2012 ESP Handbook - Alabama Education Association
2012 ESP Handbook - Alabama Education Association
2012 ESP Handbook - Alabama Education Association

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
• Sick leave is granted “upon request” – when you ask<br />
to use it, you can. It is presumed that you are using it<br />
for the reasons outlined in the law.<br />
• Failure to properly “request leave” for an absence<br />
can result in charges of neglect of duty.<br />
• Unused personal leave days can be converted into<br />
sick leave days at the end of the year.<br />
Family Medical Leave<br />
• Federal law (Family Medical Leave Act) requires this<br />
benefit of all businesses that employ over 50<br />
employees.<br />
• Can be used for personal illness or injury, or<br />
attendance upon an ill family member or a new<br />
child.<br />
• To be eligible, employees must have worked a<br />
minimum of 1,250 hours during the previous year.<br />
• Employees can request up to 12 weeks of unpaid<br />
Family Medical Leave. Under some circumstances,<br />
boards may grant extensions.<br />
• During the leave, the board will continue to pay the<br />
state allocation of the employee’s health care<br />
premium (PEEHIP). This is only an advantage to<br />
those covered by PEEHIP.<br />
• If Family Medical Leave (FML) runs out before the<br />
employee is ready to return to work, the employee<br />
can request “unpaid leave” – no benefits are paid by<br />
the board once FML has expired.<br />
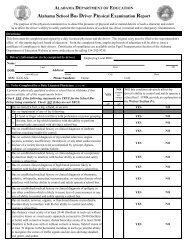
On-The-Job Injury<br />
• Report any injury within 24 hours to your immediate<br />
supervisor. This report may be verbal. However,<br />
we suggest giving a written report and retaining<br />
a copy of the report. (See sample.) In case you<br />
are physically unable to make this report, another<br />
person may make it for you.<br />
• Your school system may have established other<br />
notification procedures or forms by written policy.<br />
Check with your UniServ Director to determine<br />
if there are other procedures or forms to be<br />
completed.<br />
• Your school system may require medical certification<br />
from your physician if you are unable to return to<br />
work as a result of the injury. A second opinion from<br />
a physician may be required at the expense of the<br />
school system.<br />
This is the Law:<br />
6<br />
• Upon determination that you may not return to<br />
work as a result of the on-the-job injury, your salary<br />
and benefits shall be continued for a period of up to<br />
90 work days. Your school system may have adopted<br />
policies that extend this period. Check with your<br />
UniServ Director concerning your school system’s<br />
policies. If you do not report your injury with 24<br />
hours you will not be eligible for this on-the-job<br />
injury leave.<br />
• Additional expenses incurred by you because of the<br />
on-the-job injury may be filed for reimbursement<br />
with the State Board of Adjustment. These would<br />
include, but not be limited to, medical co-pays,<br />
prescriptions, and lost wages over 90 days. THIS<br />
CLAIM MUST BE FILED WITHIN ONE (1) YEAR<br />
OF THE INCIDENT. Your UniServ Director can<br />
provide you with assistance in filing your claim.<br />
Sick Leave Bank<br />
• Committee (elected from among participating<br />
employees) sets guidelines for operation.<br />
• Provides for “catastrophic leave” benefits –<br />
extended leave covered by days donated by other<br />
participating employees from any school system in<br />
<strong>Alabama</strong>.<br />
• Catastrophic leave may be used for pregnancy.<br />
• Only members of a sick leave bank can donate days<br />
or receive donated days in the event of a catastrophic<br />
illness.<br />
(continued on next page)<br />
Sample Initial Reporting Form:<br />
Employee Name __________________________<br />
Date _________________________<br />
School/Department _____________ _____________<br />
Site of Injury __________ _____________<br />
Description of Injury __________________________<br />
Employee Signature _________ _________________<br />
Supervisor’s Signature ____ _______________