

germ cell tumors germ cell tumors- biology - Plataforma de Oncología
germ cell tumors germ cell tumors- biology - Plataforma de Oncología
germ cell tumors germ cell tumors- biology - Plataforma de Oncología

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
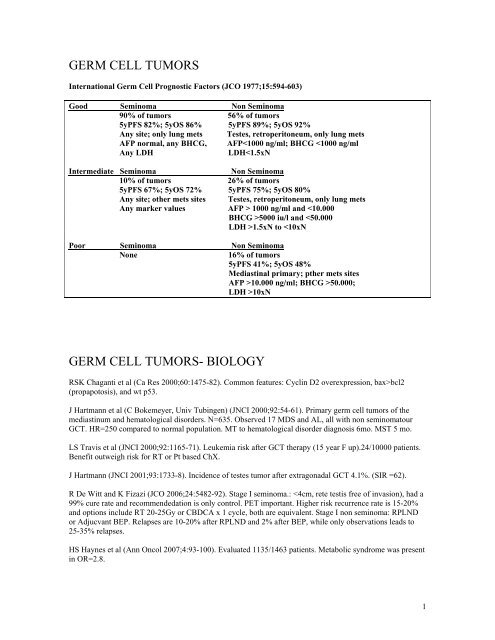
GERM CELL TUMORS<br />
International Germ Cell Prognostic Factors (JCO 1977;15:594-603)<br />
Good Seminoma Non Seminoma<br />
90% of <strong>tumors</strong> 56% of <strong>tumors</strong><br />
5yPFS 82%; 5yOS 86% 5yPFS 89%; 5yOS 92%<br />
Any site; only lung mets Testes, retroperitoneum, only lung mets<br />
AFP normal, any BHCG, AFP10xN<br />
GERM CELL TUMORS- BIOLOGY<br />
RSK Chaganti et al (Ca Res 2000;60:1475-82). Common features: Cyclin D2 overexpression, bax>bcl2<br />
(propapotosis), and wt p53.<br />
J Hartmann et al (C Bokemeyer, Univ Tubingen) (JNCI 2000;92:54-61). Primary <strong>germ</strong> <strong>cell</strong> <strong>tumors</strong> of the<br />
mediastinum and hematological disor<strong>de</strong>rs. N=635. Observed 17 MDS and AL, all with non seminomatour<br />
GCT. HR=250 compared to normal population. MT to hematological disor<strong>de</strong>r diagnosis 6mo. MST 5 mo.<br />
LS Travis et al (JNCI 2000;92:1165-71). Leukemia risk after GCT therapy (15 year F up).24/10000 patients.<br />
Benefit outweigh risk for RT or Pt based ChX.<br />
J Hartmann (JNCI 2001;93:1733-8). Inci<strong>de</strong>nce of testes tumor after extragonadal GCT 4.1%. (SIR =62).<br />
R De Witt and K Fizazi (JCO 2006;24:5482-92). Stage I seminoma.:
D Sharp et al MSKCC (JCO 2008;26:5524-9). Inci<strong>de</strong>nce of late recurrences in the literature 3.2% in non<br />
seminomatous and 1.4% in seminoma. Frequent in non operated retroperitoneal mets. MSKCC series 75<br />
patients, interval 2.1-37.7 years. Complete resection 5yOS 79%, vs non completely resected 36%. Better for<br />
untreated patients.<br />
E <strong>de</strong> Haas et al (JCO 2008;26:2817-23). Bleomycin hydrolase gene SNP A1450G homozygous G/G worst<br />
survival as compared t6o heterozygous A/G and wt A/A. Series of 31, 133 and 140 patients respectively.<br />
HR=4.97. Differences in OS at 20y were 90% vs 60%.<br />
BS Carver et al MSKCC (JCO2007;25:1033-7). Tweratoma found in 40% postchemotherapy RPLND. Series<br />
of 210 patients with teratoma: mature 85%, with malignant transformation 8%, and with inmature teratoma<br />
8%. M F up 37 mo: 5yDFS 83% and 10yDFS 80%. Recurrences were: 10 teratoma, 5 with malignant<br />
transformation and 15 (50%) with GCT.<br />
GERM CELL TUMORS – ADJUVANT THERAPY<br />
P Albers et al (JCO 2008;26:2966-72). N=382 stage I NSGCT, postorchi<strong>de</strong>ctomy, MF up 4.7y. Randomized<br />
to RPLND (15 recurrences/191; 2yRFS 91.8%, HR=7.9) vs BEPx1 (2 recurrences/191; 2yRFS 99.4%).<br />
GERM CELL TUMORS – ADVANCED DISEASE<br />
BEP: Bleo is an essential component (10% OS gain, Indiana randomized trial).<br />
VIP<br />
VeIP (only 10% long term survivors)<br />
BEP va CEP (CBDCA inferior to CDDP) (Randomized German, EORTC trials)<br />
BEP = VIP (Intergroup USA)<br />
BEP x 3 =BEP x 4<br />
POMP�EPI in poor prognosis group (2yPFS 58%)<br />
TXL-IFX-CDDP second line (OR 80%).<br />
GEM active second line<br />
S Hinton et al (L Einhorn) (JCO 2002;20:1859-63). N=28 refratory. TXL 110 mg/m2 d 1, 8 & 15 + GEM<br />
1000 mg/m2 d 1, 8, & 15 q 4 wk x 6. OR 21.4% (3 CR NED 15+ to 25+ mo).<br />
T Miki et al Osaka (Cancer 2002;95:1879-85). N=20 refractory. CPT 150 mg/m2+CDDP 20 mg/m2 x 5 d.<br />
OR 50% 5yOS 53%. Active salvage therapy.<br />
C Kollmannsberger et al (C Bokemeyer). (JCO2004;22:108-114). N=35, refractory, 89% recerrence after<br />
BMT. GEM 1000 mg/m2 d 1 & 8 + LOHP 130 mg/m2 d 1 q 4 wk. OR 46%, CR 3. CDDP refratory OR 44%.<br />
B Cushing et al POG-CCG (JCO 2004;22:2691-700). N=299, children. Randomized to BEP conventional<br />
(CDDP 20 mg/m2x 5) (6yEFS 80%, 6yOS 86%) vs HD CDDP (40 mg/m2 x 5) and rest same dose (6yEFS<br />
89.6%, 6yOS 91%(), indicating a better EFS for children at higher doses.<br />
HJ Schmall et al (C Bokemeyer) (JCO 2003;21:4083-91). N=221, poor prognosis Indiana criteria. VIP x 1<br />
�HD VIP + SCAT q 3 wk x 3-4. DLT for CDDP 100 mg/m2 + VP 1750 mg/m2 + IFX 12 g/m2 (mucositis,<br />
CNS, renal and hematological toxicity). M fup 4 y: 5y PFS 68%, 5y DSS 73%.<br />
2
C Kollmannsberger et al (Cancer 2006;106:1217-26). Review platrinum refractory testicular GCT. CDDP<br />
refractory shows progression within 4 wks of platinum based chemotherapy. Active drugs: TXL: OR 25%,<br />
GEM OR 145-17%, LOHP OR 13%. Combinations: TXL-GEM OR 21%; GEM + LOHP =R 32-46%; CPT-<br />
CDDP or CTP/LOHP 40-50% OR,(CPT no activity shown in single agent data).<br />
GV Kondagunta et al MSKCC (JCO 2005;27:6549-55). N=46, erecurrence after an initial CR. TIP:TXL 250<br />
mg/m2 civi 24 h d 1 + IFX 1500 mg/m2 x 4d d2-5+ CDDP 25 mg/m2 x 4 d 2-5 + MESNA 500 mg/m2 x 3<br />
after each IFX + DXMTS 20 mg + GCSF 5 ug/kg d 7-18. OR= 32/46 (CR 70%), 2 relapses, 29 continuously<br />
NED. M F up 69 mo, 63% durable responses. 2 yPFS 65%. Patient selection important...<br />
P Bedano et al (LH Einhorn) (JCO 2006;24:5403-7). N=30, recurrent after initial CDDP. EPI 90 mg/m2 d 1 +<br />
CDDP 20 mg/m2 d 1-5 q 3 wk x 4. OR 9 CR (7 NED 25 + to 48+ mo). Active. Acceptable toxicity.<br />
GV Kondagunta et al (JCO 2007;25:85-90). N=48 PD and high risk recurrences. TICE= TXL 200 mg/ m2<br />
civi 24 h + IFX 2 g/m2 x 3 d + Apheresis d 11-13 x 2 cycles, & then CBDCA AUC 21 +VP 400 mg/m2 x 3d<br />
+PBSC x 3 cycles. CR 49% + 6% after surgery (total 26/47. 6 relapses. 24 NED at M F up 40 mo. Prior<br />
experience reported with TICE had CR 56% and NED 50%, quite similar results).<br />
J Hartmann et al (C Bokemeyer) (JCO 2007;25:5742-7). Poor IGCC prognosis group. HDChX. Program<br />
consisted in Standard VIP (1 st cycle without TXL to collect progenitors). VP 1500 mg/m2 + IFX 10 g/m2 +<br />
CDDP 100 mg/m2 (+TXL 135-225 mg/m2, 3 cohorts). Results: 52/53 pts completed 152 cycles. MD<br />
WBC1yCR 52%).<br />
NO differences found. Poor prognostic group AFP half life >7d; BHCG half life >3.5 d had a >1yCR 34%<br />
BEP and 61% HDChX!!.<br />
3
GERM CELL TUMORS - SEMINOMA<br />
JA Arranz et al (Germa Lluch JR) (Ann Oncol 2001;12:487-91). N=64, seminoma, stage IIa/b M Fup 34 mo.<br />
CDDP 25 mg/m2 x 4 + VP 100 mg/m2 x 4 q 3 wk. OR 98% (CR 69%), Failure rate 11%, Neutropenia gr 3-4,<br />
32%. 3yTTF 89%; 3yOS 97%.<br />
J Vuky et al MSKCC (JCO 2001;20:297-301). N=27, failure 1 st line therapy. CDDP + IFX. 14 alive DFS<br />
(48%) M F up 72 mo.<br />
P War<strong>de</strong> et al (JCO 2002;20:4448-52). N=638, M F up 7 y. Stage I seminoma (pooled data from UK,<br />
Denmark, Canada). 5yRFS 82.3%, with 121 relapses. Factors: size >4cm, invasion rete testis, invasion small<br />
vessels. Multivariate HR 2 & 1.7.<br />
WG Jones et al (JCO 2005;23:1200-8). Stage I seminoma, after orchi<strong>de</strong>ctomy. M F up 61 mo. Randomized to<br />
20 Gy/10F/2wk (Relapses 10), vs 30 Gy/15F/3wk (Relapses 11, 0.7% difference. (Toxicity criteria indicated a<br />
difference 20% vs 5%).<br />
5

