

Jahresbericht 2002/2003 - DRST
Jahresbericht 2002/2003 - DRST
Jahresbericht 2002/2003 - DRST

Sie wollen auch ein ePaper? Erhöhen Sie die Reichweite Ihrer Titel.
YUMPU macht aus Druck-PDFs automatisch weboptimierte ePaper, die Google liebt.
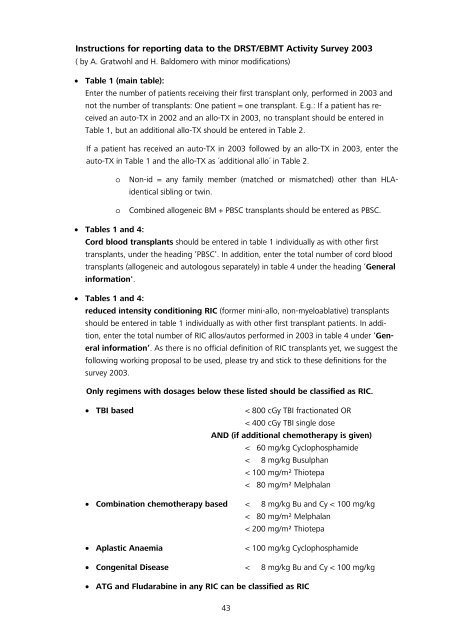
Instructions for reporting data to the <strong>DRST</strong>/EBMT Activity Survey <strong>2003</strong><br />
( by A. Gratwohl and H. Baldomero with minor modifications)<br />
• Table 1 (main table):<br />
Enter the number of patients receiving their first transplant only, performed in <strong>2003</strong> and<br />
not the number of transplants: One patient = one transplant. E.g.: If a patient has received<br />
an auto-TX in <strong>2002</strong> and an allo-TX in <strong>2003</strong>, no transplant should be entered in<br />
Table 1, but an additional allo-TX should be entered in Table 2.<br />
If a patient has received an auto-TX in <strong>2003</strong> followed by an allo-TX in <strong>2003</strong>, enter the<br />
auto-TX in Table 1 and the allo-TX as ´additional allo´ in Table 2.<br />
o Non-id = any family member (matched or mismatched) other than HLAidentical<br />
sibling or twin.<br />
o Combined allogeneic BM + PBSC transplants should be entered as PBSC.<br />
• Tables 1 and 4:<br />
Cord blood transplants should be entered in table 1 individually as with other first<br />
transplants, under the heading ‘PBSC’. In addition, enter the total number of cord blood<br />
transplants (allogeneic and autologous separately) in table 4 under the heading ‘General<br />
information'.<br />
• Tables 1 and 4:<br />
reduced intensity conditioning RIC (former mini-allo, non-myeloablative) transplants<br />
should be entered in table 1 individually as with other first transplant patients. In addition,<br />
enter the total number of RIC allos/autos performed in <strong>2003</strong> in table 4 under ‘General<br />
information’. As there is no official definition of RIC transplants yet, we suggest the<br />
following working proposal to be used, please try and stick to these definitions for the<br />
survey <strong>2003</strong>.<br />
Only regimens with dosages below these listed should be classified as RIC.<br />
• TBI based < 800 cGy TBI fractionated OR<br />
< 400 cGy TBI single dose<br />
AND (if additional chemotherapy is given)<br />
< 60 mg/kg Cyclophosphamide<br />
< 8 mg/kg Busulphan<br />
< 100 mg/m² Thiotepa<br />
< 80 mg/m² Melphalan<br />
• Combination chemotherapy based < 8 mg/kg Bu and Cy < 100 mg/kg<br />
< 80 mg/m² Melphalan<br />
< 200 mg/m² Thiotepa<br />
• Aplastic Anaemia < 100 mg/kg Cyclophosphamide<br />
• Congenital Disease < 8 mg/kg Bu and Cy < 100 mg/kg<br />
• ATG and Fludarabine in any RIC can be classified as RIC<br />
43