Dr. B. Marciniak : anesthésie néonatale, état de la question - virtanes
Dr. B. Marciniak : anesthésie néonatale, état de la question - virtanes
Dr. B. Marciniak : anesthésie néonatale, état de la question - virtanes

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
«Apoptose et Anesthésie»<br />
Anesthésie néonatale : état <strong>de</strong> <strong>la</strong> <strong>question</strong> .<br />
Département <strong>de</strong> Mé<strong>de</strong>cine Aiguë<br />
Université Catholique <strong>de</strong> Louvain<br />
«Apoptose et Anesthésie».<br />
Bruno <strong>Marciniak</strong> MD<br />
UF Anesthésie <strong>de</strong> l’Enfant<br />
Centre Hospitalier Régional<br />
Universitaire
« Agents used in pediatric and obstetrical<br />
medicine for purposes of sedation,<br />
anesthesia, and seizure management may<br />
cause apoptotic neuronal <strong>de</strong>ath in the<br />
<strong>de</strong>veloping human brain. »<br />
Ikonomidou C.-Olney JW et al. Biochem Pharmacol 2001; 62:401-405
Anesthésie néonatale : état <strong>de</strong> <strong>la</strong> <strong>question</strong> <br />
Département <strong>de</strong> Mé<strong>de</strong>cine Aiguë<br />
Université Catholique <strong>de</strong> Louvain<br />
«Apoptose et Anesthésie».<br />
Bruno <strong>Marciniak</strong> MD<br />
UF Anesthésie <strong>de</strong> l’Enfant<br />
Centre Hospitalier Régional<br />
Universitaire
« Physiologic responses to painful stimuli<br />
have been well documented in<br />
neonates of various gestational ages<br />
and are reflected in hormonal, metabolic,<br />
and cardiorespiratory changes simi<strong>la</strong>r to<br />
but greater than those observed in adult<br />
subjects »<br />
K.J.S. Anand, m.B.B.S., D.Phil., And p.R. Hickeythe Pain and its effects in the human neonate<br />
and fetus NEW ENGLAND JOURNAL OF MEDICINE, Volume 317, Number 21: Pages 1321-1329,<br />
19 November 1987.
Douleur<br />
Stress<br />
APOPTOSE<br />
A<br />
n<br />
e<br />
s<br />
t<br />
h<br />
e<br />
s<br />
i<br />
e
Anesthésie néonatale : état <strong>de</strong> <strong>la</strong> <strong>question</strong> !<br />
Département <strong>de</strong> Mé<strong>de</strong>cine Aiguë<br />
Université Catholique <strong>de</strong> Louvain<br />
«Apoptose et Anesthésie».<br />
Bruno <strong>Marciniak</strong> MD<br />
UF Anesthésie <strong>de</strong> l’Enfant<br />
Centre Hospitalier Régional<br />
Universitaire
« Blocka<strong>de</strong> of NMDAglutamate receptors for only a<br />
few hours during <strong>la</strong>te fetal or early neonatal life<br />
triggered wi<strong>de</strong>spread apoptotic<br />
neuro<strong>de</strong>generation in the <strong>de</strong>veloping rat brain.<br />
These findings may have relevance to human<br />
neuro<strong>de</strong>velopmental disor<strong>de</strong>rs involving<br />
prenatal (drug-abusing mothers) or postnatal<br />
(pediatric anesthesia) exposure to drugs that<br />
block NMDA receptors. »<br />
Ikonomidou C.-Olney JW et al. Science 1999;283:70-74
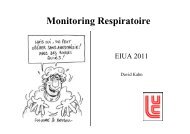
Rats <strong>de</strong> 7 jours<br />
Effet dose<br />
Effet temps<br />
dizocilpine<br />
Effet âge<br />
Rats <strong>de</strong> 0-3-7-14-21 j<br />
0 3 7 14 21<br />
Rates enceintes 17-19-21j<br />
Effet terme
Blocka<strong>de</strong> of NMDA receptors for 4 hours is sufficient to<br />
trigger apoptotic neuro<strong>de</strong>generation in the <strong>de</strong>veloping<br />
mammalian brain.<br />
Blocka<strong>de</strong> of NMDA receptors gives rise to different patterns<br />
of neuronal loss <strong>de</strong>pending on the stage of <strong>de</strong>velopment at<br />
which the interference occurs. Such a mechanism could<br />
contribute to a variety of neuropsychiatric disor<strong>de</strong>rs.
« Of mice and men »<br />
- adaptabilité<br />
- complexité<br />
Considérations méthodologiques<br />
- Dose/Durée<br />
- Métho<strong>de</strong> prélèvement/analyse<br />
- Surveil<strong>la</strong>nce<br />
- Buts<br />
- Statut nutritionnel<br />
caenorhabditis_elegans
Dose et durée<br />
• Anesthésie prolongée par halothane<br />
ou NMDA bloqueurs *<br />
– Neurodégénérescence cérébrale rats nnés<br />
Science, 1999<br />
Olney et al<br />
• Injections répétées kétamine**<br />
– Augmentation mort neuronale rat nné<br />
– Perte poids<br />
• Injection unique kétamine **<br />
– Absence d’effets<br />
Ped Anes 2002<br />
Soriano et al<br />
Scallet Toxicol sci 2004<br />
Petites doses<br />
Attention aux conditions expérimentales<br />
(peuvent correspondre à plusieurs semaines d’anesthésie chez l’homme)
Métho<strong>de</strong> prélèvement/analyse<br />
Cultures cellu<strong>la</strong>ires<br />
- <strong>de</strong>capitation<br />
- prélèvement cérébral<br />
- traitements cellu<strong>la</strong>ires<br />
…<br />
Coupes histologiques<br />
- dé<strong>la</strong>i <strong>de</strong> prélèvement<br />
- métho<strong>de</strong> <strong>de</strong> mise à mort<br />
…<br />
Quelle influence sur <strong>de</strong>s organes vulnérables
Buts<br />
Anand et al<br />
Biol Neonat 2000<br />
• Rat nné: douleur répétée entraîne<br />
changement comportemental<br />
• Analgésie peut prévenir ces<br />
changements<br />
Anand et al<br />
Physiol Behav 2001<br />
Influence du stress chirurgical non évaluée
Statut nutritionel<br />
• Malnutrition<br />
– Diminution poids cerveau<br />
– Diminution QI<br />
prématurés<br />
Br Med J, 1998<br />
Cole et al<br />
Supplémentation nutritionnelle, apport glucosé<br />
pendant toute <strong>la</strong> durée périopératoire chez l’enfant.
DEGENERESCENCE<br />
SCULPTURE<br />
DU<br />
VIVANT<br />
TUMORAL<br />
IMMUNITE<br />
APOPTOSE<br />
TOXIQUE<br />
LESIONEL
DEGENERESCENCE<br />
SCULPTURE<br />
DU<br />
VIVANT<br />
TUMORAL<br />
IMMUNITE<br />
APOPTOSE<br />
TOXIQUE<br />
VULNERABILITE<br />
LESIONEL
Aspect sélectif <strong>de</strong> <strong>la</strong> vulnérabilité régionale en fonction <strong>de</strong> l’âge au moment <strong>de</strong> <strong>la</strong> lésion<br />
24SA<br />
2 ans<br />
Terme<br />
6 j<br />
Ferriero, D. M. N Engl J Med 2004;351:1985-1995
25<br />
20<br />
15<br />
10<br />
*<br />
**<br />
***<br />
I II III IV V<br />
GROUPE D’AGE<br />
Misra et al. Ind J Med Res 1997<br />
SODIUM FLUORESCEIN IN CSF<br />
( ng/mL )
L’EVIDENCE LESIONELLE
Mecanismes<br />
Destruction cellu<strong>la</strong>ire cérébrale<br />
• necrose<br />
• apoptose<br />
• Ca +2 accumu<strong>la</strong>tion<br />
• excitotoxicité, activation protease<br />
• hyperglycolyse<br />
• radicaux libres, lésions axonales<br />
Mort neuronale
Definition<br />
Lésion neuronale : necrose<br />
Destruction <strong>de</strong> <strong>la</strong> membrane cytop<strong>la</strong>smique<br />
par excitotoxicité .<br />
Dysfonction du cytosquelette et libération du<br />
contenu intracellu<strong>la</strong>ire .<br />
Mort cellu<strong>la</strong>ire
Neurone<br />
Nécrose<br />
Contusion
Extrusion<br />
nucleaire<br />
apoptose<br />
oe<strong>de</strong>me<br />
mort<br />
Penumbra<br />
(apoptose)<br />
penlucida
Definition<br />
Apoptose :<br />
•Mort cellu<strong>la</strong>ire programmée sans<br />
libération du contenu cytop<strong>la</strong>smique ni<br />
dommage pericellu<strong>la</strong>ire.<br />
•Les proteines proapoptotiques agissent à<br />
<strong>la</strong> surface <strong>de</strong> <strong>la</strong> membrane<br />
mitochondriale, déclenchant l’activation<br />
<strong>de</strong>s caspases et <strong>la</strong> mort cellu<strong>la</strong>ire.
Inf<strong>la</strong>mmation<br />
Brainstem<br />
Reflexes<br />
ACh<br />
A<strong>de</strong>nosin<br />
Hyperglycolysis<br />
NO<br />
DSC<br />
Vasogenique<br />
Oedème<br />
Ischemie<br />
Necrose<br />
Excitotoxicité<br />
Oe<strong>de</strong>me cerebral diffus<br />
Lésion neuronale - Apoptose
apoptose<br />
Degenerescence axonale
Mecanisme <strong>de</strong> <strong>la</strong> lésion cérébrale chez le nouveau né à terme<br />
Ferriero, D. M. N Engl J Med 2004;351:1985-1995
Oedème cérébral diffus (enfants)<br />
Mécanismes<br />
• stimu<strong>la</strong>tion du locus céruléus ( DSC) Bruce Neurosur 1981<br />
• perte <strong>de</strong> l’autorégu<strong>la</strong>tion (e.g. endothelin-1)<br />
- 40% TCC sévère Armstead Am J Physiol 2001 ; Ruppel CCM 2001<br />
• vasodi<strong>la</strong>tation reflexe médiée par libération <strong>de</strong><br />
médiateurs dans le 3ème et 4ème ventricule<br />
- procalcitonine Han et al . Crit Care Med 2000<br />
- adénosine (A1 et A2a) Robertson et al . J Neurotrauma 1999<br />
- nitrosothioles Bayir et al . Neurosurgery 2001
Oedème cérébral diffus (enfants)<br />
Mécanismes (2)<br />
• hyperémie réactive (CBV ) Bruce et al . J Neurosurg 1984<br />
- ischémie cérébrale<br />
• traumatisme vascu<strong>la</strong>ire direct, altération du<br />
tonus vasomoteur (tronc cérébral) Langfitt Am J Physiol 1992<br />
• diminution du volume <strong>de</strong> LCR amortissant le<br />
dép<strong>la</strong>cement cérébral Bissonnette Ped Anesthesia Textbook 2002
Oedème cérébral diffus (enfants)<br />
Mécanismes (3)<br />
• perméabilité <strong>de</strong> <strong>la</strong> BHE (e.g. excitotoxicité)<br />
Ruppel et al . J Pediatr 2001<br />
• dysfonction <strong>de</strong> <strong>la</strong> BHE (i.e. oedème vasogénique)<br />
Ruppel et al . J Pediatr 2001<br />
• oedème ‘osmo<strong>la</strong>ire’ Bayir et al . Crit Care Med 2001<br />
• oedème ‘cellu<strong>la</strong>ire’ (e.g. cytotoxique)<br />
Janesko. J Neurotrauma 2001<br />
• dysfonction circu<strong>la</strong>toire mécanique Bissonnette (In press)
Lésion cérébrale<br />
SAH<br />
Instabilité<br />
vascu<strong>la</strong>ire<br />
cellu<strong>la</strong>ire<br />
BHE<br />
ischemie<br />
LCR<br />
resistance<br />
augmentées<br />
Volume<br />
sanguin<br />
Oe<strong>de</strong>me<br />
cérébral<br />
oe<strong>de</strong>me<br />
oe<strong>de</strong>me<br />
PIC ⇑⇑⇑<br />
oe<strong>de</strong>me
Fonction cérébrale et débit<br />
sanguin<br />
DSC<br />
25<br />
18<br />
Fonction neuronale normale<br />
Baisse fonction neuronale<br />
Abolition fonction neuronale<br />
Absence autoregu<strong>la</strong>tion<br />
}<br />
Electro<br />
-<br />
genese<br />
Inhibition vasoreactivite au CO 2<br />
Alteration membrane<br />
Abolition fonction membrane<br />
12<br />
10<br />
Mort neuronale-Apoptose
Fonction et débit sanguin cérébral<br />
[ml/min/100g brain]<br />
30<br />
20<br />
10<br />
“Penlucida” ” area<br />
“Penombre”<br />
Zone <strong>de</strong> nécrose<br />
Mort neuronale<br />
apoptose<br />
Minutes<br />
1 2 3 4<br />
E<strong>la</strong>psed time [hours]<br />
Permanent<br />
Bissonnette B. Pediatric Anesthesia: Principles and Practice, 2001
N 2 0 et ischémie cérébrale<br />
• N 2 0 est un antagoniste NMDA, reduisant<br />
<strong>la</strong> libération <strong>de</strong> glutamate (Jevtovic-Todorovic et al. Nature<br />
Med 1998)<br />
• N 2 0 peut causer lésion neuronale (Jevtovic-Todorovic<br />
et al. J Neurosurg Anesth 2003)<br />
• N 2 0 probablement délètere par activation<br />
<strong>de</strong>s GABA recepteurs (Frank et al. Nature Med 1998)<br />
• Pentobarbital eliminate les effets toxiques<br />
du N 2 0 chez le rat, mais pas étudié en cas<br />
d’ischémie (Jevtovic-Todorovic et al. Nature Med 2000)
INFLUENCE DE L’HYPOCAPNIE<br />
Laffey, J. G. et al. N Engl J Med 2002;347:43-53
Influence <strong>de</strong>s solutés<br />
PAM(mmHg)<br />
120<br />
100<br />
*<br />
18<br />
16<br />
14<br />
PIC (mmHg)<br />
*<br />
*<br />
*<br />
80<br />
12<br />
60<br />
10<br />
8<br />
40<br />
20<br />
Ringer Lacate<br />
NaCl Hyper<br />
6<br />
4<br />
2<br />
Ringer Lactate<br />
Nacl Hyper<br />
0<br />
0<br />
Baseline<br />
Hemorr.<br />
1 hr.<br />
3 hr.<br />
12 hr.<br />
Baseline<br />
Hemorr.<br />
1 hr.<br />
3 hr.<br />
12 hr.<br />
* P
7<br />
6<br />
Influence <strong>de</strong> <strong>la</strong> PA<br />
*<br />
Episo<strong>de</strong>s hypotensifs<br />
5<br />
4<br />
3<br />
2<br />
1<br />
0<br />
*<br />
Bon<br />
*<br />
*<br />
*<br />
Modéré Sévère Végétatif Mort<br />
G<strong>la</strong>sgow Outcome Scale<br />
Kokoska et al. J Pediatr Surg 1999
PRESSION ARTERIELLE<br />
Stimulus
RESSION DE LA FONTANELLE<br />
Stimulus
Conséquences<br />
Lang et al. J Neurosurg 1996
Concept thérapeutique<br />
Ischemie<br />
Défaut énergie<br />
Excitotoxicité<br />
Arrêt mitochondrie<br />
Stress Oxidatif<br />
Apoptose<br />
Inhibition Oe<strong>de</strong>me<br />
Cerebral secondaire<br />
Activation processus<br />
Biologique <strong>de</strong><br />
régénartion<br />
Maximisation <strong>de</strong><br />
compensation<br />
<strong>de</strong>s fonctions restantes<br />
- croissance neuronale<br />
- stimu<strong>la</strong>tion pharmaco<br />
- transp<strong>la</strong>ntation cell.
DEGENERESCENCE<br />
SCULPTURE<br />
DU<br />
VIVANT<br />
TUMORAL<br />
IMMUNITE<br />
APOPTOSE<br />
TOXIQUE<br />
LESIONEL
Mécanisme évoqué<br />
Bloqueur NMDA<br />
ketamine, N2O Xe<br />
(Franks NP Nature1994<br />
Jevtovic-Todorovic V NatMed 1998<br />
Mennerick S. J Neurosci 1998 )<br />
GABA A<br />
benzodiazepine, barbituriques,, propofol<br />
etomidate, iso, enf, halothane<br />
(Franks NP Nature1994)<br />
Early Exposure to Common Anesthetic Agents Causes Wi<strong>de</strong>spread Neuro<strong>de</strong>generation in the<br />
Developing Rat Brain and Persistent Learning Deficits<br />
Vesna Jevtovic-Todorovic et al. J. Neurosci. 2003
QUELLES EVIDENCES <br />
A dose thérapeutique 1 seule: N2O
Douleur<br />
Stress<br />
APOPTOSE<br />
A<br />
n<br />
e<br />
s<br />
t<br />
h<br />
e<br />
s<br />
i<br />
e
EVIDENCE EXTRAPOLATION<br />
APOPTOSE <br />
Douleur<br />
Stress<br />
A<br />
N<br />
E<br />
S<br />
T<br />
.<br />
E<br />
P<br />
I<br />
D<br />
E<br />
M<br />
I<br />
O
Frèquence <strong>de</strong> prescription hors AMM chez l’enfant<br />
`t Jong, G. W. et al. N Engl J Med 2000;343:1125
Yeh, T. F. et al. N Engl J Med 2004;350:1304-1313
INTERPRETATION<br />
CHOIX<br />
PRUDENCE<br />
PRUDENCE<br />
PRUDENCE<br />
ACTES