2010 RWISO Journal - Roth Williams International Society of ...
2010 RWISO Journal - Roth Williams International Society of ...
2010 RWISO Journal - Roth Williams International Society of ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
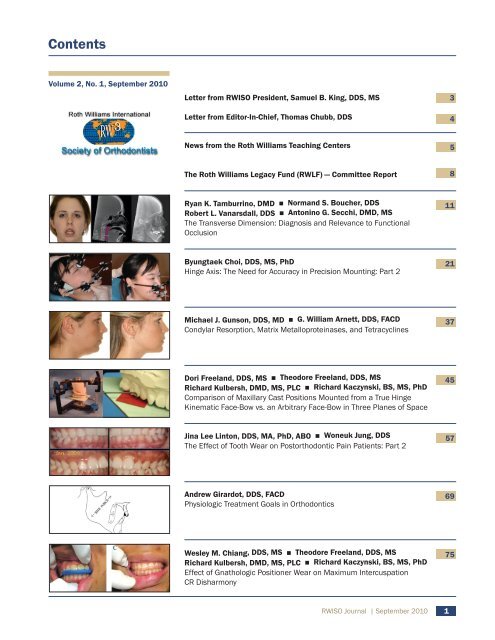
Contents<br />
Volume 2, No. 1, September <strong>2010</strong><br />
Letter from <strong>RWISO</strong> President, Samuel B. King, DDS, MS<br />
Letter from Editor-In-Chief, Thomas Chubb, DDS<br />
News from the <strong>Roth</strong> <strong>Williams</strong> Teaching Centers<br />
The <strong>Roth</strong> <strong>Williams</strong> Legacy Fund (RWLF) — Committee Report<br />
Ryan K. Tamburrino, DMD ■ Normand S. Boucher, DDS<br />
Robert L. Vanarsdall, DDS ■ Antonino G. Secchi, DMD, MS<br />
The Transverse Dimension: Diagnosis and Relevance to Functional<br />
Occlusion<br />
Byungtaek Choi, DDS, MS, PhD<br />
Hinge Axis: The Need for Accuracy in Precision Mounting: Part 2<br />
Michael J. Gunson, DDS, MD ■ G. William Arnett, DDS, FACD<br />
Condylar Resorption, Matrix Metalloproteinases, and Tetracyclines<br />
Dori Freeland, DDS, MS ■ Theodore Freeland, DDS, MS<br />
Richard Kulbersh, DMD, MS, PLC ■ Richard Kaczynski, BS, MS, PhD<br />
Comparison <strong>of</strong> Maxillary Cast Positions Mounted from a True Hinge<br />
Kinematic Face-Bow vs. an Arbitrary Face-Bow in Three Planes <strong>of</strong> Space<br />
Jina Lee Linton, DDS, MA, PhD, ABO ■ Woneuk Jung, DDS<br />
The Effect <strong>of</strong> Tooth Wear on Postorthodontic Pain Patients: Part 2<br />
Andrew Girardot, DDS, FACD<br />
Physiologic Treatment Goals in Orthodontics<br />
Wesley M. Chiang, DDS, MS ■ Theodore Freeland, DDS, MS<br />
Richard Kulbersh, DMD, MS, PLC ■ Richard Kaczynski, BS, MS, PhD<br />
Effect <strong>of</strong> Gnathologic Positioner Wear on Maximum Intercuspation<br />
CR Disharmony<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
1<br />
3<br />
4<br />
5<br />
8<br />
11<br />
21<br />
37<br />
45<br />
57<br />
69<br />
75
<strong>RWISO</strong> JOURNAL<br />
SEPTEMBER <strong>2010</strong> VOL. 2, NO. 1<br />
EDITOR IN CHIEF<br />
Dr. Thomas K. Chubb<br />
EXECUTIVE DIRECTOR/ADVERTISING SALES<br />
Jeff Milde<br />
MANAGING EDITOR<br />
Anne Evers<br />
CREATIVE DIRECTORS<br />
Brad Reynolds (www.integralartandstudies.com)<br />
BOARD OF DIRECTORS<br />
President<br />
Dr. Sam King<br />
6460 Far Hills Avenue<br />
Centerville, OH 45459 USA<br />
937-433-9530<br />
samuel_king@hotmail.com<br />
President Elect<br />
Dr. Douglas Knight, DMD<br />
3210 Westport Green Place<br />
Louisville, KY 40241 USA<br />
502-327-6453<br />
knightortho@insightbb.com<br />
Vice President<br />
Dr. Renato Cocconi<br />
Via Traversante, San Leonardo 1<br />
43100 Parma, Italy<br />
+0521-273682<br />
orthosmile@studiococconi.it<br />
Secretary<br />
Dr. Eunah Choi<br />
Somang BD 2F, 907-1<br />
Bangbae 1 Dong<br />
Seocho Gu<br />
Seoul, 137-842 Korea<br />
+822-583-2275<br />
orthoi@hanmail.net<br />
Treasurer<br />
Dr. John F. Lawson, MS<br />
2460 Nwy 63 North<br />
Rochester, MN 55906 USA<br />
507-282-6447<br />
jlawdds@aol.com<br />
2<br />
Immediate Past President<br />
Dr. Darrell Havener<br />
1420 West Canal Court,<br />
Suite 200<br />
Littleton, CO 80120 USA<br />
303-791-2021<br />
dhavener@gmail.com<br />
Executive Director<br />
Jeff Milde<br />
1712 Devonshire Road<br />
Sacramento, CA 95864 USA<br />
916-270-2013<br />
j.milde@mra-sf.com<br />
COUNCIL MEMBERS<br />
Region I - Asia<br />
Dr. Satoshi Adachi<br />
#202, 5-11-8 Minoh<br />
Minoh, Osaka 562-0001 Japan<br />
+81-72-724-2866<br />
teeth@adachi-ortho.com<br />
Dr. Eunah Choi<br />
Somang BD 2F, 907-1<br />
Bangbae 1 Dong<br />
Seocho Gu<br />
Seoul, 137-842 Korea<br />
+822-583-2275<br />
orthoi@hanmail.net<br />
<strong>RWISO</strong> <strong>Journal</strong> is published by the <strong>Roth</strong> <strong>Williams</strong> <strong>International</strong> <strong>Society</strong><br />
<strong>of</strong> Orthodontists.<br />
Copyright © <strong>2010</strong> <strong>RWISO</strong>. All Rights Reserved.<br />
ISSN 2154-4395 (print)<br />
ISSN 2154-4409 (online)<br />
Reproduction whole or in part in any form or medium without express<br />
written permission <strong>of</strong> <strong>RWISO</strong> is prohibited. Information furnished in<br />
this journal is believed to be accurate and reliable; however, no responsibility<br />
is assumed for inaccuracies or for the information’s use.<br />
Postmaster:<br />
Send address changes to<br />
<strong>RWISO</strong><br />
1712 Devonshire Road<br />
Sacramento, CA 95864<br />
<strong>RWISO</strong> <strong>Journal</strong><br />
<strong>Roth</strong> <strong>Williams</strong> <strong>International</strong> <strong>Society</strong> <strong>of</strong> Orthodontists<br />
1712 Devonshire Road<br />
Sacramento, CA 95864 USA<br />
Phone: 916-270-2013<br />
Fax: 866-746-3815<br />
info@rwiso.org<br />
We welcome your responses to this publication. Please send comments,<br />
subscriptions, advertising and submission requests to: info@rwiso.org<br />
The <strong>Roth</strong> <strong>Williams</strong> <strong>International</strong> <strong>Society</strong> <strong>of</strong> Orthodontics is the embodiment<br />
<strong>of</strong> a philosophical and technological transformation: addition <strong>of</strong><br />
physiologic to anatomics from a foundation <strong>of</strong> function and esthetics.<br />
Region II - Europe<br />
Dr. Claudia Aichinger<br />
Billrothstr. 58<br />
Vienna, A-1190 Austria<br />
+43-1-367-7222<br />
smile@draichinger.at<br />
Dr. Renato Cocconi<br />
Via Traversante, San Leonardo 1<br />
43100 Parma, Italy<br />
+0521-273682<br />
orthosmile@studiococconi.it<br />
Dr. Domingo Martin<br />
Plaza Bilbao 2-2A<br />
San Sebastian, 20005 Spain<br />
+34-943-427-814<br />
martingoenaga@arrakis.es<br />
Region III - USA, Canada<br />
Dr. Ramon Marti, MSC<br />
281 Oxford Street E.<br />
London, Ontario N6A 1V3<br />
Canada<br />
519-672-7740<br />
rmarti3@hotmail.com<br />
Region IV - South America<br />
Dra. Solange M. deFantini, MSD<br />
Al Janu 176 cj 42<br />
Sao Paulo, SP 01420-002 Brazil<br />
+55-11-3081-8440<br />
smfantin@usp.br<br />
Dra. Marisa Gianesella Bertolaccini<br />
Rua Tabapuã, 649 - Conj. 83<br />
Itaim Bibi, São Paulo, SP, 04533-<br />
012 Brazil<br />
+11- 505-25417<br />
mgianesella.odonto@gmail.com
Letter from the President<br />
Samuel B. King, DDS, MS<br />
<strong>RWISO</strong> President<br />
The world is changing rapidly. Technology is enabling us to do things never<br />
before possible. Orthodontics is changing too. New technologies, evolution<br />
<strong>of</strong> procedures, ease in obtaining information are just a few <strong>of</strong> the things that<br />
are advancing the orthodontic pr<strong>of</strong>ession. The <strong>Roth</strong> <strong>Williams</strong> <strong>International</strong><br />
<strong>Society</strong> <strong>of</strong> Orthodontists continues to evolve to provide the very best for our<br />
patients, but as we move forward with these new technologies, we are ever<br />
mindful <strong>of</strong> our treatment goals and the standards <strong>of</strong> our philosophy.<br />
The <strong>RWISO</strong> <strong>Journal</strong> embodies our commitment to remain true to our treatment<br />
goals and the standards <strong>of</strong> our philosophy. As orthodontic treatment<br />
changes, it is our duty to ensure, through evidence-based research, that new<br />
techniques and modalities achieve our goals and maintain our standards. Our<br />
<strong>Journal</strong> serves to educate our global organization about these advancements<br />
so that our members can confidently deliver the <strong>Roth</strong> <strong>Williams</strong> goals and<br />
standards to their patients.<br />
The <strong>Roth</strong> <strong>Williams</strong> <strong>International</strong> <strong>Society</strong> <strong>of</strong> Orthodontists is in the midst <strong>of</strong><br />
an exciting time. Today we are able to treat our patients better than ever before<br />
with exciting new advancements in our pr<strong>of</strong>ession. It is truly a great time<br />
to be part <strong>of</strong> the <strong>Roth</strong> <strong>Williams</strong> <strong>International</strong> <strong>Society</strong> <strong>of</strong> Orthodontists.<br />
Respectfully,<br />
Samuel B. King, DDS, MS<br />
<strong>RWISO</strong> President<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
3
Letter from the Editor<br />
Thomas Chubb, DDS<br />
Editor-In-Chief <strong>of</strong> <strong>RWISO</strong> <strong>Journal</strong><br />
4<br />
Dr. Thomas Chubb | Letter from the Editor<br />
I would first like to thank all the authors in this year’s <strong>Journal</strong> for the amount <strong>of</strong> time<br />
and energy they devoted to giving us another first class issue. They are the lifeblood <strong>of</strong><br />
the <strong>RWISO</strong> <strong>Journal</strong>. I know the authors would be interested in your feedback. Their<br />
e-mail addresses are listed on their articles, so please contact them with any comments<br />
you might have. I apologize to any author whose submission did not make it into this<br />
issue. We are already working on the next issue, which we hope will come out between<br />
now and the next meeting.<br />
I would like to thank Anne Evers, our managing editor, and Irene Elmer, our copy<br />
editor, for all their hard work and pr<strong>of</strong>essionalism. Many <strong>of</strong> the authors have felt the<br />
sting <strong>of</strong> Irene’s sharp pen and the exacting revisions they both required. Their many<br />
hours <strong>of</strong> hard work were needed to bring this issue to fruition. I would also like to<br />
thank all our sponsors who contributed generously to help publish this issue and to<br />
Jeff Milde for all his logistical support.<br />
After reading the reports from the <strong>Roth</strong> <strong>Williams</strong> regional directors, I was struck by<br />
the level <strong>of</strong> involvement in education to which this group has devoted itself. Unfortunately,<br />
we meet only once a year to reconnect with our far-flung colleagues to reinvigorate<br />
and recommit ourselves. I see the <strong>RWISO</strong> <strong>Journal</strong> as having a vital function<br />
in sharing information for those members who attend the annual meeting and, more<br />
importantly, for those who cannot. It gives us something to hand to our non-<strong>Roth</strong><br />
<strong>Williams</strong> orthodontists and dental colleges to show the type <strong>of</strong> research and clinical<br />
results that is being produced. The articles is this issue are diverse and some are<br />
groundbreaking.<br />
You will note this issue <strong>of</strong> the <strong>Journal</strong> is mostly articles with only one case report.<br />
Oddly, we have had very few case reports submitted. My feeling is that the <strong>RWISO</strong><br />
<strong>Journal</strong> needs a better balance <strong>of</strong> articles and case reports. Over the years I have seen<br />
many outstanding cases presented at the <strong>RWISO</strong> meetings. One <strong>of</strong> the strengths <strong>of</strong> our<br />
group has always been in showing well-treated cases with beautiful finishes. However,<br />
more importantly, these cases have one more thing in common: stable joints with<br />
good function <strong>of</strong> the teeth and joints. And how do we know this? We know because<br />
we evaluate our results with the use <strong>of</strong> centrically mounted models, condylar recording<br />
systems, and TMJ scans. I believe it is the documentation <strong>of</strong> our orthodontic cases<br />
that defines our group. Any journal can show a pretty orthodontic finish. It is another<br />
thing to show all the records, the treatment planning, and then the clinical execution<br />
and a measured outcome <strong>of</strong> a challenging case. Since this <strong>Journal</strong> will be seen by many<br />
non-<strong>Roth</strong> <strong>Williams</strong> orthodontists, I think it is critical we show more <strong>of</strong> our clinical<br />
orthodontic work in this journal.<br />
I hope to see this <strong>Journal</strong> grow and become a vital part <strong>of</strong> our organization as it is a<br />
reflection <strong>of</strong> who we are and what we believe in.<br />
Thomas Chubb, DDS<br />
Editor-in-Chief<br />
tkchubb1@earthlink.net
News from the <strong>Roth</strong> <strong>Williams</strong> Teaching Centers<br />
ARGENTINA<br />
We are pleased to announce that in May <strong>of</strong> this year we began the <strong>Roth</strong><br />
<strong>Williams</strong> FACE (The Foundation for Advanced Continuing Education)<br />
Course in cooperation with the Catholic University <strong>of</strong> Argentina. Dr.<br />
Oscar Palmas, Dr. Guillermo Ochoa and Dr. Eduardo Rubio (surgeon)<br />
were he instructors for this course. They had the honor <strong>of</strong> working<br />
alongside Dr. Domingo Martin and Dr. Jorge Ayala. The highlight was a<br />
lecture given by Dr. Martin on interdisciplinary treatment.<br />
Many feeder courses were developed this year in different provinces,<br />
including Salta, Jujuy, Rio Gallegos and Santiago del Estero. More than<br />
300 hundred students were taught about the <strong>Roth</strong> <strong>Williams</strong> philosophy.<br />
In September 2011, Dr. Jorge Ayala will give a feeder course<br />
entitled “Biomechanical Treatment in <strong>Roth</strong> Philosophy.”<br />
For next year we are planning a <strong>Roth</strong> <strong>Williams</strong> FACE national meeting<br />
in Jujuy, an Argentinean province. The <strong>Roth</strong> <strong>Williams</strong> Center Argentina<br />
will participate in the Mendoza <strong>Society</strong> Orthodontic Meeting in<br />
September. Dr. Oscar Palmas will give a lecture on self-ligation and<br />
micro-screw in <strong>Roth</strong> Philosophy.<br />
We are very happy to see the poster contributions for the Rome meeting<br />
from our <strong>Roth</strong> <strong>Williams</strong> students. We would also like to take this<br />
opportunity to congratulate the <strong>Journal</strong> on its second issue. We encourage<br />
you all to continue working!!<br />
Dr. Oscar Palmas<br />
Director, <strong>Roth</strong> <strong>Williams</strong> Center Argentina<br />
BRAZIL<br />
The Brazilian Center began a new CCO group in June 2009. It has<br />
attracted students from the northwest to the southwest <strong>of</strong> Brazil. Dr.<br />
Fantini has been traveling to various places in Brazil to spread the<br />
<strong>Roth</strong> Philosophy. She has been teaching courses and has even lectured<br />
at an advanced-level specialization course, where her talks about the<br />
Philosophy have become a tradition.<br />
In October <strong>2010</strong>, the SPO meeting, which is the most important meeting<br />
in Latin America, will take place in Brazil. Dr. Fantini will speak<br />
on <strong>Roth</strong>’s Philosophy: multidisciplinary treatment <strong>of</strong> skeletal class II<br />
malocclusion with bilateral condylar degeneration and generalized root<br />
resorption.<br />
Since 2009 four abstracts have been published in conference proceedings,<br />
three articles have been accepted in orthodontic magazines, and<br />
two book chapters have been dedicated to the <strong>Roth</strong> Philosophy. Dr.<br />
Fantini has participated in 10 MA, PhD, and qualifying examinations<br />
as an examiner, enhancing the concepts <strong>of</strong> the <strong>Roth</strong> Philosophy. For a<br />
complete list <strong>of</strong> the articles and abstracts, please contact the <strong>RWISO</strong><br />
<strong>of</strong>fice.<br />
The study group founded in the beginning <strong>of</strong> 2008 remains active with<br />
reunions every 2 months. We believe we have found an interesting formula<br />
to deepen the knowledge <strong>of</strong> those who took the CCOs. At each<br />
group meeting, our program includes 3 activities—a participant presentation<br />
on a given theme, a clinical case presentation and discussion,<br />
and a talk on a new topic <strong>of</strong> current interest. This format has made the<br />
study group very popular.<br />
We plan to start a new CCO group in June 2011.<br />
Finally, we are considering organizing a memorial meeting for all South<br />
America in São Paulo in November <strong>2010</strong>.<br />
Dra. Marisa Gianesella Bertolaccini<br />
Director, <strong>Roth</strong> <strong>Williams</strong> Center Brazil<br />
CHILE<br />
As is traditional, our educational activities have remained very active<br />
through continuing courses, 2- or 3-day courses, and participation<br />
in various meetings. We are currently <strong>of</strong>fering long-term courses in<br />
Mexico (two), Argentina, Paraguay, and Chile with a total <strong>of</strong> 170<br />
students. In 2009 thru <strong>2010</strong> we held 34 courses.<br />
In <strong>2010</strong> we will <strong>of</strong>fer two new continuing courses, one in Michoacán,<br />
México, and the other one at the Universidad de Tucumán, Argentina.<br />
A course in Brazil, to be held in collaboration with Dr. Solange Fantini,<br />
is also being organized.<br />
Drs. Jorge Ayala and Gonzalo Gutierrez<br />
Directors, <strong>Roth</strong> <strong>Williams</strong> Center Chile<br />
JAPAN<br />
We are pleased to announce that we now have 45 members. Members<br />
are doctors who have graduated from the 2-year course and have also<br />
presented cases with stable and repeatable jaw position. Each year we<br />
hold an annual meeting where each participant shows his/her cases<br />
treated according to the <strong>Roth</strong> philosophy. Along with the annual meeting,<br />
we are now preparing for the 15th anniversary meeting in Tokyo<br />
on November 28-29. This meeting is open to all interested doctors.<br />
We are expecting a great attendance. We <strong>of</strong> course welcome <strong>RWISO</strong><br />
members from all over the world.<br />
The ninth 2-year course is steadily ongoing and session 5 was held for<br />
5 days in June, and featured Dr. Jorge Ayala from Chile as a special<br />
instructor. The 14th basic course will be held in the fall.<br />
Dr. Kazumi Ikeda<br />
Director, <strong>Roth</strong> <strong>Williams</strong> Center Japan<br />
continued on next page...<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
5
KOREA<br />
In March <strong>2010</strong> the eighth <strong>Roth</strong> <strong>Williams</strong> <strong>International</strong> Seminar was<br />
held. The 10 participants in the course were instructed by Drs. Byungtaek<br />
Choi, Eunah Choi, and Gyehyeong Lee. All participants enthusiastically<br />
took part in the course.<br />
As visiting pr<strong>of</strong>essors, Drs. Byungtaek Choi and Eunah Choi lectured<br />
on the <strong>Roth</strong> philosophy to the residents <strong>of</strong> the Department <strong>of</strong> Orthodontics<br />
at the Seoul National University Dental Hospital. The lectures<br />
were held weekly during the month <strong>of</strong> June <strong>2010</strong>.<br />
The <strong>Roth</strong> <strong>Williams</strong> Center Korea has been encouraging our members<br />
to contribute to the <strong>Roth</strong> <strong>Williams</strong> Legacy Fund. We expect a desirable<br />
outcome by the <strong>2010</strong> annual meeting in Rome.<br />
Dr. Eunah Choi<br />
Director, <strong>Roth</strong> <strong>Williams</strong> Center Korea<br />
SPAIN<br />
Without any doubt 2009 was a great year for RW Spain/Portugal.<br />
Concerning the RW 2-year course, this year we finished group number<br />
10 (26 students) and we started group number 11 (28 students). The<br />
2-year course has truly grown to be a comprehensive orthodontic<br />
course. We now have three full-time teachers who come to every<br />
session and not only help in the clinic but also present as teachers.<br />
They are Drs. Alberto Canabez from Barcelona, Eugenio Martins<br />
from Portugal, and Iñigo Gomez from Bilbao. All three <strong>of</strong> them have<br />
contributed to the excellent quality <strong>of</strong> the RW course. Apart from these<br />
full-time teachers, we have also incorporated into our courses experts<br />
in the different fields <strong>of</strong> dentistry, who have come and taught different<br />
sessions. They are Dr. Iñaki Gamborena, prosthodontist, Drs. Jon<br />
Zabalegui and Iñigo Sada, periodontists, Dr. Dave Hatcher, radiologist,<br />
Dr. Borja Zabalegui, endodontist, Dr. Renato Cocconi, orthodontist,<br />
and Dr. Mirco Raffaini, surgeon. All <strong>of</strong> these teachers have given the<br />
RW courses a truly interdisciplinary approach, which is what FACE<br />
promotes worldwide.<br />
Another important aspect <strong>of</strong> 2009 that has been fundamental in<br />
making RW a truly interdisciplinary course is the fact that we have<br />
organized two different courses, Bioesthetics with Dr. Ken Hunt and Dr<br />
Alejandro James, and Orthognathic Surgery with Dr. Lucho Quevedo.<br />
Many <strong>of</strong> our former students have signed up for the courses, and this<br />
has given them a greater understanding <strong>of</strong> the importance <strong>of</strong> incorporating<br />
both disciplines into our interdisciplinary approach. But we<br />
cannot forget that with Osteoplac now organizing and promoting our<br />
courses they have become truly pr<strong>of</strong>essional, and without this support<br />
we could have never reached the status that we now enjoy.<br />
Dr. Domingo Martín<br />
Director, <strong>Roth</strong> <strong>Williams</strong> Center Spain and Portugal<br />
6<br />
News from the <strong>Roth</strong> <strong>Williams</strong> Teaching Centers<br />
UNITED STATES<br />
New and exciting things are happening within the Advanced Education<br />
in Orthodontics (AEO) group. In June <strong>of</strong> <strong>2010</strong>, Group VIII will<br />
have their graduation. Group VIII is the largest class, with 25 doctors.<br />
A total <strong>of</strong> 125 doctors have finished the rigorous seven sessions. The<br />
directors have been extremely uplifted by the positive responses given<br />
by the graduates as to their overall educational experience. Comments<br />
like this are the usual: “Keep up the good work. I thank you daily in<br />
the back <strong>of</strong> my mind for telling me I needed to take this course and<br />
that I would be a better orthodontist. You guys were absolutely right<br />
and as challenging as our pr<strong>of</strong>ession is and as smart as our colleagues<br />
are, I feel light years ahead <strong>of</strong> them and my GP’s thank you.” Ben.<br />
The course is continuing to improve and evolve without sacrificing any<br />
<strong>of</strong> the <strong>Roth</strong> <strong>Williams</strong> basics. Techniques such as the true horizontal<br />
hinge axis mountings combined with true horizontal hinge axis 3-D<br />
imaging have been introduced to improve accuracy <strong>of</strong> diagnosis and<br />
treatment planning. In the past, AEO was successful in improving the<br />
Visual Treatment Options (VTO) both in ease <strong>of</strong> use and in teaching<br />
technique. Now the course incorporates the latest in 3-D technology.<br />
The directors have been instrumental in developing s<strong>of</strong>tware that enhances<br />
the efficiency <strong>of</strong> orthodontic diagnosis and treatment planning.<br />
The next step is to develop 3-D s<strong>of</strong>tware that is based on the true hinge<br />
axis. This is being handled by Dr. Robert Frantz.<br />
Dr. Andrew Girardot is responsible for editing and publishing the longawaited<br />
<strong>Roth</strong> <strong>Williams</strong> Philosophy textbook. Because <strong>of</strong> the substantial<br />
commitment required for this important project, Andy will not be<br />
teaching formally until his work on the book is complete.<br />
The true standard wide archform (SWA) system that Dr. <strong>Roth</strong> developed<br />
is continuing to evolve. With the help <strong>of</strong> the Head <strong>of</strong> Product Development<br />
at GAC, Tom Macari, and AEO, improvements to the bracket are<br />
in the works.<br />
The teaching techniques developed at AEO are evolving as well. With<br />
the advent <strong>of</strong> new computer technology, many new and exciting things<br />
will be happening in the next year.<br />
The <strong>Roth</strong> <strong>Williams</strong> USA center has a new home base. Due to an excellent<br />
opportunity afforded us by Dr. Carlos Navarro, AEO will be moving<br />
to Houston, Texas. So in October <strong>of</strong> <strong>2010</strong>, Group IX will travel to<br />
Texas for the new class. The new facility will have adequate space for<br />
teaching the total <strong>Roth</strong> <strong>Williams</strong> experience. The clinical, laboratory,<br />
and lecture will now be in one location. This location is close to many<br />
fine restaurants and entertainment.<br />
Drs. Andy Girardot, Bob Frantz, and Ted Freeland<br />
Directors, <strong>Roth</strong> <strong>Williams</strong> Center USA<br />
URUGUAY<br />
Once again, it is a pleasure for the <strong>Roth</strong> <strong>Williams</strong> Center Uruguay for<br />
Functional Occlusion (RWCUFO) to be present in our <strong>Journal</strong>.<br />
We would like to inform you that finally in December 2009, our 3-year<br />
course started in the Faculty <strong>of</strong> Odontology, Catholic University <strong>of</strong><br />
Montevideo, Uruguay. The first three sessions have been completed, with<br />
a total <strong>of</strong> 13 participants. We are having real success with the contributions<br />
<strong>of</strong> our friends and outstanding speakers from all over the world.
In addition, three 8-hour courses were scheduled in April, August,<br />
and December <strong>2010</strong>. Presentations include Dr. <strong>Roth</strong>’s Philosophy: the<br />
importance <strong>of</strong> the condyle setting in the fossae:physiological principles<br />
for neuromuscular deprogramming, by Dr. Guillermo Ochoa; Treatment<br />
planning according to <strong>Roth</strong>’s Philosophy, by Dr. Oscar Palmas;<br />
and Evidence-based <strong>Roth</strong>’s Philosophy and its application in multidisciplinary<br />
treatments, by Dr. Domingo Martín. Dr. Martín will also be<br />
giving a 4-day course for all the specialists related to orthodontics.<br />
To know more about our courses, please visit the Web page www.ucu.<br />
edu.uy/Odontologia, or contact us by e-mail at rwcuruguay@gmail.<br />
com.<br />
Our group is concerned about research. To address this concern, we<br />
are encouraging our students to make a weekly commitment to our<br />
study group. We are working hard in order to achieve the best results.<br />
Dr. Daniela Domínguez Di Prisco<br />
Director, <strong>Roth</strong> <strong>Williams</strong> Center Uruguay<br />
Scenes from <strong>RWISO</strong> 2009<br />
16th Annual Conference, Boston, MA<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
7
The <strong>Roth</strong> <strong>Williams</strong> Legacy Fund Committee Report<br />
Dr. Milton D. Berkman, Chairman, RWLF<br />
Dr. Milton D. Berkman,<br />
Chairman RWLF<br />
8<br />
<strong>Roth</strong> <strong>Williams</strong> Legacy Fund<br />
Fund-Raising Progress<br />
As <strong>of</strong> June 1, <strong>2010</strong>, $208,650 had been donated to the <strong>Roth</strong> <strong>Williams</strong> Legacy Fund (RWLF).<br />
Of the money donated, $178,650 has been given to the general research and education portion<br />
<strong>of</strong> the fund and $30,000 has been specifically donated to the <strong>Roth</strong> <strong>Williams</strong> textbook portion<br />
<strong>of</strong> the fund.<br />
As <strong>of</strong> June 1, <strong>2010</strong>, $107,290 had been pledged to RWLF but had not yet been donated.<br />
RWLF is proud <strong>of</strong> the progress that has been made to date. Due in part to the worldwide<br />
economic recession, we realize that our campaign goal <strong>of</strong> $1 million in 5 years may not be<br />
attainable. However, we truly believe that the goal <strong>of</strong> $1 million will be reached as <strong>RWISO</strong><br />
continues to grow in stature and respect. The future is bright for the <strong>Roth</strong> <strong>Williams</strong> Philosophy<br />
<strong>of</strong> goal-directed interdisciplinary patient care.<br />
A special thanks to Drs. Jeff McClendon and Milt Berkman for giving the Coordinating Orthodontic and Restorative Efforts<br />
(CORE) course and raising almost $9,000 for RWLF. As <strong>of</strong> July <strong>2010</strong>, the course will have been given four times.<br />
2009 Boston Meeting and <strong>Journal</strong><br />
At the <strong>RWISO</strong> <strong>International</strong> meeting held in Boston, Massachusetts, in May 2009, the Committee was pleased with the<br />
membership’s response to the RWLF fund-raising campaign for the general endowment fund and for the <strong>Roth</strong> <strong>Williams</strong><br />
Philosophy textbook fund. The publication <strong>of</strong> the first issue <strong>of</strong> the <strong>RWISO</strong> <strong>Journal</strong>, in May 2009, came to fruition in part<br />
because <strong>of</strong> a grant from the RWLF general endowment fund for $14,000. As Dr. Domingo Martín said in the first issue <strong>of</strong><br />
the <strong>Journal</strong>, “I cannot forget it was Dra. Anka Sapunar who first founded a journal for this group, and we must all be very<br />
grateful to her for the great job that she did. This is a continuation <strong>of</strong> what she started. Muchas gracias, Anka!!!”<br />
The renewal <strong>of</strong> the <strong>Journal</strong> would not have been possible without the seed money from RWLF. This is just one <strong>of</strong> the many<br />
ways that RWLF is able to fulfill its mission to advance the scientific and clinical benefits <strong>of</strong> the <strong>Roth</strong> <strong>Williams</strong> Philosophy<br />
<strong>of</strong> goal-directed interdisciplinary patient care. What a great moment for the <strong>RWISO</strong> membership! For RWLF it was a significant<br />
first step, because it demonstrated the important role <strong>of</strong> an endowment fund in the future growth and longevity <strong>of</strong> an<br />
organization and a philosophy <strong>of</strong> patient care. RWLF and the <strong>RWISO</strong> membership are looking forward to the second issue<br />
<strong>of</strong> the <strong>RWISO</strong> <strong>Journal</strong> at the Rome Conference with great anticipation.<br />
Research Evaluation and Approval Committee (REAC)<br />
The RWLF Committee’s initial major efforts have been directed toward fund-raising, and toward gaining the trust and<br />
confidence <strong>of</strong> the <strong>RWISO</strong> membership. Now that 30% <strong>of</strong> the $1 million goal has been pledged or donated, the Committee<br />
is ready for a new endeavor—to develop research grant evaluation, approval, and funding. One <strong>of</strong> the mission<br />
statements <strong>of</strong> RWLF is “partial or full support <strong>of</strong> research projects that lead to publication <strong>of</strong> scientific and clinical<br />
papers in peer-reviewed international journals.” The Committee is pleased to announce that two research grants have<br />
been approved and are in the process <strong>of</strong> being funded by <strong>RWISO</strong>/RWLF.
Drs. Edson Illipronti and Solange Fantini from Brazil were awarded a grant for a research project entitled Evaluation<br />
<strong>of</strong> functional morphology in children with unilateral posterior crossbite before and after rapid maxillary expansion.<br />
The grant is to pay in part for MRI studies. The grant is for $16,000 over a 3-year period.<br />
Drs. Carol Weinstein and Sigal Bentolila Weiner from Chile were awarded a grant for a research project entitled Degree<br />
<strong>of</strong> apical root proximity, periodontitis, and root resorption <strong>of</strong> the upper canine and first bicuspid found in sample<br />
<strong>of</strong> <strong>Roth</strong> prescription-treated orthodontic cases using cone beam radiography compared to panoramic radiography.<br />
The grant is to pay in part for cone beam radiography studies. The grant is for $3,000 over a 3-year period.<br />
Donation and Pledges<br />
Donations to RWLF can be made in the following ways:<br />
1. Pr<strong>of</strong>essional Courtesy/Grateful Patient. Persons to whom you <strong>of</strong>fer orthodontic services as a courtesy are invited to<br />
demonstrate their appreciation by making a contribution to RWLF in your name.<br />
2. Case for the Future <strong>of</strong> the <strong>Roth</strong> <strong>Williams</strong> Philosophy. Doctors can donate one new case as a “case for the future”<br />
by paying the fee to RWLF.<br />
3. Doctors giving courses or lectures can donate a portion <strong>of</strong> the honorarium or course fees to RWLF.<br />
4. Donations can be made in memory <strong>of</strong>, or in honor <strong>of</strong>, a colleague, friend, relative, or parent.<br />
5. Or just make a donation because <strong>of</strong> what the <strong>Roth</strong> <strong>Williams</strong> Philosophy has meant to your pr<strong>of</strong>essional life<br />
Donations can be designated for the general research and education fund or for publication <strong>of</strong> the <strong>Roth</strong> <strong>Williams</strong><br />
Philosophy textbook.<br />
For more on how to donate, visit the <strong>RWISO</strong> Web site at www.rwiso.org.<br />
RWLF Committee<br />
Thank you to those individuals who serve on the Legacy Fund Committee.<br />
Milton D. Berkman, Chairman RWLF<br />
Peggy Brazones<br />
Alan Marcus<br />
Domingo Martín<br />
Jeff Milde, Executive Director <strong>RWISO</strong><br />
Joe Pelle<br />
Straty Righellis, Chairman REAC<br />
Manny Wasserman<br />
David Way<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
9
<strong>Roth</strong> <strong>Williams</strong> Legacy Fund Donors<br />
Tribute to Donors<br />
We thank all <strong>of</strong> our loyal and faithful donors for their support <strong>of</strong> the Legacy Fund. Below, we pay tribute to those donors who have given from<br />
January 1, 2006, through June 21, <strong>2010</strong>.<br />
Platinum (10,000 - $49,999)<br />
Dr. Milton D. Berkman<br />
Dr. Domingo Martin<br />
Dr. Straty Righellis<br />
Dr. Carl Roy<br />
Dr. Manny Wasserman<br />
Dr. Robert E. <strong>Williams</strong><br />
Gold Circle ($5,000 - $9,999)<br />
Dr. Margaret Brazones<br />
Dr. Byungtaek Choi<br />
Dr. Andrew Girardot<br />
Dr. Darrell Havener<br />
Dr. John Lawson<br />
Dr. Jina Linton<br />
Dr. Jeffrey McClendon<br />
Dr. James Sieberth<br />
Dr. Wayne Sletten<br />
Dr. David Way<br />
GAC <strong>International</strong><br />
Silver Circle ($1,000 - $4,999)<br />
Dr. Terry Adams<br />
Dr. Claudia Aichinger<br />
Dr. Robert Angorn<br />
Dr. Joachim Bauer<br />
Dr. Patricia Boice<br />
Dr. Renato Cocconi<br />
Dr. Frank Cordray<br />
Dr. K. George Elassal<br />
Dr. Keenman Feng<br />
Dr. Michael Goldman<br />
Dr. Frank Gruber<br />
Dr. David Hatcher<br />
Dr. Kazumi Ikeda<br />
Dr. John Kharouf<br />
Dr. L. Douglas Knight<br />
Dr. Young Jun Lee<br />
Dr. Gerald Malovos<br />
Dr. Alan Marcus<br />
Dr. Ramon Marti<br />
Dr. Roger Pitl<br />
Dr. Paul Rigali<br />
Dr. Nile Scott<br />
Dr. Sean Smith<br />
Dr. Katsuji Tanaka<br />
Reliance Orthodontic Products<br />
10 Legacy Fund Donors<br />
Bronze Circle ($1 - $999)<br />
Dr. Hideaki Aoki<br />
Dr. George Babyak<br />
Dr. Mary Burns<br />
Dr. Dara Chira<br />
Dr. Tom Chubb<br />
Dr. Warren Creed<br />
Dr. Graciela de Bardeci<br />
Dr. Chieko Himeno<br />
Dr. Takehiro Hirano<br />
Dr. Akira Kawamura<br />
Dr. Mi Hee Kim<br />
Dr. Yutaka Kitahara<br />
Dr. Shunji Kitazono<br />
Dr. Felix Lazaro<br />
Dr. N. Summer Lerch<br />
Dr. Ilya Lipkin<br />
Dr. George Marse<br />
Jeff Milde<br />
Dr. Kouichi Misaki<br />
Dr. Hideaki Miyata<br />
Dr. Yo Mukai<br />
Dr. Yoshihiro Nakajima<br />
Dr. Joseph Pelle<br />
Dr. Akiyuki Sakai<br />
Dr. Atsuyo Sakai<br />
Dr. Hidetoshi Shirai<br />
Dr. Motoyasu Taguchi<br />
Dr. Naoyuki Takahashi<br />
Dr. Hiroshi Takeshita<br />
Dr. Yasoo Watanabe<br />
Dr. Benson Wong<br />
Dr. Koji Yasuda<br />
Dr. Yeong-Charng Yen<br />
Estate Planning<br />
Dr. Charles R. de Lorimier<br />
Dr. Donald W. Linck, II<br />
Friends <strong>of</strong> <strong>Roth</strong> <strong>Williams</strong><br />
Advanced Education in Orthodontics<br />
Jewish Communal Fund<br />
T&T Design Lab (Japan)<br />
Timothy McCarthy<br />
Pledge Circle<br />
Thank you to these donors who have pledged<br />
donations to the Legacy Fund over multiple years.<br />
Dr. Satoshi Adachi<br />
Dr. Scott Anderson<br />
Dr. Jorge Ayala<br />
Dr. Milton Berkman<br />
Dr. Margaret Brazones<br />
Dr. Warren Creed<br />
Dr. Robert Good<br />
Dr. Mila Gregor<br />
Dr. Tateshi Hiraki<br />
Dr. Maria Karpov<br />
Dr. Mi Hee Kim<br />
Dr. Masako Komatsu<br />
Dr. Jina Lee Linton<br />
Dr. Ilya Lipkin<br />
Dr. Dave Livingston<br />
Dr. Yuci Ma<br />
Dr. Alan Marcus<br />
Dr. Ramon Marti<br />
Dr. Joseph M. Pelle<br />
Dr. Paul Rigali<br />
Dr. Nile Scott<br />
Dr. Wayne Sletten<br />
Dr. Manny Wasserman<br />
Dr. Benson Wong<br />
Dr. Yeong-Charng Yen<br />
Dr. Michael Yitschaky
The Transverse Dimension:<br />
Diagnosis and Relevance to Functional Occlusion<br />
Ryan K. Tamburrino, DMD ■ Normand S. Boucher, DDS ■ Robert L. Vanarsdall, DDS<br />
■ Antonino G. Secchi, DMD, MS<br />
Ry a n K. Ta m b u R R i n o , DMD<br />
rktambur@dental.upenn.edu<br />
■ Clinical Associate—Univ. <strong>of</strong> Penn.<br />
School <strong>of</strong> Dental Medicine, Dept.<br />
<strong>of</strong> Orthodontics<br />
noR m a n d S. bo u c h e R, ddS<br />
■ Clinical Associate Pr<strong>of</strong>essor—<br />
Univ. <strong>of</strong> Penn. School <strong>of</strong> Dental<br />
Medicine, Dept. <strong>of</strong> Orthodontics<br />
Rob e R T L. Va n a R S d a L L , ddS<br />
■ Pr<strong>of</strong>essor and Chair—<br />
Univ. <strong>of</strong> Penn. School <strong>of</strong> Dental<br />
Medicine, Dept. <strong>of</strong> Orthodontics<br />
anT o n i n o G. Se c c h i , DMD, MS<br />
■ Assistant Pr<strong>of</strong>essor <strong>of</strong> Orthodontics,<br />
Clinician Educatorand Clinical<br />
Director—Univ. <strong>of</strong> Penn. School <strong>of</strong><br />
Dental Medicine, Dept. <strong>of</strong> Orthodontics<br />
For complete contributor information, please see end <strong>of</strong> article.<br />
Introduction<br />
The goals <strong>of</strong> orthodontic treatment are well established<br />
for static and functional occlusal relationships. In order<br />
to achieve Andrews’ six keys to normal occlusion for the<br />
dentition, 1 the jaws must be optimally proportioned in<br />
three planes <strong>of</strong> space and positioned in CR. Orthodontists<br />
have a multitude <strong>of</strong> cephalometric analyses available to diagnose<br />
skeletal and dental variations <strong>of</strong> the sagittal and<br />
vertical dimensions. 2–6 Several analyses for the transverse<br />
dimension are also available, 3,6,7 but these analyses are not<br />
well accepted as forming part <strong>of</strong> a traditional orthodontic<br />
diagnosis.<br />
In the sagittal dimension, when the jaws do not relate<br />
optimally, the dentition will attempt to compensate, resulting<br />
in excessively proclined or retroclined anterior teeth. In the<br />
transverse dimension, when the jaws do not relate optimally,<br />
usually due to a deficiency in the width <strong>of</strong> the maxilla, 7,8 the<br />
teeth will erupt into a crossbite or reconfigure their inclinations<br />
to avoid a crossbite. This compensation typically<br />
involves lingual tipping <strong>of</strong> the mandibular posterior teeth,<br />
which are then described as being excessively negatively inclined.<br />
In addition, the maxillary posterior teeth are tipped<br />
Summary<br />
Much focus <strong>of</strong> orthodontic diagnoses has been placed on the sagittal and vertical<br />
dimensions. However, a proper evaluation <strong>of</strong> the transverse dimension<br />
must also have equal importance. Research has shown that interferences from<br />
an exaggerated curve <strong>of</strong> Wilson due to a maxillary transverse deficiency play<br />
a role in centric relation (CR)/central occlusion (CO) discrepancies, adverse<br />
periodontal stresses, and crani<strong>of</strong>acial development. This article illustrates<br />
three scientifically validated methods for evaluating the transverse dimension:<br />
Ricketts’ P-A cephalometric analysis, Andrews’ Element III analysis, and the<br />
University <strong>of</strong> Pennsylvania Cone-Beam CT transverse analysis. The aim is to<br />
show methods using traditional cephalometry, study models, and cone-beam<br />
computed tomography, not to compare one method to another. The reader<br />
may then choose to use the method that is most appropriate for his practice.<br />
facially. These teeth are then described as being excessively<br />
positively inclined (Figure 1).<br />
Figure 1 Example <strong>of</strong> excessive tooth angulations.<br />
Transverse Deficiency and CR/CO Discrepancy<br />
In the prosthodontic literature, these transverse tooth compensations<br />
have been graphically illustrated with a crossarch<br />
arc constructed through the buccal and palatal cusps <strong>of</strong><br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
11
the maxillary molars. This is known as the curve <strong>of</strong> Wilson.<br />
With excessive inclination <strong>of</strong> the maxillary molars to compensate<br />
for insufficient maxillary width, the curve <strong>of</strong> Wilson<br />
is greatly exaggerated, and the palatal cusps are positioned<br />
below the buccal cusps (Figure 2).<br />
Figure 2 An exaggerated curve <strong>of</strong> Wilson<br />
(note palatal cusps below buccal cusps).<br />
Many articles that describe the impact <strong>of</strong> CR/CO discrepancies<br />
on occlusion focus on how these discrepancies<br />
affect diagnosing the sagittal and vertical dimensions. The<br />
literature has suggested that the “plunging” palatal cusps<br />
shown in Figure 3 are <strong>of</strong>ten the primary contacts that induce<br />
vertical condylar distraction on closure from CR. From<br />
a seated condylar position, the patient may fulcrum <strong>of</strong>f the<br />
premature contacts <strong>of</strong> the terminal molars to obtain the<br />
maximal intercuspal position. The Panadent Condylar Position<br />
Indicator (CPI) and the SAM Mandibular Position Indicator<br />
(MPI) graphically identify this vertical component <strong>of</strong><br />
condylar distraction. 9-12<br />
Figure 3 Note plunging palatal cusps and extreme curve<br />
<strong>of</strong> Wilson on molars <strong>of</strong> an arch that was expanded<br />
with arch wires and brackets only.<br />
12 Tamburrino et al | The Transverse Dimension: Diagnosis and Relevance to Functional Occlusion<br />
According to McNamara and Brudon, 13 “the orientation <strong>of</strong><br />
the lingual cusps <strong>of</strong> the maxillary posterior teeth… <strong>of</strong>ten lie[s]<br />
below the occlusal plane… This common finding in patients<br />
with malocclusions <strong>of</strong>ten is due to maxillary constriction and<br />
subsequent dentoalveolar compensation in which the maxillary<br />
posterior teeth are in a slightly flared orientation.” The results<br />
<strong>of</strong> a study by McMurphy and Secchi14 indicate that vertical distraction<br />
<strong>of</strong> the condyles in CR/CO discrepancies can be related<br />
to an exaggerated curve <strong>of</strong> Wilson, secondary to a transverse<br />
deficiency <strong>of</strong> the maxilla. These authors conclude that, in the<br />
absence <strong>of</strong> a posterior crossbite, the plunging palatal cusps and<br />
exaggerated curve <strong>of</strong> Wilson become the fulcrum point for the<br />
vertical condylar distraction from CR to maximum intercuspation.<br />
Furthermore, extrapolation <strong>of</strong> this statement suggests that<br />
if the transverse skeletal dimension is normalized, the curve <strong>of</strong><br />
Wilson is flattened, and the arches are coordinated, an important<br />
component <strong>of</strong> the CR/CO discrepancy is eliminated.<br />
Transverse Deficiency and Working/Nonworking<br />
Interferences<br />
It has been a prosthetic maxim that an exaggerated curve <strong>of</strong><br />
Wilson increases the potential for working and non-working<br />
side interferences. Studies have shown that posterior occlusal<br />
contacts or interferences are linked to increased masticatory<br />
muscle activity. 15,16 In studies where these interferences have<br />
been removed, it has been demonstrated that the activity <strong>of</strong> the<br />
closing musculature is reduced. 16,17 In addition, a study that artificially<br />
created non-working interferences reported increased<br />
muscle activity. 18 These results suggest that it is prudent to normalize<br />
the transverse jaw relationship and flatten the curve <strong>of</strong><br />
Wilson to eliminate the potential for excursive posterior interferences<br />
or contacts.<br />
Transverse Deficiency and the Periodontium<br />
Herberger and Vanarsdall19 have shown an increased risk for<br />
gingival recession in the orthodontic patient with a narrow<br />
maxilla when the skeletal transverse deficiency is camouflaged<br />
with dental expansion. The envelope <strong>of</strong> treatment in the transverse,<br />
with expansion <strong>of</strong> only the dentition, is more limited than<br />
the envelope <strong>of</strong> treatment in the sagittal dimension. 20 Due to the<br />
constraints <strong>of</strong> the thin layer <strong>of</strong> cortical bone <strong>of</strong> the alveolus, as<br />
shown in Figure 4 [see next page], very little tooth movement<br />
needs to occur before the roots are fenestrated, the volume <strong>of</strong><br />
buccal alveolar bone is reduced, and, with thinning gingival tissues,<br />
the risk <strong>of</strong> gingival recession increases.<br />
In recent studies, Harrell21 and Nunn and Harrell22,23 have<br />
shown that the elimination <strong>of</strong> working and nonworking interferences<br />
enhances the long-term periodontal prognosis in patients<br />
susceptible to periodontal disease. Therefore, normalizing the<br />
transverse jaw relationship to eliminate an exaggerated curve
Figure 4 Patient with gingival recession due to orthodontic<br />
treatment in the presence <strong>of</strong> an undiagnosed severe skeletal<br />
transverse discrepancy. Note minimal alveolar bone on<br />
the buccal surface <strong>of</strong> the maxillary molars.<br />
<strong>of</strong> Wilson and nonworking interferences would be beneficial<br />
for adult patients who are periodontally at risk, and might<br />
prophylactically reduce the risk for younger patients.<br />
Transverse Deficiency and the Airway<br />
Ricketts’ description <strong>of</strong> “adenoid facies” 24 also suggests a relationship<br />
between a constricted nasopharyngeal airway and<br />
a narrow maxilla. Ricketts states children with any impairment<br />
<strong>of</strong> the nasal passages become predominantly mouth<br />
breathers. Since the tongue is positioned in the floor <strong>of</strong> the<br />
mouth to allow airflow, it cannot provide support to shape<br />
the developing palate; thus pressure from the circumoral<br />
musculature acts unopposed. The palate is narrowed, and<br />
an exaggerated curve <strong>of</strong> Wilson develops upon tooth eruption.<br />
Because the tongue is positioned low in the mouth, the<br />
patient may also develop a retruded, high-angle mandibular<br />
shape, which can increase the risk for sleep apnea. 25 An example<br />
<strong>of</strong> adenoid facies is shown in Figure 5.<br />
Figure 5 A teenager who had nasopharyngeal airway impairment<br />
during growth and development. The images show the facial,<br />
dental, skeletal, and airway presentation upon growth cessation.<br />
In one recent study, 26 patients with transverse deficien-<br />
cies due to a narrow maxilla who were treated with rapid<br />
palatal expansion, showed an increase <strong>of</strong> 8% to 10% in the<br />
volume <strong>of</strong> the upper airway. In another study, 27 patients with<br />
dental posterior crossbites who were treated with palatal expansion<br />
also showed an increase in the volume <strong>of</strong> the upper<br />
airway. Oliveria de Felippe, et al28 found that palatal expansion<br />
decreased nasal resistance and improved nasal breathing.<br />
While additional research in this area is certainly needed,<br />
the current literature suggests that any improvement in the<br />
volume <strong>of</strong> the airway, as an effect <strong>of</strong> palatal expansion to<br />
optimize the transverse dimension <strong>of</strong> the jaws, may greatly<br />
benefit overall growth and development.<br />
Methods <strong>of</strong> Transverse Diagnosis<br />
With a transverse deficiency due to a narrow maxilla, the<br />
temporomandibular joints, musculature, periodontal tissue,<br />
and airway can be adversely affected in the susceptible patient.<br />
Our goal as orthodontists should be to develop skeletal<br />
relationships and a functional occlusion that are as close to<br />
optimal as possible, to lessen the role that any discrepancies<br />
<strong>of</strong> the occlusion would play in exacerbating the detrimental<br />
effects to the joints, periodontium, or dentition. In order<br />
to achieve this a correct skeletal and dental diagnosis in all<br />
three planes <strong>of</strong> space is mandatory.<br />
In this section, we present three different methods for<br />
diagnosing the transverse dimension—one using traditional<br />
cephalometry, one using dental casts, and one using conebeam<br />
CT (computed tomography). We do not endorse any<br />
one <strong>of</strong> these methods over the others; our purpose here is<br />
simply to describe all three methods, so that readers will be<br />
able to incorporate a transverse skeletal diagnosis into their<br />
practice, no matter what level <strong>of</strong> technology is available.<br />
Regardless <strong>of</strong> which <strong>of</strong> these methods one chooses, the doctor<br />
must keep optimal treatment goals in mind as a rationale for<br />
normalizing the transverse dimension (Figures 6 and 7).<br />
Figure 6 Goals for normalizing the transverse dimension.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
13
Figure 7 Rationale for normalizing the transverse dimension.<br />
Ricketts’ P-A Analysis<br />
In 1969, Ricketts introduced analysis <strong>of</strong> the transverse skeletal<br />
dimension as part <strong>of</strong> his method <strong>of</strong> cephalometric diagnosis.<br />
3 His method uses the frontal, or posteroanterior<br />
(P-A) cephalogram, and is based on the dimensions <strong>of</strong> the<br />
jaws compared to a table <strong>of</strong> age-adjusted normative values.<br />
The premise <strong>of</strong> the analysis is based on locating two skeletal<br />
points to determine maxillary width and two additional skeletal<br />
points to determine mandibular width (Figure 8).<br />
Figure 8 Locations <strong>of</strong> Mx (green) and Ag (yellow).<br />
For the maxilla, the jugal point (Mx) is located on the right<br />
and left sides <strong>of</strong> the maxillary skeletal base at “the depth<br />
<strong>of</strong> the concavity <strong>of</strong> the lateral maxillary contours, at the<br />
junction <strong>of</strong> the maxilla and the zygomatic buttress.” 3 The<br />
maxillary width is determined by the horizontal distance<br />
connecting these two points. For the mandible, a similar<br />
measurement is taken between the two antegonial notches<br />
(Ag). These notches are located on the right and left sides<br />
<strong>of</strong> the mandibular body at the “innermost height <strong>of</strong> contour<br />
along the curved outline <strong>of</strong> the inferior mandibular border,<br />
below and medial to the gonial angle.” 3<br />
Once the measurements have been taken, the mandibular<br />
width (Ag-Ag) is subtracted from the maxillary width (Mx-<br />
Mx) to get the difference in width between the jaws. Ricketts<br />
then determined skeletal age-determined normative relationships<br />
between the maxilla and the mandible (Figure 9). This<br />
allows the analysis to accommodate growing patients, and<br />
allows for the differential growth rates and potentials <strong>of</strong> the<br />
maxilla and the mandible.<br />
Figure 9 Table for determining the age-normal<br />
difference between the maxilla and the mandible.<br />
In order to determine the skeletal age <strong>of</strong> a patient, a handwrist<br />
film is taken and is compared to an atlas <strong>of</strong> male and<br />
female skeletal age standards. 29 To determine the amount <strong>of</strong><br />
expansion needed, the age-adjusted expected difference between<br />
the jaws is subtracted from the measured difference.<br />
An example <strong>of</strong> the Ricketts method is shown in Figure 10.<br />
Figure 10 Example <strong>of</strong> Ricketts’ P-A analysis.<br />
Andrews’ Element III Analysis<br />
In 1970, L. F. Andrews published his landmark paper describing<br />
the six keys to normal static occlusion. 1 Over the next<br />
several decades, he and his son, W. A. Andrews, worked to develop<br />
the six elements philosophy <strong>of</strong> orthodontic diagnosis.<br />
One <strong>of</strong> the diagnostic criteria, Element III, is devoted to analyzing<br />
the transverse relationship <strong>of</strong> the maxilla and mandible<br />
and is based on both bony and dental landmarks. 10<br />
The Element III analysis is based on the assumption that<br />
the WALA (named after Will Andrews and Larry Andrews)<br />
14 Tamburrino et al | The Transverse Dimension: Diagnosis and Relevance to Functional Occlusion
idge determines the width <strong>of</strong> the mandible. According to<br />
Andrews’ definition, the WALA ridge is coincident with the<br />
most prominent portion <strong>of</strong> the buccal alveolar bone when<br />
viewed from the occlusal surface (Figure 11).<br />
Figure 11 Demarcation <strong>of</strong> the WALA ridge.<br />
The WALA ridge is essentially coincident with the<br />
mucogingival junction and approximates the center <strong>of</strong> resistance<br />
<strong>of</strong> the mandibular molars. In a mature patient,<br />
the WALA ridge and the width <strong>of</strong> the mandible cannot be<br />
modified with conventional treatment. Thus the WALA ridge<br />
forms a stable basis for the Element III analysis. 6<br />
The Element III analysis is based on the width change,<br />
if any, <strong>of</strong> the maxilla needed to have upper and lower posterior<br />
teeth upright in bone, centered in bone, and properly<br />
intercuspated. To determine the discrepancy, the first step is<br />
to determine the width <strong>of</strong> the mandible, or the horizontal<br />
distance from the WALA ridge on the right side to the WALA<br />
ridge on the left side. According to Andrews, optimally positioned<br />
mandibular molars will be upright in the alveolus,<br />
and their facial axis (FA) point, or center <strong>of</strong> the crown, will<br />
be horizontally positioned 2 mm from the WALA ridge. With<br />
this information, the width <strong>of</strong> the mandible is then defined as<br />
the WALA-WALA distance minus 4 mm. 6<br />
Figure 12 Determination <strong>of</strong> mandibular<br />
WALA-WALA and FA-FA distances.<br />
The width <strong>of</strong> the maxilla is based on optimization <strong>of</strong> the<br />
angulation <strong>of</strong> the maxillary molars. To determine this width,<br />
one measures the horizontal distance from the FA point <strong>of</strong><br />
the left molar to the FA point <strong>of</strong> the right molar and records<br />
the measurement.<br />
Figure 13 Determining maxillary FA-FA distance and<br />
estimating the change in maxillary molar inclination.<br />
One then looks at the angulation <strong>of</strong> the maxillary molars<br />
and estimates the amount <strong>of</strong> horizontal change that will<br />
occur between the FA points <strong>of</strong> the right and left molars<br />
when they are optimally angulated. The estimated amount <strong>of</strong><br />
change is subtracted from the original FA-FA measurement.<br />
The result represents the width <strong>of</strong> the maxilla. 6<br />
In order to have optimally positioned and optimally inclined<br />
molar teeth that intercuspate well, Andrews states that<br />
the maxillary width must be 5 mm greater than the mandibular<br />
width. 6 In order to determine the amount <strong>of</strong> transverse<br />
discrepancy, or Element III change, needed to produce an<br />
ideal result, one takes the optimal mandibular width, adds<br />
5 mm, and subtracts the maxillary width. An example <strong>of</strong> the<br />
entire analysis is shown in Figure 14.<br />
Figure 14 Example <strong>of</strong> Andrews’ Element III<br />
transverse analysis.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
15
University <strong>of</strong> Pennsylvania Cone-Beam CT Analysis<br />
The current trend in orthodontic imaging and diagnosis is<br />
toward three-dimensional analysis. With the advent <strong>of</strong> conebeam<br />
imaging, orthodontists can obtain precise measurements<br />
without any distortion caused by radiographic projections<br />
or ambiguity <strong>of</strong> point identification. The same rationale<br />
can subsequently be applied to the transverse measurement<br />
<strong>of</strong> the maxilla and the mandible. Ricketts’ and Andrews’<br />
methods for determining the amount <strong>of</strong> transverse discrepancy<br />
between the jaws are based on using readily discernable<br />
landmarks that represent the width <strong>of</strong> the base <strong>of</strong> the alveolar<br />
housing. For Ricketts, these landmarks are Mx-Mx for<br />
the maxilla and Ag-Ag for the mandible. For Andrews, these<br />
landmarks are the two sides <strong>of</strong> the WALA ridge and the FA<br />
points <strong>of</strong> the maxillary and mandibular molars. The WALA-<br />
WALA measurement represents the width <strong>of</strong> the mandible,<br />
and the FA-FA points are used, as described above, to determine<br />
the width <strong>of</strong> the maxilla. Both <strong>of</strong> these methods have<br />
merit. However, with cone-beam CT imaging, it is no longer<br />
necessary to have a measurement dictated by ease with<br />
which landmarks can be identified to represent the widths<br />
<strong>of</strong> the jaws.<br />
Before choosing a method for measuring the base <strong>of</strong> the<br />
jaws, we must first decide what location to use for measurement.<br />
In determining the location <strong>of</strong> the WALA ridge, Andrews<br />
stated that the WALA ridge is an approximation <strong>of</strong> the<br />
center <strong>of</strong> resistance <strong>of</strong> the mandibular teeth. Above the WALA<br />
ridge, the alveolus can be dimensionally molded and altered,<br />
depending on the change in angulation <strong>of</strong> the teeth. However,<br />
the same cannot be said for the portion <strong>of</strong> the alveolus below<br />
the WALA ridge. Thus, in a mature patient, any portion <strong>of</strong> the<br />
alveolus apical to the WALA ridge can be assumed to be reasonably<br />
dimensionally stable during tooth movement, and,<br />
therefore, can define the dimensions <strong>of</strong> the patient’s arch. In<br />
Ricketts’ analysis, Ag-Ag represents the basal portion <strong>of</strong> the<br />
mandible. However, when one looks at the position <strong>of</strong> Ag on<br />
a three-dimensional image, one sees that its correlation with<br />
the base <strong>of</strong> the alveolus is relatively weak in all three planes<br />
<strong>of</strong> space for mature patients (Figure 15).<br />
16<br />
Figure 15 Correlations <strong>of</strong> Mx and Ag to skeletal bases in adults.<br />
Thus, to locate the beginning <strong>of</strong> the base <strong>of</strong> the mandible<br />
with a CT scan, it would seem best to find the skeletal representation<br />
<strong>of</strong> the WALA ridge. This is approximately at the edge <strong>of</strong><br />
the cortical bone opposite the furcation <strong>of</strong> the mandibular first<br />
molars. We can also use this technique to locate the beginning <strong>of</strong><br />
the base <strong>of</strong> the maxilla. If we assume that the maxilla begins at<br />
the projection <strong>of</strong> the center <strong>of</strong> resistance <strong>of</strong> the maxillary teeth<br />
onto the buccal surface <strong>of</strong> the cortical bone, Ricketts’ use <strong>of</strong> Mx<br />
to determine maxillary width appears to be at approximately at<br />
the same horizontal position. Additionally, by using Mx point,<br />
any exostoses present along the buccal portion <strong>of</strong> the alveolus<br />
will not interfere with the measurement. Andrews’ method,<br />
on the other hand, has no directly definable skeletal landmark<br />
for the maxilla; it relies on estimated changes in the angulation<br />
<strong>of</strong> the molars to determine the skeletal transverse discrepancy.<br />
Therefore, Ricketts’ method <strong>of</strong> defining the basal skeletal width<br />
<strong>of</strong> the maxilla appears to be more appropriate.<br />
We begin, then, by defining locations for measuring maxillary<br />
and mandibular skeletal basal width. Next, we explore<br />
concepts for defining these locations on cone-beam CT imaging.<br />
The basic premise for the mandible is to locate the most buccal<br />
point on the cortical plate opposite the mandibular first molars<br />
at the level <strong>of</strong> the center <strong>of</strong> resistance. According to Katona, this<br />
location is approximately coincident with the furcation <strong>of</strong> the<br />
roots <strong>of</strong> the molars. 30 As we explained above, the authors chose<br />
this point due to the relative immutability <strong>of</strong> the alveolus apical<br />
to this location with orthodontics and because it represents the<br />
absolute minimal width <strong>of</strong> the basal bone for each jaw.<br />
For the purposes <strong>of</strong> this technique, the authors used Dolphin<br />
3D, release 11 (Patterson Dental, Chatsworth, CA), but<br />
the concepts can be applied to any s<strong>of</strong>tware with the capability<br />
to analyze a cone-beam CT image. After properly orienting<br />
the image, we open the multiplanar view (MPV) screen to see<br />
simultaneous axial, sagittal, and coronal cuts <strong>of</strong> the image.<br />
Tamburrino et al | The Transverse Dimension: Diagnosis and Relevance to Functional Occlusion
Figure 16 MPV <strong>of</strong> a cone-beam CT scan.<br />
To determine the width <strong>of</strong> the mandible, we scroll down<br />
through the image until we locate the furcation <strong>of</strong> the first<br />
molar. Then we scroll posteriorly through the scan until we<br />
locate the coronal cross-section through the center <strong>of</strong> the<br />
mandibular first molars.<br />
Figure 17 Location <strong>of</strong> the mandibular axial and coronal cuts.<br />
Now we switch to full-screen axial view. Using the cut<br />
lines as a guide, we measure the width <strong>of</strong> the mandible from<br />
the intersection <strong>of</strong> the cut line with the most buccal portion<br />
<strong>of</strong> the cortical plate on both the right and left sides.<br />
Figure 18 Measurement <strong>of</strong> mandibular skeletal width.<br />
For the maxilla, a similar method is employed. The only<br />
difference is that the axial and coronal cuts must be taken at<br />
the position Mx-Mx, and the same measurement as in the<br />
Ricketts’ analysis is used.<br />
Figure 19 Measurement <strong>of</strong> maxillary axial and coronal cuts.<br />
Figure 20 Measurement <strong>of</strong> maxillary skeletal width.<br />
The analysis <strong>of</strong> the width <strong>of</strong> the maxilla and mandible at<br />
the level <strong>of</strong> the first molars is straightforward once we have<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
17
taken the measurements <strong>of</strong> both jaws. By subtracting the<br />
mandibular width from the maxillary width, we determine<br />
the difference between the two jaws. Both Ricketts’ and Andrews’<br />
analyses demonstrate that the optimal transverse difference<br />
between the maxilla and mandible is 5 mm in mature<br />
patients. A preliminary analysis <strong>of</strong> 5 cases where the maxillary<br />
and mandibular molars were upright in the alveolus,<br />
centered in the alveolus, and well intercuspated, produced<br />
measurements where the difference between the width <strong>of</strong> the<br />
jaws approximated 5 mm on a consistent basis. Therefore,<br />
the seemingly ideal difference for the width <strong>of</strong> the jaws in<br />
mature patients using the Penn CBCT analysis would also<br />
appear to be 5 mm. To determine the amount <strong>of</strong> expansion<br />
necessary to achieve an ideal jaw relationship in the transverse<br />
dimension, the measured difference between the jaws<br />
should be subtracted from 5.<br />
Figure 21 Example <strong>of</strong> optimal transverse skeletal<br />
relationships using cone-beam CT analysis.<br />
Research performed by Simontacchi-Gbologah, et al31 ,<br />
has verified the validity <strong>of</strong> the University <strong>of</strong> Pennsylvania<br />
CBCT analysis for the transverse diagnosis. However, the<br />
difference between the described method here and the method<br />
in the aforementioned research is that the measurements<br />
were taken on coronal cuts, not axial ones. Due to the cross<br />
section <strong>of</strong> the mandibular coronal cut being taken at an angle<br />
that is not perpendicular to the alveolus, a false perception <strong>of</strong><br />
the thickness <strong>of</strong> cortical bone is possible, as shown in Figure<br />
22. Therefore, to reduce errors in judgment and to improve<br />
visualization <strong>of</strong> the most buccal portion <strong>of</strong> the cortical bone,<br />
the authors believe that the axial cut allows for greater precision<br />
<strong>of</strong> measurement over the coronal cross section.<br />
Figure 22 Visualization <strong>of</strong> cortical bone thickness<br />
on coronal and axial cuts <strong>of</strong> the same patient<br />
Future Directions<br />
Now that the methodology <strong>of</strong> the Penn CBCT analysis has<br />
been verified, the next goal will be to extrapolate the analysis<br />
to determine a diagnostic transverse relationship for the canines.<br />
With this, the goal will be to determine the appropriate<br />
arch form for proper stability and function on an individual<br />
basis. An additional study’s aim will be to develop age-specific<br />
transverse normative criteria for Penn CBCT analysis,<br />
similar to Ricketts’ norms for the P-A ceph. ■<br />
References<br />
1. Andrews LF. The six keys to normal occlusion. Am J Orthod. 1972;<br />
62(3):296-309.<br />
2. Jarabak cephalometric analysis. In: <strong>Roth</strong>-<strong>Williams</strong>/AEO Course<br />
Manual; 2006.<br />
3. Ricketts RM. Introducing Computerized Cephalometrics. Rocky<br />
Mountain Data Systems; 1969.<br />
4. Steiner CC. The use <strong>of</strong> cephalometrics as an aid to planning and assessing<br />
orthodontic treatment. Am J Orthod. 1960; (29):8.<br />
5. Downs WB. Analysis <strong>of</strong> the dent<strong>of</strong>acial pr<strong>of</strong>ile. Angle Orthod. 1956;<br />
(26):191.<br />
6. Andrews LF, Andrews WA. Andrews analysis. In: Syllabus <strong>of</strong> the Andrews<br />
Orthodontic Philosophy. 9th ed. Six Elements Course Manual;<br />
2001.<br />
7. McNamara JA, Brudon WL. Orthodontics and Dent<strong>of</strong>acial Orthopedics.<br />
2nd ed. Ann Arbor, MI: Needham Press; 2002: 102-103.<br />
18 Tamburrino et al | The Transverse Dimension: Diagnosis and Relevance to Functional Occlusion
8. Vanarsdall RL. Transverse dimension and long-term stability. Sem in<br />
Orthod. 1999; 5(3):171-180.<br />
9. Cordray FE. Three-dimensional analysis <strong>of</strong> models articulated in the<br />
seated condylar position from a deprogrammed asymptomatic population:<br />
a prospective study, I. Am J Orthod Dent<strong>of</strong>ac Orthop. 2006;<br />
(129): 619-630.<br />
10. Utt TW, Meyers CE, Wierzbe TF, Hondrum SO. A three-dimensional<br />
comparison <strong>of</strong> condylar position changes between centric relation<br />
and centric occlusion using the mandibular position indicator. Am J<br />
Orthod Dent<strong>of</strong>ac Orthop. 1995; (107): 298-308.<br />
11. Crawford SD. The relationship between condylar axis position<br />
as determined by the occlusion and measured by the CPI instrument<br />
and signs and symptoms <strong>of</strong> TM joint dysfunction. Angle Orthod.<br />
1999;(69): 103-115.<br />
12. Tamburrino RK, Secchi AG, Katz SH, Pinto AA. Assessment <strong>of</strong> the<br />
three-dimensional condylar and dental positional relationships in CRto-MIC<br />
shifts. <strong>RWISO</strong> <strong>Journal</strong> 2009; 1(1): 33-42.<br />
13. McNamara JA, Brudon WL. Orthodontics and Dent<strong>of</strong>acial Orthopedics.<br />
2nd ed. Ann Arbor, MI: Needham Press; 2002: 104-105.<br />
14. McMurphy JS, Secchi AG. Effect <strong>of</strong> Skeletal Transverse Discrepancies<br />
on Functional Position <strong>of</strong> the Mandible [thesis]. University <strong>of</strong><br />
Pennsylvania; 2007.<br />
15. Greco PM, Vanarsdall RL, Levrini M, Read R. An evaluation <strong>of</strong><br />
anterior temporal and masseter muscle activity in appliance therapy.<br />
Angle Orthod. 1999; 69(2): 141-141.<br />
16. <strong>Williams</strong>on EH, Lundquist DO. Anterior guidance: its effect on<br />
electromyographic activity <strong>of</strong> the temporal and masseter muscles. J.<br />
Prosthet Dent. 1983; (69): 816-823.<br />
17. Manns A, Chan C, Miralles R. Influence <strong>of</strong> group function and<br />
canine guidance on electromyographic activity <strong>of</strong> elevator muscles. J<br />
Prosthet Dent. 1987; (57): 494-501.<br />
18. Okano N, Baba K, Igarashi Y. Influences <strong>of</strong> altered occlusal guidance<br />
on masticatory muscle activity during clenching. J Oral Rehab.<br />
2007; (9): 679-684.<br />
19. Herberger T, Vanarsdall RL. Rapid Palatal Expansion: Long-Term<br />
Stability and Periodontal Implications [thesis]. University <strong>of</strong> Pennsylvania;<br />
1987.<br />
20. Sarver DM, Pr<strong>of</strong>fit WR. In: Graber TM, Vig KL, Vanarsdall RL,<br />
eds. Orthodontics: Current Principles and Techniques. 4th ed. St.<br />
Louis, MO: Elsevier-Mosby; 2005: 15.<br />
21. Harrell SK. Occlusal forces as a risk factor for periodontal disease.<br />
Periodon. 2003; (32): 111-117.<br />
22. Nunn ME, Harrell SK. The effect <strong>of</strong> occlusal discrepancies on<br />
periodontitis: relationship <strong>of</strong> initial occlusal discrepancies to initial<br />
clinical parameters. J Periodontol. 2001; (72): 485-494.<br />
23. Nunn ME, Harrell SK. The effect <strong>of</strong> occlusal discrepancies on<br />
periodontitis: relationship <strong>of</strong> occlusal treatment to the progression <strong>of</strong><br />
periodontal disease. J Periodontol. 2001; (72): 495-505.<br />
24. Ricketts RM. Respiratory obstruction syndrome. Am J Orthod.<br />
1968;(54):495-507.<br />
25. Comyn FL. MRI Comparison <strong>of</strong> Crani<strong>of</strong>acial Structures in Sleep<br />
Apneic Patients [master’s thesis]. University <strong>of</strong> Pennsylvania; 2009.<br />
26. Cappetta LS, Chung CH, Boucher NS. Effects <strong>of</strong> Bonded Rapid<br />
Palatal Expansion on Nasal Cavity and Pharyngeal Airway Volume: A<br />
Study <strong>of</strong> Cone-Beam CT Images [thesis]. University <strong>of</strong> Pennsylvania;<br />
2009.<br />
27. Kilic N, Oktay H. Effects <strong>of</strong> rapid maxillary expansion on nasal<br />
breathing and some naso-respiratory and breathing problems in growing<br />
children: a literature review. Int J Pediatr Otorhinolaryngol. 2008;<br />
72(11): 1595-1601.<br />
28. Oliveira de Felippe NL, Da Silveira AC, Viana G, Kusnoto B, Smith<br />
B, Evans CA. Relationship between rapid maxillary expansion and<br />
nasal cavity size and airway resistance: short- and long-term effects.<br />
Am J Orthod Dent<strong>of</strong>ac Orthop. 2008; 134(93): 370-382.<br />
29. Greulich WW, Pyle SI. Radiographic Atlas <strong>of</strong> Skeletal Development<br />
<strong>of</strong> the Hand and Wrist. 2nd ed. Stanford, CA: Stanford University<br />
Press; 1959.<br />
30. Katona TR. An engineering analysis <strong>of</strong> dental occlusion principles.<br />
Am J Orthod Dent<strong>of</strong>ac Orthop. 2009; 135(6): 696.<br />
31. Simontacchi-Gbologah MS, Tamburrino RK, Boucher NS, Vanarsdall<br />
RL, Secchi AG. Comparison <strong>of</strong> Three Methods to Analyze<br />
the Skeletal Transverse Dimension in Orthodontic Diagnosis [thesis].<br />
University <strong>of</strong> Pennsylvania; <strong>2010</strong>.<br />
For complete contributor information, please see next page.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
19
Contributors<br />
Ryan K. Tamburrino, DMD<br />
■ Clinical Associate—Univ. <strong>of</strong> Penn., School <strong>of</strong> Dental Medicine,<br />
Dept. <strong>of</strong> Orthodontics<br />
■ Andrews Foundation “Six Elements Philosophy” Course—2007<br />
■ Advanced Education in Orthodontics—<strong>Roth</strong>-<strong>Williams</strong> Center<br />
for Functional Occlusion—2008<br />
■ University <strong>of</strong> Pennsylvania, School <strong>of</strong> Dental Medicine,<br />
Certificate in Orthodontics—2008<br />
■ University <strong>of</strong> Pennsylvania, School <strong>of</strong> Dental Medicine, DMD<br />
—2006<br />
Normand S. Boucher, DDS<br />
■ McGill University, School <strong>of</strong> Dental Medicine, DMD, 1974<br />
■ University <strong>of</strong> Pennsylvania, School <strong>of</strong> Dental Medicine,<br />
Certificates in Orthodontics and Periodontics, 1982<br />
■ Advanced Education in Orthodontics, <strong>Roth</strong>-<strong>Williams</strong> Center<br />
for Functional Occlusion, 1993<br />
■ Andrews Foundation, “Six Elements Philosophy” Course, 1998<br />
■ Clinical Associate Pr<strong>of</strong>essor, University <strong>of</strong> Pennsylvania, School<br />
<strong>of</strong> Dental Medicine, Department <strong>of</strong> Orthodontics<br />
Robert L. Vanarsdall, DDS<br />
■ Pr<strong>of</strong>essor and Chair— University <strong>of</strong> Pennsylvania School <strong>of</strong><br />
Dental Medicine, Department <strong>of</strong> Orthodontics<br />
■ DDS—Medical College <strong>of</strong> Virginia<br />
■ Certificates in Orthodontics and Periodontics—University <strong>of</strong><br />
Pennsylvania<br />
■ 80 publications and 11 textbook contributions<br />
■ Former President <strong>of</strong> the Philadelphia <strong>Society</strong> <strong>of</strong> Orthodontists<br />
and Eastern Component <strong>of</strong> the EH Angle <strong>Society</strong><br />
Antonino G. Secchi, DMD, MS<br />
■ Assistant Pr<strong>of</strong>essor <strong>of</strong> Orthodontics-Clinician Educator and<br />
Clinical Director, Dept. <strong>of</strong> Orthodontics, University <strong>of</strong> Penn.<br />
■ Andrews Foundation “Six Elements Philosophy” Course, USA,<br />
—2005<br />
■ Institute for Comprehensive Oral Diagnosis and Rehabilitation,<br />
OBI Level III—2005<br />
■ Advanced Education in Orthodontics—<strong>Roth</strong>/<strong>Williams</strong> Center<br />
for Functional Occlusion USA—2005<br />
■ University <strong>of</strong> Pennsylvania, MS in Oral Biology—2005<br />
■ University <strong>of</strong> Pennsylvania, DMD—2005<br />
■ University <strong>of</strong> Pennsylvania, Certificate in Orthodontics—2003<br />
■ University <strong>of</strong> Chile—Chile, Certificate in Occlusion, 1998<br />
■ University <strong>of</strong> Valparaiso—Chile, DDS, 1996<br />
20 Tamburrino et al | The Transverse Dimension: Diagnosis and Relevance to Functional Occlusion
Hinge Axis: The Need for Accuracy in Precision Mounting<br />
Part 2<br />
Byungtaek Choi, DDS, MS, PhD<br />
byu n G T a e K ch o i , ddS, mS, Phd<br />
joydog@unitel.co.kr<br />
■ Graduated from Seoul National<br />
University, College <strong>of</strong> Dentistry<br />
(DDS), Seoul, Korea, 1981<br />
■ Graduated from Seoul National<br />
University, College <strong>of</strong> Dentistry<br />
(MS), Seoul, Korea, 1984<br />
■ Graduated from Seoul National<br />
University, College <strong>of</strong> Dentistry<br />
(PhD), Seoul, Korea, 1990<br />
■ Private Practice, Seoul, Korea<br />
■ Chairman <strong>of</strong> Korean Foundation <strong>of</strong><br />
Gnatho-Orthodontic Research<br />
■ Director <strong>of</strong> <strong>Roth</strong> <strong>Williams</strong> Center,<br />
Korea<br />
■ Attending Pr<strong>of</strong>essor <strong>of</strong> Medical<br />
School <strong>of</strong> Hanlim University<br />
■ Attending Pr<strong>of</strong>essor at Seoul<br />
National University<br />
The Axi-Path System<br />
Many clinicians use the Panadent Axi-Path system for the<br />
following purposes: (Figure 17)<br />
• To locate the true hinge axis (THA)<br />
• To determine the sagittal anterior condylar path inclination,<br />
non-working-side sagittal lateral condylar<br />
path inclination, and the Bennett movement to<br />
select the Motion Analog Blocks<br />
• To assess the functional structural conditions <strong>of</strong> the<br />
temporomandibular joint<br />
Figure 17 Axi-Path recording: Panadent Company.<br />
The upper head frame <strong>of</strong> the Axi-Path recorder is composed<br />
<strong>of</strong> two symmetrical arms that move around a hinge<br />
joint at the center <strong>of</strong> the frame (Figure 18). The upper frame<br />
is fitted and fastened to the head by tightening the hinge with<br />
Summary<br />
This is the second part <strong>of</strong> a two-part paper discussing the need for accuracy<br />
in the mounting <strong>of</strong> dental models for orthodontic diagnosis and treatment.<br />
Part 1 discussed the accuracy differences between an arbitrary hinge axis<br />
(AHA) mounting and a true hinge axis (THA) mounting. Part 2 discusses the<br />
differences between two popular true hinge axis recording devices, the Panadent<br />
Axi-Path system and the Axiograph III system.<br />
a thumbscrew. A straight ruler can be used to make the two<br />
flag tables parallel to each other. (Figure 19).<br />
Figure 18 Head frame (upper frame).<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
21
Figure 19 Flag tables are set to be parallel to each other.<br />
The lower head frame <strong>of</strong> the Axi-Path recorder is at-<br />
tached to the lower jaw with the use <strong>of</strong> a clutch. Two side<br />
arms which hold the styli are attached to the cross rod to<br />
record the mandibular movement (Figure 20).<br />
Figure 20 Lower frame for adjustable axis-locating arms.<br />
To place the Axi-Path recorder correctly, the upper<br />
frame is first fitted and fastened to the head. The lower frame<br />
is then attached to the lower jaw. Finally, the axis-locating<br />
arms are attached to the lower jaw (Figure 21).<br />
Figure 21-a The upper frame is placed and fastened to the head.<br />
Figure 21-b Axis-locating arms are attached to the lower jaw.<br />
Figure 22 is the schematic drawing <strong>of</strong> the head viewed<br />
from the top when the Axi-Path recorder has been placed on<br />
the head correctly.<br />
22 Choi | Hinge Axis: The Need for Accuracy in Precision Mounting Part 2<br />
Figure 22 Schematic drawing <strong>of</strong> the head viewed from the<br />
top when the Axi-Path recorder has been placed on the head.<br />
Figure 23 Asymmetrical head configuration.<br />
If the patient’s head configuration is asymmetrical, the<br />
face-bow may not be centered on the head when the nasion<br />
relator is placed on Nasion (Figure 23). Since the nasion relator<br />
cannot move transversely, the face-bow should be rotated<br />
until the nasion relator sits on Nasion (Figure 24). When the<br />
lower frame is placed, the stylus may not be perpendicular
to the flag table (Figure 25). The Axi-Path is not a collinear<br />
system, and errors <strong>of</strong>ten occur when the clinician attempts<br />
to determine the THA. If a recording system is not collinear<br />
and rectilinear, the clinician is likely to mark the inaccurate<br />
hinge points on the skin.<br />
Figure 24 Nasion relator cannot<br />
move along the horizontal part <strong>of</strong> the bow.<br />
Figure 25 When the lower frame is placed, the<br />
stylus may not be perpendicular to the flag table.<br />
The following experiment can be used to determine the<br />
magnitude <strong>of</strong> measurement error. The experiment is set up so<br />
that the measurement shows the right condyle 5 mm forward<br />
<strong>of</strong> its actual position. For purposes <strong>of</strong> illustration, the situation<br />
is assumed to be noncollinear (Figure 26).<br />
Figure 26 Supposition. Right condyle moved 5 mm forward.<br />
The new hinge axis diverges from the original hinge axis<br />
as it goes farther from the anatomic structure (Figure 27).<br />
Figure 27 New hinge axis passing through<br />
newly positioned condyle.<br />
The right recording stylus is placed at the new hinge<br />
point on the flag table (Figure 28).<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
23
Figure 28 Stylus placed at the new<br />
hinge point on the flag table.<br />
A hinge axis is not a line that connects the centers <strong>of</strong> the<br />
condyles. It is the axis around which the mandible shows<br />
pure hinge movement. Therefore, the hinge axis may pass<br />
through any point in the condyle. In Figure 29, the center<br />
points have been marked for clarity. Figure 30 is a magnified<br />
view <strong>of</strong> the right joint area.<br />
Figure 29<br />
Right condyle 5 mm<br />
anterior to the left<br />
condyle.<br />
Figure 30 Magnified view <strong>of</strong> the right joint area.<br />
24 Choi | Hinge Axis: The Need for Accuracy in Precision Mounting Part 2<br />
The example assumes that the distance between the<br />
centers <strong>of</strong> the two condyles is 110 mm, and the distance at<br />
skin level is 140 mm (Figure 31). If the condyle moves 5 mm<br />
forward, it will appear to move slightly more on the graph<br />
(Figure 32). If the condyle moves 5 mm forward, the hinge<br />
point on the skin moves 5.68 mm forward (Figure 33).<br />
Figure 31 The supposition is that the distance<br />
between the centers <strong>of</strong> the two condyles is 110 mm,<br />
and the distance at the skin level is 140 mm.<br />
Figure 32 If the condyle moves 5 mm forward,<br />
it will appear to move slightly more on the graph.<br />
Figure 33 If the condyle moves 5 mm forward,<br />
the hinge point on the skin moves 5.68 mm forward.
The Axi-Path is designed so that the flag table is very<br />
close to the preauricular skin. For some patients, depending<br />
on the configuration <strong>of</strong> the temporal region, the flag table<br />
may be farther from the skin. Figure 34 shows 5 mm <strong>of</strong> distance<br />
between the skin and the flag table.<br />
Figure 34 Axi-Path is designed so that the flag table is<br />
very close to the preauricular skin. This picture shows<br />
5 mm <strong>of</strong> distance between the skin and the flag table.<br />
If the distance from where the stylus contacts the flag<br />
table to the skin is 5 mm, the measurement error will be 0.23<br />
mm. The amount <strong>of</strong> error will decrease as the stylus gets<br />
closer to the skin. The Axi-Path system uses the skin mark<br />
for face-bow transfer. Hence, the smaller the error, the more<br />
accurate the hinge axis. Accuracy depends on the distance<br />
between the flag table and the skin (Figure 35).<br />
Figure 35 If the distance from the stylus to the skin is 5 mm,<br />
the amount <strong>of</strong> error is calculated as follows:<br />
5.68 : 125 = X : 5 mm (X = 284 ÷ 125 = 0.23 mm)<br />
The Axi-Path system has some advantages. Because the<br />
flag table is very close to the skin, measurement error can be<br />
minimized (Figure 36). And the reference tattoo on the skin<br />
can be used for precision mounting at any time, once it has<br />
been marked (Figure37).<br />
Figure 36 Advantages <strong>of</strong> Axi-Path system:<br />
Proximity <strong>of</strong> the flag table to the skin.<br />
Figure 37 Advantages <strong>of</strong> Axi-Path system:<br />
Proximity <strong>of</strong> the flag table to the skin.<br />
However, the Axi-Path system also has shortcomings.<br />
The head frame <strong>of</strong>ten cannot be fastened tightly to the head.<br />
It is somewhat unstable compared to the frame <strong>of</strong> the Axiograph<br />
III. An unstable frame can make it difficult or impossible<br />
to get a reproducible reference point and may be<br />
misdiagnosed as an unstable joint (Figure 38).<br />
Figure 38 Shortcomings <strong>of</strong> Axi-Path system:<br />
Unstable head frame.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
25
Since the nasion relator is not movable transversely on<br />
the face-bow, it is difficult to center the midline <strong>of</strong> the bow<br />
perpendicular to the hinge axis in asymmetrical cases. If we<br />
attempt to do so, the face-bow will be seated <strong>of</strong>f center (Figure<br />
39).<br />
Figure 39 Shortcomings <strong>of</strong> Axi-Path system:<br />
Off-center placement <strong>of</strong> the upper frame in asymmetrical cases.<br />
In short, the Axi-Path system records the hinge axis on a<br />
flag table that is relatively close to the skin. If the flag table is<br />
close to the skin, it produces a more accurate hinge mark on<br />
the skin. However, the primary disadvantages <strong>of</strong> this system<br />
are the structural instability <strong>of</strong> the head frame when fastened<br />
to the head and the <strong>of</strong>f-centered seating <strong>of</strong> the face-bow on<br />
the asymmetrical head.<br />
26 Choi | Hinge Axis: The Need for Accuracy in Precision Mounting Part 2<br />
The Axiograph III System<br />
The Axiograph III system is shown in Figure 41. Orthodontists<br />
use this system for the same purposes as the Axi-Path<br />
system. The Axiograph III system differs from the Axi-Path<br />
system in several important ways.<br />
Figure 41 Axiograph III: SAM.<br />
Figure 42 is a schematic drawing <strong>of</strong> the head viewed<br />
from the top when the upper frame <strong>of</strong> the Axiograph III has<br />
been placed on the head correctly. If the patient’s head is<br />
symmetrical, every part <strong>of</strong> the frame will be parallel or perpendicular<br />
to the sagittal plane <strong>of</strong> the head.<br />
Figure 42 Schematic drawing and real picture <strong>of</strong> upper frame.<br />
This system is collinear and rectilinear. Since the nasion<br />
relator moves transversely, the upper frame can be placed<br />
on the head without losing the parallelism, even when the<br />
patient’s head is asymmetrical (Figure 43).<br />
Figure 44 shows the upper and lower frames placed on<br />
the head. The lower frame has two side arms, with a stylus<br />
on the end <strong>of</strong> each arm. The two styli are in collinear alignment,<br />
rectilinear with the upper Axiomatic flag-bow recording<br />
plates (Figure 45).
Figure 43 Nasion relator moves transversely along<br />
the horizontal part <strong>of</strong> frame so the frame can be<br />
placed on the head without losing parallelism.<br />
Figure 44 Upper and lower frames<br />
that have been placed on the head.<br />
Figure 45 Axiograph III uses two recording styli in a<br />
collinear alignment, rectilinear with the upper<br />
Axiomatic flag-bow recording plates.<br />
The upper frame is fastened to the head first, and the<br />
lower frame is placed next. If earplugs are inserted into the<br />
auditory canals, the alignment pins automatically indicate<br />
the approximate hinge positions. The alignment pins also<br />
make the upper and lower parts <strong>of</strong> the face-bow parallel and<br />
perpendicular to each other (Figure 46).<br />
Figure 46 If ear plugs are inserted into auditory canals,<br />
alignment pins automatically indicate approximate hinge<br />
positions. The alignment pins also make the upper and lower<br />
parts <strong>of</strong> the face-bow parallel and perpendicular to each other.<br />
As was done in the Axi-Path experiment, the amount <strong>of</strong><br />
measurement error is then determined when the right condyle<br />
is moved 5 mm forward (Figure 47). This movement<br />
produces a new hinge axis, which in turn makes new hinge<br />
points on the skin. The new hinge axis diverges from the<br />
original hinge axis as it moves farther from the anatomic<br />
structure (Figure 48).<br />
Figure 47 Supposition: Right condyle moved 5 mm forward.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
27
Figure 48 New hinge axis passing<br />
through newly positioned condyle.<br />
Figure 49 is a magnified view <strong>of</strong> the right joint area.<br />
Right condyle 5 mm<br />
anterior to the left<br />
condyle.<br />
Figure 49 The supposition is that the distance between<br />
the centers <strong>of</strong> the two condyles is 110 mm, and the<br />
distance at the skin level is 140 mm.<br />
The example assumes that the distance between the cen-<br />
ters <strong>of</strong> the two condyles is 110 mm, and that the distance at<br />
skin level is 140 mm. If the condyle moves 5 mm forward, it<br />
will appear to move slightly more on the graph (Figure 50).<br />
The recording stylus will point to the new hinge on the<br />
flag table (Figure 51).<br />
If the condyle moves 5 mm forward, the hinge point on<br />
the skin will move 5.68 mm forward (Figure 52).<br />
28 Choi | Hinge Axis: The Need for Accuracy in Precision Mounting Part 2<br />
Figure 50 If the condyle moves 5 mm forward,<br />
it will appear to move slightly more on the graph.<br />
Figure 51 The recording styli will point<br />
to the new hinge on the flag table.<br />
Figure 52 IIf the condyle moves 5 mm forward,<br />
the hinge point on the skin will move 5.68 forward.<br />
The distance between the skin and the graph table<br />
is usually greater in Axiograph III than in Axi-Path.<br />
Taking this into account, the distance between the<br />
skin and the graph was set at 8 mm in Axiograph III,<br />
instead <strong>of</strong> 5 mm, as in Axi-Path.
The distance between the preauricular skin and the flag<br />
table is usually greater in the Axiograph III than it is in the<br />
Axi-Path. Taking this into account, the distance between the<br />
skin and the flag table was set at 8 mm in the Axiograph III.<br />
When the flag table is 8 mm away from the skin, the measurement<br />
error will be 0.36 mm. This is 0.13 mm larger than<br />
the 0.23 mm measurement error with the Axi-Path, which<br />
has the flag table 5 mm away from the skin (Figure 53).<br />
Figure 53 If the distance from the stylus to the skin is 8 mm,<br />
the amount <strong>of</strong> error will be calculated as follows:<br />
5.68 : 125 = X : 8 mm (X = 45.4 ÷ 125 = 0.36 mm)<br />
If we were to transfer the face-bow <strong>of</strong> the Axiograph III<br />
system in the same way as we transfer the face-bow <strong>of</strong> the<br />
Axi-Path system, we would have to shorten the distance between<br />
the skin and the flag table to reduce the measurement<br />
error. However, in the Axiograph III system we use hinge<br />
marks on the graph, rather than hinge marks on the skin, for<br />
precision mounting.<br />
Now let us further suppose that the stylus is placed 50<br />
mm, rather than 8 mm, away from the skin (Figure 54).<br />
Figure 54 Supposition: The stylus is 50 mm away from the skin.<br />
Although this situation is one that we may not encoun-<br />
ter in practice, it is useful as an example to explain an extreme<br />
case (Figure 55).<br />
Figure 55 Magnified view.<br />
It is obvious that the measurement error becomes larger<br />
when the distance from the stylus to the skin is 50 mm (Figure<br />
56). In fact, the measurement error will be 2.3 mm (Figure 57).<br />
Figure 56 The measurement error becomes larger<br />
when the distance from the stylus to the skin<br />
changes from 8 mm to 50 mm.<br />
Figure 57 If the distance from the stylus to the skin<br />
is 50 mm, the amount <strong>of</strong> error will be calculated as follows:<br />
5.6 8: 125 = X : 50 mm (X = 284 ÷ 125 = 2.3 mm)<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
29
This is an extremely large error when we are attempting<br />
to locate a THA. Fortunately, it seldom happens that we attempt<br />
to locate a THA from a distance <strong>of</strong> 50 mm in clinical<br />
practice (Figure 58).<br />
Figure 58 If we try to extend the stylus to the skin to mark a<br />
hinge point from a point located at a far distance from the<br />
skin using Axiograph III, it would result in a very large error.<br />
The fact remains, however, that the greater the distance<br />
between the skin and the stylus, the less accurate are the<br />
marks on the skin (Figure 59). Therefore, we are likely to<br />
make a large error if we use a false hinge axis that deviates<br />
substantially from the THA (Figure 60).<br />
Figure 59 The greater the distance between the skin<br />
and the stylus, the less accurate the marks <strong>of</strong><br />
the THA on the skin will be.<br />
Precision mounting<br />
using a false hinge<br />
axis results in a very<br />
large error.<br />
Figure 60 We are likely to create a large error if we use the<br />
false hinge axis, which deviates substantially from the THA.<br />
30 Choi | Hinge Axis: The Need for Accuracy in Precision Mounting Part 2<br />
Next, let us examine the precision mounting system <strong>of</strong><br />
the Axiograph III. Figure 61 shows a magnified view <strong>of</strong> the<br />
highlighted area. The various parts <strong>of</strong> the highlighted area<br />
are shown in Figure 62. They are, respectively, the side arm<br />
<strong>of</strong> the upper frame, the flag table attached to the side arm,<br />
the recording arm <strong>of</strong> the lower frame, and the stylus attached<br />
to the recording arm.<br />
Figure 61 Schematic drawing and<br />
real picture <strong>of</strong> the stylus area.<br />
Figure 62 Magnified view<br />
The THA is the line that connects the left and the right<br />
styli. It passes through an imaginary hole in the flag table.<br />
The stylus marks the hinge point in red or blue on the graph<br />
<strong>of</strong> the flag table (Figures 63 and 64).
Figure 63 Flag table.<br />
Figure 64 Flag table.<br />
The hinge point on the graph is isolated with the hinge<br />
axis clamp. The hinge axis clamp has two bars. Each bar has<br />
a hole in it, and the two holes are aligned (Figures 65 and<br />
66).<br />
Figure 65 Flag table with hinge axis clamp.<br />
Figure 66 Schematic drawing and real<br />
picture <strong>of</strong> the flag table and the clamp.<br />
The precision mounting stand has two hinge axis align-<br />
ment pins. These pins are designed to fit into the small holes<br />
on the inner bar <strong>of</strong> the hinge axis clamp (Figures 67-a, b).<br />
Figure 67-a Hinge axis alignment pin<br />
fits into the inner clamp hole.<br />
Figure 67-b Hinge axis alignment belongs to mounting stand.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
31
In this respect, the Axiograph III system differs from<br />
the Axi-Path system; in the Axi-Path, the stylus <strong>of</strong> the lower<br />
frame fits into the female part <strong>of</strong> the mounting shaft. Therefore,<br />
we do not need to re-mark the hinge point on the skin<br />
with the Axiograph III as we do with the Axi-Path. Instead,<br />
we use the hinge points on the graphs for precision mounting.<br />
In other words, we treat the graph as if it were the skin<br />
in the Axiograph III system (Figure 68).<br />
Figure 68 In Axi-Path, the stylus (axis pin) <strong>of</strong> the lower frame<br />
is adapted to the female part <strong>of</strong> the mounting shaft. In<br />
Axiograph III, the hinge axis alignment pins <strong>of</strong> the mounting<br />
stand are fitted into the small holes on the inner bar <strong>of</strong> the<br />
hinge axis clamp. Therefore, we need not re-mark the hinge<br />
point on the skin, as we do with Axi-Path. Instead, we use<br />
the hinge points on the graphs for precision mounting.<br />
The distance from the tip <strong>of</strong> the hinge axis alignment<br />
pin to the THA is the measurement error (Figure 69). It is interesting<br />
to observe that the measurement error increases as<br />
the flag table moves closer to the skin medially (Figure 70).<br />
Conversely, the measurement error decreases as the flag table<br />
moves farther from the skin laterally (Figure 71).<br />
Figure 69 The distance from the tip <strong>of</strong> the hinge axis<br />
alignment pin to the THA is the measurement error.<br />
32 Choi | Hinge Axis: The Need for Accuracy in Precision Mounting Part 2<br />
Figure 70 Measurement error increases as the<br />
flag table moves closer to the skin medially.<br />
Figure 71 Measurement error decreases as the<br />
flag table moves farther from the skin laterally.<br />
If we try to extend the hinge axis-locating stylus from<br />
the flag to the skin to mark an axis as we do in the Axi-Path<br />
system, the new hinge point on the skin will not correspond<br />
to the true hinge point. As a result, the precision mounting<br />
will be inaccurate. In the Axiograph III system, the measurement<br />
error decreases as the flag table gets farther away from<br />
the skin and the constructed hinge axis gets closer to the<br />
THA (Figure 72).<br />
Now let us consider two situations that we may encounter<br />
in clinical practice. In the first situation, the side arm <strong>of</strong><br />
the upper frame contacts the skin <strong>of</strong> supraauricular area<br />
(Figure 73). The side arm is 6 mm wide and the flag table is<br />
4.5 mm thick.<br />
In the second situation, there may be some distance between<br />
the condyle and the recording flag, depending on the<br />
configuration <strong>of</strong> the patient’s head. For the purposes <strong>of</strong> illustration,<br />
we will assume that the side arm is 3 mm away from
Figure 72<br />
Figure 73 Supposition: The side arm contacts the skin.<br />
Figure 74 Supposition: The side arm is separated<br />
3 mm from the skin. The hinge point is measured<br />
at level <strong>of</strong> entrance <strong>of</strong> the clamp hole.<br />
the skin. In fact, this does not actually happen in clinical<br />
practice, because we always push the side arm onto the skin<br />
to fasten the upper frame to the head. If, however, we assume<br />
3 mm <strong>of</strong> separation, this means that the flag table will be 6.5<br />
mm away from the skin, and the hinge point locator clamp<br />
will be attached to the flag table (Figure 74).<br />
In this example (Figure 74) the thickness <strong>of</strong> the hinge<br />
axis clamp is 5.75 mm; the distance from the skin to the<br />
inner surface <strong>of</strong> the flag table is 6.5 mm; the distance from<br />
the skin to the outer surface <strong>of</strong> the flag table is 11 mm; the<br />
distance from the left condyle to the skin on the right side <strong>of</strong><br />
is 110 + 15 mm; and the distance from the left condyle to the<br />
inner surface <strong>of</strong> the flag table is 110 + 15 + 6.5 mm. This is<br />
indicated by the yellow arrow.<br />
The measurement error at the position indicated by the<br />
arrow is calculated as follows:<br />
•<br />
Y is the measurement error on the inner surface <strong>of</strong> the<br />
flag table. The amount <strong>of</strong> error is 0.20 mm (Figure 75).<br />
Figure 75 Y is the measurement error on the inner surface<br />
<strong>of</strong> the flag table. The amount is 0.20 mm.<br />
•<br />
The measurement error at the inner entrance <strong>of</strong> the<br />
hinge axis clamp increases slightly (Figure 76).<br />
Figure 76 Supposition: The side arm is separated 3 mm<br />
from the skin. The hinge point is measured at<br />
level <strong>of</strong> entrance <strong>of</strong> the clamp hole.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
33
•<br />
•<br />
•<br />
•<br />
The measurement error at the inner entrance is 0.47<br />
mm (Figure 77).<br />
Figure 77 The amount <strong>of</strong> measurement error will be 0.47 mm.<br />
The measurement error on the skin increases even<br />
more (Figure 78).<br />
Figure 78 Supposition: The side arm is separated 3 mm<br />
from the skin. The hinge point is measured at<br />
level <strong>of</strong> entrance <strong>of</strong> the clamp hole.<br />
The measurement error on the skin is 0.5 mm<br />
(Figure 79).<br />
Figure 79 The amount <strong>of</strong> measurement error will be 0.5 mm.<br />
34 Choi | Hinge Axis: The Need for Accuracy in Precision Mounting Part 2<br />
•<br />
The measurement error on the inner surface <strong>of</strong> the<br />
flag table is 0.20 mm and this is almost the same as<br />
or smaller than that <strong>of</strong> Axi-Path.<br />
Although the clamp hole provides a bit <strong>of</strong> leeway with<br />
the pin fitted, this seems to have no clinical significance. Since<br />
the Axiograph III system uses the hinge point on the graph,<br />
while the Axi-Path system uses the hinge mark on the skin,<br />
the two systems seem to yield almost the same accuracy in<br />
precision mounting (Figure 80).<br />
Figure 80 The measurement error on the inner surface<br />
<strong>of</strong> the flag table is 0.20 mm. Error is the same as,<br />
or less than, with Axi-Path.<br />
Summary and Conclusions<br />
The measurement errors <strong>of</strong> the hinge axis locations were<br />
calculated for the two recording systems, the Axi-Path <strong>of</strong><br />
Panadent and the Axiograph III <strong>of</strong> SAM. The amount <strong>of</strong><br />
the measurement errors were nearly the same for both systems.<br />
While the Axiograph III system locates the hinge axis<br />
using hinge points on the flag table, the Axi-Path system<br />
locates the hinge axis using hinge marks on the skin. Although<br />
the distance between the flag table and the skin is<br />
greater in the Axiograph, we found no significant difference<br />
in accuracy between the two systems, as explained<br />
previously. (Figure 83)
Figure 83 The distance between the flag table and the skin is longer in Axiograph III than in Axi-Path.<br />
But since Axiograph III uses hinge points on graph paper to locate the hinge axis, it is equally accurate.<br />
Since the Axiograph III system does not mark hinge<br />
points on the skin, it may be necessary to relocate the axes<br />
for each mounting. Mechanical stability <strong>of</strong> the recording device<br />
is very important for precision. The device must remain<br />
firmly seated on the head. In this respect, the Axiograph III<br />
seems to be superior to the Axi-Path (Figure 85). ■<br />
Figure 85 Mechanical stability <strong>of</strong> the recording device is very important for precision.<br />
In this respect Axiograph III seems to be superior to Axi-Path.<br />
Further Reading<br />
Baldauf A, Mack H, Wirth C G. Bestommung der Scharnierachse mittels<br />
des äußeren Gehörgangs. IOK, 28. JAHRG. 1996.<br />
Broderson S P. Anterior guidance: The key to successful occlusal treatment.<br />
J Prosthet Dent. 1978;39:396–400.<br />
Cho Y, Hobo S, Takahashi H.Occlusion. Seoul: Kunja; 1996.<br />
Dawson P E. Evaluation, Diagnosis, and Treatment <strong>of</strong> Occlusal Problems.<br />
2nd ed. St. Louis, Mo: Mosby; 1989.<br />
Glossary <strong>of</strong> Dental Prosthodontics. Korea: Korean Association <strong>of</strong><br />
Prosthodontics; 2006.<br />
Hobo S. Twin-tables technique for occlusal rehabilitation. Pt. 1:<br />
Mechanism <strong>of</strong> anterior guidance. J Prosthet Dent. 1991;66:299–303.<br />
Hobo S. Twin-tables technique for occlusal rehabilitation. Pt. 2: Clinical<br />
procedures. J Prosthet Dent. 1991;66:471–477.<br />
Lee R L. Panadent instruction manual for advanced articulator system.<br />
Panadent Corporation, CA, USA, 1988.<br />
Lundeen H C, Gibbs C H. The Function <strong>of</strong> Teeth. L and G; 2005.<br />
Nagy W W, Smithy T J, Wirth C G. Accuracy <strong>of</strong> a predetermined transverse<br />
horizontal mandibular axis point. J Prosthet Dent. 2002;87:387–<br />
394.<br />
Okeson J P. Fundamentals <strong>of</strong> Occlusion and Temporomandibular<br />
Disorders. St. Louis, Mo: Mosby; 1985.<br />
continued on next page...<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
35
Ramfjord S, Ash M M. Occlusion. 3rd ed. Philadelphia: WB Saunders;<br />
1983.<br />
Simpson J W, Hesby R A, Pfeifer D L, Pelleu G B Jr. Arbitrary mandibular<br />
hinge axis locations. J Prosthet Dent. 1984;51:819–822.<br />
Takahashi I. Surgical-orthodontic treatment <strong>of</strong> a patient with temporomandibular<br />
disorder stabilized with a gnathologic splint. Am J Orthod<br />
Dent<strong>of</strong>acial Orthop. 2008;133: 909–919.<br />
Theusner J, Plesh O, Curtis D A, Hutton J E. Axiographic tracings <strong>of</strong><br />
temporomandibular joint movements. J Prosthet Dent. 1993;69:209–<br />
215.<br />
Wirth C G. 20 Jahre Axiographie. IOK, 28. JAHRG. 1996.<br />
36<br />
Choi | Hinge Axis: The Need for Accuracy in Precision Mounting Part 2
Condylar Resorption, Matrix Metalloproteinases,<br />
and Tetracyclines<br />
Michael J. Gunson, DDS, MD ■ G. William Arnett, DDS, FACD<br />
mic h a e L J. Gu n S o n , ddS, md<br />
gunson@arnettgunson.com<br />
■ Graduated from UCLA School <strong>of</strong><br />
Dentistry, 1997<br />
■ Graduated from UCLA School <strong>of</strong><br />
Medicine 2000<br />
■ Specialty Certificate in Oral and<br />
Maxill<strong>of</strong>acial Surgery UCLA, 2003<br />
G. Wi L L i a m aR n e T T , ddS, Facd<br />
■ Graduated from USC School <strong>of</strong><br />
Dentistry, 1972<br />
■ Specialty Certificate in Oral and<br />
Maxill<strong>of</strong>acial Surgery UCLA, 1975<br />
Introduction<br />
Orthodontists and maxill<strong>of</strong>acial surgeons are well acquainted<br />
with the effects <strong>of</strong> condylar resorption (Figure 1).<br />
Figure 1 Tomograms reconstructed from cone-beam CT scan.<br />
They show severe condylar resorption in a 19-year-old female<br />
over a 2-year period. Note the progressive osseous destruction.<br />
The clinical outcomes <strong>of</strong> condylar resorption have been described<br />
at length in the literature. 1-6 The causes, however,<br />
have been elusive, hence the common name idiopathic condylar<br />
resorption. Over the last several years, the pathophysiology<br />
<strong>of</strong> articular bone erosion secondary to inflammation<br />
Summary<br />
Mandibular condylar resorption occurs as a result <strong>of</strong> inflammation and hormone<br />
imbalance. The cause <strong>of</strong> the bone loss at the cellular level is secondary<br />
to the production <strong>of</strong> matrix metalloproteinases (MMPs). MMPs have been<br />
shown to be present in diseased temporomandibular joints (TMJs). There is<br />
evidence that tetracyclines help control bone erosions in arthritic joints by<br />
inactivating MMPs. This article reviews the pertinent literature in support <strong>of</strong><br />
using tetracyclines to prevent mandibular condylar resorption.<br />
has been well studied. A number <strong>of</strong> cytokines and proteases<br />
are found in joints that show osseous erosions that are not<br />
present in healthy joints, namely TNF-α, IL-1β, IL-6, and<br />
RANKL and matrix metalloproteinases.<br />
Matrix Metalloproteinases<br />
MMPs are <strong>of</strong> interest because they are directly responsible<br />
for the enzymatic destruction <strong>of</strong> extracellular matrix in normal<br />
conditions (angiogenesis, morphogenesis, tissue repair)<br />
and in pathological conditions (arthritis, metastasis, cirrhosis,<br />
endometriosis). MMPs are endopeptidases that are made<br />
in the nucleus as inactive enzymes, or zymogens. The zymogens<br />
travel to the cell membrane, where they are incorporated.<br />
The zymogen is then cleaved into the extracellular matrix<br />
as the active enzyme, where it makes cuts into the protein<br />
chains (collagen types I through IV, gelatin, etc). These cuts<br />
cause the proteins to denature, which results in the destruction<br />
<strong>of</strong> the matrix. The action <strong>of</strong> the MMP requires the mineral<br />
zinc—which is an important part <strong>of</strong> the MMP’s protein<br />
structure; hence the name metalloproteinase (Figure 2).<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
37
Figure 2 The zymogen pro-MMP is transcribed in the nucleus<br />
and then attached to the cell membrane. It is activated when<br />
it is cleaved from the membrane. The zinc (Zn) portion binds<br />
to protein and the enzyme cleaves the protein, destroying the<br />
extracellular matrix.<br />
In joints, MMPs are produced by monocytes, mac-<br />
rophages, polymorphonuclear neutrophils, synoviocytes, osteoblasts,<br />
and osteoclasts. MMPs are generally classified by<br />
the kind <strong>of</strong> matrix they degrade; thus collagenase, gelatinase<br />
and stromelysin (Figure 3).<br />
Figure 3 A list <strong>of</strong> the 28 known MMPs. They are generally<br />
named after the extracellular protein that they degrade.<br />
The extracellular activity <strong>of</strong> MMPs is regulated in two<br />
ways, by transcription and by extracellular inhibition. The<br />
transcription <strong>of</strong> MMPs in the nucleus is controlled by multiple<br />
pathways. MMP transcription is activated by sheer stress<br />
to the cell, by free radicals, and by the cytokines TNF-α, IL-<br />
1β, Il-6 and RANKL (Figure 4a). Transcription is suppressed<br />
by the cytokine osteoprotegerin and by the the hormones<br />
vitamin D and estradiol (Figure 4b). After transcription, the<br />
pro-MMP is then sent to the cell membrane, where it is incor-<br />
38 Gunson, Arnett | Condylar Resorption, Matrix Metalloproteinases, and Tetracyclines<br />
porated. Activation <strong>of</strong> the MMP occurs when the active side<br />
<strong>of</strong> the MMP is cleaved from the cell and liberated into the extracellular<br />
matrix. Extracellular inhibition comes from proteins<br />
called tissue inhibitors <strong>of</strong> metalloproteinases (TIMPs).<br />
TIMPs bind to active matrix metalloproteinases and inhibit<br />
their activity (Figure 4c). The ratio <strong>of</strong> MMP:TIMP activity<br />
influences the amount <strong>of</strong> matrix degradation. 7-10<br />
Figure 4-a MMP transcription is activated in the cell nucleus by<br />
cytokines (TNF-α, IL-1β, Il-6, and RANKL); by metabolic<br />
by-products (free radicals); and by direct sheer stress<br />
to the cell membrane.<br />
Figure 4-b MMP transcription is inhibited by hormones such<br />
as vitamin D and estradiol, as well as the bone-protective<br />
cytokine osteoprotegerin.
Figure 4-c The extracellular activity <strong>of</strong> MMPs is controlled by the<br />
presence <strong>of</strong> inhibitory proteins called tissue inhibitors <strong>of</strong><br />
metalloproteinases, or TIMPs. TIMPs bind directly to the<br />
MMPs, causing conformational changes that prevent the<br />
destruction <strong>of</strong> matrix proteins.<br />
MMPs and Arthritis<br />
The hallmark sign <strong>of</strong> arthritis is articular bone loss. In the<br />
past, clinicians have differentiated between inflammatory arthritis<br />
and osteoarthritis (OA). Recently, however, the cellular<br />
processes that result in bone and cartilage loss in both forms<br />
<strong>of</strong> arthritis have been shown to be quite similar. 11 While inflammatory<br />
arthritis is promoted by a systemic problem, the<br />
result is an inflammatory cytokine cascade, which ultimately<br />
results in osteoclastic activity and bone loss at the articular<br />
surface. OA is not a systemic problem but a local one, secondary<br />
to oxidation reactions, free radical production, or sheer<br />
stress—all three <strong>of</strong> which result from overuse. 12, 13 Despite<br />
the localized nature <strong>of</strong> OA, the cascade <strong>of</strong> cellular events that<br />
cause articular surface loss is the same as the systemically induced<br />
cascade. An increase in TNF-α and IL-1β increases the<br />
number <strong>of</strong> osteoclasts and their activity. TNF-α, IL-1β, IL-<br />
6, and RANKL all cause increased expression <strong>of</strong> the MMP<br />
genes. The end result is destruction <strong>of</strong> cartilage, bone, and<br />
connective tissue in both arthritis models. 14-18<br />
MMPs also respond to systemic hormones such as estrogen,<br />
vitamin D, and parathyroid hormones. We found an association<br />
between low estrogen levels and low vitamin D levels<br />
in patients with severe condylar resorption. 3 All <strong>of</strong> these<br />
hormones and cytokines are intimately involved in osteoclast<br />
differentiation and activation. This makes sense: MMPs are<br />
osteoclast produced and are responsible for bone and cartilage<br />
destruction.<br />
MMPs and the TMJ<br />
There is substantial evidence indicating that MMPs play an<br />
important role in bone and cartilage degradation associated<br />
with degenerative temporomandibular joint (TMJ) arthriti-<br />
des. This evidence supports the presence <strong>of</strong> 6 <strong>of</strong> the known<br />
28 matrix metalloproteinases (MMP-1, MMP-2, MMP-3,<br />
MMP-8, MMP-9, and MMP-13) in fluid or tissue samples<br />
obtained from diseased human TMJs. 13, 16, 17, 19-34 Some cases<br />
<strong>of</strong> degenerative joint disease also result from an imbalance<br />
between the activities <strong>of</strong> MMPs and TIMPs, favoring unreg-<br />
35, 36<br />
ulated degradation <strong>of</strong> tissue by MMPs.<br />
Tetracyclines<br />
Because MMPs are found to be elevated in patients with<br />
TMJ arthritis and are so destructive to articular tissues, finding<br />
a way to reduce their activity or their production would<br />
be helpful in treating patients with arthritis and condylar<br />
resorption.<br />
From 1972-1982, at the School <strong>of</strong> Dental Medicine in<br />
Stony Brook New York, Ramurmathy and Golub discovered<br />
that tetracyclines have anti-collagenolytic properties.<br />
In 1998, Golub and colleagues showed that tetracyclines<br />
inhibit bone resorption in two ways—by controlling the expression<br />
and activity <strong>of</strong> MMPs and by regulating osteoclasts<br />
and their activity. 37<br />
Controlling MMPs With Tetracyclines<br />
Tetracyclines inhibit MMPs by chelating zinc and by regulating<br />
MMP gene expression. As noted above, MMPs need<br />
zinc to actively cleave collagen proteins. Tetracyclines bind<br />
divalent ions, such as zinc. By reducing the amount <strong>of</strong> free<br />
zinc in tissues, tetracyclines reduce the number <strong>of</strong> MMPs<br />
available. 38 In addition, tetracyclines bind to the MMP itself,<br />
which causes a conformational change in the enzyme, inactivating<br />
it (Figure 5). 39 Tetracyclines have also been shown to<br />
decrease the transcription <strong>of</strong> MMPs by blocking both pro-<br />
40, 41<br />
tein kinase C and calmodulin pathways.<br />
Figure 5 Tetracycline binds directly to the zinc <strong>of</strong> the MMP.<br />
This deactivates the enzyme and protects the matrix<br />
from degradation. Tetracycline also controls osteoclastic<br />
activity and MMP transcription.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
39
Regulating Osteoclasts With Tetracyclines<br />
Osteoclasts are responsible for the breakdown <strong>of</strong> bone and<br />
cartilage. Their activity is tightly controlled by cytokines<br />
such as IL-6, TNF-α, nitric oxide, and IL-1β. Tetracyclines<br />
have been shown to prevent the liberation <strong>of</strong> these cytokines,<br />
diminishing the activity <strong>of</strong> osteoclasts. 42-46 Tetracyclines also<br />
prevent the differentiation <strong>of</strong> osteoclast precursor cells into<br />
osteoclasts. 47 Finally, tetracyclines promote the programmed<br />
cell death (apoptosis) <strong>of</strong> osteoclasts. 48, 49 All these actions result<br />
in a decrease <strong>of</strong> bone and cartilage loss secondary to<br />
osteoclast activity when tetracyclines are present.<br />
Tetracyclines and Arthritis<br />
In short, the literature shows that tetracyclines exert control<br />
over MMP transcription and activity and regulate osteoclast<br />
activity as well. The clinical evidence supporting the use <strong>of</strong><br />
tetracyclines to protect articular bone and cartilage from arthritic<br />
inflammation is encouraging.<br />
In the animal model <strong>of</strong> arthritis, tetracyclines have been<br />
shown to inhibit MMPs and to prevent the progression <strong>of</strong><br />
osseous disease. 50-52 Yu et al52 induced knee arthritis in dogs<br />
by severing the anterior cruciate ligament. Half the dogs<br />
were pretreated with doxycycline. Doxycycline prevented<br />
the full-thickness cartilage ulcerations that were seen in the<br />
untreated group.<br />
In human studies, tetracyclines have been successfully<br />
used to diminish bone erosions in patients with inflammatory<br />
arthritis. One meta-analysis <strong>of</strong> 10 clinical trials that used<br />
tetracycline for rheumatoid arthritis (RA) showed significant<br />
improvement in disease activity with no side effects. 53 In a<br />
single-blinded controlled study, doxycycline was shown to<br />
be as effective as methotrexate in treating inflammatory ar-<br />
thritis. 54<br />
Israel et al reported that doxycycline administered at a<br />
dose <strong>of</strong> 50 mg twice daily for 3 months significantly suppressed<br />
MMP activity in three patients diagnosed with advanced<br />
osteoarthritis <strong>of</strong> the TMJ. Two <strong>of</strong> the three patients<br />
reported marked improvement in symptoms, including improved<br />
mandibular range <strong>of</strong> motion. One patient did not<br />
experience symptomatic relief despite a marked reduction in<br />
MMP activity. 55 While symptomatic relief would be important,<br />
it must be noted that inhibition <strong>of</strong> MMPs has a direct<br />
effect on bony resorption, which is <strong>of</strong>ten unrelated to TMJ<br />
symptoms. Clinicians need to keep this in mind when reviewing<br />
the literature.<br />
Dosing<br />
At present, there are no definitive studies demonstrating the<br />
efficacy <strong>of</strong> tetracycline therapy for degenerative TMJ arthritides.<br />
However, based on the available information, tet-<br />
40 Gunson, Arnett | Condylar Resorption, Matrix Metalloproteinases, and Tetracyclines<br />
racyclines may be considered for the treatment <strong>of</strong> rapidly<br />
progressive condylar resorption, and in patients with degenerative<br />
TMJ disease. They may also be used in patients at increased<br />
risk for resorption. This includes patients with bruxism,<br />
inflammatory arthritis, or a past history <strong>of</strong> resorption<br />
who are undergoing occlusal treatment. Of all the available<br />
tetracyclines, Golub et al found that doxycycline was the<br />
most effective at suppressing MMP activity. 56 Appropriate<br />
studies to determine effective dose schedules have not been<br />
conducted to date. However, based on the limited clinical<br />
data, it is reasonable to consider doxycycline at a dose <strong>of</strong> 50<br />
mg twice daily.<br />
Side Effects<br />
The adverse effects <strong>of</strong> tetracyclines are well known. They<br />
include allergic reactions; gastrointestinal symptoms (ulcers,<br />
nausea, vomiting, diarrhea, Candida superinfection); photosensitivity;<br />
vestibular toxicity with vertigo and tinnitus; decreased<br />
bone growth in children; and discoloration <strong>of</strong> teeth<br />
if administered during tooth development. Tetracyclines may<br />
also reduce the effectiveness <strong>of</strong> oral contraceptives, potentiate<br />
lithium toxicity, increase digoxin availability and toxicity,<br />
and decrease prothrombin activity. 57<br />
If tetracycline therapy is initiated, the patient should be<br />
advised <strong>of</strong> the potential for reduced efficacy <strong>of</strong> oral contraception.<br />
In addition, the patient should be cautioned against<br />
sun exposure, and should be monitored for other side effects.<br />
If surgery is contemplated, the patient’s coagulation status<br />
should be evaluated.<br />
There is some question as to whether bacterial resistance<br />
may develop with the chronic use <strong>of</strong> antibiotics. Studies<br />
show that long-term low-dose doxycycline (20 mg twice<br />
daily) does not lead to a significant increase in bacterial resis-<br />
58, 59<br />
tance or to a change in fecal or vaginal flora.<br />
Other Medications to Control MMPs<br />
Tetracyclines are not the only medications that can prevent<br />
MMP-induced bone erosions. There are promising studies<br />
that show the benefits <strong>of</strong> TNF-α inhibitors; osteoprotegerin<br />
analogues; HMG-CoA reductase inhibitors (eg, simvastatin);<br />
and hormone replacement therapies, including vitamin<br />
D and estradiol. 60-63 These medications, along with doxycycline,<br />
show great promise in controlling articular bone loss<br />
in the face <strong>of</strong> inflammation.<br />
Conclusion<br />
When patients present with condylar resorption, clinicians<br />
have long been resigned to two choices: watch and wait or<br />
surgical resection with the resulting disability and deformity.<br />
Doxycycline is just one pharmacological intervention that
shows promise in curbing the bone loss associated with arthritis<br />
and condylar resorption (Figures 6-a, b, c, d, e). ■<br />
Figure 6-a, b, c, d, e This is a 31-year-old patient with condylar<br />
resorption secondary to rheumatoid arthritis. She was treated<br />
with orthognathic surgery to correct her malocclusion. The<br />
effects <strong>of</strong> MMPs were controlled pre- and postoperatively by<br />
prescribing the following medications: doxycycline, simvastatin,<br />
Enbrel, Feldene, vitamin D, and omega-3 fatty acids. She is 10<br />
months postsurgery with minimal osseous change to her condyles<br />
and a stable class I occlusion with good overbite and overjet.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
41
References<br />
1. Arnett GW, Milam SB, Gottesman L. Progressive mandibular<br />
retrusion-idiopathic condylar resorption, II. Am J Orthod Dent<strong>of</strong>ac<br />
Orthop. 1996 August;110(2):117-27.<br />
2. Arnett GW, Milam SB, Gottesman L. Progressive mandibular<br />
retrusion—idiopathic condylar resorption, I. Am J Orthod Dent<strong>of</strong>ac<br />
Orthop. 1996; 110(1):8-15.<br />
3. Gunson MJ, Arnett GW, Formby B, Falzone C, Mathur R, Alexander<br />
C. Oral contraceptive pill use and abnormal menstrual cycles in<br />
women with severe condylar resor ption: a case for low serum 17betaestradiol<br />
as a major factor in progressive condylar resorption. Am J<br />
Orthod Dent<strong>of</strong>ac Orthop. 2009;136(6):772-779.<br />
4. Wolford LM, Cardenas L. Idiopathic condylar resorption: diagnosis,<br />
treatment protocol, and outcomes. Am J Orthod Dent<strong>of</strong>ac Orthop.<br />
1999;116(6):667-677.<br />
5. Hwang SJ, Haers PE, Zimmermann A, Oechslin C, Seifert B,<br />
Sailer HF. Surgical risk factors for condylar resorption after orthognathic<br />
surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.<br />
2000;89(5):542-552.<br />
6. Hwang SJ, Haers PE, Seifert B, Sailer HF. Non-surgical risk factors<br />
for condylar resorption after orthognathic surgery. J Craniomaxill<strong>of</strong>ac<br />
Surg. 2004;32(2):103-111.<br />
7. Cambray GJ, Murphy G, Page-Thomas DP, Reynolds JJ. The<br />
production in culture <strong>of</strong> metalloproteinases and an inhibitor by joint<br />
tissues from normal rabbits, and from rabbits with a model arthritis, I:<br />
synovium. Rheumatol Int. 1981;1(1):11-16.<br />
8. Murphy G, Cambray GJ, Virani N, Page-Thomas DP, Reynolds<br />
JJ. The production in culture <strong>of</strong> metalloproteinases and an inhibitor<br />
by joint tissues from normal rabbits, and from rabbits with a model<br />
arthritis, II: Articular cartilage. Rheumatol Int. 1981;1(1):17-20.<br />
9. Milner JM, Rowan AD, Cawston TE, Young DA. Metalloproteinase<br />
and inhibitor expression pr<strong>of</strong>iling <strong>of</strong> resorbing cartilage reveals procollagenase<br />
activation as a critical step for collagenolysis. Arthritis Res<br />
Ther. 2006;8(5):R142.<br />
10. Dean DD, Martel-Pelletier J, Pelletier JP, Howell DS, Woessner<br />
JF Jr. Evidence for metalloproteinase and metalloproteinase inhibitor<br />
imbalance in human osteoarthritic cartilage. J Clin Invest.<br />
1989;84(2):678-685.<br />
11. Burrage PS, Mix KS, Brinckerh<strong>of</strong>f CE. Matrix metalloproteinases:<br />
role in arthritis. Front Biosci. 2006;11:529-543.<br />
12. Miyamoto K, Ishimaru J, Kurita K, Goss AN. Synovial matrix metalloproteinase-2<br />
in different stages <strong>of</strong> sheep temporomandibular joint<br />
osteoarthrosis. J Oral Maxill<strong>of</strong>ac Surg. 2002;60(1):66-72.<br />
13. Mizui T, Ishimaru J, Miyamoto K, Kurita K. Matrix metalloproteinase-2<br />
in synovial lavage fluid <strong>of</strong> patients with disorders <strong>of</strong> the temporomandibular<br />
joint. Br J Oral Maxill<strong>of</strong>ac Surg. 2001;39(4):310-314.<br />
14. Lai YC, Shaftel SS, Miller JN, et al. Intraarticular induction<br />
<strong>of</strong> interleukin-1beta expression in the adult mouse, with resultant<br />
temporomandibular joint pathologic changes, dysfunction, and pain.<br />
Arthritis Rheum. 2006;54(4):1184-1197.<br />
42 Gunson, Arnett | Condylar Resorption, Matrix Metalloproteinases, and Tetracyclines<br />
15. Yamaguchi A, Tojyo I, Yoshida H, Fujita S. Role <strong>of</strong> hypoxia and<br />
interleukin-1beta in gene expressions <strong>of</strong> matrix metalloproteinases in<br />
temporomandibular joint disc cells. Arch Oral Biol. 2005;50(1):81-87.<br />
16. Ijima Y, Kobayashi M, Kubota E. Role <strong>of</strong> interleukin-1 in induction<br />
<strong>of</strong> matrix metalloproteinases synthesized by rat temporomandibular<br />
joint chondrocytes and disc cells. Eur J Oral Sci. 2001;109(1):50-59.<br />
17. Puzas JE, Landeau JM, Tallents R, Albright J, Schwarz EM,<br />
Landesberg R. Degradative pathways in tissues <strong>of</strong> the temporomandibular<br />
joint:use <strong>of</strong> in vitro and in vivo models to characterize<br />
matrix metalloproteinase and cytokine activity. Cells Tissues Organs.<br />
2001;169(3):248-256.<br />
18. Abramson SB, Yazici Y. Biologics in development for rheumatoid<br />
arthritis: relevance to osteoarthritis. Adv Drug Deliv Rev.<br />
2006;58(2):212-225.<br />
19. Muroi Y, Kakudo K, Nakata K. Effects <strong>of</strong> compressive loading on<br />
human synovium-derived cells. J Dent Res. 2007;86(8):786-791.<br />
20. Miyamoto K, Ishimaru J, Kurita K, Goss AN. Synovial matrix metalloproteinase-2<br />
in different stages <strong>of</strong> sheep temporomandibular joint<br />
osteoarthrosis. J Oral Maxill<strong>of</strong>ac Surg. 2002;60(1):66-72.<br />
21. Yamaguchi A, Tojyo I, Yoshida H, Fujita S. Role <strong>of</strong> hypoxia and<br />
interleukin-1beta in gene expressions <strong>of</strong> matrix metalloproteinases in<br />
temporomandibular joint disc cells. Arch Oral Biol. 2005;50(1):81-87.<br />
22. Tiilikainen P, Pirttiniemi P, Kainulainen T, Pernu H, Raustia A.<br />
MMP-3 and -8 expression is found in the condylar surface <strong>of</strong> temporomandibular<br />
joints with internal derangement. J Oral Pathol Med.<br />
2005;34(1):39-45.<br />
23. Lai YC, Shaftel SS, Miller JN, et al. Intraarticular induction<br />
<strong>of</strong> interleukin-1beta expression in the adult mouse, with resultant<br />
temporomandibular joint pathologic changes, dysfunction, and pain.<br />
Arthritis Rheum. 2006;54(4):1184-1197.<br />
24. Yoshida K, Takatsuka S, Hatada E, et al. Expression <strong>of</strong> matrix metalloproteinases<br />
and aggrecanase in the synovial fluids <strong>of</strong> patients with<br />
symptomatic temporomandibular disorders. Oral Surg Oral Med Oral<br />
Pathol Oral Radiol Endod. 2006;102(1):22-27.<br />
25. Srinivas R, Sorsa T, Tjaderhane L, et al. Matrix metalloproteinases<br />
in mild and severe temporomandibular joint internal derangement<br />
synovial fluid. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.<br />
2001;91(5):517-525.<br />
26. Tanaka A, Kumagai S, Kawashiri S, et al. Expression <strong>of</strong> matrix<br />
metalloproteinase-2 and -9 in synovial fluid <strong>of</strong> the temporomandibular<br />
joint accompanied by anterior disc displacement. J Oral Pathol Med.<br />
2001;30(1):59-64.<br />
27. Tanaka A, Kawashiri S, Kumagai S, et al. Expression <strong>of</strong> matrix metalloproteinase-2<br />
in osteoarthritic fibrocartilage from human mandibular<br />
condyle. J Oral Pathol Med. 2000; 29(7):314-320.<br />
28. Kubota T, Kubota E, Matsumoto A, et al. Identification <strong>of</strong> matrix<br />
metalloproteinases (MMPs) in synovial fluid from patients with temporomandibular<br />
disorder. Eur J Oral Sci. 1998;106(6):992-998.
29. Zardeneta G, Milam SB, Lee T, Schmitz JP. Detection and preliminary<br />
characterization <strong>of</strong> matrix metalloproteinase activity in<br />
temporomandibular joint lavage fluid. Int J Oral Maxill<strong>of</strong>ac Surg.<br />
1998;27(5):397-403.<br />
30. Kubota E, Imamura H, Kubota T, Shibata T, Murakami K. Interleukin<br />
1 beta and stromelysin (MMP3) activity <strong>of</strong> synovial fluid as<br />
possible markers <strong>of</strong> osteoarthritis in the temporomandibular joint. J<br />
Oral Maxill<strong>of</strong>ac Surg. 1997;55(1):20-27.<br />
31. Kubota E, Kubota T, Matsumoto J, Shibata T, Murakami KI. Synovial<br />
fluid cytokines and proteinases as markers <strong>of</strong> temporomandibular<br />
joint disease. J Oral Maxill<strong>of</strong>ac Surg. 1998;56(2):192-198.<br />
32. Kanyama M, Kuboki T, Kojima S, et al. Matrix metalloproteinases<br />
and tissue inhibitors <strong>of</strong> metalloproteinases in synovial fluids <strong>of</strong><br />
patients with temporomandibular joint osteoarthritis. J Or<strong>of</strong>ac Pain.<br />
2000;14(1):20-30.<br />
33. Marchetti C, Cornaglia I, Casasco A, Bernasconi G, Baciliero U,<br />
Stetler-Stevenson WG. Immunolocalization <strong>of</strong> gelatinase-A (matrix<br />
metalloproteinase-2) in damaged human temporomandibular joint<br />
discs. Arch Oral Biol. 1999;44(4):297-304.<br />
34. Kapila S, Wang W, Uston K. Matrix metalloproteinase induction<br />
by relaxin causes cartilage matrix degradation in target synovial joints.<br />
Ann N Y Acad Sci. 2009;1160:322-328.<br />
35. Shinoda C, Takaku S. Interleukin-1 beta, interleukin-6, and tissue<br />
inhibitor <strong>of</strong> metalloproteinase-1 in the synovial fluid <strong>of</strong> the temporomandibular<br />
joint with respect to cartilage destruction. Oral Dis.<br />
2000;6(6):383-390.<br />
36. Kanyama M, Kuboki T, Kojima S, et al. Matrix metalloproteinases<br />
and tissue inhibitors <strong>of</strong> metalloproteinases in synovial fluids <strong>of</strong><br />
patients with temporomandibular joint osteoarthritis. J Or<strong>of</strong>ac Pain.<br />
2000;14(1):20-30.<br />
37. Golub LM, Lee HM, Ryan ME, Giannobile WV, Payne J, Sorsa T.<br />
Tetracyclines inhibit connective tissue breakdown by multiple nonantimicrobial<br />
mechanisms. Adv Dent Res. 1998;(12):12-26.<br />
38. Golub LM, Lee HM, Greenwald RA, et al. A matrix metalloproteinase<br />
inhibitor reduces bone-type collagen degradation fragments and<br />
specific collagenases in gingival crevicular fluid during adult periodontitis.<br />
Inflamm Res. 1997;(46):310-319.<br />
39. Smith GN Jr, Mickler EA, Hasty KA, Brandt KD. Specificity <strong>of</strong> inhibition<br />
<strong>of</strong> matrix metalloproteinase activity by doxycycline: relationship<br />
to structure <strong>of</strong> the enzyme. Arthritis Rheum. 1999;42(6):1140-1146.<br />
40. Schlondorff D, Satriano J. Interactions with calmodulin: potential<br />
mechanism for some inhibitory actions <strong>of</strong> tetracyclines and calcium<br />
channel blockers. Biochem Pharmacol. 1985;34(18):3391-3393.<br />
41. Webster GF, Toso SM, Hegemann L. Inhibition <strong>of</strong> a model <strong>of</strong> in<br />
vitro granuloma formation by tetracyclines and cipr<strong>of</strong>loxacin: involvement<br />
<strong>of</strong> protein kinase C. Arch Dermatol. 1994;130(6):748-752.<br />
42. Kirkwood K, Martin T, Andreadis ST, Kim YJ. Chemically modified<br />
tetracyclines selectively inhibit IL-6 expression in osteoblasts by decreasing<br />
mRNA stability. Biochem Pharmacol. 2003;66(9):1809-1819.<br />
43. Arner EC, Hughes CE, Decicco CP, Caterson B, Tortorella MD.<br />
Cytokine-induced cartilage proteoglycan degradation is mediated by<br />
aggrecanase. Osteoarthritis Cartilage. 1998;6(3):214-228.<br />
44. Amin AR, Attur MG, Thakker GD, et al. A novel mechanism <strong>of</strong> action<br />
<strong>of</strong> tetracyclines: effects on nitric oxide synthases. Proc Natl Acad<br />
Sci U S A. 1996;93(24):14014-14019.<br />
45. Borderie D, Hernvann A, Hilliquin P, Lemarchal H, Kahan<br />
A, Ekindjian OG. Tetracyclines inhibit nitrosothiol production<br />
by cytokine-stimulated osteoarthritic synovial cells. Inflamm Res.<br />
2001;50(8):409-414.<br />
46. Shlopov BV, Stuart JM, Gumanovskaya ML, Hasty KA. Regulation<br />
<strong>of</strong> cartilage collagenase by doxycycline. J Rheumatol. 2001;28(4):835-<br />
842.<br />
47. Holmes SG, Still K, Buttle DJ, Bishop NJ, Grabowski PS. Chemically<br />
modified tetracyclines act through multiple mechanisms directly<br />
on osteoclast precursors. Bone. 2004;35(2):471-478.<br />
48. Bettany JT, Peet NM, Wolowacz RG, Skerry TM, Grabowski PS.<br />
Tetracyclines induce apoptosis in osteoclasts. Bone. 2000;27(1):75-80.<br />
49. Bettany JT, Wolowacz RG. Tetracycline derivatives induce apoptosis<br />
selectively in cultured monocytes and macrophages but not in<br />
mesenchymal cells. Adv Dent Res. 1998;12(2):136-143.<br />
50. Ramamurthy N, Greenwald R, Moak S, et al. CMT/Tenidap<br />
treatment inhibits temporomandibular joint destruction in adjuvant<br />
arthritic rats. Ann N Y Acad Sci. 1994; (732):427-430.<br />
51. Yu LP Jr, Burr DB, Brandt KD, O’Connor BL, Rubinow A, Albrecht<br />
M. Effects <strong>of</strong> oral doxycycline administration on histomorphometry<br />
and dynamics <strong>of</strong> subchondral bone in a canine model <strong>of</strong> osteoarthritis.<br />
J Rheumatol. 1996;(23):137-142.<br />
52. Yu LP Jr, Smith GN Jr, Brandt KD, Myers SL, O’Connor BL, Brandt<br />
DA. Reduction <strong>of</strong> the severity <strong>of</strong> canine osteoarthritis by prophylactic<br />
treatment with oral doxycycline. Arthritis Rheum. 1992;(35):1150-<br />
1159.<br />
53. Stone M, Fortin PR, Pacheco-Tena C, Inman RD. Should tetracycline<br />
treatment be used more extensively for rheumatoid arthritis?<br />
Metaanalysis demonstrates clinical benefit with reduction in disease<br />
activity. J Rheumatol. 2003;30(10):2112-2122.<br />
54. Sreekanth VR, Handa R, Wali JP, Aggarwal P, Dwivedi SN. Doxycycline<br />
in the treatment <strong>of</strong> rheumatoid arthritis--a pilot study. J Assoc<br />
Physicians India. 2000;(48):804-807.<br />
55. Israel HA, Ramamurthy NS, Greenwald R, Golub L. The potential<br />
role <strong>of</strong> doxycycline in the treatment <strong>of</strong> osteoarthritis <strong>of</strong> the temporomandibular<br />
joint. Adv Dent Res. 1998; (12):51-55.<br />
56. Golub LM, Sorsa T, Lee HM, et al. Doxycycline inhibits neutrophil<br />
(PMN)-type matrix metalloproteinases in human adult periodontitis<br />
gingiva. J Clin Periodontol. 1995; 22(2):100-109.<br />
57. Baxter BT, Pearce WH, Waltke EA, et al. Prolonged administration<br />
<strong>of</strong> doxycycline in patients with small asymptomatic abdominal aortic<br />
aneurysms: report <strong>of</strong> a prospective (phase II) multicenter study. J Vasc<br />
Surg. 2002;36(1):1-12.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
43
58. Walker C, Preshaw PM, Novak J, Hefti AF, Bradshaw M, Powala<br />
C. Long-term treatment with sub-antimicrobial dose doxycycline<br />
has no antibacterial effect on intestinal flora. J Clin Periodontol.<br />
2005;32(11):1163-1169.<br />
59. Walker C, Puumala S, Golub LM, et al. Subantimicrobial dose<br />
doxycycline effects on osteopenic bone loss: microbiologic results. J<br />
Periodontol. 2007;78(8):1590-1601.<br />
60. Suzuki Y, Inoue K, Chiba J, Inoue Y, Kanbe K. Histological analysis<br />
<strong>of</strong> synovium by treatment <strong>of</strong> etanercept for rheumatoid arthritis. Int J<br />
Rheum Dis. 2009;12(1):7-13.<br />
61. Wu YS, Hu YY, Yang RF, Wang Z, Wei YY. The matrix metalloproteinases<br />
as pharmacological target in osteoarthritis: statins may be <strong>of</strong><br />
therapeutic benefit. Med Hypotheses. 2007;69(3):557-559.<br />
62. Cohen SB, Dore RK, Lane NE, et al. Denosumab treatment effects<br />
on structural damage, bone mineral density, and bone turnover in<br />
rheumatoid arthritis: a twelve-month, multicenter, randomized, doubleblind,<br />
placebo-controlled, phase II clinical trial. Arthritis Rheum.<br />
2008;58(5):1299-1309.<br />
63. Tetlow LC, Woolley DE. Expression <strong>of</strong> vitamin D receptors and<br />
matrix metalloproteinases in osteoarthritic cartilage and human articular<br />
chondrocytes in vitro. Osteoarthritis Cartilage. 2001;9(5):423-431.<br />
44 Gunson, Arnett | Condylar Resorption, Matrix Metalloproteinases, and Tetracyclines
Comparison <strong>of</strong> Maxillary Cast Positions Mounted from a True Hinge<br />
Kinematic Face-Bow vs. an Arbitrary Face-Bow in Three Planes <strong>of</strong> Space<br />
Dori Freeland, DDS, MS ■ Theodore Freeland, DDS, MS<br />
■ Richard Kulbersh, DMD, MS, PLC ■ Richard Kaczynski, BS, MS, PhD<br />
doR i FR e e L a n d, ddS, mS<br />
tdfortho@freelandorthodontics.com<br />
■ Private Practice, Lake Orion, MI<br />
The o d o R e FR e e L a n d, ddS, mS<br />
■ Adjunct Pr<strong>of</strong>essor, Orthodontic<br />
Dept., School <strong>of</strong> Dentistry,<br />
University <strong>of</strong> Detroit Mercy<br />
■ Director <strong>Roth</strong>/<strong>Williams</strong> USA<br />
■ Private Practice, Gaylord, MI<br />
Ric h a R d Ku L b e R S h, dmd, mS, PLc<br />
■ Program Director, Orthodontic<br />
Dept., School <strong>of</strong> Dentistry,<br />
University <strong>of</strong> Detroit Mercy<br />
Ric h a R d Ka c z y n S K i , bS, mS, Phd<br />
■ Statistician, Dept. <strong>of</strong> Psychiatry,<br />
Yale University School <strong>of</strong> Medicine<br />
Introduction<br />
The quest to understand the multifaceted movements <strong>of</strong><br />
the mandible and its relationship to the rest <strong>of</strong> the cranial<br />
complex began in the early 1800s. 1 Gray’s Anatomy was<br />
one <strong>of</strong> the first sources to publish the fact that the mandible<br />
moves on a hinge as well as by forward and lateral movements<br />
from the condyles in the glenoid fossae. 1 Thus, the<br />
temporomandibular joint (TMJ) became known as a ginglymo-arthrodial<br />
joint and was seen as one <strong>of</strong> the most complex<br />
joints in the human body. Although the TMJ is considered<br />
a compound joint, it consists <strong>of</strong> only two actual bones. An<br />
articular disc interposed between the condyles and the mandibular<br />
fossa <strong>of</strong> the temporal bone keeps the two bones from<br />
direct articulation. The disc serves as a nonossified bone; it<br />
serves as the third bone <strong>of</strong> the compound joint and allows<br />
complex movements to occur. 2<br />
When occlusal function is ideal, the condyles are positioned<br />
in the glenoid fossae and the mandible should be<br />
able to move by joint-dictated patterns without any interfer-<br />
Summary<br />
There are many methods <strong>of</strong> performing a face-bow transfer, but only two<br />
current methods <strong>of</strong> replicating the position <strong>of</strong> the maxilla in three planes <strong>of</strong><br />
space: with a true hinge face-bow or with an arbitrary earpiece face-bow. The<br />
purpose <strong>of</strong> this study was to determine if a clinically significant difference in<br />
three planes <strong>of</strong> space occurs in the mounting <strong>of</strong> the maxillary cast when the<br />
mounting is done with an arbitrary earpiece face-bow versus a true hinge<br />
face-bow.<br />
The sample consisted <strong>of</strong> 51 subjects with complete permanent dentitions<br />
through the second molars, including class I, class II, and class III subjects.<br />
Two maxillary impressions were taken on each subject. One maxillary cast<br />
was mounted using an arbitrary earpiece face-bow and the other using a true<br />
hinge face-bow. Each cast was measured and compared in three planes <strong>of</strong><br />
space on an adjustable occlusal table containing graph paper. The positions<br />
<strong>of</strong> the maxillary right central and right and left first molars were recorded for<br />
the true hinge mounting in red on the graph paper and the arbitrary earpiece<br />
face-bow measurements were recorded in blue. The vertical, anteroposterior<br />
(A-P), and transverse differences between the two mountings were recorded,<br />
and a paired t-test was used to analyze the data. The two face-bow techniques<br />
were statistically significantly different in all three planes <strong>of</strong> space (p ≤ .001).<br />
ence from the teeth. 3 According to Okeson, this position is<br />
achieved when the muscles <strong>of</strong> mastication and the ligaments<br />
combine to seat the condyle into the glenoid fossa. 2 Stability<br />
<strong>of</strong> the joint is maintained by constant muscle activity, even<br />
in resting states, which allows the articular surfaces to come<br />
into contact, although a true structural attachment or union<br />
is not present in the TMJ. 2 The muscles play an active role in<br />
the opening and closing <strong>of</strong> the mandible, while the ligaments<br />
act as passive restraining devices to limit joint movements.<br />
Specifically, the temporomandibular ligament plays a role<br />
in limiting the extent <strong>of</strong> mouth opening. During the initial<br />
phase <strong>of</strong> opening, the condyle rotates around a fixed point<br />
for about 20 mm, until the temporomandibular ligament<br />
becomes strained and the condyle is forced into a forward<br />
movement down the articular eminence. 2 Posselt defined<br />
this opening as the mandibular terminal hinge opening and<br />
closing. 4 The Glossary <strong>of</strong> Prosthodontic Terms similarly describes<br />
this movement as “an imaginary line around which<br />
the mandible may rotate through the sagittal plane” and<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
45
terms the movement the transverse horizontal axis. 5<br />
Study <strong>of</strong> mandibular movements raised questions among<br />
the dental pr<strong>of</strong>ession as to whether a hinge axis actually exists,<br />
and if so, whether it is one axis or more than one. The<br />
dental pr<strong>of</strong>ession also debated how accurately the hinge axis<br />
can be located, if in fact one exists; the clinical usefulness <strong>of</strong><br />
locating it; and whether an arbitrary point on the face can<br />
satisfactorily be substituted for a specific point as a location<br />
for the hinge axis. 6 No other topic inspires more controversy<br />
in oral physiology than the role <strong>of</strong> the jaw joints in dental<br />
articulation.<br />
Campion, working in 1902, made the first graphic<br />
record <strong>of</strong> the mandibular movements in a patient. He concluded<br />
that both a rotation <strong>of</strong> the bone on an axis and a<br />
forward-downward movement <strong>of</strong> the condyles occurred.<br />
Campion designed an adjustable face-bow fixed to the mandibular<br />
teeth with modeling plaster to graphically record the<br />
various positions <strong>of</strong> the condyles on the face with a succession<br />
<strong>of</strong> dots. He concluded that “the only part <strong>of</strong> the opening<br />
movement which an articulator reproduction is concerned<br />
with is the initial stage, which is seen in the tracings to be a<br />
7, 8<br />
simple rotation about an axis passing through the condyles.”<br />
Bennett also recognized that the mandible was capable <strong>of</strong><br />
two independent movements, but he felt that no single fixed<br />
center <strong>of</strong> rotation for the mandible existed. 8 He judged that<br />
the initial center <strong>of</strong> rotation <strong>of</strong> the mandible was located behind<br />
and below the condyle. 8<br />
During this same period, Stallard introduced the term—<br />
and the concept <strong>of</strong>—gnathology—the study <strong>of</strong> the harmonious,<br />
interrelated functioning <strong>of</strong> the jaws and teeth. 1,7,9 In<br />
1924, McCollum developed the first method <strong>of</strong> locating the<br />
hinge axis with an instrument called the gnathoscope, and<br />
its later model, the gnathograph. 1,7 McCollum demonstrated<br />
that no external anatomical landmarks would indicate the<br />
position <strong>of</strong> the opening axis, nor could this be done by palpating<br />
the joint or by measuring a distance in any direction. 1,7<br />
McCollum explained that the hinge axis must be determined<br />
instrumentally, and that the movement <strong>of</strong> this axis is a component<br />
<strong>of</strong> every masticatory movement <strong>of</strong> the mandible. 1,7<br />
After McCollum’s death, Stuart continued to study mandibular<br />
movement and developed his own gnathological system,<br />
including a fully adjustable articulator and pantograph. 1,7<br />
Gnathologically oriented studies produced and still produce<br />
conflicting conclusions that divide the dental community.<br />
One group believes that there is a definite transverse<br />
hinge axis, and that it is necessary to find its point <strong>of</strong> rotation.<br />
Another group believes that methods <strong>of</strong> locating an<br />
arbitrary hinge point are just as reliable, and more operator<br />
friendly. Still others believe that it is not necessary to locate<br />
the transverse axis at all.<br />
46 Freeland et al | Comparison <strong>of</strong> Maxillary Cast Positions<br />
Trapozzano and Lazzari found that 57.2% <strong>of</strong> the subjects<br />
in their study had more than one condylar hinge axis<br />
point located on either one or both sides <strong>of</strong> the mandible.<br />
Therefore, the attempt to locate the hinge axis, was seriously<br />
questioned because multiple axis points may exist. 10,11 Other<br />
studies have demonstrated that the center <strong>of</strong> rotation is movable<br />
during every phase <strong>of</strong> jaw opening and closing; therefore<br />
these studies also refute the hinge axis theory. 12,13 Still<br />
other studies have questioned the use <strong>of</strong> a hinge axis, due<br />
to the complexity <strong>of</strong> its location, and the technical operator<br />
error that is inherent in the procedure. 14,15 Many investigators<br />
believe that it may be impractical to construct clutches,<br />
locate the hinge axis, make multiple interocclusal records,<br />
and use a fully adjustable articulator on every patient. 16 Still<br />
the theory that the hinge axis is a reliable reference—one in<br />
which the position <strong>of</strong> the maxillary cast on an articulator can<br />
be reproduced—is a very strong one. 4<br />
Many studies have demonstrated that the terminal hinge<br />
movements <strong>of</strong> the mandible pass through both condyles.<br />
These studies support the theory that there is only one hinge<br />
axis . 4,17-19 Beard and Clayton reached this conclusion by using<br />
an apparatus that records arcs on paper; they argued that<br />
the terminal hinge axis can be accurately located by finding<br />
the one and only stylus position where no arcing occurs. 19<br />
There are many methods <strong>of</strong> locating the arbitrary hinge<br />
axis for transfer to an articulator. Following are some examples<br />
<strong>of</strong> these methods.<br />
1. The Gysi point is located 13 mm in front <strong>of</strong> the<br />
most upper part <strong>of</strong> the external auditory meatus on<br />
a line passing to the ectocanthion.<br />
2. The Lauritzen-Bodner axis is located 12 mm anterior<br />
to and 2 mm below the porion.<br />
3. Abdal-Hadi axis is located using a linear regression<br />
formula to predict the anteroposterior (A-P) site <strong>of</strong><br />
the hinge point, according to the width pr<strong>of</strong>ile axis<br />
theory <strong>of</strong> the face.<br />
4. The arbitrary hinge axis is located using the earpiece<br />
face-bow. In this method, the ear rods <strong>of</strong> a<br />
fixed face-bow are inserted into the external auditory<br />
meati.<br />
5. The arbitrary hinge axis is located by external palpation<br />
<strong>of</strong> the condylar anatomy. 20,21<br />
Studies have shown that when an arbitrary earpiece<br />
face-bow is used to reproduce the condylar positions, the<br />
results are fairly reliable. 22-27 Clinically, it has become acceptable<br />
that as long as the arbitrary point is within 5 mm <strong>of</strong> the<br />
true hinge axis, the arbitrary earpiece face-bow is accurate<br />
enough to study the patient’s occlusion. 22-27 Nagy et al conducted<br />
another study comparing the location <strong>of</strong> an anatomically<br />
predetermined hinge axis point with marked hinge axis
points. They found that the mean distance between any two<br />
points was 1.1 mm. More than 96% <strong>of</strong> predetermined points<br />
were within 2 mm <strong>of</strong> the true hinge axis. 23 Schallhorn also<br />
found that approximately 98% <strong>of</strong> all true anatomical hinge<br />
axis points were within a 5-mm radius. 26<br />
In comparison, studies that compared maxillary cast positions<br />
mounted with four different face-bows showed wide<br />
variation in the mounted maxillary cast positions. All arbitrary<br />
hinge axis points deviated from the true hinge baseline<br />
point by anywhere from 1.5 mm to 4 mm. Therefore, the<br />
authors <strong>of</strong> these studies concluded that it was not possible<br />
to establish the clinical superiority <strong>of</strong> one arbitrary face-bow<br />
over another. 28,29<br />
Lauritzen and Bodner located 100 true hinge points on<br />
50 subjects. They found that 67% <strong>of</strong> the axis points were<br />
5 mm to 13 mm away from the arbitrarily marked hinge<br />
points. This discrepancy may introduce gross errors in the<br />
mounting <strong>of</strong> the casts on an articulator, resulting in large<br />
occlusal errors. 30 Palik et al got similar results. They found<br />
that only 50% <strong>of</strong> the arbitrary hinge axes located with the<br />
arbitrary earpiece face-bow were within a 5-mm radius <strong>of</strong><br />
the terminal hinge axis. This indicated that the arbitrary<br />
earpiece face-bow hinge axis location does not represent the<br />
total population. 31 Schulte et al concluded from their study<br />
that errors in locating the arbitrary hinge axis will produce<br />
a three-dimensional occlusal error. 32 This study and others<br />
have recommended that if a thick vertical dimension <strong>of</strong> wax<br />
was used for an interocclusal record, or if the vertical dimension<br />
will be changed with treatment, a true hinge axis should<br />
be located on the patient. 32,33 Due to anatomical variations,<br />
the arbitrary earpiece face-bow may introduce significant errors<br />
in an A-P or vertical dimension, resulting in mandibular<br />
displacement. 34,35 The only way to be relatively certain that<br />
errors due to malpositioning <strong>of</strong> maxillary casts on an articulator<br />
have been avoided is to locate the true hinge axis. 30,36-40<br />
Studies indicate that coincidence between the two hinge<br />
axis points does not usually occur. 41 This results in a discrepancy<br />
between the arbitrary hinge axis and the true hinge axis<br />
points. This discrepancy will cause changes in the mounted<br />
position <strong>of</strong> the maxillary cast, which in turn can produce a<br />
positional change <strong>of</strong> all teeth in the three planes <strong>of</strong> space. 41<br />
Zuckerman mathematically demonstrated that discrepancies<br />
between the true hinge axis and the arbitrary hinge axis points<br />
can produce changes in the A-P direction <strong>of</strong> the occlusion. He<br />
verified in his analog tracing that the arc <strong>of</strong> the incisal edge<br />
does not change in the A-P direction in centric occlusion, as<br />
long as the mandible is also coincident in centric relation.<br />
However, when an error in the arbitrary hinge axis occurs<br />
and it is anterior to the true hinge, the incisor arc <strong>of</strong> closure<br />
is anterior to the actual arc <strong>of</strong> closure. 41 Errors in the verti-<br />
cal position <strong>of</strong> the arbitrary hinge axis (AHA) produce the<br />
largest A-P discrepancies upon mandibular closing. 41 Other<br />
authors have graphically illustrated how errors in true hinge<br />
axis location can produce occlusal aberrations. 33,35,36,42 These<br />
authors also showed that the greatest errors occurred when<br />
the hinge axis was incorrectly located in a vertical direction<br />
perpendicular to the correct hinge axis closure. An arbitrary<br />
hinge axis positioned superior to the true hinge axis also<br />
produced premature contacts on the anterior teeth. In addition,<br />
if the arbitrary hinge axis was placed inferior to the true<br />
hinge axis, premature posterior contacts occured. 33,35,36,42<br />
Brotman’s geometric representation related changes in<br />
the hinge axis point locations between the true hinge axis<br />
and the arbitrary axis to differences produced at the occlusal<br />
level in mounted casts. 43 Brotman concluded that “if the<br />
hinge axis has been improperly located by as much as 3 mm,<br />
the error at the occluding position <strong>of</strong> the casts (anteroposteriorly)<br />
will be about .09 mm or less than 1/250 inch.” 43<br />
Gordon et al looked at the location <strong>of</strong> the terminal hinge<br />
axis and its effect on the second molar cusp position on the<br />
position <strong>of</strong> the second molar cusp. 6 Their results showed that<br />
incorrect anterior location <strong>of</strong> the hinge axis produced the effect<br />
<strong>of</strong> having moved the mandibular arch backward. Incorrect<br />
posterior location <strong>of</strong> the hinge axis produced the effect<br />
<strong>of</strong> having moved the mandibular arch forward. Incorrect inferior<br />
location <strong>of</strong> the hinge axis caused slight retrusion <strong>of</strong> the<br />
mandibular cast with premature posterior contacts. Incorrect<br />
superior location <strong>of</strong> the hinge axis caused protrusion <strong>of</strong> the<br />
mandibular cast with premature anterior contacts. 6<br />
Since studies vary in reporting the percentage <strong>of</strong> placement<br />
<strong>of</strong> the arbitrary hinge axis less than 5 mm from the true<br />
hinge axis, it can be assumed that larger errors in occlusion<br />
may occur. It has been found that an occlusal discrepancy <strong>of</strong><br />
0.01 inch can cause pulpitis or periodontal disease, though<br />
the patient may not be able to detect so small a discrepancy. 44<br />
To limit occlusal errors in mountings, it is necessary to locate<br />
the hinge axis to within 1 mm, and the kinematic true hinge<br />
can be done to this degree <strong>of</strong> accuracy. 44 Therefore, the importance<br />
<strong>of</strong> the true hinge axis is substantial when changing<br />
the vertical dimension upon mandibular closure. 38<br />
Orthodontics deals specifically with the movement <strong>of</strong><br />
all teeth and their occlusal fit. Therefore, it calls for extreme<br />
accuracy during diagnosis, treatment planning, and rendering<br />
treatment. 9 Clinically finding the true hinge axis may be<br />
the only way to ensure a reproducible and accurate starting<br />
point—one from which optimum esthetic and functional results<br />
can be obtained. 6,38,45 The purpose <strong>of</strong> this study was to<br />
compare the maxillary cast mountings <strong>of</strong> 51 patients in three<br />
planes <strong>of</strong> space when mounted using a true hinge axis facebow<br />
versus an arbitrary earpiece face-bow.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
47
Materials and Methods<br />
The records <strong>of</strong> 51 patients—34 females and 17 males—treated<br />
in a gnathologically oriented practice constituted the sample.<br />
Subjects ranged in age from 13 to 57 years, and all had<br />
unremarkable medical histories with no contraindications to<br />
orthodontic treatment. All upper and lower permanent teeth,<br />
except third molars, were present on all subjects. TMJ exams<br />
were conducted by a single operator before orthodontic records<br />
were conducted. Evaluation included subjective symptomatology,<br />
as well as clinical examination. Subjects who<br />
presented with TMJ symptoms were placed on a gnathological<br />
maxillary splint for a minimum <strong>of</strong> 3 months, or until<br />
subjects were symptom free. Twenty <strong>of</strong> the 51 subjects had<br />
records taken after splint therapy. The remaining 31 subjects,<br />
all in active orthodontic treatment and with asymptomatic<br />
TMJ, had records taken one appointment prior to deband.<br />
All subjects had two maxillary alginate impressions taken<br />
using Jeltrate alginate (Dentsply, Milford, Delaware). The<br />
impressions were taken using sterilized metal rim lock trays<br />
(Dentsply, Milford, Delaware). All impressions were disinfected<br />
using Sterall Plus Spray (Colgate-Palmolive Company,<br />
Canton, Massachusetts), and were rinsed with water and air<br />
dried before being poured up.<br />
All impressions were wrapped in moistened paper towels<br />
and placed in plastic bags for approximately 20 minutes<br />
prior to being poured up with Velmix (KerrLab, Orange,<br />
California). Each model was poured up utilizing a waterpowder<br />
ratio consistent with the manufacturer’s instructions<br />
for Velmix. The Velmix was vacuum mixed to remove any<br />
entrapped air. The models were trimmed, and all bubbles<br />
were removed from the occlusal surfaces.<br />
Arbitrary earpiece face-bow transfers using the external<br />
auditory meati were taken on each subject. (Panadent, Grand<br />
Terrace, California) (Figure 1).<br />
48 Freeland et al | Comparison <strong>of</strong> Maxillary Cast Positions<br />
Figure 1-a, b Estimated facebow.<br />
Figure 1-b<br />
A true hinge face-bow was then taken on each subject,<br />
using the true hinge axis instrument (Panadent, Grand Ter-<br />
race, California) (Figure 2). A single operator completed<br />
both face-bow records within 20 minutes <strong>of</strong> each procedure.<br />
Intraoperator reliability tests for each <strong>of</strong> the two transfer<br />
techniques were calculated.
Figure 2-a, b True-hinge facebow.<br />
Figure 2-b.<br />
One maxillary cast was mounted using the true hinge<br />
kinematic face-bow transfer on a single Panadent articulator<br />
(Panadent, Grand Terrace, California), with Snow White<br />
Plaster #2 (Kerrlab, Orange, California) mixed according to<br />
the manufacturer’s instructions. The second maxillary cast<br />
was mounted with the arbitrary face bow on a single Panadent<br />
articulator (Panadent, Grand Terrace, California), using<br />
the same mounting plaster as was used for the first cast.<br />
The true hinge maxillary cast was placed on a single<br />
Panadent articulator, and an adjustable occlusal table (Panadent,<br />
Grand Terrace, California), with graph paper adhered<br />
to the surface, was attached to the articulator in place <strong>of</strong> the<br />
mandibular cast. With the occlusal pin at zero, the occlusal<br />
plane relater was stabilized by allowing contact at the maximum<br />
number <strong>of</strong> maxillary cast teeth (Figure 3).<br />
Figure 3 Maxillary cast mounted with<br />
occlusal relater and pin at zero.<br />
A 1-mm step ruler (Panadent, Grand Terrace, California)<br />
was used to measure the vertical distance <strong>of</strong> the mesiobuccal<br />
cusp tip <strong>of</strong> the right and left first permanent molar and the<br />
upper right central incisor (Figure 4).<br />
Figure 4-a Vertical measurements with 1-mm<br />
incremental step ruler: Measurement <strong>of</strong> anterior tooth<br />
vertical discrepancy.<br />
Figure 4-b Vertical measurements with 1-mm<br />
incremental step ruler: Measurement <strong>of</strong> posterior tooth<br />
vertical discrepancy.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
49
A straight wire with a 90-degree bend at the tip was<br />
held with the handle parallel to the occlusal plane relater<br />
(Figure 5).<br />
Figure 5 Straight-lined measurement instruments.<br />
The tip was placed perpendicular to the tooth and held<br />
touching the height <strong>of</strong> contour <strong>of</strong> the upper first permanent molars<br />
and the upper right permanent central incisor (Figure 6).<br />
Figure 6 Articulating paper used with straight-lined<br />
measurement instrument for tooth markings.<br />
It was then used to mark the position <strong>of</strong> the mesiobuccal<br />
cusp <strong>of</strong> the upper molars and the entire incisal-edge position<br />
<strong>of</strong> the upper central incisor. Red articulating paper for the<br />
maxillary cast mounted with the true hinge axis face-bow<br />
mounted maxillary cast was then placed beneath each tooth<br />
(Figure 7).<br />
Figure 7 Tooth markings on graph paper.<br />
50 Freeland et al | Comparison <strong>of</strong> Maxillary Cast Positions<br />
This allowed the instrument to register the position <strong>of</strong><br />
each tooth on the graph paper (Figure 8).<br />
Figure 8 Comparing arbitrary hinge axis points vs.<br />
true hinge axis point:<br />
1= Lower incisor will arc closed posterior to actual arc <strong>of</strong> closure<br />
if AHA is inferior to TH.<br />
2= Lower incisor will arc closed anterior to actual arc <strong>of</strong> closure<br />
if AHA is superior to TH.<br />
3= Lower incisor will arc closed slightly posterior to actual arc <strong>of</strong><br />
closure if AHA is anterior to TH.<br />
4= Lower incisor will arc closed slightly anterior to actual arc <strong>of</strong><br />
closure if AHA is posterior to TH.<br />
The occlusal plane relater was left in place, and the same<br />
measuring procedure was then conducted on the maxillary<br />
cast mounted with the estimated face-bow, utilizing blue articulating<br />
paper. A new sheet <strong>of</strong> graph paper was adhered to<br />
the occlusal plane relater each time a new set <strong>of</strong> casts was<br />
measured.<br />
To measure the differences between the red and blue<br />
markings, a Boley gauge was used. Five total measurement<br />
comparisons were done. The first measurement assessed the<br />
change in vertical dimension between the casts at the mesiobuccal<br />
cusp tip <strong>of</strong> the maxillary right permanent first<br />
molar. The second measurement assessed the vertical discrepancy<br />
<strong>of</strong> the upper left first permanent molar. The third<br />
measurement assessed the vertical discrepancy between the<br />
upper right permanent central incisors. The fourth measurement<br />
compared the difference in an A-P direction between<br />
the mesiobuccal cusp tips <strong>of</strong> the upper right and left first<br />
permanent molars. The fifth measurement assessed the transverse<br />
discrepancy between the mesiobuccal cusp tips <strong>of</strong> the<br />
upper molars. All measurements were conducted by a single<br />
operator. Intraoperator reliability testing was used to validate<br />
this measurement technique.<br />
Results<br />
A two-tailed matched-pairs t-test was used to evaluate for<br />
significant difference in occlusal measurements in three<br />
planes <strong>of</strong> space between maxillary casts mounted with a true<br />
hinge face-bow and mounted with an estimated face-bow.<br />
For this experiment, an α level <strong>of</strong> 0.05 was chosen. Given<br />
the number <strong>of</strong> measurements being evaluated (8), we decided
to adjust for experimentwide error by reducing our desired<br />
significance level to 0.001.<br />
Measurements<br />
Table 1 Mean values <strong>of</strong> the two face-bow techniques.<br />
Table 1 shows the means and standard deviations for<br />
the arbitrary face-bow technique and the true hinge facebow<br />
technique in the vertical, A-P, and transverse dimensions<br />
with respect to the maxillary right and left first molars and<br />
the maxillary right central incisor. The mean measurements<br />
taken on the cast mounted with a true hinge face-bow were<br />
significantly smaller than those measured on the arbitrary<br />
earpiece face-bow mountings. The standard deviations for<br />
the true hinge face-bow were also one-half to one-third<br />
smaller, indicating less variation around the sample mean.<br />
Results <strong>of</strong> the paired t-test are shown in Table 2.<br />
Table 2 Paired t-tests for differences between<br />
estimated and true hinge technique.<br />
The two face-bow techniques differed significantly in<br />
all three planes <strong>of</strong> space. The mean vertical discrepancy <strong>of</strong><br />
the maxillary right first molar between the estimated and the<br />
true hinge face-bow was 2.19 +/- 2.31 (t = 6.76, df = 50, p<br />
< .001). The mean vertical discrepancy for the maxillary left<br />
first molar was 2.45 +/- 2.21 (t = 7.90, df = 50, p < .001).<br />
The mean vertical discrepancy for the upper right central<br />
was 1.90 +/- 1.75 (t = 7.76, df = 50, p < .001).<br />
The mean difference in the A-P dimension was 3.82 +/-<br />
5.51 (t = 8.163, df = 50, p < .001) for the maxillary right first<br />
molar and 3.10 +/- 2.63 (t = 8.28, df = 50, p < .001) for the<br />
maxillary left first molar. The maxillary right central incisor<br />
showed a mean difference <strong>of</strong> 3.05 +/- 2.62 (t = 8.25, df = 50,<br />
p < .001). Finally, the transverse dimension was evaluated.<br />
The mean difference for the maxillary right first molar was<br />
2.23 +/- 1.33 (t = 12.11, df = 50, p < .001). The mean differ-<br />
ence for the maxillary left first molar was 2.60 +/- 1.49 (t =<br />
11.57, df = 50, p < .001).<br />
The measurement differences in the vertical direction <strong>of</strong><br />
the maxillary right first molar ranged from 0.0 to 3.0 mm.<br />
The measurement differences in the vertical direction <strong>of</strong> the<br />
maxillary left second molar ranged from 1.0 mm to 3.0 mm.<br />
The measurement differences in the vertical direction <strong>of</strong> the<br />
maxillary upper right central incisor ranged from 0.0 to 5.0<br />
mm. The differences in the A-P dimension <strong>of</strong> the upper right<br />
molar ranged from 0.0 to 13.1 mm; <strong>of</strong> the upper left molar<br />
from 0.0 to 15.0 mm; and <strong>of</strong> the upper central incisor from<br />
0.0 to 13.0 mm. The differences in the transverse dimension<br />
ranged from 0.0 to 7.0 mm for the upper right first molar<br />
and from 0.5 to 7.9 mm for the upper left first molar.<br />
Discussion<br />
Mounting dental casts on an articulator allows the clinician<br />
to simulate maxillo-mandibular position in centric relation<br />
and makes possible a visible simulation <strong>of</strong> mandibular border<br />
movements. It has been recommended that mounting<br />
diagnostic dental casts on an articulator should be incorporated<br />
into routine clinical orthodontic practices. 3,46 Recording<br />
the hinge axis and transferring it to an articulator is <strong>of</strong><br />
considerable value in the diagnosis and treatment <strong>of</strong> occlusal<br />
malfunction. 42 In this diagnostic process, a face-bow transfer<br />
is one <strong>of</strong> the first steps in taking accurate intermaxillary<br />
records. Many face-bow techniques are in use today. 20,21<br />
However, this study conducted a comparison <strong>of</strong> only two<br />
face-bow techniques, an arbitrary earpiece face-bow and a<br />
true hinge face-bow.<br />
The null hypothesis for this study: “There is no difference<br />
in the vertical, horizontal, or transverse position <strong>of</strong> the<br />
maxillary cast mounted with a true hinge face-bow versus an<br />
arbitrary earpiece face-bow” was rejected. Paired t-tests indicated<br />
that the maxillary cast position using an arbitrary facebow<br />
transfer was significantly different in all three planes <strong>of</strong><br />
space from the maxillary cast position mounted using a true<br />
hinge face-bow transfer.<br />
In previous comparison studies when the arbitrary earpiece<br />
face-bow is located anywhere along a 5-mm radius <strong>of</strong><br />
the true hinge axis point, some authors have found that the<br />
mandibular arc <strong>of</strong> closure may not be very different from the<br />
true hinge arc <strong>of</strong> closure. 21,26,39,40,42 However, Lauritzen and<br />
Bodner found that in only 33% <strong>of</strong> the 50 patients they examined<br />
did the arbitrary hinge point fall within 5 mm <strong>of</strong> the<br />
true hinge point. In the other 67%, the arbitrary hinge points<br />
were 5 mm to 13 mm away from the true hinge points. Arbitrary<br />
markings <strong>of</strong> the hinge axis introduce severe errors<br />
in mounting casts on an articulator, which may introduce<br />
occlusal errors in the centric jaw relation record. 30 Ricketts<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
51
found that there can be extreme variation in the s<strong>of</strong>t tissue<br />
around the ear. 34 This variation can make it difficult to locate<br />
the hinge point with an arbitrary earpiece face-bow.<br />
The present study found larger mean values for the arbitrary<br />
earpiece face-bow measurements. This suggests that the true<br />
hinge face-bow may not be as sensitive to anatomical changes<br />
as the arbitrary earpiece face-bow.<br />
Goska and Christensen conducted a similar study to<br />
to the present study, in which they compared the positions<br />
<strong>of</strong> maxillary cast permanent first molars in three planes <strong>of</strong><br />
space, using four different face-bow techniques. A true hinge<br />
face-bow determined axis point was chosen as a baseline<br />
against which to compare the other three arbitrary face-bow<br />
techniques. 28 They found that deviations between this baseline<br />
and the other three face-bow mountings ranged from 1.5<br />
mm to 4 mm. 28 They found that deviations between the true<br />
hinge face-bow and the arbitrary earpiece face-bow ranged<br />
from 1.9 mm to 3.8 mm. Like the authors <strong>of</strong> the present<br />
study, they concluded that variations in the arbitrary earpiece<br />
face-bows might have resulted from naturally occurring<br />
variations in ear anatomy or the fact that the arbitrary<br />
earpiece face-bow is an average measurement. 28<br />
In general, the present study suggests that error introduced<br />
from arbitrary earpiece face-bow hinge axis location<br />
may produce occlusal discrepancies caused by malpositioning<br />
<strong>of</strong> the maxillary cast. The present study differs from<br />
other previous studies in that it evaluates changes at the<br />
occlusal level <strong>of</strong> the maxillary cast, as opposed to looking<br />
at the joint level when comparing arbitrary and true hinge<br />
mounting techniques. This study also differs from previous<br />
studies in that it does not measure the occlusal discrepancies<br />
that result from contacts during the mandibular arc <strong>of</strong><br />
closure, since the mandibular cast was not incorporated into<br />
the measurements.<br />
Zuckerman, in analog tracing the arc <strong>of</strong> the incisal edge,<br />
verified that no A-P change occurred in the arc <strong>of</strong> closure, as<br />
long as the mandible rotated along the accurate hinge axis.<br />
However, when an error in the arbitrary earpiece face-bow<br />
hinge axis occurred anterior to the true hinge, the incisor arc<br />
<strong>of</strong> closure was anterior to the actual arc <strong>of</strong> closure, and when<br />
the arbitrary earpiece face-bow hinge axis occurred posterior<br />
to the true hinge axis, the opposite effect occurred. Errors in<br />
the vertical position <strong>of</strong> the arbitrary earpiece face-bow hinge<br />
axis were found to produce the largest A-P discrepancies<br />
upon mandibular closing41 (Figure 9).<br />
52 Freeland et al | Comparison <strong>of</strong> Maxillary Cast Positions<br />
Figure 9-a True hinge mandibular cast vs. estimated hinge<br />
maxillary cast: True hinge mounting.<br />
Figure 9-b True hinge mandibular cast vs. estimated hinge<br />
maxillary cast: Estimated hinge mounting substituted for true<br />
hinge maxillary mounting.<br />
Zuckerman found that an anterior incisor displacement<br />
<strong>of</strong> 1.5 mm could occur if the arbitrary hinge axis was <strong>of</strong>f from<br />
the true hinge axis by approximately 10 mm. 41 Although the<br />
method for the present study does not incorporate the mandibular<br />
cast arc <strong>of</strong> closure, wax bite thickness, or condylar<br />
positioning, it is interesting to note that the largest discrepancy<br />
in maxillary cast position occurred in the A-P direction<br />
with a mean difference greater than 3 mm in all three areas<br />
measured (maxillary right and left first permanent molar and<br />
the upper right permanent central incisor).<br />
Gordon et al conducted a mathematical study to calculate<br />
the amount <strong>of</strong> cusp height and mesiodistal error at the<br />
second molar that results from arbitrary earpiece face-bow<br />
hinge axis location 5 mm and 8 mm anterior, superior, posterior,<br />
and inferior to the true hinge axis. 6 They concluded<br />
that incorrect location <strong>of</strong> the hinge axis caused a positional<br />
change in the occlusal relationship between the maxilla and<br />
the mandible, resulting in various premature contacts. De-
pending upon the direction in which the arbitrary earpiece<br />
face-bow hinge axis was displaced from the true hinge axis,<br />
the premature contacts occurred either anterior or posterior<br />
to the actual arc <strong>of</strong> closure. Total error that could occur at<br />
the second molar cusp ranged from 0.15 mm <strong>of</strong> open cuspal<br />
space to 0.4 mm <strong>of</strong> excess cuspal height. The mesiodistal<br />
error <strong>of</strong> the second molar cusps ranged from 0.51mm toward<br />
the distal to 0.52 mm toward the mesial. 6 Brotman also<br />
found that a 0.09-mm A-P discrepancy would occur between<br />
occluding casts if the arbitray earpiece face-bow hinge axis<br />
was improperly located by as much as 3 mm from the true<br />
hinge point. Brotman concluded that if the arbitrary earpiece<br />
face-bow hinge axis is incorrectly placed superior to the true<br />
hinge axis, the lower cast will occlude in a more protrusive<br />
direction, with premature contacts on the anterior teeth.<br />
If the arbitrary earpiece face-bow hinge axis is incorrectly<br />
placed inferior to the true hinge axis, the lower cast will occlude<br />
in a more distal direction, with premature contacts on<br />
the posterior teeth. 43 This conclusion resembles the findings<br />
<strong>of</strong> Gordon et al. Weinberg and Fox drew similar conclusions;<br />
the values they obtained for calculated horizontal error in<br />
cusp heights closely resembled each other. 35,44 This suggests<br />
that errors <strong>of</strong> several millimeters in axis location might produce<br />
occlusal errors that are clinically intolerable on the part<br />
<strong>of</strong> the patient. 43<br />
The authors <strong>of</strong> the present study found a mean difference<br />
in incisor position <strong>of</strong> 3.04 mm. The occlusal discrepancies<br />
found in the present study suggest that a range greater<br />
than 5 mm existed between hinge axis points located with<br />
the arbitrary earpiece face- bow mounting and the true hinge<br />
face-bow. The discrepancy in maxillary cast position found<br />
in this study might possibly introduce a change in the closure<br />
<strong>of</strong> the mandible into occlusion. The problems caused<br />
by the occlusal errors resulting from inaccurate location <strong>of</strong><br />
the hinge axis point are illustrated in Figure 10. The photos<br />
suggest an exaggerated discrepancy between the two casts<br />
because two completely different face-bow techniques were<br />
used. They serve to illustrate occlusal error that may result<br />
from error in maxillary cast position. In some cases, however,<br />
the autorotated mandibular casts closed with only a<br />
small degree <strong>of</strong> occlusal error (Figure 9). Other casts showed<br />
severe positional changes resulting in larger occlusal errors<br />
when this was attempted. (Figure10).<br />
Figure 10-a Mounted maxillary estimated cast vs.<br />
true hinge mounted maxillary cast: True hinge mounting.<br />
Figure 10-b Mounted maxillary estimated cast vs.<br />
true hinge mounted maxillary cast: Estimated hinge mounting<br />
substituted for true hinge maxillary mounting.<br />
It may be difficult to detect which patients have arbitrary<br />
earpiece face-bow hinge points naturally located within<br />
5 mm <strong>of</strong> their true hinge point. Therefore, if any degree <strong>of</strong><br />
accuracy is needed or if any change in vertical dimension,<br />
such as an occlusal equilibration or orthognathic surgery, is<br />
planned, use <strong>of</strong> a true hinge axis face-bow should be considered.<br />
Previous studies have suggested that location <strong>of</strong> a<br />
kinematic true hinge axis point prior to treatment for dentulous<br />
patients who require extensive treatment saves time and<br />
results in a more satisfactory occlusion. 6 The present study<br />
found a statistically significant difference in the maxillary<br />
cast position in all three planes <strong>of</strong> space between the two<br />
face-bow techniques compared.<br />
Conclusions<br />
1. Statistically significant differences (p < .001) were<br />
found between the true hinge face-bow mounted maxillary<br />
cast and the estimated earpiece face-bow hinge mounted max-<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
53
illary cast in the vertical dimension, with a mean <strong>of</strong> 2.19 mm<br />
for the maxillary right first molar, 2.45 mm for the maxillary<br />
left first molar, and 1.90 mm for the maxillary right central<br />
incisor.<br />
2. Statistically significant differences (p < .001) were<br />
found between the true hinge face-bow mounted maxillary<br />
cast and the estimated earpiece face-bow hinge mounted<br />
maxillary cast in the A-P direction, with a mean difference<br />
<strong>of</strong> 3.82 mm between the maxillary right first molars, 3.10<br />
mm between the maxillary left first molars, and 3.05 mm<br />
between the maxillary right central incisors.<br />
3. Statistically significant differences (p < .001) were<br />
found between the true hinge face-bow mounted maxillary<br />
cast and the estimated earpiece face-bow hinge mounted<br />
maxillary cast in the transverse dimension, with a 2.23-mm<br />
difference between the maxillary right first molars and a<br />
2.60-mm difference between the maxillary left first molars.<br />
4. This study found that there is a significant difference<br />
between the arbitrary earpiece face-bow hinge axis and<br />
the true hinge face-bow hinge aixs. Thus, when an arbitray<br />
earpiece face-bow hinge axis transfer is used, the maxillarymandibular<br />
complex is placed in an incorrect position in the<br />
articulator. The end result is a lack <strong>of</strong> functional harmony. ■<br />
References<br />
1. McCollum BB. The mandibular hinge axis and a method <strong>of</strong> locating<br />
it. J Prosthet Dent. 1960;(10): 430-435.<br />
2. Okeson JP. Functional Anatomy and Biomechanics <strong>of</strong> the Masticatory<br />
System: Management <strong>of</strong> Temporomandibular Disorders and Occlusion.<br />
4th ed. St. Louis, MO: Mosby; 1998: 3-38.<br />
3. <strong>Roth</strong> RH. Functional occlusion for the orthodontist. J Clin Orthod.<br />
1981;(15):32-51.<br />
4.Posselt, U. Terminal hinge movement <strong>of</strong> the mandible. J Prosthet<br />
Dent. 1957;(7): 787-796.<br />
5. Glossary <strong>of</strong> prosthodontic terms. J Prosthet Dent. 1987; (58): 721.<br />
6. Gordon SR, St<strong>of</strong>fer WM, Connor SA. Location <strong>of</strong> the terminal hinge<br />
axis and its effect on the second molar cusp position. 1984;(52): 99-<br />
105.<br />
7. Starcke EN. The history <strong>of</strong> articulators: from face-bows to the<br />
gnathograph, a brief history <strong>of</strong> early devices developed for recording<br />
condylar movement, Part II. J Prosthet Dent. 2002;(11): 53-62.<br />
8. Winstanley RB. The hinge-axis: a review <strong>of</strong> the literature. J Oral<br />
Rehab. 1985;(12): 135-139.<br />
9. Klar NA, Kulbersh R, Freeland TD, Kaczynski R. Maximum tntercuspation-<br />
centric relation disharmony in 200 consecutively finished cases in<br />
a gnathologically oriented practice. Semin in Orthod. 2003;(9): 109-116.<br />
54 Freeland et al | Comparison <strong>of</strong> Maxillary Cast Positions<br />
10. Trapozzano VR, Lazzari JB. The physiology <strong>of</strong> the terminal<br />
rotational position <strong>of</strong> the condyles in the temporomandibular joint. J<br />
Prosthet Dent. 1967;(17): 122-133.<br />
11. Trapozzano VR, Lazzari JB. A study <strong>of</strong> hinge axis determination. J<br />
Prosthet Dent. 1961;(11): 858-863.<br />
12. Ferrario VF, Sforza C, Miani A, Serrao G, Tartaglia G. Open-close<br />
movements in the human temporomandibular joint: does a pure<br />
rotation around the intercondylar hinge axis exist? J Oral Rehab.<br />
1996;(23): 401-408.<br />
13. Hellsing G, Hellsing E, Eliasson S. The hinge axis Concept: a radiographic<br />
study <strong>of</strong> its relevance. J Prosthet Dent. 1995; (73): 60-64.<br />
14. Bowley JF, Michaels GC, Lai TW, Lin PP. Reliability <strong>of</strong> a face-bow<br />
transfer procedure. J Prosthet Dent. 1992;(67): 491-498.<br />
15. Bowley JF, Pierce CJ. Reliability and validity <strong>of</strong> a transverse horizontal<br />
axis location instrument. J Prosthet Dent. 1990;(64): 646-650.<br />
16. Strohaver, RA. A comparison <strong>of</strong> articulator mountings made with<br />
centric relation and myocentric position records. J. Prosthet Dent.<br />
1972;(28): 379-390.<br />
17. Aull AE. A study <strong>of</strong> the transverse axis. J. Prosthet Dent. 1963;(13):<br />
469-479.<br />
18. Borgh O, Posselt U. Hinge axis registration: experiments on the<br />
articulator. J Prosthet Dent. 1958;(8): 35-40.<br />
19. Beard CC, Clayton JA. Studies on the validity <strong>of</strong> the terminal hinge<br />
axis. J Prosthet Dent. 1981;(46): 185-191.<br />
20. Abdal-Hadi L. The hinge axis: evaluation <strong>of</strong> current arbitrary<br />
determination methods and a proposal for a new recording method. J<br />
Prosthet Dent. 1989;(62): 463-467.<br />
21. Razek MKA. Clinical evaluation <strong>of</strong> methods used in locating the<br />
mandibular hinge axis. J Prosthet Dent. 1981;(46): 369-373.<br />
22. Choi DG, Bowley JF, Marx DB, Lee S. Reliability <strong>of</strong> an ear-bow<br />
arbitrary face-bow transfer instrument. J Prosthet Dent. 1999;(82):<br />
150-156.<br />
23. Nagy WW, Smithy TJ, Wirth CG. Accuracy <strong>of</strong> a predetermined<br />
transverse horizontal mandibular axis point. J Prosthet Dent.<br />
2002;(87): 387-393.<br />
24. Piehslinger E. Reproducibility <strong>of</strong> the condylar reference position. J<br />
Or<strong>of</strong>ac Pain. 1993;(7): 68-75.<br />
25. Proschel PA, Nat R, Maul T, Morneburg T. Predicted incidence <strong>of</strong><br />
excursive occlusal errors in common modes <strong>of</strong> articulator adjustment.<br />
J. Prosthet Dent. 2000;(13): 303-310.<br />
26. Schallhorn RG. A study <strong>of</strong> the arbitrary center and the kinematic<br />
center <strong>of</strong> rotation for face-bow mountings. J Prosthet Dent. 1957;(7):<br />
162-169.<br />
27. Wood DP, Korne PH. Estimated and true hinge axis: a comparison<br />
<strong>of</strong> condylar displacements. Angle Orthod. 1992;(62): 167-175.
28. Goska JR, Christensen LV. Comparison <strong>of</strong> cast positions by using<br />
four face-bows. J Prosthet Dent. 1988;(59): 42-44.<br />
29. Simpson, JW, Hesby RA, Pfeifer DL, Pelleu GB. Arbitrary mandibular<br />
hinge axis locations. J Prosthet Dent. 1984;(51):819-823<br />
30. Lauritzen AG, Bodner GH. Variations in location <strong>of</strong> arbitrary and<br />
true hinge axis points. J Prosthet Dent. 1961;(11): 224-229.<br />
31. Palik JF, Nelson DR, White JT. Accuracy <strong>of</strong> an earpiece face-bow. J<br />
Prosthet Dent. 1985;(53): 800-804.<br />
32. Schulte JK, Rooney DJ, Erdman AG. The hinge axis transfer procedure:<br />
a three-dimensional error analysis. J Prosthet Dent. 1984;(51):<br />
247-251.<br />
33. Morneburg TR, Proschel PA. Predicted incidence <strong>of</strong> occlusal errors<br />
in centric closing around arbitrary axes. Int J Prosthod. 2002;(15):<br />
358-364.<br />
34. Ricketts, RM, Perspectives in the Clinical Application <strong>of</strong> Cephalometrics.<br />
Angle Orthod. 1981;(51): 115-150.<br />
35. Weinberg LA. An evaluation <strong>of</strong> the face-bow mounting. J Prosthet<br />
Dent. 1961;(11): 32-42.<br />
36. Adrien P., Schouver J., Methods for minimizing the errors<br />
in mandibular model mounting on an articulator. J Oral Rehab.<br />
1997;(24):929-935.<br />
37. Brotman DN. Hinge axes, part I: the transverse hinge axis. J Prosthet<br />
Dent. 1960;(10): 436-440.<br />
38. Preston JD. A reassessment <strong>of</strong> the mandibular transverse horizontal<br />
axis theory. J Prosthet Dent. 1979; 41: 605-613.<br />
39. Teteruck WR. Lundeen HC. The accuracy <strong>of</strong> an ear face-bow. J<br />
Prosthet Dent. 1966;(16):1039-1046.<br />
40. Walker PM. Discrepancies between arbitrary and true hinge axes. J<br />
Prosthet Dent. 1980;(43): 279-285.<br />
41. Zuckerman GR. The geometry <strong>of</strong> the arbitrary hinge axis as it<br />
relates to the occlusion. J Prosthet Dent. 1982;(48): 725-733.<br />
42. Collett Henry A. The movements <strong>of</strong> the temporomandibular<br />
joint and their relation to the problems <strong>of</strong> occlusion. J Prosthet Dent.<br />
1955;(5): 486-496.<br />
43. Brotman DN. Hinge Axes, ,part II: geometric significance <strong>of</strong> the<br />
transverse axis. J Prosthet Dent. 1960;(10): 631-636.<br />
44. Fox SS. The significance <strong>of</strong> errors in hinge axis location. J Am Dent<br />
Assoc. 1967;(74):1262-1272.<br />
45. <strong>Williams</strong>on EH, Evans DL, Barton WA, <strong>Williams</strong> BH. The effect<br />
<strong>of</strong> bite plane use <strong>of</strong> terminal hinge axis location. Angle Orthod.<br />
1977;(47): 25-33.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
55
Notes<br />
56 Notes
The Effect <strong>of</strong> Tooth Wear on Postorthodontic Pain Patients: Part 2<br />
Jina Lee Linton, DDS, MA, PhD, ABO ■ Woneuk Jung, DDS<br />
Jin a Le e Li n T o n , ddS, ma, Phd, abo<br />
jinalinton@hotmail.com<br />
■ Graduated from Yonsei University<br />
(DDS, PhD), 1986<br />
■ Graduated from Columbia University,<br />
SDOS, 1988<br />
■ Graduated from Columbia University<br />
Orthodontic Department (MA), 1991<br />
■ Private Practice in Seoul, Korea,<br />
1991–present<br />
Wo n e u K Ju n G , ddS<br />
■ Graduated from Dan Kook<br />
University, 1991<br />
■ Private practice in Seoul, Korea,<br />
1991–present<br />
Introduction<br />
Tooth attrition is classified as tooth disease under the Inter-<br />
national Classification <strong>of</strong> Diseases, published by the World<br />
Health Organization. According to Jablonski, tooth attrition<br />
takes place when tooth-to-tooth contact, as in mastication,<br />
occurs on the occlusal, incisal, and proximal surfaces. 1 It is<br />
differentiated from tooth abrasion (the pathologic wearing<br />
away <strong>of</strong> the tooth substance by friction, as brushing, bruxism,<br />
clenching, and other mechanical causes) and from tooth<br />
erosion (the loss <strong>of</strong> substance caused by chemical action<br />
without bacterial action).<br />
In reality, the wear may be related to a combination <strong>of</strong><br />
factors including attrition, abrasion, and erosion; that is,<br />
physical-mechanical and chemical effects can have an impact<br />
on the loss <strong>of</strong> physiologic and habitual tooth surface morphology.<br />
2 Grippo et al state that three physical and chemical<br />
mechanisms are involved in the etiology <strong>of</strong> tooth surface lesions.<br />
These mechanisms are stress, corrosion, and friction.<br />
The various types <strong>of</strong> dental lesion are caused by these mechanisms<br />
acting either alone or in combination. Friction, including<br />
abrasion (which is exogenous) and attrition (which is<br />
endogenous), leads to the dental manifestation <strong>of</strong> wear. Corrosion<br />
leads to the dental manifestation <strong>of</strong> chemical or elec-<br />
Summary<br />
Malocclusion and occlusal interference in excursive movement is the major<br />
cause <strong>of</strong> pathologic tooth wear. Tooth wear starts with shortening <strong>of</strong> the anterior<br />
teeth. As interference in mandibular movement increases, the posterior<br />
teeth gradually become more flat. Recognizing tooth wear before and after<br />
orthodontic treatment is important for retention <strong>of</strong> the treated result and for<br />
ensuring functional occlusion. For this reason, orthodontic treatment should<br />
be detailed and completed with restorative rehabilitation <strong>of</strong> the lost tooth<br />
material.<br />
trochemical degradation. Stress, which results in compression,<br />
flexure, and tension, leads to the dental manifestation<br />
<strong>of</strong> micr<strong>of</strong>racture. 3<br />
Loss and excessive wear <strong>of</strong> hard dental tissues is a permanent<br />
problem <strong>of</strong> the dentition, especially in the modern<br />
man; it is found in almost all age groups. Tooth wear is an<br />
inherent part <strong>of</strong> the aging process; it occurs continuously but<br />
slowly throughout life. In some individuals, tooth wear occurs<br />
more rapidly than in others, leading to severe morphologic,<br />
functional, and vital damage to the teeth, which cannot<br />
be considered normal. 4 Hand et al found that in a sample <strong>of</strong><br />
520 adults, 84.2% had enamel attrition, 72.9% had dentin<br />
attrition, and 4.2% had severe attrition. 5 In cases <strong>of</strong> severe<br />
attrition, Sivasithamparam et al found that 11.6% <strong>of</strong> 448<br />
adult patients had either near-pulpal exposures or frank pulpal<br />
exposures. 6<br />
Schneider and Peterson found that 15% <strong>of</strong> children<br />
demonstrate tooth wear due to bruxism. 7 Most <strong>of</strong> the prevalence<br />
studies in Europe and North America indicate that the<br />
prevalence <strong>of</strong> wear on enamel in children is common (up to<br />
60% involvement), while the prevalence <strong>of</strong> exposed dentin<br />
varies from 2% to 10%. 8,9<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
57
Case Reports<br />
The six cases below show individual clinical cases with various<br />
severity <strong>of</strong> attrition with or without treatment.<br />
Case 1: Attrition Occurred With no Orthodontic Treatment<br />
An 11-year-old female came in for checkup in April 2006,<br />
at which time the upper lateral incisor edges and canine tips<br />
showed wear (Figure 1). She had class I canine and molar<br />
relationships and a 3-mm overbite and overjet (April 2006).<br />
When she came back for orthodontic treatment 3 years later<br />
(January 2009), the wear on the laterals and canines had<br />
progressed significantly (red arrows).<br />
Figure 1 Attrition occurred with no orthodontic treatment.<br />
Case 2: Attrition Occurred During Orthodontic Treatment<br />
A 12-year-old male had a crossbite on the left laterals and an<br />
open bite on the central incisors (Figure 2). His canines and<br />
molars were in class I relationship (September 2002). After<br />
a year and a half without treatment, the upper left canine<br />
showed slight wear on the mesial side (January 2004). After<br />
8 months <strong>of</strong> fixed appliance therapy, that canine showed<br />
marked flattening on the tip (October 2004).<br />
Figure 2 Attrition occurred during orthodontic treatment.<br />
58 Linton, Jung | The Effect <strong>of</strong> Tooth Wear on Postorthodontic Pain Patients: Part 2<br />
Case 3: No Attrition Occurred During Orthodontic Treatment<br />
A 17-year-old male had class II div. 2 malocclusion (Figure<br />
3) and displayed no wear on the upper right canine tip (September<br />
1995). After 22 months <strong>of</strong> treatment with mandibular<br />
advancement surgery, the sharp canine tip remained (July<br />
1997).<br />
Figure 3 No attrition occurred during orthodontic treatment.<br />
Case 4: Slight Attrition Occurred During Orthodontic<br />
Treatment<br />
A 13-year-old male with class I malocclusion came in presented<br />
with sharp upper canine tips (June 1998). After 1½<br />
years <strong>of</strong> fixed-appliance therapy (January 2000), the right<br />
canine tip remained intact (blue arrow), while the left canine<br />
tip showed wear. A photograph taken 2 years posttreatment<br />
(January 2002) showed wear on the right canine<br />
tip (Figure 4).
Figure 4 Slight attrition occurred during orthodontic treatment.<br />
Case 5: No Attrition Occurred During or Following<br />
Orthodontic Treatment<br />
A 24-year-old female came in for treatment <strong>of</strong> bimaxillary<br />
dentoalveolar protrusion (June 1998). The canine tip remained<br />
the same immediately after orthodontic treatment<br />
(April 2001) and 7 years posttreatment (April 2008). This patient<br />
had no apparent anterior tooth attrition over the 10-year<br />
observation period (Figure 5). On lateral excursive movement,<br />
canine guidance existed with adequate separation <strong>of</strong> posterior<br />
teeth on both the chewing and the nonchewing sides.<br />
Figure 5 No attrition occurred during or after orthodontic treatment.<br />
Case 6: Attrition Occurred During Orthodontic Treatment<br />
A 13-year-old male came to the clinic in January 2000 for<br />
treatment <strong>of</strong> protruding upper incisors. The patient’s face<br />
showed a protrusive upper lip and a normal-size mandible,<br />
with no apparent asymmetry. He had class II malocclusion<br />
with maxillary dentoalveolar protrusion, severe crowding<br />
in the upper and lower arches, and a constricted maxillary<br />
arch. The upper right canine had not erupted due to lack <strong>of</strong><br />
space, even though the root had almost formed (Figure 6).<br />
Figure 6 Preorthodontic treatment photographs and x-rays.<br />
Figure 6-a Front facial<br />
smiling photograph.<br />
Figure 6-b Lateral facial<br />
photograph showing lip<br />
protrusion and strained<br />
mentalis muscle.<br />
Figure 6-c Right lateral intraoral photograph<br />
showing class II molar relationship in MIP.<br />
Figure 6-d Front intraoral photograph in MIP showing<br />
crowding and crossbite in the upper right lateral incisor.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
59
Figure 6-e Left lateral intraoral photograph in MIP showing<br />
class II molar relationship and retained deciduous canine.<br />
Figure 6-f Panoramic x-ray. The upper left canine showing<br />
root apex almost formed, but not erupted, due to lack <strong>of</strong> space.<br />
Figure 6-g Lateral cephalogram showing slightly<br />
retrusive mandible and protrusive upper incisors.<br />
Jarabak’s cephalometric analysis showed a strong counterclockwise<br />
growth tendency expressed in such measurements<br />
as a posterior facial height-anterior facial height ratio<br />
<strong>of</strong> 70%, a long ramus height in comparison to the posterior<br />
cranial base length, and a small Y-axis-to-SN angle (Table 1).<br />
60 Linton, Jung | The Effect <strong>of</strong> Tooth Wear on Postorthodontic Pain Patients: Part 2<br />
Table 1 Jarabak’s analysis <strong>of</strong> case 6 in January 2000.<br />
The maxillary arch was rapidly expanded with a fixed-<br />
type expander, which was retained for 6 months. Growth<br />
modification <strong>of</strong> the maxillary protrusion was accomplished<br />
simultaneously with a high-pull headgear for 10 months. The<br />
diagnostic study models mounted before and after headgear<br />
therapy clearly showed the effect <strong>of</strong> the growth modification<br />
treatment (Figure 7).<br />
Figure 7 Mounted models <strong>of</strong> the case before and after the<br />
first phase <strong>of</strong> growth modification treatment. The models were<br />
mounted on a semiadjustable articulator with estimated<br />
face-bow transfer and with centric relation bite registration<br />
records. The class II relationship <strong>of</strong> the first molars (blue lines)<br />
in January 2001, was improved compared to the molar<br />
relationship <strong>of</strong> the case in January 2000.<br />
Subsequent to headgear therapy, the four first premolars<br />
were extracted, and the patient received fixed-appliance<br />
therapy for the following 20 months. Class I canine and<br />
molar relationships were achieved with maximum anchorage<br />
in the upper arch and moderate anchorage in the lower<br />
arch in December 2002. The patient’s facial appearance was
improved, with retraction <strong>of</strong> the upper anterior teeth and<br />
favorable mandibular growth (Figure 8).<br />
Figure 8-a Front facial<br />
smiling photograph.<br />
Figure 8 Postorthodontic treatment records.<br />
Figure 8-b Lateral facial<br />
photograph showing<br />
improvement in pr<strong>of</strong>ile<br />
compared to Figure 1b.<br />
Figure 8-c Right lateral intraoral photograph showing<br />
that class I canine and molar relationships were achieved.<br />
Figure 8-d Front intraoral photograph showing<br />
that approximately 2 mm <strong>of</strong> overjet was achieved.<br />
Figure 8-e Left lateral intraoral photograph showing<br />
that class I canine and molar relationships were achieved.<br />
Figure 8-f Maxillary arch showing alignment<br />
without any extraction spaces left.<br />
Figure 8-g Panoramic x-ray showing overcorrection in<br />
root angulation <strong>of</strong> the canines and developing third molars.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
61
Figure 8-h Lateral cephalogram.<br />
Figure 8-i Superimposition <strong>of</strong> cephalometric tracings before<br />
(black line) and after (red line) orthodontic treatment shows<br />
that maximum anchorage control <strong>of</strong> the upper molars was<br />
accomplished. The maxilla and the mandible grew<br />
downward and forward as predicted.<br />
62 Linton, Jung | The Effect <strong>of</strong> Tooth Wear on Postorthodontic Pain Patients: Part 2<br />
The patient returned to the clinic for correction <strong>of</strong> lower<br />
anterior tooth crowding at age 20 in April 2008 (Figure 9).<br />
Figure 9 Four-year retention photographs.<br />
Figure 9-a Front facial<br />
smiling photograph showing<br />
well-developed gonial angle.<br />
Figure 9-b Lateral facial<br />
photograph.<br />
Figure 9-c Right lateral intraoral photograph showing that<br />
class I canine and molar relationships were retained.<br />
Figure 9-d Front intraoral photograph showing that the<br />
lower dental midline was shifted 2 mm to the left.
Figure 9-e Left lateral intraoral photograph<br />
showing end-on class II canine relationship.<br />
Figure 9-f Panoramic x-ray.<br />
Figure 9-g Lateral cephalogram.<br />
Figure 9-h Superimposition <strong>of</strong> the cephalometric tracings<br />
after orthodontic treatment (red line) and 4-year retention<br />
(green line), showing that there was little change in the<br />
s<strong>of</strong>t-tissue and hard-tissue structures.<br />
Upon clinical examination, wear on the maxillary canine<br />
tips was noted as being quite severe for his age. Upon further<br />
questioning, the patient complained <strong>of</strong> occasional headache<br />
and pain in the area <strong>of</strong> the temporomandibular joint (TMJ).<br />
His static occlusion showed 1.5 mm <strong>of</strong> overbite at the central<br />
incisors and no overbite on the left lateral incisor. The lower<br />
anterior teeth were tipped to the left side, resulting in a lower<br />
midline shift to the left side. Dentin exposures were present<br />
on the upper lateral incisal edges and the lower anterior<br />
teeth. The upper and lower first molars also showed marked<br />
wear on the cusp tips. Upon excursive movement <strong>of</strong> both<br />
right and left sides <strong>of</strong> the madible, the posterior teeth on the<br />
chewing side showed simultaneous contacts—that is, group<br />
function—and teeth on the nonchewing side showed harmful<br />
contacts (Figure 10).<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
63
Figure 10 Mandibular movements.<br />
Figure 10-a Due to wear on the canine tip, there are multiple<br />
tooth contacts on the right chewing side and harmful contacts<br />
on the left nonchewing side during the right chewing movement.<br />
Figure 10-b Incisive movement indicates<br />
multiple contacts on the posterior teeth.<br />
Figure 10-c Due to wear on the canine tip, there are multiple<br />
tooth contacts on the left chewing side and harmful contacts on<br />
the right nonchewing side during the left chewing movement.<br />
64 Linton, Jung | The Effect <strong>of</strong> Tooth Wear on Postorthodontic Pain Patients: Part 2<br />
The patient’s records were reviewed to compare the<br />
amount <strong>of</strong> tooth wear at age 15 immediately after orthodontic<br />
treatment (December 2002) with the amount <strong>of</strong> tooth<br />
wear at age 20 (Figure 11).<br />
Figure 11 Comparison <strong>of</strong> tooth wear over a 5-year period.<br />
Progression <strong>of</strong> tooth wear from 1.5 mm <strong>of</strong> vertical overbite<br />
in the upper and lower canines in December 2002 down to<br />
minimum vertical overbite in April 2008.<br />
(Red arrows indicate flattened anterior teeth.)<br />
The canine tips already showed wear at age 15. Progression<br />
<strong>of</strong> tooth wear was evident; 1.5 mm <strong>of</strong> vertical overbite in<br />
the upper and lower canines in December 2002 was reduced<br />
down to minimum vertical overbite in April 2008. The occlusal<br />
views showed the beginning <strong>of</strong> dentin exposure on the<br />
upper lateral incisors and the canines. The first molar wear<br />
caused no obvious incisal changes but the progression <strong>of</strong> the<br />
wear was definitely observable as wider wear facets and dimples<br />
on the molar cusp tips in April 2008 (Figure 12).<br />
Figure 12 Occlusal views <strong>of</strong> tooth wear. Wear on the posterior<br />
teeth is less apparent than wear on the anterior teeth. On close<br />
examination, tooth wear (red arrows) is shown as facets or<br />
dimples on the cusp tips.
All available intraoral photographs that had been taken<br />
in the past were put together to analyze the event <strong>of</strong> tooth<br />
wear in this patient (Figure 13).<br />
Figure 13 The event <strong>of</strong> upper canine wear during orthodontic<br />
treatment. The right canine shows definite wear (red arrows)<br />
during fixed-appliance therapy. The sharp anatomy (blue circle)<br />
<strong>of</strong> the left canine tip at the time <strong>of</strong> eruption is shown in the<br />
photograph (May 2000). It was gone before the<br />
fixed-appliance therapy.<br />
The upper right canine showed no wear before the<br />
initial stage <strong>of</strong> fixed-appliance therapy in June 2001. The<br />
canine wear occurred sometime during the following 8<br />
months, and further wear seemed to have occurred between<br />
February 2002 and December 2002. The upper left canine<br />
erupted with sharp anatomy in May 2000. However, the tip<br />
was worn down already on the day <strong>of</strong> bracket bonding, and<br />
the wear progressed during the fixed-appliance therapy. In<br />
the absence <strong>of</strong> anatomy at the cusp tips and incisal edges, as<br />
in Figures 3-c and 3-e, proper anterior guidance and canine<br />
guidance in movement would not have taken place (Figure<br />
14). This in turn would have caused further wear with the<br />
passage <strong>of</strong> time, as shown in Figures 6 and 7. 10<br />
Figure 14 Mandibular movement <strong>of</strong> the mounted models.<br />
Figure 14-a Intraoral movement shown in Figure 5-a was<br />
reproduced with models mounted on a semiadjustable<br />
articulator in SCP. There were nonchewing-side interferences<br />
<strong>of</strong> the functional cusps <strong>of</strong> the upper left molars (red arrows).<br />
Figure 14-b Intraoral movement shown in Figure 5-b was reproduced<br />
using models. There were nonchewing-side interferences<br />
<strong>of</strong> the functional cusps <strong>of</strong> the right upper molars (red arrows).<br />
Stable condylar position (SCP) could not be recorded in<br />
the presence <strong>of</strong> dysfunction <strong>of</strong> the masticatory system, 11 so<br />
a maxillary anterior-guided orthosis12 was prepared and the<br />
patient wore it for 2 months, until all clinical signs and symptoms<br />
<strong>of</strong> TMJ dysfunction disappeared. The orthosis (Figure<br />
15) allowed the condyles to assume their superior, anterior,<br />
and medial (SAM) positions in intimate contact with the<br />
thinnest part <strong>of</strong> the biconcavity <strong>of</strong> the disc, and made possible<br />
the diagnosis <strong>of</strong> a SCP from the maximum intercuspal<br />
position (MIP). The SCP was recorded with Axi-Path recording,<br />
so the mounted models would arc close in centric. 13,14<br />
Figure 15 Maxillary anterior guided orthosis. The patient<br />
wore the removable plate continuously until all the<br />
symptoms disappeared and SCP was obtained.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
65
Subtractive coronaplasty 15 was done on the posterior<br />
teeth to achieve equal stops and maximum intercuspation in<br />
SCP, and to preserve the natural tooth forms (Figure 16).<br />
Figure 16 Before and after coronaplasty.<br />
Figure 16-a The maxillary arch after coronaplasty shows<br />
that coronaplasty does not necessarily flatten the occlusal<br />
surfaces. Rather, it can redefine the anatomy.<br />
Figure 16-b The mandibular arch after coronaplasty also<br />
shows redefined anatomic form <strong>of</strong> the posterior teeth.<br />
Anterior maxillary and mandibular teeth were built up<br />
with wax on the diagnostic casts to relegate all eccentric<br />
tooth contacts to the anterior teeth (Figure 17).<br />
The additive coronaplasty was done by duplicating the<br />
wax-up <strong>of</strong> the casts on the anterior teeth with composite<br />
resin (Figure 18). 16<br />
Figure 17 Wax-up on the mounted model to achieve 3 mm to 4<br />
mm <strong>of</strong> vertical overbite and 2 mm to 3 mm <strong>of</strong> horizontal overjet.<br />
Figure 18 Additive coronaplasty was done with a hybrid-type<br />
composite resin on each anterior tooth according to the<br />
wax-up in Figure 12.<br />
66 Linton, Jung | The Effect <strong>of</strong> Tooth Wear on Postorthodontic Pain Patients: Part 2<br />
The average unworn maxillary central incisor is approx-<br />
imately 12 mm and the mandibular central incisors are 10<br />
mm according to the American Academy <strong>of</strong> Cosmetic Dentistry<br />
(AACD). In the patient’s case, they were 12 mm and<br />
7.7 mm and were restored to 12.3 mm and 9.8 mm respectively<br />
(Figure 19). 17<br />
Figure 19 Measurements <strong>of</strong> the teeth before and after positive<br />
coronaplasty. The upper central incisors were 12.0 mm long<br />
and became 12.3 mm long. The lower central incisor was<br />
7.7 mm long and became 9.8 mm long.<br />
According to Lee, adequate anterior guidance can be obtained<br />
with incisor vertical overlap <strong>of</strong> 3 mm to 4 mm and<br />
horizontal overlap <strong>of</strong> 2 mm to 3 mm. 18 Initially in April 2008<br />
the patient’s MIP and SCP did not coincide and his overjet<br />
was 2 mm. In SCP the overjet increased to 3.5 mm, which was<br />
corrected to 2 mm with additive coronaplasty (Figure 20).<br />
Figure 20 Overjet change after coronaplasty. When MIP<br />
and SCP did not coincide, the overjet was 2 mm. In SCP,<br />
the overjet increased to 3.5 mm, which was corrected<br />
to 2 mm with additive coronaplasty.<br />
Only after additive coronaplasty could a complete elimination<br />
<strong>of</strong> eccentric occlusal interferences be achieved with<br />
excursive movements <strong>of</strong> the mandible (Figure 21).
Figure 21 Mandibular movement after coronaplasty.<br />
Figure 21-a In the right chewing movement, both the chewing<br />
and the nonchewing sides show sufficient clearance between<br />
the upper and lower posterior teeth (blue arrows).<br />
Figure 21-b In the left chewing movement, both the chewing and<br />
the nonchewing sides show sufficient clearance (blue arrows).<br />
With coronaplasty the patient’s bite was stable, and the<br />
patient was pleased with his smile and with the overall appearance<br />
<strong>of</strong> his face (Figure 22).<br />
The abnormal tooth wear the patient demonstrated before<br />
coronaplasty was due to improper incisal guidance and<br />
canine guidance. Since tooth wear progresses much faster in<br />
the dentin layer than in enamel, his entire dentition would<br />
have become significantly shorter over the next 10 to 20<br />
years, if no intervention had taken place. The patient’s occlusion<br />
was completed with coronaplasty, and the longevity<br />
and stability <strong>of</strong> his dentition were greatly enhanced.<br />
Discussion<br />
At the present, the majority <strong>of</strong> dentists believe that teeth<br />
can successfully compensate for the loss <strong>of</strong> tissue by migration<br />
and elongation, and that these do not disturb the basic<br />
functions <strong>of</strong> the masticatory system (mastication, speech,<br />
and swallowing). 19 However, some researchers have argued<br />
that anatomical tooth form plays an important role in the<br />
proper function <strong>of</strong> the masticatory system. 17,18 Knight and<br />
et al conducted a longitudinal study on 223 orthodontically<br />
treated patients 20 years posttreatment. They found that<br />
there was a strong relationship between incisal and occlusal<br />
tooth wear during the mixed dentition and subsequent<br />
wear <strong>of</strong> the adult dentition. 20 Tooth wear that occurred during<br />
the mixed dentition in these subjects actually occurred<br />
on the permanent incisors. Even though the malocclusion<br />
was corrected, the loss <strong>of</strong> tissue due to wear in the previously<br />
affected teeth persisted. Consequently, the patients’<br />
incomplete anterior and canine guidance systems continued<br />
to influence their permanent dentition.<br />
Figure 22 Comparison <strong>of</strong> the case before and after coronaplasty.<br />
Figure 22-a Full-smile facial photograph taken after<br />
coronaplasty shows that the patient’s smile became<br />
more esthetically pleasing.<br />
Figure 22-b Lateral facial photographs taken<br />
before and after coronaplasty show little change.<br />
With regard to interferences in mandibular movement,<br />
Masatoshi and Masanori studied occlusal factors in relation<br />
to TMD in 146 young adults; they concluded that molarguided<br />
occlusion patterns were associated with a high risk<br />
<strong>of</strong> TMD. 21 All subjects with TMD had nonchewing interferences<br />
in border excursions and in tooth-dictated excursions.<br />
Without additive coronaplasty to restore the lost volume <strong>of</strong><br />
tooth material, complete elimination <strong>of</strong> interferences may<br />
not be possible, nor may it be possible to maintain the optimal<br />
health <strong>of</strong> the teeth. 16 As we saw in case 6, the teeth<br />
were too worn down to allow for adequate function, and<br />
the post-orthodontic result was an incomplete occlusion vulnerable<br />
to relapse. The patient’s TMJ symptoms would have<br />
persisted, and the attrition process would have accelerated<br />
once the dentin layer was exposed. Tooth wear that occurred<br />
while the patient was receiving treatment was unavoidable in<br />
this case. Early intervention <strong>of</strong> malocclusion in mixed denti-<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
67
tion might have enabled us to circumvent pathologic tooth<br />
wear while the patient was undergoing treatment?<br />
In canine guidance, the horizontal forces are minimized<br />
by limiting the contact <strong>of</strong> the supporting cusps with their opposing<br />
fossae at or near their intercuspal position. All other<br />
lateral contacts are prevented by the steeper inclination <strong>of</strong><br />
the canines. This causes the chewing movement to be more<br />
vertical in the frontal view. Case 5 exemplifies the preservation<br />
<strong>of</strong> tooth material in the presence <strong>of</strong> functional occlusion.<br />
Upon lateral excursive movements, the canine guidance<br />
provided sufficient clearance in the posterior teeth.<br />
Many <strong>of</strong> our orthodontic patients already have worn<br />
canines and incisors. Occlusal interferences, premature contacts,<br />
and habitual bruxism and/or clenching all may act as<br />
stressors. Tooth contact during swallowing occurs 2,400<br />
times a day, according to Straub23 and Kydd. 24 These repetitive<br />
static and cyclic occlusal loads could also cause wear<br />
on the anterior, as well as the posterior, teeth. Although it is<br />
difficult to quantify the amount <strong>of</strong> tooth wear precisely, especially<br />
in cross-sectional studies, orthodontists can appraise<br />
attrition <strong>of</strong> the incisal edges and canine tip most easily from<br />
intraoral photographs. Why should orthodontists be aware<br />
<strong>of</strong> tooth wear? What happens if the dentist ignores if they<br />
ignore the problem? These are important questions, because<br />
any patient who is not informed <strong>of</strong> tooth surface loss is put<br />
at risk <strong>of</strong> having no choice in treating what can become a<br />
severe condition. ■<br />
References<br />
1. Jablonski, S. Jablonski’s Dictionary <strong>of</strong> Dentistry. 2nd ed. Philadelphia:<br />
Saunders, 1992.<br />
2. Litonjua L, Andreana S, Bush PJ, et al. Tooth wear: attrition, erosion,<br />
and abrasion. Quintessence Int. 2003;(34):435-446.<br />
3. Grippo J, Simring M, Schreiner S. A new perspective on tooth surface<br />
lesions. J Am Dent Assoc. 2004;135(8):1109-1118.<br />
4. Badel T, Keros J, Šegović S, Komar D. Clinical and tribological view<br />
on tooth wear. Acta Stomatol Croat. 2007;41(4):355-365.<br />
5. Hand J, Beck J, Turner K. The prevalence <strong>of</strong> occlusal attrition and<br />
considerations for treatment in a noninstitutionalized older population.<br />
Spec Care Dentist. 1987;(7):202-206.<br />
6. Sivasithamparam K, Harbrow D, Vinczer E, et al. Endodontic sequelae<br />
<strong>of</strong> dental erosion. Aust Dent J. 2003;(48):97-101.<br />
7. Schneider P, Peterson J. Oral habits: considerations in management.<br />
Pediatr Clin North Am. 1982;(29):523-546.<br />
8. Dugmore C, Rock W. The prevalence <strong>of</strong> tooth erosion in 12-year-old<br />
children. Br Dent J. 2004;196(5):279-282.<br />
68 Linton, Jung | The Effect <strong>of</strong> Tooth Wear on Postorthodontic Pain Patients: Part 2<br />
9. Bardsley P, Taylor S, Milosevic A. Epidemiological studies <strong>of</strong> tooth wear<br />
and dental erosion in 14-year-old children in north west England, part I:<br />
the relationship with water fluoridation and social deprivation. Br Dent J.<br />
2004;197(7):413-416.<br />
10. Cordray F. Centric relation treatment and articulator mountings<br />
inorthodontics. Angle Orthod. 1996;66(2):153-158.<br />
11. Lee R. Jaw movements engraved in solid plastic for articulator controls,<br />
part I: recording apparatus. J Prosthet Dent. 1969;(22):209-224.<br />
12. Academy <strong>of</strong> Prosthodontics. Glossary <strong>of</strong> prosthodontic terms.<br />
J Prosthet Dent. 2005;94(7):10-92.<br />
13. Lundeen H. Centric relation records: the effect <strong>of</strong> muscle action.<br />
J Prosthet Dent. 1974;31(3):244-253.<br />
14. Crawford S. Condylar axis position, as determined by the occlusion<br />
and measured by the CPI instrument, and signs and symptoms <strong>of</strong> temporomandibular<br />
dysfunction. Angle Orthod.1999;69(2):103-116.<br />
15. Hunt K. Bioesthetics: Working with nature to improve function and<br />
appearance. Am Acad Cosmet Dent. 1996;12(2):45-50.<br />
16. Hunt, K. Full-mouth rejuvenation using the biologic approach: an 11year<br />
case report follow-up. Contemp Esthet Restor Pract. 2002;6(6):1-6.<br />
17. Lee R. Esthetics and its relationship to function. In: Rufenacht CR, ed.<br />
Fundamentals <strong>of</strong> Esthetics. Chicago: Quintessence; 1990:137-209.<br />
18. Hunt K, Turk M. Correlation <strong>of</strong> the AACD accreditation criteria and<br />
the human biologic mode. J Cosmet Dent. 2005;21(3):120-131.<br />
19. Ash M, Nelson S. Dental Anatomy, Physiology and Occlusion. 8th ed.<br />
St Louis, MO: Saunders; 2003.<br />
20. Knight D, Leroux B, Zhu C, Almond J, Ramsay D. A longitudinal<br />
study <strong>of</strong> tooth wear in orthodontically treated patients. Am J Orthod<br />
Dent<strong>of</strong>ac Orthop. 1997;112(6):17-18.<br />
21. Masatoshi K, Masanori F. Occlusal factors associated with temporomandibular<br />
disorder based on a prospective cohort study <strong>of</strong> young adults.<br />
Prosthod Res Pract. 2006;5(2):72-79.<br />
22. Jemt T, Lundquist S, Hedegard B. Group function or canine protection.<br />
J Prosthet Dent. 1982;(48):719-724.<br />
23. Straub W. Malfunctions <strong>of</strong> the tongue. Am J Orthod. 1960;(40):404-420.<br />
24. Kydd W. Maximum forces exerted on the dentition by the perioral and<br />
lingual musculature. J Am Dent Assoc. 1957;(55):646-651.
Physiologic Treatment Goals in Orthodontics<br />
Andrew Girardot, DDS, FACD<br />
and R e W Gi R a R d o T , ddS, Facd<br />
ragfishing@hotmail.com<br />
■ Graduated from USC School <strong>of</strong><br />
Dentistry (DDS), 1968<br />
■ Graduated from USC School <strong>of</strong><br />
Dentistry, Dept. <strong>of</strong> Orthodontics<br />
(certificate in orthodontics), 1972<br />
■ Part-time Faculty University <strong>of</strong><br />
Colorado, School <strong>of</strong> Dentistry,<br />
Dept. <strong>of</strong> Orthodontics<br />
■ C<strong>of</strong>ounder, codirector and faculty,<br />
<strong>Roth</strong> <strong>Williams</strong> USA, 1997-present<br />
Introduction<br />
For the better part <strong>of</strong> a hundred years, orthodontists have<br />
used Angle’s classification as a means <strong>of</strong> communication.<br />
When we say “Class I,” orthodontists share the same image,<br />
which is generally a positive concept <strong>of</strong> how teeth should fit<br />
together. There certainly can be a Class I case with problems,<br />
but Class I is the first major step in describing optimal tooth<br />
relationships. To this day, Angle’s Class I describes a morphologic<br />
treatment goal for the orthodontic specialty.<br />
Why do we not have a similar physiologic treatment<br />
goal? Often we talk about “occlusion” in orthodontics, but<br />
it clearly means different things to different people. The term<br />
occlusion lacks the communication value <strong>of</strong> Class I. A “good<br />
occlusion” is a nebulous term that varies depending on the<br />
person using it. We have a communication problem. We enjoy<br />
general agreement, and hence communication clarity,<br />
regarding morphology, but this is not the case for physiology.<br />
It would certainly be <strong>of</strong> value to our patients and the<br />
orthodontic specialty if we had a clear definition <strong>of</strong> what<br />
constitutes optimal physiology or “good occlusion.”<br />
As in all biologic systems, the structural elements <strong>of</strong><br />
the human gnathic system have evolved to perform best un-<br />
Summary<br />
Angle’s class I has long served the orthodontic specialty as a morphologic<br />
treatment goal and a means <strong>of</strong> communication. Certainly a physiologic<br />
treatment goal would be <strong>of</strong> equal value. There are sound data to define and<br />
support such a physiologic goal, which can help orthodontists to better serve<br />
their patients, communicate with other dental pr<strong>of</strong>essionals, and avoid numerous<br />
clinical problems.<br />
der certain conditions <strong>of</strong> form and function. For example,<br />
there is considerable evidence to support a clear definition<br />
<strong>of</strong> healthy function for the temporomandibular joint in its<br />
loaded state, such as during a swallow. When loaded, the<br />
condyle should be positioned upward, forward and midsagittally.<br />
This definition <strong>of</strong> optimal joint position is agreed<br />
upon by most authorities1-15 and is well supported by the<br />
literature. 16-36 Okeson defines this as the “most musculoskeletally<br />
stable position <strong>of</strong> the mandible.” 7(112) There also are<br />
data indicating the optimal relationship <strong>of</strong> the condyle, disc,<br />
and eminence when the mandible is moving into or out <strong>of</strong><br />
the loaded position. In this condition, there should be constant<br />
contact between the condyle, disc, and eminence. 37-40<br />
There are numerous data indicating that neuromuscular<br />
function is highly influenced by tooth contacts and tooth positions.<br />
41-55 For example, as the mandible moves into and out<br />
<strong>of</strong> intercuspation, guidance from properly positioned anterior<br />
teeth aids in separating the posterior teeth. This reduces<br />
the activity <strong>of</strong> the powerful elevating muscles, which, in turn,<br />
downloads the system while facilitating constant contact between<br />
the condyle, disc, and eminence. 39,43,46,47,55-64<br />
Thus, current data point to an optimal physiologic rela-<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
69
tionship between the teeth, the joints, and the neuromusculature.<br />
This information provides a physiologic treatment goal<br />
for the orthodontist, a summary <strong>of</strong> which can be made by analyzing<br />
the system in loaded and unloaded conditions. When<br />
loaded, eg, during a swallow, the condyles are fully seated<br />
upward and forward in the fossae, the elevating muscles are<br />
active, and the dentition is in full intercuspation. 41,55,62,63,65,66<br />
When unloaded, the condyles remain in firm and constant<br />
contact with the disc and eminence, elevating muscles are inactive<br />
and positioning muscles (eg, lateral pterygoids) are active,<br />
posterior teeth are out <strong>of</strong> contact, and the anterior teeth<br />
play a major role in guiding mandibular movements. 67-75<br />
Given a reliable perspective <strong>of</strong> optimal static and dynamic relationships<br />
between the teeth, joints, and neuromusculature,<br />
we can consider some additional principles regarding gnathic<br />
function. There are at least three reasons why the intercuspal<br />
position is important. First, the positions and the shapes <strong>of</strong><br />
the teeth determine mandibular movements at and near the<br />
intercuspal position. 7,50,61,76-100 Second, when the mandible is<br />
brought to full intercuspation in a functionally healthy system,<br />
the powerful elevating muscles are active and the system<br />
is heavily loaded; the bulk <strong>of</strong> the resultant force is absorbed<br />
by posterior teeth. 32,50-52,101-103 Third, condylar position is determined<br />
by the dentition at intercuspation. 61,83,104-106<br />
An additional important factor well supported in the literature<br />
is the clinical observation that the neuromusculature<br />
is exquisitely programmed to guide the mandible to the intercuspal<br />
position80,85-100,107 ; the intercuspal position is dominant<br />
over condylar position. 61,83,103,105,106,108-110 Thus, asking<br />
a patient to “bite down” provides no dependable information<br />
as to where the condyle is positioned. Moreover, efforts<br />
to identify the seated condylar position through clinical<br />
maneuvers such as manipulating the mandible are not reliable.<br />
28,111-116 To quote the master clinician Dr. Thomas Basta,<br />
“Don’t believe what you see in the mouth.” 2 Thus the value<br />
<strong>of</strong> using interocclusal devices such as cotton rolls, anterior<br />
jigs, and splints to deprogram the neuromusculature.<br />
If we are to apply these physiologic principles to the<br />
practice <strong>of</strong> orthodontics, we need additional information<br />
besides that which we have traditionally used; for example,<br />
techniques that record the optimal or “seated” position <strong>of</strong><br />
the condyle. Currently there are numerous such techniques<br />
employed in restorative dentistry. Many clinicians use a hard<br />
stop at the incisor midline to separate the posterior teeth,<br />
along with a s<strong>of</strong>t posterior material that can be hardened<br />
thermally or chemically. When the patient bites against the<br />
hard anterior stop and the neuromusculature seats the condyles<br />
superioranteriorly, the posterior material is hardened,<br />
and the musculoskeletally stable position <strong>of</strong> the mandible is<br />
recorded (Figure 1).<br />
70 Girardot | Physiologic Treatment Goals in Orthodontics<br />
Figure 1 The anterior stop is hard and flat; it separates the<br />
posterior teeth to create appropriate space for a recording<br />
medium. The patient is instructed to close firmly, which<br />
seats the condyles to the musculoskeletally stable<br />
position <strong>of</strong> the mandible.<br />
The information then must be transferred from the patient<br />
to a device that will allow study and treatment planning<br />
<strong>of</strong> the gnathic system in three dimensions. Currently,<br />
the articulator appears to be the best tool for this purpose,<br />
although computer-generated three-dimensional technology<br />
may replace the articulator in the near future. Casts mounted<br />
on an articulator provide invaluable physiological information<br />
for diagnosis and treatment planning. For example,<br />
numerous studies show that there is nearly always vertical<br />
distraction <strong>of</strong> the condyle when the patient closes to intercuspation.<br />
33,113,117-122 It is all but impossible to record, analyze,<br />
and treatment plan this vertical discrepancy without the<br />
use <strong>of</strong> a device such as an articulator.<br />
Joint images are another tool that can serve orthodontists<br />
with regard to physiologic treatment. Tomograms, as<br />
first advocated by Ricketts, have provided an effective way<br />
to study the health <strong>of</strong> the temporomandibular joint and the<br />
position <strong>of</strong> the condyle in the fossa. 123-125 At present, cone<br />
beam CT is a more effective way to study the temporomandibular<br />
joint, as it provides a more-lucid, three-dimensional<br />
view <strong>of</strong> joint structures. 36<br />
There are sound data to support the concept that optimal<br />
gnathic function can be defined and used as an evidence-based<br />
treatment goal. There is little doubt that this<br />
would also aid communication between orthodontists and<br />
other dental pr<strong>of</strong>essionals. In addition, knowledge <strong>of</strong> gnathic<br />
physiology is <strong>of</strong> substantial value to orthodontists in that it<br />
helps them to recognize and avoid myriad problems that occur<br />
in everyday practice. ■
REFERENCES<br />
1. Dawson PE. The Concept <strong>of</strong> Complete Dentistry. St. Petersburg, FL:<br />
Center for Advanced Dental Study; 1994.<br />
2. Basta T. Lecture and Clinical Procedures. Burlingame, CA: Foundation<br />
for Advanced Education; 1975-2000.<br />
3. Guichet NF. Occlusion – A Teaching Manual. 2nd ed. Anaheim, CA:<br />
Denar Corportion; 1977.<br />
4. Lee RL. Esthetics and its relationship to function. In: Claude<br />
Rufenacht, ed. Fundamentals <strong>of</strong> Esthetics. Chicago, IL: Quintessence;<br />
1990:145-148.<br />
5. McHorris WH. Occlusion with particular emphasis on the functional<br />
and parafunctional role <strong>of</strong> anterior teeth. J Clin Orthod.<br />
1979;(13):606-608.<br />
6. McNeill C. Fundamental treatment goals. In: McNeill C, ed. Science<br />
and Practice <strong>of</strong> Occlusion. Chicago, IL: Quintessence;1997:306-322.<br />
7. Okeson JP. Management <strong>of</strong> Temporomandibular Disorders and<br />
Occlusion.3rd ed. St. Louis, MO: Mosby;1993:103, 111-115.<br />
8. <strong>Roth</strong> RN. The maintenance system and occlusal dynamics. Dent<br />
Clinics N Am. 1976;(20):761.<br />
9. McCollum, Stuart CE. A Research Report. Ventura, CA: Chas. E.<br />
Stuart; 1955.<br />
10. Spear FM. Fundamental occlusal therapy considerations. In:<br />
McNeil C, ed. Science and Practice <strong>of</strong> Occlusion. Chicago,IL: Quintessence;1997:421-434.<br />
11. Lucia VO. A technique for recording centric relation. J Prosthet<br />
Dent. 1964;(14):492.<br />
12. <strong>Williams</strong>on EH: Occlusal concepts in orthodontic diagnosis and<br />
treatment, part I: the seated condylar position.In Johnson LE, ed. New<br />
Vistas in Orthodontic. Philadelphia, PA: Lea and Bebiger; 1985: 11.<br />
13. Shore NA. Temporomandibular Joint Dysfunction and Occlusal<br />
Equilibration. 2nd ed. Philadelphia, PA: JB Lippincott;1976:238-241.<br />
14. Dyer EH. Dental articulation and occlusion. J Prosthet Dent.<br />
1967;(17):238.<br />
15. Celenza FV, Nasedkin JN. Occlusion: The State <strong>of</strong> the Art. Chicago,<br />
IL: Quintessence; 1987.<br />
16. Hylander WL, Bays RA. Bone strain in the subcondylar region <strong>of</strong><br />
the mandible in Macaca fascicularis and Macaca mulatta. Am J Phys<br />
Anthrop. 1978;(48):408.<br />
17. Hylander WL, Bays RA. An in vivo strain-gauge analysis <strong>of</strong><br />
the squamosal-dentary joint reaction force during mastication and<br />
incision in Macaca mulatta and Macaca fasicularis. Arch Oral Biol.<br />
1979;(24):689.<br />
18. Hylander WL. An experimental analysis <strong>of</strong> temporomandibular<br />
joint reaction force in macaques. Am J Phys Anthrop. 1979;(51):433.<br />
19. Hylander WL. Functional anatomy. In: Sarnat BG, Laskin DM,<br />
eds. The Temporomandibular Joint. 3rd ed. Springfield, IL: Charles C<br />
Thomas; 1979:85-89.<br />
20. Boyd RL, Gibbs CH, Mahan PE, Richmond AF, Laskin JL.<br />
Temporomandibular joint forces measured at the condyle <strong>of</strong> Macaca<br />
arctoides. Am J Orthod Dent<strong>of</strong>ac Orthop. 1990;(97):472.<br />
21. Hansson T, Oberg T, Carlsson GE, Kopp S. Thickness <strong>of</strong> the s<strong>of</strong>t<br />
tissue layers and the articular disk in the temporomandibular joint.<br />
Acta Odont Scan. 1977;(5):77.<br />
22. M<strong>of</strong>fett BC, Johnson L, McCabe J, Askew H. Articular remodeling<br />
in the adult human temporomandibular joint. Am J Anat.<br />
1964;(115):119-142.<br />
23. Okeson JP. Bell’s Or<strong>of</strong>acial Pains. 5th ed. Carol Stream, IL: Quintessence;.<br />
1995:297.<br />
24. Hatcher DC, McEvoy SP, Mah RT, Faulkner MG. Distribution <strong>of</strong><br />
local and general stresses in the stomatognathic system, In: McNeill<br />
C, ed. Science and Practice <strong>of</strong> Occlusion. Chicago, IL: Quintessence;1997:259-270.<br />
25. Lundeen HC. Centric relation records: the effect <strong>of</strong> muscle action. J<br />
Prosthet Dent. 1974; (31):244.<br />
26. Ito T, Gibbs CH, Marguelles-Bonnet R, et al. Loading on the<br />
temporomandibular joints with five occlusal conditions. J Craino Funct<br />
Dysf. 1986;(56):478.<br />
27. <strong>Williams</strong>on EH, Steinke RM, Morse PK, Swift TR. Centric relation:<br />
a comparison <strong>of</strong> muscle determined position and operator guidance.<br />
Angle Orthod. 1980;(77):133.<br />
28. <strong>Williams</strong>on EH, Evans DL, Barton WA, <strong>Williams</strong> BH. The effect<br />
<strong>of</strong> bite plane use on terminal hinge axis location. Angle Orthod.<br />
1977;(47):25-33.<br />
29. Strohaver RA. A comparison <strong>of</strong> articulator mountings made with<br />
centric relation and myocentric position records. J Prosthet Dent.<br />
1972;(28):379.<br />
30. Yustin D. Treatment position <strong>of</strong> the condyle. Research findings presented<br />
at: 44th Annual Meeting <strong>of</strong> the American Equilibration <strong>Society</strong>;<br />
February 1, 1999; Chicago, IL.<br />
31. Teo CS, Wise MD. Comparison <strong>of</strong> retruded axis articular mounting<br />
with and without applied muscular force. J Oral Rehab. 1986;(8):363.<br />
32. Lundeen HC, Gibbs CH. Advances in Occlusion. Boston, MA: J<br />
Wright-PSG;1982:7-11.<br />
33. Girardot RA. The nature <strong>of</strong> condylar displacement in patients with<br />
temporomandibular pain-dysfunction. Orthod Rev. 1987;(1):16.<br />
34. Wood DP, Floreani KJ, Galil KA, Teteruck WR. The effect <strong>of</strong> incisal<br />
bite force on condylar seating. Angle Orthod. 1994;(64):53.<br />
35. Radu M, Marandici M, Hottel T. The effect <strong>of</strong> clenching on condylar<br />
position: a vector analysis. J Prosthet Dent. 2004;(91):171-179.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
71
36. Ikeda K, Kawamura A. Assessment <strong>of</strong> optimal condylar position<br />
with limited cone-beam computed tomography. Am J Orthod Dent<strong>of</strong>ac<br />
Orthop. 2009;(135):495-501.<br />
37. Sicher H. Oral Anatomy. 4th ed. St. Louis, MO: Mosby; 1965:179.<br />
38. Scapino RP. Morphology and mechanism <strong>of</strong> the jaw joint. In: Mc-<br />
Neill C, ed. Science and Practice <strong>of</strong> Occlusion. Chicago, IL: Quintessence;1997:31-37.<br />
39. Lundeen HC, Gibbs CH. Human Chewing: Part I [videotape].<br />
Gainesville, FL: University <strong>of</strong> Florida; 1983.<br />
40. Okeson JP. Management <strong>of</strong> Temporomandibular Disorders and<br />
Occlusion. 3rd ed. St. Louis, MO: Mosby;1993:26.<br />
41. <strong>Williams</strong>on EH. Structural (occlusal) factors related to TMD.<br />
In: Current Controversies in Temporomandibular Disorders. Carol<br />
Stream, IL: 1991:83-89.<br />
42. Belser UC, Hannam AG. The influence <strong>of</strong> altered working-side<br />
occlusal guidance on masticatory muscles and related jaw movement. J<br />
Prosthet Dent. 1985;(53):406.<br />
43. MacDonald JWC, Hannam AG. Relationship between occlusal<br />
contacts and jaw-closing muscle activity during tooth clenching, part I.<br />
J Prosthet Dent. 1984;(52):718.<br />
44. Krough-Poulson WG, Olsson A. Management <strong>of</strong> the occlusion <strong>of</strong><br />
the teeth, part. I: background, definitions, rationale. In: Schwartz L,<br />
Chayes CM, eds. Facial Pain and Mandibular Dysfunctions. Philadelphia,<br />
PA: WB Saunders; 1968:236-249.<br />
45. Kloprogge MJG, van Griethuysen AM. Disturbances in the contraction<br />
and coordination pattern <strong>of</strong> the masticatory muscles due to<br />
dental restorations. J Oral Rehab. 1976;(3):207.<br />
46. <strong>Williams</strong>on EH. Occlusion and TMJ dysfunction, part I. J Clin<br />
Orthod. 1981;(15):333.<br />
47. Greco PM, Vanarsdall RL Jr, Levrini M, Read T. An evaluation <strong>of</strong><br />
anterior temporal and masseter muscle activity in appliance therapy.<br />
Angle Orthod. 1999;(69):141.<br />
48. Riise C, Sheikholeslam A. Influence <strong>of</strong> experimental interfering<br />
occlusal contacts on the activity <strong>of</strong> the anterior temporal and masseter<br />
muscles during mastication. J Oral Rehab. 1984;(11):325.<br />
49. Hannam AJ. Jaw muscle structure and function. In: McNeill C,ed.,<br />
Science and Practice <strong>of</strong> Occlusion. Chicago, IL: Quintessence; 1997:41-<br />
48.<br />
50. Gibbs CH, Fujimoto J. Patient response to occlusal therapy: In:<br />
Lundeen HC, Gibbs CH, eds., Advances in Occlusion. Boston, MA:<br />
John Wright; 1982:33-50.<br />
51. Moller E, Scheikholeslam A, Louis I. Response <strong>of</strong> elevator activity<br />
during mastication to treatment <strong>of</strong> functional disorders. Scand J Dent<br />
Res. 1984;(92):64.<br />
52. Hannam AG, De Cou RE, Scott JD, Wood WW. The relationship<br />
between dental occlusion, muscle activity and associated jaw movement<br />
in man. Arch Oral Biol. 1977;(22):25.<br />
72 Girardot | Physiologic Treatment Goals in Orthodontics<br />
53. Ingervall C, Carlsson GE. Masticatory muscle activity before and<br />
after elimination <strong>of</strong> balancing side occlusal interference. J Oral Rehab.<br />
1982;(9):183.<br />
54. Hansson T. Temporomandibular joint changes related to dental<br />
occlusion. In: Solberg WK, Clark GT, eds. Temporomandibular Joint<br />
Problems: Biologic Diagnosis and Treatment. Chicago, IL: Quintessence;<br />
1980:129-139.<br />
55. Shupe RJ, Mohamed SE, Christensen LV, Finger IM, Weinberg R.<br />
Effects <strong>of</strong> occlusal guidance on jaw muscle activity. J Prosthet Dent<br />
1984;51:811.<br />
56. Crum RJ, Loiselle RJ. Oral perception and proprioception: a review<br />
<strong>of</strong> the literature and its significance to prosthodontics. J Prosthet<br />
Dent. 1972;(28):215.<br />
57. Desjardin RP, Winkelman RK, Gonzalez JB. Comparison <strong>of</strong> nerve<br />
endings in normal gingiva with those <strong>of</strong> mucous membranes covering<br />
edentulous ridges. J Dent Res. 1971;(50):867.<br />
58. Hannam AG. The innervation <strong>of</strong> the periodontal ligament. In:<br />
Berkowitz BK, ed. Periodontal Ligament in Health and Disease. Oxford:<br />
Pergammon; 1981: 224-237.<br />
59. Woda A, Vigneron P, Kay D. Non-functional and functional occlusal<br />
contacts: a review <strong>of</strong> the literature. J Prosthet Dent. 1979;(42):335.<br />
60. Kawamura Y. Neurophysiologic background <strong>of</strong> occlusion. Periodon.<br />
1967;(5):175.<br />
61. Dubner R, Sessle BJ, Storey AT. The Neural Basis <strong>of</strong> Oral and<br />
Facial Function. New York, NY: Plenum; 1978:147-174.<br />
62. Manns A, Chan C, Miralles R. Influence <strong>of</strong> group function and<br />
canine guidance on electromyographic activity <strong>of</strong> elevator muscles. J<br />
Prosthet Dent. 1987;(57):494.<br />
63. <strong>Williams</strong>on EH, Lundquist DO. Anterior guidance: its effect on<br />
electromyographic activity <strong>of</strong> the temporal and masseter muscles. J<br />
Prosthet Dent. 1983;(49):816.<br />
64. Manns A, Mirrales R, Valdivia J, Bull R. Influence <strong>of</strong> variation<br />
in anteroposterior occlusal contacts on electromyographic activity. J<br />
Prosthet Dent. 1989;(61):617.<br />
65. Wilkinson T. Comparing TMJ imaging and anatomy. Lecture presented<br />
at: The Craniomandibular Institute; January 25, 1996; Squaw<br />
Valley, CA.<br />
66. Lundeen CL, Gibbs C H. The Function <strong>of</strong> Teeth. 1st ed. Gainsville,<br />
FL: L and G Publishers LLC; 2005:78-81.<br />
67. Stalberg E, Eriksson PO, Antoni L, Thornell LE. Electrophysiological<br />
study <strong>of</strong> size and fiber distribution <strong>of</strong> motor units in the human<br />
masseter and temporal muscles. Arch Oral Biol. 1986;(31):521.<br />
68. Moller E. The chewing apparatus. Acta Physiol Scand 1966;(67):1.<br />
69. Griffin CJ, Munro RR. Electromyography <strong>of</strong> the jaw-closing<br />
muscles in the open-close-clench cycle in man. Arch Oral Biol.<br />
1969;(14):141.
70. McNamara JA Jr. The independent functions <strong>of</strong> the two heads <strong>of</strong><br />
the lateral pterygoid muscle. Am J Anat. 1973;(138):197.<br />
71. Aziz MA, Cowie RJ, Skinner CE, Abudi TS, Orzame G. Are the two<br />
heads <strong>of</strong> the human lateral pterygoid separate muscles? A perspective<br />
based on their nerve supply. J Or<strong>of</strong>ac Pain. 1998;(12):226.<br />
72. Widmer, CG. Jaw-opening reflex activity in the inferior head <strong>of</strong> the<br />
lateral pterygoid muscle in man. Arch Oral Biol. 1987;(32):135.<br />
73. Wood, WW, Takada K, Hannam AG. The electromyographic activity<br />
<strong>of</strong> the inferior part <strong>of</strong> the human lateral pterygoid muscle during<br />
clenching and chewing. Arch Oral Biol. 1986;(31):245.<br />
74. Mahan PE, Wilkinson TM, Gibbs CH, Mauderli A, Brannon LS.<br />
Superior and inferior bellies <strong>of</strong> the lateral pterygoid muscle EMG activity<br />
at basic jaw positions. J Prosthet Dent. 1983;(50):710.<br />
75. Osborn JW, Baragar FA. Predicted pattern <strong>of</strong> human muscle<br />
activity during clenching derived from a computer assisted model: symmetrical<br />
vertical bite forces. Biomechanics. 1985;(18): 599.<br />
76. Girardot RA. Functioning Tooth Relationships in the Adult<br />
Dentition [master’s thesis]. Los Angeles, CA. University <strong>of</strong> Southern<br />
California; 1972.<br />
77. Slavicek R. Clinical and instrumental functional analysis for<br />
diagnosis and treatment planning,part IV:instrumental analysis <strong>of</strong> mandibular<br />
casts using the mandibular position indicator. J Clin Orthod.<br />
1988;(23):566.<br />
78. Hannam AG, Matthews B. Reflex jaw opening in response to<br />
stimulation <strong>of</strong> periodontal mechanoreceptors in the cat. Arch Oral<br />
Biol. 1969;(14):415.<br />
79. Anderson DJ, Hannam AG, Matthews B. Sensory mechanism<br />
in mammalian teeth and their supporting structures. Physiol Rev.<br />
1970;(50):171.<br />
80. Scharer P, Stallard RE. The use <strong>of</strong> multiple radio transmitters in<br />
studies <strong>of</strong> tooth contact patterns. Periodon. 1965;(3):5.<br />
81. Ide Y, Nakazawa K. Anatomical Atlas <strong>of</strong> the Temporomandibular<br />
Joint. Chicago: Quintessence; 1991:82.<br />
82. Throckmorton GS, Groshan GJ, Boyd SB. Muscle activity patterns<br />
and control <strong>of</strong> temporomandibular joint loads. J Prosthet Dent.<br />
1990;(63):685.<br />
83. M<strong>of</strong>fett BC. Histologic aspects <strong>of</strong> temporomandibular joint derangements.<br />
Double-Contrast Arthrography and Clinical Correlation.<br />
Seattle, WA: University <strong>of</strong> Washington; 1984:47. Diagnosis <strong>of</strong> Internal<br />
Derangements <strong>of</strong> the Temporomandibular Joint; vol 1.<br />
84. Hickey JC, Allison ML, Woelfel JB, Boucher CO, Stacy RW. Mandibular<br />
movements in three dimensions. J Prosthet Dent. 1963;(13):72.<br />
85. Butler JH, Zander HA. Evaluation <strong>of</strong> two occlusal concepts. Parodontologie<br />
Acad Rev. 1968; (2):5.<br />
86. Adams SH, Zander HA. Functional tooth contacts in lateral and in<br />
central occlusion. J Am Dent Assoc. 1964;(69):465.<br />
87. Beyron HL. Occlusal relations and mastication in Australian Aborigines.<br />
Acta Anat Scand. 1964;(22):596.<br />
88. Beyron HL. Characteristics <strong>of</strong> functionally optimal occlusion and<br />
principles <strong>of</strong> occlusal rehabilitation. J Am Dent Assoc. 1954;(48):648.<br />
89. Dierkes DD. A Cephalometric Radiographic and Clinical Study <strong>of</strong><br />
Certain Mandibular Movements in Individuals With Excellent Anatomical<br />
Occlusion <strong>of</strong> the Teeth [master’s thesis]. Chicago, IL: Northwestern<br />
University; 1957.<br />
90. Graf H, Zander HA. Tooth contact patterns in mastication. J Prosthet<br />
Dent. 1963;(13):1055.<br />
91. Hildebrand GY. Studies in the masticatory movements <strong>of</strong> the human<br />
lower jaw. Scand Arch Physio. 1937;(Suppl):61.<br />
92. Jerge CR. The neurologic mechanism underlying cyclic jaw movements.<br />
J Prosthet Dent. 1964;(14):667.<br />
93. Moyers RE. Some physiologic considerations <strong>of</strong> centric and other<br />
jaw relations. J Prosthet Dent 1956;(6):183.<br />
94. Pameijner JHN, Glickman I, Robert FW. Intraoral occlusal telemetry,<br />
part II: registration <strong>of</strong> tooth contacts in chewing and swallowing.<br />
J Prosthet Dent. 1968;(19):151-159.<br />
95. Perry HT. Functional electromyography <strong>of</strong> temporal and masseter<br />
muscles in Class III, Div 1 malocclusion and excellent occlusion. Angle<br />
Orthod. 1955;(25):49.<br />
96. Reynolds MJ. The organization <strong>of</strong> occlusion for natural teeth. J<br />
Prosthet Dent. 1971;(25):56.<br />
97. Schweitzer JM. Masticatory function in man. J Prosthet Dent.<br />
1961;(11):708.<br />
98. Shepherd RW. A further report on mandibular movement. Aust<br />
Dental J. 1960;(5):337.<br />
99. Yeager JA. Mandibular path in the grinding phase <strong>of</strong> mastication: a<br />
review. J Prosthet Dent. 1978;(39):569.<br />
100. Sicher H. Oral Anatomy. 4th ed. St. Louis, MO: Mosby;1965:188.<br />
101. Ramfjord SP. Bruxism: a clinical and electromyographic study. J<br />
Am Dent Assoc. 1961; (62):21.<br />
102. Ahlgren J, Owall B. Muscular activity and chewing force: a<br />
polygraphic study <strong>of</strong> human mandibular movements. Arch Oral Biol.<br />
1970;(18):271.<br />
103. Lundeen HC, Gibbs CH. Advances in Occlusion. Boston, MA:<br />
John Wright; 1982:28-29.<br />
104. Johnston LE. A systems analysis <strong>of</strong> occlusion. In: McNamara JA,<br />
Carlson DS, Ribbens KR, eds. Developmental Aspects <strong>of</strong> Temporomandibular<br />
Joint Disorders. Crani<strong>of</strong>acial Growth Series Monograph<br />
16. Ann Arbor, MI: Center for Human Growth and Development,<br />
University <strong>of</strong> Michigan; 1985;(16):191-205.<br />
105. Posselt U. The Physiology <strong>of</strong> Occlusion and Rehabilitation. 2nd<br />
ed. Philadelphia, PA: FA Davis; 1968:37.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
73
106. Luecke PE III, Johnston LE. The effect <strong>of</strong> maxillary first premolar<br />
extraction and incisor retraction on mandibular position: testing the<br />
central dogma <strong>of</strong> “functional orthodontics.” Am J Orthod Dent<strong>of</strong>ac<br />
Orthop. 1992;(101):4.<br />
107. Brill N, Schubeler S, Tryde G. Influence <strong>of</strong> occlusal patterns on<br />
movements <strong>of</strong> the mandible. J Prosthet Dent. 1962;(12):255.<br />
108. Hylander WL. Implications <strong>of</strong> in vivo experiments for interpreting<br />
the functional significance <strong>of</strong> “robust” Australopithecine jaws, In:<br />
Grine RE, ed. Evolutionary History <strong>of</strong> the “Robust” Australopithecines.<br />
New York, NY: Aldine de Gruyter; 1988:55-83.<br />
109. Korioth TWP, Hannam AG. Deformations <strong>of</strong> the human mandible<br />
during simulated tooth clenching. J Dent Res. 1994;(73):56.<br />
110. Korioth YWP, Hannam AG. Mandibular forces during simulated<br />
tooth clenching. J Or<strong>of</strong>ac Pain. 1994;(8):178.<br />
111. <strong>Roth</strong> RH, Rolfs DA. Functional occlusion for the<br />
orthodontist,part II. J Clin Orthod. 1981;(15):100.<br />
112. Dawson PE. Evaluation, Diagnosis, and Treatment <strong>of</strong> Occlusal<br />
Problem., St Louis, MO: Mosby; 1974:48-70.<br />
113. Cordray FE. Three-dimensional analysis <strong>of</strong> models articulated<br />
in the seated condylar position from a deprogrammed asymptomatic<br />
population: a prospective study, part I. Am J Orthod Dent<strong>of</strong>ac Orthop.<br />
2006;(129):619-630.<br />
114. <strong>Williams</strong>on EH, et al. The effect <strong>of</strong> bite plane use on terminal<br />
hinge axis location. Angle Orthod. 1977;(47):25.<br />
115. Karl PJ, Foley TF: The use <strong>of</strong> a deprogramming appliance to<br />
obtain centric relation records. Angle Orthod. 1999;(69):117.<br />
116. Calagna LJ, et al. Influence <strong>of</strong> neuromusculature conditioning on<br />
centric relation registration. J Prosthet Dent. 1973;(30):598.<br />
117. Alexander R, Moore RN, DuBois L. Mandibular condyle position:<br />
comparison <strong>of</strong> articulator mountings and magnetic resonance<br />
imaging. Am J Orthod Dent<strong>of</strong>ac Orthop. 1993;(104):230-239.<br />
118. Utt TW, et al. A three-dimensional comparison <strong>of</strong> condylar position<br />
changes between centric relation and centric occlusion using the<br />
mandibular position indicator. Am J Orthod Dent<strong>of</strong>ac Orthop. 1995;<br />
(107):298.<br />
119. Crawford SD: Condylar axis position, as determined by the occlusion<br />
and measured by the CPI instrument, and signs and symptoms <strong>of</strong><br />
temporomandibular dysfunction. Angle Orthod. 1999; (69):103.<br />
120. Hidaka O, Adachi S, Takada K. The difference in condylar position<br />
between centric relation and centric occlusion in pretreatment<br />
Japanese orthodontic patients. Angle Orthod. 2002;(72):295-301.<br />
121. Girardot RA. Comparison <strong>of</strong> condylar position in hyperdivergent<br />
and hypodivergent facial skeletal types. Angle Orthod. 2001;(71):240-<br />
246.<br />
122. Wood DP, et al. The effect <strong>of</strong> incisal bite force on condylar seating.<br />
Angle Orthod. 1994;(64):53-62.<br />
74<br />
Girardot | Physiologic Treatment Goals in Orthodontics<br />
123. Ricketts RM. Abnormal function <strong>of</strong> the temporomandibular joint.<br />
Am J Orthod. 1955;(41):62.<br />
124. Ricketts RM. Variations <strong>of</strong> the Temporomandibular Joint As Revealed<br />
by Cephalometric Laminography. [master’s thesis]. Chicago, IL:<br />
University <strong>of</strong> Illinois; 1950.<br />
125. Ricketts RM. Laminography in the diagnosis <strong>of</strong> temporomandibular<br />
joint disorders. J Am Dent Assoc. 1953;(46):32.
Effect <strong>of</strong> Gnathologic Positioner Wear on Maximum<br />
Intercuspation CR Disharmony<br />
Wesley M. Chiang, DDS, MS ■ Theodore Freeland, DDS, MS<br />
■ Richard Kulbersh, DMD, MS, PLC ■ Richard Kaczynski, BS, MS, PhD<br />
We S L e y m. ch i a n G , ddS, mS<br />
■ MA Candidate, Orthodontic Dept.,<br />
University <strong>of</strong> Detroit Mercy School<br />
<strong>of</strong> Dentistry<br />
The o d o R e FR e e L a n d, ddS, mS<br />
tdfortho@freelandorthodontics.com<br />
■ Adjunct Pr<strong>of</strong>essor, Orthodontic<br />
Dept., University <strong>of</strong> Detroit Mercy<br />
School <strong>of</strong> Dentistry<br />
■ Director <strong>Roth</strong>/<strong>Williams</strong> USA;<br />
■ Private Practice, Gaylord, MI<br />
Ric h a R d Ku L b e R S h, dmd, mS, PLc<br />
■ Program Director, Orthodontic<br />
Dept., University <strong>of</strong> Detroit Mercy<br />
School <strong>of</strong> Dentistry<br />
Ric h a R d Ka c z y n S K i , bS, mS, Phd<br />
■ Statistician, Dept. <strong>of</strong> Psychiatry,<br />
Yale University School <strong>of</strong> Medicine<br />
Introduction<br />
Centric relation (CR) refers to a physiologic position <strong>of</strong> the<br />
mandible when the condyles are located in the superoanterior<br />
position in the articular fossae, fully seated and resting<br />
against the posterior slopes <strong>of</strong> the articular eminences with<br />
the discs properly interposed. 1 It is a reproducible position<br />
that is obtained independent <strong>of</strong> the occlusion by manipulating<br />
the mandible in a purely rotary movement about the<br />
transverse horizontal axis. 2<br />
Orthodontic treatment is aimed at achieving static goals<br />
from Andrews’ six keys to normal occlusion and the functional<br />
scheme <strong>of</strong> mutually protected occlusion recommended<br />
by Stuart and Stallard. 3,4 In the 1970s, <strong>Roth</strong> introduced gna-<br />
Summary<br />
The goal <strong>of</strong> a gnathological approach in orthodontics is to achieve a functional<br />
occlusion, in which the mandible can close into maximum intercuspation (MI) without<br />
deflecting the condyles from centric relation (CR). Gnathologic positioners are<br />
used at the end <strong>of</strong> orthodontic treatment to settle the occlusion while maintaining<br />
MI-CR harmony. The objective <strong>of</strong> this prospective study was to examine the effect<br />
<strong>of</strong> gnathologic positioners on MI-CR discrepancy for patients treated with the <strong>Roth</strong><br />
gnathological approach.<br />
Methods.The sample consisted <strong>of</strong> 26 consecutively finished cases in a gnathologically<br />
oriented practice. All cases were treated with a gnathological treatment approach,<br />
using the <strong>Roth</strong> prescription straight-wire appliance. A gnathologic positioner was<br />
delivered at the time <strong>of</strong> debonding and was worn for a period <strong>of</strong> 2 months. Pre- and<br />
postpositioner records were taken. These included a maximum-intercuspation wax<br />
bite; a two-piece <strong>Roth</strong> power centric CR bite registration; and upper and lower models<br />
mounted using a true hinge transfer and CR bite. The control group consisted <strong>of</strong> 8<br />
randomly selected finished cases in the orthodontic clinic at the University <strong>of</strong> Detroit<br />
Mercy and was retained with Hawley retainers. MI-CR discrepancy was measured<br />
with a condylar position Indicator (CPI).<br />
Results. Results indicate a statistically significant improvement in MI-CR discrepancy<br />
in the right horizontal, right vertical, left vertical, and transverse planes after 2 months<br />
<strong>of</strong> gnathologic positioner wear. The amount <strong>of</strong> condylar distraction in these 4 measurements<br />
showed statistically significant improvement and came within the envelope<br />
<strong>of</strong> susceptibility.<br />
Conclusions.The positioner and control groups tend to change differently over time<br />
in the vertical and horizontal planes, with the positioner group improving and the<br />
control group getting worse. In the transverse plane, gnathologic positioners improve<br />
the result <strong>of</strong> orthodontic treatment with respect to condylar axis distraction.<br />
thological concepts into orthodontic treatment. 5,6,7 The goal<br />
<strong>of</strong> a gnathological approach in orthodontics is to achieve a<br />
functional occlusion, in which the mandible can close into<br />
maximum intercuspation (MI) without deflecting the condyles<br />
from CR. 8 Dr. <strong>Roth</strong> believed that a large discrepancy<br />
between MI and CR can lead to breakdown in the stomatognathic<br />
system, because the condyles are distracted from<br />
the glenoid fossae when the teeth come into occlusion. Signs<br />
and symptoms <strong>of</strong> occlusal disharmony include temporomandibular<br />
joint pain-dysfunction syndrome, occlusal wear and<br />
bruxism, excessive tooth mobility associated with periodontal<br />
disease, and movement or relapse <strong>of</strong> tooth positions. 9<br />
Occlusal discrepancies, if associated with joint compression,<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
75
can also lead to condylar resorption. 10<br />
The clinical acceptable difference between CR and MI<br />
in terms <strong>of</strong> condylar position is approximately 1.0 mm anteroposteriorly,<br />
1.0 mm vertically, and 0.5 mm transversely.<br />
11,12,13,14 The condylar position indicator (CPI) has been<br />
used to accurately record condylar movements. 15 A comparison<br />
between pretreatment and posttreatment records in patients<br />
treated in a gnathologically oriented practice showed a<br />
statistically significant reduction in MI-CR discrepancy in all<br />
3 planes <strong>of</strong> space. 16 The posttreatment records were obtained<br />
before delivery <strong>of</strong> the gnathologic positioner.<br />
The purpose <strong>of</strong> this study was to examine the effect <strong>of</strong><br />
gnathologic positioners on MI-CR discrepancy for patients<br />
treated with the <strong>Roth</strong> gnathological approach. The effectiveness<br />
<strong>of</strong> gnathologic positioners can be determined if there<br />
is a decrease in MI-CR discrepancy following 2 months <strong>of</strong><br />
positioner wear.<br />
Research Design and Methods<br />
The positioner group consisted <strong>of</strong> 26 consecutively finished<br />
cases in a gnathologically oriented practice (Theodore Freeland,<br />
DDS, MS, Gaylord, Michigan). The sample consisted <strong>of</strong><br />
15 males and 11 females. The average age was 15 years and<br />
8 months. All cases were treated with a gnathological treatment<br />
approach, using the <strong>Roth</strong> prescription straight-wire<br />
appliance (GAC, Glendora, California). 12 Seven cases were<br />
treated with 4 premolar extractions, while 19 cases were<br />
treated with nonextraction. Four weeks prior to the debonding<br />
appointment, prepositioner records were taken (time 1).<br />
The records included upper and lower alginate impressions<br />
in rim lock trays, a true hinge face-bow transfer; an MI wax<br />
bite taken using 10x pink wax (Myoco Industries, Inc, Philadelphia,<br />
Pennsylvania); and CR bite registration taken using<br />
a two-piece <strong>Roth</strong> power centric method with Delar blue wax<br />
(Delar Corporation, Lake Oswego, Oregon) (Figure 1).<br />
Figure 1 Two-piece CR bite – anterior segment (A).<br />
Two-piece CR bite – posterior and anterior segments (B).<br />
MI bite (C). Two-piece CR and MI bite (D).<br />
The models were poured with a vacuum mixed white stone<br />
(Whip Mix Corporation, Louisville, Kentucky) and mounted<br />
with Whip Mix mounting plaster (Whip Mix corp, Louisville,<br />
Kentucky), using a true hinge transfer and CR bite<br />
(Figures 2,3).<br />
Figure 2 True hinge axis.<br />
Figure 3 True hinge mounted models with two-piece CR bite.<br />
Fabrication <strong>of</strong> Gnathologic Positioner<br />
The gnathologic positioner was fabricated using Oralastic<br />
80 silicone. The true hinge positioner set up is fabricated<br />
according to posterior determinants (angle <strong>of</strong> the articular<br />
eminence and Bennett side shift). At time 1, a second set <strong>of</strong><br />
upper and lower alginate impressions was taken and poured<br />
with white stone. The models were left unmounted, while the<br />
first set <strong>of</strong> models was mounted using true hinge face-bow<br />
transfer and CR bite. Unmounted models were used to fabricate<br />
the gnathologic positioner, using the mounted models<br />
as a reference. Teeth were separated from the models, and<br />
brackets were ground <strong>of</strong>f the teeth. Mandibular teeth were<br />
set to an occlusal plane with proper curve <strong>of</strong> Spee and curve<br />
<strong>of</strong> Wilson, and set on arc <strong>of</strong> closure in CR. The upper teeth<br />
were set to the lower teeth in accordance with ideal overbite/<br />
overjet (OB/OJ).<br />
At the debonding appointment, the braces were removed,<br />
and the gnathologic positioner was delivered. The arc <strong>of</strong> clo-<br />
76 Chiang, Freeland, et al | Effect <strong>of</strong> Gnathologic Positioner Wear on Maximum Intercuspation CR Disharmony
sure was first checked in the mounting on the true hinge ar-<br />
ticulator and then checked intraorally with and without the<br />
positioner. The patient was instructed to wear the positioner<br />
full time for the first 3 days (with the exception <strong>of</strong> eating and<br />
brushing). After the first 3 days, the patient was instructed to<br />
wear the positioner at night, with 4 hours <strong>of</strong> positioner exercise<br />
during the day. If the positioner should fall out during<br />
the night, the patient was instructed to wear the positioner<br />
for 6 hours during the day.<br />
Positioner Exercise and Wear Protocol<br />
The patient was instructed to bite into the positioner just<br />
enough to seat all <strong>of</strong> the teeth and to fully engage the teeth in<br />
the positioner. The patient was instructed to bite with pressure<br />
for about 10 seconds and then to relax for about 15<br />
seconds. The exercise was done in 15-minute intervals, with<br />
15 to 20 minutes <strong>of</strong> rest in between. For nighttime wear, the<br />
patient was instructed to put the positioner into the mouth<br />
and close the mouth to engage the positioner as much as possible<br />
without putting pressure on the positioner.<br />
The gnathologic positioner was checked for fit and arc<br />
<strong>of</strong> closure at 1, 2, and 4 weeks after delivery. After 2 months<br />
<strong>of</strong> positioner wear, postpositioner records were taken (time<br />
2). These consisted <strong>of</strong> the same records that had been taken<br />
at time 1. Upper splint and lower spring retainers were then<br />
delivered.<br />
The control group consisted <strong>of</strong> 8 randomly selected<br />
finished cases in the orthodontic clinic at the University <strong>of</strong><br />
Detroit Mercy. The control group was not preselected with<br />
regard to MI-CR discrepancy at debond. At the debonding<br />
appointment (time 1), braces were removed and records<br />
were taken. Upper and lower Hawley retainers were delivered,<br />
and the patient was instructed to wear them full time.<br />
After 2 months <strong>of</strong> Hawley retainer wear, records were taken<br />
again (time 2).<br />
MI-CR discrepancy was measured with a CPI (Panadent<br />
Corporation, Grand Terrace, California) at times 1 and 2 for<br />
both groups (Figure 4,5).<br />
Results<br />
The mean differences between MI and CR <strong>of</strong> the articulators’<br />
condylar axis position were recorded for the transverse,<br />
and separately for the right and for the left condyles in the<br />
vertical and anteroposterior (A-P) directions. Pre- and posttreatment<br />
measurements <strong>of</strong> MI-CR discrepancy <strong>of</strong> the control<br />
and positioner groups are summarized in Table 1.<br />
Figure 4 CPI registration with two-piece CR bite (A).<br />
CPI registration with MI bite (B). CPI Recording – transverse (C).<br />
CPI Recording – right (D).<br />
Figure 5 Condylar position indicator recording graph<br />
(CR – red dot, MI – blue dot).<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
77
Measurements<br />
Table 1 MI-CR Discrepancy Assessment <strong>of</strong> Control and Positioner Groups.<br />
Mean<br />
(mm)<br />
Control Positioner<br />
(n=8) (n=26)<br />
Time 1 Time 2 Time 1 Time 2<br />
SD (mm) Mean<br />
(mm)<br />
SD<br />
(mm)<br />
Mean<br />
(mm)<br />
SD<br />
(mm)<br />
Table 2 Independent t-test for MI-CR Discrepancies <strong>of</strong> Control Versus Positioner Group.<br />
Mean<br />
(mm)<br />
Right AP 0.700 0.499 1.225 1.383 1.306 0.897 0.733<br />
Right vertical 0.863 0.407 1.238 0.845 1.217 0.969 0.623<br />
Left AP 0.750 0.864 1.625 1.201 0.867 1.010 0.671<br />
Left vertical 0.825 0.292 1.062 0.686 1.162 0.794 0.669<br />
Transverse 0.350 0.267 0.288 0.309 1.031 1.106 0.248<br />
As the table shows, pretreatment means for the control<br />
group were all within the clinical envelope <strong>of</strong> ± 1.0 mm for<br />
the A-P and vertical dimensions, and ± 0.5 mm for the transverse.<br />
Conversely, 4 out <strong>of</strong> 5 pretreatment means for the positioner<br />
group were outside this envelope; only the mean left<br />
A-P measurement, at 0.87, was within the clinical envelope.<br />
The control and positioner groups were then assessed by an<br />
independent t-test for any statistically significant pretreatment<br />
differences. As shown in Table 2, no differences were<br />
found between the two groups (0.08 < p
For these analyses, the desired significance level <strong>of</strong> 0.05<br />
was reduced by a factor <strong>of</strong> 5 (for the 5 variable CPI readings:<br />
right A-P, right vertical, left A-P, left vertical, and transverse)<br />
to control experimentwide alpha and to avoid the risk <strong>of</strong><br />
type I errors. Thus a significance level <strong>of</strong> α = 0.01 was used<br />
for each test <strong>of</strong> the condylar axis position measurements. The<br />
results indicated statistically significant differences between<br />
time 1 and time 2 for the positioner group in the right A-P (Δ<br />
= 0.57 mm, t = 3.03, p = .006); right vertical (Δ = 0.59 mm,<br />
t = 2.79, p = .009); left vertical (Δ = 0.49 mm, t = 3.05, p =<br />
.005); and transverse (Δ = 0.78 mm, t = 3.49, p = .002) measurements.<br />
There was no statistically significant difference in<br />
the magnitude <strong>of</strong> condylar distraction in the left condyle in<br />
the A-P direction (Δ = 0.20 mm, t = 0.92, N.S.).<br />
Mixed-design analyses <strong>of</strong> variance compared the positioner<br />
and control groups’ change in MI-CR discrepancy<br />
over time (Table 4).<br />
Table 4 Mixed Design Analysis <strong>of</strong> Variance for MI-CR Discrepancies from time 1 to time 2 between Control Versus Positioner Group.<br />
Using the adjusted significance level described above<br />
(α = 0.01), these comparisons between the 2 groups showed<br />
no statistically significant differences in any <strong>of</strong> the 5 CPI<br />
measurements. However, 4 <strong>of</strong> the 5 dimensions fell below<br />
Effect F* p<br />
Right AP Time 0.012 .915<br />
Time x group 6.096 .019<br />
Right vertical Time 0.266 .609<br />
Time x group 5.203 .029<br />
Left AP Time 2.431 .129<br />
Time x group 6.053 .019<br />
Left vertical Time 0.599 .445.<br />
Time x group 4.917 034<br />
Transverse Time 4.102 .051<br />
* df for all tests are 1, 32.<br />
Time x group 2.978 .094<br />
the traditional α = 0.05 level. Graphical representations <strong>of</strong><br />
the change in MI-CR discrepancy over time for the positioner<br />
and control groups are shown in Figures 6 through 10.<br />
Figure 6 Right horizontal MI/CR discrepancy. Figure 7 Right vertical MI/CR discrepancy.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
79
Figure 8 Left horizontal MI/CR discrepancy.<br />
Figure 9 Left vertical MI/CR discrepancy.<br />
Figure 10 Transverse MI/CR discrepancy.<br />
Discussion<br />
Results <strong>of</strong> the present study indicate a statistically significant<br />
improvement in MI-CR discrepancy in the right horizontal,<br />
right vertical, left vertical, and transverse planes<br />
with 2 months <strong>of</strong> gnathologic positioner wear. The condylar<br />
axis distraction differences in the left horizontal planes<br />
were not statistically significantly different. Before positioner<br />
wear, the mean right horizontal, right vertical, left vertical,<br />
and transverse measurements were 1.306 mm, 1.217 mm,<br />
1.162 mm, and 1.031 mm respectively, and fell outside the<br />
± 1.0 mm vertical and horizontal as well as the ± 0.5 mm<br />
transverse distraction envelope proposed by Crawford, Utt<br />
et al, and Slavicek. 12,13,14 Following 2 months <strong>of</strong> positioner<br />
wear, the amount <strong>of</strong> condylar distraction in these 4 measurements<br />
showed statistically significant improvement and<br />
came within the distraction envelope. Before positioner wear,<br />
3 patients (11.5%) had MI-CR discrepancy that fell within<br />
the envelope <strong>of</strong> susceptibility in all 5 <strong>of</strong> the measurements<br />
examined, while 11 patients had all 5 measurements within<br />
the envelope after positioner wear (42.3%). Reducing MI-<br />
CR discrepancies is an important treatment goal in the gnathological<br />
philosophy, and the use <strong>of</strong> gnathologic positioner<br />
is essential to achieving this goal.<br />
Although these changes were nonsignificant when compared<br />
to change in the control group, the level <strong>of</strong> significance<br />
in the right horizontal, right vertical, and left vertical<br />
planes was very close to the significance level <strong>of</strong> 0.01 used<br />
for this study, and below the more common 0.05 level <strong>of</strong><br />
significance. Figures 6, 7 and 9 show a similar pattern with<br />
reduction in MI-CR discrepancy over time with positioner<br />
wear, while the group with the Hawley retainers shows an<br />
increase in MI-CR discrepancy. This trend is observed in 3 <strong>of</strong><br />
the 5 measurements studied (right horizontal, right vertical,<br />
and left vertical planes). The positioner and control groups<br />
tend to change differently over time in the vertical and horizontal<br />
planes, with the positioner group improving and the<br />
control group getting worse. This is consistent with <strong>Roth</strong>’s<br />
claim that general retention protocols with Hawley-type appliances<br />
following orthodontic therapy will tend to make<br />
MI-CR discrepancy worse, while gnathologic positioners<br />
will improve MI-CR discrepancy. Interestingly enough, all<br />
mean vertical and horizontal CPI measurements for the control<br />
group started within the distraction envelope <strong>of</strong> ± 1.0<br />
mm and finished outside the envelope following 2 months <strong>of</strong><br />
Hawley retainer wear.<br />
The small sample size <strong>of</strong> the control group is a limitation<br />
<strong>of</strong> this study. A larger sample size would eliminate type II error<br />
and might show a statistically significant difference in the<br />
change in MI-CR discrepancy over time between the control<br />
and the positioner group. However, the p-values are below<br />
80 Chiang, Freeland, et al | Effect <strong>of</strong> Gnathologic Positioner Wear on Maximum Intercuspation CR Disharmony
the .05 level <strong>of</strong> significance in the right horizontal, right ver-<br />
tical, and left vertical planes. Furthermore, the MI-CR pattern<br />
is observed, suggesting that this is not a purely random<br />
phenomenon. Since the control group was small, there is the<br />
possibility <strong>of</strong> an underpowered study.<br />
In the transverse plane, there appears to be no difference<br />
between the 2 groups over time. A condylar axis distraction<br />
in the transverse plane is more sensitive to clinical problems<br />
than a condylar axis distraction in the horizontal and vertical<br />
planes. 17,18,19 It appears that gnathologic positioners improve<br />
the result <strong>of</strong> orthodontic treatment with respect to condylar<br />
axis distraction.<br />
Conclusion<br />
Results <strong>of</strong> the present study indicate a statistically significant<br />
improvement in MI-CR discrepancy in the right horizontal,<br />
right vertical, left vertical, and transverse planes with 2<br />
months <strong>of</strong> gnathologic positioner wear. The amount <strong>of</strong> condylar<br />
distraction in these 4 measurements showed statistically<br />
significant improvement and came within the envelope<br />
<strong>of</strong> susceptibility. The positioner and control groups tend to<br />
change differently over time in the vertical and horizontal<br />
planes, with the positioner group improving and the control<br />
group getting worse. In the transverse plane, gnathologic positioners<br />
improve the result <strong>of</strong> orthodontic treatment with<br />
respect to condylar axis distraction. ■<br />
References<br />
1. Okeson JP. Management <strong>of</strong> Temporomandibular Disorders and Occlusion.<br />
3rd ed. St Louis, MO: Mosby; 1998:109-125.<br />
2. Schmitt ME, Kulbersh R, Freeland T, et al. Reproducibility <strong>of</strong> the<br />
<strong>Roth</strong> power centric in determining centric relation. Semin in Orthod.<br />
2003;9(2):102-108.<br />
3. Andrews LF. The six keys to normal occlusion. Am J Orthod.<br />
1972;(62):196-309.<br />
4. Stuart CE. Good occlusion for natural teeth. J Prosthet Dent.<br />
1964;(14):716-724.<br />
5. <strong>Roth</strong> RH. Temporomandibular pain dysfunction and occlusal relationships.<br />
Angle Orthod. 1973;(43):136-153.<br />
6. <strong>Roth</strong> RH. Treatment mechanics for the straight wire appliance. In:<br />
Graber TM, Swain BH, eds. Orthodontics: Current Principles and<br />
Techniques. St Louis, MO: Mosby; 1985:665-716.<br />
7. <strong>Roth</strong> RH. Occlusion and condylar position. Am J Orthod Dent<strong>of</strong>ac<br />
Orthop. 1995;(107):315-318.<br />
8. Pangrazio-Kulbersh V, Poggio V, Kulbersh R, et al. Condylar distraction<br />
effects <strong>of</strong> two-phase functional appliance/edgewise therapy versus<br />
one-phase Gnathologically based edgewise therapy. Semin in Orthod.<br />
2003;9(2):128-139.<br />
9. <strong>Roth</strong>, RH. The maintenance system and occlusal dynamics. Dent<br />
Clin North AM 1976;20:761-788<br />
10. Arnett GW, Milam SB, Gottesman L. Progressive mandibular<br />
retrusion-idiopathic condylar resorption, part II. Am J Orthod.<br />
1996;(110):117-127.<br />
11. <strong>Roth</strong> RH. Functional occlusion for the orthodontist, part I. J Clin<br />
Orthod. 1981;(15):32-51.<br />
12. Crawford SD. Condylar axis position, as determined by the occlusion<br />
and measured by the CPI instrument, and signs and symptoms <strong>of</strong><br />
temporomandibular dysfunction. Angle Orthod. 1999;(69):103-116.<br />
13. Utt TW, Meyers CE Jr, Wierzba TF, Hondrum SO. A three-dimensional<br />
comparison <strong>of</strong> condylar position changes between centric relation<br />
and centric occlusion using the mandibular position indicator. Am<br />
J Orthod Dent<strong>of</strong>ac Orthop. 1995;(107):298-308.<br />
14. Slavicek R. Interviews on clinical and instrumental functional<br />
analysis for diagnosis and treatment planning, part I. J Clin Orthod.<br />
1988;(22):358-370.<br />
15. Lavine D, Kulbersh R, Bonner P, Pink FE. Reproducibility <strong>of</strong> the<br />
condylar position indicator. Semin in Orthod. 2003;9(2):96-101.<br />
16. Klar NA, Kulbersh R, Freeland T, et al. Maximum intercuspationcentric<br />
relation disharmony in 200 consecutively finished cases in a<br />
gnathologically oriented practice. Semin in Orthod. 2003;9(2):109-<br />
116.<br />
17. Kulbersh R, Dhutia M, Navarro M, et al. Condylar distraction<br />
effects <strong>of</strong> standard edgewise therapy versus gnathologically based<br />
edgewise therapy. Semin in Orthod. 2003;9(2):117-127.<br />
18. Freeland T, Kulbersh R. Orthodontic therapy using the <strong>Roth</strong> gnathologic<br />
approach. Semin in Orthod. 2003;9(2):140-152.<br />
19. <strong>Roth</strong> RH, Rolfs DA. Functional occlusion for the orthodontist, part<br />
II. J Clin Orthod. 1981;(15):100-123.<br />
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
81
Notes<br />
82 Notes
<strong>RWISO</strong> <strong>Journal</strong> | September <strong>2010</strong><br />
83
This year, Rome, next year. . .<br />
Hotel Swissôtel Chicago!<br />
Registration opens December 1, <strong>2010</strong><br />
<strong>RWISO</strong> 2011<br />
18th Annual Conference<br />
May 18-20, 2011 Swissôtel Chicago<br />
Chicago, Illinois, USA