
Holmes 1993, Kite <strong>and</strong> Pearson 1995); therefore assessments are poor, <strong>and</strong> are using<br />
inappropriate interventions. The assessment guides available have not been validated or proven<br />
reliable which therefore limits the clinical usefulness of these tools (Turner 1996, Longhurst 1998).<br />
For the purposes of developing a tool to be used in assessment, we as a group have chosen to<br />
develop Eiliers et al (1998) oral assessment tool. This tool was chosen as it was easy to follow,<br />
simple to underst<strong>and</strong>, <strong>and</strong> could easily be adapted for use in various clinical settings. The tool<br />
takes the form of a flow chart. The tool lacks sufficient detail, which is an argument supported by<br />
Holmes (1993). However, for the purpose of setting our guidelines, we have adapted it for our<br />
needs.<br />
In order to be user friendly, the flow chart, by using pointers of describing the condition of the <strong>mouth</strong><br />
<strong>and</strong> to aid the nurse in deciding appropriate action by following the appropriate arrows returning<br />
always to the beginning to repeat the assessment.
• STANDARD MOUTH CARE<br />
Page 10 of 21<br />
REF: PAT/PA 17 v.1<br />
From the literature reviewed, the authors recognise the importance of regular oral hygiene (Turner<br />
1995, Buglass 1995, Thurgood 1994, Kite <strong>and</strong> Pearson 1995). Buglass (1995) argues that<br />
frequency is more important than the agents used.<br />
Basic st<strong>and</strong>ard <strong>mouth</strong> <strong>care</strong> – (Literature states that the frequency of carrying out basic <strong>mouth</strong> <strong>care</strong><br />
is more important than the agents which are used to facilitate <strong>mouth</strong> <strong>care</strong>) Buglass EA 1995 Oral<br />
Hygiene British Journal of Nursing 4 (a) 516-519. Guidelines for Oral Care BDA April 2000.<br />
Guidelines for Record Keeping (2002). London Nursing <strong>and</strong> Midwifery Council.<br />
There is however, no general agreement regarding how frequently <strong>care</strong> should be given or the tools<br />
<strong>and</strong> agents which should be used. (Buglass 1995). For the purpose of our guidelines we have<br />
agreed st<strong>and</strong>ard <strong>care</strong> entails 12 hourly tooth brushing using a soft brush <strong>and</strong> toothpaste as research<br />
suggests the massaging effect of a soft brush stimulates mucosa promoting healthy gums. It is also<br />
the most effective way to loosen debris <strong>and</strong> remove plaque without causing trauma providing that<br />
<strong>care</strong> is taken (Thurgood 1994), Ransier et al 1995, Kite <strong>and</strong> Pearson 1995). Rinsing well with warm<br />
water is important as any remaining toothpaste may have a drying effect.<br />
Toothpaste gives a pleasant taste; always use a fluoride paste or Corsodyl gel if gingivitis is<br />
present.<br />
For patients with dentures the literature states all dentures should be removed overnight to prevent<br />
shrinkage. Debris must be removed as c<strong>and</strong>ida may be present <strong>and</strong> be harboured in the dentures<br />
therefore prevents introducing/ reintroducing infection. Dentures should be stored in a clean, dry<br />
container.<br />
Evidence suggests reassessment of the oral cavity should occur every 12 hours to ensure ongoing<br />
<strong>care</strong> is maintained. The flowchart should be used to aid assessment.<br />
Patient Requiring Assistance<br />
Often patients require assistance with oral hygiene. St<strong>and</strong>ard <strong>mouth</strong> <strong>care</strong> should be maintained. In<br />
addition, water soaked swabs may be required to keep the <strong>mouth</strong> moist. Suction may also be<br />
required to remove excess secretions. The use of soft paraffin ointment to the lips will keep them<br />
moist <strong>and</strong> prevent them from drying <strong>and</strong> cracking. (Turner 1995).<br />
Somerville (1999) suggests nurses, in particular intensive <strong>care</strong> nurses, are fearful of using tooth<br />
brushes especially in intubated patients preferring to the use of sponge sticks. However, this is not<br />
effective in the removal of plaque <strong>and</strong> debris. There is also the danger of the sponge becoming<br />
separated from the stick. Therefore sponge sticks are not recommended.<br />
Ulceration<br />
If ulceration is present, but there is no c<strong>and</strong>ida coating the tongue teeth or mucosa, Difflam<br />
<strong>mouth</strong>wash should be used in addition to st<strong>and</strong>ard <strong>mouth</strong> <strong>care</strong>. Difflam enhances oral <strong>care</strong> as it<br />
contains a topical anaesthetic <strong>and</strong> has anti-inflammatory <strong>and</strong> anti-microbial properties (Thurgood<br />
1994). However, it has numbing analgesic effect <strong>and</strong> must be prescribed by medical staff.
Coated Tongue, Teeth or Mucosa<br />
Page 11 of 21<br />
REF: PAT/PA 17 v.1<br />
If the tongue, teeth or mucosa are coated <strong>and</strong> c<strong>and</strong>ida is present, anti-fungal preparations must be<br />
used along with st<strong>and</strong>ard <strong>care</strong> <strong>and</strong> Difflam <strong>mouth</strong> wash. Nystatin or amphoterecin act on the<br />
c<strong>and</strong>ida. These must also be prescribed by medical staff. When c<strong>and</strong>ida is present it may also be<br />
harboured in the patient’s dentures. (Buglass 1989). The Trust Infection Control Team suggests<br />
brushing dentures at least four hourly in addition to the half hour soaking in milton to reduce this<br />
problem.<br />
If there is no c<strong>and</strong>ida present <strong>care</strong>fully brushing the tongue with chlorhexidene solution <strong>and</strong> the<br />
teeth with corsodyl gel is suggested. The acts by preventing the development <strong>and</strong> build-up of<br />
plaque <strong>and</strong> also has an anti-microbial effect (Kite <strong>and</strong> Pearson 1995, Thurgood 1994). Pineapple<br />
chunks contain a proteloytic enzyme, annase, which helps remove adherent coatings any may be<br />
used to remove the coating (Regnard 1898). Vitamin C tablets work by having an effervescent<br />
effect when placed on the tongue also aid in removing coating however there is limited research on<br />
its effect. Care must be taken in patients receiving radiotherapy/chemotherapy.<br />
Dry Mouth (Xerostomia) Saliva products - see below<br />
If the patient’s <strong>mouth</strong> is dry, it is important to treat the cause. Thurgood (1994) states that artificial<br />
saliva can be used without any detrimental effect <strong>and</strong>, is particularly useful in patients with impaired<br />
saliva production. Thurgood (1994) <strong>and</strong> Buglass (1989) suggest ice cubes, pineapple chunks <strong>and</strong><br />
ice lollies may provide comfort as will using soft paraffin to moisten lips. Frequent sips of cold<br />
water, milk or sugar free, non acidic cool drinks will help. Gel Clair provides a protective coating if<br />
eating <strong>and</strong> drinking is painful.<br />
Xerostomia is the prime effect of severe <strong>and</strong> rapid dental decay (Gelbart 1998). Sweeney (1998)<br />
notes that, it can often lead to oral fungal infection. This is found in connective tissue complaints,<br />
such as Reiter’s syndrome, as well as in menopausal women <strong>and</strong> HIV patients.<br />
Painful Mouth<br />
If on assessment the patient has a painful <strong>mouth</strong> it is important to determine the cause. This could<br />
be due to ill fitting dentures, radiotherapy, chemotherapy, or infection. Topical analgesics are<br />
effective along with st<strong>and</strong>ard <strong>mouth</strong> <strong>care</strong> in relieving pain. Difflam as described earlier has an antiinflammatory<br />
effect. Bongela has a local numbing effect (Thurgood 1994)<br />
Mucositis (inflammation of the <strong>mouth</strong>) is painful <strong>and</strong> an extremely unpleasant side effect of some<br />
cancer treatments. It has an acute phase usually due to chemotherapy or radiotherapy to the oral<br />
cavity. Normal tooth brushing should continue using a soft toothbrush if possible; alternatively<br />
chlorhexidene <strong>mouth</strong> wash can be used. It should be used 3-4 times daily. It helps with plaque<br />
control although its value in reducing symptoms of mucositis is less clear. Very few therapies have<br />
been used in r<strong>and</strong>omised prospective trials. Recent <strong>evidence</strong> suggests that the use of an antibiotic<br />
lozenge may reduce the most severe symptoms of mucositis. Experimental <strong>evidence</strong> supports the<br />
use of Gel Clair in the first instance<br />
In normal saliva production we produce 1-2mls per minute. 80% is from the Parotid Gl<strong>and</strong>. Saliva is<br />
anti-bacterial <strong>and</strong> anti-fungal <strong>and</strong> helps maintain oral PH for food digestion.
Page 12 of 21<br />
REF: PAT/PA 17 v.1<br />
Parotid function can be partially maintained by radiotherapy delivery that spares the contralateral<br />
gl<strong>and</strong>. The symptoms of Xerostomia can be helped by:<br />
i) Frequent sips of cold water/milk or other sugar free non acidic cool drinks<br />
ii) Saliva substitutes:<br />
Saliva Orthana ) both contain flouride <strong>and</strong> are<br />
) appropriate saliva<br />
) substitutes for dentate<br />
) people<br />
* Oral Balance Mouthwash<br />
Gl<strong>and</strong>osane <strong>mouth</strong>wash<br />
Salivix Pastilles ) for edentate patients only. These<br />
) are acidic <strong>and</strong> consequently will<br />
) rapidly erode natural teeth <strong>and</strong><br />
) cause tooth sensitivity.<br />
* For these materials to be effective Oral Balance dentifrice must be<br />
substituted for conventional toothpaste. The sodium lauryl<br />
succinate in toothpaste destroys the bulking agent within the Oral<br />
Balance saliva replacement gel.<br />
iii) Flavourless salad oil or dietary fat at night time lubricates the lips <strong>and</strong> tongue<br />
iv) Sugar free chewing gum stimulates saliva production (e.g. Orbit).<br />
v) Salivary stimulants can cause unwanted side effects that are often more distressing than<br />
the Xerostomia. The following have been used:<br />
Pilocarpoine – ophthalmic drops – 5-10mgs. 3 times daily.<br />
Whilst this stimulates salivary secretion it cannot resurrect a damaged gl<strong>and</strong> i.e. parotids<br />
in radiotherapy for head <strong>and</strong> neck cancer patients.<br />
Anatholetrithione ( Sialor-sulfarlem, latema) 1-2 tablets can be used 3 times daily.<br />
Pilocarpine <strong>and</strong> Anetholetrithione can be combined<br />
vi) Ripe bananas are a good lubricant; however, they should be avoided for dentate patients<br />
because of their high refined sugar content.<br />
• When <strong>mouth</strong> is too painful for cleaning <strong>and</strong> <strong>mouth</strong>wash cannot be used, the oral<br />
tissues should be swabbed with Polygon oral swabs (Rochaille Medical Ltd<br />
Cambridge UK) or gauze.soaked in chlorhexidene 3 – 4 times daily. (Fitton 1989)<br />
• Hydration <strong>and</strong> nutrition are frequently reported as important factors in oral hygiene<br />
(Thurgood 1994). Reduced oral intake has the effect of reducing the production of<br />
saliva thus the cleansing effect of saliva on the tongue <strong>and</strong> the mucous membrane is<br />
lost. Much of the literature notes that a factor in the control of bacterial growth is the<br />
production of saliva. Saliva contains several anti-bacterial factors which suppress<br />
bacterial <strong>and</strong> fungal colonisation. Also, the mechanical action of mastication<br />
promotes the washing action of saliva, <strong>and</strong> helps prevent the firm attachment of<br />
micro organisms to the surfaces (Somerville 1999).
Page 13 of 21<br />
REF: PAT/PA 17 v.1<br />
• Gilbart (1998) cites certain systemic illnesses that are associated with Aphthous<br />
ulcers. These include Crohn’s disease, sarcoidosis <strong>and</strong> coelic disease. Sweeney<br />
(1998) adds other various factors that contribute to ulceration. For example,<br />
haematological <strong>and</strong> other deficiency states, (iron or vitamin B12 deficiency,<br />
anaemia), endocrine problems, stress, allergy, autoimmune diseases <strong>and</strong> HIV.<br />
• Oral thrush is commonly found in diabetes, as a side effect of antibiotic or radiation<br />
treatment, <strong>and</strong> as a result of insufficient saliva. C<strong>and</strong>ida is also associated with HIV.<br />
• Inflammation of the gingival (gingivitis), often with minor bleeding, is caused by poor<br />
hygiene <strong>and</strong> consequently a build up of plaque (Gelbart 1998). It is the first stage of<br />
periodontitis. Due to the highly vascular nature of the mucosal tissue in the gums,<br />
tissue destruction can lead to the formation of a communication channel between the<br />
bacteria in the plaque <strong>and</strong> the bloodstream (Somerville 1999). Additionally,<br />
inflammation of this area can lead to tissue <strong>and</strong> bone destruction <strong>and</strong> then to tooth<br />
loss (Kite <strong>and</strong> Pearson 1995).<br />
• Patients with oral cancers tend to be elderly, wear dentures <strong>and</strong> seldom visit their<br />
dentists (Gelbart 1998). Combined high intake of tobacco <strong>and</strong> alcohol are particular<br />
risk factors. Health education <strong>and</strong> health promotion is paramount to reduce this risk<br />
<strong>and</strong> improve oral health.<br />
INFORMATION FOR ‘AT RISK’ GROUPS<br />
Oncology <strong>and</strong> Haematology<br />
Much of the literature surrounding oral <strong>care</strong> in oncology is United States <strong>based</strong> <strong>and</strong> involves small<br />
samples. It is therefore worthy of caution when generalising to the population as a whole.<br />
Incidence<br />
Both radiotherapy <strong>and</strong> chemotherapy can cause specific oral problems. The oral mucosal cells are<br />
extremely vulnerable to the effects of antineoplastic therapy. Oral complications increase in severity<br />
if the patient is receiving concurrent radiotherapy <strong>and</strong> chemotherapy.<br />
The incidence of oral complications in adults undergoing chemotherapy for solid tumours ranged<br />
between 12 – 40% (Niedwig et al 1992, Graham et at 1993). However Holmes (1997) states that<br />
48% to 75% of patients receiving 5Fu report Stomatitis. Dodd (1996) agrees that the figure for 5Fu<br />
induced Stomatitis is 75%.<br />
Patients undergoing radiotherapy to the Head <strong>and</strong> Neck routinely have oral complications. (Ganley<br />
1996).<br />
These figures indicate the extent of the problem in this group of patients.<br />
Patho-Physiology<br />
Visible signs of inflammation <strong>and</strong> oral ulceration can be observed 7-14 days following<br />
chemotherapy/radiotherapy (Madaya, 196a), although Graham et al (1993) report effects as early<br />
as 3 days into treatment.
Page 14 of 21<br />
REF: PAT/PA 17 v.1<br />
Pain caused by Stomatitis initially presents as a burning sensation (Graham et al 1993). This<br />
progresses to a general sensitivity to hot <strong>and</strong> cold (Nieweg et al, 1992). In severe cases there may<br />
be infection present.<br />
Chemotherapy<br />
Cytotoxic drugs inhibit cellular replication. Thus the production of new cells is insufficient to<br />
maintain mucosal integrity. Stomatitis may result from damage o the mucous membranes of the<br />
<strong>mouth</strong> <strong>and</strong> is largely unpreventable.<br />
Problems occur either due to direct effects of chemotherapy or indirect effects of myelosuppression<br />
or immunosuppression when neutropenia renders the patient vulnerable to infection. Therefore any<br />
drug causing myelosuppression may indirectly cause Stomatitis.<br />
Thinning <strong>and</strong> ulceration of the mucus membrane occurs within four to seven days of the<br />
commencement of chemotherapy. Fluid <strong>and</strong> food intake are also reduced, due to nausea, vomiting<br />
<strong>and</strong> general malaise. This compounds the problem as debris <strong>and</strong> plaque accumulate in the <strong>mouth</strong><br />
(Turner 1996). Thus the mucus membrane is ineffective to invasive infections <strong>and</strong> there is an<br />
increased risk of gingivitis <strong>and</strong> dental caries. The nausea <strong>and</strong> vomiting may also result in<br />
malnutrition <strong>and</strong> therefore poor tissue healing <strong>and</strong> repair. However, Stomatitis tends to be self<br />
limiting <strong>and</strong> resolves once treatment has completed. Indirect effects occur within 12-16 days usually<br />
coinciding with the nadir period when patients are neutropenic. The mucosa, which is already<br />
compromised, becomes more susceptible to bleeding <strong>and</strong> infection. Healing occurs as the<br />
neutorphil count returns to normal (Holmes 1997).<br />
Most oral infections amongst chemotherapy patients originate from their own microflora, with the<br />
oral cavity acting as the primary source in the development of septicaemia in immunosuppressed<br />
patients. (Eilers et al 1988, Holmes 1997). By reducing the number of microbes in the oral cavity<br />
patients may be able to reduce their risk of acquiring a systemic infection (Ransier et at 1995).<br />
Patients with impaired renal <strong>and</strong>/or hepatic function are at an increased risk of oral complications<br />
due to the reduced metabolism <strong>and</strong>/or excretion of antineoplastic drugs (Holmes 1997). This is<br />
thought to be because persistent blood or tissue levels of cytotoxic agents delay re-epitheliaisation.<br />
Effects on the Oral Cavity Associated With Chemotherapy (Holmes 1997)<br />
Generalised effects<br />
• Xerostomia<br />
• Altered taste perception<br />
Inflammatory changes<br />
• Mucositis<br />
• Ulceration<br />
Infectious Complications<br />
• Periodontal infection/disease<br />
• Dental caries<br />
• Viral infections (e.g. herpes simplex)<br />
• Fungal infections (e.g. c<strong>and</strong>ida albicans)
Indirect effects of secondary to myelosuppression<br />
• Gingival bleeding<br />
• Atrophy of tongue <strong>and</strong> buccal mucosa<br />
Radiotherapy<br />
Page 15 of 21<br />
REF: PAT/PA 17 v.1<br />
Radiotherapy to the head <strong>and</strong> neck can also cause localised problems. The oral mucosa is very<br />
sensitive to the radiation because of its short cell life. This reduction in cell renewal results in<br />
mucosal atrophy <strong>and</strong> ulceration. Hypertrophy of the salivary gl<strong>and</strong>s follows radiotherapy treatment<br />
<strong>and</strong> reduces the salivary flow, causing Xerostomia <strong>and</strong> dysphagia (Turner 1996). Xerostomia (dry<br />
<strong>mouth</strong> due to failure of salivary secretion) is the most frequently reported side effect associated with<br />
radiotherapy to the Head <strong>and</strong> Neck. It may be permanent or temporary. The protective cleansing of<br />
the mucus membranes <strong>and</strong> teeth is lost, as is the acidic protective barrier against bacteria.<br />
Oral complications can also affect the taste buds <strong>and</strong> the ability to swallow, therefore impinging on<br />
fluid <strong>and</strong> nutritional intake (Graham et al 1993, Dudjak 1987).<br />
Additionally, radiotherapy to the head <strong>and</strong> neck can affect the structures can occur of the <strong>mouth</strong>,<br />
including oral musculature, alveolar bone <strong>and</strong> developing teeth. Damage to teeth up to three years<br />
following treatment (Gelbart 1998).<br />
Older Patients<br />
The aging process, even when uncomplicated by illness, produces a multitude of changes in the<br />
structure <strong>and</strong> function of the body which may combine to make maintenance of oral health difficult.<br />
Age related changes to oral cavity<br />
• Gingiva may recede, causing teeth to loosen, <strong>and</strong> forming pockets for food to sit it, which will<br />
increase the risk of caries.<br />
• The root pulp of the tooth fibroses <strong>and</strong> the teeth become more brittle, increasing the risk of<br />
fractures, particularly in the base of the tooth.<br />
• Mucosal atrophy <strong>and</strong> thinning results in a higher likelihood of traumatic damage <strong>and</strong><br />
ulceration.<br />
• Changes in the shape of the bony ridges may result in ill fitting dentures, which themselves<br />
may be the cause of traumatic damage.<br />
• Saliva production decreases with age, sometimes dropping to 1/3 of original adult<br />
production; so the patient may suffer from Xerostomia. As saliva also plays a part in<br />
controlling bacteria <strong>and</strong> fungal growth within the oral cavity, the patient will also be more<br />
prone to C<strong>and</strong>idiasis.<br />
• The tongue atrophies causing reduction in taste sensation (Dysgensia).<br />
• Swallowing time slows; food may not be effectively cleared from the <strong>mouth</strong> which will<br />
enhance the development of plaque.<br />
Other age related physiological changes which may relate to the maintenance of a healthy oral<br />
cavity<br />
.<br />
• Decreased response to painful stimuli <strong>and</strong> an increasing tolerance to pain may<br />
increase the risk of insult to the oral cavity.<br />
• Muscle tremors associated with degeneration of the extrapyrimidal system; <strong>and</strong><br />
deterioration of cartilage surface at joints; <strong>and</strong> the formation of bone spurs may all<br />
limit patients functional ability to self <strong>care</strong> for their <strong>mouth</strong> <strong>and</strong> teeth.
Page 16 of 21<br />
REF: PAT/PA 17 v.1<br />
• A reduction in the amount of intracellular fluid causes an increased risk of<br />
dehydration leading to thickened saliva, or dry <strong>mouth</strong>.<br />
• Cognitive motivation for learning lessens; attention span may be reduced; both of<br />
which may reduce patients’ ability to <strong>care</strong> effectively for their <strong>mouth</strong> <strong>and</strong> teeth.<br />
Elipoulous (1997) suggests “an underst<strong>and</strong>ing of common ageing changes is essential to ensure<br />
competent gerontological nursing practices”<br />
In addition to these physiological processes, a number of abnormal conditions, which may present<br />
at any time but are common in the elderly patient, may occur, <strong>and</strong> these should be considered in<br />
combination with the normal changes of ageing. The following list is not comprehensive but<br />
provides some examples.<br />
Other conditions:<br />
• Cerebrovascular accident: depending on the area of the brain affected, may affect<br />
swallowing, speech, general functional ability; cognitive ability, all of which, as already<br />
discussed, have a bearing on the condition of the oral cavity.<br />
• Dementia: may cause reduced functional ability; patients may also experience a reduced<br />
appetite, <strong>and</strong> are at risk of becoming dehydrated.<br />
• Parkinson’s disease: Reduced function <strong>and</strong> some associated dementia may occur.<br />
• Depression: can cause loss of appetite, reduced motivation to self <strong>care</strong> <strong>and</strong> to take oral<br />
fluids.<br />
• Drug therapy: as a response to abnormal conditions. Xerostomia is a side effect of a<br />
number of drugs, including anxiolytics, antidepressants, antipsychotics, (particularly<br />
anticholinergic drugs), diuretics (due to fluid/electrolyte intolerance). Antibiotics to treat<br />
infection may results in oral thrush. See Drugs <strong>and</strong> Treatments table, page 5.
REFERENCES<br />
Page 17 of 21<br />
REF: PAT/PA 17 v.1<br />
• Buglass E A (1995) Oral Hygiene, British Journal of Nursing, 4(9): 516-519<br />
• Dodd, M et al (1996) R<strong>and</strong>omised Clinical Trial of Chlorhexadine Versus Placebo for<br />
Prevention of Oral Mucositis in Patients Receiving Chemotherapy. Oncology Nursing Forum,<br />
23(6): 921-927<br />
• Dudjak (1994) Mouth <strong>care</strong> for mucositis due to radiation therapy. Cancer Nursing, 10(3):<br />
131-140.<br />
• Eilers, J et al (1998) Development, Testing, <strong>and</strong> application of the Oral Assessment Guide.<br />
Oncology Nursing Forum, 15(3): 325-330.<br />
• Elipoulous, C (1997) Gerontological Nursing (4 th Edition) Ed Lippincote (Philadelphia).<br />
• Ganley, B (1996) Mouth Care for the Patient Undergoing Head <strong>and</strong> Neck Radiation Therapy:<br />
A Survey of Radiation Oncology Nurses. Oncology Nursing Forum, 23 (10): 1619-1623.<br />
• Gelbart, M. (1998) All Mouth. Nursing Times, November 18, 94(46): 26-28<br />
• Graham, K. et all (1993) Reducing the incidence of Stomatitis using a quality assessment<br />
<strong>and</strong> improvement approach. Cancer Nursing, 16(2): 117-122<br />
• Holmes, S. (1997) Cancer Chemotherapy – A Guide for Practice, Second Edition Asset<br />
Books, Surrey, Chapter 11; 190-199.<br />
• Holmes, S. (1996) Nursing Management of oral <strong>care</strong> in older patients, nursing Times 92(9):<br />
37-39.<br />
• Kite, K & Pearson, L (1995) A rationale for <strong>mouth</strong> <strong>care</strong>: the integration of theory with<br />
practice. Intensive <strong>and</strong> Critical Care Nursing, 11: 71-76.<br />
• Madeya, M. (1996a) Oral complications From Cancer Therapy: Part 1 – Pathophysiology<br />
<strong>and</strong> Secondary Complications. Oncology Nursing Forum, 23(5): 801-807.<br />
• Nieweg, R. et al (1992) Nursing <strong>care</strong> for oral complications associated with chemotherapy.<br />
Cancer Nursing, 15(5): 313-321.<br />
• Pearson, L S (1996) A Comparison of the Ability of Foam Swabs <strong>and</strong> Toothbrushes to<br />
Remove Dental Plaque: Implications for Nursing Practice, Journal of Advance Nursing, 213:<br />
62-69.<br />
• Ransier, A. et al (1995) a combined analysis of a toothbrush, foam brush, <strong>and</strong> a<br />
chlorhexidene-soaked foam brush in maintaining oral hygiene. Cancer Nursing, 18(5): 393-<br />
396.<br />
• Regnard, C & Fitton, S (1989) Mouth <strong>care</strong>: a flow diagram. Palliative Medicine, 3: 67-69<br />
• Regnard, C et al (1997) Mouth <strong>care</strong>, skin <strong>care</strong>, <strong>and</strong> lymphoedema. BMJ, 18 October, 315,<br />
1002-1005.<br />
• Somerville, R. (1999) Oral <strong>care</strong> in intensive <strong>care</strong> setting: a case study. Nursing in Critical<br />
Care, 41(1): 7-13<br />
• Sweeney, P. (1998) Mouth <strong>care</strong> in nursing – Part 1. Common oral conditions. Journal of<br />
Nursing Care, spring, 4-7.<br />
• Thurgood, G. (1994) Nurse maintenance of oral hygiene. British Journal of Nursing, 3(7):<br />
332-353<br />
• Turner, G. (1996) Oral <strong>care</strong>. Nursing St<strong>and</strong>ard, April 3, 10(28): 51-56.<br />
• UKCC (1998) Guidelines for Records <strong>and</strong> Record Keeping. UKCC:London<br />
• White, R. (2000) Nurse assessment of oral health: a review of practice <strong>and</strong> education. British<br />
Journal of Nursing, 9(5): 260-266.
• BACKGROUND TO RESEARCH<br />
Key Words<br />
Page 18 of 21<br />
REF: PAT/PA 17 v.1<br />
“CANCER, ORAL CARE, ORAL ASSESSMENT, ORAL ASSESSMENT TOOL, ORAL HYGENE<br />
AND MOUTH CARE WERE USED”<br />
Literature Review<br />
The literature review in relation to <strong>mouth</strong> <strong>care</strong> focuses on the need for an initial nursing assessment.<br />
(Holmes 1993, Turner 1996, Lomghurst 1998) It also highlights that there is a lack of a tangible<br />
knowledge base in this field. (Turner 1996, Holmes 1993, Kite <strong>and</strong> Pearson 1995). However authors<br />
recognise the importance of regular oral hygiene. Buglass (1995) argues that frequency is far more<br />
important than the agents used. However there is no general agreement regarding frequency of<br />
<strong>care</strong>, agents to be used or recommended assessment tool.<br />
For the purpose of this paper it was intended to adapt an approved assessment tool (RCS <strong>and</strong><br />
BDSH 2001) to enhance <strong>mouth</strong> <strong>care</strong> practice. Whilst it is agreed that the assessment tool may be<br />
useful as a research outcome measure it is open to criticism in that it produces a score rather than a<br />
diagnosis. However if used with a flow guide to oral assessment <strong>and</strong> <strong>care</strong> it is thought that this will<br />
highlight any problems, st<strong>and</strong>ardise <strong>care</strong> <strong>and</strong> give advice on treatments.
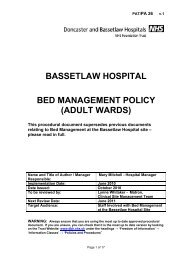
ORAL ASSESSMENT TOOL<br />
Page 19 of 21<br />
REF: PAT/PA 17 v.1<br />
Appendix 1<br />
Please insert appropriate number in relevant box <strong>based</strong> on your clinical examination of the patient.<br />
Contact the Medical Team for further advice on the management of patients with scores of 3.<br />
PATIENT NAME: ____________________________ PLEASE DATE AND SIGN<br />
METHOD OF<br />
1 2 3 4 5 6 7<br />
ASSESSMENT<br />
ASSESSMENT DATE:<br />
VOICE<br />
3 = difficult/painful speech<br />
2 = deeper/raspy<br />
1 = normal<br />
SWALLOW<br />
Converse with the patient.<br />
3 = unable to swallow<br />
2 = painful<br />
1 = normal<br />
LIPS AND ANGLE OF MOUTH<br />
Ask patient to swallow.<br />
3 = ulcerated/with or without bleeding Observe <strong>and</strong> palpate the<br />
2 = dry/cracked<br />
1 = normal<br />
TONGUE<br />
tissues<br />
3 = blistered/cracked<br />
Observe the appearance of the<br />
2 = coated or loss of papillae<br />
1 = smooth, pink, moist<br />
SALIVA<br />
tissues<br />
3 = Absent<br />
Insert tongue depresser <strong>and</strong><br />
2 = thick/ropy<br />
observe tongue <strong>and</strong> floor of<br />
1 = watery<br />
MUCOUS MEMBRANES/GINGIVA<br />
<strong>mouth</strong><br />
3 = Ulceration/bleeding – gentle pressure Observe the appearance of the<br />
2 = c<strong>and</strong>idal infection suspected –<br />
reddened/coated or white patches<br />
1 = pink <strong>and</strong> moist<br />
ORAL CLEANSING COMPLIANCE<br />
tissues<br />
3 = unable to clean<br />
Observe tooth brushing/denture<br />
2 = cleans but needs help<br />
1 = no difficulties - self <strong>care</strong><br />
cleaning<br />
(Adapted from Eilers, J, Berger, A, Peterson, M. Development, testing <strong>and</strong> application of the Oral Assessment Guide. Ongology Nursing Forum 15 (3): pp 325-330a: 1988) Copyright Host<br />
Defence Unit Great Ormond Street Hospital Trust.
NAME:<br />
UNIT NUMBER:<br />
(Use with Oral assessment tool)<br />
DATE/<br />
TIME<br />
<strong>Doncaster</strong> <strong>and</strong> <strong>Bassetlaw</strong> Hospitals NHS Foundation Trust<br />
SCORE<br />
ORAL HYGIENE RECORD CHART<br />
ACTION TAKEN<br />
INCLUDING PRODUCT<br />
USED<br />
Page 20 of 21<br />
REF: PAT/PA 17 v.1<br />
EVALUATION<br />
Appendix 2
The Oral Cavity <strong>and</strong> Oropharynx<br />
Page 21 of 21<br />
REF: PAT/PA 17 v.1<br />
Appendix 3