Wall-July PV-Review - VetLearn.com
Wall-July PV-Review - VetLearn.com
Wall-July PV-Review - VetLearn.com
- TAGS
- cp.vetlearn.com

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
CE<br />
614 Vol. 24, No. 8 August 2002<br />
Article #3 (1.5 contact hours)<br />
Refereed Peer <strong>Review</strong><br />
KEY FACTS<br />
■ Bacteremia, either transient or<br />
permanent, must occur in order<br />
for infective endocarditis (IE) to<br />
develop.<br />
■ Echocardiography is the best<br />
diagnostic tool for confirming IE.<br />
■ Early diagnosis followed<br />
immediately by aggressive<br />
antibiotic therapy is critical<br />
for long-term survival of<br />
dogs with IE.<br />
Comments? Questions?<br />
Email: <strong>com</strong>pendium@medimedia.<strong>com</strong><br />
Web: <strong>VetLearn</strong>.<strong>com</strong> • Fax: 800-556-3288<br />
Infective Endocarditis<br />
in Dogs<br />
University of Georgia<br />
Michelle <strong>Wall</strong>, DVM<br />
Clay A. Calvert, DVM, DACVIM<br />
Craig E. Greene, DVM, MS, DACVIM<br />
ABSTRACT: Infective endocarditis (IE) most often affects young to middle-aged, large-breed<br />
dogs with no history of heart disease. Coagulase-positive staphylococci and streptococci are<br />
the most <strong>com</strong>monly associated bacteria. Clinical findings indicative of IE include fever, an<br />
inflammatory leukogram, a heart murmur of recent onset, and lameness; but these findings<br />
are not consistently present. Echocardiography and blood cultures are important aspects of<br />
the diagnostic database. The aortic or mitral valve is involved in almost 100% of cases;<br />
involvement of the aortic valve is most <strong>com</strong>mon. The echocardiographic appearance of aortic<br />
valve IE is pathognomonic. A diastolic murmur of aortic regurgitation is <strong>com</strong>mon and highly<br />
suggestive of IE. The femoral pulses associated with advanced aortic valve IE are bounding<br />
and quick. Long-term (6 to 8 weeks or longer), high-dose, bactericidal antibiotic therapy is<br />
required to treat IE. Intravenous therapy should be maintained as long as possible (at least 2<br />
weeks) and followed by subcutaneous administration. Combination therapy using clindamycin<br />
plus enrofloxacin is re<strong>com</strong>mended. IE may be difficult to recognize, often imitates immunemediated<br />
or rickettsial diseases, and is usually lethal. Congestive heart failure is the usual out<strong>com</strong>e,<br />
especially with aortic valve IE.<br />
Endocarditis denotes inflammation of the endocardial surface of the<br />
heart. 1–11 Infective endocarditis (IE), also referred to as vegetative or bacterial<br />
endocarditis, is the invasion by an infective microbe of the endothelial<br />
surface of the heart, usually the valves. 1–14<br />
When infectious microbes colonize a heart valve, they not only produce proliferative<br />
lesions (vegetations) but also destroy valvular tissue. 7,8 The vegetations<br />
are of variable size and shape, from small warty nodules to large cauliflower-like<br />
masses (Figure 1). The vegetations are <strong>com</strong>prised of three layers 7–11 :<br />
• A large inner layer of platelets, fibrin, red blood cells (RBCs), white blood<br />
cells, and bacteria<br />
• A middle layer of bacteria<br />
• An outer layer of fibrin<br />
BACTEREMIA AND ADHERENCE<br />
Bacteremia, either transient or permanent, must occur in order for IE to<br />
develop. 5,7,12 Culmination into IE involves the endothelium, hemostatic mecha-<br />
www.<strong>VetLearn</strong>.<strong>com</strong>
Compendium August 2002 Infective Endocarditis 615<br />
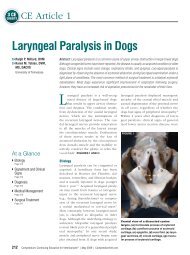
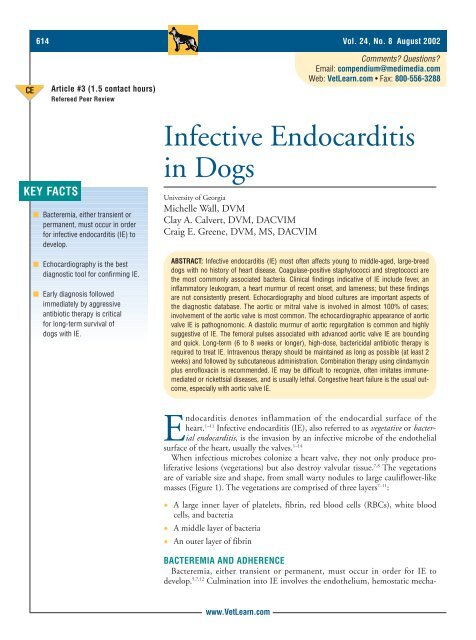
Figure 1—Gross pathology specimen demonstrating the aortic<br />
valve of a dog with IE. One of the valve leaflets was pale, cauliflower-like,<br />
firm on palpation, and appeared to be calcified.<br />
nisms, the host’s immune system, surface properties of<br />
the microorganisms, and peripheral events that initiate<br />
bacteremia. 7,8 Resistance of the intact endothelium to<br />
infection can be deduced from the relative infrequency<br />
of IE <strong>com</strong>pared with the known frequency of bacteremias.<br />
8,13 Although phagocytic cells remove<br />
Factors Predisposing Dogs to Bacteremia<br />
and Infective Endocarditis<br />
Bacterial infections<br />
Prostatitis<br />
Diskospondylitis<br />
Pyoderma<br />
Infected wounds/abscesses<br />
Stomatitis/gingivitis<br />
Invasive procedures<br />
• Protracted surgery<br />
• Infected tissue manipulation<br />
• Indwelling catheters<br />
Immunosuppression<br />
• Exogenous corticosteroid administration<br />
• Drugs<br />
• Neoplasia<br />
Congenital heart defect (subaortic stenosis)<br />
microbes from the blood, platelet-fibrin depositions<br />
may occur spontaneously; microorganisms may adhere<br />
to these sites and initiate IE before the immune system
616 Small Animal/Exotics Compendium August 2002<br />
can obliterate the infection. 8<br />
Chronic, low-grade microbemia predisposes dogs to<br />
IE. 7,13,14 Infective microorganisms in the blood must be<br />
capable of adhering to a platelet-fibrin matrix. 7,8,15<br />
Within this matrix, not only are white blood cells<br />
unable to phagocytize bacteria, but the bacteria are very<br />
concentrated. 7,8,15 Very few granulocytes are within the<br />
vegetation; and layers of fibrin, platelets, and RBCs<br />
protect the microorganisms. 7,8<br />
VALVE INVOLVEMENT<br />
Heart valves are subject to constant trauma as they<br />
open and close. 7,8 The incidence of IE appears to be<br />
directly related to the force placed upon each valve. 16,17<br />
The mitral and aortic valves are most <strong>com</strong>monly<br />
infected, and the tricuspid and pulmonic valves are seldom<br />
involved. 2,4,6,9–16,18,19 In a study of 45 dogs, 22 had<br />
aortic involvement, 16 had mitral, 1 had both aortic<br />
and mitral, and only 1 had tricuspid involvement. 6<br />
During the past 10 years, our experience is that approximately<br />
90% of infections involve the aortic valve.<br />
EPIZOOTIOLOGY<br />
The prevalence of IE is much lower than that of<br />
dilated cardiomyopathy and myxomatous mitral valve<br />
degeneration. The incidence rates at two referral institutions<br />
were both approximately five cases per year. 6,10<br />
During the last 10 years, two to five dogs with IE have<br />
been recognized annually at the University of Georgia.<br />
Typically, affected dogs are 4 to 8 years of age and<br />
medium to large sized (less than 10% weigh less than<br />
10 kg). 6,10 Affected dogs are seldom younger than 2 or<br />
older than 10 years of age. German shepherds, boxers,<br />
golden retrievers, Labrador retrievers, and rottweilers<br />
may be overrepresented. 1–4,6,9–11 Males are affected more<br />
often; a 2:1 ratio, possibly due to chronic bacterial prostatitis,<br />
has been reported. 6<br />
PREDISPOSING FACTORS<br />
There are numerous factors predisposing dogs to the<br />
development of IE. A <strong>com</strong>mon misconception is that IE<br />
is associated with structural heart disease. It is interesting<br />
that dogs with the highest incidence of advanced<br />
myxomatous mitral valve degeneration (older, smallbreed<br />
dogs) have a very low incidence of IE. Furthermore,<br />
IE is seldom associated with congenital heart diseases<br />
in dogs, with the exception of subvalvular aortic<br />
stenosis (SAS). 1–4,6,19 With SAS, turbulent, high-velocity<br />
blood flow in the left heart may produce microtrauma<br />
on the valve leaflets and facilitate microbe colonization.<br />
9,10,19,20 Boxers, rottweilers, and golden retrievers<br />
have relatively high incidences of both IE and<br />
SAS. 2,3,6,19,20 Less than 10% of dogs with SAS develop IE,<br />
www.<strong>VetLearn</strong>.<strong>com</strong><br />
and possibly less than 10% of dogs with IE have<br />
SAS. 2,3,6,19,20 Establishing or eliminating an ultrasonographic<br />
diagnosis of SAS with aortic valve IE can be difficult<br />
because the vegetation may obscure the SAS lesion.<br />
Predisposing factors for platelet–fibrin–RBC deposition<br />
on the endocardium include procedures involving<br />
the gingiva, oropharynx, gastrointestinal tract, or<br />
infected tissues and intravenous (IV) catheters. 6,8,9,12,21–23<br />
Although gingivitis/stomatitis may be associated with<br />
bacteremia and IE, dogs with the highest incidence of<br />
this condition (older, small-breed dogs) seldom develop<br />
IE. 2,3,6 Hypercoagulability associated with malignancies,<br />
disseminated intravascular coagulation, hypercortisolemia,<br />
or immune-mediated diseases may predispose<br />
dogs to IE. 7,8,24 Any abnormality that either is associated<br />
with chronic bacteremia (e.g., gingivitis, urinary or prostatic<br />
infection, pyoderma, wounds) or impairs host<br />
defenses (e.g., neoplasia, diabetes mellitus, hyperadrenocorticism,<br />
exogenous corticosteroids or other<br />
immunosuppressive therapies) increases the risk for<br />
IE. 5,8,12,13 However, dogs most prone to hyperadrenocorticism<br />
have a low incidence of IE, and we have rarely<br />
identified the two conditions in the same dog. The<br />
source of infection may be suspected but is proven in<br />
less than 50% of cases. 6,12,13<br />
Damaged endothelium exposes the extracellular polysaccharide<br />
dextran, which facilitates the attachment of<br />
some bacterial species. 25,26 Because of the limited species<br />
of microbes that account for the vast majority of IE<br />
cases, it can be deduced that certain organisms (e.g.,<br />
coagulase-positive staphylococci and some streptococci)<br />
have an increased ability to colonize the endocardium.<br />
2,3,6–8,15 Fibronectin can be produced by<br />
endothelial cells and platelets in response to vascular<br />
injury, and receptors for fibronectin are present on the<br />
surface of some bacteria, including coagulase-positive<br />
staphylococci and some streptococci. 26 Fibronectin may<br />
even facilitate the adherence of some bacteria, including<br />
staphylococci, to intact endothelium. 15,26<br />
Corticosteroids<br />
Dogs affected with IE often have a history of receiving<br />
corticosteroids. 6 In some instances, corticosteroids<br />
were administered in the weeks preceding the development<br />
of IE to treat an illness associated with unrecognized<br />
bacteremia, skin disease, or presumed immunemediated<br />
disease. Survival rates of dogs with mitral<br />
valve IE that received corticosteroids were lower than<br />
those that did not receive them. 6<br />
Infective Microbes<br />
The vast majority of IE cases are the result of bacteria;<br />
rickettsial agents are occasionally identified, but fungal
Compendium August 2002 Infective Endocarditis 617<br />
IE is rare in dogs. 2,4–6,12,14,27,28 More than 50% of infections<br />
in dogs are the result of coagulase-positive staphylococci<br />
and streptococci. 2,6,10–12,29,30 Bartonella, Brucella,<br />
Coxiella, and Chlamydia have been identified as causative<br />
agents in culture-negative IE cases in humans. 31–34 Factors<br />
predisposing humans to fungal infections (e.g., prosthetic<br />
valve replacement, IV drug abuse, chronic<br />
immunosuppressive therapy, chronic broad-spectrum<br />
antibiotic usage 8,27 ) are less <strong>com</strong>mon in dogs.<br />
PATHOPHYSIOLOGY<br />
Aside from the constitutional signs of infection,<br />
which are mediated by cytokines, the clinical manifestations<br />
of IE are the result of valvular destruction,<br />
embolic phenomena, and immune-<strong>com</strong>plex disease. 3,6–8<br />
Congestive heart failure (CHF) is the usual out<strong>com</strong>e in<br />
dogs with aortic valve IE. 2,4,6,9–12<br />
Embolization leads to organ infarction and metastatic<br />
infection. 6–9,24 Embolization is a frequent cause of clinical<br />
signs and clinical deterioration. Even in the absence<br />
of clinical evidence, dogs almost always have systemic<br />
emboli at necropsy, and the kidneys are almost always<br />
infarcted. 9–11 Emboli are usually present in many organs<br />
and tissues. 2,4,6,10,12<br />
Persistent bacteremia stimulates both cell-mediated<br />
and humeral immune systems. 7–10 Circulating immune<br />
<strong>com</strong>plexes containing IgG, IgA, IgM, and <strong>com</strong>plement<br />
may be deposited subendothelially along glomerular<br />
basement membranes, in joint capsules, and in blood<br />
vessels, leading to glomerulonephritis, arthritis, and vasculitis.<br />
3–5,7,8,10,35–40 Clinical signs of IE frequently mimic<br />
those of immune-mediated disorders, and positive<br />
immune-test results (e.g., Coombs test, antinuclear antibody<br />
test) can occur because of antigen–antibody–<strong>com</strong>plement<br />
interaction. 6,35 Rheumatoid factor, antinuclear<br />
Clinical Findings That May Be Associated with<br />
Infective Endocarditis<br />
Heart murmur<br />
• Recent onset<br />
• Diastolic <strong>com</strong>ponent<br />
Fever<br />
Inflammatory leukogram<br />
Systemic embolic phenomena<br />
• Saddle thrombus<br />
• Limb edema<br />
• Lameness<br />
Arthropathy<br />
• Joint swelling<br />
• Pain<br />
• Lameness<br />
www.<strong>VetLearn</strong>.<strong>com</strong><br />
antibodies, and circulating immune <strong>com</strong>plexes contribute<br />
to the development of polyarthritis, renal disease,<br />
and myocarditis. 6–9,35–40<br />
CLINICAL FINDINGS<br />
Clinical signs and diagnostic abnormalities associated<br />
with IE are often nonspecific and often include<br />
extracardiac manifestations. The interval between the<br />
initiating bacteremic event and diagnosis of IE is usually<br />
uncertain, and a predisposing factor is not always<br />
evident. 6 Occasionally, there is a history of an illness<br />
that, in retrospect, may have initiated bacteremia 1 to<br />
3 months before the diagnosis of IE. 6 Affected dogs<br />
often have signs of systemic infection, including fever<br />
and leukocytosis. Septic or sterile embolization/infarction,<br />
metastatic infections, and organ failure are<br />
responsible for many of the clinical signs. 6–8,12 Clinical<br />
signs associated with IE are diverse and misleading,<br />
and IE has frequently been called “the great imitator.”<br />
10 Owners variably report lethargy, depression,<br />
weakness, anorexia, weight loss, lameness, neurologic<br />
signs, and signs consistent with CHF. 2–4,6,12,19 Fever,<br />
either current or a history thereof, is not always present<br />
and may be easily overlooked. 3,6,12 Fever is often<br />
absent at the time of diagnosis because the bacteremia<br />
is low grade or there was previous therapy with antibiotics,<br />
steroids, or NSAIDs. 6,12<br />
Heart Murmurs<br />
Cardiac sequelae of IE include valvular insufficiency<br />
because infection destroys the valvular tissue and interferes<br />
with function. 7–10 The severity of destruction varies<br />
with chronicity and the virulence of the organism. 7–10 IE<br />
is the most <strong>com</strong>mon cause of a murmur of aortic regurgitation<br />
(the aortic valve is the most <strong>com</strong>monly<br />
infected 2,6 ), which can be detected over the left heart<br />
base or on the right thoracic wall midway between the<br />
tricuspid valve area and the manubrium. Systolic murmurs<br />
result from mitral regurgitation or aortic valve vegetation–generated<br />
systolic flow turbulence. A murmur<br />
of recent onset, especially with a diastolic <strong>com</strong>ponent,<br />
ac<strong>com</strong>panied with fever is very suggestive of IE. 2,6 The<br />
femoral pulses associated with mitral valve endocarditis<br />
are typically normal but may be weak if left-sided CHF<br />
is present. 2–4,6 The femoral pulses associated with aortic<br />
valve endocarditis may be normal or hyperdynamic and<br />
bounding. 2 The systolic pulse pressure with aortic regurgitation<br />
is often increased because of volume overload<br />
and resultant increased stroke volume. Diastolic pressure<br />
may be low because of arterial blood runoff back into<br />
the left ventricle during diastole; thus not only may the<br />
diastolic pressure be low, but the systolic pressure wave<br />
duration may be shortened.
618 Small Animal/Exotics Compendium August 2002<br />
Lameness<br />
Lameness due to IE is an occasional finding rarely<br />
caused by septic emboli but usually the result of<br />
immune-mediated arthritis. 3,4,6,9,35,36,39 Synovial tissue<br />
may contain IgG, IgM, and <strong>com</strong>plement, indicating an<br />
immune basis for the arthropathy. 35,36<br />
Organ Failure<br />
Dogs with IE may present with signs consistent with<br />
CHF (usually left-sided), including coughing, dyspnea,<br />
pulmonary crackles (pulmonary edema), shortness of<br />
breath, weakness, and/or collapse. 3,6 CHF is most frequently<br />
associated with aortic valve IE. When the left<br />
heart appears radiographically normal in size, but pulmonary<br />
edema is present, IE should be considered<br />
because dramatic heart enlargement may not yet have<br />
occurred in the case of acute IE. The index of suspicion<br />
of IE rises in dogs that have no history of a heart murmur<br />
or are not prone to cardiomyopathy or myxomatous<br />
valvular degeneration. 6<br />
Renal failure is another <strong>com</strong>plication that may<br />
detract from recognizing IE. Renal failure is usually<br />
due to chronic infarction or glomerulonephritis<br />
(Figure 2). 3,6,13,37,38<br />
Polysystemic Signs<br />
The constitutional signs of IE can mimic those of<br />
any polysystemic disease. 3,6 Many diagnostic differentials<br />
must be considered, including immune-mediated<br />
diseases, rickettsial infections, bacteremia alone, sequelae<br />
of neoplasia, causes of CHF, and causes of renal failure.<br />
2,6,12,13,33,35,36 Localized signs, such as lameness,<br />
edema, and pain, often arise from <strong>com</strong>plications of<br />
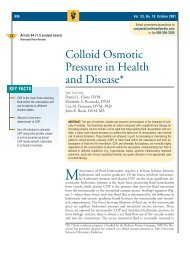
Figure 2—Gross pathology kidney specimen from a dog with<br />
aortic valve IE. The kidney has been sectioned in the sagittal<br />
plane. Multiple triangular-shaped, pale infarctions of variable<br />
age are visible within the renal parenchyma.<br />
www.<strong>VetLearn</strong>.<strong>com</strong><br />
infection. 6,35,36,39 In order to avoid overlooking IE, the<br />
possibility should be investigated when one or more of<br />
the following signs are present:<br />
• An unexplained fever<br />
• A heart murmur of recent onset<br />
• A source of infection<br />
• Embolic phenomena<br />
Systemic Embolization<br />
IE always results in embolization. The kidneys consistently<br />
exhibit old and new infarcts that contribute to<br />
proteinuria and renal failure. The spleen, liver, and<br />
iliac or mesenteric arteries are sometimes involved.<br />
Splenic septic abscesses may contribute to persistent<br />
fever and leukocytosis.<br />
CLINICAL PATHOLOGY<br />
Hematologic findings of systemic inflammation are<br />
often absent in IE. This may be due to antibiotic or<br />
steroid administration or chronic, low-grade bacteremia.<br />
6,12 Although an inflammatory leukogram is not<br />
always present, monocytosis is present in 90% of<br />
cases. 6,12 In some instances, mature neutrophilia and<br />
monocytosis indicate low-grade, chronic inflammation.<br />
Thrombocytopenia is another <strong>com</strong>mon finding and<br />
can be attributed to systemic vasculitis and immune or<br />
coagulatory consumption. 6,12<br />
A variety of serum biochemical abnormalities may<br />
be observed. A septic triad may be present, characterized<br />
by low or decreasing albumin, increased serum<br />
alkaline phosphatase activity, and absolute or relative<br />
hypoglycemia. 6,13 Hypoalbuminemia may be explained<br />
by proteinuria, anorexia, or decreased liver function<br />
caused by toxins. 6,13 Increased serum alkaline phosphatase<br />
activity is usually due to toxin interference<br />
with bile metabolism or prior steroid use. 6,13,14 Hypoglycemia<br />
can be explained by bacterial toxin effects on<br />
intermediary metabolism. 13,14 Azotemia may be prerenal<br />
or caused by infarction and glomerulopathy. 3,9,10,37,38<br />
The urine often contains protein, blood, casts, and/or<br />
bacteria. 6,13 Urine culture is re<strong>com</strong>mended not only<br />
because bacteria are filtered from the blood into the<br />
urine but also because the urinary tract may be a<br />
source of infection. 6,13<br />
SPECIAL DIAGNOSTICS<br />
The diagnosis of IE requires integration of clinical<br />
and laboratory findings. Arrhythmias (usually atrial or<br />
ventricular premature contractions) are present in at<br />
least 50% to 75% of documented cases; seldom life<br />
threatening; and best evaluated by long-term, continuous<br />
electrocardiographic monitoring (either cage-side
Compendium August 2002 Infective Endocarditis 619<br />
or Holter recorded). Other less-<strong>com</strong>mon electrocardiographic<br />
abnormalities include bundle branch and atrioventricular<br />
blocks.<br />
Radiographic interpretation may reveal chamber<br />
enlargements or no abnormalities. Chamber enlargement<br />
(most <strong>com</strong>monly left atrial) is usually present<br />
when IE is chronic. 2–4,6,41 If overt or impending leftsided<br />
CHF is present, pulmonary edema and/or distention<br />
of the pulmonary veins will be present. 2–4,6,9,10,41<br />
Echocardiography is the best diagnostic tool but is<br />
neither 100% sensitive nor 100% specific. 3,9–11 Modern,<br />
two-dimensional equipment can resolve 1-mm lesions<br />
in dogs. 10 Detection of an echogenic oscillating intracardiac<br />
mass on the aortic or mitral valve is a strong<br />
indication of the presence of IE. Both the M-mode and<br />
two-dimensional appearance of aortic valve vegetations<br />
are virtually pathognomonic (Figure 3). Echoes from<br />
vegetations on the mitral valve are usually on the cra-<br />
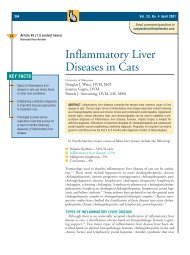
Figure 3—M-mode echocardiogram of a thickened aortic<br />
valve (AV). This echocardiographic image is typical of aortic<br />
valve vegetations.<br />
Figure 4—Two-dimensional echocardiogram in the right<br />
parasternal, long-axis plane demonstrating vegetative lesions<br />
on the cranial (anterior) mitral valve (arrowhead) and the aortic<br />
valve (arrow) leaflets during diastole. A = aorta; LA = left<br />
atrium; LV = left ventricle.<br />
www.<strong>VetLearn</strong>.<strong>com</strong><br />
nial (anterior) leaflet but are not pathognomonic; in<br />
some cases, however, the lesion is so large that IE<br />
should be suspected (Figure 4). Operator skill and<br />
experience, as well as image quality, influence interpretation.<br />
Furthermore, results must be considered in the<br />
context of other clinical and laboratory findings. Falsepositive<br />
test interpretation is most <strong>com</strong>monly attributable<br />
to mitral valve myxomatous degeneration. 9,10 A clinician<br />
should always consider the signalment and<br />
history of the dog in question. The signalment associated<br />
with IE is largely different from that of dogs with<br />
advanced myxomatous degeneration. The presence of a<br />
new heart murmur is of special importance if the breed<br />
or age of the patient is not characteristic of dogs<br />
affected by myxomatous valvular degeneration.<br />
Chamber enlargements and altered contractility may<br />
be evident. 3,6,9,10 Decreased contractility is typical of the<br />
high-pressure volume overload of advanced aortic valve<br />
IE but not of the low-pressure volume overload of<br />
mitral valve IE. Decreased contractility may also be<br />
related to chronicity of volume overload. Diastolic fluttering<br />
of the anterior (cranial) mitral valve leaflet is<br />
indicative of aortic insufficiency and, therefore, suggestive<br />
of endocarditis. This fluttering is the result of the<br />
jet of aortic regurgitation striking the anterior mitral<br />
valve leaflet when it is open in diastole. Color-flow<br />
imaging is used to identify hemodynamic consequences<br />
of endocarditis, such as valvular regurgitation or left<br />
ventricular outflow tract turbulence (Figure 5).<br />
Doppler interrogation of aortic regurgitation is used to<br />
confirm the severity. The spectral display of severe aortic<br />
regurgitation is characterized by a rapid deceleration<br />
of regurgitant velocity during diastole. Severe aortic<br />
regurgitation is in<strong>com</strong>patible with survival.<br />
DIAGNOSIS<br />
The diagnosis of IE requires integration of clinical<br />
and laboratory data. The advent of echocardiography<br />
has greatly facilitated the diagnosis. Because the aortic<br />
valve is usually involved in IE, 2,3,6 ultrasonographic<br />
recognition is seldom difficult. Diagnosis of mitral<br />
valve IE is more difficult because the lesions of myxomatous<br />
degeneration can resemble those of IE. 3 It<br />
should be recognized that dogs with the highest incidence<br />
of myxomatous degeneration of the mitral valve<br />
(older, small-breed dogs) are seldom affected by IE. Signalment,<br />
clinical findings, femoral pulse characteristics,<br />
confirmation of bacteremia, and a murmur of recent<br />
onset (especially a diastolic murmur) are important to<br />
the diagnosis of IE if echocardiography is not available.<br />
Identification of Bacteremia<br />
Although blood cultures lack sensitivity and speci-
620 Small Animal/Exotics Compendium August 2002<br />
Figure 5A Figure 5B<br />
Figure 5C Figure 5D<br />
Figure 5—(A) Two-dimensional echocardiogram in the left apical, long-axis, two-chamber imaging plane. During systole, an aortic<br />
valve leaflet thickened by vegetation (arrow) is opened into the aorta (A). There are also vegetations on the mitral valve leaflets<br />
(arrowhead). (B) In diastole, the vegetative aortic valve is closed, and a portion of the vegetation is protruding (arrowhead) into<br />
the left ventricle (LV). The open cranial (anterior) mitral valve leaflet is also thickened by vegetation (arrow). (C) Color-flow<br />
Doppler imaging in systole demonstrating the turbulent mitral regurgitation (arrowhead). (D) Color-flow Doppler imaging in<br />
diastole demonstrating the turbulent jet of aortic regurgitation (arrowhead). LA = left atrium.<br />
ficity, they should always be performed in an attempt<br />
to identify the offending organism. 10,12,14,42,43 Bacteremia<br />
may occur in other conditions, such as diskospondylitis,<br />
chronic wounds, prostate infections, and periodontal<br />
disease. 6,12–14 Performed properly, blood cultures often<br />
yield positive results (in our experience, approximately<br />
30% to 50% of patients have positive results). 6,9–11,13,14<br />
Decreased sensitivity may be explained by fastidious,<br />
slow-growing organisms; improper laboratory techniques;<br />
the failure to culture for anaerobes; low-blood<br />
bacterial concentrations; endogenous bactericidal<br />
factors (<strong>com</strong>plement and phagocytes); intermittent<br />
shedding of the organism; chronic IE with encapsulated<br />
vegetative lesions; or infections with Bartonella.<br />
13,31–33,42–44 Other variables affecting the yield of<br />
microorganisms include the volume of the blood sample,<br />
number of cultures performed, and incubation<br />
atmosphere of the culture. 14,44<br />
www.<strong>VetLearn</strong>.<strong>com</strong><br />
Two or three sets of blood samples should be taken<br />
aseptically, preferably before antibiotic administration.<br />
6,13,14,43,44 Samples should be taken either from a<br />
freshly placed, meticulously maintained jugular<br />
catheter or from different veins. 14,42 Commercial vacuum<br />
bottles should be used. If the animal is receiving<br />
antibiotic therapy, collect the sample at the antibiotic<br />
trough level and use an antibiotic removal device. 14<br />
Duration of antimicrobial therapy is an important factor<br />
in detecting bacteria. 45 Therapy for only 2 to 3 days<br />
may not interfere; however, longer courses of therapy<br />
require the use of antibiotic removal devices or discontinuation<br />
of therapy. Suppression of bacteremia often<br />
persists longer than antibiotic blood levels.<br />
Sterile technique should be practiced when collecting<br />
blood samples. The area must be clipped and disinfected,<br />
and sterile gloves should be worn. Samples (7 to 10<br />
ml of whole blood) should be placed in two bottles:
Compendium August 2002 Infective Endocarditis 621<br />
Criteria for the Antemortem Diagnosis of Infective<br />
Endocarditis<br />
Without Echocardiographic Examination<br />
A murmur of recent onset<br />
plus<br />
Positive blood culture results (it is preferable to find<br />
more than one of the same microbe)<br />
plus<br />
Clinical findings and laboratory data consistent with<br />
bacteremia and IE<br />
With Echocardiographic Examination<br />
Aortic valve<br />
• Echocardiographic appearance is pathognomonic<br />
Mitral valve<br />
• Echocardiographic appearance is suggestive of IE<br />
• Supportive clinical data<br />
Signalment<br />
Murmur of recent onset<br />
Positive blood culture results<br />
Fever<br />
one unvented for anaerobic culture, and one vented for<br />
aerobic culture. 9–11,14 If acute sepsis is suspected, take<br />
three cultures 1 hour apart, and then institute antibiotic<br />
therapy. 10,42<br />
Many negative blood cultures in humans with IE are<br />
due to infection with Bartonella, a fastidious, gramnegative<br />
organism. 31 The incidence of Bartonella endocarditis<br />
is unknown but less than that of bacterial endocarditis<br />
and has been proven in a few dogs. Bartonella<br />
resides within or on the surface of RBCs, making it difficult<br />
to isolate from blood cultures; therefore, special<br />
techniques are re<strong>com</strong>mended. 31–34 Special cultivation<br />
methods may be necessary to isolate fastidious<br />
pathogens. Tissue culture methods may be required for<br />
obligate, intracellular organisms, such as Coxiella, some<br />
Bartonella, and Chlamydia. Extraction of nucleic acid<br />
from blood and subsequent polymerase chain reaction<br />
amplification has been beneficial in the early diagnosis<br />
of bacteremia and confirmation of infection with fastidious<br />
or unculturable agents. 31,34<br />
TREATMENT<br />
Prolonged parenteral administration of one or more<br />
bactericidal antibiotics is re<strong>com</strong>mended. The goal of<br />
treatment is to kill the organism as well as minimize<br />
and manage the consequences of infection. Therapy is<br />
ideally based on blood culture antibiogram results, but<br />
treatment is usually initiated before results. 46–49 Within<br />
the vegetation, organisms are protected, be<strong>com</strong>e meta-<br />
www.<strong>VetLearn</strong>.<strong>com</strong><br />
Principles of Antibiotic Treatment of Infective<br />
Endocarditis<br />
• Use bactericidal antibiotics.<br />
• Ensure high antibiotic serum concentrations by<br />
administering high doses intravenously.<br />
• Continue IV antibiotic administration for at least 1<br />
to 2 weeks.<br />
• Replace IV administration of antibiotics by SC<br />
administration when the former is no longer<br />
practical.<br />
• Continue antibiotic therapy for at least 2 to 3<br />
months.<br />
• Use oral antibiotics only after at least 1 month of IV<br />
and SC administration.<br />
bolically dormant, and are less vulnerable to the killing<br />
activities of antimicrobials. 8–11,14<br />
Because antibiotics reach the central areas of avascular<br />
vegetations by passive diffusion, antimicrobial therapy<br />
should be bactericidal and antibiotic serum concentrations<br />
should be high. 46 High serum<br />
concentrations are mandatory, and antibiotic serum<br />
concentrations should be maintained at the high end of<br />
the therapeutic range for at least 1 month. 4,6,9–13 We re<strong>com</strong>mend<br />
at least 1 to 2 weeks of IV antibiotic therapy<br />
followed by subcutaneous (SC) administration 50 for<br />
several weeks, if possible; then oral bactericidal antibiotics<br />
should be continued for 1 to 2 months. 47<br />
For some drugs, SC administration produces higher<br />
serum concentrations than oral administration. For<br />
example, the sodium salt of ampicillin administered at<br />
10 mg/kg SC achieves a peak serum concentration of<br />
up to 80 µg/ml, whereas administration at 20 to 30<br />
mg/kg PO achieves a serum concentration of only 2 to<br />
4 µg/ml. Likewise, the salt of amoxicillin administered<br />
at 20 mg/kg PO achieves a peak serum concentration<br />
of only 8 µg/ml. Among the cephalosporins, cephapirin<br />
administered at 20 to 30 mg/kg SC produces peak<br />
serum concentrations of 20 to 30 µg/kg, and the same<br />
dosage of cefazolin produces peak serum concentrations<br />
of 40 to 60 µg/ml. Cephalexin at 30 mg/kg PO produces<br />
a peak concentration of 25 µg/ml. Clindamycin<br />
administered at 10 mg/kg SC produces a peak serum<br />
concentration of 8 µg/ml <strong>com</strong>pared with 5 µg/kg when<br />
administered orally at the same dose. 50<br />
The most <strong>com</strong>mon infective bacteria are known, and<br />
their antimicrobial sensitivity patterns are somewhat<br />
predictable (Table 1). If blood cultures are negative or<br />
treatment is deemed necessary before culture results are<br />
obtained, ampicillin, a first-generation cephalosporin,<br />
or ticarcillin plus gentamicin or amikacin may be used.<br />
A fluoroquinolone may be substituted for an aminogly-
622 Small Animal/Exotics Compendium August 2002<br />
Table 1. Antimicrobial Re<strong>com</strong>mendations for Bacteria Commonly Isolated in Dogs with Infective<br />
Endocarditis 9–11,13,14,42,48–50<br />
Antibiotic Staphylococci a Streptococci Gram-Negative Organisms Anaerobes<br />
Cephalosporins<br />
First generation S S V R<br />
Second generation S S V Gram negative<br />
Third generation<br />
Cefotaxime b V S S c S<br />
Ceftiofur d V V V V<br />
Penicillin G R S R S<br />
Ampicillin R S V V<br />
Amoxicillin–clavulanate V S V S<br />
Ticarcillin e S S V V<br />
Ticarcillin–clavulanate f S S S S<br />
Fluoroquinolones S V S R<br />
Aminoglycosides S V S R<br />
Clindamycin g V S R S<br />
a Coagulase-positive staphylococci.<br />
b Claforan ® , Hoechst Marion Roussel.<br />
c Pseudomonas resistant.<br />
d Naxcel ® , Pharmacia and Upjohn Co.<br />
e Ticar ® , GlaxoSmithKline.<br />
f Timentin ® , GlaxoSmithKline.<br />
g Cleocin ® , Pharmacia and Upjohn Co.<br />
R = usually resistant; S = usually sensitive; V = Variable sensitivity; use only if indicated by antibiogram.<br />
coside. 49 Clindamycin or metronidazole administration<br />
extends the anaerobic spectrum. A good <strong>com</strong>bination is<br />
clindamycin plus enrofloxacin. Aminoglycoside therapy<br />
duration should be limited to 5 to 7 days because renal<br />
toxicity is possible and concurrent fluid support is necessary<br />
8–11 (Table 2).<br />
The choice for SC antibiotic administration should<br />
ideally be based on an antibiogram, but if blood cultures<br />
are negative or not performed, ceftiofur (2.2<br />
mg/kg SC q12h), azithromycin (5 mg/kg SC q12h), or<br />
ticarcillin (50 to 100 mg/kg SC q8h) may be used. 14<br />
We re<strong>com</strong>mend that blood cultures be performed 4<br />
weeks after treatment to ensure eradication of the<br />
organism. Patients, including those with negative cultures,<br />
are monitored for improvement via constitutional<br />
signs, serial CBC and serum chemistry profiles,<br />
and echocardiography. The emergence of overt CHF is<br />
ominous. Although it may offer temporary amelioration<br />
of signs, glucocorticoid administration is associated<br />
with decreased survival. 6<br />
Supportive therapy is always a <strong>com</strong>ponent of treatment.<br />
Acid–base, fluid, and electrolyte balance must<br />
be addressed. Nutritional support may be an important<br />
<strong>com</strong>ponent of therapy and may be maintained by<br />
either parenteral or tube alimentation. The consequences<br />
of valvular destruction must be addressed.<br />
www.<strong>VetLearn</strong>.<strong>com</strong><br />
Although a positive influence on disease progression is<br />
unproven, 51 angiotensin-converting enzyme (ACE)<br />
inhibition is usually re<strong>com</strong>mended if there is unequivocal<br />
left-atrial or left-ventricular enlargement.<br />
Enalapril (0.25 mg/kg PO q12h for 1 week followed<br />
by 0.5 mg/kg PO q12h) or benazepril (0.25 mg/kg PO<br />
q24h for 1 week followed by 0.5 mg/kg PO q24h) are<br />
<strong>com</strong>mon choices. Spironolactone (1 to 2 mg/kg PO<br />
q12h), an aldosterone antagonist, may be added to the<br />
regimen as cardiac enlargement progresses. A diuretic<br />
and digoxin (0.005 to 0.01 mg/kg PO q12h) should<br />
be used if CHF is overt. Again, the influence of<br />
digoxin on disease progression may be negligible. 52<br />
Furosemide (1 to 4 mg/kg PO q12h) is the diuretic of<br />
choice. A serum digoxin concentration should be<br />
obtained after 7 days of treatment from a sample<br />
drawn at 6 hours after the morning dose. For most<br />
laboratories, a desirable serum digoxin concentration is<br />
1 to 1.5 ng/ml. Renal function and serum electrolyte<br />
monitoring at 1 to 2 weeks and then monthly is re<strong>com</strong>mended.<br />
Augmented afterload reduction may be a<br />
useful adjunct to ACE inhibition. Adjuvant afterload<br />
reduction (arteriolar dilation) may result in reduction<br />
of aortic or mitral regurgitant volume. When the total<br />
peripheral arteriolar resistance is decreased by increasing<br />
the total arteriolar cross-sectional area, the change
Compendium August 2002 Infective Endocarditis 623<br />
Table 2. Intravenous and Subcutaneous Antibiotic<br />
Dosages Re<strong>com</strong>mended for Treating Bacterial<br />
Endocarditis 11,14<br />
Antibiotic Dose (mg/kg) Frequency<br />
Ampicillin 20–40 tid<br />
Amoxicillin–clavulanate 20 bid<br />
Cephalosporins<br />
First generation 22 tid<br />
Second generation<br />
Cefuroxime a 15 tid<br />
Cefaclor b 10–15 tid<br />
Cefoxitin c 20–30 tid<br />
Third generation<br />
Cefotaxime 50 bid<br />
Ceftiofur 2.2–4.4 bid<br />
Clindamycin 10 tid<br />
Azithromycin d 5–10 bid<br />
Enrofloxacin 10 Once daily<br />
5 bid<br />
Ticarcillin, ticarcillin– 50–100 tid<br />
clavulanate<br />
Gentamicin 6 Once daily<br />
Amikacin 10 Once daily<br />
a Ceftin ® , GlaxoSmithKline.<br />
b Ceclor ® , Eli Lilly Co.<br />
c Mefoxin ® , Merck and Co.<br />
d Zithromax ® , Pfizer Inc.<br />
in relative resistance to systolic and diastolic blood<br />
flow facilitates increased forward stroke volume and<br />
decreased aortic regurgitation.<br />
Systemic blood pressure should be monitored as adjuvant<br />
afterload reduction is initiated and up-titrated.<br />
Amlodipine and felodipine are effective afterload reducers<br />
when instituted at 0.1 mg/kg PO q12h and up-titrated<br />
every 4 to 7 days to a maximum of 0.3 to 0.4 mg/kg PO<br />
q12h. Indirect blood pressure monitoring is important,<br />
although it is subject to inaccuracies. Dogs that subsequently<br />
develop signs of hypotension have consistently<br />
had lower indirect blood pressures <strong>com</strong>pared with pretreatment<br />
and during early dose titration. We discontinue<br />
up-titration if the systolic blood pressure is less than<br />
approximately 110 mm Hg. If clinical signs of hypotension<br />
(e.g., lethargy, trembling, weakness, anorexia) occur,<br />
withdraw amlodipine, ACE inhibitor, spironolactone,<br />
and diuretic therapy for 24 hours, and then reinstitute all<br />
drugs with amlodipine at the previous lower dose. Severe<br />
hypotension requires IV fluid administration.<br />
Anticoagulant Therapy<br />
Anticoagulant therapy has not been shown to prevent<br />
embolization and may increase the risk of hemor-<br />
www.<strong>VetLearn</strong>.<strong>com</strong><br />
rhage. 52 The role of aspirin in preventing embolization<br />
is under evaluation. 53 However, it may reduce vegetation<br />
bacterial density, bacterial dissemination, and<br />
embolic events. 53<br />
PROGNOSIS<br />
The prognosis for long-term survival of dogs with IE<br />
is poor. 1–4,6,8–14 Early diagnosis followed immediately by<br />
aggressive antibiotic therapy is critical for long-term<br />
survival, especially when the aortic valve is infected.<br />
Unfortunately, early diagnosis is difficult, and valvular<br />
damage is often advanced by the time of diagnosis.<br />
Aortic valve endocarditis is associated with a grave<br />
prognosis because animals with it develop left-sided<br />
CHF (often within 1 to 3 months, and almost always<br />
within 6 months of diagnosis).<br />
PREVENTION<br />
Chemoprophylaxis is controversial because the<br />
risk:benefit ratio and economic rationale can be questioned<br />
and clinical studies supporting efficacy are limited.<br />
9–11 Chemoprophylaxis, even if effective, does not<br />
apply to the majority of cases. However, the mortality<br />
associated with IE warrants chemoprophylaxis in<br />
patients at increased risk. 54,55<br />
It is re<strong>com</strong>mended to use prophylactic antibiotics<br />
when performing dental scaling, dental extractions, or<br />
surgery in dogs with congenital heart diseases. 9–11 Such<br />
procedure-focused chemoprophylaxis should not be initiated<br />
several days before the procedure because of the<br />
potential to select for antibiotic-resistant organisms. 8<br />
Maintenance of oral hygiene is a more important preventive<br />
than procedure-focused chemoprophylaxis. 8 The<br />
male dog’s urinary tract is suspected to be a <strong>com</strong>mon<br />
source of chronic bacteremia; therefore, castration can be<br />
viewed as a prophylactic measure because it reduces the<br />
risk of bacterial prostatitis. For oral/dental procedures in<br />
patients that are at increased risk, it is prudent to administer<br />
ticarcillin or a first-generation cephalosporin intravenously<br />
1 hour before and 6 hours after the procedure.<br />
Because incision and drainage of infected skin are associated<br />
with coagulase-positive staphylococci, a first-generation<br />
cephalosporin, ticarcillin, or ticarcillin–clavulanate<br />
is a good choice for prophylaxis. 54,56<br />
REFERENCES<br />
1. Shouse CL, Meier H: Acute vegetative endocarditis in the dog<br />
and cat. JAVMA 129:278–289, 1956.<br />
2. Sisson D, Thomas WP: Endocarditis of the aortic valve in the<br />
dog. JAVMA 184:570–577, 1984.<br />
3. Lombard CW, Buergelt CD: Vegetative bacterial endocarditis in<br />
dogs: Echocardiographic diagnosis and clinical signs. J Small<br />
Anim Pract 24:325–329, 1993.<br />
4. Anderson CA, Dubielzig RR: Vegetative endocarditis in dogs.
624 Small Animal/Exotics Compendium August 2002<br />
JAAHA 20:149–152, 1984.<br />
5. Freedman LR: The pathogenesis of infective endocarditis. J<br />
Antimicrob Chemother 20:1–6, 1987.<br />
6. Calvert CA: Valvular bacterial endocarditis in the dog. JAVMA<br />
180:1080–1084, 1982.<br />
7. Weinstein L, Schlesinger JJ: Pathoanatomic, pathophysiologic<br />
and clinical correlations in endocarditis. N Engl J Med<br />
291:1122–1126, 1974.<br />
8. Karchmer AW: Infective endocarditis, in Braunwald E (ed):<br />
Heart Disease: A Textbook of Cardiovascular Medicine, ed 5.<br />
Philadelphia, WB Saunders Co, 1997, pp 1077–1099.<br />
9. Miller MW, Sisson D: Infectious endocarditis, in Fox PR, Sisson<br />
D, Moise NS (eds): Textbook of Canine and Feline Cardiology, ed<br />
2. Philadelphia, WB Saunders Co, 1999, pp 552, 567–580, 908.<br />
10. Kittleson MD: Infective endocarditis, in Kittleson MD, Kienle<br />
RD (eds): Small Animal Cardiovascular Medicine. St. Louis,<br />
Mosby, Inc, 1998, pp 402–412.<br />
11. DeFrancesco TC: CVT update: Infectious endocarditis, in<br />
Bonagura JD (ed): Kirk’s Current Veterinary Therapy VIII.<br />
Philadelphia, WB Saunders Co, 2000, pp 768–772,<br />
1241–1264.<br />
12. Calvert CA, Greene CE, Hardie EM: Cardiovascular infections<br />
in dogs: Epizootiology, clinical manifestations, and prognosis.<br />
JAVMA 187:612–616, 1985.<br />
13. Calvert CA, Greene CE: Bacteremia in dogs: Diagnosis, treatment,<br />
and prognosis. Compend Contin Educ Pract Vet 8:<br />
179–184, 1986.<br />
14. Calvert CA: Cardiovascular infections, in Greene CE (ed): Infectious<br />
Diseases of the Dog and Cat, ed 2. Philadelphia, WB Saunders<br />
Co, 1998, pp 567–582, 790–919.<br />
15. Thompson J, Meddens MJ, Thorig L, et al: The role of bacterial<br />
adherence in the pathogenesis of infective endocarditis. Infection<br />
10:196–198, 1982.<br />
16. Lepeschkin E: On the relation between the site of valvular<br />
involvement in endocarditis and the blood pressure resting on<br />
the valve. Am J Med Sci 224:318–322, 1952.<br />
17. Rodbard S: Blood velocity and endocarditis. Circulation 27:<br />
18–20, 1963.<br />
18. Buchbinder NA, Roberts WC: Left-sided valvular infective<br />
endocarditis: A study of forty-five necropsy patients. Am J Med<br />
53:20–35, 1972.<br />
19. Muna WF, Ferrans VJ, Pierce JE, et al: Discrete subaortic stenosis<br />
in Newfoundland dogs: Association of infective endocarditis.<br />
Am J Cardiol 41:746–754, 1978.<br />
20. Kienle RD, Thomas WP, Pion PD: The natural clinical history<br />
of canine congenital subaortic stenosis. J Vet Intern Med<br />
8:423–431, 1994.<br />
21. Wahl MJ: Myths of dental-induced endocarditis. Arch Intern<br />
Med 154:137–144, 1994.<br />
22. Bender IB, Barkan MJ, Einstein A: Dental bacteremia and its<br />
relationship to bacterial endocarditis: Preventive measures. Compend<br />
Contin Educ Pract Vet 10:472, 475–477, 1994.<br />
23. Black AP, Crichlow AM, Saunders JR: Bacteremia during ultrasonic<br />
teeth cleaning and extraction in the dog. JAAHA<br />
16:611–616, 1980.<br />
24. Ellison GW, King RR, Calderwood-Mays M: Medical and surgical<br />
management of multiple organ infarctions secondary to<br />
endocarditis in a dog. JAVMA 193:1289–1291, 1988.<br />
25. Ramirez-Ronda CH: Effects of molecular weight of dextran on<br />
the adherence of Streptococcus sanguis to damaged heart valves.<br />
Infect Immun 29:1–7, 1980.<br />
www.<strong>VetLearn</strong>.<strong>com</strong><br />
26. Hamill RJ: Role of fibronectin in infective endocarditis. Rev<br />
Infect Dis 9(Suppl 4):360–371, 1987.<br />
27. Rubinstein E, Lang R: Fungal endocarditis. Eur Heart J 16<br />
(Suppl B):84–89, 1995.<br />
28. Scheld WM, Mandell GL: Enigmatic enterococcal endocarditis.<br />
Ann Intern Med 100:904–905, 1984.<br />
29. Eriksen K, Fossum K, Gamlem H, et al: Endocarditis in two<br />
dogs caused by Erysipelothrix rhusiopathiae. J Small Anim Pract<br />
28:117–122, 1987.<br />
30. Takahashi T, Tamura Y, Yoshimura H, et al: Erysipelothrix tonsillarum<br />
isolated from dogs with endocarditis in Belgium. Res Vet<br />
Sci 54:264–265, 1993.<br />
31. Breitschwerdt EB, Kordick DL, Malarkey DE, et al: Endocarditis<br />
in a dog due to infection with a novel Bartonella subspecies. J<br />
Clin Microbiol 33:154–160, 1995.<br />
32. Raoult D, Fournier PE, Drancourt M, et al: Diagnosis of 22<br />
new cases of Bartonella endocarditis. Ann Intern Med 125:<br />
646–652, 1996.<br />
33. Breitschwerdt EB, Atkins CE, Brown TT, et al: Bartonella vinsonii<br />
subsp. berkhoffi and related members of the Alpha Subdivision<br />
of the Proteobacteria in dogs with cardiac arrhythmias, endocarditis,<br />
or myocarditis. J Clin Microbiol 37:3618–3626, 1999.<br />
34. Breitschwerdt EB, Kordick DL: Bartonellosis. JAVMA 206:<br />
1928–1931, 1995.<br />
35. Bennett D, Bilbertson EM, Grennan D: Bacterial endocarditis<br />
with polyarthritis in two dogs associated with circulating<br />
autoantibodies. J Small Anim Pract 19:185–196, 1993.<br />
36. Bennett D, Taylor DJ: Bacterial endocarditis and inflammatory<br />
joint disease in the dog. J Small Anim Pract 29:347–353, 1988.<br />
37. Neugarten J, Gallo GR, Baldwin DS: Glomerulonephritis in<br />
bacterial endocarditis. Am J Kidney Dis 3:371–379, 1984.<br />
38. Perez GO, Rothfield N, Williams RC: Immune-<strong>com</strong>plex<br />
nephritis in bacterial endocarditis. Arch Intern Med 136:<br />
334–336, 1976.<br />
39. Caywood DD, Wilson JW, O’Leary TP: Septic polyarthritis<br />
associated with bacterial endocarditis in two dogs. JAVMA<br />
171:549–552, 1977.<br />
40. Gutman RA, Striker GE, Gilliland BC, et al: The immune <strong>com</strong>plex<br />
glomerulonephritis of bacterial endocarditis. Medicine<br />
51:1–25, 1972.<br />
41. Root CR, Bahr RJ: The heart and great vessels, in Thrall DE<br />
(ed): Textbook of Veterinary Diagnostic Radiology, ed 3. Philadelphia,<br />
WB Saunders Co, 1994, pp 304–318.<br />
42. Dow SW, Curtis CR, Jones RL, et al: Bacterial culture of blood<br />
from critically ill dogs and cats: 100 cases (1985–1987). JAVMA<br />
195:113–117, 1989.<br />
43. Washington JA: The microbiologic diagnosis of infective endocarditis.<br />
J Antimicrob Chemother 20:29–39, 1987.<br />
44. Washington JA: The role of the microbiology laboratory in the<br />
diagnosis and antimicrobial treatment of endocarditis. Mayo<br />
Clin Proc 57:22–32, 1982.<br />
45. Hoen B, Selton-Suty C, Lacassin F, et al: Infective endocarditis<br />
in patients with negative blood cultures. Clin Infect Dis<br />
20:501–506, 1995.<br />
46. Cremieux AC, Maziere B, Vallois JM, et al: Evaluation of antibiotic<br />
diffusion into cardiac vegetations by quantitative autoradiography.<br />
J Infect Dis 159:938–944, 1989.<br />
47. Working Party of the British Society for Antimicrobial<br />
Chemotherapy. Antibiotic treatment of streptococcal, enterococcal,<br />
and staphylococcal endocarditis. Heart 1998 79:207–210, 1998.
Compendium August 2002 Infective Endocarditis 625<br />
48. Wilson WR, Karchmer AW, Dajani AS, et al: Antibiotic treatment<br />
of adults with infective endocarditis due to streptococci,<br />
enterococci, and staphylococci, and HACEK microorganisms.<br />
JAMA 274:1706–1713, 1995.<br />
49. Scheld WM: Evaluation of quinolones in experimental animal<br />
models of infection. Eur J Clin Microbiol Infect Dis 10:275–290,<br />
1991.<br />
50. Aronson AL, Aucoin DP: Antimicrobial drugs, in Ettinger SJ<br />
(ed): Textbook of Veterinary Internal Medicine, ed 3. Philadelphia,<br />
WB Saunders Co, 1989, pp 409–410.<br />
51. Kvart C, Haggstrom J, Pedersen HD, et al: Efficacy of enalapril<br />
for prevention of congestive heart failure in dogs with myxomatous<br />
valve disease and asymptomatic mitral regurgitation. J Vet<br />
Intern Med 16:80–88, 2002.<br />
52. Tormas P, Almirante B, Mirabet S, et al: Infective endocarditis<br />
due to Staphylococcus aureus: Deleterious effect of anticoagulant<br />
therapy. Arch Intern Med 159:473–475, 1999.<br />
53. Kupferwasser LI, Yeaman MR, Shapiro SM, et al: Acetylsalicylic<br />
acid reduces vegetation bacterial density, hematogenous bacterial<br />
dissemination, and frequency of embolic events in experimental<br />
Staphylococcus aureus endocarditis through antiplatelet and antibacterial<br />
effects. Circulation 99:2791–2797, 1999.<br />
54. Blatter M, Francioli P: Endocarditis prophylaxis: From experimental<br />
models to human re<strong>com</strong>mendation. Eur Heart J 16<br />
(Suppl B):107–109, 1995.<br />
55. Durack DT: Prevention of infective endocarditis. N Engl J Med<br />
332:38–44, 1995.<br />
56. Rosin E, Dow SW, Daly WR, et al: Surgical wound infection and<br />
use of antibiotics, in Slatter D (ed): Textbook of Small Animal<br />
Surgery, ed 2. Philadelphia, WB Saunders Co, 1993, pp 89–91.<br />
ARTICLE<br />
CE<br />
#3 CE TEST<br />
The article you have read qualifies for 1.5 contact<br />
hours of Continuing Education Credit from<br />
the Auburn University College of Veterinary Med-<br />
icine. Choose the best answer to each of the follow-<br />
ing questions; then mark your answers on the<br />
postage-paid envelope inserted in Compendium.<br />
1. Which dog is least likely to develop IE?<br />
a. 6-year-old male German shepherd<br />
b. 11-year-old male miniature poodle<br />
c. 5-year-old male golden retriever<br />
d. 7-year-old female boxer<br />
e. 3-year-old female rottweiler with congenital<br />
subaortic stenosis<br />
2. Which heart valve is most often affected by IE?<br />
a. mitral<br />
b. pulmonic<br />
c. tricuspid<br />
d. aortic<br />
e. All valves are affected with equal frequency.<br />
3. Which sign by itself is most indicative of IE?<br />
a. diastolic heart murmur<br />
b. fever<br />
www.<strong>VetLearn</strong>.<strong>com</strong><br />
c. inflammatory leukogram<br />
d. systolic heart murmur<br />
e. shifting leg lameness<br />
4. Which microbe is least often a proven cause of IE in<br />
dogs?<br />
a. staphylococci<br />
b. gram-positive bacteria<br />
c. fungal agents<br />
d. streptococci<br />
e. Bartonella<br />
5. When the infecting microbe and its antibiogram<br />
results are not identified, which drug is the best first<br />
choice for treating IE in dogs?<br />
a. ampicillin<br />
b. first-generation cephalosporin<br />
c. gentamicin<br />
d. clindamycin plus enrofloxacin<br />
e. metronidazole<br />
6. Which clinical sign of CHF is least likely in a dog with IE?<br />
a. coughing<br />
b. dyspnea<br />
c. pulmonary edema<br />
d. ascites<br />
e. exercise intolerance<br />
7. Which sign is most suggestive of IE in a 4-year-old<br />
German shorthaired pointer?<br />
a. V/VI systolic heart murmur that was not present 6<br />
months previously<br />
b. inflammatory leukogram<br />
c. monocytosis<br />
d. fever<br />
e. lameness<br />
8. The most difficult aspect of antibiotic treatment of IE is<br />
a. choosing an antibiotic.<br />
b. the cost.<br />
c. safety.<br />
d. maintaining long-term parenteral administration.<br />
e. developing antibiotic resistance.<br />
9. Which drug is most likely to kill the two bacterial<br />
species most often involved in canine IE?<br />
a. gentamicin d. penicillin<br />
b. enrofloxacin e. ampicillin<br />
c. cephazolin<br />
10. Which factor is least likely to predispose dogs to IE?<br />
a. stomatitis/gingivitis<br />
b. chronic wounds<br />
c. bacterial prostatitis<br />
d. corticosteroid administration<br />
e. myxomatous mitral valve disease