Multicellular Parasites
Multicellular Parasites
Multicellular Parasites

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
M U L T I C E L L U L A R P A R A S I T E S<br />
A number of species of parasitic worms can inhabit the human<br />
intestinal tract and cause disease. While not microorganisms,<br />
they are studied and diagnosed using microscopic and immunologic<br />
techniques familiar to microbiologists. Some invade tissue<br />
and others do not, so that their presence in the body is often<br />
called an infestation rather than an infection. These worms, or<br />
helminths, are divided into two groups, the roundworms and<br />
the flatworms, and the flatworms are further divided into the<br />
tapeworms and the flukes. Tapeworms are ribbon-shaped and<br />
segmented, while flukes are generally shorter and leaf-shaped.<br />
Tapeworms differ from the other parasitic helminths in that they<br />
lack a digestive tract; they absorb nutrients through their skin. In<br />
most instances the helminths themselves are difficult to find and<br />
examine, so that they are identified by the microscopic appearance<br />
of their eggs, or ova, which are often present in the host’s<br />
feces in large numbers. The ova of each helminth species are distinctive<br />
and can be identified on the basis of size, shape, thickness<br />
of the outer covering, embryonation, and other features.<br />
Some helminths have complex life cycles, involving one or more<br />
intermediate hosts where early stages of development occur,<br />
and a definitive host where the sexually mature forms occur.<br />
Generally, helminths have male and female forms, but most of<br />
the flatworms are hermaphroditic, meaning that both male and<br />
female sex organs reside in the same worm.<br />
Diseases Due to Intestinal<br />
Roundworms<br />
Some notable examples of diseases due to roundworms (nematodes)<br />
are discussed in this section. Pinworm disease, whipworm<br />
disease, and ascariasis are acquired by ingesting ova. Hookworm<br />
disease and strongyloidiasis are contracted by skin penetration<br />
by worm larvae, and trichinosis by eating undercooked meat<br />
containing worm larvae.<br />
Pinworm Disease (Enterobiasis)<br />
Pinworm disease, enterobiasis, is caused by the pinworm, Enterobius<br />
vermicularis. It is the most common helminth disease seen<br />
by American physicians, and pinworms infest more than 200<br />
million people worldwide.<br />
Symptoms<br />
About one-third of individuals infested with E. vermicularis are<br />
asymptomatic. The most common symptom in adults is anal<br />
itching, sometimes accompanied by vaginal irritation. Sleeplessness,<br />
nightmares, nervousness, irritability, anal pain, and weight<br />
loss are common in affected children.<br />
Causative Agent.<br />
Enterobius vermicularis is a tiny roundworm; the females average<br />
about 10 mm in length, and the males, 2 to 3 mm. The<br />
female has a sharply pointed tail end, which inspired its popular<br />
name pinworm. The worms can often be detected in the anal<br />
area by using a flashlight about 2 hours after retiring, or early in<br />
the morning. Ova can be collected from the anal area by pressing<br />
transparent tape against the anus. The pinworm ova are<br />
elongated and have a distinctive appearance, flat on one side and<br />
containing a larval worm (figure 24.26a).<br />
Pathogenesis<br />
The worms live mainly in the upper part of the large intestine.<br />
They may, however, migrate throughout the intestinal and<br />
female genital tracts during their 1- to 2-month life span, feeding<br />
on bacteria and other intestinal material. Tiny ulcerations<br />
and inflammation occur where the worms attach to the intestinal<br />
epithelium. The male worms die soon after mating. The<br />
mature females containing 5,000 to 15,000 ova migrate out of<br />
the anus, usually while their host is sleeping, deposit their eggs<br />
in a sticky matrix, and die. Figure 24.26b shows the enormous<br />
numbers of ova present in a single worm. The sensation caused<br />
by worms exiting the anus leads to scratching, bleeding, and<br />
bacterial infection. If the anal area is not kept clean, eggs<br />
deposited there hatch, and the larval worms crawl through the<br />
anus, enter the intestine, and perpetuate the infestation.<br />
Epidemiology<br />
Scratching deposits E. vermicularis ova on the fingers and under<br />
the fingernails. Because of the enormous numbers of ova, clothing,
(a)<br />
(b)<br />
Ova<br />
Body<br />
100 µm<br />
0.5 mm<br />
Figure 24.26 Pinworm, Enterobius vermicularis (a) Microscopic view of<br />
the ova, showing flattened side and developing worm larva. (b) Body of the adult<br />
worm surrounded by thousands of its ova.<br />
bedding, various surfaces, and even the air in the household<br />
become contaminated. Inhaled and ingested ova are swallowed<br />
and hatch in the small intestine, and the larval worms reach<br />
maturity in 2 to 6 weeks. Ova can survive for about a week in<br />
cool moist conditions, but they quickly die if conditions are hot<br />
and dry. Enterobiasis occurs worldwide and, unlike most other<br />
helminth diseases, is more common in temperate climates and<br />
does not spare upper socioeconomic groups. Humans are the<br />
only host for E. vermicularis.<br />
Prevention and Treatment<br />
Hygienic habits and good ventilation minimize the risk of<br />
acquiring E. vermicularis. Treatment is easy because effective<br />
medications are available, but preventing reinfestation is difficult.<br />
All members of a household must be treated simultaneously,<br />
even those without symptoms. Clothing and bedding<br />
should be washed in hot water, and household surfaces thor-<br />
(a)<br />
(b)<br />
20 µm<br />
Figure 24.27 Whipworm, Trichuris trichiura (a) The slender anterior<br />
portion is embedded in the mucous membrane, while the thicker portion protrudes into<br />
the intestinal lumen. (b) Ovum. Notice the long oval shape, thick wall, and plugs at<br />
each end.<br />
oughly cleaned. Ideally, heat in the household should be turned<br />
up and all members take a vacation for a week.<br />
Whipworm Disease (Trichuriasis)<br />
Whipworm disease, trichuriasis, affects an estimated 500 to 800<br />
million people in warm and wet regions of the world where people<br />
defecate on the ground or use human feces for fertilizer.<br />
Symptoms<br />
Most infestations, even with as many as 100 worms, are asymptomatic.<br />
Very heavy infestations can cause anemia from blood<br />
loss, weight loss, abdominal pain, diarrhea, and protrusion of<br />
the bowel through the rectum from forcefully straining to expel<br />
the worms.<br />
Causative Agent<br />
The causative agent of trichuriasis is the whipworm, Trichuris<br />
trichiura. The worms are 3 to 5 cm long, with a slender anterior<br />
portion and a short, thicker posterior portion, hence the<br />
name whipworm (figure 24.27a). The unmistakable ova can be<br />
found by microscopic examination of the feces (figure 24.27b).
Pathogenesis<br />
Trichuriasis is contracted by ingesting the mature T. trichiura ova.<br />
The ova hatch in the small intestine, and the emerging larvae burrow<br />
into pockets in the intestinal epithelium. Here they develop<br />
for about a week, then return to the bowel lumen and migrate to<br />
the large intestine. They become sexually mature and start producing<br />
eggs in 1 to 2 months. The slender anterior region of the<br />
worm is inserted into the intestinal mucosa, with the thicker portion<br />
protruding into the bowel lumen. The intestinal epithelium<br />
is damaged by the penetrating worm, causing blood loss and an<br />
inflammatory response. Sometimes people infested with T. trichiuria<br />
develop hives because of allergy to worm antigens.<br />
Epidemiology<br />
Infection is by the fecal-oral route. Each mature female worm produces<br />
about 5,000 ova per day. These ova are eliminated with the<br />
feces and can contaminate hands and foods, but they are not immediately<br />
infectious. The ova require about 3 weeks in a warm, moist,<br />
and shady place before they are capable of parasitizing a new host.<br />
The worms can live 3 to 8 years, so that repeated ingestions of eggs<br />
can cause a large buildup of the numbers of the worms in a person’s<br />
intestine. Also, because of the long life of T. trichiura, the<br />
worms are frequently found in people who traveled to endemic<br />
areas years ago. Humans are the only reservoir for T. trichiura.<br />
Prevention and Treatment<br />
Trichuriasis is prevented by proper disposal of human feces and<br />
other sanitary measures. Several medications provide safe and<br />
effective treatment of the disease.<br />
Ascariasis<br />
Ascariasis is a helminthic disease caused by Ascaris lumbricoides,<br />
the largest and most prevalent human roundworm. Worldwide,<br />
an estimated 1 billion people are infested.<br />
Symptoms<br />
Most cases of ascariasis are asymptomatic. Many individuals<br />
infested with the worms, however, develop one or more bouts of<br />
fever, trouble breathing, coughing, and wheezing. Some infested<br />
people have the frightening experience of vomiting up a large<br />
worm, or passing one in their feces; others develop abdominal<br />
pain when the worms obstruct the intestine or gallbladder.<br />
Causative Agent<br />
Ascaris lumbricoides (see figure 24.28) is a roundworm prevalent<br />
worldwide in areas where human feces contaminate the<br />
soil. Female worms are enormous, ranging from 20 to 45 cm<br />
long and 3 to 6 mm wide, while males are somewhat smaller.<br />
The ova are nearly spherical, with a thick wall and irregular<br />
outer surface (see figure 24.28). The life cycle of A. lumbricoides<br />
is complex. The ova released by mature females are eliminated<br />
with the host’s feces. The tiny worm larva inside the ova<br />
must develop in soil or other location outside the host’s body<br />
for at least 1 1 / 2 weeks before they can survive and mature in a<br />
new host. After being swallowed by the new host, the ova hatch<br />
in the duodenum. At this point, the tiny larval worms do some-<br />
thing totally unexpected. Instead of staying in the intestine,<br />
they burrow through the intestinal epithelium, enter the circulatory<br />
system, and are carried throughout the body. Those that<br />
reach the lungs push through the capillary walls into the alveoli.<br />
Here they undergo further development, reach 1 to 2 mm<br />
in length, and shed their covering twice to get ready for the rest<br />
of their journey. After about 10 days, they move out of the alveoli<br />
into the air passages of the lungs, and they are coughed up<br />
and swallowed (figure 24.28). The developmental changes<br />
that take place in the lungs make them resistant to stomach<br />
juices, and so they pass safely through the stomach into the<br />
small intestine. They mature to adulthood after about 2 months<br />
in the upper small intestine, feeding on intestinal contents.<br />
They live about 1 year.<br />
Pathogenesis<br />
Large masses of worms can obstruct the intestine, while wandering<br />
worms can obstruct or perforate various organs. Except<br />
for the larval worms that reach the lung, circulating larvae lodge<br />
in capillaries throughout the body and die, causing an inflammatory<br />
and immune response and consequent aches, pains, and<br />
fever. The larval penetration into the lungs causes microscopic<br />
bleeding, which if widespread, can predispose one to bacterial<br />
pneumonia; lesser amounts of damage provoke inflammatory<br />
and immune responses, coughing, wheezing, and pain.<br />
Roundworms of some species of animals can penetrate<br />
human tissues but cannot complete their life cycle. Instead, their<br />
larvae wander through the tissues and eventually die, causing an<br />
intense inflammatory reaction. Preschool children are especially<br />
susceptible to this condition, called visceral larva migrans,<br />
because of their tendency to put rocks and dirt into their<br />
mouths. If the material is contaminated with certain roundworm<br />
ova, the eggs hatch, and the larvae migrate through body<br />
tissues. One example is Toxocara canis, an intestinal roundworm<br />
of dogs that resembles A. lumbricoides. This helminth can cause<br />
damage to various organs of a child, even blindness when its larvae<br />
lodge in the eyes.<br />
Epidemiology<br />
Humans are the only natural hosts of A. lumbricoides. A closely<br />
similar helmith of pigs can sometimes infect people. The<br />
helminth female produces more than 200,000 ova daily. These<br />
ova are remarkably resistant to heat, cold, drying, and disinfectants.<br />
Moreover, the ova remain infectious for up to 10 years,<br />
contaminating soil, dust, and food. In many areas of the world,<br />
human feces is used as fertilizer for food crops, and children<br />
defecate outdoors causing extensive soil contamination. Young<br />
children commonly place soiled objects into their mouth, and<br />
they are prone to eat soil if they are anemic or iron deficient.<br />
Children may have 50 or more worms, the record being well<br />
over 1,000.<br />
Prevention and Treatment<br />
Prevention of ascariasis depends on hygienic practices and sanitary<br />
disposal of human feces. Effective and safe medications are<br />
available for treating the disease.
Bronchiole<br />
Alveolus<br />
(c) Larvae in the lung<br />
leave the capillaries<br />
and enter alveoli<br />
and bronchioles<br />
(d) Larvae from lung<br />
enter esophagus<br />
and then gastrointestinal<br />
tract<br />
Figure 24.28 (a–f) Life Cycle of Ascaris<br />
lumbricoides, the Largest Roundworm Infesting<br />
the Human Intestine Curiously, larvae hatching in the<br />
intestine migrate through the lungs and back to the<br />
intestine before maturing to adulthood.The ova are nearly<br />
spherical, thick-walled, with a ruffled border.<br />
(f) Eggs passed<br />
in feces<br />
Hookworm Disease<br />
Hookworms infest about 900 million people in warm, wet areas<br />
around the world where people defecate on the ground and do<br />
not wear shoes. Hookworm disease was once common in the<br />
southeastern United States. Asymptomatic individuals are still<br />
seen in most states, but they have contracted their hookworms<br />
in other countries.<br />
Symptoms<br />
The vast majority of hookworm infestations are asymptomatic.<br />
An itchy foot rash commonly occurs at the site of skin penetration<br />
by the worms. Cough, fever, and shortness of breath can<br />
occur, and later, diarrhea, nausea, and vomiting. The most<br />
important symptoms of hookworm disease are mental and physical<br />
retardation in children.<br />
Causative Agents<br />
Necator americanus and Ancylostoma duodenale account for<br />
most cases of human hookworm disease. The worms are about<br />
10 mm long and live in the small intestine, attaching by means<br />
of small hooks or plates located about their mouth. The hookworm<br />
life cycle is shown in figure 24.29. The female worm<br />
(e) Larvae mature<br />
to adulthood<br />
(a) Worm eggs from<br />
contaminated<br />
soil are ingested<br />
(b) Ingested eggs<br />
hatch; larvae<br />
penetrate intestinal<br />
capillaries and<br />
are carried to lung<br />
6 cm<br />
FPO<br />
100 µm<br />
releases her eggs, and they are discharged with the feces, contaminating<br />
soil in places that lack toilets. The eggs hatch in the<br />
soil, releasing tiny larvae that develop in the soil and become<br />
infectious. These larvae generally penetrate the skin of a person’s<br />
feet, wiggle their way into the bloodstream, and are carried<br />
to the heart and lungs. In the lungs, as in ascariasis, they<br />
push through the capillary walls into the alveoli, migrate into<br />
the bronchial tubes, and then enter the gastrointestinal system<br />
when lower respiratory tract secretions are coughed up and<br />
swallowed. Once in the small intestine, the larvae attach and<br />
mature to complete their life cycle.<br />
Pathogenesis<br />
Hookworms feed by sucking the blood of the host. More than<br />
1,000 worms may be found in a single person, and the constant<br />
loss of blood frequently produces anemia. Children who acquire<br />
hookworms may be undernourished already, and the anemia<br />
resulting from hookworm disease may cause weakness, fatigue,<br />
and physical and mental retardation. Initial attachment of the<br />
worms can cause nausea and vomiting. Migration of the larvae<br />
through the lungs causes microscopic bleeding and inflammatory<br />
and immune responses that result in coughing, wheezing,<br />
and shortness of breath. The itchy rash, called ground itch, that
(c) Larvae<br />
mature in the<br />
small intestine<br />
and produce ova<br />
Large<br />
intestine<br />
(d) Hookworm ova<br />
from feces<br />
hatch in soil;<br />
larvae develop<br />
into an<br />
infectious<br />
form<br />
50 µm<br />
Bronchioles Alveoli<br />
(b) Larvae in the<br />
lung leave the<br />
capillaries,<br />
enter the<br />
alveoli and<br />
bronchioles<br />
(a) Larvae penetrate<br />
skin and enter<br />
capillaries<br />
Figure 24.29 (a–d) Life Cycle of a Hookworm Infection begins with penetration of the<br />
skin by the worm larvae.The micrograph shows the thin-walled ovum containing the developing<br />
worm embryo.<br />
often develops between the toes at the site of larval penetration,<br />
is probably an allergic response to repeated exposures.<br />
The larvae of dog and cat hookworms can contaminate<br />
soil and penetrate the skin, especially of people such as plumbers<br />
that sometimes have to crawl in dirt under buildings. The larvae<br />
wander just under the skin surface, causing itchy red tracts<br />
(figure 24.30) that advance as much as 1 to 2 cm per day for a<br />
month or more, before dying. This condition is called cutaneous<br />
larva migrans.<br />
Epidemiology<br />
Hookworm disease occurs around the world in temperate and<br />
tropical climates where the soil is moist, human feces is<br />
deposited on the ground, and people are barefooted. Each<br />
female worm can produce 25 million ova in her lifetime of 2 to<br />
10 years.<br />
Prevention and Treatment<br />
Prevention of hookworm disease depends on sanitary<br />
disposal of human feces and wearing shoes. Highly<br />
effective medications are available to eliminate the<br />
infestation.<br />
Strongyloidiasis<br />
Strongyloidiasis, the disease caused by Strongyloides<br />
stercoralis, occurs in a spotty distribution in warm, wet<br />
areas of the world, with an estimated 400,000 cases in<br />
the southeastern United States and Puerto Rico. This<br />
disease differs from most other helminthic diseases in<br />
that it perpetuates itself indefinitely in the absence of<br />
reexposure to the causative agent.<br />
Symptoms<br />
Most infections are asymptomatic, but abdominal<br />
pain, diarrhea, recurrent rashes on the buttocks and<br />
lower back, and respiratory symptoms can occur with<br />
heavy infestations.<br />
Causative Agent<br />
The adult Strongyloides stercoralis (figure 24.31),<br />
sometimes called a threadworm, is only about 2 mm<br />
long. Its life cycle is similar to that of hookworms with<br />
two important exceptions: (1) the worms can multiply<br />
sexually in the soil; and (2) ova produced by intestinal<br />
worms hatch before they are discharged in the feces.<br />
These intestinal larvae can mature to an infectious<br />
form, penetrate the intestine or the anal skin, and<br />
thereby perpetuate the infection indefinitely.<br />
Pathogenesis<br />
Most individuals with strongyloidiasis are asymptomatic<br />
because their immune system limits tissue invasion.<br />
Heavy infestations, however, can damage the<br />
lungs and intestine, sometimes leading to invasion by<br />
bacterial pathogens. Recurrent rashes result from<br />
hypersensitivity to the larvae at the sites of penetration.<br />
In people who are debilitated, alcoholic, or immunosuppressed,<br />
massive numbers of the worms arise, penetrating<br />
all parts of the body, including the brain. These massive<br />
infections are rapidly fatal unless treated.<br />
Epidemiology<br />
Strongyloidiasis occurs in much the same distribution as hookworm,<br />
but favoring tropical areas. Since the organisms can multiply<br />
in soil, contaminated areas may remain infectious even<br />
when there are no new deposits of human feces. Human infections<br />
can last for a lifetime, and they can be transmitted to other<br />
people through close physical contact. Many American soldiers<br />
contracted the disease during World War II while imprisoned in<br />
Southeast Asia.<br />
Prevention and Treatment<br />
Prevention of strongyloidiasis is the same as for hookworm disease.<br />
Effective medications are available but require a longer
Figure 24.30 Cutaneous Larva Migrans, an Occupational Hazard of<br />
Plumbers and Others Who Crawl Under Buildings Where Dog or Cat Feces<br />
Have been Deposited Larval hookworms from the feces penetrate and wander<br />
under the skin, causing serpentine tracts of inflammation before dying.<br />
100 µm<br />
Figure 24.31 Strongyloides stercoralis Larva in Feces The adult worm is<br />
only about 2 mm long, and has a life cycle similar to hookworms. Unlike other<br />
intestinal roundworms, however, S. stercoralis can multiply in the soil and in the body<br />
of a single host.<br />
period of treatment than for hookworm, and even so, relapses<br />
may occur.<br />
Trichinosis (Trichinellosis)<br />
Trichinosis, also known as trichinellosis, differs from all the roundworm<br />
diseases discussed previously in that it is contracted by eating<br />
inadequately cooked meat. Since pork is a leading source of<br />
infection, the incidence of the disease has fallen markedly in the<br />
United States over the years due largely to federal regulations on<br />
how pigs raised commercially are fed. Nevertheless, the potential<br />
for large outbreaks of the disease still exists because the meat of a<br />
number species of animals can be infectious.<br />
Symptoms<br />
Trichinosis is characterized by abdominal pain and diarrhea, followed<br />
in about a week by fever, muscle pain, swelling around<br />
the eyes, and sometimes a rash. Occasional cases are fatal<br />
because of damage to the heart or brain. The disease occurs<br />
worldwide except for Australia and some Pacific Islands.<br />
Causative Agent<br />
The cause of trichinosis is usually Trichinella spiralis, a 1 to 4 mm<br />
long roundworm that lives in the small intestine of meat-eating<br />
animals, especially rats, pigs, bears, dogs, and humans. Its life<br />
cycle is shown in figure 24.32. The female worm discharges her<br />
living young into the lymph and blood vessels of the host’s<br />
intestine without an intervening egg stage, and those larvae are<br />
carried to all parts of the body. Most of the larvae are killed by<br />
body defenses, but some survive in the muscles of the host<br />
where they become encased with scar tissue. The worms then<br />
stay alive for months or years within the muscle. If the flesh of<br />
an infested pig or other carnivorous animal is eaten by humans<br />
or other animals, the digestive juices of the new host release the<br />
larvae, permitting them to burrow into the new host’s intestinal<br />
lining. The larvae then mature, and the females begin producing<br />
larvae in the new host to complete the life cycle of the<br />
worm. Each female adult Trichinella may live 4 months or more<br />
and produce 1,500 young.<br />
Pathogenesis<br />
The penetration of larval worms into the host’s tissues is responsible<br />
for the symptoms of trichinosis. Abdominal pain and diarrhea<br />
begin within the first week after eating meat containing T.<br />
spiralis, when the worms mature and begin discharging their<br />
larvae. Fever, muscle pain, rash, and facial swelling result from<br />
inflammatory and immune reactions to larvae lodged in various<br />
tissues. Only larvae that penetrate skeletal muscle survive.<br />
Epidemiology<br />
In trichinosis, the same animal generally serves as both the<br />
definitive and the intermediate host, human beings one hopes<br />
being the exception. Almost all warm-blooded carnivores can<br />
be hosts for T. spiralis. Many cases of the disease have been contracted<br />
from the meat of wild animals, including bear, wild boar,<br />
walrus, and cougar.<br />
Prevention and Treatment<br />
Prevention of trichinosis depends on thorough cooking of meat<br />
so that all parts reach at least 170°F (77°C). Pigs raised commercially<br />
must by law be fed only cooked garbage to ensure that<br />
they do not receive meat scraps containing viable Trichinella larvae.<br />
Government inspection of meat does not detect Trichinella<br />
infestation. Larvae in pork are generally killed at 5°F (:15°C) or<br />
lower for 3 weeks if the meat is less than 15 cm thick. Wild<br />
game, however, often harbors Trichinella species that are not<br />
killed by freezing. Medication is available that can probably prevent<br />
the disease in persons who have eaten meat shown to contain<br />
Trichinella, but there is no effective treatment.<br />
MICROCHECK<br />
Parasitic worms are divided into the roundworms<br />
(nematodes) and the flatworms. Flatworms are further<br />
divided into tapeworms (cestodes) and flukes
(b) Larvae deposited<br />
by adult worms into<br />
blood or lymph vessels<br />
(a) Infested meat<br />
is ingested<br />
(trematodes). Roundworm diseases include pinworm,<br />
whipworm, and ascariasis contracted by ingesting worm<br />
ova; hookworm disease and strongyloidiasis, contracted<br />
through skin penetration by the worm larvae; and<br />
trichinosis, acquired by ingesting inadequately cooked<br />
meat containing encysted worm larvae.<br />
■ Why might asymptomatic strongyloidiasis pose a serious<br />
threat to an individual who develops<br />
immunodeficiency?<br />
■ Would you be surprised to see new cases of ascariasis<br />
turning up 3 years after all the inhabitants of a<br />
Southeast Asian village began using outhouses to<br />
deposit their feces? Why or why not?<br />
Diseases Due to Intestinal Flatworms<br />
This section gives some examples of diseases due to tapeworms,<br />
cestodes, and an example of a disease caused by a very large<br />
intestinal fluke, or trematode. ■ cestodes, p. 317 ■ trematodes, p. 318<br />
(c) Larvae lodge<br />
in muscle<br />
and encyst<br />
150 µm<br />
Figure 24.32 (a–c) Life cycle of<br />
Trichinella spiralis, the Cause of<br />
Trichinosis Most cases of the disease<br />
result from eating inadequately cooked<br />
pork or bear meat.<br />
Tapeworm Disease<br />
Tapeworms can exceed 10 m (more than 30 ft.) in length and<br />
have a ribbonlike appearance. Their structure is quite distinctive in<br />
that there is no digestive tract. The head end, called a scolex, is<br />
only 1 to 2 mm in diameter and is merely an attachment device to<br />
anchor the organism so that it is not eliminated by peristalsis. The<br />
neck region continuously produces segments called proglottids<br />
that become more mature the further they are from the scolex.<br />
The proglottids are little more than hermaphroditic egg factories;<br />
depending on the species, ova are discharged from an opening in<br />
the proglottid, or the proglottid separates from the rest of the<br />
worm and releases its ova by breaking apart. People become<br />
infested with tapeworms by eating inadequately cooked red meat<br />
or fish. Three important tapeworms are the beef tapeworm, the<br />
pork tapeworm, and the fish tapeworm. Beef, pork, and fish refer<br />
to the sources of human infection, not where the adult worms<br />
exist; human beings are the definitive host for all three.<br />
Symptoms<br />
Most tapeworm victims have few or no symptoms. An occasional<br />
individual will develop vomiting and abdominal pain.
Rarely, weakness, unsteadiness, mental abnormalities, tumorlike<br />
swellings, blindness, or epilepsy occur.<br />
Causative Agents<br />
The tapeworms Taenia saginata or beef tapeworm, Taenia<br />
solium or pork tapeworm, and Diphyllobothrium latum or fish<br />
tapeworm can be distinguished by the structure of their scolices,<br />
their proglottids, and their ova. Taenia saginata and T. solium<br />
each have a single intermediate host, cattle and pigs, respectively,<br />
while D. latum has two or more.<br />
Cattle ingest T. saginata ova when they feed on pasture<br />
contaminated with feces from people who carry the adult worm.<br />
The ova hatch in the cattle intestines, releasing larvae that burrow<br />
through the intestinal wall and lodge in the flesh of the animals.<br />
Here each of the parasites develops into a cysticercus, a<br />
cystic structure containing an immature<br />
scolex. When the inadequately cooked beef is<br />
eaten by a person, the cysticercus is released<br />
from the meat by digestive enzymes, matures,<br />
attaches to the intestinal wall, and soon develops<br />
into an egg-producing adult tapeworm.<br />
The life cycle for the pork tapeworm, Taenia<br />
solium, is similar except pigs rather than cattle<br />
are the intermediate host. Cysticerci in inadequately<br />
cooked meat represent the only<br />
source of adult worms in people.<br />
The intermediate hosts of D. latum are<br />
water fleas and fish, whereas the definitive<br />
host, the mature egg-producing form, occurs<br />
in humans; bears, dogs, and other animals can<br />
be definitive hosts for the same or similar<br />
tapeworms. When ova of D. latum passed<br />
with a person’s feces enter fresh water, they<br />
soon release ciliated larvae, which are<br />
devoured by water fleas (figure 24.33). The<br />
larvae lose their cilia, claw their way into the<br />
water flea’s body using tiny hooks, absorb<br />
nutrients from the flea’s blood, and increase<br />
in size. These larvae can develop further only<br />
if the water flea is eaten by a fish. In a fish’s<br />
muscle, the organism continues developing<br />
and becomes infectious for humans. Usually,<br />
however, it gets passed from one fish to<br />
another as bigger fishes eat smaller ones,<br />
before being eaten by the human host. In the<br />
human host, the flesh of the fish is digested<br />
away by stomach juices, releasing the wormlike<br />
larva. It attaches to the small intestine,<br />
rapidly matures, and begins producing ova.<br />
Pathogenesis<br />
Symptoms of tapeworm disease can arise from<br />
the presence of adult worms in the intestine.<br />
Nausea, vomiting, and abdominal pain sometimes<br />
arise because the worms partly obstruct<br />
the intestine. Also, large fish tapeworms can<br />
absorb almost 100% of vitamin B 12 from<br />
(h) Degenerating<br />
worm segments<br />
containing<br />
many eggs<br />
(g) Adult worm<br />
develops in<br />
human small<br />
intestine<br />
intestinal juices, depriving the host of this essential vitamin and<br />
causing anemia, weakness, unsteadiness, and other manifestations<br />
of nervous system malfunction.<br />
The intermediate developmental forms of tapeworms can<br />
also infect humans and cause symptoms. This occurs in the case<br />
of D. latum when infected water fleas are accidentally ingested, as<br />
might happen with drinking lake water. Infection can also result<br />
from the practice of applying raw meat or fish to open wounds in<br />
the mistaken belief that the meat will aid recovery. If larvae are<br />
present in the flesh, they penetrate the tissues via the wound.<br />
Pork tapeworms are the most dangerous of the three<br />
types, because its eggs may hatch before being discharged in the<br />
persons’s feces or ova contaminating fingers or foods can be<br />
ingested and hatch. Larvae emerging from the ova do the same<br />
as they would do in a pig. Although humans are a poor excuse<br />
Swimming larva<br />
(a) Ovum in<br />
fresh water<br />
(f) Infested fish<br />
eaten by<br />
human<br />
(d) Small fish eaten<br />
by large fish<br />
(c) Water flea eaten<br />
by small fish<br />
(b) Larva<br />
eaten by<br />
water flea<br />
Figure 24.33 (a–h) Life Cycle of the Fish Tapeworm,<br />
Diphylobothrium latum Notice that this species requires two or more<br />
intermediate hosts. Distinctive features of the ovum are its large size, oval<br />
shape, and operculum, a trapdoor through which the larva exits the<br />
ovum. Infestation is a risk for those who are fond of eating uncooked fish.<br />
20 µm<br />
Knob<br />
(e) Larvae in<br />
muscle of<br />
fish<br />
Operculum
for an intermediate host, the larvae penetrate the intestinal wall<br />
by means of tiny hooklets. Then they enter the bloodstream,<br />
from which they invade tissues throughout the body, including<br />
the eyes, brain, heart, and muscles. In the tissues they develop<br />
into cysticerci, 0.5 to 5 or more cm in diameter. The condition<br />
resulting from cysticerci in the tissues is called cysticercosis and<br />
can mimic a brain tumor or cause epilepsy (figure 24.34).<br />
Epidemiology<br />
Tapeworm disease occurs wherever people eat raw meat or fish.<br />
The beef tapeworm is the most common in the United States,<br />
reported from eight states in one survey. The fish tapeworm<br />
mainly occurs in the north central part of the United States,<br />
where formerly outhouses were constructed so as to discharge<br />
directly into the lakes. The pork tapeworm is rare in the United<br />
States, but it may occur in immigrants from parts of Mexico,<br />
India, the Philippines, and other parts of the world where eating<br />
raw pork is traditional.<br />
Prevention and Treatment<br />
Control of tapeworms depends on adequate cooking of meat<br />
until it is no longer pink in the center. Fish should also be thor-<br />
Hooklets<br />
Adult worm<br />
200 µm<br />
Scolex<br />
Proglottid<br />
Sucker<br />
Cysticerci<br />
(d) Cysticercus develops<br />
into mature tapeworm<br />
in small intestine<br />
(e) Ova and ova-filled<br />
proglottids passed<br />
in human feces<br />
oughly cooked, or if eaten raw should be deep frozen for a week<br />
before eating. Proper disposal of human feces and good<br />
hygienic habits are especially important for controlling pork<br />
tapeworm disease. Effective medicines are available both for ridding<br />
the body of adult worms and for treating cysticercosis.<br />
Giant Intestinal Fluke Disease (Fasciolopsiasis)<br />
Fasciolopsiasis, disease caused by Fasciolopsis buski, may be<br />
acquired in a number of countries of Southern Asia, including<br />
parts of China, India, Myanmar (Burma), Thailand, Laos, Cambodia,<br />
Vietnam, Malaysia, Indonesia, and the Philippines. An<br />
estimated 10 million people are infested worldwide.<br />
Symptoms<br />
Symptoms of fasciolopsiasis are diarrhea, abdominal pain, generalized<br />
weakness, and swelling of the face and other parts of the<br />
body.<br />
Causative Agent<br />
Fasciolopsis buski, also known as the giant intestinal fluke, can be as<br />
large as 7.5 cm long and 2.0 cm wide. This hermaphroditic<br />
helminth lives in the upper and middle small intestine; attachment<br />
(c) Inadequately cooked<br />
pork containing<br />
cysticerci ingested<br />
by human<br />
Figure 24.34 (a–e) Life Cycle of the Pork Tapeworm, Taenia solium, Acquired by Eating<br />
Inadequately Cooked Pork If worm ova hatch in the intestine, larval forms called cysticerci can develop throughout<br />
the person’s tissues. A cysticercus in the brain can cause epilepsy.<br />
(f) Ova ingested<br />
by human leads<br />
to cysticercosis<br />
(b) Cysticercus develops<br />
in flesh of pig<br />
(a) Pig ingests embryonated<br />
ovum from human feces
and movement is aided by two suckers. Unlike tapeworms, flukes<br />
like F. buski have a digestive system. Ova are passed in the feces of<br />
the definitive hosts, humans and pigs, and the enclosed embryos<br />
mature in warm fresh water in about 6 weeks (figure 24.35). The<br />
ova then hatch, releasing ciliated larvae, which penetrate the flesh<br />
of certain snail species that serve as intermediate hosts. In the snail,<br />
the organisms develop and multiply asexually, eventually exiting<br />
the snail in the form of motile long-tailed larvae called cercariae.<br />
These cercariae attach to the outer covering of water plants such<br />
as water chestnuts, where they form cysts infectious for pigs and<br />
human beings. People generally become infected when they peel<br />
off the outer portion of water plants with their teeth in order to<br />
eat the edible inner portion of the plant. The worms exit from<br />
their cysts in the duodenum, attach, and after several months<br />
begin producing ova.<br />
Pathogenesis<br />
Inflammation occurs at the site of attachment of the helminths,<br />
followed by ulceration and bleeding. Heavy infestations can interfere<br />
with nutrition or even obstruct the intestinal tract. Severe<br />
symptoms also arise from toxicity and allergy to substances<br />
released by the worms and absorbed by the host’s circulation.<br />
(e) Asexual multiplication<br />
and differentiation into<br />
cercariae occur over a<br />
number of weeks<br />
(g) Cercariae attach to<br />
water plant and encyst<br />
(f) Cercariae exit<br />
the snail<br />
(d) Miracidium<br />
burrows into<br />
flesh of snail<br />
(c) Miracidium<br />
emerges after<br />
3 to 6 weeks<br />
Epidemiology<br />
Fasciolopsiasis occurs in warm climates where people raise pigs<br />
and eat raw freshwater plants, and where a suitable snail intermediate<br />
host exists. Feces from infested humans or pigs must<br />
reach the ponds inhabited by the snails and edible water plants.<br />
Each adult worm produces more than 20,000 ova per day and<br />
lives about 1 year.<br />
Prevention and Treatment<br />
Fasciolopsiasis can be prevented by killing encysted F. buski on<br />
water plants by dipping them in boiling water for a few seconds<br />
before peeling and eating. Rinsing the edible portion thoroughly<br />
in clean water after peeling is probably also effective.<br />
The disease is effectively treated with praziquantel. Table 24.17<br />
compares some features of these parasitic helminths.<br />
MICROCHECK<br />
Tapeworms are ribbonlike creatures, consisting largely<br />
of a string of hermaphroditic egg-producing segments.<br />
The pork tapeworm, Taenia solium, is the most<br />
dangerous because its ova can hatch in the human<br />
intestine, the larvae entering brain and other tissues,<br />
(h) Cyst is ingested by human or pig;<br />
larva excysts in the duodenum<br />
and becomes adult worm<br />
Oral sucker<br />
Ventral sucker<br />
Figure 24.35 (a–h) Life Cycle of the “Giant Intestinal Fluke,” Fasciolopsis buski The infectious larva of<br />
this worm encysts on certain edible water plants, including a kind of water chesnut. People become infested when they<br />
peel the edible portion with their teeth.<br />
(a) Adult worm<br />
in duodenum<br />
(b) Ova in feces reach<br />
warm fresh water,<br />
embryo develops
TABLE 24.17 Notable Helminthic Diseases of Human Beings<br />
Disease and Causative Agent How Acquired Disease Characteristics Prevention and Control<br />
Enterobiasis (pinworm), Hand to mouth; inhalation Itching of anal region, restless- Handwashing, daily change of<br />
Enterobius vermicularis ness, nervousness, irritability,<br />
poor sleep<br />
underclothing and bed sheets<br />
Trichuriasis, (whipworm) Ingestion of eggs of parasite Abdominal pain, bloody stools, Sanitary disposal of human<br />
Trichuris trichiura along with contaminated food<br />
or water<br />
diarrhea, and weight loss feces; frequent handwashing<br />
Ascariasis, Ascaris lumbricoides Ingestion of eggs of parasite or Abdominal pain, live worms Sanitary disposal of human<br />
water along with contaminated food vomited or passed in stool feces<br />
Hookworm disease, Larvae penetrate bare feet Anemia, weakness, fatigue, Sanitary disposal of human<br />
Necator americanus and physical and mental retardation feces; wearing shoes<br />
Ancylostoma duodenale in children<br />
Strongyloidiasis, Larvae penetrate bare feet Skin rash at site of penetration, Sanitary disposal of human<br />
Strongyloides stercoralis cough, abdominal pains, weight<br />
loss<br />
feces; wearing shoes<br />
Trichinosis, Trichinella spiralis Eating raw or undercooked Fever, swelling of upper eyelids, Adequate cooking of meat<br />
meat, usually pork muscle soreness<br />
Tapeworm disease, Eating raw or undercooked Abdominal pain, anemia, Thorough cooking or deep<br />
Taenia solium, T. saginata,<br />
Diphyllobothrium latum<br />
meat or fish cysticercosis freezing of meat and fish<br />
Fasciolopsiasis, Eating raw water plants with Diarrhea, abdominal pain, Brief treatment of plants in<br />
Fasciolopsis buski encysted larvae weakness, body swelling boiling water<br />
resulting in cysticercosis. Tapeworm disease is usually<br />
acquired by eating inadequately cooked beef, pork, or<br />
fish. Fasciolopsiasis is caused by the giant intestinal<br />
fluke, a relatively short, nonsegmented hermaphoditic<br />
flatworm usually acquired when a person uses their<br />
teeth to peel certain edible aquatic plants having<br />
encysted fluke larvae on their surface.<br />
■ Describe the anatomy of a tapeworm.<br />
■ How might you explain the development of epilepsy in<br />
a Mexican man fond of eating traditional dishes made<br />
from raw pork?<br />
F U T U R E C H A L L E N G E S<br />
Defeating Diarrhea<br />
Development of better preventive and treatment techniques<br />
for alimentary tract diseases has an urgency<br />
arising from massive food and beverage production<br />
and distribution methods. For example, in 1994, an<br />
estimated 224,000 people became ill because a tanker truck used to<br />
transport ice cream mix had previously carried liquid eggs. One<br />
day’s production from a ground beef factory can yield hundreds of<br />
thousands of pounds of hamburgers, which are soon sent to many<br />
parts of this or other countries. The challenge is to better educate<br />
the producers and transporters, to develop guidelines to help them<br />
avoid contamination, and to utilize newly approved methods such<br />
as meat irradiation.<br />
Other challenges include the following:<br />
■ Exploit the power of molecular biology techniques to<br />
produce effective vaccines against rotavirus, hepatitis C<br />
virus, and bacterial pathogens. There is special need for<br />
bacterial vaccines that can be administered by mouth and<br />
evoke long-lasting mucosal immunity.<br />
■ Find better ways of preventing and reversing resistance to<br />
antibacterial medications. In the early 1980s, 0.6% of<br />
Salmonella Typhimurium isolates were resistant to<br />
ampicillin, chloramphenicol, tetracycline, streptomycin,<br />
and sulfa drugs. Now, in some areas, over 30% of isolates<br />
of this common salmonellosis cause are resistant to all<br />
these medications.<br />
■ Explore further the influence of global warming on<br />
alimentary tract diseases. A study of Peruvian children by<br />
Johns Hopkins University scientists found an 8% increase<br />
in clinic visits for diarrhea with each 1°C increase in<br />
temperature from the normal.<br />
■ Explore new prevention and treatment options. Scientists<br />
at the University of Florida have developed a genetically<br />
engineered Streptococcus mutans that does not produce<br />
lactic acid but readily displaces wild strains of the dental<br />
decay causing bacterium. Researchers at the University of<br />
Alberta have custom-designed a molecule that binds<br />
circulating Shiga toxin, potentially preventing hemolytic<br />
uremic syndrome. Others work on finding an effective<br />
therapy for cryptosporidiosis.
STD Caused by<br />
<strong>Multicellular</strong> <strong>Parasites</strong><br />
Two common STDs are caused by lice or mites, multicellular<br />
skin parasites that are distributed worldwide and infect only<br />
human beings. Nonsexual transmission can sometimes occur in<br />
both instances. Besides the discomfort they cause, their chief<br />
importance is to raise the possibility that other, unrecognized,<br />
STDs might be present. Fortunately, neither of these parasites<br />
are vectors of microbial diseases.<br />
“Crabs” (Pubic Lice, Pediculosis Pubis)<br />
Pediculosis pubis results from infestation by a species of louse.<br />
Lice are wingless insects dependent for nutrition on sucking<br />
blood from their host.<br />
Symptoms<br />
The principal symptoms are itching in the pubic area, and psychological<br />
stress from seeing the tiny lice and their eggs, called<br />
nits, both visible to the unaided eyes. Sometimes, tiny spots of
lood are seen on the underclothing. In heavy infestations,<br />
these lice may cling to hair of parts of the body other than the<br />
pubic area, sometimes even the eyebrows and eyelashes.<br />
Causative Agent<br />
Pediculosis pubis is caused by Phthirus pubis, a slow-moving<br />
insect resembling a microscopic crab (figure 25.22). The adult<br />
form is approximately 2 mm in diameter; smaller juvenile forms<br />
feed along with the adults. The females lay about six eggs daily,<br />
attached tightly to body hairs. Hatching occurs in about 1 week,<br />
and after several developmental stages, adulthood is reached in<br />
about 2 weeks. Their life span is approximately 1 month.<br />
Pathogenesis<br />
Crab lice have piercing mouthparts with which they penetrate<br />
the skin to obtain a blood meal. They usually feed for several<br />
hours twice daily, leaving a tiny puncture site that can ooze a little<br />
blood. Symptoms are due to an allergic reaction to the feeding<br />
lice, and they do not appear for about a week after the<br />
infestation begins. If the host becomes reinfested at a later date,<br />
symptoms begin almost immediately. The intense itching leads<br />
to scratching, which can in turn lead to secondary bacterial<br />
infection.<br />
Epidemiology<br />
Phthirus pubis is slow moving and prefers to cling to the host’s<br />
hair using its clawlike hooks. Since it can live only about 24 hours<br />
away from a human host, transmission generally occurs during<br />
close physical contact, mainly but not exclusively during sexual<br />
intercourse. Fomites such as a towel or a theater seat can occasionally<br />
transmit the organisms.<br />
Prevention and Treatment<br />
Condoms do not prevent transmission. Several insecticides are<br />
approved for treating pediculosis pubis, but they must be used<br />
exactly as directed to avoid possible serious toxicity. Bedding<br />
1 mm<br />
Figure 25.22 Crab Louse, Phthirus pubis, is Usually Sexually<br />
Transmitted It is not known to be a vector of infectious agents.<br />
and clothing is washed in hot water, dry cleaned, or kept from<br />
human contact for 3 days. Any sexual partners over the prior<br />
month are examined and treated if needed. All are reexamined<br />
after 1 week and retreated if necessary.<br />
“Seven-Year Itch” (Scabies)<br />
Scabies, also known as the “seven-year itch,” results from infestation<br />
with a mite, a tiny member of the arachnids, the class of<br />
eight-legged creatures that includes spiders and scorpions. Other<br />
mites, such as the house mouse mite, can transmit microbial diseases,<br />
and the dust mite causes allergic asthma. The scabies mite<br />
is restricted to human beings, and it does not transmit microbial<br />
diseases. Scabies occurs worldwide predominantly associated<br />
with poverty and crowding, but anyone can contract the disease.<br />
Symptoms<br />
As with pediculosis pubis, the dominant symptom of scabies is<br />
intense itching. Besides the pubic area, the space between the<br />
fingers, the wrists, and the area under the breasts are often<br />
involved. Rarely, the entire body below the neck is infested,<br />
causing a scaly rash.<br />
Causative Agent<br />
The causative agent of scabies is Sarcoptes scabiei. The adult<br />
female (figure 25.23a) is only 330 to 450 µm long; the male is<br />
smaller. The organisms live on the surface of the human skin.<br />
The females make burrows into the outer layers of epidermis<br />
(figure 25.23b), forming tunnels where they lay several eggs<br />
daily over a life span of 1 to 2 months. The tunnels are visible<br />
to the unaided eyes as short, dark-colored wavy lines, sometimes<br />
with a vesicle overlying the end containing the mite. The mites<br />
can be scraped from the tunnels with a scalpel and identified<br />
microscopically, the only way accurately to diagnose scabies. Sixlegged<br />
larvae hatch from the eggs and mature on the skin surface<br />
to the eight-legged form in about 2 weeks.<br />
Pathogenesis<br />
Usually it takes 2 to 6 weeks after contracting scabies for symptoms<br />
to appear. If following a cure scabies is contracted again,<br />
however, symptoms appear in 1 to 4 days. Thus as with pediculosis<br />
pubis, the host’s allergic response to the mites and their<br />
feces is largely responsible for symptoms of the disease. In the<br />
usual individual with scabies, the number of mites is less than<br />
100 and the disease goes away by itself in a matter of months.<br />
In individuals with AIDS and other immunodeficiencies, however,<br />
millions of the organisms can be present, spreading over<br />
much of the body and causing a severe rash with thickening and<br />
peeling of the skin. Opportunistic bacterial pathogens, introduced<br />
by scratching, are a serious threat to patients with scabies.<br />
Epidemiology<br />
Scabies is usually transmitted by close contact with a person who<br />
has the disease. In adults, transmission often occurs as a result<br />
of sexual contact; in children, this is rarely so. Adults with the<br />
disease should be checked for other possible STDs. Nonsexual<br />
transmission of scabies occurs readily among children, especially<br />
those less than five years old.
(a)<br />
TABLE 25.17 Pediculosis Pubis and Scabies<br />
0.25 mm<br />
Prevention and Treatment<br />
Scabies is prevented by avoiding contact with those who have<br />
scabies, their bedding, and their clothing. Sexual and other close<br />
contacts within the month prior to diagnosis need to be examined<br />
and treated. Bedding and clothing is washed in hot water,<br />
dry cleaned, or removed from human contact for 3 days. Insecticides<br />
suitable for use on the skin are effective against S. scabiei,<br />
as is a sulfur-containing ointment, and ivermectin, an antiparasitic<br />
medication that paralyzes the organism. These medications<br />
must be used exactly as prescribed in order to minimize the risk<br />
of serious side effects.<br />
The main characteristics of pediculosis pubis and scabies<br />
are presented in table 25.17.<br />
MICROCHECK<br />
The main importance of pubic lice and scabies is to<br />
raise the possibility of other sexually transmitted<br />
diseases. The possibility of secondary infection<br />
Skin surface<br />
Epidermis<br />
Figure 25.23 Seven-Year Itch Mite, Sarcoptes scabiei, Commonly Sexually Transmitted<br />
(a) Microscopic appearance in scrapings of a scabies burrow. (b)The female mite burrows into the outer layer of skin to<br />
lay her eggs, causing an intensely itchy rash. Sarcoptes scabiei is not known to be a vector of infectious diseases.<br />
introduced by scratching the involved area is another<br />
important consideration.<br />
■ Explain why it takes 2 to 6 weeks for symptoms to<br />
appear after first contracting scabies, but only a few<br />
days after contracting the disease again.<br />
■ What further testing should be considered once pubic<br />
lice or scabies is diagnosed in an adult?<br />
■ What evidence can you present that the immune system<br />
plays a role in controlling scabies?<br />
■ Why will condoms not prevent the spread of crab lice?<br />
F U T U R E C H A L L E N G E S<br />
Getting Control of Sexually Transmitted Diseases<br />
Few problems are as complicated as getting control of sexually<br />
transmitted diseases because of the psychological,<br />
cultural, religious, and economic factors that are<br />
involved, which vary from one population to another.<br />
Pediculosis Pubis (“Crabs”) Scabies (“Seven-Year Itch”)<br />
Symptoms Intense itching, visible lice and eggs Intense itching<br />
Incubation period Usually about 1 week Usually about 1 month (2 to 6 weeks)<br />
Causative agent Phthirus pubis, a louse Sarcoptes scabiei, a mite<br />
Pathogenesis Skin penetration by a blood-sucking insect; Burrowing into the epidermis by an arachnid;<br />
allergic reaction to it allergic reaction to it<br />
Epidemiology Transmitted by sexual intercourse and other<br />
close physical contact; sometimes by fomites<br />
Same as for pediculosis pubis<br />
Prevention and treatment Avoidance of persons with the disease, their Same as for pediculosis pubis.<br />
clothing and bedding; treatment of contacts; Additional treatment options include ivermectin<br />
insecticide medications applied to the skin and a sulfur ointment<br />
(b)
<strong>Multicellular</strong> <strong>Parasites</strong><br />
A number of species of roundworms can infect the blood and<br />
lymphatic vessels of humans. Mostly, they are contracted in<br />
tropical countries, transmitted by biting insects. The adult<br />
female worms live in the lymphatic vessels and deposit their offspring,<br />
tiny microfilaria, directly into the skin, lymphatics, or<br />
bloodstream, where they can be identified in biopsies or blood<br />
smears to make the diagnosis. The disorder these roundworms<br />
produce is termed filariasis, and it may be asymptomatic or<br />
produce dramatic symptoms. Two examples are elephantiasis,<br />
marked swelling of a body part due to lymphatic obstruction,<br />
caused by Wuchereria bancrofti and Brugia sp., and river blindness,<br />
caused by Onchocerca volvulus.<br />
Completely different kinds of parasitic worms live in the<br />
blood vessels that carry venous blood from the intestines to the<br />
liver, or in the veins of the bladder. They are responsible for the<br />
disease schistosomiasis.<br />
Schistosomiasis<br />
Schistosomiasis, endemic in countries of Africa, Asia, the<br />
Caribbean, and South America, involves more than 200 million<br />
people worldwide and causes over 500,000 deaths annually.<br />
About 400,000 individuals with the disease now live in the<br />
United States, having emigrated from places where schistosomiasis<br />
is endemic. Schistosomiasis is caused not by roundworms,<br />
but by flukes. Flukes are short, bilaterally symmetrical worms<br />
that usually attach by one or more sucking discs.<br />
Symptoms<br />
Itching skin may occur at the time of exposure to fresh water containing<br />
the worm larvae. The itching subsides, and weeks later, a
generalized acute illness occurs, with fever, hives, cough, abdominal,<br />
joint and muscle pain, and diarrhea. Some people die during<br />
this stage, but usually the symptoms subside and infected individuals<br />
are free of symptoms for a number of years. Then a chronic,<br />
slowly progressing illness appears, with weakness, accumulation of<br />
fluid in the abdominal cavity, and sometimes vomiting blood.<br />
Causative Agent<br />
Most cases of schistosomiasis are caused by three species of<br />
flukes in the genus Schistosoma. Other genera of flukes that<br />
infect humans are hermaphroditic, meaning that each worm has<br />
both male and female reproductive organs, but Schistosoma<br />
species have male and female worms. Schisto-soma means “splitbody,”<br />
referring to a deep groove running along the male’s<br />
body in which he clasps his female partner. Schistosoma mansoni,<br />
the only species established in the Americas, and the most common<br />
cause of schistosomiasis worldwide, is 10 to 20 mm long<br />
Figure 28.13 Life Cycle of<br />
Schistosoma mansoni (a) Eggs (ova)<br />
from feces reach fresh water. (b) First larval<br />
form (miracidium) hatches from ovum and<br />
(c) infects snail. (d) Asexual reproduction in<br />
body of snail and transformation into<br />
another larval form (cercaria). (e) Cercariae<br />
break out of snail and penetrate human<br />
skin.Tail left behind, larva enters capillary, is<br />
carried by bloodstream to intestinal veins,<br />
and develops into mature fluke. (f) Ova<br />
deposited, break into the intestine or are<br />
swept to the liver by the blood.<br />
(f) Ova that fail<br />
to rupture<br />
into the<br />
intestine<br />
are swept<br />
to the<br />
liver,<br />
cause<br />
scarring<br />
Blood vessel<br />
(e) Larvae from<br />
skin capillaries<br />
mature in<br />
intestinal vein and<br />
produce ova<br />
Eggs<br />
and lives in the small veins of the human intestine. Because it<br />
lives in blood vessels, it is called a blood fluke. The life cycle of<br />
S. mansoni is shown in figure 28.13. The slender female worm<br />
deposits ova that rupture through the tiny intestinal veins and<br />
wall of the intestine to enter the lumen, ultimately to be eliminated<br />
with the feces. The ova hatch in fresh water, releasing ciliated<br />
larvae called miracidia which can live up to 6 hours. When<br />
a miracidium encounters a certain species of snail, it penetrates<br />
the snail’s body and multiplies asexually. Over about 6 weeks,<br />
thousands of elongated fork-tailed larvae called cercariae<br />
develop and leave their snail intermediate host to enter the<br />
water. When they encounter a human being wading in the<br />
water, they burrow through his or her skin, leaving their tails<br />
behind them. These larvae proceed to enter the circulatory system,<br />
are carried by the bloodstream through the heart and<br />
lungs, and eventually reach veins of the intestine, where they<br />
mature, mate, and begin ova production.<br />
(a) Ovum<br />
(d) Cercaria<br />
from snail<br />
penetrates<br />
skin<br />
(c) Snail<br />
(b) Miracidium
Pathogenesis<br />
Many of the cercariae die upon entering the skin, causing an<br />
inflammatory and immune response that becomes more and<br />
more intense with each exposure to the parasites. Each skin penetration<br />
by the schistosomes causes an itchy skin rash that gradually<br />
subsides. Weeks later, when the mature worms begin to<br />
deposit their ova, a generalized illness occurs, probably due to<br />
circulating schistosomal antigens reacting with antibodies.<br />
Although some people die from the reaction, usually it subsides<br />
within several months. Unfortunately, the worms continue to<br />
deposit hundreds of ova per day over a lifetime that can exceed<br />
a quarter century. Perpetuation of the species depends on ova<br />
staying close to the intestine, where an intense inflammatory<br />
response liquefies the tissue and allows them to rupture into the<br />
intestinal lumen. The spine on the ovum probably helps hold<br />
them in place, but many are swept away by the bloodstream to<br />
the liver. The same inflammatory response to the ova occurs in<br />
the liver, causing gradual destruction of liver cells and their<br />
replacement with scar tissue. The end result is malnutrition and<br />
a buildup of pressure in the abdominal veins and connecting<br />
veins in the esophagus. Fluid accumulates in the abdominal cavity<br />
(figure 28.14), and hemorrhage occurs if the engorged<br />
esophageal veins rupture.<br />
Swimmer’s itch is a schistosomal disease that is common<br />
across the United States. The disease is characterized by an itchy<br />
rash caused by cercariae of schistosomes of wild birds and other<br />
animals. The cercariae penetrate the skin of swimmers and then<br />
die. These schistosomes are otherwise harmless, since they are<br />
unable to complete their life cycle in humans.<br />
Epidemiology<br />
Transmission occurs in northern and eastern South America,<br />
parts of the Caribbean, much of the African continent, parts of<br />
the Middle and Far East, Philippines, Southeast Asia, China,<br />
and Japan. The distribution depends on abundant fresh water,<br />
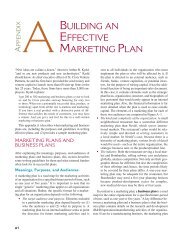
Figure 28.14 Child with Schistosomiasis Notice the distended abdomen,<br />
probably due to inflammatory enlargement of the liver and spleen. Later in the<br />
development of the disease the abdomen will fill with fluid, the result of scarring that<br />
obstructs the flow of blood throught the liver.<br />
extensive contamination of water by human feces, and a suitable<br />
snail intermediate host. Farmers and people who fish or<br />
wade in fresh water are at high risk for the disease. Large irrigation<br />
projects to enhance agriculture have extended the<br />
range of the disease. Schistosomiasis cannot be contracted in<br />
continental United States because there is no appropriate snail<br />
intermediate host.<br />
Prevention and Treatment<br />
Preventing schistosomiasis depends on avoiding skin exposure<br />
to fresh water contaminated with the miracidia, preventing<br />
untreated human feces from entering fresh water, treatment of<br />
cases of the disease, and measures, both chemical and biological,<br />
to control the snail intermediate hosts. Promising synthetic<br />
peptide and DNA vaccines are under development. Effective<br />
medications are available that kill the parasites in disease victims.<br />
The main features of schistosomiasis are presented in<br />
table 28.9.<br />
TABLE 28.9 Schistosomiasis<br />
Symptoms Acutely: fever, hives, cough, abdominal, joint, and<br />
muscle pain.These symptoms subside and after years<br />
are replaced by generalized weakness and swelling<br />
of the abdomen<br />
Incubation period Usually 2 to 6 weeks<br />
Causative agents Most cases are caused by three species of Schistosoma,<br />
the most prevalent being S. mansoni.The male<br />
schistosome has a longitudinal slit in its body in which<br />
he clasps the female. Perpetuation of the life cycle<br />
depends on rupture of their eggs into the lumen of the<br />
intestine from the tiny intestinal veins where the<br />
adults live.The eggs hatch in fresh water, releasing a<br />
free-swimming miracidium that penetrates into the<br />
flesh of the snail intermediate host. In the snail, the<br />
organism multiplies and differentiates into forked-tail<br />
cercariae that leave the snail and can infect humans<br />
by penetrating their skin<br />
Pathogenesis Inflammatory and immune response to skin<br />
penetration by the cercariae causes intense itching.<br />
Allergic reaction to released schistosomal antigens as<br />
the worms mature and begin depositing ova causes<br />
the acute illness. Chronic malnutrition and swelling of<br />
the abdomen result from liver damage caused by<br />
ova that fail to penetrate into the intestinal lumen,<br />
and are carried to the liver by the bloodstream<br />
Epidemiology Distribution of the disease is favored by large<br />
bodies of shallow fresh water, extensive contamination<br />
of the water with human feces, and a suitable snail<br />
intermediate host. Farmers, people who fish, and<br />
children who wade in fresh water at high risk<br />
Prevention and Prevention depends on proper disposal of human<br />
treatment feces, identifying and treating infected patients, and<br />
measures to control the snail intermediate host.<br />
Praziquantel is effective treatment
MICROCHECK<br />
The health and economic burden of multicellular<br />
parasite infections challenges that of malaria. The<br />
complex life cycle of Schistosoma mansoni provides a<br />
number of possibilities for attacking schistosomiasis.<br />
■ Trace the life cycle of Schistosoma mansoni.<br />
■ How long would it take S. mansoni to become extinct<br />
if snail-eating fish eliminated the intermediate host?