

Ludwig's angina and mediastinitis due to Streptococcus milleri ...
Ludwig's angina and mediastinitis due to Streptococcus milleri ...
Ludwig's angina and mediastinitis due to Streptococcus milleri ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Eur Respir J<br />
1990, 3, 728-731<br />
CASE REPORT<br />
<strong>Ludwig's</strong> <strong>angina</strong> <strong>and</strong> <strong>mediastinitis</strong> <strong>due</strong> <strong>to</strong> Strep<strong>to</strong>coccus <strong>milleri</strong>:<br />
usefulness of computed <strong>to</strong>mography<br />
X. van der Brempt*, G. Derue*, F. Severin**, L. Colin***, J-P. Gilbeaut, F. Heifer*<br />
<strong>Ludwig's</strong> <strong>angina</strong> <strong>and</strong> <strong>mediastinitis</strong> <strong>due</strong> <strong>to</strong> Strep<strong>to</strong>coccus <strong>milleri</strong>: usefulness of<br />
computed <strong>to</strong>mography. X. van der Brempt, G. Derue, F. Severin, L. Colin,<br />
J-P. Gilbeau, F. Helier.<br />
ABSTRACT: Despite Intensive use of antibiotics, <strong>Ludwig's</strong> <strong>angina</strong><br />
remains a potentially lethal Infection because of the risk of upper airway<br />
obstruction <strong>and</strong> spread In<strong>to</strong> the mediastinum. We present two patients<br />
who survived <strong>mediastinitis</strong> complicating <strong>Ludwig's</strong> <strong>angina</strong> <strong>due</strong> <strong>to</strong><br />
Strep<strong>to</strong>coccus <strong>milleri</strong>. Computed <strong>to</strong>mography performed early In the<br />
course of the disease detected pus collections <strong>and</strong> directed appropriate<br />
drainage procedures.<br />
Eur Respir J., 1990, 3, 728-731.<br />
<strong>Ludwig's</strong> <strong>angina</strong> (LA) is a rapidly spreading cellulitis<br />
involving sublingual <strong>and</strong> submaxillary spaces [1]. Two<br />
major complications of LA are life-threatening upper<br />
airway obstruction <strong>and</strong> infectious seeding of the mediastinum,<br />
which were responsible for a high mortality<br />
rate before the antibiotic era: more than 50% in LA [2],<br />
<strong>and</strong> from 50% (with surgical drainage) <strong>to</strong> 86% (without<br />
surgical drainage) in <strong>mediastinitis</strong> [3]. We report<br />
two cases of LA <strong>and</strong> <strong>mediastinitis</strong> of dental origin.<br />
Although the detection of the cervical <strong>and</strong> mediastinal<br />
collections is usually difficult in such cases, the early<br />
use of computed <strong>to</strong>mography (CT) allowed appropriate<br />
surgical drainage <strong>and</strong> probably contributed <strong>to</strong> the<br />
survival of our patients.<br />
Case 1<br />
A mildly retarded 17 yr old girl was admitted because<br />
of fever <strong>and</strong> dysphagia. She complained of <strong>to</strong>othache for<br />
several days. Two days before entry, temperature rose<br />
<strong>to</strong> 39.5°C.<br />
Physical examination showed bilateral subm<strong>and</strong>ibular<br />
swelling, trismus <strong>and</strong> oedema of the floor of the<br />
mouth. Pulse rate was 120 b·min· 1 • Temperature was<br />
36.8°C <strong>and</strong> the patient was not dyspnoeic.<br />
Abnormal labora<strong>to</strong>ry findings included erythrocyte<br />
sedimentation rate 70 mm·h- 1 , fibrinogen level 622<br />
mg·dl· 1 , white blood cell count 11,800·mm- 3 with 10,000<br />
neutrophils. Chest X-ray showed slight enlargement of<br />
the superior mediastinum. Ampicillin (2 g i.v. every 6 h)<br />
was given as well as indomethacin (100 mg·day· 1 for 2<br />
days) <strong>and</strong> a single dose of methylprednisolone (125 mg)<br />
for the incipient upper airway obstruction.<br />
On the second day, cellulitis extended <strong>to</strong> the anterior<br />
chest wall with subcutaneous emphysema. A left pleural<br />
rub was heard <strong>and</strong> the abdomen was tender <strong>and</strong> silent.<br />
• Dept of Internal Medicine, •• Dept of Bacteriology,<br />
•u Intensive Care Unit <strong>and</strong> ' Dept of Radiology,<br />
Hopital de Jolimont, Haine-Saint-Paul, Belgium.<br />
Correspondence: Dr G. Derue, H()pital de Jolimont,<br />
Rue Ferrer, B-7161 Ha.ine-Saint-Paul, Belgium.<br />
Keywords: Computed <strong>to</strong>mography; <strong>Ludwig's</strong> <strong>angina</strong>;<br />
<strong>mediastinitis</strong>.<br />
Received: August 9, 1989; accepted after revision<br />
February 17, 1990.<br />
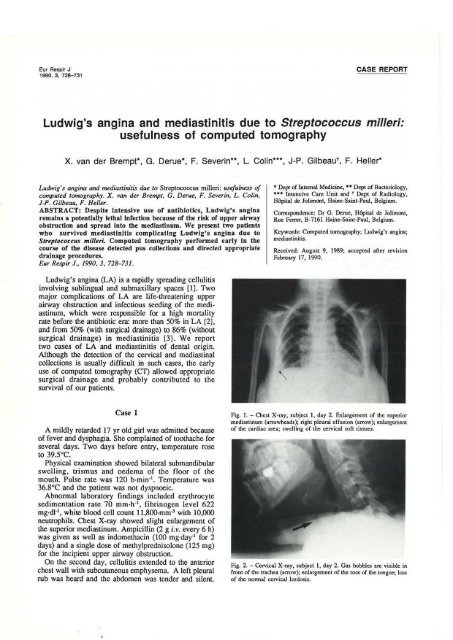
Fig. I.- Chest X-ray, subject I, day 2. Enlargement of the superior<br />
mediastinum (arrowheads); right pleural effusion (arrow); enlargement<br />
of the cardiac area; swclling of the cervical soft tissues_<br />
Fig. 2. -Cervical X·ray, subject I, day 2. Gas bubbles are visible in<br />
front of the trachea (arrow); enlargement of the root of the <strong>to</strong>ngue; loss<br />
of the normal cervical lordosis-
a<br />
c<br />
LUDWIG'S ANGINA AND MEDIASTINITIS 729<br />
Fig. 3. - CT scan of subject 1, day 3 (without contrast medium). a) CT scan of the neck at the level of the subglonic trachea. Infectious process<br />
infiltrates the anterior pan of the neck with gas production <strong>and</strong> abnormal densities of fat, partially blurring the thyroid <strong>and</strong> vessels margins. b) CT<br />
scan of the chest at the level of the carina. Gas bubbles in the anterior compartment of the mediastinum; posterior right pleural collection. c) CT<br />
scan of the chest at the level of the right inferior pulmonary vein. Gas is visible in the retrostemal space. Right pleural collections are visible in<br />
the interlobar <strong>and</strong> posterior pleural space.<br />
Chest X-ray showed a right pleural effusion, gas bubbles<br />
in the pretracheal space <strong>and</strong> enlargement of the cardiac<br />
area (figs 1 <strong>and</strong> 2).<br />
On the third day, a loud pericardial friction rub<br />
was noted. Temperature was 37 .6°C. Blood cultures<br />
remained sterile. Cervical echography failed <strong>to</strong> demonstrate<br />
an abscess formation, whereas CT showed free<br />
gas in the pretracheal space <strong>and</strong> in the retrostemal space,<br />
an abnormal density of fat <strong>due</strong> <strong>to</strong> infiltration by the<br />
infectious process with partial blurring of the normal<br />
cervico-mediastinal structure, <strong>and</strong> a right pyothorax<br />
(fig. 3). Echocardiogram was normal.<br />
The patient was transferred <strong>to</strong> the intensive care unit.<br />
After endotracheal intubation, surgical drainage of the<br />
cervical, mediastinal <strong>and</strong> pleural collections were<br />
performed according <strong>to</strong> the CT data. Cultures yielded<br />
Strep<strong>to</strong>coccus <strong>milleri</strong> sensitive <strong>to</strong> penicillin <strong>and</strong> its<br />
derivatives.<br />
b<br />
Despite an acute respira<strong>to</strong>ry distress syndrome,<br />
the patient's condition slowly improved. Her carious<br />
teeth were extracted <strong>and</strong> she was discharged after 77<br />
days.<br />
Case 2<br />
A 49 yr old alcoholic man presented 7 days after<br />
multiple dental extractions with stridor, swelling of<br />
the cervical region, trismus <strong>and</strong> elevation of the<br />
floor of the mouth. Temperature was 39.6°C. Erythrocyte<br />
sedimentation rate was 70 mm·h- 1 , fibrinogen<br />
level 579 mg·dt-1, white blood cell count 19,800·mm- 3 •<br />
Chest X-ray showed a normal mediastinum<br />
<strong>and</strong> bilateral basal pulmonary infiltrates. The patient<br />
was treated with amoxycillin (1 g i. v. every 6 h)<br />
<strong>and</strong> metronidazole (500 mg i.v. every 8 h);
730<br />
methylprednisolone (40 mg every 8 h) was added<br />
because of upper airway oedema.<br />
Eighteen hours after entry, subcutaneous emphysema<br />
was noted with persistent stridor <strong>and</strong> increased dyspnoea.<br />
Chest X-ray showed enlargement of the superior<br />
mediastinum. The patient was transferred <strong>to</strong> the intensive<br />
care unit. Pharyngeal haemorrhage <strong>and</strong> aspiration of<br />
blood required endotracheal intubation.<br />
On the third day, er showed a m<strong>and</strong>ibular abscess<br />
extending <strong>to</strong> the pretracheal space <strong>and</strong> the anterior<br />
mediastinum with bilateral pulmonary infiltrates. Surgical<br />
drainage of the cervical <strong>and</strong> mediastinal collections<br />
allowed aspiration of foul-smelling pus. Cultures<br />
yielded Strep<strong>to</strong>coccus <strong>milleri</strong>.<br />
Despite a cardiac arrest with resuscitation, the<br />
patient's condition improved slowly <strong>and</strong> he was<br />
discharged after 67 days.<br />
Discussion<br />
Causative organisms of LA are mostly commensals of<br />
oropharyngeal mucosae (strep<strong>to</strong>cocci, anaerobes). Mixed<br />
aero-anaerobic infections are common [1, 4]. In the two<br />
reported cases, the only isolated pathogen was<br />
Strep<strong>to</strong>coccus <strong>milleri</strong>, but cultures were obtained after<br />
the beginning of treatment with antibiotics <strong>and</strong> we<br />
cannot be sure that S. <strong>milleri</strong> was the only causative<br />
micro-organism. This microaerophilic bacterium was first<br />
isolated in dental abscesses [5], but it may cause<br />
other suppurative infections including sinusitis,<br />
meningitis, arthritis, endocarditis, peri<strong>to</strong>nitis, perineal<br />
hidradenitis, perirenal abscess <strong>and</strong> empyema [6-8]. It is<br />
one of the most common pathogens isolated in frontal<br />
brain [9] <strong>and</strong> liver abscesses [10]. S. <strong>milleri</strong> is susceptible<br />
in vitro <strong>to</strong> penicillin, clindamycin <strong>and</strong> chloramphenicol;<br />
it is resistant <strong>to</strong> tetracyclines in 36% of the cases<br />
<strong>and</strong> always resistant <strong>to</strong> metronidazole [6].<br />
The most common aetiological fac<strong>to</strong>r of LA is dental<br />
infection, which is responsible for 85% of cases [11].<br />
Other causes include nasopharyngeal surgery or trauma,<br />
<strong>to</strong>nsillitis (post-<strong>angina</strong>l sepsis) <strong>and</strong> rarely subm<strong>and</strong>ibular<br />
sialadenitis, erysipelas, furuncles or infected thyroglossal<br />
duct cysts [4, 12].<br />
In a recent review on LA, spread of infection in<strong>to</strong> the<br />
neck <strong>and</strong> mediastinum occurred in 5 of 141 cases (4%)<br />
[11]. This spread is influenced by several fac<strong>to</strong>rs: 1) the<br />
ana<strong>to</strong>my of the cervical fascia allows cervical infections<br />
<strong>to</strong> spread easily in<strong>to</strong> the mediastinum, by creating<br />
longitudinal spaces: the pretracheal space, the retropharyngeal<br />
space ("the danger space", which communicates<br />
freely with the mediastinum), the visceral compartment<br />
containing carotid arteries, jugular veins <strong>and</strong> vagus<br />
nerves [12-14]; 2) the inspira<strong>to</strong>ry negative intrathoracic<br />
pressure occurring during spontaneous ventilation<br />
might favour aspiration of infected material (air,<br />
saliva, bacteria) from the neck in<strong>to</strong> the mediastinum [13];<br />
3) spread of cervical infections is more frequent in<br />
diabetics, alcoholics <strong>and</strong> in other conditions of<br />
immunodepression <strong>and</strong> poor nutrition [11, 15]; 4)<br />
inadequate initial management <strong>and</strong> treatment can<br />
X. VAN DER BREMPT ET AL.<br />
worsen the prognosis, e.g. insufficient or delayed<br />
surgical drainage, or use of antibiotics inactive against<br />
anaerobic flora. Corticosteroids were used in our cases<br />
<strong>and</strong> in some others [16-18] in order <strong>to</strong> reduce the upper<br />
airway oedema. Although no controlled studies are<br />
available concerning their efficacy or harmfulness,<br />
steroidal <strong>and</strong> nonsteroidal anti-inflamma<strong>to</strong>ry agents<br />
might be deleterious in a clearly infectious process<br />
because of their immunosuppressive action [19].<br />
The complications of <strong>mediastinitis</strong> include empyema<br />
(often bilateral), pneumothorax, pulmonary abscess,<br />
aspiration pneumonia, pericarditis with or without<br />
effusion, septic oesophageal perforation, erosion of the<br />
aorta, subphrenic abscess <strong>and</strong> retroperi<strong>to</strong>nitis [4, 12, 13,<br />
15].<br />
Other complications of LA include thrombophlebitis<br />
of the internal jugular vein, rupture of the carotid<br />
artery, metastatic abscesses <strong>and</strong> necrosis of the <strong>to</strong>ngue<br />
[4, 11, 13].<br />
Because of the rapid spread of this infection through<br />
the cervical <strong>and</strong> mediastinal compartments, <strong>and</strong> the<br />
possible insidious initial course of the disease, CT should<br />
be performed as soon as possible. Conventional X-ray<br />
films of the neck <strong>and</strong> chest may show gas in the tissue,<br />
air-fluid levels, loss of the normal cervical lordosis<br />
or mediastinal widening [13, 16], but they do not delineate<br />
the extension of the infection. In contrast, in our<br />
cases <strong>and</strong> in some others [16, 20--23], CT adequately<br />
detected pus collections <strong>and</strong> mediastinal extension.<br />
CT findings included pleural <strong>and</strong> pericardial<br />
effusions [22, 23], osteomyelitis of the rib [22],<br />
retropharyngeal, parapharyngeal <strong>and</strong> mediastinal abscesses<br />
or air collections [16, 20--22], usually ill-defined <strong>and</strong><br />
infiltrating the normal cervico-mediastinal structures.<br />
These findings allowed adequate surgical drainages,<br />
which are m<strong>and</strong>a<strong>to</strong>ry when <strong>mediastinitis</strong> is present.<br />
Although the number of patients is <strong>to</strong>o small <strong>to</strong> draw<br />
definite conclusions, the early use of CT appears <strong>to</strong><br />
improve the prognosis of these patients.<br />
Acknowledgements: The authors thank Dr J. Orehek<br />
<strong>and</strong> Dr. W. Merrill for their suggestions concerning the<br />
manuscript.<br />
References<br />
1. Patterson HC, Kelly JH, Strome M. -<strong>Ludwig's</strong> <strong>angina</strong>:<br />
an update. Laryngoscope, 1982, 92, 370-377.<br />
2. Williams AC. - <strong>Ludwig's</strong> <strong>angina</strong>. Surg Gynecol Obstet,<br />
1940, 70, 140-149.<br />
3. Pearse HE. - Mediastinitis following cervical suppuration.<br />
Ann Surg, 1938, 108, 588-611.<br />
4. Hall SF. - <strong>Ludwig's</strong> like <strong>angina</strong> (pseudo-<strong>angina</strong><br />
Ludovici). J O<strong>to</strong>laryngol, 1984, 13, 321-324.<br />
5. Guthof 0. -Pathogenic strains of Strep<strong>to</strong>coccus viridans,<br />
strep<strong>to</strong>cocci found in dental abscesses <strong>and</strong> infiltrates in the<br />
region of the oral cavity. Zentralbl Bakteriol Naturwiss, 1956,<br />
166, 553-564.<br />
6. Higuet AS, Warren RE, Staugh<strong>to</strong>n RCD, Roberts SOB.<br />
Strep<strong>to</strong>coccus <strong>milleri</strong> causing treatable infection in<br />
perineal hidradenitis suppurativa. Br J Derma<strong>to</strong>l, 1980, 103,<br />
375-382.
7. Murray HW, Gross KC, Masur H, Roberts RB.- Serious<br />
infections caused by Strep<strong>to</strong>coccus <strong>milleri</strong>. Am J Med, 1978,<br />
64, 759-764.<br />
8. Tecson-Tumang F, Sen P, Kapila R. - Fatal Strep<strong>to</strong>coccus<br />
MG-intermedius (Strep<strong>to</strong>coccus <strong>milleri</strong>) meningitis in an<br />
adult. Am J Clin Pathol, 1982, 77, 480-484.<br />
9. De Louvois J, Gortvai P, Hurley R. - Bacteriology<br />
of abscesses of the central nervous system: a multicentre<br />
prospective study. Br Med J, 1977, 2, 981-984.<br />
10. Moore-Gillon JC, Eykyn SJ, Phillips I. - Microbiology<br />
of pyogenic liver abscess. Br Med J, 1981, 283, 819-821.<br />
11. Morel<strong>and</strong> LW, Corey J, McKenzie R. - <strong>Ludwig's</strong> <strong>angina</strong>:<br />
report of a case <strong>and</strong> review of the literature. Arch Intern Med,<br />
1988, 148, 461-466.<br />
12. Bounds GA. - Subphrenic <strong>and</strong> mediastinal abscess<br />
formation: a complication of <strong>Ludwig's</strong> <strong>angina</strong>. Br J Oral<br />
Maxillofac Surg, 1985, 23, 313-321.<br />
13. Scully RE, Galdabini JJ, McNeely BU. - Case records<br />
of the Massachusetts General Hospital: case 15-1978. N Engl<br />
J Med, 1978, 298, 894-902.<br />
14. Moncada R, Warpeha R, Picklemen J, Spak M, Cardoso<br />
M, Berkow A, White H. - Mediastinitis from odon<strong>to</strong>genic<br />
<strong>and</strong> deep cerival infection. Chest, 1978, 73, 497-500.<br />
15. Howell HS, Prinz RA, Pickleman JR. - Anaerobic<br />
<strong>mediastinitis</strong>. Surg Gynecol Obstet, 1976, 143, 353-359.<br />
16. Barsamian JG, Scheffer RB. - Spontaneous pneumothorax:<br />
an unusual occurence in a patient with <strong>Ludwig's</strong> <strong>angina</strong>.<br />
J Oral Maxillofac Surg, 1987, 45, 161-168.<br />
17. Baron D, Malinge M, Mercier J, Blanloeil Y, Nicolas<br />
F, Delaire J. - Gas gangrene of dental origin; report on<br />
four cases. Rev S<strong>to</strong>matal Chir Maxillofac, 1981, 82,<br />
366--369.<br />
LUDWIG'S ANGINA AND MEDIASTINITIS 731<br />
18. Guittard P, Ducasse JL, Jorda MF, Eschapasse H, Lareng<br />
L. - Anaerobic odon<strong>to</strong>genic <strong>mediastinitis</strong>. Ann Fr Anesth<br />
Reanim, 1984, 3, 216-218.<br />
19. Rimailho A, Riou B, Richard C, Auzepy P. -Fulminant<br />
necrotizing fasciitis <strong>and</strong> non-steroidal anti-inflamma<strong>to</strong>ry drugs.<br />
J Infect Dis, 1987, 155, 143-146.<br />
20. Rubin MM, Cozzi GM. - Fatal necrotizing <strong>mediastinitis</strong><br />
as a complication of an odon<strong>to</strong>genic infection. J Oral Maxillofac<br />
Surg, 1987, 45, 529-533.<br />
21. Snow N, Lucas AE, Grau M, Steiner M. - Purulent<br />
mediastinal abscess secondary <strong>to</strong> <strong>Ludwig's</strong> <strong>angina</strong>. Arch<br />
O<strong>to</strong>laryngol, 1983, 109, 53-55.<br />
22. Levine TM, Wurster' CF, Krespi YP. - Mediastinitis<br />
occuring as a complication of odon<strong>to</strong>genic infections.<br />
Laryngoscope, 1986, 96, 747-750.<br />
23. Estrera AS, L<strong>and</strong>ay MJ, Grisham JM, Sinn DP, Platt MR.<br />
- Descending necrotizing <strong>mediastinitis</strong>. Surg Gynecol Obstet,<br />
1983, 157, 542-552.<br />
Angine de Ludwig et midiastinite <strong>due</strong>s a Strep<strong>to</strong>coccus rnilleri.<br />
Inter et d' une <strong>to</strong>mographie computerisee. X. van der Brempt, G.<br />
Derue, F. Severin, L. Colin, J-P. Gilbeau, F. Helier.<br />
RESUME: Malgre !'usage intensif des antibiotiques, l'angine<br />
de Ludwig reste une infection potentiellement mortelle a cause<br />
du risque d'obstruction des voies aeriennes superieures et de<br />
dissemination vers le mediastin. Nous presen<strong>to</strong>ns deux patients<br />
ayant survecu a une mediastinite compliquant une angine de<br />
Ludwig a Strep<strong>to</strong>coccus <strong>milleri</strong>. Un scanner cervico-thoracique<br />
pratique precocement permit la detection des collections<br />
purulentes et guida les manoeuvres de drainage appropriees.<br />
Eur Respir J., 1990, 3, 728-731.













