Employment Standards Claim Form
Employment Standards Claim Form
Employment Standards Claim Form

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Employment</strong> <strong>Standards</strong> <strong>Employment</strong> <strong>Standards</strong><br />
<strong>Claim</strong> <strong>Form</strong><br />
Ministry of Labour
Your Name: Telephone No.<br />
Please be sure you have read the “Before You Start” booklet before filling out the <strong>Claim</strong> <strong>Form</strong>.<br />
Use a pen to fill out the form. PRINT as clearly as possible. Please use blue or black ink only.<br />
Collective Agreement<br />
Detailed instructions on how to fill out this section can be found on page 9 of the <strong>Claim</strong> Guide.<br />
Were you covered by a collective agreement when the matter you are claiming about happened? *<br />
Yes No Do not know<br />
If “Yes”, contact your union representative for assistance. Generally, you cannot file a claim with the Ministry of Labour.<br />
Section A1 – Information About Your Experience Contacting Your Employer<br />
Detailed instructions on how to fill out Sections A1 through A4 can be found on pages 10 to 13 of the <strong>Claim</strong> Guide.<br />
Did you already contact your employer? *<br />
Yes If “Yes”, please GO TO section A2.<br />
No If “No”, please GO TO section A3.<br />
Section A2 – Yes, I Tried to Contact my Employer<br />
How did you contact your employer? (Choose all that apply) *<br />
Phone In person By letter Email<br />
Other:<br />
When did you try to contact your employer? *<br />
Note: Please wait a few days to give your employer a chance to get back to you (e.g. 7 to 10 days)<br />
What <strong>Employment</strong> <strong>Standards</strong> issue(s) did you contact your employer about? *<br />
What did your employer say? (Please check one box and provide some details about your employer’s response in the<br />
space provided) *<br />
Refused to help Did not say anything Other<br />
Explain:<br />
Section A3 – No, I Have Not Contacted my Employer<br />
Your claim may still be investigated if you have a good reason for not contacting your employer. The following are generally<br />
considered to be good reasons for not contacting your employer. Please check the box(es) that apply to you: *<br />
You already tried to contact your employer.<br />
The money owed to you is from 5 months ago or more<br />
(there are time limits to file).<br />
Your workplace has closed down.<br />
Your employer has gone bankrupt.<br />
You are afraid to do so.<br />
Your issue does not involve money.<br />
MOL-ES-002E (2010/08)<br />
You are or were working as a live-in caregiver.<br />
You have difficulty with communicating in the language<br />
spoken by your employer.<br />
You are a young employee.<br />
You have a disability that makes it difficult for you to<br />
contact your employer.<br />
There is any reason relating to a ground under the<br />
Ontario Human Rights Code.<br />
1
Your Name: Telephone No.<br />
Other (explain):<br />
Section A4 – Information About You<br />
Last (Family) Name * Mr. Miss<br />
Mrs. Ms<br />
First (Given) Name *<br />
Mailing Address *<br />
Street Number *<br />
Rural Route<br />
Province/State *<br />
MOL-ES-002E (2010/08)<br />
Suffix (e.g. A)<br />
PO Box<br />
Home Telephone Number<br />
Daytime Telephone Number<br />
Email Address<br />
Commonly Used First Name<br />
(if applicable)<br />
Street Name *<br />
Postal Station<br />
Postal Code/Zip Code *<br />
Previous Last (Family) Name (if your employer knows you by<br />
that name)<br />
City/Town *<br />
Country<br />
Middle<br />
Initial(s)<br />
Type<br />
Cell Telephone Number<br />
Students Only: Date of Birth<br />
(yyyy/mm/dd)<br />
Direction<br />
Who can we leave a message with concerning your claim at the daytime telephone number?<br />
What is the best way to reach you between 9:00 am and 5:00 pm on weekdays?<br />
Home Telephone Number Cell Telephone Number Daytime Telephone Number Email Address<br />
Other Mailing Address<br />
Same as above<br />
Street Number<br />
Rural Route<br />
Province/State<br />
Suffix (e.g. A)<br />
PO Box<br />
Street Name<br />
Postal Station<br />
Postal Code/Zip Code<br />
City/Town<br />
Country<br />
Type<br />
Direction<br />
Do you authorize anyone to act on your behalf? (for example family member, friend, legal counsel)<br />
Yes (please fill in the contact information section below)<br />
Name of the person<br />
Relationship to you<br />
Unit<br />
Unit<br />
Telephone Number<br />
2
Your Name: Telephone No.<br />
Section B1 – Information about the Employer<br />
Detailed instructions on how to fill out Section B1 can be found on pages 13 to 15 of the <strong>Claim</strong> Guide.<br />
IMPORTANT: Is your claim submission related to a temporary help agency? *<br />
Yes If “Yes”, please provide information about the temporary help agency in sections B1 and B2.<br />
No<br />
Employer’s Business Name (Please provide the legal name or name of company) *<br />
If this business operates using any other name(s), please provide these name(s)<br />
Type of Business<br />
Business Number (This is in reference to your employer’s Canada Revenue Agency Business Number. See page 26 of<br />
the <strong>Claim</strong> Guide for more information)<br />
This business is: Still operating No longer operating In receivership or bankruptcy Do not know<br />
If in receivership/bankruptcy, provide the receiver or trustee’s name<br />
If your employer is bankrupt or in receivership, and your employment has been terminated, please consult the federal<br />
government’s Wage Earner Protection Program website www.servicecanada.gc.ca/eng/sc/wepp/index.shtml for more<br />
information on money you may be entitled to receive.<br />
Address of Employer (For tips on finding your employer’s address, GO TO page 14 of the <strong>Claim</strong> Guide) *<br />
Street Number *<br />
Rural Route<br />
Province/State *<br />
MOL-ES-002E (2010/08)<br />
Suffix (e.g. A)<br />
PO Box<br />
Street Name *<br />
Postal Station<br />
Postal Code/Zip Code *<br />
City/Town *<br />
Country<br />
I don’t know my employer’s address (Please explain in section D2).<br />
Address of the location where you work(ed)<br />
Same as above<br />
Street Number<br />
Rural Route<br />
Province<br />
Suffix (e.g. A)<br />
PO Box<br />
Street Name<br />
Postal Station<br />
Additional Information about the Employer<br />
Employer’s Email Address<br />
Name of your supervisor, or contact<br />
City/Town<br />
Postal Code<br />
Employer’s Website<br />
Type<br />
Type<br />
Employer’s Telephone Number<br />
Direction<br />
Direction<br />
Unit<br />
Unit<br />
Employer’s Fax Number<br />
3
Your Name: Telephone No.<br />
Section B2 – Your Work History with the Employer<br />
Detailed instructions on how to fill out Section B2 can be found on pages 15 to 17 of the <strong>Claim</strong> Guide.<br />
NOTE: If you have no work history with the employer, leave this section blank. (See page 15 of the <strong>Claim</strong> Guide for<br />
more information about these situations)<br />
What was your job title? What kind of work did you do?<br />
Do you have a record of your hours of work? (e.g. in a diary or calendar) Yes No<br />
Did you work the same number of hours each day?<br />
No If “No”, please explain:<br />
Yes If “Yes”, please answer the following three questions:<br />
How many hours did you work each<br />
day?<br />
MOL-ES-002E (2010/08)<br />
How many days did you work each<br />
week?<br />
Total number of hours worked each<br />
week?<br />
Pay Period Weekly Every two weeks Twice a month Once a month<br />
Other (explain)<br />
How were you paid? Per hour Salary Commission Piecework<br />
Other (explain)<br />
Rate of pay before<br />
deductions (choose<br />
Per hour $ Per week $ Per annum (year) $<br />
one) Other (explain)<br />
When did you start working for this employer? Current status: *<br />
(yyyy/mm/dd)<br />
Still working for this employer<br />
Other (explain)<br />
Fired Laid Off Quit<br />
Last day you worked for this employer?<br />
(yyyy/mm/dd)<br />
Date notice of termination was received?<br />
(yyyy/mm/dd)<br />
Did you receive notice of termination before your last day of work?<br />
Yes No N/A<br />
The notice was:<br />
Written Oral I don’t know N/A<br />
4
Your Name: Telephone No.<br />
IMPORTANT: Are you claiming that a client of the temporary help agency punished or threatened to<br />
penalize you for asking for or asking about your rights under the <strong>Employment</strong> <strong>Standards</strong> Act, 2000? *<br />
Yes If “Yes”, please fill out section C1 below.<br />
No If “No”, please GO TO section D1 on page 7.<br />
Section C1 – Reprisal: Information about the Client<br />
Detailed instructions on how to fill out Section C1 can be found on pages 18 to 19 of the <strong>Claim</strong> Guide.<br />
Client Business Name (Please provide the legal name or name of company) *<br />
If this business operates using any other name(s) please provide these name(s)<br />
Type of Business<br />
This client is: Still operating No longer operating In receivership/bankrupt Do not know<br />
If in receivership/bankruptcy, provide the receiver or trustee’s name<br />
Address of the Client Location Where You Work(ed) *<br />
Street Number * Suffix (e.g. A) Street Name *<br />
Rural Route<br />
Province *<br />
MOL-ES-002E (2010/08)<br />
PO Box<br />
Postal Station<br />
I don’t know the address of where I worked<br />
Additional Information about the Client<br />
Client Email Address<br />
Name of your supervisor, or other contact<br />
City/Town *<br />
Type<br />
Postal Code *<br />
Client Website<br />
Client Telephone Number<br />
Direction<br />
Unit<br />
Client Fax Number<br />
5
Your Name: Telephone No.<br />
Section C2 – Your Work History with the Client<br />
Detailed instructions on how to fill out Section C2 can be found on pages 19 to 20 of the <strong>Claim</strong> Guide.<br />
NOTE: If you have no work history with the Client, please GO TO section D1.<br />
What was your job title? What kind of work did you do for the client?<br />
Do you have a record of your hours of work? (e.g. in a diary or calendar) Yes No<br />
Did you work the same number of hours each day?<br />
No If “No”, please explain:<br />
Yes If “Yes”, please answer the following three questions:<br />
How many hours did you work each<br />
day?<br />
When did you start working for this client? (yyyy/mm/dd)<br />
MOL-ES-002E (2010/08)<br />
How many days did you work each<br />
week?<br />
Total number of hours worked each<br />
week?<br />
When did you finish working for this client? (yyyy/mm/dd)<br />
I am still working for the same client.<br />
6
Your Name: Telephone No.<br />
Section D1– Details About Your <strong>Claim</strong><br />
Detailed instructions on how to fill out Section D1 can be found on pages 20 to 25 of the <strong>Claim</strong> Guide.<br />
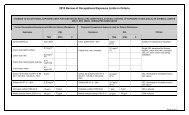
Please tell us which employment standard(s) you are claiming and provide an estimate of the amount you are<br />
owed. You will be asked to answer questions about each employment standard you are claiming in section D2.*<br />
<strong>Employment</strong> Standard Estimate Amounts ($)<br />
Unpaid Wages<br />
Overtime Pay<br />
Vacation Pay / Vacation Time<br />
Public Holidays / Public Holiday Pay<br />
Deductions from Wages<br />
Minimum Wage<br />
Termination Pay<br />
Severance Pay<br />
Temporary Help Agency charged prohibited fees<br />
Temporary Help Agency did not provide required information<br />
Temporary Help Agency restricted the Client from hiring you or<br />
providing you with references<br />
Limits on Hours of Work / Eating Periods / Rest Periods (between<br />
shifts, daily, weekly or biweekly)<br />
Leaves of Absence (Pregnancy, Parental, Family Medical, Organ<br />
Donor, Personal Emergency, Reservist)<br />
Reprisal by the Employer (which includes a Temporary Help Agency)<br />
Reprisal by the Client of the Temporary Help Agency:<br />
Check this box ONLY if you work(ed) for a temporary help agency AND<br />
if you are claiming a reprisal by the Client. Please ensure that you have<br />
completed Section C.<br />
Other (specify):<br />
MOL-ES-002E (2010/08)<br />
7
Your Name: Telephone No.<br />
Section D2 – Background Information About Your <strong>Claim</strong><br />
Detailed instructions on how to fill out Section D2 can be found on pages 25 to 30 of the <strong>Claim</strong> Guide.<br />
Tell us why you are filing a claim submission. To help tell your story, please see the questions on the next page.<br />
Please try your best to answer the questions in full sentences. You do not have to answer all the questions.<br />
Only answer the questions about the employment standard(s) you are claiming. For example, if your claim is<br />
about overtime pay and public holiday pay, answer the questions outlined under the headings “Overtime Pay”<br />
and “Public Holidays / Public Holiday Pay”. If there is other information you feel might help explain what<br />
happened, please tell us in this section.<br />
Provide as much relevant detail as possible about which employment standards have been violated, including<br />
the dates on which those violations occurred. If you need more space, please attach additional pages to your<br />
claim. Write your name on each page, and telephone number if possible. *<br />
MOL-ES-002E (2010/08)<br />
8
Your Name: Telephone No.<br />
Section D2 – Background Information About Your <strong>Claim</strong><br />
Please answer the questions that relate only to the employment standard(s) you are claiming in the space provided<br />
in D2. You do not have to answer all the questions. For example if your claim relates to overtime pay and public<br />
holidays, answer the questions under overtime and public holidays.<br />
Unpaid Wages Temporary Help Agency charged prohibited fees<br />
� What days/hours/work were you not paid for?<br />
� Were you unable to cash your pay cheque?<br />
� What is the amount of wages you are owed?<br />
� Please provide any other information you feel would<br />
clarify any disputes about the wages you are claiming.<br />
Overtime Pay<br />
� When were you not paid overtime?<br />
� Do you have an agreement that your employer will pay<br />
overtime after a certain number of hours? If yes, tell us<br />
the number of hours.<br />
Vacation Pay / Vacation Time<br />
� Did you not get vacation pay, vacation time or both?<br />
� Have you received any vacation pay or vacation time<br />
off? If yes, please indicate when you received it and how<br />
much time and/or pay you received.<br />
Public Holidays / Public Holiday Pay<br />
� For which holiday(s) did you not receive time off and/or pay?<br />
� Did you agree to work on the public holiday(s) in question?<br />
� Did you receive any substitute days off?<br />
� Did you work your shifts before and after the holiday(s)?<br />
If no, please explain why.<br />
Deductions from wages Leaves of Absence<br />
� What deductions were made?<br />
� Did you give your employer permission to make these<br />
deductions? If yes, explain.<br />
� How much was deducted and when?<br />
Minimum Wage<br />
� When were you not paid minimum wage?<br />
� How many hours do you normally work in each pay<br />
period, and how much do you usually get paid?<br />
MOL-ES-002E (2010/08)<br />
� What fees were charged?<br />
� What was the amount of fee(s) charged?<br />
� When were the fee(s) charged?<br />
Temporary Help Agency did not provide required<br />
information<br />
� What information did you not receive?<br />
� On what date should you have received this<br />
information?<br />
Temporary Help Agency stopped the Client from<br />
hiring you or providing you with references<br />
� Briefly explain what happened, and when.<br />
Limits on Hours of Work / Eating Periods / Rest<br />
Periods (between shifts, daily, weekly or biweekly)<br />
� Tell us about your hours of work issue.<br />
� Do you receive breaks or eating periods? If yes, how<br />
often do you take them and how long are they?<br />
� When did this issue happen?<br />
� What kind of leave of absence is your claim<br />
submission about?<br />
� Tell us the main events concerning your claim<br />
submission.<br />
Reprisal by the Employer (which includes a<br />
Temporary Help Agency)<br />
� Tell us what happened with your employer.<br />
� Tell us the main events that led to your employer<br />
threatening or penalizing you.<br />
Termination Pay and/or Severance Pay Reprisal by the Client of the Temporary Help Agency<br />
� Did you get any notice before your employment ended?<br />
If yes, how much?<br />
� Did you receive any money when your employment<br />
ended? If yes, how much?<br />
� Did your employer tell you why he/she ended your<br />
employment? If yes, please tell us.<br />
� If you quit, please explain why.<br />
� Please tell us the main events that led to your<br />
employment ending.<br />
� Tell us what happened with the client.<br />
� Tell us the main events that led to the client<br />
threatening or penalizing you.<br />
Other (specify)<br />
� Tell us about the employment standard(s) not already<br />
identified above–what happened, and when?<br />
9
Your Name: Telephone No.<br />
Section D3 – Supporting Documents<br />
Detailed instructions on Section D3 can be found on page 30 of the <strong>Claim</strong> Guide.<br />
Please tell us which of the following supporting documents you have. Once we review your claim<br />
submission, we will ask you to send photocopies of relevant documents to the Ministry of Labour.<br />
Please mark boxes with a check mark (�): *<br />
I have these<br />
documents<br />
MOL-ES-002E (2010/08)<br />
I do not<br />
have these<br />
documents<br />
Document(s)<br />
Business cards, letterhead, or job ads. These documents will have information about<br />
your employer’s address, phone number(s), email address and website.<br />
Pay stubs for the periods you are claiming you are owed wages (including overtime<br />
pay, vacation pay, public holiday pay, termination pay, severance pay, minimum<br />
wage, or where an employer unlawfully deducted money from your wages).<br />
Pay cheques, including those that have “bounced”, or are “NSF” (“non-sufficient<br />
funds”).<br />
Record of <strong>Employment</strong> form (ROE). This document will tell you the Employer’s<br />
Business Number. If you have already given your ROE to Human Resources and<br />
Skills Development Canada, contact them and ask for a photocopy (1-800-206-<br />
7218).<br />
Written contract of employment, if there is one.<br />
Records of the hours you have worked (e.g. time sheets, attendance records,<br />
calendar, diary, or notes).<br />
T4 Slips.<br />
Section E – <strong>Claim</strong>ant’s Declaration<br />
Documents related to a leave of absence (e.g. a medical certificate in the case<br />
of a family medical leave).<br />
Written notice of termination, if received.<br />
Any receipts, invoices, or cancelled cheques relating to fees charged by the<br />
Temporary Help Agency.<br />
Any other documents that help with the investigation.<br />
I declare that, to the best of my knowledge, this information is accurate.<br />
This claim must be signed and dated. *<br />
Name<br />
Signature Date (yyyy/mm/dd)<br />
10
MOL-ES-002E (2010/08)<br />
Ministry of Labour<br />
<strong>Employment</strong> <strong>Standards</strong> Program<br />
Collection, use and disclosure of personal information<br />
<strong>Employment</strong> <strong>Standards</strong> Act<br />
<strong>Claim</strong><br />
Any information, either written or spoken, that you give to the Ministry of Labour in support of your claim,<br />
including the information provided on the claim form, is collected under the authority of the <strong>Employment</strong><br />
<strong>Standards</strong> Act, 2000 to assist in the investigation of alleged violations of the <strong>Employment</strong> <strong>Standards</strong> Act,<br />
2000. The Freedom of Information and Protection of Privacy Act, R.S.O. 1990 F.31 (as amended) governs<br />
the collection, use and disclosure of this information.<br />
Any information that you give to an employment standards officer that is relevant to your claim and is<br />
considered necessary for the investigation and enforcement of the claim may be shared with your employer<br />
or the employer’s representative.<br />
The Ministry of Labour or its agent may contact you for the purposes of conducting a survey about the<br />
quality of the ministry’s service. Any information you give to the Ministry of Labour that is necessary to<br />
conduct the survey may be shared with the ministry’s agent.<br />
If you have any questions about the collection, use and disclosure of personal information by the Ministry of<br />
Labour, you may telephone 416-326-7786 or write to:<br />
Ministry of Labour<br />
Freedom of Information and Privacy Office<br />
400 University Ave., 10th Floor<br />
Toronto ON M7A 1T7<br />
11
MOL-ES-002E (2010/08)<br />
Your Name:<br />
Send your fully-completed claim form to the Ministry of<br />
Labour and receive your claim submission number<br />
Please look over your claim form to ensure that you have filled out all necessary sections,<br />
including section D2.<br />
Please write your name at the top of each page, and include your telephone number, if<br />
possible.<br />
Once your claim form has been processed, you will receive a claim submission number.<br />
NOTE: Only send pages 1 to 10 of this claim form to the Ministry of Labour.<br />
You can file your claim form in person at a ServiceOntario Centre or by fax or mail.<br />
Your claim form can be sent to the Ministry of Labour as follows:<br />
By fax at 1-888-252-4684.<br />
In person at a ServiceOntario Centre (1-800-267-8097).<br />
By mail to:<br />
Provincial <strong>Claim</strong>s Centre<br />
Ministry of Labour<br />
70 Foster Drive, Suite 410<br />
Roberta Bondar Place<br />
Sault Ste. Marie ON P6A 6V4<br />
Note: If you file your claim submission by fax, in person, or by mail, you will receive a letter in the mail with<br />
your claim number once all of your required information has been verified. If your claim submission is<br />
missing required information, you will receive a letter in the mail with your claim submission number, and a<br />
request to provide more information.<br />
A claim submission number is assigned as soon as the ministry receives and registers your <strong>Claim</strong> <strong>Form</strong>. You<br />
will be provided with a claim number and your claim will be assigned for investigation once the ministry has<br />
verified that all required information has been completed.<br />
Please only file your claim once. For example, if you have filed your claim submission online, please do<br />
not send another copy of your claim form to the Ministry of Labour.<br />
Write your name on the envelope and on each page that you mail.<br />
Once you receive your claim submission number, make sure you keep it in a safe place.<br />
Please contact the Ministry of Labour immediately, with your claim submission number, if:<br />
� You change your address, phone number, or email address;<br />
� You and your employer resolve all or part of your claim; or<br />
� You want to add information to your claim.<br />
�<br />
12
<strong>Employment</strong> <strong>Standards</strong><br />
<strong>Claim</strong> <strong>Form</strong><br />
© Queens Printer for Ontario, 2010<br />
ISBN 978-1-4435-2934-1 (Print)<br />
ISBN 978-1-4435-2935-8 (PDF)<br />
Le présent document est aussi disponible en français sous le titre – «Normes d'emploi <strong>Form</strong>ulaire de<br />
réclamation » [ISBN 978-1-4435-2936-5 (imprimé) et ISBN 978-1-4435-2937-2 (PDF)].