mmpc - National Indian Health Board
mmpc - National Indian Health Board
mmpc - National Indian Health Board

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
MEDICARE, MEDICAID, & HEALTH REFORM<br />
POLICY COMMITTEE (MMPC)<br />
FACE TO FACE MEETING<br />
Tuesday, November 13, 2012<br />
9:00am-5:00pm EST<br />
KAISER FAMILY FOUNDATION, BARBARA CONFERENCE CENTER
MISSION STATEMENT<br />
The Medicare, Medicaid and <strong>Health</strong> Reform Policy Committee (MMPC) is a<br />
standing committee of the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NIHB). The committee<br />
is chaired by a member of the NIHB <strong>Board</strong> of Directors. The primary purpose of<br />
MMPC is to provide technical support to the Tribal Technical Advisory Group to<br />
the Centers for Medicare and Medicaid Services (TTAG). TTAG is a group<br />
codified by the American Reinvestment and Recovery Act of 2009 and is<br />
composed of formally appointed representatives from each <strong>Indian</strong> <strong>Health</strong><br />
Service (IHS) Areas as well as from specific national <strong>Indian</strong><br />
organizations. TTAG advises the Centers for Medicare and Medicaid Services<br />
(CMS) on <strong>Indian</strong> issues related to Medicare, Medicaid, the Children’s <strong>Health</strong><br />
Insurance Program (CHIP), and any other health care program funded (in whole<br />
or part) by CMS. MMPC continues work on the Affordable Care Act (ACA) and<br />
<strong>Indian</strong> <strong>Health</strong> Care Improvement Act (IHCIA) health policy issues, regulation<br />
review and the development of draft positions with the greatest opportunities<br />
and highest priority for the <strong>Indian</strong> <strong>Health</strong> System.<br />
MMPC also acts as a national forum to identify, discuss, advise and act on issues<br />
that will improve the health of American <strong>Indian</strong>s and Alaska Natives. In this<br />
capacity MMPC has the ability to pool expertise in <strong>Indian</strong> health care from<br />
across the country in order to develop information and recommendations on<br />
current issues. Implementation of components of the <strong>Indian</strong> <strong>Health</strong> Care<br />
Improvement Act and the Patient Protection and Affordable Care Act that are<br />
outside the jurisdiction of CMS are examples.<br />
Membership in MMPC is open to individuals authorized to represent: a Tribe;<br />
Tribal Organization; Urban <strong>Indian</strong> Program; or <strong>Indian</strong> <strong>Health</strong> Service (IHS). For<br />
more information or to join the MMPC distribution list please contact Liz<br />
Heintzman at lheintzman@nihb.org.
GENERAL INFORMATION<br />
TABLE OF CONTENTS<br />
MMPC FACE TO FACE AGENDA 1<br />
MMPC ACTION PLAN, TASKS, & ASSIGNMENTS 3<br />
MMPC OCTOBER TELECONFERENCE AGENDA NOTES 16<br />
ACTIVE, NEW & ONGOING MMPC/TTAG ISSUES, STATUS, GOALS & NEXT STEPS<br />
IRS SEPTEMBER MEETING NOTES 20<br />
INDIAN ADDENDUM COMPANION PIECE 23<br />
INDIAN ADDENDUM 30<br />
TRIBAL CONSULTATION WITH HHS ON FFE/MEDICAID EXPANSION NOTES 35<br />
NIHB COMMENT TO ALL INCLUSIVE REIMBURSEMENT RATE AGREEMENT 44<br />
TSGAC COMMENT TO ALL INCLUSIVE REIMBURSEMENT RATE AGREEMENT 46<br />
SUMMARY OF INDIAN SPECIFIC BENEFITS AND PROTECTIONS 50<br />
CHART OF INDIAN SPECIFIC HEALTH CARE PROVISIONS 52<br />
WHITE HOUSE LETTER FROM CRIHB & NPAIHB 53<br />
AMENDMENT TO ACA REGARDING AI/AN DEFINITION 56<br />
ENABLING EXCHANGES IMPLEMENT A STREAMLINED APPLICATION PROCESS PAPER 57<br />
MEDICAID REPORT FROM CRIHB 73<br />
DEAR TRIBAL LEADER REGARDING HHS CONSULTATION LETTER 123<br />
TRIBAL CONSULTATION POLICY 124<br />
TTAG FACE TO FACE PREPARATION ___<br />
TTAG AGENDA 134<br />
BEHAVIORAL HEALTH DOCUMENTS ___<br />
HHS BLOCK GRANT REGULATIONS 137<br />
NPAIHB COMMENTS TO IHS NATIONAL BEHAVIORAL STRATEGIC PLAN 150<br />
NPAIHB COMMENTS FOR UNIFORM APPLICATION FOR MENTAL HEALTH BLOCK GRANT 154<br />
NPAIHB COMMENTS ON TRIAL LAW & ORDER ACT OF 2010 158<br />
GO THE EXTRA MILE INITIATIVE ___<br />
EXECUTIVE DIRECTOR LETTER 161<br />
GO THE EXTRA MILE FACT SHEET 162<br />
ADDITIONAL ITEMS ___<br />
LEGISLATIVE ACTION ALERT 165
Last Updated: November 12, 2012<br />
Medicare, Medicaid, and <strong>Health</strong> Reform Policy Committee (MMPC)<br />
Face to Face Meeting<br />
Tuesday, November 13, 2012<br />
9:00 AM-5:00 PM EST<br />
Call in number: NIHB conference line: 1-866-303-3137<br />
Passcode: 414526<br />
AGENDA<br />
Purpose: To review and provide updates and detailed discussion of 2012 MMPC Action Plan priorities and assignments.<br />
Outcomes:<br />
1. Continue work on the Affordable Care Act (ACA) and the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act (IHCIA)<br />
health policy issues, regulation review and development of draft positions with the greatest opportunities and<br />
highest priority for the <strong>Indian</strong> health system;<br />
2. Review strategies and process for advancing issues; and identified tasks and timeframes; and,<br />
3. Prepare for TTAG November 14-15, 2012 Face to Face meeting.<br />
9:00 am Welcome<br />
Opening Prayer<br />
Introductions<br />
9:10 am Review of Agenda, Purpose of Meeting and General Housekeeping Items<br />
9:30 am Regulations Review Update (MMPC Action Plan #5) (also see handout)<br />
Review status of proposed comments<br />
Upcoming regulations<br />
10:00 am Prepare for Office of Personal Management (OPM) Guest Speaker-John O’ Brien, Director,<br />
<strong>Health</strong>care & Insurance, OPM (also see handout)<br />
10:10 am John O’Brien OPM (tentative time)<br />
Kaiser Family Foundation/ Barbara Jordan Conference Center<br />
1330 G Street, NW, Washington, DC 20005<br />
Phone: (202) 347-5270; fax: (202) 347-5274<br />
10:50 am Active, New and Ongoing MMPC/TTAG Issues, Status, Goals, and Next Steps<br />
(Review of Current MMPC Action Plan and Strategies)<br />
1. Update on IRS Issues (MMPC Action Plan #9)<br />
a. Assignment of tax refunds<br />
b. Treatment of <strong>Indian</strong> income under MAGI
Last Updated: November 12, 2012<br />
2. Discussion on CCIIO Policy Issues (MMPC Action Plan # 6)<br />
a. Status of internal clearance on <strong>Indian</strong> Addendum and companion piece<br />
b. Timing on response to tribal comments on the Federally-facilitated exchanges.<br />
3. Tribal Hospital EHR Charity Care Calculation (Myra Munson) (MMPC Action Plan #10)<br />
4. Update on VA/IHS Draft Reimbursement Agreement (MMPC Action Plan #11)<br />
5. Single Enrollment Form for Exchanges and Medicaid (MMPC Action Plan #6)<br />
a. Request schedule and process for dealing with open issues, including how CMS is dealing<br />
with process for vetting with other groups<br />
6. Working with States on Exchanges and Medicaid Expansion (MMPC Action Plan #19) (also see<br />
handout)<br />
a. Status of letter to Tribes (development of a template from CMS) for outlining process at state<br />
level for those Tribes not moving forward with Medicaid Expansion (Jim Roberts)<br />
b. Need a process to ensure that Medicaid Expansion is addressed through the ACA Policy<br />
Subcommittee; raise this at the TTAG meeting<br />
c. State Waivers<br />
7. Standard Operating Procedures (SOP) on the CMS Tribal Consultation Policy (MMPC Action Plan<br />
#2)<br />
a. needs to be reviewed by the TTAG Consultation Policy Subcommittee<br />
8. Data Issues (MMPC Action Plan #28)<br />
9. Consultation (MMPC Action Plan #2, 3, 4)<br />
12:00 pm Lunch on Your Own<br />
1:00 pm Continue Discussion of Active, New and Ongoing MMPC/TTAG Issues, Status, Goals, and Next<br />
Steps<br />
1:50 pm Prepare questions to ask Dr. Yvette Roubideaux<br />
2:00 pm Dr. Yvette Roubideaux Q/A<br />
3:00 pm Break<br />
3:15 pm Prepare for TTAG Face to Face<br />
Review TTAG Agenda<br />
Prepare TTAG Talking Points<br />
4:30 pm Additional Discussion Topics<br />
5:00 pm Adjourn MMPC<br />
Upcoming Calls/Meeting dates<br />
Post-Election<br />
Need for more active participation on TTAG subcommittee calls<br />
Decision to dissolve or keep active/reorganize across state borders and behavior health<br />
subcommittees<br />
NIHB GO the EXTRA MILE Initiative<br />
MMPC Teleconference Call-December 5, 2012, 2:00-4:00 PM EST<br />
TTAG Teleconference Call-December 12, 2012, 2:30-4:00 PM EST
Ref.<br />
#<br />
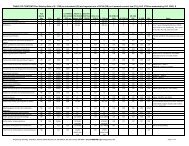
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Please Note: This Summary of issues, assignments and strategies has been organized to follow the<br />
general Goals and Objectives identified in the “draft” 2013-2018 CMS-TTAG AI/AN Strategic Plan.<br />
I. CONSULTATION<br />
Task/Issue Person(s)<br />
1. Invites/Presentation at<br />
MMPC/TTAG November<br />
2012 Face-to-Face<br />
meetings<br />
NIHB<br />
Liz Heintzman<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
Oct 2012 Finalize topics and<br />
speakers for CMS Day;<br />
plenary and workshops<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
MMPC November 2012 Meeting:<br />
1. Invite OPM<br />
2. Review Data Report (request copy from Jim Crouch/Carol Korenbrat)<br />
TTAG October 2012 Meeting – Additional Agenda Items/Topics:<br />
1. Request updates from CCIIO on (1) status of internal clearance on<br />
<strong>Indian</strong> Addendum and companion piece; and (2) timing on response<br />
to tribal comments on the Federally-facilitated exchanges.<br />
2. Request Schedule and Process for dealing with open issues on the<br />
Single Enrollment Form for Exchanges and Medicaid including how<br />
CMS is dealing with process for vetting with other groups.<br />
3. Status of letter to Tribes (development of a template from CMS) for<br />
outlining process at state level for those Tribes not moving forward<br />
with Medicaid Expansion (Jim Roberts)<br />
TTAG November 2012 Meeting:<br />
1. Invite Gary Cohen<br />
2. Invite OIG to report and present on Safe Harbors and Medicaid<br />
Collections<br />
3. Take final action on CMS TTAG Strategic Plan<br />
4. Fuller discussion and update on working with States on Exchanges<br />
and Medicaid Expansion<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 1 of 13 10/9/12
Ref.<br />
#<br />
2.<br />
Task/Issue Person(s)<br />
CMS Consultation<br />
Policy<br />
3. State/Tribal<br />
Consultation<br />
Jim Roberts<br />
Myra Munson<br />
MMPC<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
On-going CMS Policy Finalized<br />
November 2011<br />
MMPC On-going Need to engage with<br />
States and establish<br />
process for Tribal<br />
consultation<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
Final CMS Consultation Policy released November 2011. There are some<br />
substantive differences between the originally approved Tribal Consultation<br />
Workgroup version and the final copies released by CMS. Talking points of these<br />
issues and concerns were drafted for Tribal leaders to use for the all Tribes call<br />
hosted by CMS on Friday, December 9th .<br />
Draft letter has been developed to CMS on behalf of TTAG Co-Chairs regarding<br />
Tribal recommendations on the process & timeline for revising the Consultation<br />
policy. To be finalized by April 10, 2012.<br />
Letter approved by TTAG and forwarded 4/11/12.<br />
Standard Operating Procedures (SOP) being prepared by Kitty on the CMS Tribal<br />
Consultation Policy (needs to be reviewed by the TTAG Consultation Policy<br />
Subcommittee).<br />
1. Monitor SPA’s<br />
2. Tribes engage in planning efforts with States on <strong>Health</strong> Exchanges<br />
3. Engage and monitor State legislative action<br />
4. Medicaid Managed Care – Kansas Tribes’ Strategy.<br />
7/24/12 Update:<br />
13 States are going forward with State Exchanges.<br />
HHS Secretary directed States to work with Tribes.<br />
Only 4 States are actively working with Tribes (OR, RI, WA, and MN)<br />
Only 3 States have formal Tribal consultation policies (OR, RI and WA)<br />
Next Steps/Recommendations:<br />
1. Have a Tribal TTAG Representative participate on monthly CCIIO calls on<br />
State Exchanges.<br />
2. Request updated list of State Exchange contacts.<br />
3. Request CCIIO to report back on which States with establishment grants<br />
have Tribal consultation policies.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 2 of 13 10/9/12
Ref.<br />
#<br />
Task/Issue Person(s)<br />
4. Tribal Consultation<br />
Sessions on Federallyfacilitated<br />
Exchanges<br />
MMPC<br />
Mim Dixon<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
July-August<br />
2012<br />
Action(s) Needed<br />
Discuss strategy, review<br />
talking points, and assign<br />
people to speak to issues<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
4. Have Area <strong>Health</strong> <strong>Board</strong>s reach out to Tribes and assist in communication.<br />
5. 9/5/12 - Need a process to ensure that Medicaid Expansion is<br />
addressed through the ACA Policy Subcommittee; raise this at the<br />
next TTAG meeting in November 2012.<br />
6. Need to develop a letter to Tribes on process of what needs to<br />
happen at State level for those States not moving forward with<br />
Medicaid Expansion; Work with CMS on a template.<br />
HHS held 3 Tribal consultation sessions: July 26 (Washington, DC); August 7<br />
(Anchorage, AK) and August 9 (Denver, CO)<br />
Next Steps:<br />
1. Conference call held 7/31/12. Additional talking points and strategy<br />
developed for presentation at the August 7 & 9 th Consultations. Talking<br />
Points to be circulated.<br />
2. Request CCIIO to share information with Tribes/TTAG that is being<br />
communicated with States.<br />
3. Need clarify from IHS regarding their ability to pay premiums. (This may<br />
require a technical fix.)<br />
4. Comments forwarded on behalf of NIHB and TTAG (Sept 2012).<br />
5. TTAG to request an update from CCIIO on the timing and response to<br />
Tribal recommendations and comments.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 3 of 13 10/9/12
Ref.<br />
#<br />
II. POLICY<br />
Task/Issue Person(s)<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
5. Regulation Review NIHB On-going Identify Regs<br />
Coordinate & Submit<br />
Comments<br />
Track Responses<br />
6. TTAG ACA Policy<br />
Committee<br />
NIHB On-going Conduct weekly<br />
conference calls to<br />
review issues<br />
(Wednesdays 3-5 pm<br />
eastern)<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
NIHB to continue to provide CMS with on-going written Regulation Review and<br />
Update Report on a bi-monthly basis.<br />
Reg. Report, v.2.10 covering the time period through August 15, 2012 was<br />
distributed. NIHB received new cycle of funding end of September 2012. Will<br />
review the process and timeframes for continuing the on-going Reg. Report<br />
on a bi-monthly basis.<br />
10/9/12 - Upcoming Regs and Comments due as follows:<br />
1. CMS #10003 Paperwork Reduction Request (Medicare coverage and<br />
payment in a single form) – Due 11/6/212<br />
2. OPM certification of Qualified <strong>Health</strong> Plans – Due 10/22/12<br />
Current issues include:<br />
1. <strong>Indian</strong> Addendum plus companion piece explaining Addendum.<br />
(completed and forwarded to CCIIO) - TTAG to request an update from<br />
CCIIO on the status of internal clearance..<br />
2. Tribal Sponsorship<br />
3. Other topics will be prioritized as high impact, high value topics.<br />
4. Draft response to Data Elements for application to support eligibility<br />
determinations for enrollment in exchanges, Medicaid and CHIP<br />
5. TTAG to request schedule and process for dealing with open issues<br />
on single enrollment form exchanges and Medicaid (including how<br />
CMS is dealing with process for vetting with other groups.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 4 of 13 10/9/12
Ref.<br />
#<br />
Task/Issue Person(s)<br />
7. Strategy for ACA<br />
Legislative Issues<br />
following Supreme<br />
Court Decision<br />
8. Strategy for moving<br />
forward on determining<br />
eligibility for <strong>Health</strong><br />
Insurance Exchange<br />
Applications (Definition<br />
of <strong>Indian</strong>)<br />
MMPC<br />
Myra Munson<br />
Jennifer Cooper<br />
Elliott Milhollin<br />
MMPC<br />
ACA Policy<br />
Committee<br />
NIHB<br />
NCAI<br />
NCUIH<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
July 2012 Consideration of possible<br />
legislative fixes to ACA<br />
On-going Need to monitor actions<br />
being taken by CMS<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
Following the Supreme Court decision that removed the penalty for States to<br />
courage the Medicated Expansion, there may be a legislative fix and the MMPC<br />
might want to develop a list of other items that would like to be included in any<br />
legislation. The following issues were preliminary identified:<br />
(a) definition of <strong>Indian</strong>; (b) CHSDA for purchasing services; (c) Section 206; (d)<br />
Qualified <strong>Health</strong> Providers; ( e) dental health Section 119; and (f) other<br />
technical corrections.<br />
Next Steps:<br />
1. Create MMPC workgroup to identify areas that need to be fixed and<br />
develop technical corrections.<br />
2. Develop a list of all the issues (Broad brush picture).<br />
3. Fix when there is an opportunity.<br />
TTAG formally submitted recommended questions to be included in the Exchange<br />
applications to determine who is eligible for benefits and protections. This was<br />
narrowed down to 1 question, but no feedback from CMS has been received.<br />
No final rule has been published. There are concerns with waiting for definition and<br />
that it might be narrowly defined. States are currently writing code and it could be<br />
too late to address services for AI/AN.<br />
Need to develop a broader strategy and next steps. (<strong>National</strong> organizations to<br />
take the lead, NIHB, NCAI and NCUIH.)<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 5 of 13 10/9/12
Ref.<br />
#<br />
Task/Issue Person(s)<br />
9. Strategy to engage<br />
CMS & IRS Re: <strong>Health</strong><br />
Exchanges and<br />
Medicaid Expansion<br />
10. Tribal Hospital EHR<br />
Charity Care<br />
Calculation<br />
Mim Dixon<br />
Jim Roberts<br />
Ron Allen<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
On-going Continue to advance<br />
priorities identified by<br />
MMPC<br />
Myra Munson On-going Respond to latest set of<br />
questions from CMS<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
IRS Representatives Jonathan R. Damm & Telly J. Meir, Tax Law Specialists, Office<br />
of <strong>Indian</strong> Tribal Government met with the MMPC representatives at the face-to-face<br />
meeting on 2/21/12; and again on 7/24/12. IRS issued final rule on May 23, 2012.<br />
Many Tribal recommendations were rejected. MMPC inquired on practicial<br />
implementation issues, including:<br />
What is the process for implementation and how will they coordinate<br />
with HHS?<br />
How will they determine who is AI/AN?<br />
How will Tribes be consulted? Tribes want an opportunity to be<br />
consulted before a final decision is made.<br />
IRS reps responded that a complicated flow chart to outline the process has been<br />
developed; and they’re working within the timeframes established in the ACA. They<br />
appreciate the need for on-going communication with Tribes; and IRS follows the<br />
Dept. of Treasury’s consultation policy. They are also informally communicating<br />
with Tribes through outreach in meetings and request for written comments.<br />
Follow up:<br />
1. Invite IRS reps to NIHB Annual Consumer Conference.<br />
2. IRS urged Tribes to continue to communicate in writing on issues of key<br />
concern and Tribal recommendations.<br />
3. Tribes recommended that a TTAG subcommittee be identified to work with<br />
IRS on these issues. (Send follow up email and/or letter with this<br />
recommendation.) Meeting held with Christie Jacobs in Denver<br />
during the ACC meeting.<br />
4. Need to develop an IRS Outreach and Education Plan.<br />
Conference calls are continuing. Technical Workgroup needs to re-write and finalize<br />
response. Myra will finalize prior to the November 2012 TTAG meeting.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 6 of 13 10/9/12
Ref.<br />
#<br />
11.<br />
Task/Issue Person(s)<br />
VA/IHS Draft<br />
Reimbursement<br />
Agreement<br />
13. Coordination with OPM<br />
on Multi-State<br />
Exchange Plans<br />
14. Coordination with OPM<br />
on implementation<br />
issues regarding FEHB<br />
and FEGLI<br />
MMPC<br />
Stacy Bohlen<br />
Elliot Milhollin<br />
NIHB<br />
MMPC<br />
NIHB<br />
NCAI<br />
MMPC<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
On-going Need to Identify next 1. Alaska has finalized and entered into Agreements; some provisions are<br />
steps for Advancing<br />
different than the draft VA/IHS Reimbursement Agreement that was<br />
Agreements between VA circulated for Tribal comment.<br />
& IHS/Tribes<br />
2. VA consultation held during NIHB ACC. The Tribal Self-Governance<br />
Advisory Committee sent a follow up letter regarding comments on<br />
Negotiation of Participating Tribal <strong>Health</strong> Program Agreements with Local<br />
VA Facilities NIHB to send letter similar and to include clarification<br />
regarding rates.<br />
On-going On December 20, 2011, a small group of MMPC members met with OPM, including<br />
Susan McNally, the Assistant Director of <strong>National</strong> <strong>Health</strong>care Operations, John<br />
Cutler, the team leader for the Multi-State Plans Program, Kay Pestura, Deputy<br />
Direct for <strong>National</strong> <strong>Health</strong>care Operations, and Florence Jackson, who works for Ms.<br />
McNally and Ms. Pestura. OPM is not as far along as CCIIO in implementing<br />
Exchange plans, and is in the beginning stages. They are in the pre-consideration<br />
phase of rulemaking, and were unable to provide much in the way of specifics.<br />
MMPC provided an overview of some of the most pressing issues, including<br />
inclusion of ITU providers in any multi-state exchange plan, inclusion of the <strong>Indian</strong><br />
addendum, etc. Ms. McNally indicated that OPM is very interested in hearing from<br />
Tribes on what they would like to see in a multi-state exchange plan.<br />
On-going Continue outreach and The first effective date of coverage began May 1, 2012. Tribes, Tribal organizations<br />
education efforts on and urban <strong>Indian</strong> organizations may also purchase FEHB coverage effective after<br />
FEHB implementation. this date. OPM and NFC are also working with a Tribal Technical Work Group to<br />
finalize operational details related to the program. This Work Group is comprised of<br />
individuals from Tribes, Tribal organizations and urban <strong>Indian</strong> organizations of<br />
various sizes and geographic locations. For more information, please see<br />
www.opm.gov/tribalprograms<br />
1. As of June 2012, OPM reported approximately 30 Tribes covering<br />
approximately 3,000 Tribal employees are now covered. OPM is continuing to<br />
provide training and detailed information regarding the roll-out of the FEHB<br />
program implementation. They are also developing policy handbooks and draft<br />
guidance. Final guidance will be completed when regulations are complete.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 7 of 13 10/9/12
Ref.<br />
#<br />
Task/Issue Person(s)<br />
15. Evaluation of ARRA<br />
5006 Implementation<br />
16.<br />
MMPC Staffing and<br />
Funding<br />
Carmelita Skeeter<br />
MMPC<br />
Stacy Bohlen<br />
Jim Roberts<br />
(Budget<br />
Subcommitte)<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
On-going TTAG to recommend to<br />
CMS to conduct an<br />
evaluation of ARRA 5006<br />
implementation.<br />
On-going Seek both short and longterm<br />
resources to support<br />
MMPC efforts.<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
2. Additional outreach and education with Tribes is needed. OPM plans to release<br />
a Dear Tribal Leader letter in the near future to address some of the questions<br />
and concerns raised during the initial trainings.<br />
3. New guidance for Tribal employers was provided by OPM; identifies what types<br />
of benefit packages have been included.<br />
Recommend state-by-state evaluation; include survey with State Medicaid Directors,<br />
Tribes, Regional <strong>Health</strong> <strong>Board</strong>s and other organizations.<br />
1. Develop and prepare a budget identifying staffing and financial resources<br />
needed, including:<br />
a. Full time regulation review staff (short-term funding identified for<br />
regulation review through September 2012)<br />
b. Dedicated NIHB staff for coordination of MMPC/TTAG activities, including<br />
staffing and facilitation.<br />
2. Encourage IHS to build capacity and resources (IHS benefits from this work)<br />
3. Seek private sector funding:<br />
a. Identify potential foundation funding, e.g. Kellogg, Robert Wood Johnson,<br />
etc. (Stacy)<br />
b. Other outreach<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 8 of 13 10/9/12
Ref.<br />
#<br />
17.<br />
III. LONG-TERM SERVICES AND SUPPORT<br />
Task/Issue Person(s)<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
Long Term Care MMPC On-going Continue to monitor<br />
activities and resources<br />
available under the<br />
ACA/IHCIA.<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
IHS LTC & Behavioral <strong>Health</strong> experts have been meeting regularly.<br />
1. LTC Subcommittee is working with KAI regarding coordination of the upcoming<br />
Long Term Care Support and Services Conference to be held March 21-23 in<br />
Denver.<br />
2. LTC Subcommittee is drafting comments in response to IHS Director, Dr.<br />
Roubideaux’s January 6, 2012 Dear Tribal Leader letter requesting comments<br />
on the recommendations from the previous LTC conference and report. Draft<br />
comments have been shared with the MMPC. Comments were submitted on<br />
March 16, 2012.<br />
3. LTC Subcommittee is planning a conference call with Anita Yuskauskas to<br />
discuss “Money Follows the Person” initiative. Conference call to be<br />
scheduled with the Long-Term Care Committee.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 9 of 13 10/9/12
IV. OUTREACH AND EDUCATION<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Ref.<br />
#<br />
Task/Issue Person(s)<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
18. Outreach and<br />
MMPC On-going Regional Trainings NIHB/NCAI/NCUIH conducted a survey and gathering information for their website.<br />
Education<br />
Targeted groups include (1) tribal governments; (2) tribes as providers; (3) area<br />
health directors; and (4) consumers. It was reported that all information must be<br />
vetted by IHS. Information is currently being developed and area health boards; and<br />
MMPC/TTAG is encouraged to provide their input on these educational materials.<br />
Need TTAG involvement in identification of materials, projects and other<br />
contractual work being developed.<br />
19. Engaging with States<br />
on Planning for <strong>Health</strong><br />
Exchanges (including<br />
those not involved in<br />
planning efforts.)<br />
20.<br />
State Associations<br />
(and other related<br />
Websites)<br />
MMPC<br />
NIHB<br />
MMPC<br />
Tyra Baer<br />
On-going 1. Seek resources for<br />
outreach and<br />
education activities.<br />
2. Establish Planning<br />
Group for<br />
Consultation<br />
On-going Seek funding to provide<br />
for posting of AI/AN<br />
Issues.<br />
1. Recommendations included:<br />
a. Development of Toolkit for Tribal leaders, health providers, and community<br />
beneficiaries.<br />
b. Development of Navigators.<br />
c. Have NIHB develop and complete a list of what is occurring at state level.<br />
d. Request and identify a representative from each state to work with NIHB<br />
on a standard format and process.<br />
e. Post the <strong>Indian</strong> addendum on the R(e)form website.<br />
f. Continue to share what is happening across states. AZ/NM have<br />
established working group which include Tribes.<br />
g. NIHB/NCAI are launching on a new website. Draft materials will be<br />
presented the end of March 2012.<br />
MMPC recommended that funding be sought to provide for AI/AN issues as part of<br />
the State website for <strong>Health</strong> Exchange Planning.<br />
Websites related to MMPC issues on NIHB website on MMPC link:<br />
http://www.nihb.org/<strong>mmpc</strong>/<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 10 of 13 10/9/12
Ref.<br />
#<br />
Task/Issue Person(s)<br />
21. Create TTAG project on<br />
new payment<br />
structures, I/T/U<br />
analysis and outreach<br />
to Tribes<br />
22. Follow up with Office<br />
of Innovation at CCIIO<br />
RE: ACA provisions<br />
that identify IHS<br />
23. Waivers/Exemptions<br />
for AI/AN from<br />
Medicaid Cuts<br />
24. <strong>Indian</strong> Eligibility in<br />
State Basic <strong>Health</strong><br />
Plans<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
MMPC New Issue<br />
July 2012<br />
Action(s) Needed<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
To be discussed and addressed MMPC Face-to-Face Meeting.<br />
MMPC July 2012 CCIIO Office of Innovation participated at the July 25, 2012 TTAG meeting.<br />
Issues to be clarified included:<br />
Jim Roberts<br />
Jim Crouch<br />
On-going Re-convene Benefits<br />
Options Workgroup<br />
MMPC On-going Identify preliminary<br />
comments for MMPC<br />
review<br />
1. What is the plan to put money into <strong>Indian</strong> Country for Projects in the<br />
following three areas:<br />
Tele-health<br />
Behavioral health<br />
Unique Providers<br />
2. Need to ensure there is culturally appropriate evaluation criteria<br />
included in the process.<br />
Share WA State concept paper (NPAIH) and CRIHB’s work with California with the<br />
Workgroup.<br />
Request made to CMS to make available, upon requests by Tribes in States, all<br />
pending waiver requests.<br />
Waivers on posted on CMS website, but the documents are not accessible when<br />
trying to access.<br />
Need to review and determine <strong>Indian</strong> eligibility and how it will be defined in Basic<br />
<strong>Health</strong> Plans.<br />
HHS Secretary sent letter to state insurance commissioners to consult with Tribes<br />
on Medicaid and Exchanges. Need to ensure that states are also consulting with<br />
Tribes on BHPs that address that 133%-200% federal poverty level.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 11 of 13 10/9/12
Ref.<br />
#<br />
Task/Issue Person(s)<br />
25. Medicaid<br />
Administrative Match<br />
(MAM)<br />
26. Update Strategic Plan<br />
27.<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
MMPC On-going Need to develop<br />
advocacy at State-level<br />
Jim Roberts<br />
Mim Dixon<br />
MMPC<br />
Nov 2012 NPAIHB taking lead on<br />
the development of an<br />
updated Plan<br />
Behavioral <strong>Health</strong> Linda Frizzell On-going Continue to monitor<br />
activities and resources<br />
available under the<br />
ACA/IHCIA.<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
More education is needed for Tribal health programs. Need to work with CMS to<br />
provide support for MAM agreements. MMPC recommended:<br />
1. Hold Workshop at NIHB Annual Consumer Conference.<br />
2. Conduct Regional Trainings<br />
3. NIHB Area Association Meeting<br />
1. Status of Draft Plan, and Schedule and Process for Completion (Subcommittee<br />
has met in person and held several teleconferences)<br />
2. Conducted interviews of CMS representatives and identified initiatives for TTAG<br />
to consider.<br />
3. Met with Michael Hash – CCIIO<br />
4. Draft presented at NIHB Annual Consumer Conference in Sept 2012.<br />
5. NIHB shared through their distribution lists, TTAG, MMPC and current<br />
draft is out for 30 day comment. Comments due on October 30, 2012.<br />
6. Final report to be presented for review at the November 2012 TTAG<br />
meeting.<br />
Recommendations:<br />
Integrate Strategic Plan Issues into CMS Operations for easier tracking.<br />
Conduct at least 1 TTAG meeting/annually at CMS Headquarters in<br />
Baltimore.<br />
The various HHS agencies responsible for implementation should assure that the<br />
<strong>Indian</strong> health system and <strong>Indian</strong> people have a fair opportunity to benefit from ALL<br />
behavioral health provisions in the new law.<br />
Most recent work of Subcommittee has revolved around the Essential <strong>Health</strong><br />
Benefits package.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 12 of 13 10/9/12
Ref.<br />
#<br />
V. DATA<br />
Task/Issue Person(s)<br />
28. Data MMPC<br />
Jim Crouch<br />
MMPC: SUMMARY OF ISSUES, STRATEGIES & ASSIGNMENTS<br />
UPDATED 10/9/12<br />
(RECENT UPDATES IN RED AND HIGHLIGHTED IN YELLOW)<br />
Due Date/<br />
Timeline<br />
Action(s) Needed<br />
On-going Review on-going issues<br />
regarding Policy and<br />
Data<br />
Brief Summary of Next Steps and Follow-up<br />
Notes/Comments<br />
TTAG letter was sent to CMS Acting Administrator Marilyn Tavenner on April<br />
10, 2012 summarizing the concerns related to the implementation of the<br />
<strong>National</strong> Data Hubs by CMS and recommendations.<br />
Other recommendations:<br />
1. Form Tribal/CMS Workgroup on Policy and Data Issues (CMS committed to<br />
forming this Workgroup.)<br />
2. Advise CMS Office of Enterprise Management on having appropriate AI/AN<br />
identifiers and making data useful of AI/AN and I/T/U on CMS website being<br />
developed<br />
3. Medicaid data project ended June 30 to expand State data from 400 to 1,000<br />
data elements with no Tribal consultation, but States will be submitting State<br />
Plan Amendments to change their data and this will require Tribal consultation.<br />
We need to prepare Tribes for this consultation and discuss enforcement with<br />
CMS. States in the pilot project with Tribes include: WA, OR, CA, MN, AX, MI,<br />
NM, NC and TX.<br />
4. <strong>Health</strong> Disparities Data on a national basis for AI/AN. The IHS discontinued the<br />
Trends reports in 2007 and the data from the last report is getting too dated to<br />
be reliable.<br />
5. Data report from Jim Crouch/Carol Korenbrot to be reviewed at the MMPC<br />
November 2012 face-to-face meeting.<br />
Need to continue tracking all these items 2-4 listed above.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, MMPC Issues, Strategies & Assignments Page 13 of 13 10/9/12
MMPC October 9, 2012 Teleconference Agenda Notes<br />
Roll Call: Liz Heintzman, Myra Munson, Rhonda Butcher (IHS), Jennifer Cooper, John Stevens, Sam Ennis,<br />
Mim Dixon, Trevelyn Cross, Jay Stiener, Doneg McDonough, Carmealita Skeeter, Phil Norrgard, Jessica<br />
Imotichey, Elliot Milhollin, Jim Roberts, Anthony Yepa, Sherri Varner (IHS), Tammy Clay (IHS), Tom<br />
Gordon, Carol Chicharello, Don Wright, John Rael, Judy Parker, Trevlyn Cross Jim Roberts, Ed Fox, Jessica<br />
Imotichey, Gerald Moses, Dee Sabattus, Diddy Nelson, Valerie Davidson, Doneg McDonough, Sam Ennis,<br />
Myra Munson, D’Shane Barnett, Mim Dixon, John Stephens, and Jim Crouch met with John Dann and<br />
Christie Jacobs from IRS.<br />
Facilitator: Cyndi Ferguson<br />
1. Update on meeting with IRS during the NIHB ACC Conference<br />
Items discussed:<br />
To do List:<br />
-<strong>Indian</strong> definition<br />
-Identify a path to call on Treasury Secretary and HHS Secretary to collaborate together for IHS<br />
essential coverage<br />
-Advanced premium tax credit-can be split between health plan and dental plan?<br />
-MAGI-resource exemptions are consistent with Medicaid’s<br />
-Outreach-what will IRS be doing with the requirements/responsibilities and how related to<br />
<strong>Indian</strong> country<br />
-tribal representatives suggest that IHS database should be used for electronic identification for<br />
coverage-Christi said those discussions are just starting now<br />
-Organize a Tribal meeting during the NCAI Conference to be held in Sacramento later this<br />
month*will report later (Jim Roberts and Ron Allen are setting this up)<br />
-Provide recommendation to have Christi join in on TTAG ACA subcommittee call with Pete from<br />
CCIIO<br />
Questions still to be answered:<br />
What extent can taxpayers assign a refund to someone else (prove the like-hood that tribe could<br />
subsidize into the exchange)? Individual can apply 100% tax credit to purchase insurance in exchange or<br />
use portion?
-Oregon has a provision in the insurance system to make the individual put 100% tax credit into<br />
exchange for tribes to help sponsor payment to the health plan<br />
-Christi said that IRS can’t pose a requirement because that is an Individual right<br />
2. Update on Companion Piece to <strong>Indian</strong> Addendum<br />
To Do List:<br />
-Has been finalized and gone through CCIIO internal review process<br />
-Oregon is making an addendum; and would like to use it if the federal addendum is not as<br />
good; but if it is, want it to be the threshold<br />
-Pete wants to have a meeting with insurance issuers with Tribal representation-<br />
-Need tribal consultation after the review process<br />
3. Update on TTAG Strategic plan:<br />
To Do List:<br />
-new version of the draft for 2013-2017; retained objectives from last one with additional items<br />
TTAG presented at NIHB conference and distributed copies through NIHB distribution lists and<br />
website, and shared with TTAG members of region and area health board; 30 day comment<br />
period with comments due by October 30, 2012.<br />
Plan to be finalized and formally approved by the TTAG during the November face-to-face<br />
meeting.<br />
-Incorporate any changes by November Face to Face TTAG meeting for adoption and<br />
implementation by new election<br />
*send another email to TTAG about commenting on strategic plan for next week<br />
4. Update on Single Enrollment Form for Exchanges/Medicaid, including Tribal Sponsorship<br />
-There is no reference for tribal sponsorship on application itself-no direct tie<br />
-problem in explanatory: core item is wrong that AI/AN can qualify for extra tax credits if they<br />
hold premiums in advance (no mention about cost sharing-got it backwards)<br />
-enrollment form includes categories and subcategories if you are AI/AN<br />
5. Update on Tribal Hospital EHR Charity Care Calculation
To do List:<br />
-Myra will have draft by the 3 rd week; goal to have it done by November face to face meeting<br />
6. Update on CMS/IHS Process for Electronic Verification Process<br />
7. Medicaid expansion and exchange update<br />
-reg. side on expansion-state questions wanting to know if they can go to 100% instead of 133%<br />
-feedback won’t come back until after election<br />
8. Update on VA Reimbursement Agreement Consultation<br />
To Do List:<br />
- Self advisory group sent a letter for Medicare reimbursement that only includes Medicare for<br />
all in exclusive rates because of lower reimbursement rate<br />
-VA said won’t use Medicaid for all in exclusive rates because it is a system issue and would be a<br />
delay in processing Tribal claim; more quick to handle Medicare rates; concerned about error<br />
rates/budget<br />
*NIHB to see a similar letter as the Tribal Self-Governance Advisory Committee and to include<br />
clarification regarding rates<br />
*Myra Munson agreed to circulate the letter sent by Alaska representatives<br />
Regulations Review and Update<br />
RRAR updated through August, 15, 2012; circulated right before ACC<br />
Upcoming Regulations and Comments:<br />
Comment to CMS #10003—paperwork reduction request (Medicare coverage and payment into one<br />
form; could pertain to section 206; need to look at what form means and what it could do for AI/AN,<br />
due on Nov 6 th<br />
OPM comment regarding certification of qualified health plans due October 22<br />
To Do List and Items to Include for Next Meetings:<br />
October 10 th TTAG call:<br />
Request Update from CCIIO on (1) Status of Internal Clearance on <strong>Indian</strong> Addendum and<br />
Companion Piece; and (2) Timing on Response to Tribal Recommendations and Comments on<br />
the Federally-Facilitated Exchanges
-Request Schedule and Process for dealing with open issues on Single Enrollment Form for<br />
Exchanges and Medicaid (including how CMS is dealing with process for vetting with other<br />
groups)<br />
-Status of letter to Tribes (development of CMS Template) for outlining process at state level for<br />
those Tribes not moving forward with Medicaid Expansion-Jim Roberts<br />
TTAG November Face-to Face Meeting<br />
-Invite Gary Cohen<br />
-Invite OIG to report and present on Safe Harbors and Medicaid Collections<br />
-Take final action and approval of Strategic Plan<br />
-Discussion on working with states on exchanges and Medicaid expansion<br />
MMPC November Face-to-Face Meeting:<br />
-Request Data Report from Jim Crouch/Carol Korenbrot and review/discuss findings<br />
-Invite OPM (coordinate with Elliott)
Internal Revenue Service Meeting Notes<br />
Denver, Colorado Meeting<br />
September 25, 2012<br />
Participants: Christie Jacobs, Jonathon Damm, IRS<br />
Jim Roberts, Ed Fox, Jessica Imotochi, Gerald Moses, Dee Sabattus, Diddy Nelson,<br />
Valerie Davidson, Doneg McDonough, Sam Ennis, Myra Munson, D’Shane Barnett, Mim<br />
Dixon, John Stephens, Jim Crouch<br />
1. <strong>Health</strong> Insurance Penalty Exemption Discussion<br />
a. We covered definition issue and strategy to align. IRS not much to do here aligning ACA<br />
with Medicaid. This is HHS.<br />
o IRS seemed agree that the three statutory references to def. of <strong>Indian</strong> under ACA<br />
are the same, including under IRC § 45(A)(c)(6).<br />
o For IRS, their primary concern seemed to be, after comparing the ACA-referenced<br />
definitions to the Medicaid reg., is that non-Federally recognized tribes would be<br />
included under the Medicaid reg., if used.<br />
b. Tax Penalty<br />
o There may be administrative authority by Treasury Secretary and HHS Secretary to<br />
grant IHS coverage as meeting “essential coverage” pursuant to Treasury regulation.<br />
But it will take collaboration and agreement of both Secretaries. Doneg had citation<br />
in Treasury reg....Section 5000(A)(f)(1)????<br />
o This request would apply only to the tax penalty and not eligibility for the APTC.<br />
o TTAG should draft a letter to this effect requesting that Secretaries act on this.<br />
2. Identification of <strong>Indian</strong>s: IHS data base of users<br />
a. It was mentioned to IRS staff that the HIS-maintained database for users is an important<br />
mechanism to more easily identify AI/AN<br />
b. The fact that not all IHS eligibles are captured in the database should not mean that the HIS<br />
database not be used.<br />
c. Christy stated that “discussions are just starting on how this [identification of AI/AN] is going<br />
to work.”<br />
3. MAGI<br />
a. Chart that IRS and CMS are working on this. They have created a chart with the <strong>Indian</strong><br />
exemptions for each of the programs. There are only one or two items that are not on the<br />
IRS exemption list. Aside these, most exempt items for IRS & CMS are the same. If IRS<br />
exempts <strong>Indian</strong> income, it will not collect information about the income that is exempt. The<br />
two items still under discussion are:<br />
i. Education costs and the BIA<br />
ii. Per capita distributions<br />
b. These items are also under discussion with regard to the General Welfare guidance that<br />
Treasury is preparing with regard to Tribes and tribal members.<br />
c. Follow up item: Can we get a copy of the chart?<br />
4. Tribal Sponsorship/APTC items
a. RE: premium subsidies and applying full APTC for purpose of Tribal sponsorship. Up to<br />
individual and IRS may not impose any requirements on how individual uses.<br />
b. When asked whether APTC could be split between a medical plan and a dental plan, Christy<br />
said she didn’t know. Doneg noted that HHS is responsible for issuing guidance re APTC for<br />
pediatric dental plans.<br />
c. Myra asked whether IRS could enter into assignment agreements whereby people who<br />
accept tribal sponsorship for payment of health insurance premiums can have any<br />
underpayment of premium tax credits paid to the sponsoring organization. IRS was not<br />
enthusiastic about the chances of this happening because IRS only uses this for limited<br />
situations and Christy thought the Tribe might not be the right kind of entity to qualify for<br />
assignment of tax refunds.<br />
d. John Stephens asked whether over or under recovery of APTC at the end of the year could<br />
be moved to the following year’s taxes. Christie responded that they couldn’t let it ride to<br />
the next year without interest. John was very effective in making the point that it will only<br />
take one tax bill for one person to end tribal sponsorship. Jim Roberts commented that<br />
Washington State was working with tribes on an aggregator model for tribal sponsorship,<br />
but it may not work due to assignment of tax credits. He asked if IRS was working with<br />
states on this. Christy said IRS isnot working with States.<br />
e.<br />
f. Follow up item: IRS is to send us the section of the tax code that applies to similar<br />
assignment so that Tribal policy wonks can determine if there is some application here that<br />
can be used for Tribal sponsorship.<br />
5. IRS Form 1040<br />
a. Christy indicated that IRS will want to consult with tribes on the question(s) put on Form<br />
1040<br />
b. We mentioned that TTAG submitted recommendations on a “single question” to ask<br />
c. It seems we should resend the old TTAG recommendations to Christy/IRS, or send a revised<br />
recommendation if preferred.<br />
6. IRS Outreach & Education<br />
a. IRS does plan to have special outreach to AI/AN, with an increase in outreach activities in<br />
2013. IRS is tied into the overall O&E campaign of HHS. IRS not in position to conduct<br />
outreach until final rules & decisions are in place.<br />
b. Voluntary tax assistance centers. There are tribal sponsors for these centers now and IRS<br />
expects to use them for ACA.<br />
i. Follow-up Item: How can Tribes become Voluntary Tax Assistance centers if they<br />
are not? Can IHS/Tribal benefits coordinators be trained to provide this assistance?<br />
Non-tribal sites will need special training about tribal benefits and sponsorship; how<br />
will this happen?<br />
c. In IRS all training is now electronic. Christie recognizes the need for face-t0-face, small<br />
group training for Tribes, but she says that the IRS needs to hear this from Tribes.<br />
d. Follow-up item: Tribes should send letter to IRS Commissioner and Sec of Treasury with cc<br />
to Christy.<br />
e. Christie recommended that we stay in touch with her about such issues as they become<br />
more clear in the coming months.<br />
f. Who do we direct our advocacy to? Normally the Deputy Secretary is responsible for Tribal<br />
issues however position is vacant (Aaron Kline left, but someone else checks in mailbox)
with a “interim/acting”. Can always direct information to IRS Commissioner, with copy to<br />
Christie Jacobs.<br />
g. John Stephens asked whether a person had to file taxes previously in order to apply for<br />
APTC through the Exchange. Christy said she didn’t know the answer to that question.<br />
7. Recommendation to form IRS-Tribal Workgroup<br />
a. The Department of Treasury Tribal Consultation Policy is on their website on a Tribal page.<br />
The Department of Treasury does not seem willing to have IRS Advisory Groups.<br />
b. Christie will check with Pete Nakata to see if they can combine this effort. She didn’t seem<br />
willing to do something different than the ACA Policy Subcommittee meetings that we have<br />
with CCIIO. Christie preferred to site in on the CCIIO meetings and use that venue if she<br />
needs to engage on Tribal issues. She will get back to us.
I. Purpose.<br />
DRAFT EXPLANATION OF ADDENDUM<br />
FOR INDIAN HEALTH CARE PROVIDERS TO NETWORK PROVIDER<br />
AGREEMENTS OF HEALTH PLANS OFFERING PRODUCTS ON<br />
HEALTH INSURANCE EXCHANGES<br />
CMS has developed the attached Addendum for <strong>Indian</strong> <strong>Health</strong> Care Providers to promote<br />
inclusion of <strong>Indian</strong> health care providers in qualified health plan (QHP) provider networks and<br />
help health insurance issuers develop health plans that comply with the QHP certification<br />
standards set forth in 45 CFR Part 156. Based upon a similar standardized contract addendum<br />
used in the Medicare Part D program, this addendum has been developed for QHP issuers to use<br />
when contracting with <strong>Indian</strong> <strong>Health</strong> Care Providers.<br />
The federal government has a historic and unique relationship with American <strong>Indian</strong> and Alaska<br />
Native (AI/AN) tribes. The purpose of this addendum is to further the aims of the Federal trust<br />
responsibility by fostering participation of <strong>Indian</strong> health care providers in QHP networks, and<br />
help issuers meet QHP certification standards, particularly with respect to network adequacy and<br />
access to essential community provider participation. In adhering to QHP certification standards,<br />
QHP issuers will need to reach out to <strong>Indian</strong> health care providers in many parts of the country.<br />
It is anticipated that the addendum will assist health plans meet the “sufficient number and type<br />
of provider” criterion required for QHP certification, and will facilitate acceptance of network<br />
contracts by <strong>Indian</strong> health providers.<br />
Most AI/AN people access care through their longstanding providers in the <strong>Indian</strong> health system.<br />
As a result, an important consideration in evaluating network adequacy and essential community<br />
provider accessibility will be the extent to which a QHP includes <strong>Indian</strong> providers in their<br />
networks and whether it can assure that services to AI/AN consumers will be accessible without<br />
unreasonable delay.<br />
Offering contracts that include the Addendum will provide QHPs with an efficient and effective<br />
way to establish network contract relationships with <strong>Indian</strong> Providers, and also ensure that<br />
American <strong>Indian</strong> and Alaska Native consumers can continue to be served by their <strong>Indian</strong><br />
provider of choice. <strong>Indian</strong> tribes are entitled to special protections and provisions under Federal<br />
laws, which are described further in Section II.<br />
The addendum identifies specific provisions that have been established in Federal<br />
law that apply when contracting with <strong>Indian</strong> <strong>Health</strong> Care Providers (i.e. I/T/Us). Use of this<br />
Addendum benefits both QHPs and the <strong>Indian</strong> Providers by lowering the perceived barriers to<br />
contracting, assuring QHP issuers comply with key Federal laws that apply when contracting<br />
with <strong>Indian</strong> providers, and minimizing potential disputes. AI/ANs consumers will be better<br />
served if their QHP encourages <strong>Indian</strong> providers to coordinate their care through the QHP<br />
network.<br />
8/7/12 DRAFT COMPANION TO ADDENDUM – PAGE 1
8/7/12 DRAFT COMPANION TO ADDENDUM – PAGE 2
II. Explanation of the Addendum for <strong>Indian</strong> <strong>Health</strong> Care Providers<br />
1. Purpose of Addendum<br />
Building on the success achieved in the Medicare Part D program, this Addendum for <strong>Indian</strong><br />
<strong>Health</strong> Care Providers has been developed for use in Exchange’s Qualified <strong>Health</strong> Plan<br />
network contracts with <strong>Indian</strong> <strong>Health</strong> Care Providers. .<br />
2. Definitions.<br />
The definitions of terms used in the Addendum relate to federal laws.<br />
3. Description of <strong>Health</strong> Care Provider.<br />
This addendum can be used with different types of <strong>Indian</strong> health providers. This section gives<br />
the opportunity to check the provider type that applies to the specific organization or facility<br />
which is covered by the contract or agreement.<br />
4. Cost-Sharing Exemption for <strong>Indian</strong>s; No Reduction in payments.<br />
Section 1402(d)(2) of the ACA provides that QHPs may not impose any cost-sharing on AI/AN<br />
plan enrollees and may not reduce payments to an <strong>Indian</strong> <strong>Health</strong> Care Provider or contract health<br />
services provider that would otherwise be due. The ACA directs the Secretary of HHS to<br />
reimburse issuers for the increase in the actuarial value of the plan due to these costs.<br />
5. Persons eligible for items and services from <strong>Indian</strong> <strong>Health</strong> Care Provider.<br />
This section of the Addendum protects the QHP from charges of discrimination if the I/T/U<br />
provider sees only people who are eligible IHS beneficiaries. <strong>Indian</strong> health programs are<br />
generally not open to the public; they are established to serve AI/ANs, as provided in the IHCIA.<br />
The applicable eligibility rules are generally set out in IHS regulations at 42 C.F.R. Part 136.<br />
IHCIA §813 (25 U.S.C. §1680c) sets out the circumstances under which certain non-AI/ANs<br />
connected with an AI/AN (such as minor children or a spouse) can receive services as<br />
beneficiaries. IHCIA § 813 also authorizes services to certain other non-AI/ANs if carefully<br />
defined requirements are satisfied.<br />
6. Applicability of other Federal laws.<br />
This section identifies a number of Federal laws that apply variously to IHS, Tribal health<br />
programs, and urban <strong>Indian</strong> programs. These laws are briefly described here.<br />
Anti-Deficiency Act, 31 U.S.C. §1341. This law applies to the <strong>Indian</strong> <strong>Health</strong> Service as a<br />
Federal agency. It prohibits agency personnel from obligating the expenditure of Federal<br />
funds in excess of appropriations made by Congress.<br />
8/7/12 DRAFT COMPANION TO ADDENDUM – PAGE 3<br />
Comment [A1]: Something to consider – in the<br />
interest of brevity, should we just include a<br />
description of selected provisions which require<br />
clarification?<br />
RESPONSE – If a summary of only certain<br />
provisions is to be included, then perhaps only the<br />
provisions listed in Section 6 could be included.
<strong>Indian</strong> Self-Determination and Education Assistance Act (ISDEAA), 25 U.S.C. §450 et<br />
seq. This law directs the Secretary of HHS, at the request of an <strong>Indian</strong> tribe, to enter into<br />
a contract or compact with a tribe, a tribal organization, or an inte- tribal consortium to<br />
operate Federal health programs for <strong>Indian</strong>s with the funds the <strong>Indian</strong> <strong>Health</strong> Service<br />
would have otherwise used to carry out the program directly. It is through this law that<br />
many <strong>Indian</strong> tribes and tribal organizations have taken over direct operation of health<br />
programs from IHS.<br />
Federal Tort Claims Act (FTCA), 28 U.S.C. §§2671-2680. This law waives the United<br />
States’ sovereign immunity from suit with regard to the torts enumerated in the FTCA,<br />
and is the exclusive remedy for suits against Federal agencies such as the <strong>Indian</strong> <strong>Health</strong><br />
Service. Congress extended the FTCA to cover <strong>Indian</strong> tribes and tribal organizations<br />
operating Federal programs pursuant to contracts or compacts under the ISDEAA. 25<br />
U.S.C. §450f note. Urban <strong>Indian</strong> organization health providers who acquire FQHC status<br />
under Sec. 224 of the Public <strong>Health</strong> Service Act can acquire FTCA coverage pursuant to<br />
the Federally Supported <strong>Health</strong> Centers Assistance Act. Since a claim under the FTCA is<br />
the exclusive remedy for actions against <strong>Indian</strong> health care providers that are covered by<br />
the FTCA, those entities are not required to obtain professional liability insurance.<br />
Federal Medical Care Recovery Act (FMCRA), 42 U.S.C. §§2651-2653. This law<br />
authorizes Federal agencies, including the <strong>Indian</strong> <strong>Health</strong> Service, to recover from a<br />
tortfeasor (or an insurer of a tortfeasor) the reasonable value of health services furnished<br />
to a tortfeasor’s victim. The right of recovery under the FMCRA extends to <strong>Indian</strong> tribes<br />
and tribal organizations operating ISDEAA contracts and compacts. 25 U.S.C.<br />
§1621e(e)(3).<br />
Federal Privacy Act, 5 U.S.C. §552a and regulations at 45 C.F.R. Part 5b. This law and<br />
its regulations apply to the IHS, and to <strong>Indian</strong> tribes, tribal organizations and urban <strong>Indian</strong><br />
organizations that operate Federally-funded health care programs. The Privacy Act<br />
governs the use and disclosure of personally identifiable information about individuals<br />
that is maintained in a federal records system.<br />
Confidentiality of Alcohol and Drug Abuse Patient Records, 42 C.F.R. Part 2. These<br />
regulations restrict disclosure and use of drug abuse patient records that are maintained in<br />
connection with the performance of any federally assisted alcohol or drug abuse program.<br />
The restrictions would apply to any such records maintained by the IHS, an <strong>Indian</strong> tribe,<br />
tribal organization or urban <strong>Indian</strong> organization.<br />
<strong>Health</strong> Insurance Portability and Accountability Act (HIPAA) regulations at 45 C.F.R.<br />
Parts 160 and 164. These regulations restrict access to and disclosure of protected health<br />
information maintained by the IHS, <strong>Indian</strong> tribes, tribal organizations and urban <strong>Indian</strong><br />
organizations.<br />
<strong>Indian</strong> <strong>Health</strong> Care Improvement Act (IHCIA), 25 U.S.C. §1601 et seq. This law supplies<br />
the comprehensive statutory framework for the delivery of health care services to <strong>Indian</strong><br />
people. It applies to all <strong>Indian</strong> health providers – the IHS; <strong>Indian</strong> tribes and tribal<br />
organizations operating ISDEAA contracts and compacts from the Secretary of HHS; and<br />
8/7/12 DRAFT COMPANION TO ADDENDUM – PAGE 4
urban <strong>Indian</strong> organizations that receive grants from IHS under Title V of the IHCIA.<br />
Specific provisions of the IHCIA that would impact contracts between <strong>Indian</strong> health care<br />
providers and QHPs are cited in various provisions of the Addendum.<br />
7. Non-taxable entity.<br />
Because of provisions in federal law, QHPs may not require <strong>Indian</strong> <strong>Health</strong> Care Providers to<br />
collect or remit any federal, state or local taxes.<br />
8. Insurance and indemnification.<br />
The IHS, Tribes and Tribal Organizations and Urban <strong>Indian</strong> Organizations that qualify are<br />
covered by the FTCA. Since a claim under the FTCA is the exclusive remedy for actions against<br />
<strong>Indian</strong> health care providers that are covered by the FTCA, those entities are not required to<br />
obtain professional liability insurance.<br />
9. Licensure of <strong>Health</strong> Care Professionals.<br />
This section safeguards a QHP from state licensing requirements for health care<br />
professionals with respect to <strong>Indian</strong> providers. IHCIA §221 (25 U.S.C. §1621t) permits an<br />
<strong>Indian</strong> tribe or tribal organization to employ a health care professional who is subject to licensure<br />
if that individual is licensed in any state. Employees of the IHS obtain their “licensed in any<br />
state” status through other Federal law.<br />
10. Licensure of Provider, eligibility for payments.<br />
This provision waives QHP requirements for State licensing of facilities. IHCIA §408 (25<br />
U.S.C. §1647a) deems a health program operated by the IHS, an <strong>Indian</strong> tribe, tribal organization<br />
or urban <strong>Indian</strong> organization to be licensed under state or local law if it meets all requirements<br />
for such license regardless of whether it obtains such a license.<br />
11. Dispute Resolution.<br />
This provision provides that the <strong>Indian</strong> <strong>Health</strong> Care Providers agree to meet and confer to resolve<br />
any dispute in good faith, and that any disputes that cannot be resolved in good faith will be<br />
subject to the laws of the United States . The IHS and Tribes are generally not subject to State<br />
laws, and may only be subject to binding arbitration if specifically authorized by law.<br />
12. Governing Law.<br />
Tribes are generally subject to Federal law. This provision states that the QHP agreement and<br />
the addendum shall be governed by Federal law., and that nothing in the agreement shall subject<br />
an <strong>Indian</strong> tribe, tribal organization, or urban <strong>Indian</strong> organization to State law to any greater<br />
extent than State law is already applicable.<br />
13. Medical Quality Assurance Requirements.<br />
8/7/12 DRAFT COMPANION TO ADDENDUM – PAGE 5<br />
Comment [A2]: Because of…..<br />
Comment [A3]: Because of…..(federal law?)
Under federal law, There are privacy rules governing quality assurance for the I/T/U that must<br />
be considered as requirements are imposed by the QHP. IHCIA §805 (25 U.S.C. §1675)<br />
facilitates internal medical program quality reviews; shields participants in those reviews; and<br />
restricts disclosure of medical quality assurance records. This provision applies to the IHS,<br />
<strong>Indian</strong> tribes, tribal organizations and urban <strong>Indian</strong> organizations.<br />
14. Claims Format.<br />
An I/T/U may use a claims format offered by the QHP, or it may submit claims in a format that<br />
is consistent with Medicare claims. IHCIA §206(h) (25 U.S.C. §1621e(h) prohibits insurance<br />
carriers from denying a claim submitted by IHS, an <strong>Indian</strong> tribe or tribal organization based on<br />
the format on which the claim is submitted if the format complies with the Medicare claims<br />
format requirements.<br />
15. Payment Rate.<br />
IHCIA §206(a) and (i) (25 U.S.C. §1621e(a) and (i)) provides that the IHS, an <strong>Indian</strong> tribe, tribal<br />
organization and urban <strong>Indian</strong> organization have the right to recover the reasonable charges<br />
billed, or, if higher, the highest amount an insurance carrier would pay to other providers. This<br />
Addendum provision states that a QHP must pay claims to the I/T/U according to IHCIA Section<br />
206 except to the extent the <strong>Indian</strong> <strong>Health</strong> Care Provider expressly agrees in writing to accept rates or<br />
amounts specified in [specify payment schedule here] as payment in full, except that such rates or<br />
amounts may not be lower than the Qualified <strong>Health</strong> Plan pays to any of its other preferred or in-network<br />
providers .<br />
16. Hours and Days of Service.<br />
QHP may not require the I/T/U to provide services at times they would not otherwise provide<br />
services for the IHS beneficiaries. For example, some I/T/U clinics are open only a few days a<br />
week and some do not provide 24-call.<br />
17. Sovereign Immunity.<br />
Becasuse tribes are soverign governments, This provision provides that nothing in the agreement<br />
shall constitute a waiver of federal or tribal sovereign immunity from suit.<br />
18. Endorsement.<br />
IHS providers and employees are prohibited from officially endorsing any non-federal entity.<br />
This provision ensures that no such endorsement is implied by signing the agreement.<br />
8/7/12 DRAFT COMPANION TO ADDENDUM – PAGE 6<br />
Comment [A4]: State the basis. Can we hook to<br />
some federal provision?
Appendix A. I/T/U Programs in Each State<br />
8/7/12 DRAFT COMPANION TO ADDENDUM – PAGE 7
1. Purpose of Addendum; Supersession.<br />
DRAFT<br />
Addendum for <strong>Indian</strong> <strong>Health</strong> Care Providers<br />
The purpose of this Addendum for <strong>Indian</strong> <strong>Health</strong> Care Providers is to apply special terms and conditions<br />
necessitated by Federal law and regulations to the agreement by and between ______________________<br />
(herein "Qualified <strong>Health</strong> Plan") and ___________________________ (herein "<strong>Indian</strong> <strong>Health</strong> Care<br />
Provider"). To the extent that any provision of the Qualified <strong>Health</strong> Plan's network provider agreement or<br />
any other addendum thereto is inconsistent with any provision of this Addendum for <strong>Indian</strong> <strong>Health</strong> Care<br />
Providers, the provisions of this Addendum for <strong>Indian</strong> <strong>Health</strong> Care Providers shall supersede all such<br />
other provisions.<br />
2. Definitions. (NOTE: NEED TO CHANGE THE ORDER TO BE ALPHABETICAL)<br />
For purposes of the Qualified <strong>Health</strong> Plan's agreement, any other addendum thereto, and this Addendum<br />
for <strong>Indian</strong> <strong>Health</strong> Care Providers, the following terms and definitions shall apply:<br />
(a) "Qualified <strong>Health</strong> Plan" has the meaning given in Sec. 1301 of the Patient Protection and Affordable<br />
Care Act (ACA), 42 U.S.C. §18021.<br />
(b) <strong>Indian</strong> <strong>Health</strong> Care Provider" means a health program administered by the <strong>Indian</strong> <strong>Health</strong> Service<br />
(IHS), a tribal health program, an <strong>Indian</strong> tribe or tribal organization to which funding is provided<br />
pursuant to section 23 of the Act of June 25, 1910 (25 U.S.C. § 47(commonly known as the “Buy<br />
<strong>Indian</strong> Act”)) or an urban <strong>Indian</strong> organization that receives funding from the IHS pursuant to Title V<br />
of the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act, Pub. L. 94-437, as amended (IHCIA).<br />
(c) "<strong>Indian</strong> <strong>Health</strong> Service" means the agency of that name within the U.S. Department of <strong>Health</strong> and<br />
Human Services established by IHCIA Sec. 601, 25 USC §1661.<br />
(d) "<strong>Indian</strong> tribe" has the meaning given in IHCIA Sec. 4(14), 25 USC § 1603(14).<br />
(e) The term "tribal organization" has the meaning given in IHCIA Sec. 4(26), 25 USC §1603(26).<br />
(f) "Urban <strong>Indian</strong> organization" has the meaning given in IHCIA Sec. 4(29), 25 USC §1603(29).<br />
(g) The term "<strong>Indian</strong>," has the meaning given in 45 C.F.R. 155.300(a).<br />
(h) The term "contract health services" has the meaning given in IHCIA Sec. 4(5), 25 U.S.C. §1603(5).<br />
(i) The term “Tribal health program” has the meaning given in IHCIA Sec. 4(25), 25 U.S.C. § 1603(25).<br />
3. Description of <strong>Indian</strong> <strong>Health</strong> Care Provider.<br />
The Provider identified in Section 1 of this Addendum for <strong>Indian</strong> <strong>Health</strong> Care Providers is (check<br />
appropriate box):<br />
/_/ The <strong>Indian</strong> <strong>Health</strong> Service (IHS).<br />
/_/ An <strong>Indian</strong> tribe that operates a health program under a contract or compact to carry out programs of<br />
the IHS pursuant to the <strong>Indian</strong> Self-Determination and Education Assistance Act (ISDEAA), 25 USC<br />
§450 et seq.<br />
/_/ A tribal organization that operates a health program under a contract or compact to carry out programs<br />
of the IHS pursuant to the ISDEAA, 25 USC §450 et seq.<br />
/_/ A tribe or tribal organization that operates a health program with funding provided in whole or part<br />
pursuant to section 23 of the Act of June 25, 1910 (25 U.S.C. § 47 (commonly known as the Buy<br />
8/7/12 DRAFT Addendum – Page 1<br />
Comment [A1]: While the QHP issuer might also<br />
be an MCO, the QHP is a commercial health<br />
insurance product that is not governed by medicaid<br />
requirements. The Medicaid definition is not<br />
applicable in this context.
<strong>Indian</strong> Act), or urban <strong>Indian</strong> organization that receives funding from the IHS pursuant to Title V of<br />
the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act, Pub. L. 94-437, as amended (IHCIA)<br />
/_/ An urban <strong>Indian</strong> organization that operates a health program with funds in whole or part provided by<br />
IHS under a grant or contract awarded pursuant to Title V of the IHCIA.<br />
4. Cost-Sharing Exemption for <strong>Indian</strong>s; No Reduction in Payments.<br />
If an <strong>Indian</strong> enrolled in a qualified health plan is furnished an item or service directly by the <strong>Indian</strong> <strong>Health</strong><br />
Service, an <strong>Indian</strong> Tribe, Tribal Organization, or Urban <strong>Indian</strong> Organization or through referral under<br />
contract health services –<br />
(a) No cost-sharing under the plan shall be imposed under the plan for such item or service; and<br />
(b) The issuer of the plan shall not reduce the payment to any such entity for such item or service by<br />
the amount of any cost-sharing that would be due from the <strong>Indian</strong> but for subparagraph (a). .<br />
ACA §1402(d) (2) (42 USC 18071(d)(2)).<br />
5. Persons eligible for items and services from <strong>Indian</strong> <strong>Health</strong> Care Provider.<br />
(a) The parties agree that the IHS is limited to serving eligible IHS beneficiaries, except under limited<br />
circumstances pursuant to 42 CFR Part 136 and IHCIA Sec. 813, 25 USC §1680c.<br />
(b) The parties agree that the <strong>Indian</strong> <strong>Health</strong> Care Provider that is an <strong>Indian</strong> tribe, a tribal organization, or<br />
an urban <strong>Indian</strong> organization has the authority to limit its service population in accordance with the<br />
following authorities:<br />
(1) Sec. 813 of the IHCIA, 25 USC §1680c;<br />
(2) 42 CFR Part 136; and<br />
(3) The terms of the ISDEAA contract or compact or IHCIA grant or contract, as<br />
applicable.<br />
(c) No term or condition of the Qualified <strong>Health</strong> Plan's agreement or any addendum thereto shall be<br />
construed to change, reduce, expand or alter the eligibility of persons for services of the <strong>Indian</strong> <strong>Health</strong><br />
Care Provider that is inconsistent with the authorities identified in subsection (a) or (b).<br />
6. Applicability of Other Federal laws.<br />
Federal laws and regulations affecting an <strong>Indian</strong> <strong>Health</strong> Care Provider, include but are not limited to the<br />
following:<br />
(a) The IHS as an <strong>Indian</strong> <strong>Health</strong> Care Provider:<br />
(1) Anti-Deficiency Act 31 U.S.C. §1341;<br />
(2) <strong>Indian</strong> Self Determination and Education Assistance Act (ISDEAA) ; 25 USC §450 et seq.;<br />
(3) Federal Tort Claims Act (“FTCA”), 28 U.S.C. §§2671-2680;<br />
(4) Federal Medical Care Recovery Act, 42 U.S.C. §§2651-2653;<br />
(5) Federal Privacy Act of 1974 (“Privacy Act”), 5 U.S.C. §552a, 45 CFR Part 5b;<br />
(6) Confidentiality of Alcohol and Drug Abuse Patient Records, 42 C.F.R. Part 2;<br />
(7) <strong>Health</strong> Insurance Portability and Accountability Act of 1996 ("HIPAA"), 45C.F.R. Parts 160<br />
and 164; and<br />
(8) IHCIA, 25 U.S.C. §1601 et seq.<br />
(b) An <strong>Indian</strong> tribe or a tribal organization that is an <strong>Indian</strong> <strong>Health</strong> Care Provider:<br />
8/7/12 DRAFT Addendum – Page 2
(1) ISDEAA, 25 USC §450 et seq.;<br />
(2) IHCIA, 25 USC §1601, et seq.;<br />
(3) FTCA, 28 USC §§2671-2680;<br />
(4) HIPAA, and regulations at 45 CFR parts 160 and 164.<br />
(c) An urban <strong>Indian</strong> organization that is an <strong>Indian</strong> <strong>Health</strong> Care Provider:<br />
(1) IHCIA, 25 USC §1601, et seq.;<br />
(2) Privacy Act, 5 USC §552a and regulations at 45 CFR Part 5b; and<br />
(3) HIPAA, and regulations at 45 CFR parts 160 and 164.<br />
7. Non-taxable entity.<br />
To the extent an <strong>Indian</strong> <strong>Health</strong> Care Provider is a non-taxable entity, such Provider shall not be required<br />
by a Qualified <strong>Health</strong> Plan to collect or remit any Federal, State, or local tax.<br />
8. Insurance and indemnification.<br />
(a) <strong>Indian</strong> <strong>Health</strong> Service. The <strong>Indian</strong> <strong>Health</strong> Service is covered by the Federal Tort Claims Act (FTCA)<br />
which obviates the requirement that IHS carry private malpractice insurance as the United States<br />
consents to be sued in place of federal employees for any damages to property or for personal injury<br />
or death caused by the negligence or wrongful act or omission of federal employees acting within the<br />
scope of their employment. 28 U.S.C. §2671-2680. Nothing in the Qualified <strong>Health</strong> Plan's agreement<br />
shall be interpreted to authorize or obligate any IHS employee to perform any act outside the scope of<br />
his/her employment. The IHS shall not be required to acquire insurance, provide indemnification, or<br />
guarantee that the Qualified <strong>Health</strong> Plan will be held harmless from liability.<br />
(b) <strong>Indian</strong> Tribes and Tribal Organizations. An <strong>Indian</strong> <strong>Health</strong> Care Provider which is an <strong>Indian</strong> tribe or a<br />
tribal organization shall not be required to obtain or maintain professional liability insurance to the<br />
extent such Provider is covered by the Federal Tort Claims Act (FTCA) pursuant to Federal law<br />
(Pub.L. 101-512, Title III, §314, as amended by Pub.L. 103-138, Title III, §308 (codified at 25 USC<br />
§450f note); and regulations at 25 CFR Part 900, Subpt. M. Nothing in the Qualified <strong>Health</strong> Plan's<br />
agreement or any addendum thereto shall be interpreted to authorize or obligate such Provider or any<br />
employee of such Provider to operate outside of the scope of employment of such employee. Such<br />
Provider shall not be required to acquire insurance, provide indemnification, or guarantee that the<br />
Qualified <strong>Health</strong> Plan will be held harmless from liability.<br />
(c) Urban <strong>Indian</strong> Organizations. To the extent an <strong>Indian</strong> <strong>Health</strong> Care Provider that is an urban <strong>Indian</strong><br />
organization is covered by the FTCA pursuant to section 224(g)-(n) of the Public <strong>Health</strong> Service Act,<br />
as amended by the Federally Supported <strong>Health</strong> Centers Assistance Act, Pub.L. 104-73, (codified at 42<br />
USC §233(g)-(n)) and regulations at 42 CFR Part 6, such Provider shall not be required to obtain or<br />
maintain professional liability insurance. Nothing in the Qualified <strong>Health</strong> Plan's agreement or any<br />
addendum thereto shall be interpreted to authorize or obligate such Provider or any employee of such<br />
Provider to operate outside of the scope of employment of such employee. Such Provider shall not be<br />
required to acquire insurance, provide indemnification, or guarantee that the Qualified <strong>Health</strong> Plan<br />
will be held harmless from liability.<br />
9. Licensure of <strong>Health</strong> Care Professionals.<br />
(a) <strong>Indian</strong> <strong>Health</strong> Service. States may not regulate the activities of IHS-operated health care programs nor<br />
require that IHS health care professionals be licensed in the State where they are providing services,<br />
8/7/12 DRAFT Addendum – Page 3
whether the IHS employee is working at an IHS-operated facility or has been assigned to a health care<br />
program of a tribe, tribal organization or urban <strong>Indian</strong> organization. The parties agree that during the<br />
term of the Qualified <strong>Health</strong> Plan's agreement, IHS health care professionals shall hold state licenses<br />
in accordance with applicable federal law, and that IHS facilities shall be accredited in accordance<br />
with federal statutes and regulations.<br />
(b) <strong>Indian</strong> tribes and tribal organizations. Sec. 221 of the IHCIA (25 U.S.C. §1621t) exempts a health<br />
care professional employed by an <strong>Indian</strong> tribe or tribal organization from the licensing requirements<br />
of the state in which such tribe or organization performs services, provided the health care<br />
professional is licensed in any state. Sec. 408 of the IHCIA (25 U.S.C. § 1647a) provides that a<br />
health program operated by an <strong>Indian</strong> tribe or tribal organization shall be deemed to have met a<br />
requirement for a license under state or local law if such program meets all the applicable standards<br />
for such licensure, regardless of whether the entity obtains a license or other documentation under<br />
such state or local law. The parties agree that these federal laws apply to the Qualified <strong>Health</strong> Plan's<br />
agreement and any addenda thereto.<br />
(c) Urban <strong>Indian</strong> organizations. To the extent that any health care professional of an urban <strong>Indian</strong><br />
Provider is exempt from State regulation, such professional shall be deemed qualified to perform<br />
services under the Qualified <strong>Health</strong> Plan Sponsor's agreement and all addenda thereto, provided such<br />
employee is licensed to practice in any State. Sec. 408 of the IHCIA (25 U.S.C. § 1647a) provides<br />
that a health program operated by an urban <strong>Indian</strong> organization shall be deemed to have met a<br />
requirement for a license under state or local law if such program meets all the applicable standards<br />
for such licensure, regardless of whether the entity obtains a license or other documentation under<br />
such state or local law.<br />
10. Licensure of Provider; eligibility for payments.<br />
To the extent that the <strong>Indian</strong> <strong>Health</strong> Care Provider is exempt from State licensing requirements, such<br />
Provider shall not be required to hold a State license to receive any payments under the Qualified <strong>Health</strong><br />
Plan's agreement and any addendum thereto.<br />
11. Dispute Resolution.<br />
In the event of any dispute arising under the Qualified <strong>Health</strong> Plan's agreement or any addendum thereto,<br />
the parties agree to meet and confer in good faith to resolve any such disputes. The laws of the United<br />
States shall apply to any problem or dispute hereunder that cannot be resolved by and between the parties<br />
in good faith. Notwithstanding any provision in the Qualified <strong>Health</strong> Plan's agreement or any addendum<br />
thereto to the contrary, the <strong>Indian</strong> <strong>Health</strong> Care Provider shall not be required to submit any disputes<br />
between the parties to binding arbitration.<br />
12. Governing Law.<br />
The Qualified <strong>Health</strong> Plan's agreement and all addenda thereto shall be governed and construed in<br />
accordance with Federal law of the United States. In the event of a conflict between such agreement and<br />
all addenda thereto and Federal law, Federal law shall prevail. Nothing in the Qualified <strong>Health</strong> Plan's<br />
agreement or any addendum thereto shall subject an <strong>Indian</strong> tribe, tribal organization, or urban <strong>Indian</strong><br />
organization to State law to any greater extent than State law is already applicable.<br />
8/7/12 DRAFT Addendum – Page 4
13. Medical Quality Assurance Requirements.<br />
To the extent the Qualified <strong>Health</strong> Plan imposes any medical quality assurance requirements on its<br />
network providers, any such requirements applicable to <strong>Indian</strong> <strong>Health</strong> Care Providers shall be subject to<br />
Sec. 805 of the IHCIA (25 U.S.C. §1675).<br />
14. Claims Format.<br />
Pursuant to Sec. 206(h) of the IHCIA (25 USC §1621e(h)), the Qualified <strong>Health</strong> Plan may not deny a<br />
claim submitted by the <strong>Indian</strong> <strong>Health</strong> Care Provider based on the format in which submitted if the format<br />
used complies with that required for submission of claims under Title XVIII of the Social Security Act or<br />
recognized under section 1175 of such Act.<br />
15. Payment of Claims.<br />
The Qualified <strong>Health</strong> Plan shall pay claims from the <strong>Indian</strong> <strong>Health</strong> Care Provider in accord with Federal<br />
law, including Sec. 206 of the IHCIA (25 U.S.C. §1621e), and Sec. 1402(d)(2)(B) of the ACA (42 U.S.C.<br />
§18071(d)(2)(B)), except to the extent the <strong>Indian</strong> <strong>Health</strong> Care Provider expressly agrees in writing to the<br />
rates or amounts specified in [specify payment schedule here] as payment in full, provided that such rates<br />
or amounts shall not be lower than the Qualified <strong>Health</strong> Plan pays to any of its other preferred or innetwork<br />
providers .<br />
16. Hours and Days of Service.<br />
The hours and days of service of the <strong>Indian</strong> <strong>Health</strong> Care Provider shall be established by such Provider.<br />
At the request of the Qualified <strong>Health</strong> Plan, such Provider shall provide written notification of its hours<br />
and days of service.<br />
17. Sovereign Immunity.<br />
Nothing in the Qualified <strong>Health</strong> Plan's agreement or in any addendum thereto shall constitute a waiver of<br />
federal or tribal sovereign immunity.<br />
18. Endorsement.<br />
An endorsement of a non-Federal entity, event, product, service, or enterprise may be neither stated nor<br />
implied by the IHS provider or IHS employees in their official capacities and titles. Such agency names<br />
and positions may not be used to suggest official endorsement or preferential treatment of any non-<br />
Federal entity under this agreement.<br />
APPROVALS<br />
For the Qualified <strong>Health</strong> Plan: For the <strong>Indian</strong> <strong>Health</strong> Care Provider:<br />
____________________________________ __________________________________<br />
Date ________________________________ Date ______________________________<br />
8/7/12 DRAFT Addendum – Page 5<br />
Comment [A2]: The base agreement will specify<br />
the payment rate. Not sure what legal standing this<br />
statement would have.
Notes from Tribal Consultation with HHS on Federally-facilitated Exchange (FFE)<br />
and Medicaid Expansion<br />
July 26 (Washington, DC), August 6 (Anchorage, AK), August 9 (Denver, CO), as well<br />
as IHS consultation with tribes on ACA August 8 (Denver, CO)<br />
Notes from Mim Dixon (with additions from Doneg McDonough shown in bold)<br />
1. We now have agenda for FFE Tribal Consultation Sessions.<br />
a. Jennifer Cooper put together talking points that tracked the agenda for DC<br />
session and revised for Anchorage session.<br />
- A revised version was prepared for the Denver session.<br />
b. No real opportunity for written statements or comments unrelated to topics.<br />
c. Morning about Medicaid Expansion.<br />
2. FFE Developments<br />
i. No real news about Medicaid Expansion alternatives.<br />
ii. Administration is encouraging interest groups (Tribes, Hospital Assn) to<br />
work together to pressure Republican governors and legislatures to adopt<br />
ME.<br />
a. TTAG’s ACA Policy Committee is meeting weekly to work on some issues.<br />
Only agenda items identified to date are:<br />
i. Addendum + Companion piece explaining addendum<br />
ii. Tribal Sponsorship<br />
iii. Network adequacy / contracting with I/T/U<br />
iv. Other topics will be prioritized as high impact, high value topics<br />
b. For Addendum and companion piece, Pete Nakahata has said process will<br />
be: ACA Subcommittee – HHS Legal Counsel – Tribal Consultation – completion<br />
in September.<br />
- A session with the ACA Policy Committee on the <strong>Indian</strong> Addendum<br />
was held during a break in the Denver consultation. Policy<br />
Committee reviewed edits on documents from P. Nakahata. Final<br />
1
edits on documents are due back from tribal reps to P. Nakahata by<br />
8/14.<br />
- P. Nakahata recommended that the topic for the 8/16 ACA Policy<br />
Committee meeting will be tribal sponsorship.<br />
c. CCIIO has a request for input on data elements pertaining to an “<strong>Indian</strong><br />
placeholder” to be included in the single application form being developed by<br />
CMS for use by Exchanges.<br />
i. Formal comments are due back to CMS on CMS-10439 by<br />
September 4, 2012<br />
- Jennifer Cooper agreed to prepare a draft response by<br />
pulling from prior comments on this issue that were submitted<br />
by NIHB/TTAG.<br />
ii. A Webinar will be held on this issue on August 20 at 3:00 pm EDT<br />
iii. An all tribes call is scheduled for September 7 at 1:00 pm EDT.<br />
iv. TTAG asked that the whole process be explained to put AI questions<br />
in context – not sure whether this will be ACA Policy Subcommittee or<br />
another group.<br />
v. TTAG had already submitted questions to use, but it doesn’t seem like<br />
these are being referenced by CCIIO.<br />
d. CCIIO has stated that monthly enrollment periods for AI/AN will have a cut-off<br />
date of the 15 th of each month for enrollment beginning on the 1 st of the following<br />
month. (People who apply on the 16 th wouldn’t be enrolled for 6 weeks.)<br />
e. CCIIO has stated that termination of coverage requires 14 days notice.<br />
f. According to CCIIO, ACA does not include IHS as ECPs, and therefore any<br />
requirement for QHPs to contract with ECPs would not include IHS.<br />
g. At the TTAG meeting, the website and data management folks spoke for the<br />
first time and they said they are using open source computer software that allows<br />
them to re-program quickly and easily to add elements over time. They seem to<br />
grasp AI issues.<br />
h. At MMPC meeting, IRS representatives said they expected that AI/AN<br />
applying for waiver of penalty would only have to use self-attestation that they<br />
2
are eligible for the waiver (i.e., they would not have to go through the Exchange<br />
application process to determine their eligibility as AI/AN).<br />
i. NPRM on AI/AN cost sharing waiver and how providers/QHPs will be paid by<br />
Federal government for the amount of cost sharing they are not collecting from<br />
AI/AN will be issued in August.<br />
3. New Issues that came up at FFE Tribal Consultation in DC, July 26<br />
a. Partnerships - Administration is encouraging Partnership arrangements with<br />
states and it’s not clear whether Tribes need to be consulting with States or<br />
Feds, or both. More work for Tribes and very confusing.<br />
b. State Exchange Tribal Consultation Policies - States are not being required to<br />
have Tribal Consultation Policy for Exchanges until they submit the package to<br />
be certified (April 2013) – which means Tribes will not necessarily be consulted in<br />
the decisions about Exchanges.<br />
- Example: Essential <strong>Health</strong> Benefits<br />
c. <strong>Indian</strong> questions on application - Amy Erhardt is working on the applications<br />
and she said that waiver of cost sharing will only happen if applicant declares<br />
that they want to be considered for an “Insurance Accessibility Program”.<br />
i. The law says all AI are eligible for cost sharing waivers, even if they<br />
don’t want one of the Insurance Accessibility Programs (Medicaid, CHIP,<br />
Advanced Tax Credits).<br />
ii. This is important because we don’t want MAGI calculated for people<br />
who haven’t filed tax returns.<br />
iii. This approached was not challenged in the DC meeting.<br />
iv. New acronym: APTC/CSR (= Advanced Payment of Tax Credits and<br />
Cost Sharing Reductions)<br />
c. Navigators and In Person Assistance - (Holly Whalen is CCIIO point person<br />
on this)<br />
I. Looks like there will be competition for Navigator grants at federal level<br />
– no set aside for Tribes.<br />
ii. A second source of funding that can come from federal establish<br />
grants, but is not identified in the law is “in-person assistance.”<br />
3
d. CCIIO Philosophy - CCIIO is taking the approach that “where we start is not<br />
where we finish”, in other words, they want to stand up the FFE as quickly as<br />
possible and go back and correct things that aren’t working.<br />
i. Tribes know from experience with CMS that it is better to get things right<br />
the first time rather than going back and trying to fix things that are in<br />
writing later.<br />
ii. Too many people in CMS/HHS are referring to Tribes as “Stakeholders”<br />
and not acknowledging the special legal/political status and governmentto-government<br />
relationship<br />
4. Additional information provided during teleconference<br />
a. State Exchanges are expecting to decide on their QHP requirements for<br />
network adequacy in September or October and they are looking to CCIIO for<br />
guidance, including decisions about the FFE.<br />
b. State Exchange Tribal Consultation<br />
i. NM is moving forward on planning an exchange using a consultant, and<br />
the Exchange will be housed in the NM <strong>Health</strong> Alliance. Tribal input has<br />
been limited.<br />
ii. AZ is planning a State Exchange.<br />
c. Basic <strong>Health</strong> Programs<br />
i. Only 3 states are expected to have BHP: WA, VT, RI<br />
ii. CA has a BHP now, but they may drop it.<br />
5. Next steps recommended in teleconference<br />
a. Alaska Consultation, August 7<br />
i. Val should invite Pete and other federal officials to lunch at ANMC and<br />
include a tour of the facility and SCF outpatient services.<br />
ii. Comments in Alaska should focus on network adequacy, including both<br />
ANMC and village clinics.<br />
iii. Participants should tell Pete that they realize that not many federal<br />
officials could attend, but they are relying on him to communicate issues to<br />
others, particularly those whose decisions are outside his control.<br />
4
iv. Suggest that Medicaid/CHIP representative be at the table for<br />
discussion of single application and data elements.<br />
b. Doneg volunteered to take notes at Anchorage and Denver and distribute a<br />
document to Tribes (through TSGAC and MMPC) with new issues that are<br />
identified. Issues identified in Anchorage will be distributed quickly, so that they<br />
can be included in the Denver consultation.<br />
c. Denver Consultation, August 9<br />
i. Diddy will organize a Tribal caucus on the evening of August 8<br />
ii. Jim Roberts will facilitate the Tribal caucus<br />
iii. MMPC and TSGAC will notify Tribes about the caucus date, time,<br />
place.<br />
iv. There is also a 3 hour time slot in the IHS consultation for ACA and the<br />
following topics are recommended:<br />
(1) How will IHS respond to sponsorship opportunity for people in<br />
Direct Service Tribes?<br />
d. Letter to Michael Hash to be sent by NIHB, TSGAC (and possibly TTAG) with<br />
cc to Secretary to cover these topics: 1) referring to AI/AN and Tribes as<br />
“stakeholders” is not consistent with CMS policy; and 2) need for greater<br />
oversight on State Tribal consultation in Exchanges.<br />
e. Second letter to Michael Hash with summary of issues that surfaced in the 3<br />
FFE Tribal Consultation meetings and the Tribal positions on those issues.<br />
6. Points made at the Anchorage and Denver tribal consultations with HHS on<br />
FFE and Medicaid Expansion<br />
a. CMS stated that the new (and ACA-intended mandatory) Medicaid<br />
expansion to adults without dependent children with incomes up to<br />
138% FPL will be considered a “voluntary” expansion group. As with<br />
other voluntary expansion groups under Medicaid --<br />
i. A state is able to cancel the expansion in the future.<br />
ii. AI/AN-specific protections (e.g., ARRA premium and cost-sharing<br />
protections) carry over to the expansion population, including –<br />
- No premiums or cost sharing<br />
- Ability to choose an I/T/U provider that is in plan network<br />
5
- I/T/U provider receives their all-inclusive or FQHC rate<br />
(either directly from the plan or Medicaid makes up the<br />
difference between plan payment and the I/T/U’s rate)<br />
iii. There is not a specific date by which a state has to inform CMS<br />
that it intends to expand Medicaid. The standard State Plan<br />
Amendments procedures apply.<br />
b. Other changes to Medicaid called for under the ACA are to be<br />
implemented whether or not a state exercises the Medicaid expansion<br />
option.<br />
i. Application of a uniform definition of income using the new<br />
definition of modified adjusted gross income (MAGI)<br />
ii. No asset test for non-long term care service eligibility<br />
iii. Maintenance of effort requirements on income eligibility continue<br />
through 2019 for children and through 2014 for others<br />
c. The ACA-directed study of a Navajo “single state agency for Medicaid”<br />
was referenced several times by CMS and IHS.<br />
i. The initial draft of the study is due from the contractor<br />
Econometrica to CMS by October 2013.<br />
ii. A final report is due to Congress from CMS by early 2014<br />
d. Determining “<strong>Indian</strong>” for Exchange and IRS-related provisions.<br />
i. In response to the question “How will AI/AN prove that they don’t<br />
have to have insurance”, CMS staff responded “Exchange will<br />
have to issue a letter or other document to an AI/AN so they have<br />
proof.”<br />
- It seems that this answer needs further clarification, if not<br />
revision.<br />
ii. A follow-up question was asked: “what documentation is required<br />
by an AI/AN to provide to the Exchange to prove being an AI/AN”.<br />
CMS staff responded: “CMS needs more input from tribes.”<br />
e. Certification standards applied to Qualified <strong>Health</strong> Plans offered through<br />
an Exchange.<br />
6
i. CMS stated on a couple of occasions that states have the ability to<br />
apply additional standards on QHP than the minimum standards<br />
established by CMS<br />
- Imposing a requirement that all QHP’s in a state Exchange<br />
must offer to contract with I/T/U would be allowable.<br />
ii. CMS stated they would need to issue additional formal<br />
regulations if the FFE were to impose additional requirements on<br />
QHP, such as requiring a plan to offer to contract with each I/T/U.<br />
- CMS staff also indicated that, while it is not certain and<br />
they didn’t offer to include any AI/AN-specific provisions if<br />
they do, it is likely that CMS will be issuing further formal<br />
guidance on the FFE.<br />
f. Who should tribes engage in tribal consultation with regarding Exchange<br />
operations?<br />
i. For state-based Exchanges, state officials.<br />
ii. For strictly FFE, engage CMS but no explanation was given yet of<br />
how tribes will engage CMS on state-specific issues that may<br />
apply solely to one specific state FFE (versus the discussions<br />
going on now between TTAG and CMS on the national FFE<br />
design.)<br />
iii. For Partnership exchanges, engage states on the specific<br />
functions a state may decide to operate.<br />
- Plan management (e.g., certification of QHP)<br />
- Outreach and enrollment assistance (e.g., Navigator<br />
program and “in-person assistance”)<br />
g. Liability for tax penalty for certain IHS beneficiaries<br />
- In response to questions, the IHS Director and CMS staff<br />
acknowledged that some IHS beneficiaries who choose not to<br />
purchase health insurance coverage and who do not meet the<br />
definition of <strong>Indian</strong> under the IRC definition could be liable for the<br />
tax penalty administered by the IRS for not having “creditable<br />
coverage”.<br />
h. Analysis of impact of Medicaid expansion on states<br />
7
i. CMS rep. commented that an analysis is underway to determine<br />
the impact on each state from exercising the new Medicaid<br />
expansion option, but the analysis isn’t complete.<br />
- It wasn’t clear if CMS or another party was doing the<br />
analysis.<br />
- CMS rep. noted that it looks as if the Medicaid expansion will<br />
prove to reduce some/many state’s overall local<br />
expenditures.<br />
ii. CMS rep. cited statistics for a select number of states on the<br />
reduction in the percentage of uninsured persons in the state<br />
solely from a state exercising the new Medicaid expansion option<br />
(up to 138%). The data source was not cited.<br />
- Montana: 66%<br />
- North Dakota: 67%<br />
- South Dakota: 50%<br />
- Oklahoma: 74%<br />
- Arizona: 65%<br />
i. For non-expansion states, in response to questions raised in<br />
Anchorage and Denver --<br />
i. CMS commented “We would be very interested in waiver<br />
proposals” from states/tribes designed to expand Medicaid<br />
coverage solely to AI/AN through I/T/U, possibly structured<br />
similar to the approved approach for AI/AN-specific benefits in<br />
Arizona.<br />
ii. CMS is considering developing a template for states to use in<br />
requesting a waiver to extend Medicaid coverage to AI/AN.<br />
j. State Plan Amendment or waiver request to CMS<br />
i. CMS emphasized that tribes in a state have the ability to request<br />
tribal consultation directly with CMS if they are not satisfied with<br />
the tribal consultation process and outcomes undertaken with the<br />
state.<br />
8
ii. New Mexico tribes raised concerns about the state’s tribal<br />
consultation held with regard to their pending Medicaid waiver,<br />
and they may wish to request the direct consultation with CMS.<br />
k. IHCIA section 206 and “reasonable charges”<br />
i. CMS and IHS were asked if an I/T/U’s FQHC or IHS all-inclusive<br />
rates would meet the definition of “reasonable charges” under<br />
section 206.<br />
ii. The CMS and IHS reps did not know.<br />
l. Outreach and Education Funding<br />
i. Tribes and tribal organizations are eligible to apply for grants<br />
under the Navigator program.<br />
ii. Funding will be available under the “in-person assistance”<br />
program for assisting individuals to enroll in Exchange and<br />
Medicaid coverage.<br />
- The lead CMS staff member / contact for the in-person<br />
assistance program is Holly Whelan, Consumer Support<br />
Group, CCIIO-CMS, holly.whelan@cms.hhs.gov<br />
iii. Medicaid Administrative Match (MAM) remains an option for<br />
states to be reimbursed by CMS for the costs of tribes<br />
performing enrollment assistance.<br />
- A question was raised as to how funding may be used /<br />
time may be allocated between combined Medicaid and<br />
Exchange eligibility assistance but a specific answer<br />
was not given.<br />
iv. $4 million in CMS CHIPRA funding for AI/AN-specific<br />
education and outreach in 2013.<br />
v. $32 million in CMS CHIPRA funding for general education and<br />
outreach in 2013.<br />
– Tribes and tribal organizations can apply for the<br />
general CHIPRA funds.<br />
9
IHS TRIBAL SELF-GOVERNANCE ADVISORY COMMITTEE<br />
c/o Self-Governance Communication and Education<br />
5060 Pacific Highway, Suite 101, Ferndale, WA 98248<br />
Telephone (360) 380-1820 ~ Facsimile (360) 380-1981 ~ Website: www.tribalselfgov.org<br />
October 5, 2012<br />
Sent Via Fax Dr. Petzel: (202) 273-5787<br />
Sent Via Email Dr. Roubideaux: Rene.Joseph@ihs.gov<br />
Originals Sent Via USPS<br />
Dr. Robert A. Petzel, M.D. Dr. Yvette Roubideaux, M.D., M.P.H., Director<br />
Under Secretary for <strong>Health</strong> <strong>Indian</strong> <strong>Health</strong> Service<br />
Department of Veterans Affairs Department of <strong>Health</strong> and Human Services<br />
810 Vermont Avenue, NW Room 448, The Reyes Building<br />
Room 800 801 Thompson Avenue<br />
Washington, DC 20420 Rockville, MD 20852<br />
RE: Negotiation of Participating Tribal <strong>Health</strong> Program Agreements with Local<br />
VA Facilities: Need for Inclusion of Agreed Upon Payment Methodologies<br />
Dear Dr. Petzel & Dr. Roubideaux:<br />
On behalf of the Tribal Self-Governance Advisory Committee (TSGAC), we are writing to<br />
provide comments on one component of the latest set of materials released by the Department<br />
of Veterans Affairs (VA) regarding implementation of section 405(c) of the <strong>Indian</strong> <strong>Health</strong> Care<br />
Improvement Act (IHCIA). We appreciate the opportunity last week during the <strong>National</strong> <strong>Indian</strong><br />
<strong>Health</strong> <strong>Board</strong> Annual Consumer Conference in Denver, Colorado to discuss with the VA, as well<br />
as with the <strong>Indian</strong> <strong>Health</strong> Service (IHS), securing reimbursement for health care services<br />
provided to eligible veterans by the IHS, Tribes and Tribal Organizations. The sessions were<br />
helpful to the Tribal participants, and we are encouraged that the VA is moving forward with<br />
establishing agreements with Tribal health programs without restricting participation to a small<br />
number of Tribal organizations under a demonstration project. We remain concerned, though,<br />
that the <strong>National</strong> Reimbursement Agreement between the VA and IHS has not been finalized<br />
and executed.<br />
The TSGAC has previously provided comments on various aspects of implementation of IHCIA<br />
section 405(c) since the provision was enacted in March of 2010. (TSGAC letters to VA/IHS<br />
dated April 4, April 18, and May 25, 2012.) We believe the successful implementation of section<br />
405(c) will serve to: (1) improve access to health care services for our veterans by expanding<br />
access and reimbursement at IHS and Tribal facilities; and (2) strengthen and improve the care<br />
received by veterans through improved coordination of their care across VA, IHS and Tribal<br />
facilities. We wish to acknowledge the apparent inclusion by the VA (as indicated in the VA’s<br />
August 24, 2012 Dear Tribal Leader letter) of a number of items TSGAC had previously<br />
recommended, particularly the exclusion of copayments for Tribally-provided services and the<br />
inclusion of behavioral health care and long-term care services as reimbursable services.<br />
In an earlier VA document titled “VA-IHS Draft Agreement – Reimbursement for Direct <strong>Health</strong><br />
Care Services: Summary” (Summary of Reimbursement Agreement dated March 2, 2012), it<br />
stated that a number of items had been successfully negotiated between the VA and the IHS,
Letter: Dr. Robert Petzel, Under Secretary, VA & Dr. Yvette Roubideaux, Director, IHS<br />
RE: Negotiation of Participating Tribal <strong>Health</strong> Program Agreements with Local<br />
VA Facilities: Need for Inclusion of Agreed Upon Payment Methodologies<br />
Page 2 of 4 October 5, 2012<br />
including the payment methodologies to be used in the Participating Tribal <strong>Health</strong> Program<br />
Agreements. The Summary of Reimbursement Agreement document stated:<br />
Payment methodologies are proposed to be basically the same as what IHS<br />
hospitals and clinics are reimbursed for now: Inpatient hospital services would be<br />
based on Medicare payment methodologies specific to the type of rate already<br />
received (IPPS, CAH, etc); Outpatient services would be based on the IHS all<br />
inclusive rate for Medicare and Medicaid. Other specific rates will be spelled out in<br />
the document.<br />
In the April 5, 2012 “Final Consultation Draft” of the “Draft Agreement between the Department<br />
of Veterans Affairs and Department of <strong>Health</strong> and Human Services <strong>Indian</strong> <strong>Health</strong> Service for<br />
Reimbursement for Direct <strong>Health</strong> Care Services” (Draft <strong>National</strong> Reimbursement Agreement),<br />
additional detail on the agreed upon payment methodologies was included. TSAGC endorses<br />
section VII. Reimbursement for Direct Care Services, subsections A – F, of the Draft <strong>National</strong><br />
Reimbursement Agreement, as follows:<br />
VII. REIMBURSEMENT FOR DIRECT CARE SERVICES<br />
A. Except to the extent inconsistent with the rate methodology explained herein, VA<br />
shall reimburse at rates based on Medicare payment methodologies for services,<br />
including home and community based services, to Eligible AI/AN Veterans.<br />
B. Inpatient Hospital Services. Except to the extent inconsistent with the rate<br />
methodology explained herein, VA shall reimburse at rates based on Medicare<br />
payment methodologies for services to Eligible AI/AN Veterans. The payment<br />
methodology under this section applies to all inpatient services furnished by the<br />
hospital, whether provided by part of a department, subunit, distinct part, or other<br />
component of a hospital (including services furnished directly by the hospital or<br />
under arrangements with contract providers who provide Direct Care Services<br />
onsite in an IHS or Tribal health facility).<br />
1. Payment for hospital services that the Medicare program would pay under a<br />
prospective payment system (PPS) will be based on the applicable PPS. For<br />
example, payment for inpatient hospital services shall be made per discharge<br />
based on the applicable PPS used by the Medicare program to pay for similar<br />
hospital services under 42 C.F.R. Part 412.<br />
2. For hospitals that furnish inpatient services but are exempt from PPS and receive<br />
reimbursement based on reasonable costs (for example, critical access hospitals<br />
(CAHs)), including provider subunits exempt from PPS, payment shall be made<br />
per discharge based on the reasonable cost methods established under 42<br />
C.F.R. Part 413, except that the interim payment rate under 42 C.F.R. Part 413,<br />
subpart E shall constitute payment in full.<br />
3. The inpatient rates set forth above do not include inpatient physician services<br />
and practitioner services. The inpatient physician and other practitioner services<br />
shall be billed based on the Medicare fee schedule.
Letter: Dr. Robert Petzel, Under Secretary, VA & Dr. Yvette Roubideaux, Director, IHS<br />
RE: Negotiation of Participating Tribal <strong>Health</strong> Program Agreements with Local<br />
VA Facilities: Need for Inclusion of Agreed Upon Payment Methodologies<br />
Page 3 of 4 October 5, 2012<br />
C. Outpatient Hospital Services and Freestanding Clinic Services. VA shall pay for<br />
outpatient and free standing clinics services to Eligible AI/AN Veterans at the all<br />
inclusive rate approved each year by the Director of IHS, under the authority of<br />
sections 321(a) and 322(b) of the Public <strong>Health</strong> Service Act (42 U.S.C. §§ 248<br />
and 249(b)), Public Law 83-568 (42 U.S.C. § 2001(a)), and the <strong>Indian</strong> <strong>Health</strong><br />
Care Improvement Act (25 U.S.C. § 1601 et seq.). This rate is published annually<br />
in the Federal Register under the title: Outpatient Per Visit Rate (Excluding<br />
Medicare).<br />
D. Federally Qualified <strong>Health</strong> Centers. For facilities reimbursed by Medicare at the<br />
Medicare Federally Qualified <strong>Health</strong> Center Rate, VA shall pay for services to<br />
Eligible AI/AN Veterans at the Medicare Federally Qualified <strong>Health</strong> Center rate.<br />
E. Ambulatory Surgical Services. VA shall reimburse for services to Eligible AI/AN<br />
Veterans at established Medicare rates for freestanding Ambulatory Surgery<br />
Centers.<br />
F. Inpatient Pharmacy Services/Outpatient Pharmacy Services/ Take-Home Drugs.<br />
VA agrees to provide reimbursement for inpatient medications for Eligible AI/AN<br />
Veterans receiving direct inpatient care in IHS and Tribal hospitals. For outpatient<br />
medications, IHS, Tribes and VA agree to use the VA Consolidated Mail<br />
Outpatient Pharmacy (CMOP) for routine/ongoing/regular prescriptions written for<br />
Eligible AI/AN Veterans under this agreement. VA agrees to provide<br />
reimbursement of the cost of medication dispensed for the provision of outpatient<br />
emergent need prescriptions or other outpatient prescriptions requiring provision<br />
to eligible patients to initialize or continue therapy before CMOP can provide. In<br />
those instances, those prescriptions are to be limited to not more than a 14-day<br />
(Alaska: 30-day) supply.<br />
We would like to emphasize that the rates in subsections A through E – which parallel the<br />
reimbursement methodologies in use today under Medicare for IHS, Tribe and Tribal health<br />
programs – were established in order to cover the costs of care at these facilities to the eligible<br />
beneficiaries. Any proposed reductions to these rates would result in revenues to the facilities<br />
being below the costs of providing the care to the AI/AN veterans, which would not be<br />
acceptable.<br />
In closing, we strongly recommend, to the extent that participating Tribal health program<br />
agreements with local VA facilities are put in place prior to the execution of a <strong>National</strong><br />
Agreement on Reimbursement for <strong>Health</strong> Care Services, that the above payment policies<br />
contained in the Draft <strong>National</strong> Reimbursement Agreement be incorporated into each<br />
participating Tribal health program agreement unless the participating Tribal health program<br />
specifically requests that alternate payment policies be employed. We further recommend that<br />
the payment methodologies contained in the Draft <strong>National</strong> Reimbursement Agreement be<br />
retained in the final <strong>National</strong> Reimbursement Agreement.<br />
We encourage the VA and IHS to finalize this agreement as soon as possible, after taking into<br />
consideration the remaining issues identified in the previous TSGAC comment letters. We look
Letter: Dr. Robert Petzel, Under Secretary, VA & Dr. Yvette Roubideaux, Director, IHS<br />
RE: Negotiation of Participating Tribal <strong>Health</strong> Program Agreements with Local<br />
VA Facilities: Need for Inclusion of Agreed Upon Payment Methodologies<br />
Page 4 of 4 October 5, 2012<br />
forward to continuing to work with you. If you have any questions, you can reach me at (860)<br />
862-6192; or via email: lmalerba@moheganmail.com.<br />
Sincerely,<br />
Chief Lynn Malerba, Mohegan Tribe<br />
Chairwoman, TSGAC<br />
cc: P. Benjamin Smith, Director, Office of Tribal Self-Governance, IHS<br />
Stephanie E. Birdwell, M.S.W. Director, Office of Tribal Government Relations, VA<br />
Stacy Bohlen, Executive Director, <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
TSGAC Members<br />
TSGAC Technical Workgroup Members
October 17, 2012<br />
Dr. Robert Petzel, M.D. Dr. Yvette Roubideaux, M.D., M.P.H., Director<br />
Under Secretary <strong>Indian</strong> <strong>Health</strong> Service<br />
Department of Veterans Affairs Room 448, The Reyes Building<br />
810 Vermont Avenue 801 Thompson Avenue<br />
Washington, D.C. 20420 Rockville, MD 20852<br />
RE: <strong>National</strong> All Inclusive Reimbursement Rate Agreement<br />
Dear. Dr. Petzel, and Dr. Roubideaux:<br />
On behalf of the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NIHB), I respectfully submit the following<br />
recommendation contained in this letter regarding the Department of Veterans Affairs’ (VA)<br />
implementation of the reimbursement requirements under Section 405(c) of the <strong>Indian</strong> <strong>Health</strong><br />
Care Improvement Act (IHCIA). 1 Tribes see the implementation of reimbursement rates as a top<br />
priority that remains to be fulfilled.<br />
NIHB recommends that all Tribal facilities and <strong>Indian</strong> <strong>Health</strong> Service (IHS) operating<br />
programs receive reimbursement from the VA for services provided to our Native<br />
American Veterans based upon the Medicaid All-Inclusive rate rather than the Medicare<br />
Fee Schedule cost reimbursement rate that is applicable to a Federally Qualified <strong>Health</strong><br />
Center (FQHC). This important issue will play a critical role in allowing AI/AN access to<br />
quality health care, especially as Tribes enter into negotiations with the VA for terms and<br />
conditions for reimbursement rates for ambulatory services.<br />
In the April 5, 2012, “Final Consultation Draft” of the “Draft Agreement between the VA and<br />
IHS for Reimbursement for Direct <strong>Health</strong> Care Services” (Draft <strong>National</strong> Reimbursement<br />
Agreement), additional detail on the agreed upon payment methodologies was included. Included<br />
was Section VII Reimbursement for Direct Care Services, which further articulated VA’s policy<br />
that reimbursement would be based at the Medicaid All-Inclusive Rate for outpatient hospital<br />
services. Initially, Tribes were pleased with the decision by VA to rely on the Medicaid All-<br />
Inclusive Rate approved by the IHS Director and published in the Federal Register as the basis<br />
of reimbursement.<br />
1 Section 405(c) requires the VA to reimburse the IHS, an <strong>Indian</strong> Tribe or Tribal Organization “where services are<br />
provided through the Service, an <strong>Indian</strong> Tribe or a Tribal Organization to beneficiaries eligible for services from the<br />
[VA], notwithstanding any other provisions of law.”
P a g e | 2<br />
Now there appears to be confusion among the Tribes about the rate of reimbursement that Tribal<br />
health facilities and IHS will receive from the VA for services provided to AI/AN eligible<br />
veterans. Tribes had the opportunity last month at the NIHB Annual Consumer Conference in<br />
Denver, Colorado to discuss with the VA securing reimbursement for health care services<br />
provided to AI/AN eligible veterans. Following these discussions and a brief period of tribal<br />
consultations where the reimbursement rate was not an issue, the VA has now stated that the<br />
reimbursement rate will be the Medicare Fee Schedule as opposed to the original understanding<br />
by Tribes that the Medicaid All-Inclusive Rate would apply, which was contained in the VA’s<br />
previously-published Draft Agreement with IHS.<br />
Reimbursement rates vary by payer source. For example, the Medicaid reimbursement rate is<br />
significantly higher than the Medicare FQHC rate for the same service. NIHB recommends that<br />
the reimbursement rate under the VA Agreement for all tribal health facilities be based upon the<br />
All-Inclusive Rate rather than the Medicare Fee Schedule reimbursement rate as an FQHC in<br />
order to cover the costs of care at these facilities to the eligible beneficiaries. Any proposed<br />
reductions in reimbursement rates could result in revenues to the facilities below the costs of<br />
providing the care to the AI/AN veterans.<br />
As you already know, many of the Alaska Tribal <strong>Health</strong> Programs (ATHPs) have collectively<br />
negotiated and entered into agreements with the VA under which they will be reimbursed for<br />
health care services provided to AI/AN veterans based on the Medicaid All-Inclusive Rate. This<br />
historic agreement expands access to health care to Alaska’s veterans. Already, enrollment<br />
efforts have been redoubled and the number of enrolled AI/AN veterans is increasing in Alaska.<br />
Similar to the successfully negotiated agreements between ATHPs and the VA, NIHB believes<br />
the Medicaid All-Inclusive Rate to be the appropriate reimbursement rate for all Tribes<br />
throughout <strong>Indian</strong> Country.<br />
I respectfully ask that you consider our recommendation outlined above, specifically that all<br />
tribal health facilities and IHS receive the Medicaid All-Inclusive reimbursement rate from the<br />
VA for services provided to eligible AI/AN veterans instead of the Medicare Fee Schedule rate<br />
as an FQHC.<br />
Thank you in advance for consideration of these recommendations as we jointly work to advance<br />
the health status of AI/AN individuals and communities across the United States.<br />
Yours in <strong>Health</strong>,<br />
Cathy Abramson<br />
Chairperson<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>
A BILL<br />
To correct inconsistencies in the definitions affecting Native Americans under the Patient<br />
Protection and Affordable Care Act.<br />
Be it enacted by the Senate and House of Representatives of the United States of America in<br />
Congress assembled,<br />
SECTION 1. TECHNICAL CORRECTIONS RELATING TO THE DEFINITIONS OF<br />
INDIAN IN PPACA.<br />
IN GENERAL.—Title I of the Patient Protection and Affordable Care Act is amended—<br />
(1) in section 1311(c)(6)(D), by striking ‘‘(as defined in section 4 of the <strong>Indian</strong> <strong>Health</strong><br />
Care Improvement Act)’’ and inserting ‘‘(as defined in section 447.50(b)(1) of title 42 of<br />
the Code of Federal Regulations, as in effect on July 1, 2010)’’; and<br />
(2) in section 1402(d)(1), by striking ‘‘(as defined in section 4(d) of the <strong>Indian</strong> Self-<br />
Determination and Education Assistance Act (25 U.S.C." "450b(d)))’’ and inserting ‘‘(as<br />
defined in section 447.50(b)(1) of title 42 of the Code of Federal Regulations, as in effect<br />
on July 1, 2010)’’.<br />
(3) in section 1501(b), by striking “MEMBERS OF INDIAN TRIBES. —Any applicable<br />
individual for any month during which the individual is a member of an <strong>Indian</strong> tribe (as<br />
defined in section 45A(c)(6)) and inserting ‘‘INDIANS.—Any applicable individual who<br />
is an <strong>Indian</strong> (as defined in section 447.50(b)(1) of title 42 of the Code of Federal<br />
Regulations, as in effect on July 1, 2010).”
a b c d<br />
e<br />
IHS & Medicaid Align<br />
IHS Eligibility for<br />
AI/ANs<br />
Chart of <strong>Indian</strong>-specific <strong>Health</strong> Care Provisions<br />
with Different Citations in Federal Law for Defining "<strong>Indian</strong>"<br />
Medicaid:<br />
Protections and<br />
Benefits for AI/ANs<br />
Monthly Enrollment<br />
Periods for AI/AN's<br />
Sec. 4 IHCIA<br />
Affordable Care Act-related Provisions<br />
<strong>Health</strong> Insurance Exchange-related Provisions<br />
Cost-Sharing Protections for AI/AN's<br />
Sec. 4(d) ISDEAA<br />
No cost-sharing for<br />
AI/ANs under 300%<br />
FPL (at all providers)<br />
No cost-sharing for<br />
AI/ANs served by<br />
I/T/U; payment of full<br />
amount due to I/T/U<br />
(without cost-sharing<br />
reductions)<br />
CMS stated in regulations these definitions "operationally mean the same<br />
thing."<br />
Exemption from<br />
IRC tax penalties<br />
for AI/ANs not<br />
having "minimum<br />
essential coverage"<br />
IRC 45A(c)(6)<br />
IRS stated informally in meetings these definitions are the same.<br />
NPAIHB / TSGAC v. 1.1
California Rural <strong>Indian</strong><br />
<strong>Health</strong> <strong>Board</strong><br />
September 21, 2012<br />
Valerie B. Jarrett, Senior Advisor<br />
The White House<br />
1600 Pennsylvania Avenue N.W.<br />
Washington, DC 20500<br />
Dear Ms. Jarrett and Ms. Gillette:<br />
Jodi Gillette, Senior Policy Advisor<br />
Native American Affairs<br />
1600 Pennsylvania Avenue N.W.<br />
Washington, DC 20500<br />
Northwest Portland Area<br />
<strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
The California Rural <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (CRIHB) and the Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
(NPAIHB) are Tribal organizations organized under the <strong>Indian</strong> Self-Determination and Education Assistance<br />
Act. 1 Our organizations represent health care issues of 63 federally-recognized Tribes in California, Idaho,<br />
Oregon, and Washington. We are writing to you about a very important Affordable Care Act matter.<br />
In just three months, States will be applying to the federal government for certification of their <strong>Health</strong><br />
Insurance Exchanges under the Affordable Care Act. One of the current activities for both State Exchanges<br />
and the Federally-Facilitated Exchange is to create a single streamlined application for Medicaid, Child <strong>Health</strong><br />
Insurance Programs, and the individual Exchanges. The Administration’s goal of a short and simple application<br />
that uses electronic data bases is at odds with regulatory guidance regarding identifying American <strong>Indian</strong>s and<br />
Alaska Natives (AI/AN) for the purposes of cost sharing waivers, special enrollment periods, and other<br />
protections in Medicaid, CHIP and the Exchanges. It is imperative that the White House provide guidance on<br />
this issue so that AI/AN who were intended to benefit from ACA are not left out.<br />
Here is a short list of potential problems that could occur if the definition of <strong>Indian</strong> used by Exchanges is<br />
different from the one used by Medicaid and CHIP:<br />
An AI/AN child who is not allowed to enroll as tribal members until her 18 th birthday will not be<br />
considered as AI/AN by Exchanges, although she would be considered AI/AN by Medicaid and CHIP.<br />
An Alaska Native adult will not be considered AI/AN by Exchanges until his parent dies and he inherits<br />
stock in an Alaska Native corporation. And his children will not be considered AI/AN by Exchanges<br />
until he dies and his stock in an Alaska Native corporation is passed along to his children, even though<br />
they qualify as AI/AN under Medicaid and CHIP.<br />
1 As defined in the <strong>Indian</strong> Self-Determination and Education Assistance Act, P.L. 93-638, 25 U.S.C., Section 450(b) a Tribal organization<br />
is a legally established governing body of any <strong>Indian</strong> tribe(s) that is controlled, sanctioned, or chartered by such <strong>Indian</strong> Tribe(s) and<br />
designated to act on their behalf.
An American <strong>Indian</strong> child that may not have enough blood quantum to be enrolled in a Tribe will be<br />
considered <strong>Indian</strong> under Medicaid. But not in Exchanges, because she lacks enough blood quantum to<br />
be enrolled in either of her parent’s tribe.<br />
An American <strong>Indian</strong> cannot enroll in his father’s tribe where tribal membership is passed from mother<br />
to child in what has been called matrilineal descent, and therefore he would not be considered AI/AN<br />
under Exchanges, even though he would qualify as AI/AN in Medicaid.<br />
An individual who has been determined to be AI/AN by the federal Bureau of <strong>Indian</strong> Affairs and has a<br />
Certificate of <strong>Indian</strong> Blood issued by that federal agency that is recognized by every other federal<br />
agency, is not recognized as <strong>Indian</strong> by the Federally-facilitated Exchange or state-based exchanges.<br />
A person enrolled in Medicaid as an AI/AN no longer meets the income criteria and does not purchase<br />
health insurance because she gets her care from her Tribal health clinic and assumes that she is<br />
exempt from tax penalties because she is AI/AN. However, IRS uses a different definition of AI/AN<br />
than Medicaid uses, and she finds out later that she does have to pay a tax penalty.<br />
The complications of Exchanges to administer and families to understand the varying definition of<br />
<strong>Indian</strong> and the high level of churning that is anticipated for AI/AN families will disenfranchise AI/AN<br />
families from participating in opportunities provided under the Affordable Care Act.<br />
In each of these cases, the individuals could be living in a family that is considered AI/AN, in an AI/AN<br />
community – perhaps even on a reservation, attending <strong>Indian</strong> schools funded by the federal government, and<br />
receiving their health services at an <strong>Indian</strong> <strong>Health</strong> Service clinic or hospital. They could be considered AI/AN<br />
for Medicaid, CHIP and every federal <strong>Indian</strong> program. And, still they would not be qualified for the special<br />
protections for AI/AN in <strong>Health</strong> Insurance Exchanges according to the current interpretation of ACA by the<br />
Department of <strong>Health</strong> and Human Services.<br />
As a result of the differences in how Exchange rules are being written and how Medicaid and CHIP rules are<br />
written, it is not possible to have a simple, streamlined application that relies on existing electronic data<br />
sources. The application must ask at least three different questions to determine who qualifies as <strong>Indian</strong><br />
under the different programs. Those three questions take up a lot of space on an application which will be<br />
used by a lot of people who are not AI/AN, and they will confuse a lot of people who are AI/AN. If Exchanges<br />
use the same definition as Medicaid, CHIP and the <strong>Indian</strong> <strong>Health</strong> Service, they could use the electronic<br />
registration data base from the IHS as part of the application process. However, the more restrictive<br />
definition currently in use by Exchanges may require someone at every Exchange and at every Tribal<br />
government site to process paperwork that shows that an individual has a tribal enrollment card. Ironically,<br />
the ACA calls for self-attestation for almost every aspect of the application (except citizenship), and yet AI/ANs<br />
may be expected to provide documentation instead of using self-attestation to prove that they are a member<br />
of a Tribe or Alaska Native regional or village corporation. The Administration should be trying to make it<br />
easier for underserved individuals to enroll in health insurance through Exchanges, not more difficult.<br />
Operationally, it is going to be a nightmare to have different definitions of AI/AN for Medicaid, CHIP and<br />
Exchanges. Personnel at call centers, navigators, in-person assisters, and individuals working in <strong>Indian</strong> health<br />
clinics will have to explain to people why they are considered an <strong>Indian</strong> for one federally-funded program, but<br />
not for another. Explaining the benefits of this new program will be difficult enough. As health care providers<br />
bill Medicaid Plans and Qualified <strong>Health</strong> Plans, they will need to know whether cost sharing waivers apply for<br />
some AI/AN and not for others.
As people have changes in employment, income and family size, they will churn between Medicaid to<br />
Exchange coverage assuming that the same rules apply, only to find out later that they have been<br />
disenfranchised as AI/AN from Exchanges.<br />
This is a problem that can be solved easily by having Exchanges adopt the Medicaid definition of <strong>Indian</strong> and<br />
use the same types of verification that Medicaid uses. We didn’t agree, but understood the view of lawyers<br />
and others in HHS immediately after the law passed when they asserted that since there were three different<br />
“definitions,” these problems couldn’t be fixed without a “legislative fix.” However, HHS formally, and IRS<br />
informally, have agreed that the three statutory definitions have the same meaning. We know it is not likely<br />
that Congress will amend the ACA to fix this problem in the next few months while the single, streamlined<br />
applications are being designed. It is clearly time for the Administration to reconsider relying on a regulatory<br />
correction.<br />
There are many ways to justify aligning how these definitions are implemented to correspond to how the<br />
agencies most responsible for administering programs for <strong>Indian</strong>s determine who is <strong>Indian</strong>. The attached<br />
paper discusses these. What is needed now is leadership at the highest levels to require that this problem is<br />
solved immediately through the issuance of regulations or similar guidance that applies the Medicaid<br />
definition of AI/AN to Exchanges.<br />
We would like to meet with you to discuss this issue and offer assistance to resolve it. For questions, please<br />
follow up with Jim Crouch, CRIHB Executive Director, at (916) 929-9761; or Jim Roberts, NPAIHB Policy Analyst,<br />
at (503) 347-7664.<br />
Sincerely yours,<br />
Michelle Hayward, Chairperson Andy Joseph, Jr., Chairperson<br />
California Rural <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> NW Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
Redding Rancheria Tribal Council Member Colville Tribal Council Member<br />
Attachment: “Enabling Exchanges Implement a Streamlined Application Process: The Need for a Uniform<br />
Operational Definition of <strong>Indian</strong> to Efficiently and Accurately Identify Individuals Who Are<br />
Eligible for Special Benefits and Protections”
v.7, 2012‐09‐23a<br />
Enabling Exchanges Implement a Streamlined Application Process:<br />
The Need for a Uniform Operational Definition of <strong>Indian</strong> to Efficiently and Accurately Identify<br />
Individuals Who Are Eligible for Special Benefits and Protections<br />
1, 2<br />
as American <strong>Indian</strong>s and Alaska Natives<br />
I. Executive Summary<br />
As a component of carrying out the Federal government’s special trust responsibility 3 to <strong>Indian</strong> Tribes<br />
and to American <strong>Indian</strong>s and Alaska Natives (AI/ANs), the Patient Protection and Affordable Care Act 4 –<br />
inclusive of the expansion and permanent reauthorization of the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act –<br />
authorized <strong>Indian</strong>-specific benefits and protections. The two health insurance exchange-related <strong>Indian</strong>specific<br />
provisions (i.e., monthly enrollment periods and additional cost-sharing protections) are available<br />
only to AI/ANs enrolled in the individual market through an Exchange. 5 A third <strong>Indian</strong>-specific provision<br />
in the Affordable Care Act exempts AI/ANs from tax penalties enforced through the Internal Revenue<br />
Code (IRC) for not maintaining minimum essential coverage. 6<br />
In indicating who is eligible for these <strong>Indian</strong>-specific benefits and protections, the Affordable Care Act<br />
relies upon definitions of <strong>Indian</strong> found in three different, previously-existing federal laws. Each of these<br />
definitions specifies that an <strong>Indian</strong> is “a member of an <strong>Indian</strong> tribe”, but there are slight differences in the<br />
wording of what constitutes an “<strong>Indian</strong> tribe”. Given the nearly identical language across the definitions,<br />
in the final rule for establishment of Exchanges issued by the Centers for Medicare and Medicaid Services<br />
7, 8<br />
(CMS) the two Exchange-related definitions were determined to “operationally mean the same thing.”<br />
The Internal Revenue Service has not yet formally opined on the third, IRC-based definition of <strong>Indian</strong>. 9<br />
In addition to the ACA-established special benefits and protections for AI/ANs, there are <strong>Indian</strong>-specific<br />
cost-sharing protections under Medicaid that predate the ACA. 10 For purposes of determining eligibility<br />
for the <strong>Indian</strong>-specific Medicaid cost-sharing protections, in 2010 CMS promulgated regulations at 42<br />
C.F.R. § 447.50 that drew from a range of definitions in federal law (as a definition was not provided in<br />
the law) to create a comprehensive definition of <strong>Indian</strong>. 11,<br />
To ensure AI/ANs are able to access the Medicaid- and Exchange-related special benefits and protections<br />
and Exchanges are able to efficiently and consistently make eligibility determinations, and given the<br />
apparent agreement that the definitions of <strong>Indian</strong> applicable within the Exchange are operationally the<br />
same, the primary issues remaining to resolve are 1) whether operational guidance will be issued to aid in<br />
determining eligibility for Exchange-related <strong>Indian</strong>-specific benefits and protections and 2) whether any<br />
operational guidance that is issued will apply a uniform operational definition of <strong>Indian</strong> for application<br />
across both Medicaid and the Exchange.<br />
We encourage Exchange officials to seek the flexibility that appears to be available from HHS to fashion<br />
a uniform operational definition of <strong>Indian</strong> to be used across the Medicaid and Exchange-related<br />
programs. 12, 13 This is particularly important given the complexity of “<strong>Indian</strong>” determinations and as the<br />
Affordable Care Act mandated the creation of a streamlined eligibility determination process for<br />
Medicaid and Exchange programs that relies upon a single application form. If it is ultimately determined<br />
that applying a uniform operational definition of <strong>Indian</strong> to each of the <strong>Indian</strong>-specific benefits and<br />
protections is not acceptable to HHS, we recommend that an existing set of guidance materials (namely,<br />
the CMS Medicaid eligibility guidance for AI/ANs under 42 C.F.R. § 447.50) be used as the basis for<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 1 of 16
<strong>Indian</strong> eligibility determinations, with the identification of specific exceptions to these rules when<br />
necessary for any of the <strong>Indian</strong>-specific protections and benefits.<br />
II. Focus of This Paper<br />
v.7, 2012‐09‐23a<br />
This paper is intended to address two core issues of concern. First, the reliance on three different sections<br />
of federal law to define “<strong>Indian</strong>” under the Affordable Care Act has created confusion as to how an<br />
Exchange will implement the definitions for the different ACA protections and benefits that they apply.<br />
(Ironically, because the three definitions are actually nearly identical, the definitions themselves do not<br />
create this confusion.) Second, the Center for Consumer Information and Insurance Oversight<br />
(CMS/CCIIO), an agency within CMS with primary responsibility for ACA implementation, and the<br />
Internal Revenue Service (IRS) need to utilize the knowledge and experience of agencies responsible for<br />
implementing eligibility for <strong>Indian</strong>-specific health benefits prior to enactment of the ACA. The CMS<br />
Center for Medicaid and State Operations (CMS/CMSO), which is responsible for Medicaid operations<br />
including <strong>Indian</strong>-specific Medicaid protections, have developed regulations and materials to provide the<br />
operational guidance to determine who is a “member of an <strong>Indian</strong> tribe” (which is the core element under<br />
each definition of <strong>Indian</strong>) . An Exchange 14 will ultimately learn – as did CMS/CMSO – that they need<br />
detailed guidance materials to assist Federal, Tribal and State officials in determining that a person falls<br />
within the statutory definition of <strong>Indian</strong>. 15<br />
If implementation guidance is not rooted in the CMS/CMSO’s Medicaid experiences, or if no<br />
implementation guidance is provided beyond the definition itself, the results for American <strong>Indian</strong>s and<br />
Alaska Natives are very likely to be a significant number of AI/ANs not gaining access to the benefits and<br />
protections for which they are eligible, as well as disruptions to an otherwise streamlined eligibility<br />
determination and enrollment process. For an Exchange, the results would likely be greater costs and<br />
longer processing times, as well as a heightened error rate among the Exchange staff and outside assisters.<br />
Each of these results would run counter to the expressed goals of the Affordable Care Act. 16<br />
This paper presents options for avoiding these potentially detrimental results when determining eligibility<br />
for <strong>Indian</strong>-specific benefits and protections through an Exchange. We believe the options presented are<br />
within the authority of an Exchange to implement, whether a state-based or Federally-facilitated<br />
Exchange.<br />
III. Background<br />
After a great deal of interaction with tribes, in March of 2012 CMS issued guidance that the two<br />
definitions of <strong>Indian</strong> that apply to Exchange-related protections are “operationally the same.” 17 This<br />
should largely mitigate the confusion generated from having to apply two different sections of federal law<br />
to determine who is eligible for the two <strong>Indian</strong>-specific protections available through an Exchange.<br />
Under each definition, the core criterion is that an <strong>Indian</strong> is “a member of an <strong>Indian</strong> tribe.”<br />
There is general acceptance that all tribes listed by the Bureau of <strong>Indian</strong> Affairs as Federally-recognized<br />
tribes are included in the definition of <strong>Indian</strong> tribe. But this is not the sole determination of which entities<br />
are included under “<strong>Indian</strong> tribe”, as that term is used in each of the statutory provisions cited in the ACA.<br />
In fact, the plain language of these definitions includes no reference to Federally-recognized Tribes.<br />
Instead, the three ACA-cited definitions include a list of entities – in fact the same list with the exception<br />
of the words “pueblo” and “group” not being included in all of the definitions – which includes<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 2 of 16
v.7, 2012‐09‐23a<br />
“organized groups and communities,” including Alaska Native regional and village corporations. Because<br />
it is not readily apparent from a simple read of the definitions which entities are included in the<br />
description of “<strong>Indian</strong> tribes,” IHS and CMS both previously determined – for purposes of determining<br />
eligibility for IHS services and for <strong>Indian</strong>-specific Medicaid protections, respectively – that detailed<br />
guidance was necessary on which entities are included as “<strong>Indian</strong> tribes”, who is considered a “member”<br />
of such <strong>Indian</strong> tribes, and what documentation serves to prove one’s status as an “<strong>Indian</strong>”.<br />
It is important to point out that a basic principle of tribal sovereignty is that tribes can decide who their<br />
members are. This is very similar to the United States government deciding who can be a U.S. citizen.<br />
For the United States as well as for tribes, the definition of a citizen can change over time, 18 and there<br />
may be differences between countries (and tribes) as to what qualifies an individual to be a citizen. For<br />
some tribes, tribal membership confers at a specified age, such as 18. For other tribes, parents may apply<br />
for membership for their children at time of birth. The eligibility guidance issued by IHS and CMS<br />
accommodates such differences in tribal membership/citizenship procedures to ensure that all AI/AN<br />
persons intended by Congress to be eligible for such <strong>Indian</strong>-specific benefits and protections are in fact<br />
included.<br />
To date, for purposes of implementing the <strong>Indian</strong>-specific Exchange-related provisions of the ACA, the<br />
Department of <strong>Health</strong> and Human Services, and by extension CMS, has been reluctant to issue detailed<br />
guidance on the implementation of these definitions, particularly guidance that applies a uniform<br />
operational definition across the Medicaid and Exchange provisions. As expressed by HHS before it<br />
determined that the various statutory provisions cited in the ACA were operationally the same, there was<br />
concern that the ACA-specific definitions of <strong>Indian</strong> 19 might result in different benefits being available to<br />
different individuals because the definitions might cover different individuals. Thus, HHS concluded that<br />
its ability was constrained to apply in toto the operational guidance issued by CMS in the past, which<br />
included individuals eligible under each of the definitions of who is <strong>Indian</strong>.<br />
We understand there may be disagreements between the national tribal organizations and HHS on these<br />
matters. For example, some of the specific categories used for determining eligibility for Medicaid<br />
protections that are included under the CMS operational guidelines may be considered not to be within<br />
the narrower ACA-cited definitions. But, we believe that any exclusions of eligibility categories that may<br />
be required by HHS are identifiable, would be limited, and would enable the remainder of the CMS<br />
guidance to be relied upon for purposes of determining eligibility through an Exchange-facilitated,<br />
streamlined eligibility determination process.<br />
Simultaneously, if determined necessary by HHS and the Administration to do so, a legislative fix could<br />
be pursued with Congress in order to either solidify the application of a uniform operational definition or<br />
to eliminate the need to include specific exceptions to a uniform operational definition.<br />
IV. The ACA References Different Provisions of Federal Law in Defining Persons Eligible for<br />
<strong>Indian</strong>-specific Benefits and Protections<br />
In addition to the health insurance benefits made available to all Americans, including AI/AN, the<br />
Affordable Care Act established additional benefits and protections that are specific to American <strong>Indian</strong>s<br />
and Alaska Natives. Table A presents (1) the <strong>Indian</strong>-specific protections and benefits contained in the<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 3 of 16
v.7, 2012‐09‐23a<br />
ACA, (2) the section of federal law referenced defining eligibility for the provision, and (3) the lead<br />
implementing agency for the provision.<br />
Table A: <strong>Indian</strong>-Specific Provisions of Affordable Care Act<br />
Exchange-related Provisions IRS-related<br />
Special Enrollment<br />
Periods for AI/ANs<br />
Cost-Sharing<br />
Protections for AI/ANs<br />
Section of ACA ACA § 1311(c)(6)(D) ACA § 1402(d)(1) and (2)<br />
Section of federal<br />
law cited that<br />
defines eligibility<br />
for <strong>Indian</strong>-specific<br />
provision<br />
Lead<br />
implementing<br />
agency<br />
Section 4 of IHCIA:<br />
“(D) special monthly<br />
enrollment periods for<br />
<strong>Indian</strong>s (as defined in section<br />
4 of the <strong>Indian</strong> <strong>Health</strong> Care<br />
Improvement Act).”<br />
Exchange (but with option of<br />
deferring to HHS for<br />
eligibility determinations)<br />
Section 4(d) of ISDEAA: 21<br />
“If an individual<br />
enrolled in any qualified<br />
health plan in the individual<br />
market through an Exchange<br />
is an <strong>Indian</strong> (as defined in<br />
section 4(d) of the <strong>Indian</strong><br />
Self-Determination and<br />
Education Assistance<br />
Act (25 USC 450b(d)))…”<br />
Exchange (but with option of<br />
deferring to HHS for<br />
eligibility determinations)<br />
Exemption from<br />
Penalty for Failing to<br />
Maintain Minimum<br />
Essential Coverage<br />
ACA § 1501(b)) creating<br />
IRC 20 § 5000A(e)(3)<br />
Section 45A(c)(6) of the<br />
IRC:<br />
“[A]ny applicable<br />
individual for any month<br />
during which the individual<br />
is a member of an <strong>Indian</strong><br />
tribe (as defined in section<br />
45A(c)(6)”<br />
Internal Revenue Service<br />
Two of the <strong>Indian</strong>-specific protections (special monthly enrollment periods 22 and additional cost-sharing<br />
protections 23 ) are available only to AI/ANs who are enrolled in the individual market through an<br />
Exchange. An Exchange, whether operated by a state or state-established entity or by HHS, has the<br />
responsibility for determining eligibility for these Exchange-related <strong>Indian</strong>-specific provisions, although<br />
an Exchange may rely upon HHS for determinations of eligibility for the premium tax credits and costsharing<br />
assistance as provided for under 45 CFR 155.302(c). A third provision (providing an exemption<br />
from any penalties for AI/ANs who do not maintain minimum essential coverage) is to be administered<br />
by the Internal Revenue Service, 24 We understand there will be coordination between determinations<br />
made by HHS and those that IRS must make, however the mechanics of the working relationship are as<br />
yet unknown to us.<br />
Eligibility for the special monthly enrollment periods is defined in section 4 of the IHCIA. Eligibility for<br />
the cost-sharing protections is defined in section 4(d) of the ISDEAA. Under both provisions, as well as<br />
under the Internal Revenue Code-related definition, an “<strong>Indian</strong>” is defined as a person who is a member<br />
of an <strong>Indian</strong> tribe.<br />
Exchange-related Definitions of <strong>Indian</strong> (IHCIA and ISDEAA) “Operationally Mean the Same Thing”<br />
Shown below is a combined definition of “<strong>Indian</strong> tribe” drawn from the definitions in the IHCIA and the<br />
ISDEAA that are referenced in the Exchange-related provisions. The definition of <strong>Indian</strong> tribe from the<br />
ISDEAA is shown verbatim, with any additional language from the IHCIA definition added and<br />
highlighted in underline.<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 4 of 16
<strong>Indian</strong> tribe means any <strong>Indian</strong> tribe, band, nation, or other organized<br />
group or community, including any Alaska Native village or group or<br />
regional or village corporation as defined in or established pursuant to<br />
the Alaska Native Claims Settlement Act, which is recognized as<br />
eligible for the special programs and services provided by the United<br />
States to <strong>Indian</strong>s because of their status of <strong>Indian</strong>s. 25<br />
v.7, 2012‐09‐23a<br />
As is evident, the definition of an “<strong>Indian</strong> tribe” is nearly identical under each definition, with the<br />
exception that the IHCIA definition includes the phrase “or group” in addition to the language contained<br />
in the ISDEAA definition. This additional phrase creates no functional difference in meaning. It is<br />
understood that the “or group” phrase was included in the IHCIA definition in an attempt to include<br />
redundancies to assure that the definition is comprehensive and not misunderstood. 26<br />
The position that these definitions are effectively and operationally the same is held by national tribal<br />
organizations and advisory bodies, including the Tribal Technical Advisory Group to CMS (TTAG), the<br />
<strong>National</strong> Congress of American <strong>Indian</strong>s (NCAI), the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NIHB), the Tribal<br />
Self-Governance Advisory Committee (TSGAC), and the Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
(NPAIHB), among others. 27 In addition to being the position of these tribal organizations, the opinion that<br />
these two definitions “operationally mean the same thing” is held by the United States Government.<br />
CMS included guidance in the Final Rule on the establishment of Exchanges released in March of 2012.<br />
In the Final Rule, CMS noted:<br />
[S]ince both the ISDEAA and IHCIA operationally mean the same thing,<br />
there is uniformity among the definition of <strong>Indian</strong> for purposes of the<br />
Exchange-related benefits described in this final rule. We accept that the<br />
definitions of ‘‘<strong>Indian</strong>’’ as provided under section 4(d) of ISDEAA<br />
(codified at 25 U.S.C. 450 et seq.) and section 4 of IHCIA (codified at 25<br />
U.S.C. 1603) operationally mean the same thing: an individual who is a<br />
member of an <strong>Indian</strong> tribe. In their definitions of an ‘‘<strong>Indian</strong> tribe,’’ both<br />
of these acts have nearly identical language that refers to a number of<br />
<strong>Indian</strong> entities (tribes, bands, nations, or other organized groups or<br />
communities) that are included in this definition on the basis that they are<br />
“recognized as eligible for the special programs and services provided by<br />
the United States to <strong>Indian</strong>s because of their status as <strong>Indian</strong>s.” 28<br />
An Exchange would be well within the boundaries of this guidance if the Exchange considered persons<br />
who are eligible for the Exchange-related <strong>Indian</strong>-specific special monthly enrollment periods to be<br />
eligible for the Exchange-related <strong>Indian</strong>-specific cost-sharing protections, and vice versa. As such, a<br />
uniform operational definition could be fashioned to guide eligibility determinations for these Exchangerelated<br />
provisions of the ACA.<br />
IRC-related Definition of <strong>Indian</strong>: Providing an Exemption from Potential Tax Penalties<br />
The definition of an <strong>Indian</strong> tribe found in Internal Revenue Code (IRC) § 45A(c)(6) (referenced in the<br />
ACA for purposes of eligibility of <strong>Indian</strong>s for the exemption from the penalty for not maintaining<br />
minimum essential coverage) is also identical to that in the ISDEAA, with one exception.<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 5 of 16
<strong>Indian</strong> tribe means any <strong>Indian</strong> tribe, band, nation, pueblo, or other<br />
organized group or community, including any Alaska Native village or<br />
group or regional or village corporation as defined in or established<br />
pursuant to the Alaska Native Claims Settlement Act, which is<br />
recognized as eligible for the special programs and services provided by<br />
the United States to <strong>Indian</strong>s because of their status of <strong>Indian</strong>s. 29<br />
v.7, 2012‐09‐23a<br />
The IRC § 45A(c)(6) definition includes the word “pueblo”, as in “<strong>Indian</strong> tribe means any <strong>Indian</strong> tribe,<br />
band, nation, pueblo, or other organized group…” (For reference, the phrase “or group” is also shown in<br />
the definition above, although this phrase is only found in the IHCIA Sec. 4 definition.) To further<br />
support the contention that these definitions are not in fact different, dropping the word pueblo from the<br />
definition would not actually exclude pueblos. 30 This again makes the point that the differences among<br />
the three definitions of <strong>Indian</strong> tribe referenced in the ACA are without meaning, especially when one<br />
considers that the HHS regulations implementing the ISDEAA definition actually includes pueblos,<br />
although they are not expressly referenced in the statutory definition. 31<br />
The Internal Revenue Service has not yet formally issued an opinion on this issue. In different meetings<br />
of the Medicare, Medicaid and <strong>Health</strong> Reform Policy Committee of the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>,<br />
representatives of the IRS offered different approaches that IRS may take in consideration of who is<br />
<strong>Indian</strong> for purposes of waiving the tax penalty. On February 21, 2012, IRS representatives indicated that<br />
the IRS likely would accept a determination made by an Exchange as to who is “<strong>Indian</strong>” (in instances<br />
when an individual is certified as being an <strong>Indian</strong> by an Exchange.) 32 If this position holds, a<br />
determination by an Exchange of <strong>Indian</strong> status could be used to indicate eligibility for an exemption from<br />
tax penalties under the ACA, if any. However, it is unrealistic to assume that every AI/AN who files<br />
taxes will go to an Exchange to determine their eligibility for waiver of the tax penalty. Operationally, it<br />
would be very expensive for Exchanges to provide this information for the 1.5 million AI/ANs who are<br />
not expected to enroll in Exchange plans. Furthermore, the Bureau of <strong>Indian</strong> Affairs and Tribes have<br />
been the designated entities to make these determinations long before ACA. The Exchange would only<br />
make a determination if the individual provided the Exchange with documentation from either the BIA or<br />
a Tribe, and that in turn only adds a layer of bureaucracy and works against the concept of “streamlining.”<br />
At a later meeting on July 24, 2012, representatives of the IRS said that the IRS would likely use selfattestation<br />
of <strong>Indian</strong> status on the tax forms as the basis for waiving the penalty.<br />
V. <strong>Indian</strong>-specific Cost-sharing Protections under Medicaid<br />
In 1997, Congress enacted protections for AI/ANs in the Balance Budget Act (BBA). 33 The provision<br />
prevents a state from mandating an AI/AN enroll in a managed care entity if that entity is not an <strong>Indian</strong>specific<br />
entity. Under the BBA provision, an <strong>Indian</strong> is identified as a person meeting the definition in<br />
34, 35<br />
section 4(c) of the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act of 1976 (25 U.S.C. 1603(c)).<br />
In 2008, a second set of <strong>Indian</strong>-specific cost-sharing protections in the Medicaid program were enacted<br />
through the American Recovery and Reinvestment Act of 2009 (ARRA of Recovery Act). 36 These<br />
protections block the imposition of cost-sharing for AI/ANs for items or services furnished by <strong>Indian</strong><br />
health programs, as well prevent a reduction in the amount of payment to an <strong>Indian</strong> health program as a<br />
result of no cost-sharing by AI/AN patients. But in contrast to the BBA and Affordable Care Act<br />
examples, other than indicating that the provision is applicable to “<strong>Indian</strong>s”, a specific definition of <strong>Indian</strong><br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 6 of 16
v.7, 2012‐09‐23a<br />
was not included in the Recovery Act nor was a reference to an existing definition of <strong>Indian</strong> in another<br />
federal statute provided.<br />
In order to provide guidance to states in determining eligibility for the <strong>Indian</strong>-specific Medicaid costsharing<br />
protections under ARRA, HHS promulgated regulations at 42 C.F.R. § 447.50 (effective July 1,<br />
2010) that drew from a range of definitions in federal law to create a single operational definition of<br />
<strong>Indian</strong>. 37 This CMS regulatory guidance drew from the statutory definitions of <strong>Indian</strong> in the IHCIA, the<br />
ISDEAA, and in the Snyder Act, which itself has no definition of <strong>Indian</strong>, but instead is viewed as broad<br />
underlying authority for all <strong>Indian</strong> health programs and other services to AI/ANs. 38 In doing so, “<strong>Indian</strong>”<br />
was defined to mean –<br />
any individual defined at 25 USC 1603(c)[IHCIA Sec. 4(13)], 1603(f)<br />
[IHCIA Sec. 4(28) , or 1679(b) [IHCIA Sec. 809(a)], or who has been<br />
determined eligible as an <strong>Indian</strong>, pursuant to Sec. 136.12 of this part.<br />
This means the individual:<br />
(i) Is a member of a Federally-recognized <strong>Indian</strong> tribe;<br />
(ii) Resides in an urban center and meets one or more of the following<br />
four criteria:<br />
(A) Is a member of a tribe, band, or other organized group of<br />
<strong>Indian</strong>s, including those tribes, bands, or groups terminated since<br />
1940 and those recognized now or in the future by the State in which<br />
they reside, or who is a descendant, in the first or second degree, of<br />
any such member;<br />
(B) Is an Eskimo or Aleut or other Alaska Native;<br />
(C) Is considered by the Secretary of the Interior to be an <strong>Indian</strong> for<br />
any purpose; or<br />
(D) Is determined to be an <strong>Indian</strong> under regulations promulgated by<br />
the Secretary;<br />
(iii) Is considered by the Secretary of the Interior to be an <strong>Indian</strong> for any<br />
purpose; or<br />
(iv) Is considered by the Secretary of <strong>Health</strong> and Human Services to be<br />
an <strong>Indian</strong> for purposes of eligibility for <strong>Indian</strong> health care services,<br />
including as a California <strong>Indian</strong>, Eskimo, Aleut, or other Alaska Native.<br />
To further facilitate the eligibility determination process, CMS issued guidance on the documentation that<br />
may be provided to substantiate meeting the definition of <strong>Indian</strong> under 42 C.F.R. § 447.50.<br />
Documentation that an individual is an <strong>Indian</strong> could include Tribal<br />
enrollment and membership cards, a certificate of degree of <strong>Indian</strong> blood<br />
issued by the Bureau of <strong>Indian</strong> Affairs, a Tribal census document, or a<br />
document issued by a Tribe indicating an individual‘s affiliation with the<br />
Tribe. The <strong>Indian</strong> health care programs and urban <strong>Indian</strong> health programs<br />
are responsible for determining who is eligible to receive an item or<br />
service furnished by their programs and so a medical record card or<br />
similar documentation that specifies an individual is an <strong>Indian</strong> as defined<br />
above could suffice as appropriate documentation. These documents are<br />
examples of documents that may be used, but do not constitute an allinclusive<br />
list of such documents. 39<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 7 of 16
v.7, 2012‐09‐23a<br />
In issuing this guidance, CMS commented, “We agree that administrative simplicity is very important.<br />
Therefore, we have defined the term ‘<strong>Indian</strong>’ for purposes of the exemption from premiums and cost<br />
sharing in broad terms that indicate the kinds of documentation that could support the application of the<br />
exception.” 40<br />
Although CMS did not issue a directive to states to apply § 447.50 uniformly for all <strong>Indian</strong>-specific<br />
Medicaid protections, including the BBA protections, in practice it appears that states and their eligibility<br />
workers may be applying a single definition of <strong>Indian</strong> for both sets of protections. 41 Given the more<br />
extensive operational guidance issued by CMS and a definition that would not result in the exclusion of<br />
persons for whom eligibility was intended, the definition of <strong>Indian</strong> promulgated by HHS under 42 C.F.R.<br />
§ 447.50 appears to be the uniform definition relied upon for Medicaid purposes, including Medicaid<br />
managed care.<br />
VI. Multiple Definitions of <strong>Indian</strong> May Impede <strong>Health</strong> Reform Goals<br />
Given the apparent agreement that the definitions of <strong>Indian</strong> applicable within the Exchange are<br />
operationally the same, the primary issues to resolve are 1) whether operational guidance will be issued to<br />
facilitate implementation of the Exchange-related <strong>Indian</strong>-specific benefits and protections and 2) whether<br />
the definitions of <strong>Indian</strong> under Medicaid and the Exchange will be applied in a uniform manner or with<br />
certain populations excluded under some definitions.<br />
First, what might be the problems created by applying the definitions of <strong>Indian</strong> differently? In short,<br />
applying the definitions of <strong>Indian</strong> differently may impede the central goals of health reform.<br />
A central goal of the Affordable Care Act is the streamlining of eligibility determinations for federal<br />
health insurance programs. 42 The creation of an Exchange serving each state 43 and the requirement that<br />
“the Exchange must use a single streamlined application to determine eligibility and to collect<br />
information necessary for: (1) enrollment… (3) cost-sharing reductions; and (4) Medicaid…” 44 are two<br />
primary means for achieving the streamlining of eligibility determinations. 45 But if an Exchange were<br />
required to apply different definitions of <strong>Indian</strong> when making eligibility determinations for Medicaid and<br />
Exchange-related programs – even if those definitions had very little difference in practice – the efforts at<br />
streamlining eligibility determinations could be significantly frustrated. Results of this would be likely to<br />
include –<br />
Increased inaccuracies in eligibility determinations: Enrollment staff, as well as AI/ANs<br />
themselves, could become confused – and ultimately frustrated – if they are required to<br />
understand obscure differences between the definitions. Without a thorough understanding of<br />
any differences in the application of the definitions, instances of inaccurate eligibility<br />
determinations being made are likely to increase. 46<br />
Unwarranted application of tax penalties: If an AI/AN were determined to be eligible for IHS<br />
services as an “<strong>Indian</strong>” (and therefor chose not to secure health insurance coverage), but was not<br />
determined to be eligible as an “<strong>Indian</strong>” for the exemption from the requirement to secure<br />
minimum essential coverage, this individual and his or her family could be subject to significant<br />
tax penalties.<br />
Interruption of streamlined process: Applying definitions differently will lead to individuals<br />
needing to interact with Exchange/Medicaid eligibility staff and tribal offices on multiple<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 8 of 16
v.7, 2012‐09‐23a<br />
occasions as they navigate understanding the differences in the definitions and the different<br />
documents that might satisfy one definition but not another.<br />
Increased training necessary: If enforcement of multiple definitions of <strong>Indian</strong> were required to be<br />
carried out by an Exchange, enrollment staff of an Exchange and individuals and organizations<br />
involved in outreach to AI/AN 47 would need to be educated in the nuances under each definition<br />
of <strong>Indian</strong>, including understanding the differences, if any, in documentation permitted to satisfy<br />
each definition of <strong>Indian</strong>.<br />
Increased and uncertain cost-sharing liabilities: AI/ANs determined to be “<strong>Indian</strong>” for purposes<br />
of Medicaid will be afforded comprehensive <strong>Indian</strong>-specific cost-sharing protections under<br />
Medicaid. However, if the same individuals’ income increases and the individuals are then<br />
eligible for Exchange coverage and not Medicaid, they are likely to assume they are eligible for<br />
the comprehensive <strong>Indian</strong>-specific cost-sharing protections through the Exchange. If the<br />
Exchange determines that such individuals are not eligible for cost-sharing waivers on the basis<br />
of AI/AN status, this will become very confusing to both the individuals and the QHP.<br />
Uncertainty in the applicability of cost-sharing protections could result in significant liabilities to<br />
the affected individuals without their having the slightest awareness of this discrepancy.<br />
Uncertain application of cost-sharing protections within families by providers: Providers that<br />
serve AI/ANs, and do not collect cost-sharing for the AI/ANs because of their status of being an<br />
<strong>Indian</strong> for purposes of the Medicaid program, would need to understand that patients’ status as an<br />
<strong>Indian</strong> – or the status of just some of the members of an AI/AN household – might have changed<br />
when they secured health insurance coverage through an Exchange. The provider would then<br />
need to collect cost-sharing from some or all members of a previously “<strong>Indian</strong>” household.<br />
Reduced timeliness: The streamlined application process is being designed to rely, to the extent<br />
possible, on electronic verification of application-related information. The lack of a single<br />
operational definition would complicate (although not prevent) the use of automated databases<br />
that may be available for verification purpose, such as using the IHS beneficiary roster.<br />
Reduced involvement of AI/AN in insurance options: Even if the instances of an individual<br />
being determined to be “<strong>Indian</strong>” for one Exchange-related provision and not for another were rare<br />
(which we anticipate), this outcome would likely cast a shadow over AI/ANs involvement with<br />
ACA implementation more generally. For instance, AI/ANs may be much more reluctant to<br />
transition from the IHS-based coverage model to comprehensive Exchange coverage if they could<br />
end-up subject to significant cost-sharing requirements under a different, potentially unknown<br />
application of a definition of <strong>Indian</strong>.<br />
Individually and collectively, these results would run directly counter to the central goal of the ACA to<br />
expand access to affordable health insurance coverage for all Americans. And, these results could<br />
seriously impede the specific policy declarations of the United States Congress contained in ACA §<br />
10221(a) 48 for AI/ANs that:<br />
Congress declares that it is the policy of this Nation, in fulfillment of its special<br />
trust responsibilities and legal obligations to <strong>Indian</strong>s—<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 9 of 16
(1) to ensure the highest possible health status for <strong>Indian</strong>s and urban <strong>Indian</strong>s<br />
and to provide all resources necessary to effect that policy;<br />
…<br />
(3) to ensure maximum <strong>Indian</strong> participation in the direction of health care<br />
services so as to render the persons administering such services and the<br />
services themselves more responsive to the needs and desires of <strong>Indian</strong><br />
communities;<br />
…<br />
VII. Addressing the Problem: Why a Uniform Operational Definition of <strong>Indian</strong> is Needed and<br />
Potentially Permitted<br />
v.7, 2012‐09‐23a<br />
To ensure AI/ANs are able to access the Medicaid and Exchange-related special benefits and protections<br />
that they are statutorily entitled to, and Exchanges are able to efficiently and consistently make accurate<br />
eligibility determinations, it is critical that – to the greatest extent possible – a uniform operational<br />
definition of “<strong>Indian</strong>” be employed.<br />
For purposes of determining eligibility for ARRA-enacted <strong>Indian</strong>-specific Medicaid cost-sharing<br />
provisions, HHS fashioned a single operational definition of <strong>Indian</strong> that was inclusive of the existing<br />
definitions of <strong>Indian</strong> contained in federal law. In the same manner, fashioning such an operational<br />
definition for purposes of the Medicaid and Exchange-related eligibility determinations would enable an<br />
Exchange to carry-out the requirements established for an Exchange (e.g., to conduct a streamlined<br />
eligibility determination process using a single application form) in an efficient and accurate manner.<br />
More specifically, extending the 42 C.F.R. § 447.50 guidance that was developed for <strong>Indian</strong>-specific<br />
Medicaid eligibility determinations as the uniform operational definition for both Medicaid and<br />
Exchange-related eligibility determinations would provide such uniformity of definition.<br />
In the Final Rule on the establishment of Exchanges which was promulgated on March 27, 2012, HHS<br />
may have offered states the flexibility to apply such a uniform operational definition of <strong>Indian</strong>. 49<br />
States Offered Flexibility in the Application and Verification of Definitions of <strong>Indian</strong><br />
In response to comments submitted to HHS regarding the definition of <strong>Indian</strong> and verification of an<br />
individual’s status as an <strong>Indian</strong>, the following guidance was included in the preamble to the Final Rule:<br />
We are maintaining the verification process described under § 155.350 in<br />
this final rule. This verification is tied to a full exemption from costsharing,<br />
which could involve a substantial expenditure for the Federal<br />
government; consequently, we are specifying a more stringent process<br />
for verification though we note that § 155.315(h) allows the Exchange<br />
flexibility to modify this and other verification processes with HHS<br />
approval. In addition, we note that the documentation process described<br />
under § 155.350(c)(3) is similar to the documentation process utilized by<br />
the IHS when determining eligibility for American <strong>Indian</strong>s/Alaska<br />
Natives who seek services at IHS facilities. 50 (Underline added.)<br />
In this response, HHS indicated that verification of <strong>Indian</strong> status would be required (and a simple<br />
attestation would not suffice), but the Exchange is afforded discretion in how it conducts the eligibility<br />
verification.<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 10 of 16
v.7, 2012‐09‐23a<br />
The Final Rule response continued with the following, indicating that CMS recognizes that even the<br />
definitions of <strong>Indian</strong> with the potentially greatest variance are still only “slightly different.”<br />
The [<strong>Indian</strong> eligibility] standard for Exchanges is slightly different from the<br />
[<strong>Indian</strong> eligibility] standard for such [IHS] services, however, which means that<br />
the registration database for <strong>Indian</strong> Tribe, Tribal Organization, or Urban <strong>Indian</strong><br />
Organization programs may not be a one-to-one match. With that in mind, we are<br />
working closely with the IHS and intend to work with States and tribes to<br />
determine whether and how electronic data can support this process. 51<br />
As referenced above, the definition used to determine eligibility for IHS services (which most closely<br />
resembles the CMS § 447.50 Medicaid eligibility guidance) has the most inclusive definition of <strong>Indian</strong>,<br />
and the Exchange-related definitions may be considered the most restrictive. 52 But still, these definitions<br />
are considered only “slightly different”.<br />
The language of 45 C.F.R. § 155.315(h) cited above which provides flexibility to Exchanges in<br />
implementation of eligibility determination processes, reads as follows:<br />
§ 155.315 (h) Flexibility in information collection and verification. HHS may<br />
approve an Exchange Blueprint in accordance with § 155.105(d) or a significant<br />
change to the Exchange Blueprint in accordance with § 155.105(e) to modify the<br />
methods to be used for collection of information and verification of information<br />
as set forth in this subpart, as well as the specific information required to be<br />
collected, provided that HHS finds that such modification would reduce the<br />
administrative costs and burdens on individuals while maintaining accuracy and<br />
minimizing delay, that it would not undermine coordination with Medicaid and<br />
CHIP, and that applicable requirements under § 155.260, § 155.270, paragraph<br />
(i) of this section, and section 6103 of the Code with respect to the<br />
confidentiality, disclosure, maintenance, or use of such information will be met. 53<br />
(Underline added.)<br />
As indicated, central to HHS approving a request by an Exchange for flexibility authorized under 45<br />
C.F.R. § 155.315(h) is a determination that “HHS finds that such modification would reduce the<br />
administrative costs and burdens on individuals while maintaining accuracy and minimizing delay, that it<br />
would not undermine coordination with Medicaid and CHIP…” Given the number of definitions of<br />
“<strong>Indian</strong>” involved and the nuanced differences across the definitions, the threshold requirements for<br />
applying the § 155.315(h) authority would seem to be readily satisfied if an Exchange were to rely upon a<br />
uniform operational definition of <strong>Indian</strong>, such as using the § 447.50 guidance from CMS, when<br />
determining eligibility for the Medicaid and Exchange-related <strong>Indian</strong>-specific provisions.<br />
A uniform operational definition would seem likely to result in –<br />
Administrative costs on state Exchanges being lessened;<br />
Paperwork burdens on individual AI/ANs being reduced;<br />
The overall accuracy and consistency of eligibility determinations across Medicaid and ACArelated<br />
provisions being increased;<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 11 of 16
v.7, 2012‐09‐23a<br />
Delays in accessing the special benefits and protections afforded AI/ANs through the Affordable<br />
Care Act being reduced;<br />
The seamless coordination between Medicaid and Exchange-related programs being furthered;<br />
Participation by AI/ANs in the Exchange-related programs being heightened; and<br />
Clarity across providers and QHPs in the application of <strong>Indian</strong>-specific benefits and protections<br />
would be enhanced.<br />
If it is ultimately determined that full uniformity across the application of the definitions of <strong>Indian</strong> to each<br />
<strong>Indian</strong>-specific provision cannot be achieved, we strongly recommend that Exchanges use the CMS<br />
guidance on eligibility and documentation provided under § 447.50 as the base for <strong>Indian</strong>-specific<br />
eligibility determinations and identify specific exceptions (i.e., exclusions) from eligibility, as needed, for<br />
any particular <strong>Indian</strong>-specific provision.<br />
VIII. Conclusion<br />
We encourage Exchange officials – whether operated by a state or HHS – to seek the flexibility that<br />
appears to be available under the Affordable Care Act and its implementing regulations to fashion a<br />
uniform operational definition of <strong>Indian</strong> to be used across the Medicaid and Exchange-related programs in<br />
order to be able to carry-out a streamlined eligibility determination process using a single application<br />
form, with the result being eligibility determinations conducted more efficiency and more accurately.<br />
Previous eligibility guidance issued by CMS could be relied upon to implement the uniform operational<br />
definition.<br />
If it is determined that applying a single operational definition of <strong>Indian</strong> to each of the <strong>Indian</strong>-specific<br />
benefits and protections is not agreed to by HHS, we recommend that an existing set of guidance<br />
materials (namely the CMS Medicaid eligibility guidance for AI/ANs under 42 C.F.R. § 447.50) be used<br />
as the basis for <strong>Indian</strong> eligibility determinations with specific exceptions to these rules identified where<br />
necessary.<br />
As stated previously, national and regional tribal organizations support the application of a uniform<br />
operational definition of <strong>Indian</strong> for purposes of implementing the provisions of the Affordable Care Act.<br />
These include NCAI, NIHB, TTAG, TSGAC and NPAIHB. 54 These organizations believe that providing<br />
a uniform definition will ultimately lead to advances in the health status of AI/ANs by more effectively<br />
matching available resources to the needs of eligible AI/AN individuals. We stand ready to continue to<br />
work with state and federal Exchange officials to make the determination of <strong>Indian</strong> status an efficient and<br />
effective process.<br />
1 For a more detailed exposition of the issue of the definition of an <strong>Indian</strong>, see “Tribal Technical Advisory Group to<br />
CMS, Analysis of and Comment on Definition of ‘<strong>Indian</strong>’ in Proposed Rules to Implement Provisions of the Patient<br />
Protection and Affordable Care Act,” October 31, 2011, submitted to CMS and the IRS. (“TTAG Analysis”)<br />
2<br />
A separate paper will be prepared by Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (“NPAIHB”) discussing<br />
verification materials for documenting <strong>Indian</strong> status.<br />
3<br />
The <strong>Indian</strong> <strong>Health</strong> Care Improvement Act (“IHCIA”), Pub. L. 94-347, was permanently reauthorized and amended<br />
March 23, 2010, by § 10221(a) of the ACA. IHCIA § 103 reads, in part:<br />
Congress declares that it is the policy of this Nation, in fulfillment of its special<br />
trust responsibilities and legal obligations to <strong>Indian</strong>s—<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 12 of 16
v.7, 2012‐09‐23a<br />
(1) to ensure the highest possible health status for <strong>Indian</strong>s and urban <strong>Indian</strong>s and<br />
to provide all resources necessary to effect that policy;<br />
(2) to raise the health status of <strong>Indian</strong>s and urban <strong>Indian</strong>s to at least the levels set<br />
forth in the goals contained within the <strong>Health</strong>y People 2010 initiative or<br />
successor objectives;<br />
(3) to ensure maximum <strong>Indian</strong> participation in the direction of health care<br />
services so as to render the persons administering such services and the services<br />
themselves more responsive to the needs and desires of <strong>Indian</strong> communities;<br />
(4) to increase the proportion of all degrees in the health professions awarded to<br />
<strong>Indian</strong>s so that the proportion of <strong>Indian</strong> health professionals in each Service area<br />
is raised to at least the level of that of the general population;<br />
(5) to require that all actions under this Act shall be carried out with active and<br />
meaningful consultation with <strong>Indian</strong> tribes and tribal organizations, and<br />
conference with urban <strong>Indian</strong> organizations, to implement this Act and the<br />
national policy of <strong>Indian</strong> self-determination;<br />
(6) to ensure that the United States and <strong>Indian</strong> tribes work in a government-togovernment<br />
relationship to ensure quality health care for all tribal members; and<br />
(7) to provide funding for programs and facilities operated by <strong>Indian</strong> tribes and<br />
tribal organizations in amounts that are not less than the amounts provided to<br />
programs and facilities operated directly by the Service.<br />
4<br />
The Patient Protection and Affordable Care Act (Pub. L. 111-148) as amended by the <strong>Health</strong> Care and Education<br />
Reconciliation Act of 2010 (Pub. L. 111-152), are collectively referred to herein as the “Affordable Care Act” or<br />
“ACA”.<br />
5<br />
<strong>Health</strong> insurance exchanges (“Exchanges”) are to be available by October 1, 2013 in each State in order to allow<br />
enrollment in new health insurance coverage options effective January 1, 2014. Exchanges are marketplaces for the<br />
offering of health insurance coverage, mechanisms for determining eligibility for various government health<br />
insurance programs, and vehicles for securing government assistance, if eligible, with covering all or a portion of the<br />
health insurance plan monthly premiums.<br />
6<br />
ACA § 1501(b) / IRC § 5000A(e)(3).<br />
7<br />
See Federal Register, March 27, 2012, CMS, “Patient Protection and Affordable Care Act; Establishment of<br />
Exchanges and Qualified <strong>Health</strong> Plans,” (CMS-9989-F), Vol. 77, No. 59, page 18346. (“Final Rule”) The<br />
Department of <strong>Health</strong> and Human Services (HHS) and CMS did not opine on the definition of <strong>Indian</strong> pertaining to<br />
the exemption from tax penalties afforded AI/ANs under ACA § 1501(b) as it falls within the Internal Revenue<br />
Code. (See IRC § 5000A(e)(3).) CMS did determine that the two Exchange-related definitions (contained in the<br />
IHCIA and the <strong>Indian</strong> Self-Determination and Education Assistance Act) “operationally mean the same thing.”<br />
8<br />
The position that these definitions are effectively and operationally the same is also held by numerous tribes and<br />
tribal organizations, including the <strong>National</strong> Congress of American <strong>Indian</strong>s (“NCAI”), the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong><br />
<strong>Board</strong> (“NIHB”), the Tribal Technical Advisory Group to CMS (“TTAG”), the Tribal Self-Governance Advisory<br />
Committee (“TSGAC”), and the Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NPAIHB”), among others.<br />
9<br />
In a meeting of the Medicare, Medicaid and <strong>Health</strong> Reform Policy Committee of the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
on February 21, 2012, IRS representatives indicated that the IRS likely would defer to the uniform determination<br />
made by an Exchange as to who is “<strong>Indian</strong>” and as such qualifies for an exemption from tax penalties under the<br />
ACA.<br />
10<br />
These cost-sharing protections for AI/ANs include those established under § 5006 of the American Reinvestment<br />
and Recovery Act of 2009, Pub. L. 111-5 and those enacted as part of the Balanced Budget Act of 1997 (Social<br />
Security Act § 1932(a)(2)(C).)<br />
11<br />
See 42 C.F.R. § 447.50, promulgated May 28, 2010. In particular, these regulations drew from the definitions of<br />
<strong>Indian</strong> in the Snyder Act, the IHCIA, and the <strong>Indian</strong> Self-Determination and Education Assistance Act<br />
(“ISDEAA”). A second set of <strong>Indian</strong>-specific Medicaid protections was enacted in the Balanced Budget Act of<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 13 of 16
v.7, 2012‐09‐23a<br />
1997. The provision amended section 1932(a)(2)(C) of the Social Security Act and is codified at 42 U.S.C. 1396u-<br />
2(a)(2)(C), with regulations issued at 42 C.F.R. § 438.50(d)(2).<br />
12<br />
See discussion in the Final Rule at 77 Fed. Reg. 18383; and see 45 C.F.R. § 155.315(h) “Flexibility in information<br />
collection and verification” at Final Rule, 77 Fed. Reg. 18455.<br />
13<br />
Again, the range of <strong>Indian</strong>-specific eligibility determinations include the cost-sharing and monthly enrollment<br />
protections in the individual market through an Exchange, eligibility for Medicaid cost-sharing and managed care<br />
protections, and the exemption from penalties for AI/AN not securing minimum essential coverage.<br />
14<br />
This issue is of concern under state-based Exchanges as well as the Federally-facilitated Exchange (FFE).<br />
15 While these regulations and other materials demonstrate that the statutory definitions can be reconciled, mere<br />
restatement of the statutory language is not sufficient to facilitate accurate eligibility determinations.<br />
16 See Federal Register, Vol. 75, No. 148, August 3, 2010, Request for Comments, “Planning and Establishment of<br />
State-Level Exchanges,” Section G. Enrollment and eligibility, Office of Consumer Information and Insurance<br />
Oversight, HHS, page 45588, which includes “additional requirements to assist Exchanges by… simplifying and<br />
coordinating enrollment in the Exchanges, Medicaid and the Children’s <strong>Health</strong> Insurance Program (CHIP).”<br />
17 77 Federal Register 18346.<br />
18<br />
For example, on October 30, 2000, President Clinton signed into law H.R. 2883, the Child Citizenship Act of<br />
2000. The new law, Public Law 106-395, amends the Immigration and <strong>National</strong>ity Act (INA) to permit foreign-born<br />
children — including adopted children — to acquire citizenship automatically and immediately if they meet certain<br />
requirements, rather than having citizenship conferred only after an application process is completed. This law<br />
became effective on February 27, 2001.<br />
19<br />
ACA § 1311(c)(6)(D) referring to section 4 of the IHCIA and codified at 25 U.S.C. 1603; ACA § 1402(d)(1) and<br />
(2) referring to section 4(d) of the ISDEAA and codified at 25 U.S.C. 450 et seq.; and ACA § 1501(b)) creating<br />
IRC § 5000A(e)(3) which refers to section 45A(c)(6) of the Internal Revenue Code.<br />
20<br />
The Internal Revenue Code.<br />
21 The ISDEAA, Pub. L. 93-638.<br />
22<br />
The special monthly enrollment periods are described in 45 C.F.R. § 155.420(d)(8). An AI/AN may enroll in a<br />
health plan or change from one health plan to another one time per month.<br />
23<br />
See ACA § 1402(d)(1) and (2). The additional cost-sharing protections are described in 45 C.F.R. § 155.300(a)<br />
and (b)). Under ACA § 1402(d)(1), the cost-sharing protections encompass a waiver of all cost-sharing for an<br />
AI/AN individual whose household income is not more than 300 percent of the Federal poverty level. Under ACA §<br />
1402(d)(2), there is no cost-sharing for an AI/AN individual of any income level when furnished an item or service<br />
directly or through referral by an <strong>Indian</strong> <strong>Health</strong> Care Provider. “<strong>Indian</strong> <strong>Health</strong> Care Providers” are comprised of the<br />
<strong>Indian</strong> <strong>Health</strong> Service, Tribes and tribal organizations, and urban <strong>Indian</strong> organizations. Collectively, these entities<br />
are also sometimes referred to as “I/T/U”. The <strong>Indian</strong> <strong>Health</strong> Service means the agency of that name within the U.S.<br />
Department of <strong>Health</strong> and Human Services (“HHS”) established by IHCIA § 601 (25 USC §1661). The terms<br />
“<strong>Indian</strong> tribe,” “tribal organization,” and “UIO” have the meaning given those terms in IHCIA § 4 (25 USC §1603).<br />
The issuer of a health plan shall not reduce the payment to an <strong>Indian</strong> <strong>Health</strong> Care Provider by the amount of any<br />
cost-sharing that would be due from an AI/AN but for this provision. The Secretary of HHS is to pay to the health<br />
plan the amount necessary to reflect the increase in actuarial value of the plan required by reason of this provision.<br />
24<br />
The determination of eligibility for this exemption is not within the functions of an Exchange. The IRS has<br />
responsibility for implementing this <strong>Indian</strong>-specific protection, which is found in IRC § 5000A(e)(3) and waives the<br />
penalties for AI/ANs who do not maintain minimum essential coverage, although the IRS may rely upon an<br />
Exchange’s determination of who is <strong>Indian</strong> for those individuals who have been determined to be “<strong>Indian</strong>” for<br />
purposes of Exchange-related provisions.<br />
25<br />
Wording contained in IHCIA Sec. 4(14) and ISDEAA Sec. 4(d), except that the double underlined words (“or<br />
group”) are only contained in IHCIA Sec. 4(14).<br />
26<br />
See TTAG Analysis, page 6.<br />
27<br />
TTAG October 2010; NCAI Res. # ABQ-10-080, November 2010, NIHB Res. 10-01, October 2010; TSGAC<br />
February 2011; and NPAIHB, October 21, 2010.<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 14 of 16
28 Final Rule, 77 Fed. Reg. 18346.<br />
v.7, 2012‐09‐23a<br />
29<br />
Wording contained in IHCIA § 4(14), ISDEAA § 4(d), and IRC § 45A(c)(6), except that the underlined word<br />
(“pueblo”) is only contained in IRC § 45A(c)(6) and the double underlined words (“or group”) are only contained in<br />
IHCIA Sec. 4(14).<br />
30<br />
This is the result because pueblos are also considered to be <strong>Indian</strong> Tribes, nations, organized groups, and<br />
communities recognized as eligible for the special programs and services provided by the United States to <strong>Indian</strong>s<br />
because of their status of <strong>Indian</strong>s.<br />
31<br />
25 C.F.R. § 900.6 (HHS and Department of the Interior (―DOIǁ) Title I), 25 C.F.R. § 1000.2 (DOI Title IV), 42<br />
C.F.R. § 137.10 (Title V). These regulatory definitions also include ―rancherias and colonies.<br />
32<br />
A significant percentage of American <strong>Indian</strong>s and Alaska Natives that seek an exemption from the tax penalties<br />
may not engage an Exchange as the AI/AN individuals may have determined not to pursue health insurance<br />
coverage. For these individuals, it is assumed attestations would be made and/or documentation would be provided<br />
directly to the IRS.<br />
33<br />
Public Law 105-33. The primary protection established is “A State may not require… the enrollment in a<br />
managed care entity of an individual who is an <strong>Indian</strong> (as defined in section 4(c) of the <strong>Indian</strong> <strong>Health</strong> Care<br />
Improvement Act of 1977 of 1976 (25 U.S.C. 1603(c)) unless the entity is one of the following [<strong>Indian</strong><br />
organizations] (and only if such entity is participating under the plan)… ”<br />
34<br />
For purposes implementing the protections afforded AI/AN in the Balanced Budget Act of 1997, see 42 C.F.R. §<br />
438.50(d)(2).<br />
35<br />
In referencing subsection (c) of section 4 of the IHCIA, this definition of <strong>Indian</strong> is more restrictive than the<br />
reference to “<strong>Indian</strong>” under the IHCIA for purposes of the special monthly enrollment period for AI/ANs enrolled in<br />
the individual market through an Exchange (authorized under ACA § 1311(c)(6)(D)).<br />
36<br />
These cost-sharing protections for AI/ANs were established under § 5006 of the American Reinvestment and<br />
Recovery Act of 2009, Pub. L. 111-5.<br />
37<br />
See 42 C.F.R. § 447.50, promulgated May 28, 2010.<br />
38<br />
The Snyder Act is the primary statute authorizing the Federal government to provide health care to <strong>Indian</strong>s and<br />
implementing the unique Federal obligations to <strong>Indian</strong>s. It directs and authorizes HHS to “direct, supervise, and<br />
expend such moneys as Congress may from time to time appropriate, for the benefit, care, and assistance of the<br />
<strong>Indian</strong>s throughout the United States” for the “relief of distress and conservation of health.” 25 U.S.C. § 13.<br />
39<br />
Medicaid Program; Premiums and Cost Sharing, 75 Fed. Reg., No. 103, pp. 30, 244, 30,248 (May 28, 2010).<br />
40<br />
Medicaid Program; Premiums and Cost Sharing, 75 Fed. Reg., No. 103, p. 30247.<br />
41<br />
For example, in a recent Section 1115 waiver application from the State of Kansas, a single operational definition<br />
of <strong>Indian</strong> was applied to both sets of <strong>Indian</strong>-specific Medicaid protections.<br />
42<br />
Federal Register, Vol. 75, No. 148, August 3, 2010, Request for Comments, “Planning and Establishment of<br />
State-Level Exchanges,” Section G. Enrollment and eligibility, Office of Consumer Information and Insurance<br />
Oversight, HHS, page 45588.<br />
43<br />
ACA § 1311 and 45 C.F.R. § 155.100.<br />
44<br />
ACA § 1413(b) and 45 C.F.R. § 155.405(a). “CHIP” refers to the Children’s <strong>Health</strong> Insurance Program under<br />
title XXI of the Social Security Act.<br />
45<br />
An additional approach to streamlining eligibility across federal programs is the implementation of a common<br />
methodology (“modified adjusted gross income”) for determining household income, as authorized by ACA § 1401<br />
/ IRC § 36B(d)(2)(B).<br />
46<br />
Conversely, as it appears to occur today under Medicaid, to simplify implementation a state or a subset of<br />
Exchange/Medicaid eligibility staff in a state might default to applying one definition for all <strong>Indian</strong>-specific<br />
purposes in a state. AI/ANs applying on one occasion or in one state may be found to be eligible whereas the same<br />
AI/ANs would be found to be ineligible on another occasion or in another state, or vice versus.<br />
47<br />
Such as grantees under the Navigator program authorized under ACA § 1311(i) or “in-person assisters”. See 45<br />
C.F.R. § 155.210.<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 15 of 16
v.7, 2012‐09‐23a<br />
48<br />
Enacted through the passage of the ACA, Congress made the declarations of national <strong>Indian</strong> health policy in<br />
IHCIA § 103.<br />
49<br />
See discussion in the Final Rule at 77 Fed. Reg. 18383; and see 45 C.F.R. § 155.315(h) “Flexibility in information<br />
collection and verification” at Final Rule, 77 Fed. Reg. 18455.<br />
50<br />
Final Rule, 77 Fed. Reg. 18383.<br />
51<br />
Final Rule, 77 Fed. Reg. 18383.<br />
52<br />
An additional definition is used for purposes of determining eligibility for services through the <strong>Indian</strong> <strong>Health</strong><br />
Service, although this generally aligns with the guidance under 42 C.F.R. § 447.50.<br />
53<br />
Final Rule, 77 Fed. Reg. 18455.<br />
54<br />
NCAI Res. # ABQ-10-080, November 2010, NIHB Res. 10-01, October 2010; TTAG October 2010; TSGAC<br />
February 2011; and NPAIHB, October 21, 2010.<br />
Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 16 of 16
[Type text] [Type text] [Type text]<br />
CALIFORNIA RURAL INDIAN HEALTH BOARD<br />
ANALYSIS OF MEDICAID<br />
PAYMENTS FOR<br />
AMERICAN INDIANS &<br />
ALASKA NATIVES<br />
Centers for Medicare and Medicaid Services:<br />
American <strong>Indian</strong> & Alaska Native Data Project<br />
FEEDBACK DRAFT for the Tribal Technical Advisory Group<br />
C M S T R I B A L A F F A I R S G R O U P<br />
2012
Prepared by<br />
James Crouch MPH Chair, CMS TTAG Data Subcommittee<br />
and Carol Korenbrot PhD<br />
California Rural <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Inc.<br />
Funded by<br />
The Centers for Medicare and Medicaid (CMS) Tribal Affairs Group through the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong><br />
<strong>Board</strong> pursuant to an award from the <strong>Indian</strong> <strong>Health</strong> Service (IHS), following an intra-departmental<br />
delegation of authority (CMS IDDA-09-50 and IHS 2-RAP-09-0080-DA).<br />
Please provide feedback to:<br />
California Rural <strong>Indian</strong> Heath <strong>Board</strong> (CRIHB)<br />
Phone: 916.929.9761<br />
Fax: 916.929.7246<br />
Email: carol.korenbrot@crihb.net
Contents<br />
SUMMARY I<br />
Findings .......................................................................................................................................................................................................... ii<br />
Conclusions and Recommendations .................................................................................................................................................. iii<br />
INTRODUCTION 1<br />
Purpose of this Report .............................................................................................................................................................................. 2<br />
METHODS 3<br />
Data Sources ................................................................................................................................................................................................. 3<br />
Medicaid-IHS Linked Person Summary File ............................................................................................................................... 3<br />
Medicaid Inpatient, Prescription Drug and Other Services Claims Files ........................................................................ 3<br />
Analysis Groups ........................................................................................................................................................................................... 4<br />
IHS AIAN .................................................................................................................................................................................................... 4<br />
Other AIAN ............................................................................................................................................................................................... 5<br />
Whites (Non-Hispanic) ........................................................................................................................................................................ 5<br />
Analysis Plan ................................................................................................................................................................................................. 6<br />
Outcome of Analysis: Mean Total Payment per Medicaid Recipient ................................................................................ 6<br />
Determinants of the Outcome .......................................................................................................................................................... 7<br />
Statistical Adjustments ........................................................................................................................................................................... 15<br />
FINDINGS 19<br />
Payments for AIAN Medicaid Recipients ........................................................................................................................................ 19<br />
Recipients with Fee-for-Service Medical Services ................................................................................................................. 19<br />
Recipients in Medical Comprehensive Managed Care Plans (CMCP) ............................................................................. 28<br />
Compiled Findings for All Analyses and Areas ........................................................................................................................ 32<br />
Medicaid Paid Fraction of Total <strong>Health</strong> Care Costs of IHS Active Users ............................................................................ 37<br />
IHS Calculated <strong>Health</strong> Care Costs for IHS Active Users ........................................................................................................ 37<br />
Medicaid Fraction of IHS Active User <strong>Health</strong> Care Costs ..................................................................................................... 38<br />
Medicaid Fraction Paid to IHS and Tribal Providers for IHS Active Users ................................................................... 39<br />
CONCLUSIONS AND RECOMMENDATIONS ..................................................................................................................................... 41<br />
IHS AIAN Payments Compared to Others ....................................................................................................................................... 41<br />
Medicaid-enrolled IHS Active Users without IHS Program Medicaid claims .................................................................. 42<br />
Medicaid-paid Fraction of IHS Active User Costs ........................................................................................................................ 42<br />
REFERENCES 43
Summary<br />
T<br />
he <strong>Indian</strong> <strong>Health</strong> Service (IHS) provides only part of the health care needed by the American <strong>Indian</strong>s and<br />
Alaska Natives (AIAN) who rely on the IHS health care system because of the limited funding<br />
appropriated to the agency by the federal budget. The largest alternate resource to IHS for the health<br />
care funding of AIAN who rely on the IHS health care system is Medicaid. Medicaid pays for care received<br />
not only at the IHS and tribally operated health care facilities, but from other providers when specialized or<br />
emergency care is needed. The federal Medicaid program pays 100% of state Medicaid claims from IHS health<br />
care system providers for IHS funded services provided to AIAN (IHS Program claims). Together with its<br />
companion program, the Children’s <strong>Health</strong> Insurance Program (CHIP), Medicaid has grown to provide a<br />
substantial but largely unknown fraction of the coverage of health care for the AIAN who use the IHS system.<br />
The first objective of this report to determine whether Medicaid (including the Medicaid portion of CHIP not<br />
operated by states alone) pays as much for the personal health care services of AIAN who rely on the IHS system<br />
of health care providers (IHS AIAN) as it does for other Medicaid recipients. If the per capita amounts paid for<br />
the IHS AIAN are comparable to those of others, then a basic measure of health care equity for AIAN served by<br />
the IHS system has been achieved. If not then efforts are needed to achieve equity.<br />
A second objective is to determine whether there are any Areas of the IHS health care delivery system, or<br />
subgroups of AIAN who rely on the IHS system that do not have Medicaid payment levels as high as those of<br />
other AIAN subgroups served by the IHS System. Where the payment levels for IHS AIAN are not as high as<br />
those of others in an Area, it can be because IHS AIAN have more difficulties obtaining Medicaid paid care, or<br />
because the state and IHS system provider need to work more closely to see that Medicaid claims are filed and<br />
paid successfully. If IHS system providers do not file and collect claims for services provided to Medicaid<br />
enrolled AIAN they serve, they are in effect substituting IHS funding for Medicaid funding of health care costs. In<br />
this report, analyzing only the Medicaid data of the counties of the IHS Areas allows comparison of payments<br />
across IHS Areas and using Medicaid data that has been linked with IHS registry data allows examination of<br />
AIAN subgroups served by the IHS System.<br />
A third objective of this report is to determine what fraction of the personal health care costs of the AIAN user<br />
population of the IHS system is actually provided by Medicaid payments. The IHS has current data on the<br />
Medicaid collections of the IHS and tribal facilities that they operate, but not the tribal facilities operated by<br />
tribes. About one-third of the IHS system facilities are tribally-operated facilities. The IHS estimates that about<br />
25% of the per capita costs of health care needed by AIAN they serve is paid by third-parties including Medicaid,<br />
Medicare and private insurance. The AIAN survey data on which this calculation is based is now more than 20<br />
years old, however. Medicaid payment data provides a way to update the Medicaid portion of the third-party<br />
payment fraction. In addition it offers a way to estimate how much this Medicaid fraction varies across IHS<br />
Areas. Determination of the fraction is critical because the IHS estimates that it provides only about 54% of the<br />
per capita costs of health care needed by AIAN they serve. The extent to which the 25% fraction is too high,<br />
underestimates the remaining unmet health care need of the AIAN, the extent to which the 25% fraction is too<br />
low overestimates the unmet health care need. The IHS allocates new federal funds it receives to the IHS and<br />
tribally-operated facilities based on its calculated estimates of the unmet health care need of the AIAN served by<br />
the facilities.<br />
To achieve the first two objectives, after excluding longterm care and institutionalized Medicaid recipients the<br />
per capita payments for six different types of Medicaid recipients of the remaining medical, behavioral health
Summary<br />
and dental services were analyzed with data from 2006. Medicaid recipients were classified depending on<br />
whether they were under age 65 or not, enrolled all year in Medicaid or not, and whether they received only feefor-service<br />
medical care or had any of their medical services in managed care. The payments for each type of<br />
Medicaid recipient were risk-adjusted for differences between the IHS AIAN and comparison groups with<br />
respect to age, sex, disability, and dual-enrollment with Medicare. Adjustments for differences among the<br />
groups in morbidity were possible for those enrolled all year in Medicaid. The payments were also adjusted for<br />
variation in health care prices across the IHS Areas.<br />
To achieve the third objective, the unadjusted mean per capita payments were determined for all AIAN Medicaid<br />
recipients who used IHS system providers in each Area, except those with institutionalized or longterm care.<br />
These payments were divided by the IHS estimated per capita health care costs for a standard personal health<br />
care service plan for AIAN in each IHS Area in 2006-2007 adjusted for differences in age, sex, health status, and<br />
health care prices. These adjusted per capita health care costs indicated the different payment amounts<br />
required in the different Areas from all payers combined to provide the AIAN in the Area the health care they<br />
need.<br />
Findings<br />
The total amount of Medicaid funds paid for personal health care services in 2006 for 550,000 IHS AIAN<br />
Medicaid enrollees living in the service delivery Areas of IHS and tribally operated facilities for paid personal<br />
health care services was $ 2.05 billion. An additional $15 million was paid by other third-party payers (mainly<br />
private insurance) to cover payments for the claims filed with Medicaid. Of those IHS AIAN Medicaid enrollees<br />
496,000 were recipients of Medicaid paid services during the year full or restricted benefits. For the 472,000<br />
recipients with full benefits $420 million was paid to IHS and tribally operated health care facilities or their<br />
providers of Contract <strong>Health</strong> Service referral care.<br />
Overall Medicaid risk-adjusted payments for personal health care services of IHS AIAN were higher than selfdeclared<br />
AIAN who did not use the IHS health care system and of whites living in the same counties.<br />
There were exceptions to the general finding in four of the 12 IHS Areas where risk-adjusted payments were<br />
lower: In Aberdeen and Billings Areas the payments were lower for most types of Medicaid recipients analyzed<br />
when compared to those of self-declared AIAN who did not use the IHS system or whites. In Albuquerque Area<br />
the payments overall were lower for whites, but higher for self-declared AIAN. In Oklahoma Area the payments<br />
were lower for self-declared AIAN, but higher for Whites.<br />
The overall results did not depend on whether the payments were adjusted for differences in morbidity or not,<br />
or whether IHS AIAN Medicaid recipients received their medical care in a fee-for-service or managed care<br />
system. The medical care services that contributed most to fee-for-service payments for IHS AIAN was<br />
outpatient care, rather than hospital care or prescription drugs. There were very little if any contribution of IHS<br />
Program Medicaid claims for prescription drugs to the Medicaid payments for IHS AIAN outside of Bemidji Area.<br />
One subgroup of AIAN served by the IHS system had much lower risk-adjusted payments than any other AIAN<br />
or white comparison group. This group was that of AIAN who were identified as IHS Active Users in the IHS<br />
data, and had Medicaid paid claims, but no Medicaid IHS Program paid claims. This group who constituted 33%<br />
of the IHS AIAN Medicaid recipients consistently had lower payments across all IHS Areas. The lower payments<br />
for IHS AIAN who were Active Users without IHS provider claims were found even among Medicaid recipient<br />
types where differences in morbidity could be adjusted. The persistence of this affect across all IHS Areas and<br />
Medicaid recipient types implied that IHS these AIAN were potentially receiving IHS services from IHS system<br />
ii
Summary<br />
providers that were either not being billed or paid or both. This would be substitution of limited IHS funding for<br />
Medicaid covered care.<br />
The ‘Medicaid fraction’ of health care costs needed by the IHS AIAN Active User population that is paid by<br />
Medicaid (and Medicaid-CHIP) for personal health care costs is at least 25% in 9 of 12 IHS Areas, but varies<br />
from 19% to 65% depending on the Area. Areas with the lowest fraction of about one-fifth are Nashville (19%)<br />
and Oklahoma (21%). Aberdeen, California, Albuquerque, Portland and Bemidji Areas have mid-range fractions<br />
of between a little more than one quarter and a little less than one-third (27% to 31%). Alaska and Billings are<br />
in the middle of the Area rankings with a little more than one-third of the costs paid by Medicaid (34% to 38%).<br />
It was found that very high Medicaid payments in the state of Arizona for AIAN contributes to the highest<br />
Medicaid fractions found: nearly one half for Navajo and Phoenix Areas (46% and 49% respectively) and nearly<br />
two-thirds (65%) in Tucson Area.<br />
Conclusions and Recommendations<br />
The findings reported here from 2006 support the general conclusion that in most Areas the IHS system<br />
providers and the state Medicaid programs with which they interface in these Areas were as a whole are doing<br />
well at billing and collection for services provided to AIAN Medicaid recipients in the IHS system.<br />
In Aberdeen, Billings, Albuquerque and Oklahoma Areas, it is possible that either the IHS system or others who<br />
provide Medicaid paid care could improve billing and collection. Alternatively, in Albuquerque Area the reason<br />
that lower payments were found only compared to self-declared AIAN who do not use the IHS system could be<br />
because these other AIAN have higher demands for health care when ill because they are not in the IHS system.<br />
The morbidity risk-adjustment is only a partial adjustment for health status differences, because it depends on<br />
the extent to which people use their Medicaid health care provider for completeness.<br />
In every IHS Area there were IHS Active User Medicaid recipients for whom billing and collection could be<br />
improved. This group with no IHS Program claims and such low risk-adjusted Medicaid payments that it is<br />
likely that their IHS system providers are not billing or collecting for a portion of the care of these AIAN they<br />
serve. In addition, IHS system providers were not billing or collecting for prescription drugs.<br />
The IHS estimation of unmet need of the AIAN user population for health care funding needs to use more<br />
recent Medicaid payment data and recognize higher levels of coverage of the health care costs by Medicaid and<br />
Medicaid-CHIP programs, and the variation of the coverage across IHS Areas. Data like that analyzed in this<br />
report but restricted to services included in the Federal Equivalent <strong>Health</strong> Benefit plan. Medicaid benefits vary<br />
in the state programs, though more and more states are starting to provide only the mandatory services, and<br />
dropping the optional benefits that made the services provided across states particularly variable.<br />
iii
Introduction<br />
The <strong>Indian</strong> <strong>Health</strong> Service (IHS) provides only part of the health care needed by the AIAN who rely on the IHS<br />
health care system because of the limited funding appropriated to the agency by the federal budget process.<br />
Funding of the agency has grown in recent years but has not caught up with the growth of the low income AIAN<br />
population, the amount or kinds of specialized care needed, and the increases in health care costs. The IHS<br />
estimates that they provide only 54% of the health care funds needed for the AIAN user population.<br />
The largest and most important alternate resource to IHS for the health care funding of AIAN who rely on the<br />
IHS system is Medicaid. Together with its companion program, the Children’s <strong>Health</strong> Insurance Program (CHIP),<br />
Medicaid has grown to provide a substantial but largely unknown fraction of the coverage of health care for the<br />
AIAN user population of the IHS system. Though the numbers of the user population enrolled in Medicaid and<br />
CHIP has grown substantially over the years, it has been a challenge for IHS and tribally operated health care<br />
facilities accustomed to annual appropriations of federal funds to bill and collect daily claims payments from<br />
state Medicaid programs or private Medicaid managed care plans. Even with Medicaid coverage, it can also be a<br />
challenge for AIAN to obtain the specialty medical care and non-medical services they need from providers<br />
outside the IHS system when they are required.<br />
There has been little reliable data on how much Medicaid funding has grown to cover care the Medicaid enrolled<br />
user population of the IHS system of providers since a household survey of AIAN who rely on the IHS system<br />
was conducted in 1987. While the IHS releases its estimates of total funds gathered from third-parties annually<br />
for the facilities they operate, it is not known how this compares to what is collected at tribally operated<br />
facilities, nor how it breaks down on a per capita basis.<br />
We previously analyzed Medicaid MSIS online data for 2005 on paid claims to IHS system providers on a stateby-state<br />
basis for 2005 (Crouch et al, 2009). That aggregate data could not be used to determine the per capita<br />
funding, or portions of funds spent on IHS system and other providers. The data within states was often from<br />
more than one IHS Area. We then analyzed data extracted from the MSIS data into analytical files for 2004 and<br />
provided estimates of per capita payments for AIAN who had Medicaid (or Medicaid-CHIP) IHS Program claims<br />
in each IHS Area (Crouch et al, 2010). This data could also be compared to per capita payments for AIAN who did<br />
not have such claims and were likely not to have access to the IHS system. It could also be compared to per<br />
capita payments for non-Hispanic Whites living in the same counties. But it could not be determined what the<br />
total number of AIAN Medicaid enrollees who were users of the IHS system. The extent to which there were<br />
AIAN users of the IHS system without Medicaid IHS Program claims paid was an important factor in<br />
determining the potential amounts of funds that IHS system providers might not be collecting.<br />
The data needed to reliably estimate what Medicaid (and Medicaid-CHIP) contribute to cover the health care<br />
costs of AIAN who are users of the IHS system is Medicaid payment data linked to IHS registry data. With such<br />
linked data it is possible to determine how per capita levels of payment for AIAN in the IHS system compare<br />
with those for AIAN not in the system, and to what extent AIAN in the IHS system with Medicaid paid claims do<br />
not have Medicaid IHS Program paid claims. Even more importantly, with Medicaid data linked to IHS registry<br />
data it is possible to determine the fraction of total health care costs of the AIAN user population in the IHS<br />
system is paid by Medicaid and Medicaid-CHIP programs.<br />
1
Introduction<br />
Reliable determination of the proportion of AIAN health care costs covered by this largest source of third-party<br />
payments in the IHS system is critical. To determine how to allocate any new funds that it receives for health<br />
care services among its system providers, the IHS calculates the unmet need for health care funds of the AIAN<br />
user population of its system providers by subtracting from the total calculated need the amount of funding<br />
provided by both the IHS and these alternate sources. The IHS uses data from that 1987 household survey of<br />
AIAN to estimate that Medicaid, Medicare and other third party coverage provides to allocate new health care<br />
funds to IHS and tribal facilities. Because of the relative unreliability of the aging household survey data, they<br />
estimate that a fixed 25% of the health care funds needed at any given Service Unit in the system is provided by<br />
third-party payers. They are unable to determine how this varies across the service delivery areas of the<br />
various Service Units.<br />
Purpose of this Report<br />
The first objective of this report is to determine how much the Medicaid and Medicaid-CHIP programs pay for<br />
the personal health care services of AIAN served by IHS provider system, and then compare those payment<br />
levels to how much is paid for AIAN without access to the IHS system of care, and for non-Hispanic white people<br />
living in the same counties. To achieve this objective it is necessary to understand how variation in enrollee<br />
characteristics and Medicaid payment systems determine the differences in the Medicaid funds paid for the<br />
three groups. Then adjusting for these determinants, we analyze how Medicaid payments for the three groups<br />
vary across the IHS Areas for all three groups of Medicaid enrollees.<br />
A second objective is to determine what fraction of the IHS Active User population with Medicaid paid claims,<br />
does not have any IHS Program Medicaid paid claims and whether their per capita costs are lower than<br />
expected compared to IHS Active Users with IHS Program Medicaid paid claims, and the other AIAN and white<br />
comparison groups. If their Medicaid per capita payments are lower than the other groups after adjustments<br />
for determinants of payment differences, this implies that the rest of their health care costs are not being paid to<br />
IHS providers by Medicaid. To achieve this objective we divide the IHS system users with Medicaid paid claims<br />
into those who were IHS Active Users without IHS Program Medicaid paid claims and those with IHS Program<br />
Medicaid paid claims and determine how adjusted Medicaid per capita payments compare for the two groups<br />
across the IHS Areas. We also compare how payments for IHS Active Users without IHS Program Medicaid paid<br />
claims compare to those of the AIAN and white comparison groups not in the IHS system.<br />
A third objective of this report is to determine what percent of health care funding needed for personal health<br />
care services of AIAN calculated by the IHS is actually provided by the Medicaid and Medicaid-CHIP payments.<br />
How reliable is the assumption based on 1987 data that as much as 25% of the health care costs are met by<br />
Medicaid funds? How reliable is the assumption that the proportion of Medicaid paid health care coverage is<br />
unvarying across the IHS Areas?<br />
2
Methods<br />
I<br />
n this section we describe technical issues regarding the Medicaid and IHS linked data and its<br />
analysis in this report. The term ‘Medicaid data’ in this report includes both Medicaid and CHIP<br />
data in state Medicaid programs (M-CHIP), but not CHIP data for state-only CHIP programs.<br />
Medicaid and M-CHIP data are combined because, 1) there are small numbers of AIAN found to<br />
have CHIP coverage in the IHS Areas in our past studies (American <strong>Indian</strong> and Alaska Native Medicaid<br />
Program and Policy Data, 2010); 2) there is no State-only CHIP program data uniformly collected by<br />
Medicaid; and 3) Medicaid expansion CHIP program data is required of Medicaid state programs and<br />
is included in Medicaid data. Those readers interested in separate Medicaid and M-CHIP data<br />
specific to each IHS Area for 2006 presented in exactly the same format as we did for 2004 data in<br />
2010, please see the separate companion document we prepared with the enriched (linked) data<br />
used in this report: AIAN Medicaid Data Linked to <strong>Indian</strong> <strong>Health</strong> Service Data: Medicaid and CHIP<br />
Enrollment, Service Use and Payments, 2011.<br />
Data Sources<br />
Medicaid-IHS Linked Person Summary File<br />
In 2011 we linked the CMS federal Medicaid/CHIP (MAX) Person Summary File for Calendar Year<br />
(CY) 2006 to IHS registration data from the IHS <strong>National</strong> Data Warehouse (NDW). The methods and<br />
linkage, and the resultant contents of the data file created are described in Integrating Medicaid and<br />
<strong>Indian</strong> <strong>Health</strong> Service Data, 2011. The MAX Person Summary Files included in the linkage were state<br />
files for the 35 states with IHS Contract <strong>Health</strong> Service Delivery Area (CHSDA) counties.<br />
Medicaid Inpatient, Prescription Drug and Other Services Claims Files<br />
The CMS-IHS linked Person Summary File made in 2011 was merged with MAX Inpatient,<br />
Prescription Drug and Other Services claims files for Calendar Year (CY) 2006 by MAX identification<br />
numbers. Claims paid for services in Fee-for-Service (FFS) delivery of care systems, and for<br />
premiums paid in capitated (CAP) systems were provided for services that occurred in CY2006.<br />
Payments processed through May 2007 were included in the MAX claims files, however. In this way<br />
adjustments for adjudicated claims or payments among multiple payers are likely to have been<br />
resolved so that payments represent amounts as close to ‘final’ as possible. In addition diagnostic<br />
information was provided with paid claims in FFS delivery of care systems, and with encounter<br />
records in CAP managed care plan systems.<br />
3
Analysis Groups<br />
IHS AIAN<br />
Methods<br />
The linkage of IHS registry and Medicaid data files in 2011 resulted in three groups of Medicaid<br />
enrollees who obtain services from IHS programs (‘IHS AIAN’), two of which had Medicaid claims<br />
from <strong>Indian</strong> health program providers for IHS ‘covered’ services in 2006, and a third group of which<br />
did not:<br />
1. Medicaid Recipients with IHS Program Claims who are IHS Active Users<br />
IHS AIAN in Group 1 are Medicaid enrollees with Medicaid claims from IHS or Tribal <strong>Indian</strong> (I/T)<br />
healthcare providers in the state who have designated by the state/tribe/<strong>Indian</strong> provider as AIAN<br />
whose Medicaid IHS Program claims for IHS ‘covered’ services are eligible for 100% matching funds<br />
from the federal Medicaid program (100% FMAP).<br />
IHS AIAN in Group 1 were found to be defined by the IHS as AIAN ‘Active Users’ in their data registry<br />
system. These IHS Active Users have had a medical or dental visit from an <strong>Indian</strong> healthcare<br />
provider within a period of three years. A ‘2006 IHS AIAN Active User’ had at least one visit to an<br />
IHS, tribal or Urban <strong>Indian</strong> health program service provider between October 1, 2004 and<br />
September 30, 2006.<br />
Table 1. Analysis groups resulting from linkage of <strong>Indian</strong> <strong>Health</strong> Service (IHS) and Medicaid (MAX) data sources.<br />
Analysis Groups Includes Definition<br />
IHS AIAN<br />
Other AIAN<br />
Whites, Non-Hispanic<br />
1. Medicaid<br />
‘IHS Program’ Recipients<br />
& IHS ‘Active Users’<br />
2. Medicaid<br />
‘IHS Program’ Recipients<br />
3. IHS ‘Active Users’ who are<br />
Medicaid Recipients<br />
Medicaid<br />
‘Racial AIAN’ Recipients not<br />
included in the IHS AIAN<br />
subgroups<br />
Medicaid<br />
‘Racial White Recipients<br />
without Hispanic Ethnicity’<br />
4<br />
Medicaid Enrollees who meet both the<br />
definition of IHS Program Recipients &<br />
IHS Active Users in a given year<br />
Medicaid Enrollees with<br />
at least one paid claim<br />
for an ‘IHS Program’ provided service<br />
IHS Active Users had at least one medical<br />
service from an IHS system provider in 3<br />
years according to IHS, but there is no<br />
Medicaid paid claim for an ‘IHS Program’<br />
provided service in the year of analysis<br />
Race code in the data is ‘AIAN’ either as<br />
the only Race, or in addition to any other<br />
Races, regardless of Hispanic Ethnicity<br />
Race code in the data is ‘White’ as the<br />
only Race, with no Hispanic Ethnicity
Methods<br />
2. Medicaid Recipients with IHS Program Claims who are not IHS Active Users<br />
IHS AIAN in Group 2 are Medicaid enrollees with IHS Program claims for IHS ‘covered’ services<br />
from an I/T provider as in Group 1, but they were not found in the IHS data registry system as IHS<br />
AIAN Active Users. These enrollees may not link as IHS Active Users because: 1) federal Medicaid<br />
criteria for IHS Program users are not the same as IHS criteria for AIAN Active Users and these<br />
enrollees meet the federal Medicaid criteria; 2) the method of the state Medicaid program for<br />
meeting federal Medicaid criteria for IHS Program users subject to 100% FMAP is not sufficiently<br />
specific; 3) not all IHS Active Users have a record in the IHS NDW (the number of 2006 IHS Active<br />
Users in the NDW is 86% of the total 2006 IHS Active User count).<br />
3. Medicaid Recipients without IHS Program Claims who are IHS Active Users<br />
IHS AIAN in Group 3 were Medicaid enrollees with Medicaid claims (recipients) found to be defined<br />
by the IHS as AIAN ‘Active Users’ in the IHS data registry system, but without any IHS Program<br />
claims in the Medicaid data. These Medicaid enrollees may link to the IHS Active User data because:<br />
1) they used an IHS or tribal health program at least once in 2004 or 2005, but not in 2006; 2) they<br />
could have used an IHS or tribal health program in 2006 but the encounter did not result in a<br />
Medicaid paid claim (perhaps because the IHS Program provider was a Medicaid managed care<br />
network provider and received a payment from the managed care plan not Medicaid); or 3) they<br />
could have used an Urban <strong>Indian</strong> health program which are included in IHS Active User<br />
determination, but not Medicaid IHS Program use determination (only IHS and tribally operated<br />
health programs are included in Medicaid determinations of claim payments eligible for 100%<br />
FMAP).<br />
Other AIAN<br />
The ‘Other AIAN’ were Medicaid enrollees with a self-declared race code of “AIAN” who had<br />
Medicaid claims, but did not have any IHS Program Medicaid claims and did not link to the IHS<br />
Active User registry. Since these AIAN live in the counties of the service delivery areas of <strong>Indian</strong><br />
healthcare providers (IHS CHSDA Counties) they can be AIAN who do not meet the stricter criteria of<br />
‘AIAN’ required by the local tribes or IHS Program provider to be able to receive IHS covered<br />
services at no charge, or who do meet those criteria but do not choose to use an IHS or tribal health<br />
program, or who require more specialized or institutional care not provided by the IHS Program or<br />
its Contract <strong>Health</strong> Service system. These Medicaid enrollees may also have failed to link to the IHS<br />
registry because of data limitations of the Medicaid and IHS data systems for a linkage (accurate and<br />
complete data for Social Security Number, date of birth and gender).<br />
Whites (Non-Hispanic)<br />
A random sample cohort of Medicaid enrollees with a self-declared race code of “White” and no<br />
“Hispanic” ethnicity code was constructed from the same counties of the IHS healthcare system as<br />
the IHS AIAN groups (IHS CHSDA Counties). The sampling procedure is described in the 2011 report<br />
Integrating IHS and Medicaid Data . For this analysis the White enrollees are restricted to Medicaid<br />
recipients with Medicaid claims, since the AIAN groups had to have claims to be defined. Recipients<br />
have used at least one Medicaid paid service. We selected White non-Hispanics as the reference<br />
5
Methods<br />
group for the statistical models used in this report to adjust for undetermined differences in<br />
Medicaid programs across the IHS Areas at the county level, and measure adjusted Racial Disparities<br />
in morbidity and Medicaid payments.<br />
Analysis Plan<br />
The questions to be answered by the analyses are, 1) What variables determine the mean total<br />
payment per recipient for IHS AIAN, Other AIAN and Whites? and if those determinants are adjusted,<br />
2) What are the adjusted mean payments for IHS AIAN across the 12 IHS Areas? And 3)How can<br />
those mean payments be used to determine what Medicaid pays for IHS AIAN Active User health<br />
care costs? In this Methods section we restrict the study groups in a systematic way step by step<br />
making the analytical groups more homogeneous and more and more representative of the groups<br />
we mean to compare. We then build models that adjust for determinants that affect large numbers of<br />
recipients In Findings Section I we present the findings from those models that test for the effects of<br />
potential determinants on the payment outcome. In Findings Section II we see how those effects<br />
affect the fraction of the mean total payment per IHS Active User that is paid by Medicaid for the 12<br />
IHS Areas.<br />
Outcome of Analysis: Mean Total Payment per Medicaid Recipient<br />
The analysis is governed by selection of the dependent – or outcome – variable used in the analyses<br />
to measure payments. Particular care has been taken to target the Mean Payment per Person<br />
measure that is most relevant to the goal that we were commissioned to investigate: identify the<br />
contributions of characteristics of the IHS AIAN, state Medicaid programs and the IHS system of<br />
healthcare to Medicaid program payments for medical, dental and behavioral health care of IHS<br />
AIAN. Specific objectives are to determine how those characteristics vary for IHS AIAN across the<br />
twelve IHS administrative areas, and how those characteristics differ for other AIAN and for whites<br />
who also live in the counties of the IHS Areas.<br />
Because of the varying role of private insurance in total payments for Medicaid claims in certain IHS<br />
Areas (in particular, Nashville Area) we include Third Party Payments in the outcome measure for<br />
the analyses and analyze the Total Payment to avoid bias in analyses across IHS Areas (Attachment<br />
Table C.1). Third Party Payments for Medicaid and CHIP program claims can be paid in part by third<br />
parties, rather than the Medicaid or CHIP programs themselves. Third Party Payments for Medicaid<br />
program claims are mainly private insurance payments for Medicaid enrollees under age 65, and<br />
Medicare payments for those over age 65.<br />
Because of differences in systems of claims and payments for acute medical care in Fee-for-Service<br />
(FFS) and capitated Comprehensive Managed Care Plans (CMCP, medical managed care plans), we<br />
analyze results separately for these two groups. Within each group, however, we sum paid claims<br />
and monthly premium (Capitated) paid claims for Prepaid <strong>Health</strong> Plans (PHP, behavioral health and<br />
dental managed care plans) for both FFS and CMCP recipients, and Primary Care Case Management<br />
6
Methods<br />
(PCCM), for some enrollees in FFS medical care). Enrollees with total payments less than $1 were<br />
excluded since claims with Medicaid payments of $0 and negative values (adjustments to prior paid<br />
claims) were included in MAX data (Attachment Table C.3). Outlier values for Medicaid payments<br />
(top 1%) were excluded because of the added skew to mean values while in practice these outliers<br />
are usually relegated to reinsurance mechanisms of payment.<br />
Determinants of the Outcome<br />
Institutionalized and Longterm Care<br />
Medicaid Enrollees in institutionalized and longterm care are excluded from analysis because their<br />
care includes services related to living expenses that are not acute medical or dental care.<br />
Longterm care and institutionalized enrollees include the elderly who need assistance for daily<br />
living, as well as the developmentally disabled and longterm psychiatric inpatients. When payments<br />
for longterm care and institutionalized enrollees are excluded from Total Payments, what remains<br />
is the breadth of medical and dental care covered by Medicaid for acute medical episodes of care.<br />
Total payments per enrollee for the Medicaid covered service are more than 10 times as high as the<br />
medical and dental acute care services per enrollee (See Table 2). As a result, small differences in<br />
institutionalized and longterm care payments can make large differences in mean Total Payment<br />
per Enrollee. For example, when longterm and institutionalized care payments are included, the<br />
mean payment for IHS AIAN is $4,314 (95% Confidence Limits, C.L. $4,274 and $4,354) which is<br />
lower than the $4,785 mean payment for Whites (C.L. $4,758 and $4,812). But when longterm and<br />
institutionalized care payments are excluded, the mean payment for IHS AIAN is higher $3,759 (C.L.<br />
$3,725 and $3,794) than the $3,058 mean payment for Whites (C.L. $3,040 and $3,076).<br />
Furthermore only 1% of IHS AIAN who are Medicaid enrollees use Medicaid covered longterm care,<br />
while 5% of Whites do (calculated using numbers in Table 2). For IHS Area-specific mean Total<br />
Payments per Enrollee including longterm and institutionalized care see Attachment Table C.1. For<br />
numbers and payments for enrollees with longterm and institutionalized care in each Area see<br />
Attachment Table C.2.<br />
Table 2. Mean Medicaid and Third Party payments per Medicaid enrollee with and without institutionalized and<br />
other long-term care for the main study groups. The lower and upper 95% Confidence Limits of each mean are<br />
shown.<br />
Analysis Groups*<br />
Longterm & Institutional Care<br />
IHS AIAN 8,337<br />
Other AIAN 4,488<br />
Whites, Non-Hispanic 64,831<br />
Other Enrollees<br />
Enrollees*<br />
IHS AIAN 550,016<br />
Other AIAN 176,046<br />
Whites, Non-Hispanic 1,232,415<br />
Medicaid Third Party Total<br />
Mean +/- C.L. Mean +/- C.L. Mean +/- C.L.<br />
$ 38,414 $ 308 $ 200 $ 13 $ 38,614 $ 308<br />
$ 37,137 $ 892 $ 187 $ 58 $ 37,324 $ 894<br />
$ 45,771 $ 1,818 $ 167 $ 38 $ 45,939 $ 1,819<br />
$ 3,732 $ 34 $ 27 $ 5 $ 3,759 $ 35<br />
$ 2,576 $ 66 $ 23 $ 3 $ 2,599 $ 66<br />
$ 2,995 $ 17 $ 63 $ 8 $ 3,058 $ 18<br />
7<br />
Total Payment per Enrollee<br />
*The state of Arizona could not be included because of the large numbers of enrollees in longterm care without data on<br />
payments.
Enrollees with no Payments<br />
Methods<br />
Medicaid Enrollees with no Medicaid Payment are excluded from analysis, and thus the outcome<br />
variable is Mean Total Payment per Recipient, not per Enrollee. Medicaid program payments<br />
depend on whether an enrollee has a Medicaid paid service or not. Enrollees must have a Medicaid<br />
paid claim to have any Medicaid payment regardless of whether that claim is paid to a provider for<br />
a medical or dental service, or to a managed care plan for a monthly premium. Two of the IHS AIAN<br />
subgroups in Table 1 were required to have at least one Medicaid paid claim by definition,<br />
‘Medicaid Enrollees with IHS Program Claims’ (those who were IHS Active Users, and those who<br />
were not). As a result the percent of IHS AIAN who had $0 Total Payments was 10%, while for the<br />
two comparison groups Other AIAN and Whites, 13% of the Medicaid enrollees had $0 Total<br />
Payments. Furthermore within IHS Areas the percents of IHS AIAN with $0 Total Payments varied<br />
from a low of 1% in California to a high of 20% in Phoenix and Tucson (Attachment Table C.3). Thus<br />
to avoid the bias created when analysis groups have varying proportions of enrollees with no<br />
Medicaid paid claims, we exclude Medicaid Enrollees with $0 Total Payments. The enrollees who<br />
remain are termed ‘Recipients’ of services by CMS we therefore analyze Total Payment per<br />
Recipient for all analysis groups where a Recipient is a Medicaid Enrollee who receives at least one<br />
paid service claim or one month’s premium paid for managed care. Operationally the enrollee<br />
exclusion criterion technically was enrollees with Total Payments less than $1. Though all<br />
payments in MAX data were rounded to the nearest dollar, there were some claims of less than $0<br />
as a result of payment adjustments removing all Medicaid payments for the year.<br />
Table 3. Mean Medicaid and Third Party payments per Medicaid enrollee of the main study groups with and<br />
without enrollees with zero dollar total Medicaid payments for the year. The ‘Mean Payments per Enrollee’<br />
excluding ‘Enrollees with Zero Dollar Payments for the year’ are the same as ‘Mean Payments Per Recipient.’ The<br />
95% Confidence Limits are also shown.<br />
Enrollees*<br />
Mean +/- C.L. Mean +/- C.L. Mean +/- C.L.<br />
Excluding Enrollees w ith Zero Dollar Payment for the year*<br />
IHS AIAN 495,629 $ 4,141 $ 38 $ 31 $ 6 $ 4,172 $ 38<br />
Other AIAN 153,452<br />
Whites, Non-Hispanic 1,073,924<br />
$ 2,956 $ 76 $ 26 $ 3 $ 2,982 $ 76<br />
$ 3,437 $ 19 $ 72 $ 9 $ 3,509 $ 21<br />
Including Enrollees w ith Zero Dollar Payment for the year*<br />
IHS AIAN 550,016 $ 3,732 $ 34 $ 27 $ 5 $ 3,759 $ 35<br />
Other AIAN 176,046<br />
Whites, Non-Hispanic 1,232,415<br />
$ 2,576 $ 66 $ 23 $ 3 $ 2,599 $ 66<br />
$ 2,995 $ 17 $ 63 $ 8 $ 3,058 $ 18<br />
8<br />
Total Payment per Enrollee<br />
Medicaid Third Party Total<br />
*Enrollees have payments of zero (or negative) dollars if they receive no services, have no paid claims or premiums, or only<br />
adjustments are made to previous payments. Enrollees with non-zero dollar payments for the year are known to be 'Recipients' of<br />
Medicaid paid services during the year.<br />
To determine the mean Total Payment per Enrollee for any group, all that need be done is multiply<br />
the mean Total Payment per Recipient by the number of Recipients in the group and divided by the<br />
total number of Enrollees in the group. This calculation is the same as multiplying the mean Total<br />
Payment per Recipient times the percent of Enrollees who are Recipients (or 100% minus the<br />
percent of Enrollees who are not Recipients). The proportions of Enrollees who are not Recipients
Methods<br />
are in Attachment Table C.3, and the mean Total Payment per Recipient are provided for the<br />
analysis groups in each IHS Area in Attachment Table C.4.<br />
Enrollment for Less than 12 Months<br />
Analyses are done separately for Medicaid Recipients enrolled the full 12 months of the year, and<br />
those enrolled less than 12 months. The Mean Total Payment per Year for Recipients enrolled all 12<br />
months of the year is greater than that for Medicaid Recipients enrolled less than 12 months because<br />
of shorter time of coverage (Table 4). However when analyzed as Mean Total Payment per Month,<br />
the payments for Medicaid Recipients enrolled less than 12 months is systematically larger. Reasons<br />
offered for this bias found in many studies of program enrollees is that there is a ‘pent up demand’<br />
for medical service in enrollees who start coverage during the year, and there is a high utilization at<br />
end of life that occurs for enrollees who die during the year. Varying months of enrollment and<br />
differences amounts of enrollment in managed care plans can affect this phenomenon. This<br />
phenomenon was found to occur for IHS AIAN ($424 and $505 per Recipient per Month with nonoverlapping<br />
95% Confidence Limits, C.L.) and Other AIAN ($310 and $410 per Recipient per Month<br />
with non-overlapping C.L.), but was reversed for Whites ($379 and $371 per Recipient per Month<br />
with non-overlapping C.L.) (Table 4). To avoid potentially unadjusted differences between the<br />
groups behind the phenomenon, data for Medicaid Recipients enrolled 12 months is analyzed<br />
separately from those enrolled less than 12 months. For IHS Area-specific values for the numbers of<br />
recipients and Mean Total Payment per Year for Recipients enrolled 12 months and enrolled less<br />
than 12 months see Attachment Tables C.5 and C.6.<br />
Table 4. Mean Medicaid and Third Party payments per Medicaid recipient* divided between those enrolled all 12<br />
months, and those enrolled less than 12 months for the main analysis groups. The 95% Confidence Limits are<br />
also shown.<br />
Analysis Groups Recipients* Mean +/- C.L. Mean +/- C.L. Mean +/- C.L.<br />
Recipients* enrolled 12 months<br />
IHS AIAN 271,509<br />
Other AIAN 83,156<br />
Whites, Non-Hispanic 588,629<br />
Recipients* enrolled Less than 12 months<br />
IHS AIAN 224,120<br />
Other AIAN 70,296<br />
Whites, Non-Hispanic 485,295<br />
Recipients* enrolled 12 months<br />
IHS AIAN 271,509<br />
Other AIAN 83,156<br />
Whites, Non-Hispanic 588,629<br />
Recipients* enrolled Less than 12 months<br />
IHS AIAN 224,120<br />
Other AIAN 70,296<br />
Whites, Non-Hispanic 485,295<br />
Medicaid Third Party Total<br />
$ 5,086 $ 57 $ 42 $ 10 $ 5,128 $ 58<br />
$ 3,721 $ 120 $ 35 $ 5 $ 3,756 $ 120<br />
$ 4,551 $ 31 $ 104 $ 15 $ 4,656 $ 34<br />
$ 2,997 $ 47 $ 17 $ 4 $ 3,014 $ 47<br />
$ 2,050 $ 84 $ 16 $ 3 $ 2,066 $ 85<br />
$ 2,085 $ 19 $ 33 $ 4 $ 2,118 $ 19<br />
$ 424 $ 5 $ 3 $ 1 $ 427 $ 5<br />
$ 310 $ 10 $ 3 $ 0 $ 313 $ 10<br />
$ 379 $ 3 $ 9 $ 1 $ 388 $ 3<br />
$ 505 $ 10 $ 3 $ 1 $ 507 $ 10<br />
$ 410 $ 23 $ 3 $ 1 $ 413 $ 23<br />
$ 371 $ 5 $ 7 $ 1 $ 378 $ 5<br />
9<br />
Annual Payment per Recipient<br />
Monthly Payment per Recipient<br />
*Only enrollees who are recipients of services are included because analyses exclude enrollees with zero dollar Medicaid<br />
payments.
Methods<br />
Table 5. Mean Medicaid and Third Party Payments per Recipient* divided between those Less than 65 years of<br />
age and 65 years or more for the main analysis groups. The 95% Confidence Limits are also shown.<br />
Analysis Groups Recipients Mean +/- C.L. Mean +/- C.L. Mean +/- C.L.<br />
Recipients* enrolled 12 months<br />
IHS AIAN 254,278<br />
Other AIAN 79,019<br />
Whites, Non-Hispanic 528,997<br />
Recipients* enrolled Less than 12 months<br />
IHS AIAN 220,745<br />
Other AIAN 69,131<br />
Whites, Non-Hispanic 468,157<br />
Recipients* enrolled 12 months<br />
IHS AIAN 254,278<br />
Other AIAN 79,019<br />
Whites, Non-Hispanic 528,997<br />
Recipients* enrolled Less than 12 months<br />
IHS AIAN 220,745<br />
Other AIAN 69,131<br />
Whites, Non-Hispanic 468,157<br />
Recipients* enrolled 12 months<br />
IHS AIAN 17,228<br />
Other AIAN 4,134<br />
Whites, Non-Hispanic 59,521<br />
Recipients* enrolled Less than 12 months<br />
IHS AIAN 3,322<br />
Other AIAN 1,034<br />
Whites, Non-Hispanic 16,191<br />
Recipients* enrolled 12 months<br />
IHS AIAN 17,228<br />
Other AIAN 4,134<br />
Whites, Non-Hispanic 59,521<br />
Recipients* enrolled Less than 12 months<br />
IHS AIAN 3,322<br />
Other AIAN 1,034<br />
Whites, Non-Hispanic 16,191<br />
Medical Fee-for-Service and Capitated Care<br />
Medicaid Third Party Total<br />
$ 5,008 $ 60 $ 33 $ 9 $ 5,041 $ 60<br />
$ 3,656 $ 125 $ 30 $ 5 $ 3,686 $ 125<br />
$ 4,440 $ 33 $ 98 $ 17 $ 4,538 $ 37<br />
$ 2,979 $ 47 $ 15 $ 3 $ 2,993 $ 47<br />
$ 2,038 $ 86 $ 14 $ 2 $ 2,052 $ 86<br />
$ 2,048 $ 19 $ 29 $ 4 $ 2,076 $ 20<br />
$ 417 $ 5 $ 3 $ 1 $ 420 $ 5<br />
$ 305 $ 10 $ 2 $ 0 $ 307 $ 10<br />
$ 370 $ 3 $ 8 $ 1 $ 378 $ 3<br />
$ 499 $ 10 $ 2 $ 0 $ 502 $ 10<br />
$ 407 $ 23 $ 3 $ 1 $ 411 $ 23<br />
$ 363 $ 5 $ 6 $ 1 $ 369 $ 5<br />
$ 6,230 $ 194 $ 178 $ 88 $ 6,408 $ 214<br />
$ 4,964 $ 285 $ 137 $ 54 $ 5,102 $ 292<br />
$ 5,540 $ 76 $ 158 $ 33 $ 5,698 $ 84<br />
$ 4,208 $ 476 $ 148 $ 151 $ 4,356 $ 524<br />
$ 2,919 $ 443 $ 161 $ 105 $ 3,080 $ 461<br />
$ 3,165 $ 118 $ 165 $ 54 $ 3,330 $ 132<br />
$ 519 $ 16 $ 15 $ 7 $ 534 $ 18<br />
$ 414 $ 24 $ 11 $ 5 $ 425 $ 24<br />
$ 462 $ 6 $ 13 $ 3 $ 475 $ 7<br />
$ 846 $ 153 $ 21 $ 17 $ 867 $ 155<br />
$ 557 $ 106 $ 26 $ 15 $ 583 $ 108<br />
$ 597 $ 35 $ 35 $ 14 $ 632 $ 38<br />
10<br />
Less than 65 years of Age<br />
Annual Payment per Recipient<br />
Monthly Payment per Recipient<br />
65 years of Age & Over<br />
Annual Payment per Recipient<br />
Monthly Payment per Recipient<br />
Data is analyzed separately for recipients whose Medicaid paid medical care is provided Fee-for-<br />
Service (FFS) and those whose is provided through a capitated Comprehensive Managed Care Plan<br />
(CMCP). Much of Medicaid covered care has in recent years become managed by health care plans<br />
to lower Medicaid payments. Even recipients in FFS medical care may have monthly capitated<br />
premiums paid for Primary Care Case Management (PCCM), or behavioral or dental Prepaid <strong>Health</strong><br />
Plans (PHP). For enrollment of AIAN in CMCP, PHP and PCCM in the IHS areas see Integrating<br />
Medicaid and <strong>Indian</strong> <strong>Health</strong> Service Data, 2011 .
Methods<br />
When medical care is paid through monthly capitated premiums to CMCP, hospital care may or may<br />
not be included. Thus hospital services may be paid FFS for CMCP enrollees. CMCP also vary in their<br />
breadth of other optional Medicaid services covered as well. CMCP may or may not include<br />
behavioral health or dental services. Enrollees in CMCP may or may not also have monthly<br />
capitated premiums paid for behavioral or dental Prepaid <strong>Health</strong> Plans (PHP). Alternatively these<br />
services not covered in CMCP plans may like hospital care be paid through FFS claims. When CMCP<br />
recipients are not enrolled in a CMCP for all the months they are enrolled in Medicaid, they can also<br />
have FFS claims for services.<br />
In analyses of Medicaid payments it is thus important to adjust for the effect of capitated CMCP<br />
payments in groups of Recipients. We thus analyzed Mean Total Payments for Recipients with 12<br />
months enrollment but no CMCP (that is, 12 months of FFS care, which can also include PCCM, or<br />
Dental or Behavioral <strong>Health</strong> PHP), or with any months of CMCP (Table 6). The numbers of<br />
recipients with 12 months enrollment in Medicaid but less than 12 months enrollment in CMCP was<br />
too small a group to be analyzed separately. The numbers of recipients for the IHS Areas are shown<br />
in Attachment Table C.7 (all ages combined). The payments for recipients in only FFS medical care<br />
in the IHS Areas are shown in Attachment Table C.8, and for those with any CMCP in Attachment<br />
Table C.9. Values for the hospital, other medical, prescription drug and dental FFS payments, as well<br />
as for PCCM, Dental and Behavioral <strong>Health</strong> PHP premiums are provided in Attachment Tables C.8<br />
and C.9.<br />
Table 6. Mean Medicaid and Third Party payments per Medicaid recipient enrolled 12 months divided into those<br />
not enrolled in any Comprehensive (medical) Managed Care Plan (CMCP), those enrolled less than 12 months in<br />
CMCP and those enrolled 12 months in CMCP for the main study groups. The 95% Confidence Limits for each<br />
mean value are also shown.<br />
Analysis Groups Recipients Mean +/- C.L. Mean +/- C.L. Mean +/- C.L.<br />
Recipients not enrolled in medical managed care (CMCP)<br />
IHS AIAN 237,019 $ 5,114 $ 64 $ 48 $ 12 $ 5,161 $ 65<br />
Other AIAN 61,669<br />
Whites, Non-Hispanic 371,592<br />
$ 3,751 $ 134 $ 46 $ 7 $ 3,796 $ 134<br />
$ 4,872 $ 46 $ 163 $ 24 $ 5,035 $ 53<br />
Recipients enrolled less than 12 months in medical managed care (CMCP)<br />
IHS AIAN 13,861 $ 4,886 $ 178 $ 6 $ 2 $ 4,892 $ 178<br />
Other AIAN 4,784<br />
Whites, Non-Hispanic 51,114<br />
$ 3,576 $ 209 $ 14 $ 14 $ 3,589 $ 210<br />
$ 3,594 $ 52 $ 13 $ 2 $ 3,607 $ 52<br />
Recipients enrolled 12 months in medical managed care (CMCP)<br />
IHS AIAN 20,629 $ 4,897 $ 119 $ 1 $ 0 $ 4,898 $ 119<br />
Other AIAN 16,703<br />
Whites, Non-Hispanic 165,923<br />
Medicaid Third Party Total<br />
$ 3,655 $ 326 $ 1 $ 1 $ 3,656 $ 326<br />
$ 4,129 $ 26 $ 1 $ 0 $ 4,130 $ 26<br />
11<br />
Annual Payment per Recipient<br />
While payments per recipient under age 65 are lower for every analysis group with CMCP when<br />
compared to those with FFS medical care (Table 6), the differences are not large. What is striking is<br />
the smaller proportions of AIAN in CMCP than Whites who live in the same counties. This we find<br />
depends on the IHS Area (See Attachment Table C.9.) Over age 65, the numbers of AIAN Recipients<br />
in CMCP is small for all groups, but particularly the AIAN groups (Table 6).
Restricted Benefits<br />
Methods<br />
Enrollees with Restricted Benefits were excluded from the analyses. Enrollees in certain Medicaid<br />
enrollment categories are only eligible for a restricted portion of the full scope of medical benefits:<br />
For example, women eligible only because they are pregnant (but not women who are eligible for<br />
Medicaid or CHIP and become pregnant), certain groups of Medicare-Medicaid Dual eligibles,<br />
enrollees in pharmacy only or other specially approved state ‘waiver’ programs. We found small<br />
numbers of Medicaid enrollees with Restricted Benefits (Table 7), and therefore cannot do a<br />
separate analysis for these enrollees. Adjusting analyses of the mean Total Payments per Person<br />
for Restricted Benefits in the models described below had small if any effects. We therefore<br />
excluded enrollees with Restricted Benefits from the analyses we present here.<br />
Table 7. Mean Total Payments per Recipient for enrollees with 12 months Fee-for-Service (FFS) medical care<br />
with or without managed care (PCCM, CMCP and Dental & Behavioral <strong>Health</strong> Prepaid <strong>Health</strong> Plans, PHP) paid<br />
per Medicaid recipient with Full Benefits all 12 months or at least one month of Restricted Benefits for the main<br />
study groups. The 95% Confidence Limits for each mean value are also shown.<br />
Analysis Groups Recipients Mean +/- C.L. Mean +/- C.L. Mean +/- C.L.<br />
Recipients not enrolled in medical managed care (Fee-For Service, FFS)<br />
IHS AIAN 220,368 $ 5,035 $ 67 $ 37 $ 11 $ 5,073 $ 68<br />
Other AIAN 57,865<br />
Whites, Non-Hispanic 320,435<br />
$ 3,683 $ 141 $ 39 $ 7 $ 3,722 $ 142<br />
$ 4,840 $ 52 $ 160 $ 28 $ 5,000 $ 59<br />
Recipients enrolled less than 12 months in medical managed care (CMCP)<br />
IHS AIAN 13,666 $ 4,850 $ 179 $ 5 $ 2 $ 4,855 $ 179<br />
Other AIAN 4,719<br />
Whites, Non-Hispanic 49,932<br />
$ 3,492 $ 200 $ 13 $ 14 $ 3,505 $ 200<br />
$ 3,427 $ 50 $ 12 $ 2 $ 3,439 $ 50<br />
Recipients enrolled 12 months in medical managed care (CMCP)<br />
IHS AIAN 20,244 $ 4,821 $ 107 $ 1 $ 0 $ 4,821 $ 107<br />
Other AIAN 16,435<br />
Whites, Non-Hispanic 158,630<br />
$ 3,609 $ 331 $ 1 $ 1 $ 3,610 $ 331<br />
$ 3,950 $ 26 $ 0 $ 0 $ 3,951 $ 26<br />
Recipients not enrolled in medical managed care (Fee-For Service, FFS)<br />
IHS AIAN 16,648 $ 6,154 $ 188 $ 183 $ 91 $ 6,337 $ 210<br />
Other AIAN 3,801<br />
Whites, Non-Hispanic 51,056<br />
$ 4,778 $ 294 $ 148 $ 59 $ 4,926 $ 303<br />
$ 5,068 $ 84 $ 182 $ 38 $ 5,251 $ 94<br />
Recipients enrolled less than 12 months in medical managed care (CMCP)<br />
IHS AIAN 195 $ 7,413 $ 1,107 $ 63 $ 75 $ 7,476 $ 1,107<br />
Other AIAN 65<br />
Whites, Non-Hispanic 1,177<br />
$ 9,680 $ 5,122 $ 51 $ 59 $ 9,731 $ 5,117<br />
$ 10,647 $ 638 $ 32 $ 13 $ 10,680 $ 638<br />
Recipients enrolled 12 months in medical managed care (CMCP)<br />
IHS AIAN 385 $ 8,928 $ 3,033 $ 1 $ 1 $ 8,929 $ 3,033<br />
Other AIAN 268<br />
Whites, Non-Hispanic 7,288<br />
Less than 65 years of Age<br />
$ 6,464 $ 585 $ 2 $ 4 $ 6,466 $ 587<br />
$ 8,024 $ 163 $ 5 $ 5 $ 8,029 $ 164<br />
12<br />
Annual Payment per Recipient<br />
Medicaid Third Party Total<br />
65 years of Age & Over
Medical Cost Index<br />
Methods<br />
Payments were adjusted using the Medical Cost Index used by the IHS in computing what it would<br />
cost to provide equitable services across the 12 IHS Areas<br />
(http://www.ihs.gov/NonMedicalPrograms/lnf/): This Medical Cost Index is calculated from the<br />
<strong>Health</strong> Care portion of the Cost of Living Index (COLI) published by the Council for Community and<br />
Economic Research (C2ER). Indices of regional differences of health care prices are published by<br />
C2ER for select counties and metro-areas (www.coli.org/Method.asp).<br />
Table 8. Indices of regional differences in health care costs for the IHS Areas calculated by IHS for 2009 using the<br />
health care portion of the COLI of the Council for Community and Economic Research.<br />
IHS Area<br />
13<br />
<strong>Health</strong> Care Cost<br />
of Living Index<br />
Scaled<br />
Alaska 1.31<br />
Portland 1.13<br />
California 1.08<br />
Aberdeen 1.02<br />
Billings 1.01<br />
Nashville 1.00<br />
Navajo 0.99<br />
Phoenix 0.99<br />
Tucson 0.99<br />
Bemidji 0.98<br />
Albuquerque 0.97<br />
Oklahoma 0.94<br />
The <strong>Health</strong> Care portion of their COLI is designed to provide the best possible means to compare<br />
cost of living differences in these areas based on the price of consumer goods and services, but the<br />
index has a number of limitations. The data is voluntarily provided by designated organizations.<br />
The C2ER states that all price data are obtained from sources deemed reliable and that the C2ER<br />
stringently reviews all prices reported, and attempts to eliminate errors and noncompliance with<br />
pricing specifications. Still they issue a disclaimer that, ‘no representation is made as to the complete<br />
accuracy thereof.’ In addition there are certain definitional limitations such as that the health care<br />
purchases priced are those appropriate for “professional and managerial households in the top<br />
income quintile,” while Medicaid programs purchase for households in the lowest income quintile of<br />
their state. Certainly the greatest limitation is that the price variation largely reflects variation in<br />
urban health care prices, which is but an undetermined fraction of the health care purchased by<br />
Medicaid for residents of the generally rural CHSDA counties of the IHS Areas.<br />
We used the health care C2ER COLI because it was recommended that the IHS use the health care<br />
COLI in the calculation of the IHS Federal Disparities Index by its Contract <strong>Health</strong> Service<br />
workgroup. The workgroup of tribal and technical advisors to the IHS believed it was best available<br />
index that could reflect macro differences in health care prices among regions. The determination<br />
of the <strong>Health</strong> Care COLI for the 12 IHS Areas is done by the IHS.
Age and Sex<br />
Methods<br />
Medical care payments increase with age, and yet the differences in age of populations among AIAN<br />
groups and between AIAN and Whites cannot be changed unless a Medicaid eligibility policy change<br />
occurs affecting age groups differently. Age can be coded continuously (in years), or in intervals (5<br />
or 10 year age cohorts). Usually an analytical definition is used to avoid unnecessarily large<br />
numbers of interval groups: irregular intervals are used to define age groups with substantially<br />
higher payments than the immediate younger group. We will test the use of a Continuous Age<br />
variable and an analytical Interval Age Group variable. The adjustment that explains most of the<br />
variation in the Mean Total Payment will be used in the Core Model.<br />
Medical care payments are generally higher for women than men when the services include<br />
reproductive care, and especially higher in Medicaid for women who are pregnant or give birth<br />
during the year. Alternatives for gender determinants are 1) Male, Female pregnant, & Female non-<br />
Pregnant; or 2) Male, Female, with adjustment for pregnancy and childbirth services in the Service<br />
Coverage variables. The adjustment that explains most of the variation in the Mean Total Payment<br />
will be used in the Core Model.<br />
Disability as Basis of Medicaid Eligibility and Dual Eligibility with Medicare<br />
Medical care payments are generally higher for blind or disabled individuals. We provided a list of<br />
the blind and disabled eligibility categories for Medicaid and for Dual Eligibility with Medicare in<br />
AIAN Medicaid Program and Policy Statistics: Summary Report, 2009 . The proportions of AIAN<br />
Medicaid eligibles who are Disabled or Dual eligibles in each IHS Area are documented in AIAN<br />
Medicaid Program and Policy Data, 2010 .<br />
Risk Adjustment: Morbidity<br />
Medical care costs rise as the number and severity of medical conditions increase. To determine if<br />
there are differences in payments not related to illness requires adjusting costs for differences in the<br />
morbidity burden among the study groups. This is possible with Medicaid claims tested Risk<br />
Adjustment software systems (Winkelman and Dammler, 2008). We used the Adjusted Clinical<br />
Groups® (ACG) system developed at The Johns Hopkins University to characterize the concurrent<br />
morbidity burden in the AIAN and White Medicaid populations in our study for the time period of<br />
the claims (http://www.acg.jhsph.org). With this software demographic, diagnostic and procedure<br />
code combinations on 12 continuous months of claims and encounter records were reduced to a<br />
fixed number of health status categories called Aggregated Diagnosis Groups.<br />
The ACG system captures interrelationships between co-occurring morbidities that pose the greatest<br />
demands for health care resources. ACG actuarial cells are based on Aggregated Diagnosis Groups<br />
that are similar in terms of severity and likelihood of persistence of the health condition over time.<br />
Diagnostic codes are assigned to one of the 32 clusters of Aggregated Diagnosis Groups. Since<br />
individuals can have more than one diagnosis, they may have more than one Aggregated Diagnosis<br />
Group. Individual diseases or conditions are placed into a single Aggregated Diagnosis Groups based<br />
14
Methods<br />
on five clinical dimensions: 1) Duration of the condition (acute, recurrent, or chronic); 2) Severity of<br />
the condition (e.g., minor and stable versus major and unstable); 3) Diagnostic certainty (symptoms<br />
versus documented disease); 4) Etiology of the condition (infectious, injury, or other); and 5)<br />
Specialty care involvement (e.g., medical, surgical, obstetric, hematology). The Aggregated Diagnosis<br />
Groups are then weighted and added so that a single ACG morbidity (risk) score is obtained by each<br />
individual.<br />
The ACG system provides an external standard sample of privately insured population in a managed<br />
care plan for reference, but the system recommends use of an internal reference group to<br />
standardize for unadjusted differences between Medicaid populations and provider claims and<br />
privately insured managed care data. We used the random sample of non-Hispanic White Medicaid<br />
recipients living in the same counties as the AIAN as the morbidity reference group.<br />
The software is not recommended for use without a 12 month continuous claim history for<br />
recipients, and therefore we did not apply it to recipients with less than 12 months enrollment. We<br />
did not use the feature of the software that uses pharmacy data because we found that IHS AIAN in<br />
the Medicaid data had much lower pharmacy payments than other which is likely due to access to<br />
medications through their <strong>Indian</strong> healthcare providers, which Other AIAN and Whites do not have<br />
(see Prescription Drug FFS data in the Findings section).<br />
Statistical Adjustments<br />
To adjust for the effects of determinants on mean total payments per recipient, we constructed<br />
Generalized Linear Mixed Models of SAS statistical software (version 9.2) using the log-likelihood<br />
function, assuming the gamma distribution of the dependent variable (Medicaid payments). We<br />
have previously published studies using these methods with Medicaid claims data (Wong et al,<br />
2006), including using the ACG risk adjustment (Korenbrot, Kao & Crouch, 2009).<br />
Medicaid Enrollee Exclusions were: 1) enrollees with no known months of eligibility, 2) enrollees<br />
with longterm or institutionalized care, 3) enrollees with ‘Restricted’ rather than ‘Full’ Medicaid<br />
benefits, and 4) enrollees with no paid claims of $1 or more. Recipients remaining were then<br />
grouped for analytical modeling as in Table 9:<br />
15
Methods<br />
Table 9. Findings for all six series are summarized at the end of the Findings Section. The results of Analyses 1<br />
and 2 are presented in Figures in the Findings Section with detailed tables in Attachments F and G. All findings<br />
from Analyses 3 to 6 are in Attachments H, I, J and K respectively.<br />
1 2 3 4 5 * 6 *<br />
FFS Medical<br />
Morbidity<br />
Adjustment<br />
Capitated<br />
Medical<br />
No morbidity<br />
adjustment<br />
FFS Medical<br />
No morbidity<br />
adjustment<br />
Capitated<br />
Medical<br />
No morbidity<br />
adjustment<br />
Analyses<br />
Recipients Less than 65 years of Age Recipients Aged 65 & Over<br />
12 months Enrollment<br />
Any Months of Enrollment<br />
16<br />
12 months Enrollment<br />
FFS Medical<br />
Morbidity<br />
Adjustment<br />
Capitated<br />
Medical<br />
Any Months of Enrollment<br />
FFS Medical<br />
No morbidity<br />
adjustment<br />
The numbers of recipients in each analytical group are presented in Attachment C by state and IHS<br />
Area. All recipients in Analysis 1 are included in Analysis 2, those in Analysis 3 are included in<br />
Analysis 4, and those in Analysis 5 are included in Analysis 6.<br />
Capitated<br />
Medical<br />
In Analyses 1, 2 and 5 recipients were enrolled in Medicaid 12 months, so the outcome was the<br />
Adjusted Mean Total Payment per Recipient per Year and the models could be adjusted for<br />
morbidity (Attachments E, F and I). In analyses 3, 4 and 6 the recipients could be enrolled less than<br />
12 months in Medicaid and therefore the outcome was the Adjusted Mean Total Payment per<br />
Recipient per Month and the models could not be adjusted for morbidity because there was not a 12<br />
month continuous claims history for all recipients (Attachments G, H and J).<br />
Within each of the 6 series of analytical models the study groups are nested within each of the 12<br />
IHS Areas and adjusted for Age and Sex (interaction terms) and Medicaid Disability and Dual<br />
Eligibility Status under age 65 (interaction terms). Morbidity adjustments were included for the<br />
groups enrolled 12 months in Medicaid. The first set of study groups within each series of analyses<br />
compares: IHS AIAN, Other AIAN and Whites. For further comparison the second set of study groups<br />
within each series of analyses divides the IHS AIAN into, 1) those with IHS Program claims who are<br />
also IHS Active Users, 2) those with IHS Program claims who are not also IHS Active Users, and 3)<br />
those who are IHS Active Users but did not have any IHS Program claims – and includes Other AIAN<br />
and Whites.<br />
In the models, all effects of the adjustment and study variables were significant at the P
Methods<br />
each recipient type across IHS Areas we calculated for each recipient type the difference between<br />
the adjusted mean payment for IHS AIAN and a comparison group in each IHS Area as a percent of<br />
the mean payment for IHS AIAN (Attachment Tables L.1, L.4). We then multiplied the relative<br />
percent difference in the payment times the number of the IHS AIAN in that IHS Area, and<br />
determined the weighted difference for the recipient type across the IHS Areas for the comparison<br />
group (Attachment Tables L.2, L.5).<br />
To obtain an overall measure for each IHS Area across the 6 analyses of all types of recipients, we<br />
repeated the method using the same differences between the adjusted mean payment for IHS AIAN<br />
and a comparison group in each IHS Area for each recipient type as the difference in percent of the<br />
mean payment for IHS AIAN (Attachment Tables L.1, L.4). However we multiplied the relative<br />
percent difference in the payment for each recipient type times the number of the IHS AIAN in that<br />
recipient type, and determined the weighted difference for each IHS Area across all the recipient<br />
types represented in that Area (Attachment Tables L.3, L.6).<br />
17
Methods<br />
Map 1. 12 IHS Areas: Contract <strong>Health</strong> Service Delivery Areas (CHSDA)<br />
18
Findings<br />
Findings<br />
Payments for AIAN Medicaid Recipients<br />
The total amount of Medicaid funds paid in 2006 for 550,000 IHS AIAN Medicaid enrollees living in the service<br />
delivery Areas of IHS and tribally operated facilities for paid personal health care services was $ 2.05 billion<br />
(Table 2). The personal health care services included Medical (including physician, clinic, outpatient, laboratory<br />
and imaging, pharmacy), Behavioral <strong>Health</strong> and Dental Care services. An additional $15 million was paid by<br />
other third-party payers (mainly private insurance) to cover payments for the claims filed with Medicaid. Of<br />
those IHS AIAN Medicaid enrollees 496,000 were recipients of Medicaid paid services during the year.<br />
Findings are presented here for the CHSDA counties of the IHS service delivery areas. The numbers of IHS AIAN<br />
with Medicaid coverage in the separate states of each IHS service delivery area are not large enough to give<br />
statistically reliable findings (the numbers and payments for AIAN in the counties of the IHS service delivery<br />
areas of the states in the analytical subgroups are presented in Attachments F to I). One of the main reasons why<br />
state numbers of IHS AIAN are not large enough is that not all states report IHS claims separate from other<br />
claims (see American <strong>Indian</strong> and Alaska Native Medicaid Program and Policy Statistics: Summary Report 2009)<br />
and when they do they do not capture all claims for IHS AIAN.<br />
Recipients with Fee-for-Service Medical Services<br />
Age, Sex, Disability & Morbidity Do Not Explain Differences in Payments<br />
If left unadjusted for any determinants, the mean total payment for IHS AIAN recipients with FFS medical care<br />
who are less than 65 years of age is only slightly higher than Whites ($5,104 compared to $4,960, or $144<br />
difference), but much higher than Other AIAN ($3,670, or $1,436 difference) (Figure 1). The minimal actuarial<br />
adjustment for age and sex differences increases the difference in payments between IHS AIAN and Whites<br />
($7,052 compared to $6,369, or about $600) but not with Other AIAN ($7,052 compared to $5,567, or about<br />
$1500). This effect is expected because the IHS AIAN have a younger age distribution than that of Whites and<br />
therefore lower expected payments, but a similar age distribution to that of Other AIAN and therefore similar<br />
expected payments. The mean adjusted payment increases for all three groups with the age adjustment because<br />
payments for older more costly recipients are given equal weight with less costly younger recipients which<br />
constitute the vast majority of the recipients in all three groups. This is how the statistical adjustment controls<br />
for the differences in age distributions across the three groups.<br />
Adjusting payments further for disability status, either because of Medicaid eligibility as a disabled enrollee, or<br />
as a Medicare-Medicaid ‘Dual’ enrollee under age 65, increases the adjusted means and the differences in means<br />
for all three groups (Figure 1). The mean total payment for IHS AIAN is much higher for Whites ($9,999<br />
compared to $7,884, or a $2,115 difference) and for Other AIAN ($7,319, or a $2,680 difference). Again the<br />
adjusted mean rises for all groups because the higher payments for the smaller groups of Disabled are given<br />
equal weight with less costly but higher proportions of non-disabled recipients during the statistical<br />
adjustment.<br />
19
Findings<br />
Figure 1. Adjustment of Mean Total Payment per Recipient for IHS AIAN, Other AIAN and Whites less than 65 years of age<br />
enrolled 12 months with FFS medical care (successive adjustments for age and sex, disability, & morbidity). Payments include<br />
FFS claims for medical services and either FFS claims or managed care plan premiums for non-medical services (behavioral<br />
health or dental).<br />
$10,000<br />
$9,000<br />
$8,000<br />
$7,000<br />
$6,000<br />
$5,000<br />
$4,000<br />
$3,000<br />
$2,000<br />
$1,000<br />
$-<br />
$5,104<br />
$3,670<br />
$4,960<br />
$7,052<br />
$5,567<br />
$6,369<br />
$9,999<br />
The further adjustment for the variation in morbidity among the three groups reduces the differences between<br />
IHS AIAN and Whites, and between IHS AIAN and Other AIAN, but substantial differences remain (Figure 1).<br />
The mean total payment for IHS AIAN is higher for Whites ($5,865 compared to $4,689, or a $1,176 difference)<br />
and for Other AIAN ($4,453, or a $1,412 difference). The morbidity scores for the low income Medicaid eligible<br />
Whites (1.013 with 90% Confidence Limits, C.L., from1.011 to 1.015) were actually worse than those of IHS<br />
AIAN (0.954 with 90% C.L. 0.949 to 0.959) and Other AIAN (0.880 with 90% C.L. 0.875 to 0.885). We<br />
investigated whether the lack of diagnosis codes on claims paid to <strong>Indian</strong> health care providers could explain<br />
the morbidity scores and found that it did not. More diagnosis codes per recipient were used to determine<br />
morbidity for IHS AIAN recipients with <strong>Indian</strong> health care provider claims than for Whites or Other AIAN in all<br />
Areas except Aberdeen Area (Attachment Tables D.1 and D.2).<br />
Payments across IHS Areas still Vary Substantially after Adjustments<br />
Fee-for Service payments are higher for IHS AIAN than Whites in two-thirds of the IHS Areas (Alaska, Bemidji,<br />
Billings, California, Phoenix, Portland and Tucson Areas, Figure 2). But the payments are lower for IHS AIAN in<br />
Aberdeen and Albuquerque Areas, and about the same for IHS AIAN and whites in Nashville and Oklahoma<br />
Areas. The mean adjusted total payments for Whites in the Tucson Area are exceptionally low (less than $1000<br />
per recipient) while payments for IHS AIAN are exceptionally high, so we investigated payments in Arizona<br />
more closely.<br />
20<br />
$7,884<br />
$7,319<br />
Unadjusted Age*Sex Adjusted Disabled*Medicare,<br />
Age*Sex Adjusted<br />
$5,865<br />
$4,453<br />
$4,689<br />
& Morbidity Adjusted<br />
IHS AIAN<br />
Other AIAN<br />
Whites
Findings<br />
Figure 2. Adjusted Mean Total Payment per Recipient for IHS AIAN, Other AIAN and Whites less than 65 years of age with FFS<br />
medical care across 12 IHS Areas (adjusted for age and sex, and for Disability, Dual eligibility with Medicare, & Morbidity).<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
$- $1,000 $2,000 $3,000 $4,000 $5,000 $6,000 $7,000 $8,000 $9,000 $10,000<br />
In the state of Arizona unadjusted payments are more than 7 times higher for IHS AIAN as for whites<br />
(Attachment xx) which explains the much higher payments for IHS AIAN in Navajo, Phoenix and Tucson Areas<br />
(Figure 2). When recipients in the state of Arizona are simply excluded from the adjusted analyses because of<br />
the unusually high disparities in payments with whites, payments for IHS AIAN are higher in Phoenix but not<br />
Navajo Area (Figure 3). All of Tucson Area is included in Arizona, and therefore no determination is possible for<br />
IHS AIAN after excluding recipients in the state of Arizona. There were also too few Whites in FFS care in<br />
Arizona to include them in further models with FFS recipients.<br />
Figure 3. Adjusted Mean Total Payment per Recipient for IHS AIAN, AIAN and Whites less than 65 years of age with FFS<br />
medical care across IHS Areas, excluding recipients in the state of Arizona (in Navajo, Phoenix and all Tucson Areas).<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
$- $1,000 $2,000 $3,000 $4,000 $5,000 $6,000 $7,000 $8,000 $9,000 $10,000<br />
21<br />
IHS AIAN<br />
Other AIAN<br />
Whites<br />
IHS AIAN<br />
Other AIAN<br />
Whites
Findings<br />
Payments are Higher for IHS AIAN with Medicaid IHS Program claims<br />
When the IHS AIAN are divided into those with and without Medicaid IHS Program claims paid to IHS system<br />
health care providers (I/T), payments are higher for IHS AIAN who had Medicaid IHS Program claims than those<br />
who did not in all Areas but Nashville (Figure 4). Whether the IHS AIAN who had Medicaid IHS Program claims<br />
were also IHS Active Users (Group 1) or not (Group 2), payments are higher than those of IHS Active Users who<br />
did not have any Medicaid IHS Program claims (Group 3). The only distinction was that in the Navajo Area the<br />
payments were much higher for IHS AIAN who had Medicaid IHS Program claims and were also IHS Active<br />
Users (Group 1), but not for those with Medicaid IHS Program claims who were not also IHS Active Users<br />
(Group 2). The much higher payments for IHS AIAN in Navajo Area were eliminated when all recipients in the<br />
state of Arizona were excluded from analysis (Figure 5). In fact there were no Medicaid IHS Program claims for<br />
AIAN who were not IHS Active Users when recipients from Arizona were excluded from the analysis.<br />
Figure 4. Adjusted Mean Total Payment per Recipient for IHS AIAN in Figure 2 divided into: 1) IHS AIAN with IHS Program<br />
claims who are IHS Active Users; 2) IHS AIAN with IHS Program claims who are not IHS Active Users; and 3) IHS AIAN who<br />
are IHS Active Users with no IHS Program Medicaid claims. For comparison the Other AIAN and Whites of Figure 2 are shown.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
$- $2,000 $4,000 $6,000 $8,000 $10,000<br />
22<br />
1.IHS Program claims<br />
& Active User<br />
2.IHS Program claims<br />
but Not Active User<br />
3.IHS Active User with<br />
no IHS Program claims<br />
Other AIAN<br />
Whites
Findings<br />
Figure 5. Adjusted Mean Total Payment per Recipient for IHS AIAN in Figure 3 which excluded recipients in the state of<br />
Arizona divided into the 3 IHS AIAN groups in Figure 4. Other AIAN and Whites of Figure 3 are also shown.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
$- $2,000 $4,000 $6,000 $8,000 $10,000<br />
In all Areas except the Nashville Area, payments for IHS Active Users who did not have any Medicaid IHS<br />
Program claims (Group 3) were lower or about the same (Alaska and Portland Areas) as those of Whites (Figure<br />
4).<br />
Payments for Outpatient Services had Largest Effect on Total Payments<br />
We investigated whether there were payments for particular types of services that explained the higher<br />
payments for IHS AIAN with IHS Program claims (Groups 1 and 2). The cleanest way to investigate this was to<br />
successively exclude 1) clinic and physician outpatient payments (Figure 6), then 2) hospital payments (Figure<br />
7), and finally 3) prescription drug payments (Figure 8). These three categories of services were uniformly<br />
defined by the Medicaid data extraction process into separate MAX claims files.<br />
Excluding outpatient clinic and physician payments (Figure 6) had the largest impact of the three general types<br />
of service on reducing the differences in mean total payments per recipient between IHS AIAN with IHS<br />
Program claims (Groups 1 and 2) and IHS AIAN Group 3 without IHS Program claims and Whites. The average<br />
decline in adjusted mean payments for Group 1 was $2,960, Group 2 was $2,520, while that for Group 3 was<br />
$680 and Whites was $750 (difference in values of Figure 6 and Figure 4). Particularly large differences remain<br />
for Groups 1 and 2 for the Areas with Arizona state recipients (Navajo, Phoenix and Tucson Areas). For hospital<br />
services the average decline in adjusted mean payments for Group 1 was $1068, Group 2 was $992, while that<br />
23<br />
1.IHS Program claims<br />
& Active User<br />
2.IHS Program claims<br />
but Not Active User<br />
3.IHS Active User with<br />
no IHS Program claims<br />
Other AIAN<br />
Whites
Findings<br />
for Group 3 was $600 and Whites was $737 (difference in values of Figure 7 and Figure 4). Prescription drugs<br />
contributed the least to mean payments for AIAN (difference in values of Figure 8 and Figure 4). For<br />
prescription drugs the average decline in adjusted mean payments for Whites was largest ($935) while for IHS<br />
AIAN with IHS Program claims the values were lowest: Group 1 it was only $274 and Group 2 was $234. For IHS<br />
AIAN with no IHS Program claims (Group 3) the amount was $548, more like that for Other AIAN ($400) than<br />
Groups 1 and 2 or Whites.<br />
Figure 7. Adjusted Mean Payment per Recipient excluding payments for outpatient visits to clinics, hospitals, or physicians’<br />
offices. Compare with Figure 4 Adjusted Mean Total Payments per Recipient.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
$- $2,000 $4,000 $6,000 $8,000 $10,000<br />
24<br />
1.IHS Program claims<br />
& Active User<br />
2.IHS Program claims<br />
but Not Active User<br />
3.IHS Active User with<br />
no IHS Program claims<br />
Other AIAN<br />
Whites
Findings<br />
Figure 8. Adjusted Mean Payment per Recipient excluding payments for hospital stays. Compare with Figure 4 Adjusted Mean<br />
Total Payments per Recipient, and Figure 6 Adjusted Mean Payment per Recipient excluding outpatient visits.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
$- $2,000 $4,000 $6,000 $8,000 $10,000<br />
Figure 9. Adjusted Mean Payment per Recipient excluding payments for prescription drugs. Compare with Figure 4 Adjusted<br />
Mean Total Payments per Recipient, and Figure 6 Adjusted Mean Payment per Recipient excluding outpatient visits.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
$- $2,000 $4,000 $6,000 $8,000 $10,000<br />
25<br />
1.IHS Program claims<br />
& Active User<br />
2.IHS Program claims<br />
but Not Active User<br />
3.IHS Active User with<br />
no IHS Program claims<br />
Other AIAN<br />
Whites<br />
1.IHS Program claims<br />
& Active User<br />
2.IHS Program claims<br />
but Not Active User<br />
3.IHS Active User with<br />
no IHS Program claims<br />
Other AIAN<br />
Whites
Findings<br />
Unadjusted mean payments for outpatient services to IHS and Tribal Program providers (Figure 10) for IHS<br />
AIAN were about 60% of the total paid to all providers (Figure 9, see Table 9). For Group 1 the proportion was<br />
58% ($1,800 out of at least $3100 per recipient), while for Group 2 the proportion was 62% ($1,530 out of at<br />
least $2,487 per recipient). The types of outpatient services included in IHS Program services provided by IHS<br />
and Tribal providers is more comprehensive than those included for all providers in ways that cannot be<br />
equalized with MAX claims data. In the Billings Area outpatient service payments for IHS Program outpatient<br />
services are so large that payments to IHS Program providers for IHS outpatient services actually exceed<br />
payments to all providers for Outpatient Visit, Laboratory, Imaging, and Dental services (Table 9).<br />
Figure 10. Unadjusted Mean Payment per Recipient for outpatient services including visits, laboratory and<br />
imaging, and dental services. Compare with Figure 10 unadjusted Mean Payment per Recipient for IHS or Tribal<br />
outpatient services.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
Outpatient Payments<br />
to all Providers<br />
$- $1,000 $2,000 $3,000 $4,000 $5,000 $6,000 $7,000<br />
The types of outpatient services provided by IHS Program Providers are more comprehensive than those<br />
included here for all providers in ways that cannot be equalized with MAX data. In the Billings Area (Montana &<br />
Wyoming states) these other outpatient services are so much broader that payments to IHS Program Providers<br />
for IHS Program outpatient services actually exceed payments to All Providers for Outpatient Visit, Laboratory,<br />
Imaging, and Dental services for the same recipients.<br />
26<br />
1.IHS Program claims<br />
& Active User<br />
2.IHS Program claims<br />
but Not Active User<br />
3.IHS Active User with<br />
no IHS Program claims<br />
Other AIAN<br />
Whites
Findings<br />
Figure 11. Unadjusted Mean Payment per Recipient for outpatient visits, laboratory & imaging, dental, and other IHS<br />
outpatient services through IHS or Tribal clinics or hospitals. Compare with IHS AIAN Groups 1 and 2 in Figure 9.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
Outpatient Payments<br />
to IHS & Tribal Programs<br />
$- $1,000 $2,000 $3,000 $4,000 $5,000 $6,000 $7,000<br />
27<br />
1.IHS Program claims<br />
& Active User<br />
2.IHS Program claims<br />
but Not Active User
Findings<br />
Table 10. Unadjusted Mean Fee-for-Service payments per IHS AIAN Recipient for Outpatient Visit, Laboratory, Imaging and<br />
Dental services.<br />
Outpatient Visit, Laboratory, Imaging, and Dental* Payments per IHS AIAN Recipient<br />
Group 1.IHS Program claims<br />
& Active User<br />
IHS Program<br />
All Providers Providers* All Providers<br />
28<br />
Group 2.IHS Program claims<br />
but Not Active User<br />
IHS Program<br />
Providers*<br />
IHS Area Unadjusted Mean Payments Difference Unadjusted Mean Payments Difference<br />
Aberdeen $ 2,045 $ 1,330 $ 715 $ 1,471 $ 1,045 $ 426<br />
Alaska $ 2,554 $ 554 $ 2,000 $ 2,140 $ 387 $ 1,753<br />
Albuquerque $ 2,124 $ 1,191 $ 933 $ 1,453 $ 974 $ 479<br />
Bemidji $ 2,437 $ 592 $ 1,845 $ 2,417 $ 1,105 $ 1,313<br />
Billings* $ 1,202 $ 2,039 $ (837) $ 1,202 $ 1,724 $ (521)<br />
California $ 2,026 $ 1,397 $ 629 $ 1,882 $ 1,052 $ 830<br />
Nashville $ 1,688 $ 842 $ 846 $ 2,351 $ 530 $ 1,821<br />
Navajo $ 4,827 $ 3,340 $ 1,486 $ 2,200 $ 2,200 $ -<br />
Oklahoma $ 1,854 $ 943 $ 910 $ 1,935 $ 918 $ 1,017<br />
Phoenix $ 6,892 $ 4,102 $ 2,790 $ 4,841 $ 3,318 $ 1,523<br />
Portland $ 1,963 $ 1,791 $ 173 $ 1,809 $ 1,356 $ 453<br />
Tucson $ 7,588 $ 3,470 $ 4,118 $ 6,143 $ 3,769 $ 2,374<br />
Area Mean $ 3,100 $ 1,800 $ 1,300 $ 2,487 $ 1,530 $ 956<br />
Recipients in Medical Comprehensive Managed Care Plans (CMCP)<br />
Age, Sex, Disability & Morbidity Do Not Explain Differences in Payments for Recipients with<br />
Managed Medical Care<br />
If left unadjusted for any determinants, the mean total payment for IHS AIAN recipients with capitated medical<br />
care in a Comprehensive Managed Care Plan (CMCP) who are less than 65 years of age is slightly higher for<br />
Whites ($4,268 compared to $3,865, or about $400 difference), but substantially higher for Other AIAN ($3,426,<br />
or $842 difference) (Figure 11). The minimal actuarial adjustment for age and sex differences increases the<br />
difference in payments between IHS AIAN and Whites ($6,273 compared to $5,265, or about $1,000) but not<br />
with Other AIAN ($6,273 compared to $5,398, or about $875). As with the FFS recipients not in CMCP plans, this<br />
effect is expected because the IHS AIAN have a younger age distribution than that of Whites and therefore lower<br />
expected payments, but a similar age distribution to that of Other AIAN and therefore similar expected<br />
payments. Again, the mean adjusted payment increases for all three groups with the age adjustment because<br />
payments for older more costly recipients are given equal weight with less costly younger recipients which<br />
constitute the vast majority of the recipients in all three groups. This is how the statistical adjustment controls<br />
for the differences in age distributions across the three groups.<br />
Adjusting payments further for disability status, either because of Medicaid eligibility as a disabled enrollee, or<br />
as a Medicare-Medicaid ‘Dual’ enrollee under age 65, increases the adjusted means but not the differences in<br />
means for the groups (Figure 11). The mean total payment for IHS AIAN is about $1,000 higher for Whites<br />
($7,439 compared to $6,490) and for Other AIAN ($6,479). Again the adjusted mean rises for all groups<br />
because the higher payments for the smaller groups of Disabled are given equal weight with less costly but<br />
higher proportions of non-disabled recipients during the statistical adjustment.
Findings<br />
Figure 12. Adjustment of Mean Total Payment per Recipient for IHS AIAN, Other AIAN and Whites less than 65 years of age<br />
enrolled 12 months with any months of enrollment in a Comprehensive Managed Care Plan (CMCP) (successive adjustments<br />
for age and sex, & disability). Payments include capitated plan premiums for medical services and either FFS claims or<br />
managed care plan premiums for non-medical services (behavioral health or dental).<br />
$10,000<br />
$9,000<br />
$8,000<br />
$7,000<br />
$6,000<br />
$5,000<br />
$4,000<br />
$3,000<br />
$2,000<br />
$1,000<br />
$-<br />
$4,268<br />
$3,865<br />
$3,426<br />
$6,273<br />
$5,265<br />
$5,398<br />
$7,439<br />
$6,490<br />
$6,479<br />
Unadjusted Age*Sex Adjusted Disabled*Medicare,<br />
Age*Sex Adjusted<br />
29<br />
$5,743 $5,200<br />
$5,050<br />
& Morbidity Adjusted<br />
IHS AIAN<br />
Other AIAN<br />
Whites<br />
After the further adjustment for variation in morbidity among the three groups, the differences are reduced<br />
between IHS AIAN and Whites, and between IHS AIAN and Other AIAN, but the differences remain that are as<br />
large as the unadjusted Mean Total Payments (about $700 and $500 respectively, Figure 11). CMCP plan<br />
members in all three groups had lower morbidity scores than their FFS counterpart groups in Figure 1. This<br />
could be because managed care participants are healthier or because managed care plans provide premium<br />
and encounter claims but not service claims. The morbidity scores for the low income Medicaid eligible Whites<br />
(0.949 with 90% Confidence Limits, C.L., from 0.946 to 0.952) were actually worse than those of IHS AIAN<br />
(0.863 with 90% C.L. 0.858 to 0.868) and Other AIAN (0.843 with 90% C.L. 0.835 to 0.851) (Attachment Tables<br />
D1 and D2).<br />
Payments across IHS Areas Vary Substantially for Recipients with Managed Medical Care<br />
Among recipients with any enrollment in medical managed care plans (CMCP) in their 12 months of Medicaid<br />
enrollment, mean total payments (including any FFS services) are higher for IHS AIAN than Whites in half of the<br />
10 Areas with any CMCP plans (Bemidji, California, Phoenix, Portland and Tucson Areas, Figure 13). Nashville<br />
which had lower payments for IHS AIAN who were not enrolled in any CMCP (Figure 2) is now joined by<br />
Aberdeen, Albuquerque, Navajo and Oklahoma Areas which have lower payments for IHS AIAN than Whites.<br />
Alaska and Billings Areas did not have AIAN or Whites in the counties of the IHS program service delivery areas<br />
enrolled in CMCP plans.
Findings<br />
Figure 13. Adjusted Mean Total Payment per Recipient for IHS AIAN, Other AIAN and Whites less than 65 years of age enrolled<br />
12 months with any months of managed medical care in a CMCP across the IHS Areas (adjusted for age and sex, and for<br />
Disability, Dual eligibility with Medicare, & Morbidity).<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
$- $2,000 $4,000 $6,000 $8,000 $10,000<br />
30<br />
IHS AIAN<br />
Other AIAN<br />
Whites<br />
Payments for Recipients in Managed Medical Care are Higher for IHS AIAN with Medicaid IHS<br />
Program Claims<br />
When the IHS AIAN recipients with any enrollment in medical managed care plans (CMCP) are divided into<br />
those with and without Medicaid IHS Program claims paid to IHS system health care providers (I/T), payments<br />
are higher for IHS AIAN who had Medicaid IHS Program claims than those who did not in all Areas but<br />
Aberdeen (Figure 14). Whether the IHS AIAN who had Medicaid IHS Program claims were also IHS Active<br />
Users (Group 1) or not (Group 2), payments are higher than those of IHS Active Users who did not have any<br />
Medicaid IHS Program claims (Group 3). In Alaska, Billings and Nashville Areas there were no IHS AIAN with<br />
Medicaid IHS Program claims who also were enrolled in medical managed care plans (CMCP). Albuquerque,<br />
Bemidji and Oklahoma Areas joined the three Areas with recipients in the state of Arizona (Navajo, Phoenix<br />
and Tucson Areas) to have much higher payments for IHS AIAN who had Medicaid IHS Program claims when<br />
compared to IHS Active Users who did not have any Medicaid IHS Program claims. The payments were so much<br />
higher for Bemidji, Oklahoma, Phoenix and Tucson that the scale in the figure was expanded to accommodate<br />
adjusted mean total payments between $10,000 and $12,000 per recipient.
Findings<br />
Figure 14. Adjusted Mean Total Payment per Recipient for the IHS AIAN with any months of managed medical care in a CMCP<br />
in Figure 13 divided into three groups across 12 IHS Areas. Other AIAN and White results are shown as well. Note that the<br />
scale was expanded to accommodate adjusted payments greater than $10,000 IHS AIAN with Medicaid IHS Program claims in<br />
Bemidji, Oklahoma, Phoenix and Tucson Areas.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
$- $2,000 $4,000 $6,000 $8,000 $10,000 $12,000<br />
31<br />
1.IHS Program claims<br />
& Active User<br />
2.IHS Program claims<br />
but Not Active User<br />
3.IHS Active User with<br />
no IHS Program claims<br />
Other AIAN<br />
Whites
Analysis<br />
Group<br />
Compiled Findings for All Analyses and Areas<br />
Findings<br />
Adjusted Mean Payments for IHS AIAN are Overall Higher<br />
IHS AIAN generally had higher adjusted mean total payments than either Other AIAN or Whites for nearly all<br />
types of Recipients analyzed, though the payments for IHS AIAN were only 4% to 9% higher than those of<br />
Whites (depending on the type of Recipient, Table 11). The payments were 18% to 32% higher for four of six<br />
types of Recipients when compared to Other AIAN. To obtain an overall measure for all types of Recipients in<br />
the 6 analyses, we first determined the adjusted mean total payment for each type of IHS AIAN Recipient (Table<br />
11) in each IHS Area (Attachment Table L.1). We then determined the difference between the adjusted mean<br />
total payment for IHS AIAN with that of each type of Other AIAN and White Recipients in the IHS Areas<br />
(Attachment Table L.1). The difference between the payment for the IHS AIAN and comparison group was<br />
expressed as a percent of the payment for IHS AIAN. That percent difference in mean payments was multiplied<br />
by the number of IHS AIAN in each Recipient and IHS Area to provide a weighted mean (average) of the relative<br />
differences (Attachment Table L.2). The findings for the differences thus determined across the six types of<br />
Recipients are presented in Table 11 and Figure 15. The findings across the 12 IHS Areas are presented in the<br />
next section (Figures 16 and 17, Attachment Table L.3).<br />
Table 11. Mean percent differences in the adjusted Mean Total Payments for IHS AIAN recipients compared to Other AIAN and<br />
Whites for the 6 groups of recipients. See also Figure 15 and Attachment Table L.2.<br />
Mean<br />
Payment<br />
Analyses<br />
1 2 3 4 5 * 6 *<br />
Differen<br />
ce in<br />
Means<br />
Recipients Less than 65 years of Age Recipients Aged 65 & Over<br />
12 months Enrollment Any Months of Enrollment 12 months Enrollment Any Months of Enrollment<br />
FFS Medical<br />
(220,368)<br />
Capitated Medical<br />
(34,490)<br />
Mean<br />
Payment<br />
Differe<br />
nce in<br />
Means<br />
FFS Medical<br />
(336,888)<br />
Mean<br />
Payment<br />
Differe<br />
nce in<br />
Means<br />
Capitated Medical<br />
(116,277)<br />
Mean<br />
Payment<br />
32<br />
Differen<br />
ce in<br />
Means<br />
FFS Medical<br />
(8,554)<br />
Mean<br />
Paymen<br />
t<br />
Differe<br />
nce in<br />
Means<br />
Capitated<br />
Medical<br />
(1,759)*<br />
Mean<br />
Payment<br />
IHS AIAN $ 5,976<br />
$ 6,157<br />
$ 848<br />
$ 702<br />
$ 8,609<br />
$ 888<br />
FFS Medical<br />
(14,715)<br />
Payments per Year Payments per Month Payments per Year Payments per Month<br />
Differen<br />
ce in<br />
Means<br />
Other AIAN 24% 25% -17% 32% -38% 18%<br />
Whites 13% 9% 12% 4% 8% -21%<br />
*There were insufficient numbers of recipients over age 65 in capitated medical care to analyze mean payments reliably.<br />
Capitated<br />
Medical<br />
(3,884)*
Findings<br />
Differences in adjusted mean total payments for IHS AIAN were 2% to 13% higher than those for Whites in five<br />
of the six types of Medicaid Recipients analyzed (Table 11, Figure 15). Only in the analysis of Recipients age 65<br />
and over in FFS medical care with any number of months of enrollment, was the payment lower. The adjusted<br />
mean per capita payment for IHS AIAN of $888 per month was 21% lower than the payment for Whites. When<br />
IHS AIAN payments were compared to those of Other AIAN, for four of the six types of Medicaid Recipients<br />
analyzed the payments IHS AIAN payments were higher, while in two they were not. Payments 17% lower were<br />
found for Other AIAN when compared to the adjusted mean of $848 per month for IHS AIAN Recipients under<br />
age 65 with any number of months of enrollment in FFS medical care. Payments 28% lower than the adjusted<br />
mean of $8,609 per year were found for Other AIAN when Recipients with 12 months of enrollment in FFS<br />
medical care and aged 65 and over were analyzed.<br />
Figure 15. Mean percent differences in the adjusted Mean Total Payments for IHS AIAN recipients compared to Other AIAN<br />
(red bars) and Whites (grey bars) for the 6 analytical groups of recipients in Table 11.<br />
50%<br />
40%<br />
30%<br />
20%<br />
10%<br />
0%<br />
-10%<br />
-20%<br />
-30%<br />
-40%<br />
-50%<br />
Analysis<br />
1 2 3 4 5 6<br />
33<br />
Other AIAN<br />
Whites
Findings<br />
Adjusted Mean Payments for IHS AIAN are Lower than Whites in Some IHS Areas<br />
When the overall measure for the same adjusted mean total payments examined above by type of Medicaid<br />
recipient, are calculated by IHS Area, the overall finding differs for four of the Areas: Aberdeen, Billings and<br />
Oklahoma Areas had lower adjusted mean total payments for IHS AIAN compared to Other AIAN across the<br />
different types of Recipient analyzed (Figures 16, Attachment Table L.3). Aberdeen, Billings and Albuquerque<br />
Areas had lower adjusted mean total payments for IHS AIAN compared to Whites (Figures 17, Attachment Table<br />
L.3). Findings for all other Areas tended to be higher mean payments.<br />
Figure 16. Percent differences in the adjusted Mean Total Payments for IHS AIAN recipients compared to Other AIAN for the 6<br />
analyses by IHS Area. Positive percent changes indicate the relative amount by which IHS AIAN payments were higher than<br />
Other AIAN. Negative percent changes indicate that by which they were lower.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
-60% -40% -20% 0% 20% 40% 60%<br />
Figure 17. Percent differences in the adjusted Mean Total Payments for IHS AIAN recipients compared to Whites for the 6<br />
analyses by IHS Area. Positive percent changes indicate the relative amount by which IHS AIAN payments were higher than<br />
Whites. Negative percent changes indicate that by which they were lower.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
-60% -40% -20% 0% 20% 40% 60%<br />
*There are insufficient numbers of whites in the counties of the Tucson Area for a comparison to be made.<br />
34
Findings<br />
Adjusted Mean Payments for IHS AIAN without IHS Program Medicaid Claims are Lower than<br />
Others<br />
IHS AIAN who were Active Users but had not IHS Program Medicaid claims had substantially lower payments<br />
than all other groups (Table 12). Payments for the three different subgroups of IHS AIAN created by the linkage<br />
of data with the IHS registry system were analyzed in the same way as in Table 11 to arrive at an overall<br />
measure that allowed comparison of IHS Active Users with no IHS Program Medicaid claims with the two<br />
groups of IHS AIAN with IHS Program claims as well as Other AIAN and Whites (Attachment Table L.5). There<br />
were sufficient numbers of IHS AIAN without Medicaid IHS Program claims under age 65 to allow analyses but<br />
not over age 65, and therefore a total of 4 analyses were possible. The per capita payments for IHS AIAN Active<br />
Users without IHS Program Medicaid claims were substantially lower for all types of Medicaid recipients when<br />
compared to either IHS AIAN subgroup with IHS Program Medicaid claims (IHS Active Users with IHS Program<br />
claims: 64% to 93% lower; and IHS Program claims only: 26% to 100%). Payments were substantially lower<br />
than those of other AIAN who did not use the IHS system (11% to 30% depending on the type of Recipient), and<br />
of whites living in the same counties (14% to 46% depending on the type of Recipient).<br />
Table 12. Difference in Adjusted Mean Total Payment per Recipient for IHS AIAN Active Users (group 3) with no IHS<br />
Program Medicaid claims of each type of Recipient analyzed compared to IHS AIAN groups IHS Program Medicaid claims<br />
(groups 1 and 2), Other AIAN and Whites in each Area.<br />
IHS Area Analysis Group<br />
Recipie<br />
nts<br />
1<br />
FFS Medical<br />
(220,368)<br />
Mean<br />
Paymt<br />
Differe<br />
nce<br />
Recipie<br />
nts<br />
Mean<br />
Paymt<br />
35<br />
Analyses<br />
2 3 4<br />
Recipients Less than 65 years of Age<br />
12 months Enrollment Any Months of Enrollment<br />
Capitated Medical<br />
(34,490)<br />
Differe<br />
nce<br />
Recipie<br />
nts<br />
FFS Medical<br />
(336,888)<br />
Payments per Year Payments per Month<br />
Mean<br />
Paymt<br />
Differe<br />
nce<br />
Recipie<br />
nts<br />
Capitated Medical<br />
(116,277)<br />
All Areas 1.IHS Claims & User -64% -76% -93% -71%<br />
Mean<br />
Paymt<br />
Differe<br />
nce<br />
2.IHS Claims -52% -81% -100% -26%<br />
3.IHS Active User 55670 $ 3,820<br />
13951 $ 4,134 103859 $ 585<br />
46931 $ 465<br />
Other AIAN -16% -11% -30% -16%<br />
Whites -27% -14% -32% -46%<br />
When the overall measure was calculated by IHS Area across the 4 types of Medicaid recipients, only Nashville<br />
Area was found to have overall higher payments (26% higher) for the IHS AIAN Active Users without IHS<br />
Program Medicaid claims than for Other AIAN who did not use the IHS system (Figure 18, Attachment Table<br />
L.6). Only Tucson was found to have substantially higher payments for the IHS AIAN Active User group than<br />
Whites (13%, Figure 19). Nashville had only 1% higher payments than Whites, which is negligible. Oklahoma<br />
Area had lower payments for the IHS AIAN Active User group than all four of the other groups but only 1% to<br />
4% lower (Attachment Table L.6). Aberdeen Area also had lower payments that were only 1% to 9% lower than<br />
the four other groups.
Findings<br />
Figure 18. Percent differences in the adjusted Mean Total Payments for IHS AIAN recipients without Medicaid IHS Program<br />
claims compared to Other AIAN for the 4 analyses under age 65. See Attachment Table L.6.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
-60% -40% -20% 0% 20% 40% 60%<br />
Figure 19. Percent differences in the adjusted Mean Total Payments for IHS AIAN recipients without Medicaid IHS Program<br />
claims compared to Other AIAN for the 4 analyses under age 65. See Attachment Table L.6.<br />
Aberdeen<br />
Alaska<br />
Albuquerque<br />
Bemidji<br />
Billings<br />
California<br />
Nashville<br />
Navajo<br />
Oklahoma<br />
Phoenix<br />
Portland<br />
Tucson<br />
-60% -40% -20% 0% 20% 40% 60%<br />
36
Findings<br />
Medicaid Paid Fraction of Total <strong>Health</strong> Care Costs of IHS Active Users<br />
IHS Calculated <strong>Health</strong> Care Costs for IHS Active Users<br />
The IHS determined that the actuarially calculated benchmark (standardized) cost of a Federal Employee <strong>Health</strong><br />
Plan of personal medical services for the AIAN users at the IHS and tribal provider sites in the IHS <strong>Indian</strong> health<br />
care service delivery system was an estimated $4,106 in 2006 (Table 13, 2007 calculations from the Federal<br />
Employees <strong>Health</strong> Plan Disparities Index). Within each Area, for each IHS and tribal health care site they adjusted<br />
how this benchmark amount would need to be increased or decreased (negative numbers are in parentheses in<br />
Table 13) to purchase the care at that site using standard actuarial techniques. They then aggregated results at<br />
the Area level.<br />
Table 13. IHS determined differences in per capita costs of health care costs for IHS Users across IHS Areas and the expected<br />
adjustments including Alternate Resource amounts. Amounts in parentheses (x) are negative reductions in expected costs of<br />
care to IHS and tribal providers for costs of care of their IHS Active User population.<br />
IHS Area<br />
Benchmark Adjustments Adj Bnchmk Adjustments Adj Bnchmk<br />
Cost per<br />
IHS Active<br />
User 2006<br />
Economic<br />
Adjustment<br />
<strong>Health</strong> Status<br />
& Poverty<br />
Adjustment<br />
37<br />
Cost per<br />
IHS Active<br />
User<br />
Alternate Resource<br />
Adj aggregated for<br />
Sites by Area<br />
Cost per<br />
IHS Active<br />
User<br />
Aberdeen $ 4,106 $ (189) $ 774 $ 4,691 $ (999) -21% $ 3,693<br />
Alaska $ 4,106 $ 1,856 $ (131) $ 5,831 $ (1,396) -24% $ 4,435<br />
Albuquerque $ 4,106 $ (202) $ 9 $ 3,913 $ (822) -21% $ 3,091<br />
Bemidji $ 4,106 $ (101) $ 333 $ 4,338 $ (815) -19% $ 3,523<br />
Billings $ 4,106 $ (128) $ 502 $ 4,480 $ (910) -20% $ 3,569<br />
California $ 4,106 $ 488 $ (399) $ 4,195 $ (728) -17% $ 3,467<br />
Nashville $ 4,106 $ 266 $ (263) $ 4,109 $ (678) -17% $ 3,432<br />
Navajo $ 4,106 $ (597) $ 97 $ 3,606 $ (902) -25% $ 2,705<br />
Oklahoma $ 4,106 $ (414) $ (170) $ 3,522 $ (687) -20% $ 2,834<br />
Phoenix $ 4,106 $ 95 $ (10) $ 4,191 $ (806) -19% $ 3,385<br />
Portland $ 4,106 $ 572 $ (259) $ 4,419 $ (770) -17% $ 3,649<br />
Tucson $ 4,106 $ (278) $ 102 $ 3,930 $ (867) -22% $ 3,063<br />
The $4,106 benchmark amount for the FEHP medical, dental, behavioral health? and vision care was adjusted<br />
for the following:<br />
Actuarial Adjustments for age and sex distribution of the AIAN user population of IHS and Tribal sites<br />
Economic Adjustments for differences in health care costs (the COLI Index, see Methods Medical Cost<br />
Index); Size (economies of scale of larger provider sites) and whether all hospital and specialty services are<br />
purchased because of lack of access to an IHS or tribal hospital<br />
<strong>Health</strong> and Poverty Adjustments for differences in health status (relative rates for the Areas for injuries and<br />
poisonings, alcoholism, diabetes, heart disease, cancer); Area differences in birth rates; Area differences in<br />
Percent of population over age 55; and Area and site differences in Poverty Rates among AIAN<br />
After adjustments, the expected Benchmark cost per IHS Active User varied across the IHS Area varied<br />
considerably from a low of $3,522 in Oklahoma Area to a high of %5,831 in Alaska Area.<br />
The amount deducted for third party ‘Alternate Resources’ from the adjusted benchmark cost in each IHS Area<br />
for FY2007 is shown in Table 13. The calculations included the estimate that Medicaid/CHIP, Medicare, Private<br />
Insurance and other third party payers pay about 25% of the adjusted health care costs for IHS Active Users<br />
across all IHS and tribal provider sites in the IHS Areas based on 1987 survey data. The Alternate Resources<br />
include estimated collections to the IHS and tribal sites from the third party payers and payments made to other
Findings<br />
providers for services needed by IHS and tribal site users. At sites without access to an IHS or tribal hospital the<br />
amount deducted from the benchmark cost for Alternate Resources was higher because no hospital costs were<br />
billable by IHS or tribal provider sites, and instead had to be purchased.<br />
Medicaid Fraction of IHS Active User <strong>Health</strong> Care Costs<br />
We can use the actual Medicaid (that is Total Medicaid and Third Party) payments for IHS AIAN enrollees in<br />
2006 that are documented in the Medicaid-IHS linked data in this report to update the Medicaid/CHIP portion<br />
of Alternate Resources paid in each Area per IHS Active User. Because IHS adjusted the expected benchmark<br />
cost for each Area, the proper payment information to use is the Unadjusted Mean Payment per IHS AIAN<br />
Recipient multiplied by the rate at which IHS Active Users in the IHS Registry were found to be Medicaid<br />
enrollees, and then the rate at which the IHS AIAN Medicaid enrollees were found to be Recipients with<br />
Medicaid paid claims (Table 14).<br />
When we insert the Mean Total Payments for the appropriate IHS AIAN Medicaid recipients in the IHS analytical<br />
framework (Attachment Table C.4 data inserted in column A of Table 14), we find that the Medicaid Alternate<br />
Resources are higher than expected from the 1987 survey data, (Table 14 compared to Table 13).<br />
Table 14. Calculation of the expected Medicaid Mean Total Payment per IHS Active User across IHS Areas as a percent of the<br />
FDI Adjusted Benchmark (Column F, blue column from Table 13). Total payment includes the amounts paid by Medicaid/CHIP<br />
and Third Parties for Medicaid enrollees with paid claims (recipients).<br />
IHS Area<br />
Unadjusted Mean<br />
Total Medicaid<br />
Payment per IHS<br />
AIAN Recipient*<br />
IHS Active Users<br />
w ho are Medicaid<br />
Enrollees (%)<br />
IHS AIAN Medicaid<br />
Enrollees w ho are<br />
Recipients<br />
(%)<br />
38<br />
IHS Active User<br />
Recipients<br />
(% of all IHS<br />
Active Users)<br />
Unadjusted<br />
Mean Total<br />
Medicaid<br />
Payment<br />
per IHS Active<br />
User<br />
FDI Adj Bnchmk<br />
per IHS Active<br />
User<br />
Medicaid<br />
Payments<br />
(% of FDI Adj<br />
Benchmark)<br />
A B C D = B x C E = A x D F G=E/F<br />
Aberdeen $ 3,024 44% 96% 42% $ 1,277 $ 4,691 27%<br />
Alaska $ 6,575 37% 92% 34% $ 2,238 $ 5,831 38%<br />
Albuquerque $ 3,162 39% 93% 36% $ 1,147 $ 3,913 29%<br />
Bemidji $ 4,172 35% 92% 32% $ 1,343 $ 4,338 31%<br />
Billings $ 4,078 39% 96% 37% $ 1,527 $ 4,480 34%<br />
California $ 4,261 29% 99% 29% $ 1,223 $ 4,195 29%<br />
Nashville $ 3,983 22% 88% 19% $ 771 $ 4,109 19%<br />
Navajo $ 4,065 49% 84% 41% $ 1,673 $ 3,606 46%<br />
Oklahoma $ 2,924 26% 95% 25% $ 722 $ 3,522 21%<br />
Phoenix $ 5,757 45% 79% 36% $ 2,047 $ 4,191 49%<br />
Portland $ 4,113 34% 94% 32% $ 1,315 $ 4,419 30%<br />
Tucson $ 6,244 51% 80% 41% $ 2,548 $ 3,930 65%<br />
*From Attachment C: Recipients Enrolled Any Number of Months in Medicaid (Attachment Table C.4)<br />
The percent of all IHS Active Users who are Medicaid Recipients (column D) is the product of multiplying two<br />
key rates of Medicaid participation determined from linked IHS and Medicaid data:
Findings<br />
Percent of IHS Active Users who are Medicaid enrollees (column B). The Medicaid enrollment rate for IHS<br />
Active Users was determined during the linkage of IHS Registry data to this Medicaid enrollee data (see<br />
Methods and Table 2 in the 2011 report Integrating Medicaid and <strong>Indian</strong> <strong>Health</strong> Service Data).<br />
Percent of IHS Active User Medicaid Enrollees who are Recipients of Medicaid Paid Services (column C).<br />
The Medicaid participation rate of enrollees was determined by dividing the number of IHS AIAN Medicaid<br />
enrollees that had paid claims of more than zero dollars in column A, by all the IHS AIAN Medicaid<br />
enrollees (Attachment Table C.3).<br />
When expressed as a percent of the FDI Adjusted Benchmark Costs, the Areas with lowest fractions of health<br />
care costs paid by Medicaid for their IHS Active User population are Nashville (19%) and Oklahoma (21%)with<br />
a Medicaid Fraction of about one-fifth ( Figure 15). Aberdeen, California, Albuquerque, Portland and Bemidji<br />
Areas have mid-range fractions of between a little more than one quarter and a little less than one-third (27% to<br />
31%). Alaska and Billings are in the middle of the Area rankings with a little more than one-third of the costs<br />
paid by Medicaid (34% to 38%). And Navajo and Phoenix have Medicaid fractions of nearly one half (46% and<br />
49% respectively). Tucson has the highest Medicaid paid fraction of nearly two-thirds (65%).<br />
Figure 20. Medicaid Alternate Resources paid to all providers as percent of IHS calculated FDI benchmark health care costs<br />
for IHS Active Users in each Area.<br />
Nashville<br />
Oklahoma<br />
Aberdeen<br />
California<br />
Albuquerque<br />
Portland<br />
Bemidji<br />
Billings<br />
Alaska<br />
Navajo<br />
Phoenix<br />
Tucson<br />
19%<br />
21%<br />
27%<br />
29%<br />
29%<br />
30%<br />
31%<br />
34%<br />
38%<br />
46%<br />
49%<br />
Medicaid Fraction Paid to IHS and Tribal Providers for IHS Active Users<br />
Using the Medicaid IHS Program claims payment data for IHS AIAN Medicaid recipients we can calculate the<br />
expected Mean Medicaid IHS Program Payment per IHS Active User to IHS and Tribal (I/T) providers. We<br />
substitute the unadjusted Mean Medicaid IHS Program Payment per IHS AIAN Recipient for the Total Payment<br />
in the calculations in Table 14 to obtain the percents in Figure 16.<br />
When the outcomes are expressed as a percent of the FDI Adjusted Benchmark Cost, the Areas with I/T<br />
providers with the lowest reported Alternate Resources for IHS Active User Medicaid enrollees are Nashville<br />
(2%), Bemidji (4%), Oklahoma (4%) and California (6%), (Figure 15). For Portland, Albuquerque, and Aberdeen<br />
Areas only 8% of all Medicaid payments are to IHS and Tribal providers for health care costs of their Active<br />
Users, and Alaska Area is only 9%. Medicaid resources Billings (12%), Navajo (19%), Phoenix (21%), and<br />
Tucson Areas (24%) have the highest relative Medicaid resources.<br />
39<br />
65%<br />
0% 20% 40% 60% 80% 100%<br />
Percent of FDI Benchmark Cost<br />
All Providers
Findings<br />
Figure 21. Medicaid Alternate Resources paid to I/T providers as percent of IHS calculated FDI benchmark health care costs<br />
for IHS Active Users in each Area.<br />
Nashville<br />
Oklahoma<br />
Bemidji<br />
California<br />
Portland<br />
Albuquerque<br />
Aberdeen<br />
Alaska<br />
Billings<br />
Navajo<br />
Phoenix<br />
Tucson<br />
2%<br />
4%<br />
4%<br />
6%<br />
8%<br />
8%<br />
8%<br />
9%<br />
12%<br />
19%<br />
21%<br />
24%<br />
0% 20% 40% 60% 80% 100%<br />
Percent of FDI Benchmark Cost<br />
40<br />
I/T Providers
Conclusions and Recommendations<br />
IHS AIAN Payments Compared to Others<br />
There is no evidence on a national basis that Medicaid per capita payments for the AIAN user population of IHS<br />
Programs (IHS AIAN) in 2006 are lower than for other Medicaid recipients. Overall in 9 of the 12 IHS Areas<br />
Medicaid payments for personal health care services of IHS AIAN were as high as or higher than either selfdeclared<br />
AIAN who did not use the IHS health care system and of whites living in the same counties. The<br />
exceptions to the general finding in four IHS Areas were: In Albuquerque Area the per capita payments overall<br />
were higher than those of self-declared AIAN who did not use the IHS system, but not higher than Whites. In<br />
Oklahoma Area the payments were higher than for Whites, but not the AIAN who did not use the IHS system. In<br />
Aberdeen and Billings Areas the payments were lower for most types of IHS AIAN Medicaid recipients analyzed<br />
when compared to other AIAN or whites. For the Nashville Area the conclusion requires acknowledgment that<br />
the Medicaid total payments are higher because Third Party payments for Medicaid claims were included in the<br />
total per capita payment analyzed for all the IHS areas. In the Nashville Area the contribution to the total per<br />
capita payment for Medicaid claims due to private insurance is substantial. Nashville Area also was unlike other<br />
Areas in the large number of states that do not report any IHS Program claims. Nashville Area has many states<br />
and counties, but many states have IHS system providers with small numbers of Active Users. These state<br />
Medicaid programs when interviewed were more likely to acknowledge in 2010 they had no special activities to<br />
identify IHS or tribal provider Medicaid claims (Korenbrot and Crouch, 2010).<br />
In the Tucson, Navajo and Phoenix Areas the payments for the AIAN user population of IHS Programs were<br />
highest, which was found to be attributable to the payment levels in the state of Arizona. When Medicaid<br />
recipients in Arizona were excluded, the AIAN payments for Navajo and Phoenix Areas relative to other AIAN<br />
and whites became more like those in other Areas (the Tucson Area is entirely within Arizona and could not be<br />
analyzed with the exclusion of Arizona Medicaid recipients).<br />
In making these comparisons, payments for six different types of Medicaid service recipients were analyzed.<br />
Medicaid recipients were classified depending on whether they were under age 65 or not, enrolled all year in<br />
Medicaid or not, and whether they received only fee-for-service (FFS) medical care or had any of their medical<br />
services in managed care. The payments for each type of Medicaid recipient were risk-adjusted for differences<br />
between the IHS AIAN and comparison groups with respect to age, sex, disability, and dual-enrollment with<br />
Medicare. Adjustments for differences among the groups in morbidity were possible for those enrolled all year<br />
in Medicaid, but not those enrolled less than a year. The payments were also adjusted for variation in health<br />
care prices across the IHS Areas whether analyzed as mean payment per year for recipients enrolled all year, or<br />
mean payment per month for when recipients were analyzed regardless of length of enrollment.<br />
The findings were not found to depend on any particular type of Medicaid recipient analyzed. For any given<br />
Area one or more of the recipient types the AIAN user population might have an adjusted mean per capita<br />
payment higher or lower than a comparison group. One of the implications of this finding is that the overall,<br />
results did not depend on whether the payments were adjusted for differences in morbidity or not, or whether<br />
they received their medical care in a FFS or managed care system.<br />
The IHS AIAN FFS per capita payments were dominated by outpatient services (including claims for clinic,<br />
medical care practitioners, laboratory and imaging, and dental services). Inpatient payments were a small<br />
41
Conclusions and Recommendations<br />
proportion of overall payments. Prescription drug payments contributed little to the payments for IHS AIAN<br />
compared to their contribution to payments for Other AIAN or whites. There were almost no payments for IHS<br />
Program claims for prescription drugs outside of the Bemidji Area.<br />
This evidence supports the general conclusion that in most Areas the IHS system providers and the state<br />
Medicaid programs with which they interface in these Areas are as a whole are doing a well at billing and<br />
collection for services provided to Medicaid enrolled users of the IHS system. In Aberdeen, Billings,<br />
Albuquerque and Oklahoma Areas, however, it is possible that either IHS system or other providers who<br />
provide care for these AIAN do not file as many claims, or are denied more claims for their care. It is also<br />
possible that in Albuquerque Area the reason that lower payments were found only compared to self-declared<br />
AIAN who do not use the IHS system is because these other AIAN have higher demands for health care when ill<br />
because they are not in the IHS system. The morbidity risk-adjustment is only a partial adjustment for health<br />
status differences, because it depends on people accessing their Medicaid health care provider over the year to<br />
have information on health status to adjust.<br />
Medicaid-enrolled IHS Active Users without IHS Program Medicaid claims<br />
IHS Active Users with Medicaid claims but no IHS Program Medicaid claims had substantially lower payments<br />
over all the recipient types analyzed. The per capita payments for this subgroup of IHS AIAN were substantially<br />
lower for all types of Medicaid recipients analyzed than those of: 1) other IHS AIAN with IHS Program Medicaid<br />
claims, 2) other AIAN who did not use the IHS system, and 3) whites living in the same counties. This was found<br />
as an overall conclusion for all IHS Areas when the compared to the IHS AIAN with IHS Program Medicaid<br />
claims. This was found for all but one IHS Area compared to other AIAN (Nashville) and for one IHS Area<br />
compared to whites (Tucson). The payments were risk-adjusted and therefore it is not likely that they are<br />
lower because these are healthier IHS AIAN than the other groups of IHS AIAN. This finding supports the<br />
conclusion that IHS system providers may not be doing all the billing and collections of Medicaid for care they<br />
have provided to their IHS user population.<br />
Medicaid-paid Fraction of IHS Active User Costs<br />
The fraction of health care costs needed by the IHS Active User population that is paid by Medicaid (and<br />
Medicaid-CHIP) is 25% or more in 9 of 12 IHS Areas, but varied from 19% to 65% depending on the IHS Area.<br />
Areas with the lowest fraction of about one-fifth are Nashville (19%) and Oklahoma (21%). Aberdeen,<br />
California, Albuquerque, Portland and Bemidji Areas have mid-range fractions of between a little more than one<br />
quarter and a little less than one-third (27% to 31%). Alaska and Billings are in the middle of the Area rankings<br />
with a little more than one-third of the costs paid by Medicaid (34% to 38%). And Navajo and Phoenix have<br />
Medicaid fractions of nearly one half (46% and 49% respectively). Tucson has the highest Medicaid paid<br />
fraction of nearly two-thirds (65%).<br />
When the amounts paid by Medicaid to IHS and tribal providers are separated out of the Medicaid fraction and<br />
compared to the total health care costs of their user population, the Areas with the lowest reported Medicaid<br />
fraction paid to IHS and tribal providers by Medicaid are Nashville (2%), Bemidji (4%), Oklahoma (4%) and<br />
California (6%). For Portland, Albuquerque, and Aberdeen Areas only 8% the total health care costs needed by<br />
their user population are paid to IHS and tribal providers by Medicaid, and in Alaska Area it is only 9%. Billings<br />
(12%), Navajo (19%), Phoenix (21%), and Tucson Areas (24%) receive the highest Medicaid fractions.<br />
42
References<br />
Barbero C, Milhollin E, 2012. Legal Basis for Special CMS Provisions for American <strong>Indian</strong>s and Alaska Natives,<br />
2012. Hobbs, Straus, Dean and Walker, LLP, legal technical advisors to the CMS Tribal Technical Advisory<br />
Group. [Will be posted online by the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> www.nihb.org] Available upon request.<br />
Center for Medicare and Medicaid Services. 2005. American <strong>Indian</strong> and Alaska Native Strategic Plan, 2006-<br />
2010. CMS TTAG. [Online January 22, 2010] www.cmsttag.org/policy.html<br />
Centers for Medicare and Medicaid Services. 2007. 2006 CMS Statistics. CMS Research Documents. [Online<br />
December 12, 2009] www.cms.hhs.gov/ResearchGenInfo<br />
Crouch J, Garrow R, Kao C, Harklerode R, Korenbrot C. 2009. American <strong>Indian</strong> and Alaska Native Medicaid<br />
Program and Policy Statistics: Summary Report. A Report for the Center for Medicare and Medicaid Services<br />
from the Technical Tribal Advisory Group. California Rural <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>. [Online August 14, 2012]<br />
http://crihb.org/files/2_AIAN%20Medicaid%20Report_%202009.pdf<br />
Crouch J, Kao C, Garrow R, Korenbrot J, Korenbrot C. 2010. American <strong>Indian</strong> and Alaska Native Medicaid<br />
Program and Policy Data. [Online August 14, 2012] http://crihb.org/files/0_Medicaid_Report_6_2_2010.pdf<br />
Crouch J, Kao C, Garrow R, Korenbrot J, Korenbrot C. 2009. American <strong>Indian</strong> and Alaska Native Medicare<br />
Program and Policy Statistics: Summary Report. A Report for the Center for Medicare and Medicaid Services<br />
from the Technical Tribal Advisory Group. California Rural <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>. [Online August 14, 2012]<br />
http://crihb.org/files/3_AIAN%20Medicare%20Statistics_2009.pdf<br />
Crouch J, Kao C, Korenbrot C. 2007. Gaps and Strategies to improve American <strong>Indian</strong> and Alaska Native Data<br />
in Medicare, Medicaid and SCHIP Data Bases, August 2007. A Report for the Center for Medicare and Medicaid<br />
Services from the Technical Tribal Advisory Group. California Rural <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>. [Online August 14,<br />
2012] http://crihb.org/files /2007_CMS_Data_Report.doc<br />
Crouch J, Kao C, Korenbrot C. 2011. Integrating Medicaid and <strong>Indian</strong> <strong>Health</strong> Service Data. A Report for the<br />
Center for Medicare and Medicaid Services from the Technical Tribal Advisory Group. California Rural <strong>Indian</strong><br />
<strong>Health</strong> <strong>Board</strong>. [Online August 14, 2012] http://crihb.org/files/integrating_medicaid_and_ihs_data.pdf<br />
Crouch J, Kao C, Korenbrot J, Korenbrot C. 2011. AIAN Medicaid Data Linked to <strong>Indian</strong> <strong>Health</strong> Service Data:<br />
Medicaid and CHIP Enrollment, Service Use and Payments. A Report for the Center for Medicare and Medicaid<br />
Services from the Technical Tribal Advisory Group. California Rural <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>. [Online August 14,<br />
2012] http://crihb.org/files/0.Medicaid_Report 7_27_11.pdf<br />
<strong>Indian</strong> <strong>Health</strong> Service, 2008. FDI IHS Cost per User Calculations for Sites. [Online August 23, 2012]<br />
http://www.ihs.gov/NonMedicalPrograms/lnf/2008/FDICOSTPERUSERCALCULATIONS.pdf<br />
<strong>Indian</strong> <strong>Health</strong> Service, 2008. FDI IHS Funds per User Calculations for Sites. [Online August 23, 2012]<br />
http://www.ihs.gov/NonMedicalPrograms/lnf/2008/FDIFUNDSPERUSERCALCULATIONS.pdf<br />
<strong>Indian</strong> <strong>Health</strong> Service, 2009. Federal Disparity Index, FDI Results and IHCIF Formula Results [Online August 17,<br />
2012] http://www.ihs.gov/NonMedicalPrograms/lnf/<br />
43
<strong>Indian</strong> <strong>Health</strong> Service, 2012. Federal Basis of <strong>Health</strong> Services. [Online August 24, 2012]<br />
www.ihs.gov/PublicAffairs/IHSBrochure/BasisHlthSvcs.asp<br />
<strong>Indian</strong> <strong>Health</strong> Service, 2011. <strong>National</strong> Data Warehouse. [Online July 8, 2011] http://www.ihs.gov/NDW<br />
<strong>Indian</strong> <strong>Health</strong> Services, 2012. Federal Disparity Index, <strong>Indian</strong> <strong>Health</strong> Manual Part 6, Chapter 4: Manual<br />
Exhibit, Manual Exhibit 6-4-A [Online August 17, 2012<br />
http://www.ihs.gov/IHM/index.cfm?module=dsp_ihm_pc_p6c4_ex<br />
Korenbrot C, Crouch J. 2010. American <strong>Indian</strong>s and Alaska Natives: Medicaid State Data Collection. A Report<br />
for the Center for Medicare and Medicaid Services from the Technical Tribal Advisory Group. [Online August<br />
14, 2012] http://www.crihb.org/policy-in-action/research/national-research-documents.html<br />
Korenbrot C, Kao C, Crouch J. 2009. Funding of Tribal <strong>Health</strong> Programs linked to higher rates of<br />
hospitalization for conditions sensitive to ambulatory care. Medical Care. 2009, Vol. 47, pp. 88-96.<br />
http://crihb.org/files/3_IHS%20Funding%20effects%202009.pdf<br />
Wenzlow AT, et al. 2007. Medicaid Extract Chartbook. Centers for Medicare and Medicaid Services. [Online<br />
January 28, 2010] http://www.cms.hhs.gov/MedicaidDataSourcesGenInfo/downloads/MAX_Chartbook_2007.pdf<br />
Winkelman, R, Damler, R. Risk Adjustment in State Medicaid Programs. <strong>Health</strong> Watch. 2008, No. 57, pp. 14 -<br />
19.<br />
Wong S, Kao C, Crouch J, Korenbrot CC. 2006. Rural American <strong>Indian</strong> Medicaid <strong>Health</strong> Care Use and Costs in<br />
California. American Journal of Public <strong>Health</strong>. 2006, Vol. 96, pp. 363-70.<br />
http://crihb.org/files/4_Disparities%20in%20Medicaid%20use%20in%20California.pdf<br />
44
Dear Tribal Leader:<br />
THE SECRETARY OF HEALTH AND HUMAN SERVICES<br />
WASHINGTON, D.C. 20201<br />
October 19, 20 12<br />
The Department of <strong>Health</strong> and Human Services (HHS) has been a leader in the federal<br />
government's efforts to improve its partnership with tribes. I am proud of our current<br />
government-to-government relationship with tribes from across the country. HHS continuously<br />
strives to find innovative and meaningful ways to work with you and your communities. One<br />
mechanism to ensure this collaboration is our Tribal Consultation Policy (TCP).<br />
At the very start of this administration, I requested your feedback and input with updating our<br />
TCP. I then created a federal tribal workgroup to coordinate all of your comments and<br />
recommendations. As a result of that work, in December 201 0, I signed the updated TCP. In<br />
that revision, HHS committed to evaluating that policy every few years, and that is why I write<br />
you today.<br />
In accordance with that policy, HHS has conducted tribal consultation in a variety of ways over<br />
the years, including: conference calls; direct correspondence to tribal leadership; meetings with<br />
tribal leadership at the local, area, or national levels; and national and regional consultations.<br />
Tribal leaders have indicated their agreement with current HHS policy, but we are always<br />
looking to make improvements.<br />
I am interested in your thoughts and views regarding our current TCP. I would appreciate it if<br />
you would take the time to review and evaluate our TCP and provide your feedback on what is<br />
working, what isn't, and what we can do to improve our activities to ensure meaningful tribal<br />
consultation policy. This will greatly assist us in our evaluation of the policy. Here is the link to<br />
our current policy for your review: http:ll~~ww.hhs.gov/intergovernmental/tribal/tcp.html.<br />
I ask that you provide us with your feedback by submitting your comments by Friday,<br />
December 7,2012. Comments can be sent to:<br />
Stacey Ecoffey, Principal Advisor for Tribal Affairs<br />
Office of Intergovernmental and External Affairs<br />
U.S. Department of <strong>Health</strong> and Human Services<br />
200 Independence Ave SW Room 620-E<br />
Washington, DC 2020 1<br />
Email: Consultation~,hhs.gov<br />
If you have further questions or concerns please feel free to contact Stacey Ecoffey, Principal<br />
Advisor for Tribal Affairs, via email at Stacev.Ecoffey@,hhs.aov or via phone at (202) 690-6060.<br />
Thank you in advance for your contribution and commitment to a strong HIIS Tribal<br />
Consultation Policy. 1 look forward to our continued partnership.<br />
Gthleen Sebelius
Tribal Consultation Policy HHS<br />
1. PURPOSE<br />
The U. S. Department of <strong>Health</strong> and Human Services (HHS) and <strong>Indian</strong> Tribes share the goal to<br />
establish clear policies to further the government-to-government relationship between the<br />
Federal Government and <strong>Indian</strong> Tribes. True and effective consultation shall result in information<br />
exchange, mutual understanding, and informed decision-making on behalf of the Tribal<br />
governments involved and the Federal Government. The importance of consultation with <strong>Indian</strong><br />
Tribes was affirmed through Presidential Memoranda in 1994, 2004 and 2009, and an Executive<br />
Order (EO) in 2000.<br />
The goal of this policy includes, but is not limited to, eliminating health and human service<br />
disparities of <strong>Indian</strong>s, ensuring that access to critical health and human services is maximized,<br />
and to advance or enhance the social, physical, and economic status of <strong>Indian</strong>s. To achieve this<br />
goal, and to the extent practicable and permitted by law, it is essential that Federally-recognized<br />
<strong>Indian</strong> Tribes and the HHS engage in open, continuous, and meaningful consultation.<br />
This policy applies to all Divisions of the Department and shall serve as a guide for Tribes to<br />
participate in all Department and Division policy development to the greatest extent practicable<br />
and permitted by law.<br />
2. BACKGROUND<br />
Since the formation of the Union, the United States (U.S.) has recognized <strong>Indian</strong> Tribes as<br />
sovereign nations. A unique government-to-government relationship exists between <strong>Indian</strong><br />
Tribes and the Federal Government. This relationship is grounded in the U.S. Constitution,<br />
numerous treaties, statutes, Federal case law, regulations and executive orders that establish<br />
and define a trust relationship with <strong>Indian</strong> Tribes. This relationship is derived from the political<br />
and legal relationship that <strong>Indian</strong> Tribes have with the Federal Government and is not based<br />
upon race.<br />
An integral element of this government-to-government relationship is that consultation occurs<br />
with <strong>Indian</strong> Tribes. The Executive Memorandum titled “Tribal Consultation” reaffirmed this<br />
government-to-government relationship with <strong>Indian</strong> Tribes on November 5, 2009. The<br />
implementation of this policy is in recognition of this special relationship.<br />
This special relationship is affirmed in statutes and various Presidential Executive Orders<br />
including, but not limited to:<br />
o Older Americans Act, P.L. 89-73, as amended;<br />
o <strong>Indian</strong> Self-Determination and Education Assistance Act, P.L. 93-638, as amended;<br />
o Native American Programs Act, P.L. 93-644, as amended;<br />
o <strong>Indian</strong> <strong>Health</strong> Care Improvement Act, P.L. 94-437, as amended;<br />
o Personal Responsibility and Work Opportunity Reconciliation Act of 1996, P.L.104-193;<br />
o Presidential Executive Memorandum to the Heads of Executive Departments dated April 29,<br />
1994;<br />
o Presidential Executive Order 13175, Consultation and Coordination with <strong>Indian</strong> Tribal<br />
Governments, November 6, 2000; and<br />
o Presidential Memorandum, Government-to-Government Relationship with Tribal<br />
Governments, September 23, 2004<br />
o Presidential Memorandum, Tribal Consultation, November 5, 2009
o American Recovery and Reinvestment Act of 2009, P.L. 111-5, 123 Stat. 115 (Feb. 17,<br />
2009).<br />
o Children's <strong>Health</strong> Insurance Program Reauthorization Act of 2009, P.L. 111-3, 123 Stat. 8<br />
(Feb. 4, 2009).<br />
o Patient Protection and Affordable Care Act of 2010, P.L. 111-148, 124 Stat. 119 (Mar. 23,<br />
2010).<br />
3. TRIBAL SOVEREIGNTY<br />
This policy does not waive any Tribal Governmental rights and authority, including treaty rights,<br />
sovereign immunities or jurisdiction. Additionally, this policy does not diminish any rights or<br />
protections afforded other American <strong>Indian</strong>s or Alaskan Natives (AI/AN) or entities under Federal<br />
law.<br />
The special government-to-government relationship between the Federal Government and<br />
<strong>Indian</strong> Tribes, established in 1787, is based on the Constitution, and has been given form and<br />
substance by numerous treaties, laws, Supreme Court decisions, and Executive Orders, and<br />
reaffirms the right of <strong>Indian</strong> Tribes to self-government and self-determination. <strong>Indian</strong> Tribes<br />
exercise inherent sovereign powers over their citizens and territory. The U.S. shall continue to<br />
work with <strong>Indian</strong> Tribes on a government-to-government basis to address issues concerning<br />
Tribal self-government, Tribal trust resources, Tribal treaties and other rights.<br />
Tribal self-government has been demonstrated to improve and perpetuate the government-togovernment<br />
relationship and strengthen Tribal control over Federal funding that it receives, and<br />
its internal program management. <strong>Indian</strong> Tribes participation in the development of public health<br />
and human services policy ensures locally relevant and culturally appropriate approaches to<br />
public issues.<br />
4. POLICY<br />
Before any action is taken that will significantly affect <strong>Indian</strong> Tribes it is the HHS policy that, to<br />
the extent practicable and permitted by law, consultation with <strong>Indian</strong> Tribes will occur. Such<br />
actions refer to policies that:<br />
1. Have Tribal implications, and<br />
2. Have substantial direct effects on one or more <strong>Indian</strong> Tribes, or<br />
3. On the relationship between the Federal Government and <strong>Indian</strong> Tribes, or<br />
4. On the distribution of power and responsibilities between the Federal Government and<br />
<strong>Indian</strong> Tribes.<br />
Nothing in this policy waives the Government’s deliberative process privilege. Examples of the<br />
government’s deliberative process privilege are as follows:<br />
5. The Department is specifically requested by Members of Congress to respond to or report<br />
on proposed legislation, the development of such responses and of related policy is a part<br />
of the Executive Branch’s deliberative process privilege and should remain confidential.<br />
6. In specified instances Congress requires the Department to work with <strong>Indian</strong> Tribes on the<br />
development of recommendations that may require legislation, such reports,<br />
recommendations or other products are developed independent of a Department position,<br />
the development of which is governed by Office of Management and Budget (OMB) Circular<br />
A-19.<br />
A. Each HHS Operating and Staff Division (Division) shall have an accountable process as
defined in Sections 8 and 9 of this policy to ensure meaningful and timely input by <strong>Indian</strong> Tribes<br />
in the development of policies that have Tribal implications. If Divisions require technical<br />
assistance in implementing these sections, the Office of Intergovernmental Affairs (IGA) can<br />
provide and/or coordinate assistance.<br />
B. To the extent practicable and permitted by law, no Division shall promulgate any regulation<br />
that has Tribal implications, or that imposes substantial direct compliance costs on <strong>Indian</strong> Tribes,<br />
or that is not required by statute, unless:<br />
7. Funds necessary to pay the direct costs incurred by the <strong>Indian</strong> Tribe in complying with the<br />
regulation are provided by the Federal Government; or<br />
8. The Division, prior to the formal promulgation of the regulation,<br />
a. Consulted with <strong>Indian</strong> Tribes throughout all stages of the process of developing the<br />
proposed regulation;<br />
b. Provided a Tribal summary impact statement in a separately identified portion of the<br />
preamble to the regulation as it is to be issued in the Federal Register (FR), which<br />
consists of a description of the extent of the Division's prior consultation with <strong>Indian</strong><br />
Tribes, a summary of the nature of their concerns and the Division's position<br />
supporting the need to issue the regulation, and a statement of the extent to which<br />
the concerns of Tribal officials have been met; and<br />
c. Made available to the Secretary and to the Director of OMB any written<br />
communications submitted to the Division by Tribal officials.<br />
C. To the extent practicable and permitted by law, no Division shall promulgate any regulation<br />
that has Tribal implications and that preempts Tribal law unless the Division, prior to the formal<br />
promulgation of the regulation,<br />
9. Consulted with Tribal officials throughout all stages of the process of developing the<br />
proposed regulation;<br />
10. Provided a Tribal summary impact statement in a separately identified portion of the<br />
preamble to the regulation as it is to be issued in the FR, which consists of a description of<br />
the extent of the Division's prior consultation with Tribal officials, a summary of the nature<br />
of their concerns and the Division's position supporting the need to issue the regulation,<br />
and a statement of the extent to which the concerns of Tribal officials have been met; and<br />
11. Made available to the Secretary any written communications submitted to the Division by<br />
Tribal officials.<br />
D. On issues relating to Tribal self-governance, Tribal self-determination, Tribal trust resources,<br />
or Tribal treaty and other rights, each Division shall make all practicable attempts where<br />
appropriate to use consensual mechanisms for developing regulations, including negotiated<br />
rulemaking.<br />
5. PHILOSOPHY<br />
<strong>Indian</strong> Tribes have an inalienable and inherent right to self-government. Self-government means<br />
government in which decisions are made by the people who are most directly affected by the<br />
decisions. As sovereign nations, <strong>Indian</strong> Tribes exercise inherent sovereign powers over their<br />
members, territory and lands.<br />
HHS has a long-standing commitment to working on a government-to-government basis with<br />
<strong>Indian</strong> Tribes and to work in partnership with AI/ANs. Also, HHS is committed to enhancing the<br />
collaboration among its Divisions to address Tribal issues and promoting the principle that each<br />
Division bears responsibility for addressing Tribal issues within the context of their mission.
IGA is identified as the responsible HHS entity, located in the Immediate Office of the Secretary<br />
(IOS) for monitoring compliance with EO 13175 and the Department Tribal Consultation Policy.<br />
In addition, the Secretary has charged the Intradepartmental Council on Native American Affairs<br />
(ICNAA) to meet regularly and no less then 2 times a year and to provide advice on all HHS<br />
policies that relate to <strong>Indian</strong> Tribes as well as instances where HHS activities relate to Native<br />
Americans. Regional consultation sessions have been developed as a systematic method to<br />
regularly consult with <strong>Indian</strong> Tribes on HHS programs at field locations. The goal of these efforts<br />
is to focus HHS on Tribal issues, to continue to enhance the government-to-government<br />
relationship between <strong>Indian</strong> Tribes and the U.S., as well as to make resources of HHS more<br />
readily available to <strong>Indian</strong> Tribes.<br />
6. OBJECTIVES<br />
0. To formalize the Administration’s policy that HHS seek consultation and the participation of<br />
<strong>Indian</strong> Tribes in the development of policies and program activities that impact <strong>Indian</strong><br />
Tribes.<br />
1. To establish a minimum set of requirements and expectations with respect to consultation<br />
and participation throughout HHS management, the Office of the Secretary (OS) Division,<br />
and Regional levels.<br />
2. The need to consult may be identified by the Department or by an <strong>Indian</strong> Tribe(s). Any<br />
time the Tribe(s) or the Department identifies a critical event the Department may initiate<br />
any necessary consultation in accordance with this policy.<br />
3. To identify events and partnerships that HHS would participate with <strong>Indian</strong> Tribe(s) and<br />
Tribal/<strong>Indian</strong> Organizations that establish and foster partnerships with HHS which<br />
complement and enhance consultation with <strong>Indian</strong> Tribes.<br />
4. To promote and develop innovative consultation methods with <strong>Indian</strong> Tribes in the<br />
development of HHS policy and regulatory processes.<br />
5. To uphold the responsibility of HHS to consult with <strong>Indian</strong> Tribes on new and existing<br />
health and human service policies, programs, functions, services and activities that have<br />
Tribal implications.<br />
6. To charge and hold accountable each of the HHS Operating Division Heads for the<br />
implementation of this policy.<br />
7. To be responsive to requests by an <strong>Indian</strong> Tribe(s) request for consultation and technical<br />
assistance in obtaining HHS resources.<br />
8. To charge the HHS Operating Divisions with the responsibility for enhancing partnerships<br />
with <strong>Indian</strong> Tribes which will include, requests for technical assistance, access to programs<br />
and resources, as well as collaborating with Tribal subject matter expertise.<br />
9. To provide a single point of contact within HHS and its Operating Divisions for <strong>Indian</strong> Tribes<br />
at the highest level which would have access to the IOS, the Deputy Secretary, and<br />
Operating Division Heads. The Principal Advisor for Tribal Affairs and the Division Tribal<br />
points of contact will be responsible for compliance with this policy and ensuring<br />
timeframes identified in section 9 are met.<br />
7. CONSULTATION PARTICIPANTS AND ROLES<br />
0. <strong>Indian</strong> Tribes: The government-to-government relationship between the U.S. and<br />
Federally recognized <strong>Indian</strong> Tribes dictates that the principal focus for HHS consultation is<br />
<strong>Indian</strong> Tribes, individually or collectively.<br />
1. <strong>Indian</strong> Organizations: At times it is useful that the HHS communicate with <strong>Indian</strong><br />
organizations to solicit <strong>Indian</strong> Tribe(s) advice and recommendations. The government does<br />
not participate in government-to-government consultations with these entities; rather<br />
these organizations represent the interest of <strong>Indian</strong> Tribes when authorized by those Tribes<br />
These organizations by the sheer nature of their business serve and advocate <strong>Indian</strong> Tribes<br />
issues and concerns that might be negatively affected if these organizations were excluded<br />
from the process.
2. Office of Intergovernmental Affairs (IGA): IGA is responsible for Department-wide<br />
implementation and monitoring of EO 13175 for HHS Tribal consultation. IGA serves as the<br />
Department’s point of contact in accessing department-wide information. The single point<br />
of contact within the IGA for <strong>Indian</strong> Tribes and other Tribal/<strong>Indian</strong> organizations, at a level<br />
with access to all HHS Divisions, is the Principal Advisor for Tribal Affairs. As a part of the<br />
IOS, IGA’s mission is to facilitate communication regarding HHS initiatives as they relate to<br />
Tribal, State, and local governments. IGA is the Departmental liaison to States and <strong>Indian</strong><br />
Tribes, and serves the dual role of representing the States and Tribal perspective in the<br />
Federal policymaking process, as well as, clarifying the Federal perspective to States and<br />
<strong>Indian</strong> Tribes, including Tribal consultation.<br />
3. Assistant Secretary for Finance and Resources (ASFR): ASFR is the lead office for<br />
budget consultation for the overall departmental budget request.<br />
4. HHS Divisions: The Department has numerous Staff Divisions and Operating Divisions<br />
under its purview. Each of the these Divisions share in the Department-wide responsibility<br />
to coordinate, communicate and consult with <strong>Indian</strong> Tribes on issues that affect these<br />
governments. All Operating Divisions shall establish a Tribal consultation policy to comply<br />
with the HHS Policy. All Divisions are responsible for conducting Tribal consultation to the<br />
extent practicable and permitted by law on policies that have Tribal implications.<br />
5. Intradepartmental Council on Native American Affairs(ICNAA): The ICNAA is<br />
charged with: (1) develop and promote an HHS policy to provide greater access and<br />
quality services for AI/AN/NAs throughout the Department; (2) promote implementation of<br />
HHS policy and Division plans on consultation with <strong>Indian</strong> Tribes in accordance with<br />
statutes and EOs; (3) promote an effective, meaningful AI/AN/NA policy to improve health<br />
and human services for AI/AN/NAs; (4) develop a comprehensive Departmental strategy<br />
that promotes self-sufficiency and self-determination for all <strong>Indian</strong> Tribes and AI/AN/NA<br />
people; (5) promote the Tribal/Federal Government-to-government relationship on an<br />
HHS-wide basis in accordance with EO 13175; and (6) operate in accordance with policy<br />
and timeframes identified within ICNAA charter and as directed by the Secretary and the<br />
ICNAA Executive Leadership.<br />
6. Regional Offices: The ten (10) HHS Regional Offices share in the Department-wide<br />
responsibility to consult, coordinate and communicate with <strong>Indian</strong> Tribes on issues that<br />
affect <strong>Indian</strong> Tribes and HHS programs, services and resources available to <strong>Indian</strong> Tribes<br />
through States. The Regional Directors are the Secretary’s immediate representatives in<br />
the field for the HHS. Each of the Regional Office(s) shall conduct an annual regional Tribal<br />
consultation meeting with <strong>Indian</strong> Tribes in their respective regions. Additional meetings<br />
may be conducted if requested by the Regional Director or an <strong>Indian</strong> Tribe(s) within the<br />
Region. Further, the Regional Directors will work closely with the respective <strong>Indian</strong> Tribes<br />
and State Governments to assure continuous coordination and communication between<br />
Tribes and States. The Regional Office Directors will promote and comply with this policy<br />
and its timeframes identified in Section 9.<br />
8. TRIBAL CONSULTATION PROCESS<br />
An effective consultation between HHS and <strong>Indian</strong> Tribes requires trust between all parties which<br />
is an indispensable element in establishing a good consultative relationship. The degree and<br />
extent of consultation will depend on the identified critical event. A critical event may be<br />
identified by HHS and/or an <strong>Indian</strong> Tribe(s). Upon identification of an event significantly affecting<br />
one or more <strong>Indian</strong> Tribe(s), HHS will initiate consultation regarding the event. In order to<br />
initiate and conduct consultation, the following serves as a guideline to be utilized by HHS and<br />
<strong>Indian</strong> Tribes:<br />
0. Identify the Critical Event: Complexity, implications, time constraints, and issue(s)<br />
(including policy, funding/budget development, programs, services, functions and<br />
activities).
1. Identify affected/potentially affected <strong>Indian</strong> Tribe(s)<br />
2. Determine Consultation Mechanism – The most useful and appropriate consultation<br />
mechanisms can be determined by HHS and/or <strong>Indian</strong> Tribe(s) after considering the critical<br />
event and <strong>Indian</strong> Tribe(s) affected/potentially affected. Consultation mechanisms include<br />
but are not limited to one or more of the following:<br />
a. Mailings<br />
b. Teleconference<br />
c. Face-to-Face Meetings at the Local, Regional and <strong>National</strong> levels between the HHS<br />
and <strong>Indian</strong> Tribes.<br />
d. Roundtables<br />
e. Annual HHS Tribal Budget and Policy Consultation Sessions.<br />
f. Other regular or special HHS Division or program level consultation sessions.<br />
A. Communication Methods: The determination of the critical event and the level of consultation<br />
mechanism to be used shall be communicated to affected/potentially affected <strong>Indian</strong> Tribe(s)<br />
using all appropriate methods and with as much advance notice as practicable. These methods<br />
include but are not limited to the following:<br />
3. Correspondence: Written communications shall be issued within 30 calendar days of an<br />
identified critical event. The communication should clearly provide affected/potentially<br />
affected <strong>Indian</strong> Tribe(s) with detail of the critical event, the manner and timeframe in<br />
which to provide comment. The HHS frequently uses a “Dear Tribal Leader Letter” (DTLL)<br />
format to notify individual <strong>Indian</strong> Tribes of consultation activities. Divisions should work<br />
closely with the Principal Advisor for Tribal Affairs, IOS/IGA if technical assistance is<br />
required for proper format and protocols, current mailing lists, and content.<br />
4. Official Notification: Within 30 calendar days, and upon the determination the consultation<br />
mechanism, proper notice of the critical event and the consultation mechanism utilized<br />
shall be communicated to affected/potentially affected <strong>Indian</strong> Tribe(s) using all appropriate<br />
methods including mailing, broadcast e-mail, FR, and other outlets. The FR is the most<br />
formal HHS form of notice used for consultation.<br />
5. Meeting(s): The Division shall convene a meeting, within 60 calendar days of official<br />
notification, with affected/potentially affected <strong>Indian</strong> Tribe(s) to discuss all pertinent issues<br />
in a national, regional, and/or local forum, or as appropriate, to the extent practicable and<br />
permitted by law, when the critical event is determined to have substantial impact.<br />
6. Receipt of Tribal Comment(s): The Division shall develop and use all appropriate methods<br />
to communicate clear and explicit instructions on the means and time frames for <strong>Indian</strong><br />
Tribe(s) to submit comments on the critical event, whether in person, by teleconference,<br />
and/or in writing and shall solicit the advice and assistance of the Principal Advisor for<br />
Tribal Affairs, IOS/IGA.<br />
7. Reporting of Outcome: The Division shall report on the outcomes of the consultation within<br />
90 calendar days of final consultation. For ongoing issues identified during the consultation,<br />
the Division shall provide status reports throughout the year to IOS/IGA and <strong>Indian</strong><br />
Tribe(s).<br />
A. HHS Response to Official Tribal Correspondence: Official correspondence from an <strong>Indian</strong> Tribe<br />
may come in various forms, but a resolution is the most formal declaration of an <strong>Indian</strong> Tribe’s<br />
position for the purpose of Tribal consultation. In some instances, <strong>Indian</strong> Tribes will submit<br />
official correspondence from the highest elected and/or appointed official(s) of the Tribe. HHS
will give equal consideration to these types of correspondence. Once HHS receives an official<br />
<strong>Indian</strong> Tribe correspondence and/or resolution, the Secretary/Deputy Secretary and/or their<br />
designee should respond appropriately. The process for official correspondence to <strong>Indian</strong> Tribes<br />
is described below:<br />
8. Correspondence submitted by <strong>Indian</strong> Tribes to HHS shall be officially entered into HHS<br />
correspondence control tracking system and referred to the appropriate Division(s).<br />
9. Acknowledgement of Correspondence: HHS and/or Divisions shall provide<br />
acknowledgement to <strong>Indian</strong> Tribes within 15 working days of receipt.<br />
10. Official Response to an identified critical event: HHS shall provide an official response to<br />
<strong>Indian</strong> Tribes that includes: the Division head responsible for follow up, the process for<br />
resolution of the critical event and timeline for resolution.<br />
a. If an identified critical event is national in scope the Department shall to the extent<br />
practicable respond to the request within 60 working days or less.<br />
b. If a critical event is specific to a single <strong>Indian</strong> Tribe the Department shall to the<br />
extent practicable respond to the request within 45 working days or less.<br />
B. Policy Development through Tribal Consultation Process: The need to consult on the<br />
development or revision of a policy may be identified from within HHS, an HHS Division or may<br />
be identified by <strong>Indian</strong> Tribes. This need may result from external forces such as Executive,<br />
Judicial, or Legislative Branch actions or otherwise. Once the need to consult on development or<br />
revision of a policy is identified the consultation process must begin in accordance with critical<br />
events and consultation mechanisms described above. HHS Divisions may request technical<br />
assistance from IGA for the Tribal consultation process.<br />
C. Schedule for Consultation: Divisions must establish and adhere to a formal schedule of<br />
meetings to consult with <strong>Indian</strong> Tribes and their representatives concerning the planning,<br />
conduct, and administration of applicable activities. Divisions must involve Tribal representatives<br />
in meetings at every practicable opportunity. Divisions are encouraged to establish additional<br />
forums for Tribal consultation and participation, and for information sharing with Tribal<br />
leadership. Consultation schedules should be coordinated with IGA to avoid duplications or<br />
conflicts with other national Tribal events. HHS Divisions should make every effort to schedule<br />
their consultations in conjunction with the Annual Regional Tribal Consultation Sessions.<br />
9. CONSULTATION PROCEDURES AND RESPONSIBLITIES<br />
. Consultation Parties and Mechanisms- Consultation Occurs:<br />
1. When the HHS Secretary/Deputy Secretary, or their designee, meets and/or<br />
exchanges written correspondence with a Tribal<br />
President/Chair/Governor/Chief/Principal Chief and/or elected/appointed <strong>Indian</strong> Tribal<br />
Leader, or their designee to discuss issues concerning either party.<br />
2. When an HHS Division Head, or their designee, meets or exchanges written<br />
correspondence with an <strong>Indian</strong> Tribal representative designated by an<br />
elected/appointed Tribal leader to discuss issues or concerns of either party.<br />
3. When an HHS Regional Director, who is the Secretary’s representative in the field,<br />
meets or exchanges written correspondence with an elected/appointed <strong>Indian</strong> Tribal<br />
Leader, or their designee to discuss issues or concerns of either party.<br />
4. When the Secretary/Deputy Secretary/HHS Division Head, or their designee, meets<br />
or exchanges written correspondence with a Tribal representative designated by an<br />
elected/appointed <strong>Indian</strong> Tribal leader to discuss issues or concern of either party.<br />
A. Consultation Procedures<br />
0. Tribal: Specific consultation mechanisms that will be used to consult with an <strong>Indian</strong><br />
Tribe(s) include but are not limited to mailings, meetings, teleconference and<br />
roundtables.
a. An <strong>Indian</strong> Tribe(s) has the ability to initiate consultation, i.e. meet one-on-one<br />
with an HHS Division Head or designated representative to consult on issues<br />
specific to that <strong>Indian</strong> Tribe.<br />
b. HHS Division Heads will initiate consultation to solicit official <strong>Indian</strong> Tribe(s)’<br />
comments and recommendations on policy and budget matters affecting <strong>Indian</strong><br />
Tribe(s). These sessions at roundtables, forums and meetings will provide the<br />
opportunity for meaningful dialogue and effective participation by <strong>Indian</strong><br />
Tribe(s).<br />
c. <strong>National</strong>/Regional Inter-Tribal Forums: Other types of meetings and/or<br />
conferences occur which may not be considered consultation sessions, but these<br />
meetings may provide opportunities to share information, conduct workshops,<br />
and provide technical assistance to <strong>Indian</strong> Tribes.<br />
1. HHS: Consultation mechanisms that will be used to consult with <strong>Indian</strong> Tribe(s)<br />
include but are not limited to mailings, meetings, teleconferences and roundtables.<br />
HHS has various organizational avenues in which Tribal issues and concerns are<br />
addressed. These avenues include the OS, the ICNAA, Regional Offices, and<br />
Divisions.<br />
1.<br />
2. Office of the Secretary<br />
a. The HHS <strong>National</strong> Tribal Consultation Sessions are designed to solicit<br />
<strong>Indian</strong> Tribes’ health and human services priorities and program needs.<br />
The Sessions provide an opportunity for <strong>Indian</strong> Tribes to articulate their<br />
recommendations on budgets, regulations, policies and legislation.<br />
i. Upon completion of consultation, HHS will document and notify<br />
<strong>Indian</strong> Tribes on the proceedings, noting positions and following-up<br />
on all issues raised that would benefit from ongoing consultation<br />
with <strong>Indian</strong> Tribe(s) within 90 calendar days.<br />
3. ICNAA<br />
a. The ICNAA represents the internal HHS team providing consistent<br />
direction across the Divisions for AI/AN/NA issues. One of the primary<br />
responsibilities of ICNAA is to solicit Tribal input in establishing Tribal<br />
policy and budget priorities and recommendations for Divisions.<br />
The health and human service priorities established by <strong>Indian</strong> Tribes are<br />
used to inform the development of the Divisions’ annual performance<br />
goals and measures for improving health and human services, which are<br />
linked to their budget requests.<br />
4. Regional Offices<br />
a. Regional Offices will work with the <strong>Indian</strong> Tribes and <strong>Indian</strong> organizations<br />
within their respective regional area in facilitating the Tribal perspective<br />
with HHS programs, services, functions, activities and planning Tribal<br />
regional consultation sessions. HHS Divisions have various geographic<br />
coverage, however all HHS Divisions, regardless of geographic location,<br />
are intended to serve <strong>Indian</strong> Tribe(s) in their respective locations.<br />
b. Regional Offices/Directors will work collaboratively with the HHS Division<br />
lead regional representative in communicating and coordinating on issues<br />
and concerns of <strong>Indian</strong> Tribes in those respective regions or areas.<br />
c. Regional Offices/Directors will work collaboratively to facilitate Tribal-State<br />
relations as they affect <strong>Indian</strong> Tribes in the delivery of HHS programs and<br />
services.<br />
d. Regional Tribal Consultation Sessions are held to solicit <strong>Indian</strong> Tribe(s)’<br />
priorities and needs on health and human services. The sessions also
provide <strong>Indian</strong> Tribes with a regional perspective and shall be held, at<br />
least but not limited to, annually with status reports to <strong>Indian</strong> Tribe(s) as<br />
appropriate throughout the year, or at least biannually.<br />
1. Regional Consultations will occur between February and April of<br />
every year.<br />
2. Regional Consultations shall be utilized as a venue for Divisions to<br />
coordinate their consultation responsibilities in a manner that is<br />
feasible and convenient for <strong>Indian</strong> Tribes.<br />
3. Regional Offices/Directors will contact <strong>Indian</strong> Tribes and <strong>Indian</strong><br />
Organizations in their respective regions to assist in the planning of<br />
the session. This will ensure inclusion of all perspectives and issues<br />
for the session.<br />
4. Protocol will ensure that the highest ranking official present from<br />
each respective <strong>Indian</strong> Tribe is given the opportunity to address the<br />
session first, followed by other elected officials, those designated by<br />
official letter to represent their respective <strong>Indian</strong> Tribe and<br />
representatives of <strong>Indian</strong> Organizations.<br />
a. Official letter from the <strong>Indian</strong> Tribe designating a<br />
representative must be presented to Regional Director before<br />
the session begins.<br />
5. Regional Offices/Directors will seek the assistance of Tribal Leaders<br />
to assist with moderating the annual regional consultation session.<br />
6. The official record of every regional session will be left open for 30<br />
calendar days after the conclusion of the session for submission of<br />
additional comments/materials from <strong>Indian</strong> Tribe(s)<br />
7. Regional Offices/Directors will provide a summary no later than 45<br />
calendar days after the consultation of the session.<br />
5. HHS Divisions<br />
a. Divisions will work collaboratively with the <strong>Indian</strong> Tribes on the<br />
development of consultation meetings, one-on-one meetings, roundtables,<br />
teleconferences and annual sessions.<br />
b. Divisions will work collaboratively with <strong>Indian</strong> Tribes on developing and<br />
implementing their respective Tribal Consultation Policy or Plan.<br />
c. Divisions will coordinate with IGA on their respective consultation<br />
activities in order to ensure that HHS and its Divisions are conducting<br />
Tribal consultation coordinating in a manner that is feasible and conducive<br />
to the needs of <strong>Indian</strong> Tribes.<br />
d. Divisions will participate in both the Annual Tribal Budget and Policy<br />
Consultation Session and Annual Regional Tribal Consultations with <strong>Indian</strong><br />
Tribes.<br />
e. Divisions will work collaboratively to facilitate Tribal-State relations as<br />
they affect <strong>Indian</strong> Tribes and AI/ANs in the delivery of HHS programs and<br />
services.<br />
2. States: In some instances the authority and program funding for HHS programs is<br />
administered by the States on behalf of <strong>Indian</strong> Tribes. The Divisions will consult with<br />
the Office of the General Counsel to determine whether these arrangements are<br />
based on statutes, regulations, or policy decisions. If there is no clear regulatory or
statutory basis mandating that States administer the program on behalf of the<br />
Tribe(s), the Division will consult with the affected <strong>Indian</strong> Tribe(s) as soon as<br />
practicable to review alternate options.<br />
If there is a statutory basis mandating that the State administer the program and<br />
associated funding on behalf of the <strong>Indian</strong> Tribe(s) the Division will examine the<br />
permissibility of encouraging or mandating a term requiring tribal consultation as a<br />
condition of the State’s receipt of program funds. If such a term may be mandated<br />
regarding State administered programs affecting <strong>Indian</strong> Tribes it should be<br />
incorporated. If it is not permissible, the Division shall facilitate consultation between<br />
the State and affected Tribe(s).<br />
In addition, whenever practicable and permitted by law, the Division shall notify<br />
<strong>Indian</strong> Tribes of funds administered by the State that the Division believes should be<br />
allocated to <strong>Indian</strong> Tribes.<br />
The Division shall also encourage the State to recognize that <strong>Indian</strong> Tribal members<br />
are entitled to benefits provided to all State citizens and should be provided the same<br />
access to State administered or funded services since Tribal members are citizens of<br />
the State(s). To the extent possible, data shall be collected and reported about the<br />
number of Tribal members served by the State with federal resources.<br />
10. ESTABLISHMENT OF JOINT TRIBAL/FEDERAL WORKGROUPS AND/OR TASKFORCES<br />
The need to develop or revise a policy may be identified from within the Division or by an <strong>Indian</strong><br />
Tribe(s). When new or revised national policy, regulations or legislation affects an <strong>Indian</strong><br />
Tribe(s), an <strong>Indian</strong> Tribe(s) or HHS may recommend the establishment of a workgroup and/or<br />
task force. In response, HHS may establish such a workgroup and/or task force to develop<br />
recommendations on various technical, legal, regulatory, or policy issues. In such cases, see<br />
ADDENDUM 1 which outlines the process for establishing such aforementioned workgroups<br />
and/or task forces.<br />
11. HHS BUDGET FORMULATION<br />
HHS shall consult with <strong>Indian</strong> Tribes throughout the development of the HHS Budget formulation<br />
process to the greatest extent practicable and permitted by law. The Secretary shall require the<br />
Divisions to include a process in their Tribal Consultation Policy/Plan that assures Tribal priorities<br />
and needs and requests are identified and considered in the formulation of the HHS budget.<br />
. HHS Annual Tribal Budget and Policy Consultation Session (ATBPCS): A<br />
Department-wide Tribal budget and policy consultation session will be conducted annually<br />
to give <strong>Indian</strong> Tribes the opportunity to present their budget and policy priorities and<br />
recommendations to the Department as HHS prepares to receive the budget requests of its<br />
Divisions. The session is convened in March of each year as a means for final input in the<br />
development of the Department’s budget submission to OMB.<br />
0. At a minimum, HHS conducts annually one ATBPCS to ensure the active participation<br />
of <strong>Indian</strong> Tribes in the formulation of the HHS performance budget request as it<br />
pertains to <strong>Indian</strong> Tribes, which will be held at the HHS Headquarters in Washington,<br />
DC no later than March each year.<br />
1. HHS will notify Tribes of the date of the consultation no later than 90 days prior to<br />
the session.<br />
2. The session will not exceed two days.<br />
3. Each Operating Division Head/Deputy and budget officer will attend their agency’s<br />
appropriate session(s).
4. Each Operating Division Head/Deputy will participate in other portions of the ATBPCS<br />
that affect their respective division.<br />
5. IGA/ASFR will provide a summary of the session to <strong>Indian</strong> Tribes no later than 30<br />
calendar days after the session has concluded.<br />
6. Within 90 calendar days IGA shall post the transcript of the ATBPCS with a summary<br />
of the <strong>Indian</strong> Tribes’ issues/concerns presented at the session.<br />
7. HHS will seek the assistance of <strong>Indian</strong> Tribal Leaders to assist with moderating the<br />
ATBPCS. HHS will also contact <strong>Indian</strong> Organizations in the planning of the session in<br />
order to ensure inclusion of all perspectives and issues.<br />
8. Presentation protocol will ensure that the highest ranking official from each<br />
respective Tribe is given the opportunity to address the session first, followed by<br />
other elected officials, those designated by their elected official to represent their<br />
respective <strong>Indian</strong> Tribes and representatives of <strong>Indian</strong>/Tribal Organizations.<br />
. Official letter from the <strong>Indian</strong> Tribe designating a representative must be<br />
presented to IGA before the session begins.<br />
A. Performance Budget Formulation: HHS IGA will ensure the active participation of<br />
<strong>Indian</strong> Tribes and <strong>Indian</strong> Organizations in the formulation and throughout the HHS<br />
performance budget request as it pertains to <strong>Indian</strong> Tribes to the greatest extent<br />
practicable and permitted by law.<br />
B. Budget Information Disclosure: HHS provides <strong>Indian</strong> Tribes the HHS budget related<br />
information on an annual basis: appropriations, allocation, expenditures, and funding levels<br />
for programs, services, functions, and activities.<br />
12. TRIBAL CONSULTATION PERFORMANCE AND ACCOUNTABILITY<br />
HHS and its Divisions will measure and report results and outcomes of their Tribal consultation<br />
performance to fulfill the government-to-government relationship with <strong>Indian</strong> Tribes.<br />
Parts of the HHS mission and performance objectives are designed to address the health and<br />
well-being of AI/ANs by providing for effective health and human services and by fostering<br />
strong, sustained advances in the sciences underlying medicine, public health and social<br />
services.<br />
The Divisions shall utilize the Tribal Consultation Policy to address HHS’s mission and<br />
performance objectives with respect to AI/ANs. HHS and its Divisions will follow the goals and<br />
objectives of the seated Secretary and Administration.<br />
Divisions and <strong>Indian</strong> Tribes will also promote a collaborative atmosphere to gather, share, and<br />
collect data and other information to demonstrate the effective use of Federal resources in a<br />
manner that is consistent with OMB performance measures and requirements. Divisions shall<br />
consult, to the greatest extent practicable and permitted by law, with <strong>Indian</strong> Tribes before taking<br />
actions that substantially affect <strong>Indian</strong> Tribes, including regulatory practices on Federal matters<br />
and unfunded mandates.<br />
13. EVALUATION, RECORDING OF MEETINGS AND REPORTING<br />
The consultation process and activities conducted within the policy should result in a meaningful<br />
outcome for the Department and for the affected <strong>Indian</strong> Tribes. To effectively evaluate the<br />
results of a particular consultation activity and the Department’s ability to incorporate <strong>Indian</strong><br />
Tribes’ consultation input, the Department should measure, on an annual basis, the level of<br />
satisfaction of the <strong>Indian</strong> Tribes.
0. Divisions should develop and utilize appropriate evaluation measures to assess <strong>Indian</strong><br />
Tribes’ responses to Department consultation conducted during a specific period to<br />
determine if the intended purpose of the consultation was achieved and to receive<br />
recommendations to improve the consultation process.<br />
. The Divisions will maintain a record of the consultation, evaluate whether the<br />
intended results were achieved, and report back to the affected <strong>Indian</strong> tribe(s) on the<br />
status or outcome, including, but not limited to, the annual sessions conducted<br />
below.<br />
1. At a minimum, HHS Regional Directors will conduct an Annual Regional Tribal Consultation<br />
to consult with <strong>Indian</strong> Tribes.<br />
. These sessions shall provide an opportunity to receive the <strong>Indian</strong> Tribe’s priorities for<br />
budget, regulation, legislation, and other policy matters.<br />
a. Consultation Sessions shall include evaluation components for receipt of verbal and<br />
written comments from participating <strong>Indian</strong> Tribes, HHS Divisions, and other invited<br />
participants to obtain immediate feedback on the consultation process for the session<br />
conducted.<br />
b. The Divisions and the Regional Directors will report at each regional Tribal<br />
consultation session regarding what substantive and procedural actions were taken as<br />
a result of the previous Tribal consultation session and describe how HHS addressed<br />
the consultation evaluation comments provided received by participants.<br />
c. All national and regional consultation meetings and recommended actions shall be<br />
formally recorded and made available to <strong>Indian</strong> Tribes.<br />
d. Once the consultation process is complete, and any policy decision is finalized, all<br />
recommended follow-up actions adopted shall be implemented and tracked by the<br />
appropriate Regions and/or Divisions and reported to the <strong>Indian</strong> Tribes in the IGA<br />
Annual Tribal Consultation Report.<br />
e. Unless otherwise specified, the IGA Annual Consultation Report shall provide an<br />
annual reporting mechanism for this purpose and all HHS Divisions are required to<br />
participate in providing information for this report.<br />
2. IGA will seek Tribal feedback to assist in measuring and evaluating the implementation and<br />
effectiveness of this Policy. IGA will assess the Department Tribal Consultation Policy on an<br />
ongoing basis and utilize comments from <strong>Indian</strong> Tribes and Federal participants to<br />
determine whether amendment to the Policy may be required. If amendment is needed,<br />
IGA will convene a Tribal-Federal workgroup.<br />
3. Divisions are required to submit to IGA their fiscal year Tribal consultation information<br />
within 90 calendar days from the end of the fiscal year. IGA shall compile the Division<br />
submissions, and publish and distribute the information to the <strong>Indian</strong> Tribes within 60<br />
calendar days from receipt of the Division reports. The IGA, Regional Directors and<br />
Divisions shall also report the Department’s views on the level of attendance and response<br />
from Tribal leaders during the Annual Tribal Budget and Policy Consultation Session and<br />
the Annual Regional Tribal Consultation Sessions, including evaluative comments, and<br />
provide advice and recommendations regarding the Tribal consultation process. The IGA<br />
shall post on the HHS website, the IGA Annual Tribal Consultation Report, including the<br />
evaluation results.<br />
14. CONFLICT RESOLUTION<br />
The intent of this policy is to promote partnership with <strong>Indian</strong> Tribes that enhance the
Department’s ability to address issues, needs and problem resolution. Agencies shall consult with<br />
<strong>Indian</strong> Tribes to establish a clearly defined conflict resolution process under which <strong>Indian</strong> Tribes<br />
bring forward concerns which have a substantial direct effect. However, <strong>Indian</strong> Tribes and HHS<br />
may not always agree and inherent in the government-to-government relationship, <strong>Indian</strong> Tribes<br />
may elevate an issue of importance to a higher or separate decision-making authority.<br />
Nothing in the Policy creates a right of action against the Department for failure to comply with<br />
this Policy.<br />
15. TRIBAL WAIVER<br />
Divisions shall review and streamline the processes under which <strong>Indian</strong> Tribe may apply for<br />
waivers of statutory, regulatory, policy, or procedural requirements. Each Division shall, to the<br />
extent practicable and permitted by law, consider any application by an <strong>Indian</strong> Tribe for a waiver<br />
with a general view toward increasing opportunities for utilizing flexible approaches at the <strong>Indian</strong><br />
Tribal level when the proposed waiver is consistent with the applicable Federal policy objectives<br />
and is otherwise appropriate. Each Division shall, to the extent practicable and permitted by law,<br />
render a decision upon a complete application for a waiver within 120 calendar days of receipt,<br />
or as otherwise provided by law or regulation. If the application for waiver is not granted, the<br />
Division shall provide the applicant with timely written notice of the decision and the reasons<br />
therefore. Waiver requests for statutory or regulatory requirements apply only to statutory or<br />
regulatory requirements that are discretionary and subject to waiver by the Division.<br />
16. EFFECTIVE DATE<br />
This policy is effective on the date of the signature by the Secretary of <strong>Health</strong> and Human<br />
Services.<br />
This policy replaces the Tribal Consultation Policy signed on February 1, 2008, and it applies to<br />
all Operating Divisions and Staff Divisions. Operating Divisions shall complete necessary<br />
revisions to their existing Division consultation policy/plan to conform to the revised Department<br />
Tribal Consultation Policy. Operating Divisions without a consultation policy shall utilize the<br />
guidance of the OS policy until the development of their respective policy.<br />
17. DEFINITIONS<br />
0. Agency – Any authority of the United States that is an “agency” under 44 USC 3502(1)<br />
other than those considered to be independent regulatory agencies, as defined in 44 USC<br />
3502 (5).<br />
1. Communication – The exchange of ideas, messages, or information, by speech, signals,<br />
writing, or other means.<br />
2. Consultation – An enhanced form of communication, which emphasizes trust, respect and<br />
shared responsibility. It is an open and free exchange of information and opinion among<br />
parties, which leads to mutual understanding and comprehension. Consultation is integral<br />
to a deliberative process, which results in effective collaboration and informed decision<br />
making with the ultimate goal of reaching consensus on issues.<br />
3. Coordination and Collaboration – Working and communicating together in a meaningful<br />
government-to-government effort to create a positive outcome.<br />
4. Critical Events – Planned or an unplanned event that has or may have a substantial<br />
impact on <strong>Indian</strong> Tribe(s), e.g., issues, polices, or budgets which may come from any level<br />
within HHS.
5. Deliberative Process Privilege – Is a privilege exempting the government from<br />
disclosure of government agency materials containing opinions, recommendations, and<br />
other communications that are part of the decision-making process within the agency.<br />
6. Executive Order – An order issued by the Government’s executive on the basis of<br />
authority specifically granted to the executive branch (as by the U.S. Constitution or a<br />
Congressional Act).<br />
7. Federally Recognized Tribal governments – <strong>Indian</strong> Tribes with whom the Federal<br />
Government maintains an official government-to-government relationship; usually<br />
established by a Federal treaty, statute, executive order, court order, or a Federal<br />
Administrative Action. The Bureau of <strong>Indian</strong> Affairs (BIA) maintains and regularly publishes<br />
the list of Federally recognized <strong>Indian</strong> Tribes.<br />
8. HHS Tribal Liaisons – HHS staff designated by the head of an HHS Division that are<br />
knowledgeable about the Division’s programs and budgets, and have ready access to<br />
senior HHS Division leadership, and are empowered to speak on behalf of that Division for<br />
AI/AN/NA programs, services, issues, and concerns.<br />
9. <strong>Indian</strong> – <strong>Indian</strong> means a person who is a member of an <strong>Indian</strong> tribe as defined in 25<br />
U.S.C. 479a. Throughout this policy, <strong>Indian</strong> is synonymous with American <strong>Indian</strong>/Alaska<br />
Native.<br />
10. <strong>Indian</strong> Organizations: 1). Those Federally recognized tribally constituted entities that<br />
have been designated by their governing body to facilitate DHHS communications and<br />
consultation activities. 2). Any regional or national organizations whose board is comprised<br />
of Federally recognized Tribes and elected/appointed Tribal leaders. The government does<br />
not participate in government-to-government consultation with these entities; rather these<br />
organizations represent the interests of Tribes when authorized by those Tribes.<br />
11. <strong>Indian</strong> Tribe – an <strong>Indian</strong> or Alaska Native tribe, band, nation, pueblo, village, or<br />
community that the Secretary of the Interior acknowledges to exist as an <strong>Indian</strong> tribe<br />
pursuant to the Federally Recognized <strong>Indian</strong> Tribe List Act of 1994, 25 U.S.C. 479a.”<br />
12. Intradepartmental Council on Native American Affairs (ICNAA) – Authorized by the<br />
Native American Programs Act of 1974 (NAPA), as amended. The ICNAA serves primarily to<br />
perform functions and develop recommendations for short, intermediate, or long-term<br />
solutions to improve AI/AN/NA policies and programs as well as provide recommendations<br />
on how HHS should be organized to administer services to the AI/AN/NA population.<br />
13. Joint Tribal/Federal Workgroups and or/Task Forces – A group composed of<br />
individuals who are elected Tribal officials, appointed by Federally recognized Tribal<br />
governments and/or Federal agencies to represent their interests while working on a<br />
particular policy, practice, issue and/or concern.<br />
14. Native American (NA) – Broadly describes the people considered indigenous to North<br />
America.<br />
15. Policies with Tribal Implications – Refers to regulations, statutes, legislation, and other<br />
policy statements or actions that have substantial direct effects on one or more <strong>Indian</strong><br />
Tribes, on the relationship between the Federal Government and <strong>Indian</strong> Tribes, or on the<br />
distribution of power and responsibilities between the Federal Government and <strong>Indian</strong><br />
Tribes.<br />
16. Self Government – Government in which the people who are most directly affected by<br />
the decisions make decisions.
17. Sovereignty – The ultimate source of political power from which all specific political<br />
powers are derived.<br />
18. Substantial Direct Compliance Costs – Those costs incurred directly from<br />
implementation of changes necessary to meet the requirements of a Federal regulation.<br />
Because of the large variation in Tribes, “substantial costs” is also variable by <strong>Indian</strong> Tribe.<br />
Each <strong>Indian</strong> Tribe and the Secretary shall mutually determine the level of costs that<br />
represent “substantial costs” in the context of the <strong>Indian</strong> Tribe’s resource base.<br />
19. To the Extent Practicable and Permitted by Law – Refers to situations where the<br />
opportunity for consultation is limited because of constraints of time, budget, legal<br />
authority, etc.<br />
20. Treaty – A legally binding and written agreement that affirms the government-togovernment<br />
relationship between two or more nations.<br />
21. Tribal Government – An American <strong>Indian</strong> or Alaska Native Tribe, Band, Nation, Pueblo,<br />
Village or Community that the Secretary of the Interior acknowledges to exist as an <strong>Indian</strong><br />
Tribe pursuant to the Federally Recognized <strong>Indian</strong> Tribe List Act of 1994, 25 USC 479a.<br />
22. Tribal Officials – Elected or duly appointed officials of <strong>Indian</strong> Tribes or authorized inter-<br />
Tribal organizations.<br />
23. Tribal Organization – The recognized governing body of any <strong>Indian</strong> tribe; any legally<br />
established organization of <strong>Indian</strong>s which is controlled, sanctioned, or chartered by such<br />
governing body or which is democratically elected by the adult members of the <strong>Indian</strong><br />
community to be served by such organization and which includes the maximum<br />
participation of <strong>Indian</strong>s in all phases of its activities: Provided, That in any case where a<br />
contract is let or grant made to an organization to perform services benefiting more than<br />
one <strong>Indian</strong> tribe, the approval of each such <strong>Indian</strong> tribe shall be a prerequisite to the<br />
letting or making of such contract or grant.<br />
24. Tribal Resolution – A formal expression of the opinion or will of an official Tribal<br />
governing body which is adopted by vote of the Tribal governing body.<br />
25. Tribal Self–Governance – The governmental actions of Tribes exercising self-government<br />
and self-determination.<br />
18. ACRONYMS<br />
AI/AN: American <strong>Indian</strong>/Alaska Native<br />
AI/AN/NA: American <strong>Indian</strong>/Alaska Native/Native American<br />
ASFR: Assistant Secretary for Finance and Resources<br />
BIA: Bureau of <strong>Indian</strong> Affairs<br />
Division: Staff Division and/or Operating Division<br />
EO: Executive Order<br />
FACA: Federal Advisory Committee Act<br />
FR: Federal Register<br />
HHS: U.S. Department of <strong>Health</strong> and Human Services<br />
ICNAA: Intradepartmental Council on Native American Affairs<br />
IGA: Office of Intergovernmental Affairs<br />
IOS: Immediate Office of the Secretary<br />
NPRM: Notice of Proposed Rule Making<br />
OMB: Office of Management and Budget<br />
OS: Office of the Secretary<br />
U.S.: United States<br />
U.S.C.: United States Code
S/ Kathleen Sebelius December 14, 2010<br />
_____________________________________________ ___________________<br />
__<br />
Kathleen Sebelius Date<br />
Secretary<br />
U.S. Department of <strong>Health</strong> and Human Services<br />
ADDENDUM 1<br />
1. Establishing Joint Tribal/Federal Workgroups and/or Tasks Forces:<br />
Although the special “Tribal-Federal” relationship is based in part on the government-togovernment<br />
relationship it is frequently necessary for HHS to establish Joint Tribal/Federal<br />
Workgroups and/or Task Forces to complete work needed to develop new policies, practices,<br />
issues, and/or concerns and/or modify existing policies, practices, issues, and/or concerns.<br />
These Joint Tribal/Federal Workgroups and/or Task Forces do not take the place of Tribal<br />
consultation, but offer an enhancement by gathering individuals with extensive knowledge of a<br />
particular policy, practice, issue and/or concern to work collaboratively and offer<br />
recommendations for consideration by Federally recognized <strong>Indian</strong> Tribes and Federal agencies.<br />
The subsequent work products and/or outcomes developed by the Joint Tribal/Federal<br />
Workgroup and/or Task Forces will be handled in accordance with this policy. These Workgroups<br />
will be Federal Advisory Committee Act (FACA) compliant unless exempt.<br />
1. Meeting Notices: The purpose, preliminary charge, time frame, and other specific tasks<br />
shall be clearly identified in the notice. All meetings should be open and widely publicized<br />
ideally through IGA or the Division initiating the policy.<br />
2. Workgroups: membership should be selected based on the responses received from<br />
prospective HHS Regions/<strong>Indian</strong> <strong>Health</strong> Service Areas as a result of the notice, and if<br />
possible, should represent a cross-section of affected parties. HHS staff may serve in a<br />
technical advisory capacity.<br />
A. Participation:<br />
1. Membership Notices: HHS shall seek nominations from <strong>Indian</strong> Tribes to participate in<br />
taskforces and/or workgroups. The Secretary shall select workgroup members that<br />
represent various regions and/or views of <strong>Indian</strong> Country. Membership of these<br />
workgroups shall be in compliance with FACA unless the workgroup is exempt<br />
2. Appointment of Alternates: Each primary representative may appoint an alternate by<br />
written notification. In cases where an elected Tribal Leader (primary representative)<br />
appoints an alternate who is not an elected official, and the primary member can not<br />
attend a workgroup meeting, the alternate is permitted to represent the primary member<br />
and will have the same voting rights as the primary member.<br />
3. Attendance at Meetings: Workgroup members must make a good faith effort to attend all<br />
meetings. Other individuals may accompany workgroup members, as that member<br />
believes is appropriate to represent his/her interest, however FACA requirements will be<br />
adhered to at meetings unless exempt<br />
B. Workgroup Protocols: The workgroup may establish protocols to govern the meetings. Such<br />
protocols will include, but are not limited to the following:
1. Selection of workgroup co-chairs, if applicable<br />
2. Role of workgroup members<br />
3. Process for decision-making (consensus based or otherwise)<br />
4. Developing a Workgroup Charge. Prior to the workgroup formulation, the HHS will develop<br />
an initial workgroup charge in enough detail to define the policy concept. The workgroup<br />
may develop recommendations for the final workgroup charge for the approval of the HHS<br />
Secretary, the IGA Director or the Division head.<br />
C. Process for Workgroup Final Products: Once a final draft of the work product has been created<br />
by the workgroup the following process will be used to facilitate Tribal consultation on the draft<br />
work product:<br />
1. Upon completion, the draft documents will be distributed informally to <strong>Indian</strong> Tribes and<br />
<strong>Indian</strong> Organizations for review and comment and to allow for maximum possible informal<br />
review.<br />
2. Comments will be returned to the workgroup, which will meet in a timely manner to<br />
discuss the comments and determine the next course of action.<br />
3. At the point that the proposed draft policy is considered to be substantially complete as<br />
written, the workgroup will forward the draft document to the HHS Secretary as final<br />
recommendation for consideration.<br />
4. The workgroup will also recognize any contrary comment(s) in its final report and explain<br />
the reasoning for not accepting the comment(s).<br />
5. If it is determined that the policy should be rewritten, the workgroup will rewrite and begin<br />
informal consultation again at the initial step above.<br />
6. If the proposed policy is generally acceptable to the HHS Secretary, final processing of the<br />
policy by the workgroup will be accomplished.<br />
D. Recommendations and Policy Implementation: All final recommendations made by the<br />
workgroup should be presented to the Secretary. Before any final policy decisions are adopted<br />
within HHS, the proposed policy shall be widely publicized and circulated for review and<br />
comment to <strong>Indian</strong> Tribes, <strong>Indian</strong> Organizations, and within HHS. Once the consultation process<br />
is complete and a proposed policy is approved and issued, the final policy shall be broadly<br />
distributed to all <strong>Indian</strong> Tribes.
NORTHWEST<br />
PORTLAND<br />
AREA<br />
INDIAN<br />
HEALTH<br />
BOARD<br />
Burns-Paiute Tribe<br />
Chehalis Tribe<br />
Coeur d' Alene Tribe<br />
Colville Tribe<br />
Coos, Sui slaw &<br />
Lower Umpqua Tribe<br />
Coquille Tribe<br />
Cow Creek Tribe<br />
Cowl it? Tribe<br />
Gmnd Ronde Tribe<br />
Hoh Tribe<br />
Jamestown S'Klaliam Tribe<br />
Kalispcl Tribe<br />
Klamath Tribe<br />
Kootenai Tribe<br />
Lower Elwha Tribe<br />
Lummi Tribe<br />
Makah Tribe<br />
Muekleshoot Tribe<br />
Nez Perce Tribe<br />
Nisqually Tribe<br />
Nooksack Tribe<br />
NW Band of Shoshone Tribe<br />
Port Gamble S'Klallam Tribe<br />
Puyallup Tribe<br />
QuileuteTribe<br />
Quinault Tribe<br />
Sam ish <strong>Indian</strong> Nation<br />
Sauk-Suiattlc Tribe<br />
Shoalwater Bay Tribe<br />
Shoshone-Bannock Tribe<br />
Siletz Tribe<br />
Skokomish Tribe<br />
Snoqualmie Tribe<br />
Spokane Tribe<br />
Squaxin Island Tribe<br />
Stillaguamish Tribe<br />
Suquamish Tribe<br />
Swinomish Tribe<br />
Tulalip Tribe<br />
Umatilla Tribe<br />
Upper Skagit Tribe<br />
Wann Springs Tribe<br />
Yakama Nation<br />
2121 SW Broadway<br />
Suite 300<br />
Portland, OR 97201<br />
(503) 228-4185<br />
(503)228-8182 FAX<br />
www.npaihb.org<br />
SENT VIA EMAIL: Pam.Hyde@SAMHSA.hhs.gov; blockgrants@samhsa.hhs.gov<br />
September 21,2012<br />
Ms. Pamela S. Hyde, J.D.<br />
Administrator<br />
Substance Abuse and Mental <strong>Health</strong> Service Administration<br />
1 Choke Cherry Rd.<br />
Rockville, MD 20857<br />
REF: Comments - Agency Information Collection Activities: Proposed<br />
Collection; Comment Request for: Uniform Application for the Mental<br />
<strong>Health</strong> Block Grant and Substance Abuse Block Grant FY 2014-2015,<br />
Application Guidance and Instructions (OMB No. 0930-0168)<br />
Revision.<br />
Dear Ms. Hyde:<br />
The Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NPAIHB) is a P.l. 93-638 Tribal<br />
organization 1 that represents forty-three federally-recognized Tribes in the states of<br />
Idaho, Oregon, and Washington. On behalf of our member Tribes, we are writing to<br />
provide comments for the Agency Information Collection Activities: Proposed Collection;<br />
Comment Request, published in the Federal Register, Vol. 77, No. 135, Friday, July 13,<br />
2012, notices.<br />
We understand the purpose of this notice is to comment on: information from reports<br />
will have a practical utility; have accuracy of the agency's estimate of the burden of the<br />
proposed collection of information; ways to enhance the quality, utility, and clarity of<br />
the information to be collected; and ways to minimize the burden of the collection<br />
techniques or other forms of information technology.<br />
Before providing comment it is important for us to underscore our deep concern that<br />
there is no mention of Tribal governments in the entire document. We note a "casual"<br />
citation near the end of page 41434 and the reference to Native Americans on page<br />
41435. The document overlooks the preferred reference and legislative term "American<br />
<strong>Indian</strong>s and Alaska Native (AI/AN)" and we urge SAMHSA to use the preferred term in<br />
future publications. We are concerned that past comments we provided and issues<br />
discussed at the SAMHSA Tribal Advisory Committee meetings are not adequately<br />
addressed. These issues have also been raised in SAMHSA Tribal consultation sessions.<br />
J As defined in the <strong>Indian</strong> Self-Determination and Education Assistance Act. P.L. 93-638. 25 U.S.C .• Section<br />
45O(b) a Tribal organization is a legally established governing body of any <strong>Indian</strong> tribe(s) that is controlled.<br />
sanctioned. or chartered by such <strong>Indian</strong> Tribe(s) and designated to act on their behalf.
It is unclear if this was just an oversight or a lack of understanding of the government to government<br />
requirement. The proposed application requirements will have a direct impact of the ability of SAMHSA<br />
to further its mission and services for Tribal communities.<br />
Please note the following comments from a submission dated June 6, 2011 per SAMHSA's request.<br />
Where these comment disregarded? We did not receive any feedback from the comments. These<br />
comments were directed toward the information provided in the Federal Register, Vol. 76, No. 69,<br />
Monday, April 11, 2011:<br />
In regards to States following a four-step planning process conSisting of: (1) Assessing the<br />
strengths and needs of the service system; (2) identifying the unmet service needs and<br />
critical gaps within the current system; (3) prioritize the State planning activities, and; (4)<br />
develop goals, strategies and performance indicators, there will be unintended<br />
consequences for Tribal population unless:<br />
1. Tribes are consulted to address the strengths and needs of the population they serve. It<br />
would be impossible for a State to provide a comprehensive assessment of strengths<br />
and needs of the service system without the assistance of Tribes in their respective<br />
States.<br />
Additionally, non-Medicaid encounter data from Tribal systems is often reported<br />
directly to the Federal government, (via <strong>Indian</strong> <strong>Health</strong> Service), and is not included in<br />
State databases. Furthermore, Tribal populations often do not access State services due<br />
to historical discrimination and mistreatment, resulting in an unrealized "silent need".<br />
2. The unmet service needs are difficult to identify. States have various methods for<br />
gathering data, as do the 565 Federally Recognized Tribes. Currently, most policy for<br />
service provision is driven from encounter data. This results in a fatal flaw - no valid<br />
method to determine unmet service needs when there is no access or limited access to<br />
behavioral health services. As noted in numerous publications, including the Report on<br />
State Responses to the FY 2011 Block Grant Addendum on <strong>Health</strong> Care Reform, there is a<br />
current shortage of behavioral health professionals. This shortage is projected to<br />
amplify with the surge caused by the implementation of the Affordable Care Act, thus<br />
the intense need to determine actual levels of need.<br />
This Proposed Project needs to clearly define how population needs will be assessed for<br />
people that do not have access to behavioral health services. There should be a specific<br />
section that elaborates on a method to not only determine this for Tribal populations<br />
but all rural populations as identified by the <strong>Health</strong> Professional Shortage Areas.<br />
If this measure is not taken there will be a gross underestimate of service needs from<br />
populations that are never "counted" until they self-terminate or suffer catastrophic<br />
consequences.<br />
3. States must be required to consult with Tribal representatives (specifically elected Tribal<br />
leaders or individuals formally appointed to represent their Tribal government) for any<br />
prioritization of State planning activities. Tribal populations will continue to be
underserved without this requirement.<br />
4. Only Tribes know their population's attainable goals, strategies and performance<br />
indicators that are culturally applicable. This responsibility is accepted by Tribes for<br />
their constituents and not transferable. All Tribes, which have territories within State<br />
boundaries, should be consulted for any development of goals and performance<br />
indicators.<br />
In regard to the paragraph Description of State's Consultation with Tribes, the following<br />
comments are provided:<br />
We would suggest some additional language to fortify the government to government<br />
relationship that Tribes have with the Federal government. State relations history and<br />
Tribes as noted by Administrator Hyde in the Alcoholism and Drug Abuse Weekly,<br />
" ... (Tribes) neither consulted with nor are their needs addressed when the state gets the<br />
dollars" ... , needs to be definitively improved and required.<br />
While we have been advised that SAMHSA "cannot require" State to consult with Tribes,<br />
there should be required reporting components in the State reports that tracks the<br />
dollars spent. A suggested list of those components should at a minimum include:<br />
• Name of Tribe(s)<br />
• Date of Consultation<br />
• Duration of Consultation (e.g. hours, days)<br />
• List of Tribal Representatives<br />
• Topic of Consultation<br />
Required Topics of Discussion must include:*<br />
Scope of service provision (amount and need)<br />
Strategies for service provision<br />
Utilization of services<br />
Time frame for State implementation of Proposed Project<br />
Involvement of "Dashboard" development (key performance indicators<br />
Suicide prevention<br />
- Technical assistance needs<br />
Involvement of individuals and families<br />
Use of technology<br />
Collaboration<br />
(* please note this is not an all inclusive list, more components could be required)<br />
The list above should be strongly considered as a reporting requirement. Without such<br />
a requirement, history and experience has clearly shown that Tribal populations will be<br />
neglected/excluded from access to federal dollars that are appropriately designated for<br />
the needs of American <strong>Indian</strong>s and Alaska Natives (AI/AN).<br />
Lastly, SAMSHA should require States to include official Tribal representatives (from all<br />
Tribes in the State) to be a voting member of State Behavioral <strong>Health</strong> Advisory Councils<br />
(council names may vary by State). This is critical, and important that each Tribe be<br />
invited to name a representative for State level councils. It is not enough nor
November 14 -15, 2012 TTAG<br />
FACE TO FACE MEETING<br />
<strong>National</strong> Museum of the American <strong>Indian</strong><br />
4 th floor conference room<br />
Fourth & Independence Avenue, SW<br />
Washington, DC<br />
AGENDA: Day 1 Wednesday – Nov. 14, 2012<br />
9:00 – 9:15 Welcome Call to Order: Valerie Davidson, Chair, and Alaska Area Representative<br />
Opening Prayer:<br />
Roll Call: Liz Heintzman, Legislative Program Associate, NIHB<br />
Introductions: Valerie Davidson, Chair<br />
9:15 – 9:30 Report from Chair: Valerie Davidson, Chair<br />
9:30– 9:45 Report from Secretary (TAB A): Richard Narcia, Phoenix Area Representative<br />
- Approval of TTAG Face-to-Face Meeting minutes: July 25-26, 2012<br />
9:45 – 10:15 CMS Leadership:<br />
- Ajay Gupta, Senior Advisor to the Administrator<br />
10:15 – 11:15 CMS Tribal Affairs Group Report (TAB B)<br />
- Kitty Marx, Director, TAG/CMS<br />
o Tribal Affairs Group Updates<br />
o Determine 2013 TTAG Face-to-Face Meeting Dates<br />
11:15 – 11:30 Break<br />
NIHB Update:<br />
- Stacy Bohlen, Executive Director, NIHB<br />
- Jennifer Cooper, Legislative Director, NIHB<br />
11:30– 12:00 Money Follows the Person Funding Opportunity<br />
- Kitty Marx, Director, TAG/CMS<br />
12:00 – 1:30 Lunch on your own<br />
November 14-15, 2012 TTAG Face To Face Meeting<br />
1
1:30 – 2:15 OIG: Update OIG Work Plan FY 2013 (TAB C)<br />
- Talisha Searcy, Deputy Director for Evaluation Planning and Support Division,<br />
Office of Evaluation and Inspections, OIG<br />
- Maritza Hawrey, Audit Manager, Grants and Internal Audits, Office of Audit<br />
Services, OIG<br />
2:15-2:45 Final action and Approval of TTAG AI/AN Strategic Plan 2013 -2018<br />
- Jim Roberts, Chair, TTAG Budget and Strategic Plan Subcommittee<br />
- Mim Dixon, TTAG Technical Advisor, TSGAC<br />
2:45 – 3:15 Subcommittee Reports (TAB D):<br />
- Outreach & Education: Dr. Alec Thundercloud<br />
- Long-Term Care: Judy Goforth Parker<br />
- DATA : Jim Crouch<br />
- Behavioral <strong>Health</strong>: Linda Frizzell<br />
- CMS Tribal Consultation: Ron Allen<br />
- ACA Policy Subcommittee: Jim Roberts<br />
- Across State Borders: Donita Stephens<br />
3:15 – 3:30 Break<br />
3:30 – 4:00 CCIIO Update (TAB E)<br />
- Lisa Wilson, CCIIO, CMS<br />
4:00- 5:00 Update from the Center for Medicaid and CHIP (TAB F)<br />
- Lane Terwilliger JD, LL.M., Technical Director, Div. of State Demonstrations &<br />
Waivers, CMCS/CMS<br />
5:00 Adjourn: Valerie Davidson, Chair<br />
November 14-15, 2012 TTAG Face To Face Meeting<br />
2
AGENDA: Day 2 Thursday – Nov. 15, 2012<br />
9:00 Call to Order: Valerie Davidson, Chair, Alaska Area Representative<br />
9:05 – 12:00 Other Subcommittee meetings<br />
10:00 – 11:30 Data Subcommittee meeting at HHS, Room 335G<br />
877-267-1577; Meeting ID: 7218<br />
12:00 Adjourn TTAG Meeting<br />
12:30 pm NIHOE Area & <strong>National</strong> Partnership Meeting<br />
<strong>National</strong> Congress of American <strong>Indian</strong>s<br />
1516 P Street NW, Washington, DC<br />
888-244-8150; password: 6989122<br />
Future Meetings and Conference Calls:<br />
Conference Calls: 2:30 - 4:00 PM<br />
December 12, 2012: call in number 1-877-267-1577, meeting ID: 9925<br />
January 9, 2013: call in number 1-877-267-1577. Meeting ID: TBD<br />
March 13, 2013: call in number 1-877-267-1577. Meeting ID: TBD<br />
April 10, 2013: call in number 1-877-267-1577. Meeting ID: TBD<br />
May 8, 2013: call in number 1-877-267-1577. Meeting ID: TBD<br />
June 12, 2013: call in number 1-877-267-1577. Meeting ID: TBD<br />
August 14, 2013: call in number 1-877-267-1577. Meeting ID: TBD<br />
September 11, 2013: call in number 1-877-267-1577. Meeting ID: TBD<br />
October 9, 2013:call in number 1-877-267-1577. Meeting ID: TBD<br />
December 11, 2013: call in number 1-877-267-1577. Meeting ID: TBD<br />
Face to Face Meetings:<br />
February : NMAI, Washington, D.C.<br />
July : NMAI, Washington, DC<br />
November :NMAI, Washington, DC<br />
November 14-15, 2012 TTAG Face To Face Meeting<br />
3
HHS Block Grant Regulations<br />
Title 45 (Public Welfare and Human Services, General<br />
Administration),<br />
Part 96 (Block Grants), revised as of October 1, 1996<br />
The text of the U.S. Department of <strong>Health</strong><br />
and Human Services (HHS) Block Grant<br />
Regulations (Title 45, Part 96 of the Code<br />
of Federal Regulations) is taken from<br />
the U.S. Government Printing Office via GPO<br />
Access//CITE: 45CFR96.<br />
A listing of the sections to Subparts A-L<br />
and Appendices A-B of the regulations<br />
begins HERE. Text links to the Subparts and<br />
Appendices begin HERE.<br />
LIHEAP regulations are found at Subpart H.<br />
Subparts A-F are also relevant to LIHEAP.<br />
Text links to the Subparts and Appendices<br />
Subpart A--Introduction<br />
Subpart B--General Procedures<br />
Subpart C--Financial Management<br />
Subpart D--Direct Funding of <strong>Indian</strong> Tribes<br />
Subpart E--Enforcement<br />
Subpart F--Hearing Procedure
Subpart G--Social Services Block Grant<br />
Subpart H--Low-Income Home Energy<br />
Assistance Program<br />
Subpart I--Community Services Block Grants<br />
Subpart J--Primary Care Block Grants<br />
Subpart K--Transition Provisions<br />
Subpart L--Substance Abuse Prevention and<br />
Treatment Program<br />
Appendix A to Part 96--Uniform Definitions<br />
of Services<br />
Appendix B to Part 96--SSBG Reporting Form<br />
and Instructions<br />
Subpart D--Direct Funding of <strong>Indian</strong> Tribes<br />
and Tribal Organizations | Top of Page<br />
Sec. 96.40 Scope.<br />
This subpart applies to the community<br />
services, alcohol and drug abuse and mental<br />
health services, preventive health and<br />
health services, primary care, and lowincome<br />
home energy assistance block grants.
[[Page 486]]<br />
Sec. 96.41 General determination.<br />
(a) The Secretary has determined that<br />
<strong>Indian</strong> tribes and tribal organizations would<br />
be better served by means of grants provided<br />
directly by the Secretary to such tribes and<br />
organizations out of the State's allotment<br />
of block grant funds than if the State were<br />
awarded its entire allotment. Accordingly,<br />
where provided for by statute, the Secretary<br />
will, upon request of an eligible <strong>Indian</strong><br />
tribe or tribal organization, reserve a<br />
portion of a State's allotment and, upon<br />
receipt of the complete application and<br />
related submission that meets statutory<br />
requirements, grant it directly to the tribe<br />
or organization.<br />
(b) An <strong>Indian</strong> tribe or tribal<br />
organization may request direct funding<br />
under a block grant program included in this<br />
subpart regardless of whether the State in<br />
which it is located is receiving funds under<br />
the block grant program.<br />
Sec. 96.42 General procedures and<br />
requirements.<br />
(a) An <strong>Indian</strong> tribe or tribal
organization applying for or receiving<br />
direct funding from the Secretary under a<br />
block grant program shall be subject to all<br />
statutory and regulatory requirements<br />
applicable to a State applying for or<br />
receiving block grant funds to the extent<br />
that such requirements are relevant to an<br />
<strong>Indian</strong> tribe or tribal organization except<br />
where otherwise provided by statute or in<br />
this part.<br />
(b) A tribal organization representing<br />
more than one <strong>Indian</strong> tribe will be eligible<br />
to receive block grant funds on behalf of a<br />
particular tribe only if the tribe has by<br />
resolution authorized the organization's<br />
action.<br />
(c) If an <strong>Indian</strong> tribe or tribal<br />
organization whose service population<br />
resides in more than one State applies for<br />
block grant funds that, by statute, are<br />
apportioned on the basis of population, the<br />
allotment awarded to the tribe or<br />
organization shall be taken from the<br />
allotments of the various States in which<br />
the service population resides in proportion<br />
to the number of eligible members or<br />
households to be served in each State. If<br />
block grant funds are required to be<br />
apportioned on the basis of grants during a<br />
base year, the allotment to the <strong>Indian</strong> tribe<br />
or tribal organization shall be taken from<br />
the allotment of the State whose base year<br />
grants included the relevant grants to the
tribe or organization.<br />
(d) The audit required under the block<br />
grant programs shall be conducted by an<br />
entity that is independent of the <strong>Indian</strong><br />
tribe or tribal organization receiving grant<br />
funds from the Secretary.<br />
(e) Beginning with fiscal year 1983, any<br />
request by an <strong>Indian</strong> tribe or tribal<br />
organization for direct funding by the<br />
Secretary must be submitted to the<br />
Secretary, together with the required<br />
application and related materials, by<br />
September 1 preceding the Federal fiscal<br />
year for which funds are sought. A separate<br />
application is required for each block<br />
grant. After the September 1 deadline,<br />
tribal applications will be accepted only<br />
with the concurrence of the State (or<br />
States) in which the tribe or tribal<br />
organization is located.<br />
(f) A State receiving block grant funds<br />
is not required to use those funds to<br />
provide tangible benefits (e.g., cash or<br />
goods) to <strong>Indian</strong>s who are within the service<br />
population of an <strong>Indian</strong> tribe or tribal<br />
organization that received direct funding<br />
from the Department under the same block<br />
grant program for the same fiscal year. A<br />
State, however, may not deny <strong>Indian</strong>s access<br />
to intangible services funded by block grant<br />
programs (e.g., treatment at a community<br />
health center) even if the <strong>Indian</strong>s are
members of a tribe receiving direct funding<br />
for a similar service.<br />
[47 FR 29486, July 6, 1982, as amended at 52<br />
FR 37966, Oct. 13, 1987]<br />
Sec. 96.43 Procedures during FY 1982.<br />
(a) This section applies to the fiscal<br />
year beginning October 1,1981.<br />
(b) A request for direct funding must be<br />
received by the Secretary before the<br />
Secretary has awarded all of the allotment<br />
to the State involved. The application and<br />
related submission may be submitted later<br />
but must be submitted within 75 days after<br />
the beginning of the quarter in which the<br />
State qualified for block grant funds, (or<br />
by August 20,1982 in the case of an <strong>Indian</strong><br />
tribe located in a State that has not<br />
qualified for block grant funds in FY 1982)<br />
except that the application and related<br />
submission for the low-income<br />
[[Page 487]]<br />
home energy assistance program must be<br />
submitted by December 15, 1981. A separate<br />
request and application are required for<br />
each block grant.<br />
[47 FR 29486, July 6, 1982; 47 FR 43062,<br />
Sept. 30, 1982]<br />
Sec. 96.44 Community services.
(a) This section applies to direct<br />
funding of <strong>Indian</strong> tribes and tribal<br />
organizations under the community services<br />
block grant.<br />
(b) The terms <strong>Indian</strong> tribe and tribal<br />
organization as used in the Reconciliation<br />
Act have the same meaning given such terms<br />
in section 4(b) and 4(c) of the <strong>Indian</strong> Self-<br />
Determination and Education Assistance<br />
Act (25 U.S.C. 450b). The terms also include<br />
organized groups of <strong>Indian</strong>s that the State<br />
in which they reside has determined are<br />
<strong>Indian</strong> tribes. An organized group of <strong>Indian</strong>s<br />
is eligible for direct funding based on<br />
State recognition if the State has expressly<br />
determined that the group is an <strong>Indian</strong><br />
tribe. In addition, the statement of the<br />
State's chief executive officer verifying<br />
that a tribe is recognized by that State<br />
will also be sufficient to verify State<br />
recognition for the purpose of direct<br />
funding.<br />
(c) For purposes of section 674(c)(2) of<br />
the Act (42 U.S.C. 9903(c)(2)) an eligible<br />
<strong>Indian</strong> means a member of an <strong>Indian</strong> tribe<br />
whose income is at or below the poverty line<br />
defined in section 673(2) of the Act (42<br />
U.S.C. 9902(2)). An eligible individual<br />
under section 674(c)(2) of the<br />
Reconciliation Act (42 U.S.C. 9903(c)(2))<br />
means a resident of the State whose income
is at or below the poverty line.<br />
(d) An <strong>Indian</strong> tribe or tribal<br />
organization will meet the requirements of<br />
section 675(c)(1) (42 U.S.C. 9904(c)(1)) if<br />
it certifies that it agrees to use the funds<br />
to provide at least one of the services or<br />
activities listed in that section.<br />
(e) An <strong>Indian</strong> tribe or tribal<br />
organization is not required to comply with<br />
section 675(b) (42 U.S.C. 9904(b)) or to<br />
provide the certifications required by the<br />
following other provisions of the<br />
Reconciliation Act.<br />
(1) Section 675(c)(2)(A) (42 U.S.C.<br />
9904(c)(2)(A));<br />
(2) Section 675(c)(3) (42 U.S.C.<br />
9904(c)(3)); and<br />
(3) Section 675(c)(4) (42 U.S.C.<br />
9904(c)(4)).<br />
(4) Section 675(c)(11) (42 U.S.C.<br />
9904(c)(11)).<br />
(f) In each fiscal year, <strong>Indian</strong> tribes<br />
and tribal organizations may expend for<br />
administrative expenses--comparable to the<br />
administrative expenses incurred by State at<br />
the State level--an amount not to exceed the<br />
greater of the amounts determined by:
(1) Multiplying their allotment under<br />
section 674 of the Reconciliation Act (42<br />
U.S.C. 9903) by five percent; or<br />
(2) Multiplying the allotment by the<br />
percentage represented by the ratio of<br />
$55,000 to the smallest State allotment<br />
(excluding territorial allotments) for that<br />
fiscal year.<br />
[47 FR 29486, July 6, 1982, as amended at 52<br />
FR 37967, Oct. 13, 1987]<br />
Sec. 96.45 Preventive health and health<br />
services.<br />
(a) This section applies to direct<br />
funding of <strong>Indian</strong> tribes and tribal<br />
organizations under the preventive health<br />
and health services block grant.<br />
(b) For the purposes of determining<br />
eligible applicants under section 1902(d) of<br />
the Public <strong>Health</strong> Service Act, a grantee<br />
that received a grant directly from the<br />
Secretary in FY 1981 under any of the<br />
programs replaced by the preventive health<br />
and health services block grant that was<br />
specifically targeted toward serving a<br />
particular <strong>Indian</strong> tribe or tribal<br />
organization will be considered eligible if<br />
the grantee is an <strong>Indian</strong> tribe or tribal<br />
organization at the time it requests funds
under this part. Grantees that received<br />
funds under formula or Statewide grants, and<br />
subgrantees that received funds from any<br />
program replaced by the preventive health<br />
and health services block grant, are not<br />
eligible.<br />
Sec. 96.46 Substance abuse prevention and<br />
treatment services.<br />
(a) This section applies to direct<br />
funding of <strong>Indian</strong> tribes and tribal<br />
organizations under the substance abuse<br />
prevention and treatment Block Grant.<br />
(b) For the purpose of determining<br />
eligible applicants under section 1933(d) of<br />
the Public <strong>Health</strong> Service Act (42 U.S.C.<br />
300x-33(d)) an <strong>Indian</strong> tribe or<br />
[[Page 488]]<br />
tribal organization (as defined in<br />
subsections (b) and (c) of section 4 of the<br />
<strong>Indian</strong> Self-Determination and Education<br />
Assistance Act) that received a direct grant<br />
under subpart I of part B of title XIX of<br />
the PHS Act (as such existed prior to<br />
October 1, 1992) in fiscal year 1991 will be<br />
considered eligible for a grant under<br />
subpart 2 of part B of title XIX of the PHS<br />
Act.<br />
(c) For purposes of the substance abuse<br />
prevention and treatment Block Grant, an
<strong>Indian</strong> tribe or tribal organization is not<br />
required to comply with the following<br />
statutory provisions of the Public <strong>Health</strong><br />
Service Act: 1923 (42 U.S.C. 300x-23), 1925<br />
(42 U.S.C. 300x-25), 1926(42 U.S.C. 300x-<br />
26), 1928 (42 U.S.C. 300x-28), 1929 (42<br />
U.S.C. 300x-29),and 1943(a)(1) (42 U.S.C.<br />
300x-53(a)(1)). An <strong>Indian</strong> tribe or tribal<br />
organization is to comply with all other<br />
statutes and regulations applicable to the<br />
Substance Abuse Prevention and Treatment<br />
Block Grant.<br />
In each case in which an <strong>Indian</strong> Tribe<br />
receives a direct grant, the State is also<br />
responsible for providing services to Native<br />
Americans under the State's Block Grant<br />
program.<br />
[58 FR 17070, Mar. 31, 1993]<br />
Sec. 96.47 Primary care.<br />
Applications for direct funding of<br />
<strong>Indian</strong> tribes and tribal organizations under<br />
the primary care block grant must comply<br />
with 42 CFR Part 51c (Grants for Community<br />
<strong>Health</strong> Services).<br />
Sec. 96.48 Low-income home energy<br />
assistance.<br />
(a) This section applies to direct<br />
funding of <strong>Indian</strong> tribes under the low-
income home energy assistance program.<br />
(b) The terms <strong>Indian</strong> tribe and tribal<br />
organization as used in the Reconciliation<br />
Act have the same meaning given such terms<br />
in section 4(b) and 4(c) of the <strong>Indian</strong> Self-<br />
Determination and Education Assistance Act<br />
(25 U.S.C. 450b) except that the terms shall<br />
also include organized groups of <strong>Indian</strong>s<br />
that the State in which they reside has<br />
expressly determined are <strong>Indian</strong> tribes or<br />
tribal organizations in accordance with<br />
State procedures for making such<br />
determinations.<br />
(c) For purposes of section 2604(d) of<br />
the Act (42 U.S.C. 8623(d)), an organized<br />
group of <strong>Indian</strong>s is eligible for direct<br />
funding based on State recognition if the<br />
State has expressly determined that the<br />
group is an <strong>Indian</strong> tribe. A statement by the<br />
State's chief executive officer verifying<br />
that a tribe is recognized by that State<br />
will also be sufficient to verify State<br />
recognition for the purpose of direct<br />
funding.<br />
(d) The plan required by section<br />
2604(d)(4) of the Reconciliation Act (42<br />
U.S.C. 8623(d)(4)) shall contain the<br />
certification and information required for<br />
States under section 2605 (b) and (c) of<br />
that Act (42 U.S.C. 8624 (b) and (c)). An<br />
<strong>Indian</strong> tribe or tribal organization is not<br />
required to comply with section 2605(a)(2)
of the Act (42 U.S.C. 8624(a)(2)).<br />
(e) Where a tribe requests that the<br />
Secretary fund another entity to provide<br />
energy assistance for tribal members, as<br />
provided by section 2604(d)(3) of the Act<br />
(42 U.S.C. 8623(d)(3)), the Secretary shall<br />
consider the following factors in selecting<br />
the grantee: the ability of the other entity<br />
to provide low-income home energy<br />
assistance, existing tribal-State agreements<br />
as to the size and location of the service<br />
population, and the history of State<br />
services to the <strong>Indian</strong> people to be served<br />
by the other entity.
Need for Uniform Operational Guidance in Determining Eligibility<br />
for <strong>Indian</strong>-specific Benefits and Protections under the Affordable Care Act<br />
ISSUE:<br />
The ACA includes three <strong>Indian</strong>-specific sections that provide special protections and benefits to AI/ANs. CMS<br />
has determined that the two Exchange-related definitions (for Exchange cost-sharing and enrollment<br />
protections) “operationally means the same thing.” 1 IRS has said informally that its definition section, which<br />
protects against tax penalties being applied to AI/ANs for not maintaining minimum essential coverage, has<br />
the same meaning as the definitions used for the Exchange.<br />
CMS has opined that the eligibility standard for the <strong>Indian</strong>-specific provisions under the ACA are “slightly<br />
different” from the AI/AN eligibility standards for IHS services. 2 In response to requests from States for<br />
clarification about who an “<strong>Indian</strong>” is, CMS adopted Medicaid regulations that simplified the IHS eligibility<br />
rules. See, 42 CFR 447.50.<br />
OBJECTIVE:<br />
Uniform operational guidance is needed, consistent with 42 CFR 447.50, regarding eligibility determinations<br />
for <strong>Indian</strong>-specific benefits and protections under Medicaid and the Affordable Care Act through HHS and IRS<br />
guidance or regulation.<br />
RECOMMENDED ACTIONS:<br />
1. Issue operational guidance from HHS and Treasury to assist Exchange enrollment staff and others as<br />
necessary in determining eligibility for <strong>Indian</strong>-specific benefits and protections for Exchange and<br />
Medicaid coverage;<br />
2. Rely on the CMS regulations, 42 C.F.R. § 447.50, in order to permit a uniform application across<br />
Medicaid, state and federal Exchanges and IRS (for the exemption for AI/ANs from the tax penalty for<br />
not maintaining minimum essential coverage).<br />
AUTHORITY:<br />
It is well established that (1) the federal government has a trust responsibility to provide health care to<br />
<strong>Indian</strong>s, and (2) that laws for the benefit of <strong>Indian</strong>s should be construed liberally in favor <strong>Indian</strong>s.<br />
As established under 45 C.F.R. § 155.315(h) Flexibility in information collection and verification, the Secretary<br />
of HHS has discretionary authority to approve modifications to the methods used for the collection and<br />
verification of information related to eligibility for enrollment through an Exchange and for eligibility for<br />
Exchange insurance affordability programs. This authority may be exercised by the Secretary “provided that<br />
HHS finds that such modification would reduce the administrative costs and burdens on individuals while<br />
maintaining accuracy and minimizing delay, [and] that it would not undermine coordination with Medicaid<br />
and CHIP…” As indicated below, these criteria would be met through the issuance and reliance on uniform<br />
operational guidance.<br />
TRIBAL SUPPORT FOR USING CMS’ MEDICAID REGULATIONS AS THE UNIFORM OPERATIONAL GUIDANCE<br />
<strong>National</strong> and regional tribal organizations support the application of uniform operational guidance using the<br />
CMS Medicaid regulation at 42 C.F.R. § 447.50 for purposes of implementing the <strong>Indian</strong>-specific provisions of<br />
the Affordable Care Act. Resolutions of support were adopted by the <strong>National</strong> Congress of American <strong>Indian</strong>s<br />
(NCAI), the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NIHB), and the Tribal Technical Advisory Group to CMS (TTAG).<br />
1 Exchange Establishment Final Rule, 77 Fed. Reg. 18346.<br />
2 Exchange Establishment Final Rule, 77 Fed. Reg. 18383.<br />
Page 1 of 2
POTENTIAL RAMIFICATIONS FOR FAILING TO ISSUE UNIFORM OPERATIONAL GUIDANCE:<br />
Failure to issue uniform operational guidance will impede Exchange, Medicaid and IRS staff in making accurate<br />
and consistent determinations of eligibility as well as delay or completely deny access for some AI/ANs to the<br />
<strong>Indian</strong>-specific benefits and protections established under the Affordable Care Act.<br />
Delayed eligibility for some AI/AN children: An AI/AN child who is not allowed to enroll as a tribal<br />
member until her 18 th birthday may not be considered eligible for Exchange-related <strong>Indian</strong>-specific<br />
cost-sharing and enrollment protections, despite being considered an AI/AN for purposes of IHS,<br />
Medicaid and CHIP coverage.<br />
Unwarranted application of tax penalties: If an AI/AN who is eligible and, in fact, is accessing IHS<br />
services decides not to secure health insurance coverage, but is not (ultimately) determined to be<br />
eligible as an “<strong>Indian</strong>” for the exemption from the requirement to secure minimum essential coverage,<br />
this individual could be subject to significant tax penalties imposed under the ACA by the Internal<br />
Revenue Service.<br />
Reduced timeliness: The consolidated and streamlined Medicaid and Exchange application process is<br />
intended to rely, to the greatest extent possible, on electronic verification of application-related<br />
information. The lack of uniform operational guidance would complicate (although not prevent) the<br />
use of automated databases that may be available for electronic verification, such as using the IHS<br />
beneficiary roster, hamper coordination between Medicaid and Exchange eligibility, and likely increase<br />
the administrative costs and burden on individuals.<br />
Reduced accuracy in eligibility determinations: If guidance is not issued by CMS, or if the guidance<br />
issued does not provide uniformity across the <strong>Indian</strong>-specific provisions in Medicaid, Exchange<br />
coverage, and pertaining to the exemption from tax penalties, thereby requiring each Exchange to<br />
identify any differences in eligibility standards under the various definitions, including understanding<br />
the differences, if any, in documentation permitted to satisfy each definition of <strong>Indian</strong>, error rates for<br />
eligibility determinations will increase.<br />
Blocked access for some Alaska Natives: Some Alaska Native adults and children may not be<br />
considered AI/AN by Exchanges until their parents die and they inherit stock in an Alaska Native<br />
corporation; likewise, their children would not be considered AI/AN by Exchanges until they die and<br />
the stock in an Alaska Native corporation is passed along to children even though the parent and the<br />
children would qualify as AI/AN under Medicaid and other governmental services (e.g., IHS and BIA).<br />
Reduced involvement of AI/AN in insurance options: Even if the instances of an individual being<br />
determined to be “<strong>Indian</strong>” for one <strong>Indian</strong>-specific provision and not for another represent a relatively<br />
small percentage of the total population (which we anticipate), this outcome would likely cast a<br />
shadow over AI/ANs involvement with ACA implementation more generally. For example, AI/ANs may<br />
be much more reluctant to consider transitioning from the IHS-based coverage model to<br />
comprehensive Exchange coverage if there is a risk of ending-up subject to significant cost-sharing<br />
requirements under a different, potentially unknown application of a definition of <strong>Indian</strong>.<br />
For questions please contact Jim Roberts, Policy Analyst, (503) 228-4185 or email at jroberts@npaihb.org.<br />
Page 2 of 2
Dear Tribal Representatives,<br />
October 25, 2012<br />
You are invited to join the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NIHB) on a bold journey to GO THE EXTRA MILE with NIHB. On<br />
November 1, 2012, the first day of both American <strong>Indian</strong> Heritage Month and Diabetes Awareness month, NIHB will<br />
launch its GO THE EXTRA MILE initiative, and we invite you to join us on this year-long journey. The kickoff event will<br />
take place on November 1 st at 8 AM in front of the <strong>National</strong> Museum of American <strong>Indian</strong>s in Washington, D.C., and you<br />
are invited to join us for this event and walk a mile with us. If you are unable to join us, we encourage you to organize<br />
your own community event on November 1 st to GO the EXTRA MILE and begin this journey by walking the first mile<br />
together.<br />
The GO the EXTRA MILE initiative is a result of the NIHB signing the CEO pledge, which is part of a national campaign to<br />
encourage Executive Directors to commit to supporting and fostering a physically-active workplace. NIHB’s GO the<br />
EXTRA MILE initiative achieves these goals by creating a workplace that supports physical activity for every member of<br />
its staff. Through the GO THE EXTRA MILE with NIHB initiative, we will provide staff 30 minutes during the work day to<br />
walk one mile each day for a year. We will aggregate these miles and “virtually” walk to each of the 12 <strong>Indian</strong> <strong>Health</strong><br />
Service Areas, either to an Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> or to a Tribal Partner in Areas that do not have a <strong>Board</strong>. We invite<br />
you to join NIHB by signing the CEO pledge and participating in the November 1 st launch. You will have access to the<br />
NIHB Go The Extra Mile website, which will include a toolkit, electronic mapping for your journey, and access to<br />
information like “Hot <strong>Health</strong> Tips” from our partner, the Association of American <strong>Indian</strong> Physicians. More information is<br />
also provided in the enclosed materials.<br />
As you know, American <strong>Indian</strong>s and Alaska Natives (AI/AN) have the highest age-adjusted prevalence of Type 2 diabetes<br />
among all U.S. racial and ethnic groups and our People’s obesity rate is 39% for those 18 and older. Among AI/AN adults<br />
18 and older, the percentage of inactive physical activity in 2010 was 53.9%, which was far from meeting federal physical<br />
activity guidelines (at least 150 minutes or 30 minutes a day of moderate-intensity aerobic activity per week, i.e., brisk<br />
walking). There is a correlation between physical activity and chronic diseases. The Diabetes Prevention Program clinical<br />
trial, led by the <strong>National</strong> Institutes of <strong>Health</strong>, has shown that getting at least the recommended 30 minutes a day of<br />
moderate physical activity and losing 5% to 7% of body weight can reduce the risk of developing type 2 diabetes by 58%<br />
in people at risk. NIHB’s GO the EXTRA MILE is one small step toward supporting diabetes and obesity prevention for<br />
AI/AN.<br />
Remember, the journey for health is not a marathon, nor a sprint, but a relay that we, together, walk in order<br />
to outsmart chronic diseases that threaten our health in <strong>Indian</strong> Country<br />
We will be joined for the November 1 st kick off event by the Association of American <strong>Indian</strong> Physicians, American<br />
Diabetes Association, Juvenile Diabetes Research Foundation, <strong>National</strong> Obesity Awareness Coalition, and the <strong>National</strong><br />
Coalition on Promoting Physical Activity. We hope to see you there and on the virtual road ahead, as we GO the EXTRA<br />
MILE together.<br />
Miigwech – Thank you,<br />
Stacy A. Bohlen, Executive Director, NIHB
Introduction<br />
NIHB to Launch a Workplace Fitness Program:<br />
GO the EXTRA MILE!<br />
October 25, 2012<br />
The <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NIHB) is excited to introduce our new healthy workplace initiative, GO the<br />
EXTRA MILE. The goal of the NIHB GO the EXTRA MILE initiative is to create a healthier work<br />
environment and promote employee health through providing staff members with thirty paid minutes each work<br />
day to go for a walk. Along with the NIHB Executive Director, each staff member pledged to walk an<br />
additional mile each day for an entire year. The GO the EXTRA MILE initiative stems from the CEO Pledge, a<br />
project through the <strong>National</strong> Coalition on Promoting Physical Activity (NCPPA), which urges CEOs to pledge<br />
their commitment to foster a healthy workplace. The NIHB GO the EXTRA MILE initiative is the newest<br />
element of collaborated efforts within the <strong>National</strong> Physical Activity Plan.<br />
The <strong>National</strong> Physical Activity Plan<br />
The <strong>National</strong> Physical Activity Plan, the first, national comprehensive plan to support and encourage physical<br />
activity among all Americans, was launched in 2010 through a 10 month collaboration between experts from<br />
various, diverse fields. The plan comprises a wide range of public policy recommendations across eight broad<br />
sectors. Through the <strong>National</strong> Physical Activity Plan, hundreds of organizations are working together to change<br />
our communities in ways that will enable every American to be physically active. Its ultimate purpose is to<br />
improve health, prevent disease and disability, and enhance quality of life.<br />
The CEO Pledge<br />
The <strong>National</strong> Coalition for Promoting Physical Activity (NCPPA) is a 501(c)(4) tax exempt organization that is<br />
leading the implementation of the <strong>National</strong> Physical Activity Plan at the national level through The CEO<br />
Pledge, which encourages every CEO in the United States to recognize physical activity as an important driver<br />
of employee health. Studies of employee wellness programs consistently find that executive leadership is<br />
critical to employee engagement. If employees believe that creating a culture of physical activity is an executive<br />
priority, employees are more likely to be physically active.<br />
The CEO Pledge states:<br />
“For the betterment of my company, our employees, their families, and our country, I pledge to<br />
improve employee health and wellness by providing opportunities and resources for physical<br />
activity before, during or after the workday, and to enhance my own health and wellness by<br />
engaging in regular physical activity.”<br />
GO the EXTRA MILE Initiative
There is a strong correlation between obesity and diabetes—more than 80% of people with Type 2 diabetes are<br />
overweight. With diabetes and obesity on the rise, every organization in the United States has an obligation and<br />
responsibility to lead its community to a healthier future. Nowhere is this need more urgent than in <strong>Indian</strong><br />
Country. At nearly 16.1%, American <strong>Indian</strong>s and Alaska Natives (AI/AN) have the highest age-adjusted<br />
prevalence of Type 2 diabetes among all U.S. racial and ethnic groups. The obesity rate, which is determined by<br />
having a body max index (BMI) of 30 or greater, is 39% for AI/AN 18 and older. Among AI/AN adults 18 and<br />
older, the percentage of inactive physical activity in 2010 was 53.9%, which did not meet federal physical<br />
activity guidelines (at least 150 minutes of moderate-intensity aerobic activity, i.e., brisk walking a week).<br />
Mission<br />
The NIHB recognizes this urgent need to advocate for physical activity as a preventive measure against chronic<br />
diseases. NIHB would like to welcome Executive Directors from Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>s, Tribes, and other<br />
Tribal organizations to join NIHB in recognizing this urgent need by signing the CEO Pledge and Go the<br />
EXTRA MILE.<br />
Goal<br />
NIHB’s yearly goal is to encourage every NIHB employee to walk a mile every day (an additional mile separate<br />
from daily routine) for a year. With 13 employees, the minimum yearly walking goal NIHB is aiming to achieve<br />
is 4,745 miles. With these aggregated miles, NIHB will “virtually” walk to all Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>s and<br />
the Midwest Alliance of Sovereign Tribes (Bemidji Area). The idea is to provide encouragement to Tribes and<br />
Tribal organizations to GO the EXTRA MILE. Together, we can help transform our Tribal nation’s overall<br />
health and wellbeing.<br />
The Plan<br />
As part of the CEO Pledge, NIHB has established a plan to implement exercise in the workplace.<br />
Provide thirty paid minutes a day for staff to go for a walk.<br />
Track and report miles daily.<br />
Arrange healthy incentives for meeting team walking goals.<br />
Coordinate community walks.<br />
Update monthly the “GO the EXTRA MILE” website with physical activity events, exercise<br />
information, and progress from NIHB and participating organizations.<br />
Offer a toolkit to encourage other organizations to GO the EXTRA MILE.<br />
One of NIHB’s primary areas of focus is to improve the health of AI/AN. Through exercise and diet, many<br />
American <strong>Indian</strong>s who suffer from this disease, can help mitigate the symptoms of diabetes through diet and
exercise. NIHB GO the EXTRA MILE initiative is just a small way that NIHB can demonstrate positive and<br />
supportive workplace efforts to support diabetic employees, help prevent the onset of Type 2 diabetes through<br />
added physical activity and enhance the quality of health for all employees.<br />
Kick-off Launch<br />
NIHB’s kickoff launch for the GO the EXTRA MILE is on November 1 st , 2012 at 8:00 am in front of the<br />
<strong>National</strong> Museum of American <strong>Indian</strong>s in Washington, D.C. November is Native American Heritage Month and<br />
<strong>National</strong> Diabetes Awareness Month—the perfect time to start our new healthy initiative for promoting exercise<br />
in the workplace.<br />
It is not a marathon, or a sprint, but a relay that we, together, walk in order to outsmart chronic diseases that<br />
threaten our health in <strong>Indian</strong> Country.
Wed. Nov 14 th : SDPI <strong>National</strong> Call-In Day<br />
We Need Your Voice to Save the SDPI<br />
November 14, 2012<br />
The Special Diabetes Program for <strong>Indian</strong>s (SDPI) provides critical programs that are helping our Tribal<br />
communities address complications and burdens of diabetes. This critical program is set to expire unless<br />
Congress acts to renew it. We need your help. On November 14 th - World Diabetes Day - please join NIHB<br />
and Tribal communities from across the country in asking your Senators and Representatives to support renewal<br />
of the SDPI this year! We need to make sure that Congress renews SDPI!<br />
What You Can Do: Contact your Senate and House of Representative member on November 14 th and request<br />
your Member to support renewal of SDPI.<br />
• To determine your Representative and contact information, click here.<br />
• To determine your Senators and contact information, click here.<br />
• To be connected to a Senator or Representative via phone, call the Congressional Switchboard at<br />
1-(800) 828-0498 or (202) 224-3121 and ask to be connected to your Senator or Representative and after<br />
you are connected to the office, ask to speak with the <strong>Health</strong> aide.<br />
Tell Your Representative:<br />
• I am a constituent and calling to ask Senator ____ / Representative ____ to support a multi-year renewal<br />
of the Special Diabetes Program for <strong>Indian</strong>s this year.<br />
• SDPI proves that federal investment in community-driven, culturally-appropriate prevention and<br />
education programs can reduce a person’s risk of developing diabetes or of developing complications for<br />
those who have diabetes.<br />
• If SDPI is not renewed this year, critical diabetes prevention and education services will be eliminated<br />
and the progress that has been made will be reversed.<br />
• Thank you for your support of this critical program.<br />
Questions: Please contact NIHB’s Senior Legislative Associate, Jeremy Marshall at (202) 507-4078.or<br />
Jmarshall@nihb.org.
Background on the SDPI<br />
Congress established the Special Diabetes Program for <strong>Indian</strong>s (SDPI) in 1997 to address the growing epidemic<br />
of diabetes in American <strong>Indian</strong> and Alaska Natives (AI/ANs) communities. AI/ANs have the highest rates of<br />
type 2 diabetes in the United States, 2.8 times higher than the general population. The SDPI is currently funded<br />
at $150 million per year through Fiscal Year (FY) 2013.<br />
The program will expire in 2013 unless it is reauthorized.<br />
To ensure uninterrupted funding for SDPI, it is crucial that Congress pass a reauthorization this year. SDPI<br />
proves that federal investment in community-driven, culturally-appropriate prevention programs has immensely<br />
positive results:<br />
• Average blood sugar levels among the AI/AN population decreased a full percentage point (from 9.0<br />
percent to 8.0 percent) between 1996 and 2011, translating into a 40% reduction in risks for many<br />
complications.<br />
• Average LDL (bad) cholesterol declined over 20 percent between 1998 and 2011, significantly lowering<br />
the risk of cardiovascular complications.<br />
• Between 1995 and 2006, the incidence rate of End Stage Renal Disease (ESRD) in AI/AN individuals<br />
with diabetes fell by 27.7 percent – a greater decline than for any other racial or ethnic group - which<br />
translates into millions of dollars in savings for Medicare, the <strong>Indian</strong> <strong>Health</strong> Service, and other third<br />
party payers.
Future MMPC Meetings & Conference Calls:<br />
2:00PM - 4:00 PM EST<br />
Conference Call In Number: 866-303-3137<br />
Pass Code: 414526<br />
December 5, 2012<br />
January 2013-TBD<br />
March 6, 2013<br />
April 3, 2013<br />
May 1, 2013<br />
June 5, 2013<br />
August 7, 2013<br />
September 4, 2013<br />
October 2, 2013<br />
December 4, 2013<br />
Face to Face Meetings:<br />
February 2013 TBD,Washington, D.C.<br />
July 2013, TBD, Washington, D.C.<br />
November 2013, TBD,Washington, D.C.<br />
______________________________________________________________________________<br />
Future TTAG Meetings & Conference Calls:<br />
2:30PM - 4:00 PM EST<br />
Call in number 1-877-267-1577<br />
December 12, 2012: Meeting ID: 9925<br />
January 9, 2013: Meeting ID: TBD<br />
March 13, 2013: Meeting ID: TBD<br />
April 10, 2013: Meeting ID: TBD<br />
May 8, 2013: Meeting ID: TBD<br />
June 12, 2013: Meeting ID: TBD<br />
August 14, 2013: Meeting ID: TBD<br />
September 11, 2013: Meeting ID: TBD<br />
October 9, 2013: Meeting ID: TBD<br />
December 11, 2013: Meeting ID: TBD<br />
Face to Face Meetings:<br />
February 2013: NMAI, Washington, D.C.<br />
July 2013: NMAI, Washington, D.C.<br />
November 2013: NMAI, Washington, D.C.
REGULATIONS REVIEW UPDATE<br />
TABLE OF CONTENTS<br />
FEDERAL REGISTER IDENTIFIER CMS 10445 1<br />
DRAFT NIHB COMMENT CMS 10445 3<br />
RRIAR V. 2.11 6<br />
ACTIVE, NEW & ONGOING MMPC/TTAG ISSUES, STATUS, GOALS & NEXT<br />
STEPS<br />
BIO—JOHN O’BRIEN, DIRECTOR, HEALTHCARE & INSURANCE, OPT 47<br />
NIHB COMMENTS ON DRAFT MULTI-STATE PLAN PROGRAM APPLICATION 48<br />
DEAR GOVERNOR LETTER FROM SECRETARY SEBELIUS 55<br />
ANALYSIS OF TRIBAL CONSULTATION POLICIES FOR HEALTH INSURANCE EXCHANGES 57<br />
TRIBAL CONSULTATION FOR HEALTH INSURANCE EXCHANGES SURVEY QUESTIONS 75
Regulation Review and Impact Analysis Report<br />
v. 2.11<br />
-- DRAFT --<br />
As of November 12, 2012<br />
Attachments<br />
- Table A: Listing and Status Report on Regulations Reviewed (through 11/9/2012)<br />
- Table B: Summary and Analysis of Agency Notices and Regulations (through 8/15/2012)<br />
- Table C: NIHB Recommendations and Evaluation of Agency’s Subsequent Actions (through 5/15/2012)
The purpose of the Regulation Review and Impact Analysis Report (RRIAR) is to identify and summarize key regulations issued by the Centers for<br />
Medicare and Medicaid Services (CMS) pertaining to Medicare, Medicaid, CHIP, and health reform 1 that affect (a) American <strong>Indian</strong>s and Alaska Natives<br />
and/or (b) <strong>Indian</strong> <strong>Health</strong> Service, <strong>Indian</strong> Tribe and tribal organization, and urban <strong>Indian</strong> organization providers. Furthermore, the RRIAR includes a<br />
summary of the regulatory analyses prepared by the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NIHB) 2 , if any, and indicates the extent to which the recommendations<br />
made by NIHB were incorporated into any subsequent CMS actions.<br />
In addition to this cover page, the report consists of three tables –<br />
- Table A provides a status report on the RRIAR itself, listing the regulations included in the RRIAR to date, and the components of the analysis<br />
provided under each. The regulations are organized in four sections: I. Medicaid; II. Medicare; III. <strong>Health</strong> Reform; and IV. Other.<br />
- Table B lists key regulations issued by CMS, due dates for comments, a synopsis of the CMS action, and a summary of the analysis, if any,<br />
prepared by NIHB.<br />
- Table C identifies the recommendations made by NIHB pertaining to each regulation, if any, and evaluates the extent to which the<br />
recommendations made by NIHB were incorporated into subsequent CMS actions.<br />
Regulations with pending due dates for public comments –<br />
2.d. Medicare Advantage and Part D Plan Applications (CMS-10237 and CMS-10137; comments due 11/13/2012; under review)<br />
11.e. Medicare Advantage Quality Bonus Payment Demonstration (CMS-10445; comments due 11/16/2012; comments drafted)<br />
60.d. Medicare Electronic Data Interchange Form (CMS-10164; comments due 11/16/2012)<br />
84. Monthly State File of Dual Eligible Enrollees (CMS-10143; comments due 11/16/2012)<br />
49.b. Medicare Credit Balance Reporting Requirements (CMS-838; comments due 11/16/2012)<br />
85. Minimum Data Set for Medicaid Incentives for Prevention of Chronic Diseases (CMS-10444; comments due 11/19/2012)<br />
83. Medicaid Statistical Information System (CMS-R-284; comments due 11/19/2012)<br />
3.c. DME Certificate of Medical Necessity (CMS-846-849, 10125, 0126; comments due 11/23/2012)<br />
88. Early Retiree Reinsurance Program Survey (CMS-10408; comments due 11/27/2012)<br />
95. <strong>Indian</strong> <strong>Health</strong> Service Forms to Implement Privacy Rule (IHS-810, etc.; comments due 11/30/2012 approx.)<br />
11.d. Medicare Bid Pricing Tool (CMS-10142; comments due 12/4/2012)<br />
11.f. Medicare PDP Benefit Package Formulary (CMS-R-262; comments due 12/4/2012)<br />
11.c. Outcome Measures for Quality Assessment in Medicare Advantage and Special Needs Plans (CMS-10451; comments due 12/26/2012)<br />
11.g. Medicare Advantage Reporting Requirements (CMS-10261; comments due 12/26/2012)<br />
94. Methodology for Designation of Frontier and Remote Areas (HRSA/no ref. #; comments due 1/4/2013)<br />
4.b. Hospital Outpatient and Ambulatory Service Center Payment Systems (CMS-1589-FC; comments due 1/12/2013 approx.)<br />
70.a. Medicare Physician Fee Schedule Rule (CMS-1590-FC; comments due 1/13/2013 approx.)<br />
96. IHS New System of Records (IHS/no ref. #; comments due 12/13/2012)<br />
Comments recently submitted by NIHB, TTAG and/or other tribal organizations–<br />
80. Notice of Denial of Medical Coverage (or Payment) (CMS-10003: comments submitted 11/6/2012)<br />
66. Requirements for Charitable Hospitals: Proposed Rule (IRS-130266-11; comments submitted 9/24/2012)<br />
1 “<strong>Health</strong> reform” is inclusive of (1) the Patient Protection and Affordable Care Act (Pub. L. 111-148), incorporating by reference S. 1790 as reported by the<br />
Committee on <strong>Indian</strong> Affairs of the Senate in December 2009 (containing amendments to the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act, IHCIA), and as amended by<br />
the <strong>Health</strong> Care and Education Reconciliation Act (HCERA; Public Law 111–152) (collectively referred to as “ACA”) and (2) the American Recovery and<br />
Reinvestment Act of 2009 (ARRA, Pub. L. 111-5)<br />
2 The analyses and recommendations may include those made by the Tribal Technical Advisory Group to CMS (TTAG) and other tribal organizations.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 2 of 3 11/12/2012
64. Policy on Conferring with Urban <strong>Indian</strong> Organizations: Request for Comments (No ref #; comments submitted by ANTHC and NCUIH<br />
9/23/2012)<br />
65. <strong>Health</strong> Care Reform Insurance Web Portal Requirements (CMS-10320; submitted 9/13/2012)<br />
Regulations under OMB (Office of Management and Budget) review –<br />
92. Insurance Market Rules (CMS-9972-P; sent to OMB 11/8/2012)<br />
31.d. Standards Related to <strong>Health</strong> Benefits (CMS-9980-P; sent to OMB 11/8/2012)<br />
81. Part II--Regulatory Provisions To Promote Program Efficiency, Transparency, and Burden Reduction (CMS-1367-P; sent to OMB 8/2/2012)<br />
Recent (final) rules issued –<br />
71.a. Physician Fee Schedule, ESRD, Bad Debt, etc (CMS-1352-F; issued 11/9/2012)<br />
52. Home <strong>Health</strong> Prospective Payment System Rate for CY2013 (CMS-1358;F; issued 11/8/2012)<br />
44. Medicaid Payment for Primary Care Services and Charges for Vaccine Administration: Proposed Rule (CMS-2370-P; issued 11/6/2012)<br />
1.b. MU EHR Incentive Payments--Stage 2 (CMS-0044-F; issued 9/4/2012; corrections issued 10/23/2012)<br />
Contacts: Jennifer Cooper (JCooper@nihb.org); Liz Heintzman (EHeintzman@nihb.org)<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 3 of 3 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
1.a.<br />
1.b.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
MU EHR Incentive Payments<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicare and Medicaid<br />
Programs; Electronic <strong>Health</strong><br />
Record (EHR) Incentive Program<br />
AGENCY: CMS<br />
MU EHR Incentive Payments--<br />
Stage 2<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicare and Medicaid<br />
Programs; Electronic <strong>Health</strong><br />
Record Incentive Program Stage 2<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/09/2012<br />
File Code<br />
CMS-0033-P F<br />
CMS_ FRDOC_<br />
0001-0520<br />
CMS-0044-PF<br />
CMS-0044-<br />
CN2<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
SECTION I: MEDICAID (AND DUAL<br />
MEDICAID AND MEDICARE)<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Beginning on page 1 of 38<br />
SECTION II: MEDICARE Beginning on page 9 of 38<br />
Section III: <strong>Health</strong> Reform Beginning on page 23 of 38<br />
Section IV: Other Beginning on page 36 of 38<br />
SECTION I: MEDICAID (AND DUAL<br />
MEDICAID AND MEDICARE)<br />
Issue Date: 1/13/2010<br />
Due Date: 3/15/2010<br />
NIHB File Date: Pre-2/15/2010<br />
Date of Subsequent Action, if any:<br />
Issued Final Rule 7/28/2010;<br />
issued correction 12/29/2010<br />
Additional: NIHB/TTAG provided<br />
analysis 2/03/2011; 5/23/2011;<br />
7/05/2011; 12/14/2011<br />
Issue Date: 3/7/2012;<br />
Due Date: 5:00 pm, 5/7/2012<br />
NIHB File Date: 5/7/2012<br />
Date of Subsequent Action, if any:<br />
Issued correction 4/18/2012;<br />
issued Final Rule 9/4/2012;<br />
issued correction 10/23/2012<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: [To be<br />
entered.]<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: √<br />
NIHB recommendations included: To<br />
be entered.<br />
Subsequent Agency action: [To be<br />
entered.]<br />
Analysis of Agency action: [To be<br />
conducted and entered.]<br />
: regulation review complete : reg. currently under review : regulation release pending<br />
Page 1 of 38
RRIAR<br />
Ref.<br />
#<br />
1.c.<br />
8.<br />
9.<br />
13.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
HIT Revised Standards--CMS<br />
EHR Program<br />
ACTION: Proposed Final Rule<br />
NOTICE: <strong>Health</strong> Information Tech.;<br />
Revised Standards, Implementation<br />
Specs and Cert. Criteria for EHRs<br />
AGENCY: ONC, HHS<br />
Sec. 1115 Waiver Transparency<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicaid; Review/App.<br />
Process for Sec. 1115 Demo’s<br />
AGENCY: CMS<br />
Med/Med Provider Survey<br />
ACTION: Final Rule w/Comments<br />
NOTICE: Medicare, Medicaid, and<br />
CHIP Programs; Additional<br />
Screening Requirements, App. Fee<br />
AGENCY: CMS<br />
Provider Complaint Filing<br />
ACTION: Proposed Rule<br />
NOTICE: Medicare & Medicaid<br />
Providers & Suppliers to notify<br />
beneficiaries of the right to file<br />
written complaint with QIO<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
HHS<br />
RIN 0991-<br />
AB82<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 3/7/2012<br />
Due Date: 5:00 pm, 5/7/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
9/4/2012<br />
CMS-2325-PF Issue Date: 9/17/2010<br />
Due Date: 11/16/2010<br />
NIHB File Date: 11/15/2010<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
2/27/2012<br />
CMS-6028-FC Issue Date: 9/23/2010<br />
Due Date: 11/16/2010<br />
NIHB File Date: 11/16/2010<br />
Date of Subsequent Agency<br />
Action, if any: 2/1/2011<br />
Additional: NIHB provided<br />
CMS-3225-P<br />
RIN 0938-<br />
AP94<br />
examples of hardship 3/25/11<br />
Issue Date: 2/2/2011<br />
Due Date: 4/4/2011<br />
NIHB File Date: 4/4/2011<br />
Date of Subsequent Agency<br />
action, if any: Sent Final Rule<br />
to OMB for review 6/2/2011<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
Summary of Agency<br />
action: √<br />
TTAG analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
TTAG recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: To be<br />
entered.<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: √<br />
NIHB recommendations included: √<br />
Subsequent Agency action: None as<br />
of 5/31/2011.<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 2 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
16.a.<br />
16.b.<br />
17.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
New Medicaid Community First<br />
Choice Option<br />
ACTION: Proposed Final Rule<br />
NOTICE: Community First Choice<br />
Option<br />
AGENCY: CMS<br />
Medicaid HCBS Waivers<br />
ACTION: Proposed Rule<br />
NOTICE: Medicaid; State Plan<br />
Home and Community-Based<br />
Services, 5-Year Period for<br />
Waivers, Provider Payment<br />
Reassignment; Setting<br />
Requirements<br />
AGENCY: CMS<br />
Assuring Access to Covered<br />
Services<br />
ACTION: Request for Information<br />
NOTICE: Opportunities for<br />
Alignment Under Medicaid and<br />
Medicare<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-2337-PF<br />
RIN 0938-<br />
AQ35<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 2/25/2011<br />
Due Date: 4/26/2011<br />
NIHB File Date: 4/26/2011<br />
Date of Subsequent Agency<br />
Action, if any: 5/7/2012<br />
CMS-2249-P2 Issue Date: 5/3/2012<br />
Due Date: 7/2/2012 (corrected)<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-5507-NC<br />
Issue Date: 5/16/2011<br />
Due Date: 7/11/2011<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: In<br />
progress.<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: No<br />
recommendations submitted<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 3 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
20.<br />
23.<br />
26.<br />
28.a.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Assuring Access to Services<br />
ACTION: Proposed Rule<br />
NOTICE: Medicaid Program;<br />
Methods for Assuring Access to<br />
Covered Medicaid Services<br />
AGENCY: CMS<br />
Request for Approval of<br />
Medicaid and CHIP Standard<br />
Forms<br />
ACTION: Request for Comment<br />
NOTICE: Clearance for Medicaid<br />
and CHIP State Plan, Waiver, and<br />
Program Submissions<br />
AGENCY: CMS<br />
Medicaid Home <strong>Health</strong><br />
ACTION: Proposed Rule<br />
NOTICE: Medicaid Program; Faceto-Face<br />
Requirements for Home<br />
<strong>Health</strong> Services; Policy Changes<br />
and Clarifications Related to HH<br />
AGENCY: CMS<br />
Medicaid Eligibility Under ACA<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicaid; Eligibility<br />
Changes Under the ACA<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-2328-P<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 5/6/2011<br />
Due Date: 7/5/2011<br />
NIHB File Date: 7/5/2011 (filed<br />
by ANHTC)<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10398 Issue Date: 7/1/2011<br />
Due Date: 8/30/2011<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-2348-P Issue Date: 7/12/2011<br />
Due Date: 9/12/2011<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Proposed<br />
Rule on home health payment<br />
rates 7/12/2011 (CMS-1353-P)<br />
CMS-2349-PF Issue Date: 8/12/2011<br />
Due Date: 10/31/2011<br />
NIHB File Date: 10/31/2011<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final<br />
Rule 3/23/2012 (see 28.b.)<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √ (Limited)<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: √<br />
(ANHTC recommendations)<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
None.<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
None.<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: To be<br />
completed.<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 4 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
28.b.<br />
34.<br />
40.<br />
41.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicaid Eligibility Under ACA<br />
ACTION: Interim Final Rule<br />
NOTICE: Medicaid; Eligibility<br />
Changes Under the ACA<br />
AGENCY: CMS<br />
Presumptive Eligibility<br />
ACTION:<br />
NOTICE:<br />
AGENCY: CMS<br />
State Plan Pages<br />
ACTION: Notice<br />
NOTICE: Medicaid State Plan Base<br />
Plan Pages<br />
AGENCY: CMS<br />
New Safe Harbors<br />
ACTION: Notice of Intent to<br />
Develop Regulations<br />
NOTICE: Solicitation of New Safe<br />
Harbors and Special Fraud Alerts<br />
AGENCY: HHS OIG<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-2349-IF Issue Date: 3/23/2012<br />
Due Date: 5:00 pm, 5/7/2012<br />
NIHB File Date: 5/7/2012<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-[TBD] Issue Date: [TBD]<br />
Due Date: [TBD]<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-179 Issue Date: 12/29/2011<br />
Due Date: 2/14/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
OIG–120–N Issue Date: 12/29/2011<br />
Due Date: 5:00 pm, 2/27/2012<br />
NIHB File Date: 2/27/2012<br />
Date of Subsequent Agency<br />
Action, if any: None as of<br />
5/15/2012<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: [To be<br />
entered.]<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: None.<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: [To be<br />
entered.]<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: To<br />
be entered.<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
[To be entered.]<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 5 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
43.<br />
44.<br />
46.<br />
61.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicaid Reimbursement for<br />
Outpatient Drugs<br />
ACTION: Proposed Rule<br />
NOTICE: Medicaid Program;<br />
Covered Outpatient Drugs<br />
AGENCY: CMS<br />
Medicaid Payment for Primary<br />
Care Services<br />
ACTION: Proposed Final Rule<br />
NOTICE: Payment for Primary<br />
Care Services under Medicaid<br />
Program<br />
AGENCY: CMS<br />
Medicaid DSH and Definition of<br />
Uninsured<br />
ACTION: Proposed Rule<br />
NOTICE: Medicaid Program;<br />
Disproportionate Share Hospital<br />
Payments--Uninsured Definition<br />
AGENCY: CMS<br />
Medicaid State Disallowance<br />
ACTION: Final Rule<br />
NOTICE: Medicaid and Children’s<br />
<strong>Health</strong> Insurance Programs;<br />
Disallowance of Claims for FFP and<br />
Technical Corrections<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-2345-P Issue Date: 2/2/2012<br />
Due Date: 5:00 pm, 4/2/2012<br />
NIHB File Date: 4/2/2012<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-2370-PF Issue Date: 5/11/2012<br />
Due Date: 5:00 pm, 6/11/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
11/6/2012<br />
CMS-2315-P<br />
Issue Date: 1/18/2012<br />
Due Date: 5:00 pm, 2/17/2012<br />
NIHB File Date: 2/17/2012<br />
Date of Subsequent Agency<br />
Action, if any: None as of<br />
4/30/2012<br />
CMS-2292-F Issue Date: 5/29/2012<br />
Due Date: None<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: √<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: √<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 6 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
62.<br />
65.<br />
66.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicaid State Disallowance<br />
ACTION: Request for Comment<br />
NOTICE: External Quality<br />
Review Protocols<br />
AGENCY: CMS<br />
<strong>Health</strong> Care Reform Insurance<br />
Web Portal Requirements<br />
ACTION: Request for comment<br />
NOTICE: <strong>Health</strong> Care Reform<br />
Insurance Web Portal<br />
Requirements<br />
AGENCY: CMS<br />
Requirements for Charitable<br />
Hospitals<br />
ACTION: Proposed Rule<br />
NOTICE: Additional Requirements<br />
for Charitable Hospitals<br />
AGENCY: IRS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-R-305 Issue Date: 5/31/2012<br />
Due Date: 7/2/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10320 Issue Date: 8/15/2012<br />
Due Date: 9/13/2012<br />
NIHB (TTAG and ANTHC) File<br />
Date: 9/13/2012<br />
Date of Subsequent Agency<br />
Action, if any:<br />
IRS-130266-11 Issue Date: 6/26/2012<br />
Due Date: 9/24/2012<br />
NIHB File Date: 9/24/2012<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: [To be<br />
entered.]<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
TTAG and ANTHC recommendations<br />
included: [To be entered.]<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
TTAG / NIHB recommendations<br />
included: [To be entered.]<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 7 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
83.<br />
84.<br />
85.<br />
86.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicaid Statistical Information<br />
System<br />
ACTION: Request for Comment<br />
NOTICE: Medicaid Statistical<br />
Information System<br />
AGENCY: CMS<br />
Monthly State File of Dual<br />
Eligible Enrollees<br />
ACTION: Request for Comment<br />
NOTICE: Monthly State File of<br />
Medicaid/Medicare Dual Eligible<br />
Enrollees<br />
AGENCY: CMS<br />
Medicaid Incentives for<br />
Prevention of Chronic Diseases<br />
ACTION: Request for Comment<br />
NOTICE: Minimum Data Set for<br />
MIPCD Program Grantees<br />
AGENCY: CMS<br />
Community <strong>Health</strong> Accreditation<br />
Program for Hospices<br />
ACTION: Final Notice<br />
NOTICE: Medicare and Medicaid<br />
CHAP for Continued Deeming<br />
Authority for Hospices<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-R-284 Issue Date: 8/15/2012<br />
Due Date: 10/15 11/19/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Action, if any:<br />
Issued extension without change<br />
10/19/2012<br />
CMS-10143 Issue Date: 9/17/2012<br />
Due Date: 11/16/2012<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10444 Issue Date: 10/19/2012<br />
Due Date: 11/19/2012<br />
NIHB File Date: Under review<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-3266-FN Issue Date: 10/19/2012<br />
Due Date: None<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: To be entered.<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 8 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
87.<br />
2.a.<br />
2.b.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicare and Medicaid Quarterly<br />
Listing of Program Issuances<br />
ACTION: Notice<br />
NOTICE: Medicare and Medicaid<br />
Quarterly Listing of Issuances—<br />
July through September 2012<br />
AGENCY: CMS<br />
I/T/U Addendum to Medicare<br />
Prescription Drug Plans (PDP):<br />
Revision of Current Collection<br />
ACTION: Information Collection<br />
NOTICE: Agency Information<br />
Collection Activities: Proposed<br />
Collection; Comment Request<br />
AGENCY: CMS<br />
I/T/U Addendum to Medicare<br />
Prescription Drug Plans (PDP)<br />
ACTION: Information Collection<br />
NOTICE: Information Collection<br />
Activities: Comment Request<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-9075-N<br />
CMS-10137<br />
and CMS-<br />
10237<br />
CMS-10137<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 11/9/2012<br />
Due Date: None<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
SECTION II: MEDICARE<br />
Issue Date: 6/11/2010<br />
Due Date: 8/10/2010<br />
NIHB File Date: 8/10/2010<br />
Date of Subsequent Agency Action,<br />
if any: Issued revised “Medicare<br />
PDP Sponsor contracts with<br />
Revised I/T/U Addendum” pre-<br />
1/13/2011<br />
Additional: Issued revised 2013<br />
contracts 7/1/2011 (see 2.b.)<br />
Issue Date: 7/1/2011<br />
Due Date: 8/30/2011<br />
NIHB File Date: 8/30/2011<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: To be entered.<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
From Review of 2011 Docs<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: √<br />
NIHB recommendations included: √<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 9 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
2.c.<br />
2.d.<br />
3.a.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicare Advantage and PDP<br />
Data Requirements<br />
ACTION: Request for Comment<br />
NOTICE: Application for New and<br />
Expanding Medicare Prescription<br />
Drug Plans and Medicare<br />
Advantage Prescription Drug (MA-<br />
PD) Plans, including Cost Plans<br />
and Employer Group Waiver Plans<br />
AGENCY: CMS<br />
Medicare Advantage and PDP<br />
Plan Applications<br />
ACTION: Request for Comment<br />
NOTICE: Part C Medicare<br />
Advantage and 1876 Cost Plan<br />
Expansion Application<br />
AGENCY: CMS<br />
Medicare Part B Rates<br />
ACTION: Final Rule<br />
NOTICE: Medicare Program;<br />
Payment Policies Under the<br />
Physician Fee Schedule and Other<br />
Revisions to Part B for CY 2011<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-10137 Issue Date: 7/6/2012<br />
Due Date: 9/4/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10237<br />
and CMS-<br />
10137<br />
CMS-2010-<br />
0205-0002<br />
Issue Date: 10/12/2012<br />
Due Date: 11/13/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 7/13/2010<br />
Due Date: 8/24/2010<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
11/29/2010<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action: [To be<br />
entered.]<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 10 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
3.b.<br />
3.c.<br />
4.a.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
DME Competitive Bidding<br />
ACTION: Request for Comment<br />
NOTICE: Durable Medical<br />
Equipment, Prosthetics, Orthotics,<br />
and Supplies (DMEPOS)<br />
Competitive Bidding Program<br />
AGENCY: CMS<br />
Durable Medical Equipment<br />
Certificate of Medical Necessity<br />
ACTION: Request for Comment<br />
NOTICE: DME Medicare<br />
Administrative Contractor CMN and<br />
Supporting Documentation<br />
Requirements<br />
AGENCY: CMS<br />
Medicare Outpatient Rates<br />
ACTION: Final Rule<br />
NOTICE: Medicare Program:<br />
Proposed changes to the Hospital<br />
Outpatient Prospective Payment<br />
System and CY 2011 Rates, etc.<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-10169<br />
CMS-846-849,<br />
10125, and<br />
10126<br />
CMS-2010-<br />
0205-0002<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 7/27/2012<br />
Due Date: 8/27/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 9/24/2012<br />
Due Date: 11/23/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 8/3/2010<br />
Due Date: 8/31/2010<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
11/24/2010<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 11 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
4.b.<br />
5.<br />
10.a.<br />
10.b.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicare Outpatient Rates<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicare Program:<br />
Revisions to hospital outpatient<br />
prospective and ambulatory<br />
surgical center payment systems;<br />
CY 2013 rates, etc.<br />
AGENCY: CMS<br />
PACE Information Request<br />
ACTION: Request for Comment<br />
NOTICE: Medicare and Medicaid;<br />
Programs of All-Inclusive Care for<br />
the Elderly (PACE)<br />
AGENCY: CMS<br />
ACO Standards<br />
ACTION: Request for Comment<br />
NOTICE: Medicare; Request for<br />
Info. Regarding Accountable Care<br />
Organizations (ACOs) and<br />
Medicare Shared Saving Program<br />
AGENCY: CMS<br />
ACO Standards<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicare Program;<br />
Shared Savings Program: ACOs<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-1589-<br />
PFC<br />
CMS-2010-<br />
0222-0001<br />
CMS-R-244<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 7/30/2012<br />
Due Date: 9/4/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
11/15/2012 (scheduled)<br />
Due Date for Final Rule<br />
Comments: 60 days (approx..<br />
1/12/2013)<br />
Issue Date: 7/30/2010<br />
Due Date: 9/28/2010<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-1345-NC Issue Date: 11/17/2011<br />
Due Date: 12/3/2011<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: 3/31/2011 (see<br />
10.b.)<br />
CMS-1345-P F Issue Date: 3/31/2011<br />
Due Date: 5:00 pm, 6/6/2011<br />
NIHB File Date: 6/6/2011<br />
Date of Subsequent Agency<br />
Action, if any: 11/2/2011<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action: See 10.b<br />
below.<br />
Analysis of Agency action:<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: √<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 12 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
11.a.<br />
11.b.<br />
11.c.<br />
11.d.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Revisions to PDP Requirements<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicare Program;<br />
Proposed Changes to MA and the<br />
Medicare PDP for Contract Year<br />
2012 and Other Proposed Changes<br />
AGENCY: CMS<br />
Medicare Advantage and PDP<br />
ACTION: Final Rule<br />
NOTICE: Policy and Technical<br />
Changes to Medicaid Advantage<br />
and PDP for CY 2013<br />
AGENCY: CMS<br />
Quality in Medicare Advantage<br />
and Special Needs Plans<br />
ACTION: Request for Comment<br />
NOTICE: Evaluation and<br />
Development of Outcome<br />
Measures for Quality Assessment<br />
in MA Plans and SNPs<br />
AGENCY: CMS<br />
Bid Pricing Tool<br />
ACTION: Request for Comment<br />
NOTICE: BPT for Medicare<br />
Advantage and Prescription Drug<br />
Plans<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-4144-F<br />
CMS-4157-F<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 11/22/2010<br />
Due Date: 1/11/2011 (changed<br />
from 1/22/2011)<br />
NIHB File Date: 1/11/2011<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
4/15/2011<br />
Issue Date: 4/12/2012<br />
Due Date: None<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10451 Issue Date: 10/26/2012<br />
Due Date: 12/26/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10142<br />
Issue Date: 10/5/2012<br />
Due Date: 12/4/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: √<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 13 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
11.e.<br />
11.f.<br />
11.g.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicare Advantage Quality<br />
Bonus Payment Demonstration<br />
ACTION: Request for Comment<br />
NOTICE: Medicare Advantage<br />
Quality Bonus Payment<br />
Demonstration<br />
AGENCY: CMS<br />
Plan Benefit Package and<br />
Formulary Submission<br />
ACTION: Request for Comment<br />
NOTICE: PBP and Formulary<br />
Submission for Medicare<br />
Advantage and Prescription Drug<br />
Plans<br />
AGENCY: CMS<br />
Medicare Advantage Reporting<br />
Requirements<br />
ACTION: Request for Comment<br />
NOTICE: Part C Medicare<br />
Advantage Reporting Requirements<br />
and Supporting Regulations in 42<br />
CFR 422.516(a)<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-10445<br />
CMS-R-262<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 9/17/2012<br />
Due Date: 11/16/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 10/5/2012<br />
Due Date: 12/4/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10261 Issue Date: 10/26/2012<br />
Due Date: 12/26/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: To be entered.<br />
NIHB analysis of<br />
action: To be entered.<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
TTAG / NIHB recommendations<br />
included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 14 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
18.<br />
19.<br />
21.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
eRx Incentive Program<br />
ACTION: Proposed Rule<br />
NOTICE: Medicare Program;<br />
Proposed Change to the Electronic<br />
Prescribing Incentive Program<br />
AGENCY: CMS<br />
Value-Based Purchasing<br />
ACTION: Final Rule<br />
NOTICE: Medicare Program;<br />
Hospital Inpatient Value-Based<br />
Purchasing<br />
AGENCY: CMS<br />
Medicare Outpatient Rates and<br />
Other Provider-Related Issues<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicare and Medicaid:<br />
Hospital Outpatient Prospective<br />
Payment; Ambulatory Surgical<br />
Center; Hospital Value-Based<br />
Purchasing Program, etc.<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-3248-P<br />
CMS-3239-F<br />
CMS-1525-<br />
PFC<br />
RIN 0938-<br />
AQ26<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 6/1/2011<br />
Due Date: 7/25/2011<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 5/6/2011<br />
Due Date: None<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 7/1/2011<br />
Due Date: 8/30/2011<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: 11/1/2011; issued<br />
correction 4/24/2012<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: No<br />
comments/recommendations made.<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
None.<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 15 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
22.<br />
24.<br />
25.a.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicare Physician Rates<br />
ACTION: Proposed Rule<br />
NOTICE: Medicare Program;<br />
Payment Policies Under the<br />
Physician Fee Schedule and Other<br />
Revisions to Part B for CY 2012<br />
AGENCY: CMS<br />
Transportation Barriers Study<br />
under Medicare for AI/AN<br />
ACTION: Information Request<br />
NOTICE: Analysis of Transportation<br />
Barriers to Utilization of Medicare<br />
Services by AI/AN Medicare Bene’s<br />
AGENCY: CMS<br />
Medicare Inpatient Rates<br />
ACTION: Proposed Rule<br />
NOTICE: Medicare; Hospital<br />
Inpatient PPPS for Acute Care<br />
Hospitals and the LTC Hospital<br />
PPS and Fiscal Year 2011 Rates<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-1524-P<br />
RIN 0938-<br />
AQ25<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 7/1/2011<br />
Due Date: 8/30/2011<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10399 Issue Date: 7/1/2011<br />
Due Date: 8/30/2011<br />
NIHB File Date: 8/30/2011<br />
Date of Subsequent Agency<br />
Action, if any: Issued Notice<br />
12/14/2011; issued Notice<br />
4/18/2012<br />
CMS-1518-P<br />
Issue Date: 4/19/2011<br />
Due Date: 6/20/2011<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: Partial.<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
None<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: √<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
None.<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 16 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
25.b.<br />
32.<br />
49.a.<br />
49.b.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicare Inpatient Rates<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicare; Hospital<br />
Inpatient and LTC PPS and FY<br />
2013 Rates; Hospital GME<br />
Payments; Quality Reporting<br />
Requirements for ACS and others<br />
AGENCY: CMS<br />
Bundled Payments<br />
ACTION: Request for<br />
Applications<br />
NOTICE: Bundled Payments for<br />
Care Improvement Initiatives<br />
AGENCY: CMS<br />
Reporting and Returns of<br />
Medicare Overpayments<br />
ACTION: Proposed Rule<br />
NOTICE: Medicare; Reporting and<br />
Returning of Overpayments<br />
AGENCY: CMS<br />
Medicare Credit Balance<br />
Reporting Requirements<br />
ACTION: Request for Comment<br />
NOTICE: Medicare Credit Balance<br />
Reporting Requirements and<br />
Supporting Regulations<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-1588-PF<br />
CMS-1588-<br />
CN2 & CN3<br />
CMS-1588-F2<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 4/24/2012<br />
Due Date: 5:00 pm, 6/25/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
8/31/2012; issued correction<br />
10/17/2012 and 10/29/2012<br />
CMS-5504-N Issue Date: 8/25/2011<br />
Due Date: 10/06/2011 and<br />
11/18/2011<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-6037-P Issue Date: 2/16/2012<br />
Due Date: 5:00 pm, 4/16/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-838<br />
Issue Date: 9/17/2010<br />
Due Date: 11/16/2010<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of<br />
Subsequent Agency<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 17 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
52.a.<br />
52.b.<br />
52.c.<br />
57.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicare Home <strong>Health</strong> Access<br />
ACTION: Information Request<br />
NOTICE: Surveys of Physicians<br />
and Home <strong>Health</strong> Agencies to<br />
Assess Access Issues for Specific<br />
Med. Beneficiaries in ACA §3131(d)<br />
AGENCY: CMS<br />
Medicare Home <strong>Health</strong> Payments<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicare; Revisions to<br />
Home <strong>Health</strong> Prospective Payment<br />
System Rate Update for CY 2013,<br />
Hospice Quality Reporting<br />
Requirements, etc.<br />
AGENCY: CMS<br />
Medicare Hospice Wage Index<br />
ACTION: Notice<br />
NOTICE: Medicare Program;<br />
Hospice Wage Index for FY 2013<br />
AGENCY: CMS<br />
Durable Medical Equipment<br />
ACTION: Request for Comment<br />
NOTICE: Durable Medical<br />
Equipment, Prosthetics, Orthotics,<br />
and Supplies Competitive Bidding<br />
Program<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-10429<br />
and CMS-<br />
10185<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 4/18/2012<br />
Due Date: 6/18/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-1358-PF Issue Date: 7/13/2012<br />
Due Date: 9/4/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
11/8/2012<br />
CMS-1434-N Issue Date: 7/27/2012<br />
Due Date: 9/4/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10169 Issue Date: 5/7/2012; 7/27/2012<br />
(revised)<br />
Due Date: 7/6/2012; 8/27/2012<br />
(revised)<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 18 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
58.<br />
59.<br />
60.a.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicare Hospital Conditions of<br />
Participation<br />
ACTION: Final Rule<br />
NOTICE: Medicare and Medicaid<br />
Programs; Reform of Hospital and<br />
Critical Access Hospital Conditions<br />
of Participation<br />
AGENCY: CMS<br />
Medicare Provisions to Promote<br />
Efficiency<br />
ACTION: Final Rule<br />
NOTICE: Medicare and Medicaid<br />
Provisions to Promote Program<br />
Efficiency, Transparency and<br />
Burden Reduction<br />
AGENCY: CMS<br />
<strong>Health</strong> Insurance Common<br />
Claims Form--phase-out<br />
ACTION: Comment Request<br />
NOTICE: Agency Information<br />
Collection Activities: Proposed<br />
Collection; Comment Request<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-3244-F Issue Date: 5/16/2012<br />
Due Date: None<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-9070-F Issue Date: 5/16/2012<br />
Due Date: None.<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-1500<br />
(version 08/05)<br />
and CMS-<br />
1490S<br />
Issue Date: 5/29/2012<br />
Due Date: 7/30/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 19 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
60.b.<br />
60.c.<br />
60.d.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
<strong>Health</strong> Insurance Common<br />
Claims Form--phase-in<br />
ACTION: Comment Request<br />
NOTICE: Agency Information<br />
Collection Activities: Proposed<br />
Collection; Comment Request<br />
AGENCY: CMS<br />
<strong>Health</strong> Insurance Common<br />
Claims Form<br />
ACTION: Request for Comment<br />
NOTICE: <strong>Health</strong> Insurance<br />
Common Claims Form and<br />
Supporting Regulations at 42 CFR<br />
Part 424, Subpart C<br />
AGENCY: CMS<br />
Medicare Electronic Data<br />
Interchange Form<br />
ACTION: Request for Comment<br />
NOTICE: Medicare EDI<br />
Registration and Enrollment Form<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-1500<br />
(version 2/12)<br />
CMS-1500<br />
(02/12) and<br />
CMS-1500<br />
(08/05)<br />
CMS-10164<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 5/29/2012<br />
Due Date: 7/30/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 9/21/2012<br />
Due Date: 10/22/2012<br />
NIHB File Date: None.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 9/17/2012<br />
Due Date: 11/16/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action: 49<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 20 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
70.a.<br />
70.b.<br />
71.a.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicare PFS Rule<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicare: Revisions to<br />
payment policies under physician<br />
fee schedule, DME, face-to-face<br />
encounters, etc.<br />
AGENCY: CMS<br />
Medicare Fee-for-Service<br />
Prepayment Medical Review<br />
ACTION: Request for Comment<br />
NOTICE: Medicare Fee-for-Service<br />
Prepayment Medical Review<br />
AGENCY: CMS<br />
Medicare PFS Rule<br />
ACTION: Proposed Final Rule<br />
NOTICE: Medicare Program; End-<br />
Stage Renal Disease Prospective<br />
Payment System, Quality Incentive<br />
Program, and Bad Debt Reductions<br />
for All Medicare Providers<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-1590-<br />
PFC<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 7/30/2012<br />
Due Date: 9/4/2012<br />
NIHB File Date: None<br />
ANTHC File Date: 9/4/2012<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
11/16/2012 (scheduled)<br />
Due Date for Final Rule<br />
Comments: 60 days (approx..<br />
1/13/2013)<br />
CMS-10417 Issue Date: 9/21/2012<br />
Due Date: 10/22/2012<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-1352-PF<br />
Issue Date: 7/11/2012<br />
Due Date: 5:00 pm, 8/31/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
11/9/2012<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
ANTHC analysis of<br />
action: To be entered.<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
ANTHC recommendations included:<br />
To be entered.<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 21 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
71.b.<br />
72.<br />
73.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medicare Beneficiaries with End-<br />
Stage Renal Disease<br />
ACTION: Request for Comment<br />
NOTICE: Evaluation of Patient<br />
Satisfaction and Experience of<br />
Care for Medicare Beneficiaries<br />
with ESRD<br />
AGENCY: CMS<br />
Medicare Skilled Nursing Facility<br />
Payments<br />
ACTION: Notice<br />
NOTICE: Medicare: Prospective<br />
Payment System and Consolidated<br />
Billing for Skilled Nursing Facilities<br />
for FY 2013<br />
AGENCY: CMS<br />
Medicare Inpatient Psychiatric<br />
Rates<br />
ACTION: Notice<br />
NOTICE: Medicare: Inpatient<br />
Psychiatric Facilities Prospective<br />
Payment System--Update for Fiscal<br />
Year Beginning October 1, 2012<br />
(FY 2013)<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-10425<br />
CMS-1432-N<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 9/21/2012<br />
Due Date: 10/22/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 8/2/2012<br />
Due Date: None<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-1440-N Issue Date: 8/7/2012<br />
Due Date: None<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 22 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
78.<br />
80.<br />
81.<br />
6.a.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Hospice Services<br />
ACTION: Final Rule<br />
NOTICE: Requirements for Longterm<br />
Care Facilities: Hospice<br />
Services<br />
AGENCY: CMS<br />
Notice of Denial of Medical<br />
Coverage (or Payment)<br />
ACTION: Request for comment<br />
NOTICE: Notice of Denial of<br />
Medical Coverage (or Payment)<br />
AGENCY: CMS, HHS<br />
Efficiency, Transparency, and<br />
Burden Reduction<br />
ACTION: Proposed Rule<br />
NOTICE: Part II--Regulatory<br />
Provisions to Promote Program<br />
Efficiency, Transparency, and<br />
Burden Reduction<br />
AGENCY: CMS, HHS<br />
High-Risk Pool Eligibility<br />
ACTION: Interim Final Rule<br />
NOTICE: Pre-Existing Condition<br />
Insurance Plan Program<br />
AGENCY: OCIIO<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-3140-F Issue Date: [Pending at OMB as<br />
of 9/14/2012]<br />
Due Date:<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10003 Issue Date: 9/7/2012<br />
Due Date: 11/6/2012<br />
TTAG / NIHB File Date:<br />
11/6/2012<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-1367-P Issue Date:<br />
[Pending at OMB since<br />
8/2/2012]<br />
Due Date:<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
OCIIO-9995-<br />
IFC<br />
Section III: <strong>Health</strong> Reform<br />
Issue Date: 7/30/2010<br />
Due Date: 9/28/2010<br />
NIHB File Date: 9/28/2010<br />
Date of Subsequent Agency<br />
Action, if any: None as of<br />
4/15/2012<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
TTAG / NIHB analysis<br />
of action: [To be<br />
entered.]<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
TTAG / NIHB recommendations<br />
included: [To be entered.]<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: √<br />
Subsequent Agency action: none<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 23 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
6.b.<br />
6.c.<br />
7.a.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Pre-Existing Condition Insurance<br />
Plan Program<br />
ACTION: Interim Final Rule<br />
NOTICE: Pre-Existing Condition<br />
Insurance Plan Program<br />
AGENCY: CMS<br />
Pre-Existing Condition Insurance<br />
Plan Authorization<br />
ACTION: Request for Comment<br />
NOTICE: : PCIP Authorization to<br />
Share Personal <strong>Health</strong> Information<br />
AGENCY: CMS<br />
ACA Exchange Rules<br />
ACTION: Request for Comment<br />
NOTICE: Planning and<br />
Establishment of State-Level<br />
Exchanges; RfC Exchange-Related<br />
Provisions in Title I of the ACA<br />
AGENCY: OCIIO<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-9995-<br />
IFC2<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 8/30/2012<br />
Due Date: 10/29/2012<br />
NIHB File Date: None.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10428 Issue Date: 9/21/2012<br />
Due Date: 10/22/2012<br />
NIHB File Date: None.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CIIO-9989-NC<br />
HHS-0S-2010-<br />
0021-0001<br />
Issue Date: 8/3/2010<br />
Due Date: 10/4/2010<br />
NIHB File Date: 10/4/2010<br />
Date of Subsequent Agency<br />
Action, if any: 7/15/2011 (see<br />
7.b.)<br />
Additional: Issued Tribal<br />
Sponsorship and <strong>Indian</strong><br />
Addendum 4/13/11<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
(Partial previously √)<br />
Analysis of Agency action: √<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 24 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
7.b.<br />
7.c.<br />
7.d.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Establishment of Exchange/QHP<br />
ACTION: Proposed Final/Interim<br />
Final Rule<br />
NOTICE: Establishment of<br />
Exchanges/ Qualified <strong>Health</strong> Plans,<br />
Part 1<br />
AGENCY: HHS<br />
Exchange: Eligibility<br />
Determinations<br />
ACTION: Proposed Final Rule<br />
NOTICE: Exchange Functions:<br />
Eligibility Determinations; Employer<br />
Standards<br />
AGENCY: HHS<br />
Definition of <strong>Indian</strong>, Supplement<br />
to CMS-9989, 9974, 2349, and IRS<br />
REG-131491<br />
ACTION: Proposed Rule<br />
NOTICE: Cross-reg. response<br />
AGENCY: HHS and Treasury<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-9989-PF<br />
(with item 7.c.:<br />
CMS-9974-F)<br />
CMS-9974-PF<br />
(see item 7.b:<br />
CMS-9989-F)<br />
CMS-9989-P,<br />
CMS-9974-P,<br />
CMS-2349-P,<br />
and IRS REG-<br />
131491 (see<br />
7.b. and c.)<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 7/15/2011<br />
Due Date: 10/31/2011<br />
NIHB File Date: 10/31/2011<br />
Date of Subsequent Agency<br />
Action, if any: 3/27/2012; issued<br />
correction 5/29/2012<br />
Due Date for Interim Final Rule<br />
Comments: 5:00 pm, 5/11/2012<br />
Issue Date: 8/12/2011<br />
Due Date: 10/31/2011<br />
NIHB File Date: 10/31/2011<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
3/27/2012<br />
Issue Date: 8/12/2011<br />
Due Date: 10/31/2011<br />
NIHB File Date: 10/31/2011<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
3/27/2012<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of<br />
subsequent Agency<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: √<br />
NIHB IF recommendations included:<br />
None filed.<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: √<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √ (partial)<br />
Analysis of Agency action: Entered,<br />
in part.<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 25 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
7.e.<br />
7.f.<br />
7.g.<br />
12.a.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Exchange: Cooperative<br />
Agreements<br />
ACTION: Request for comment<br />
NOTICE: Cooperative Agreement<br />
to Support Establishment of the<br />
Affordable Care Act’s <strong>Health</strong><br />
Insurance Exchanges<br />
AGENCY: HHS<br />
Exchange: Blueprint Application<br />
ACTION: Request for comment<br />
NOTICE: Cooperative Agreement<br />
to Support Establishment of the<br />
Affordable Care Act’s <strong>Health</strong><br />
Insurance Exchanges<br />
AGENCY: HHS<br />
Exchange: General Guidelines<br />
ACTION: Request for comment<br />
NOTICE: General Guidance on<br />
Federally-Facilitated Exchanges<br />
AGENCY: HHS<br />
Co-Op Plans (Sec. 1322 of ACA)<br />
ACTION: Request for comment<br />
NOTICE: Planning and<br />
Establishment of Consumer<br />
Operated and Oriented Plan<br />
Program<br />
AGENCY: OCIIO, HHS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-10424<br />
CMS-10415<br />
CMS (no<br />
reference<br />
number)<br />
OCIIO-9983-<br />
NC<br />
RIN 0950-<br />
AA19<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 5/18/2012<br />
Due Date: 6/18/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 11/10/2011<br />
Due Date: 1/10/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 5/16/2012<br />
Due Date:<br />
NIHB File Date: 6/18/2012<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 2/2/2011<br />
Due Date: 3/4/11<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: See 12.b.<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: To be entered.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: To<br />
be entered.<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: No<br />
recommendations submitted (NIHB<br />
issued paper prepared 4/12/11).<br />
Subsequent Agency action: √<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 26 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
12.b.<br />
14.<br />
15.<br />
27.a<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Co-Op Plans (Sec. 1322 of ACA)<br />
ACTION: Proposed Final Rule<br />
NOTICE: Establishment of<br />
Consumer Operated and Oriented<br />
Plan (CO-OP) Program<br />
AGENCY: OCIIO, HHS<br />
ACA Waivers for State<br />
Innovation<br />
ACTION: Proposed Final Rule<br />
NOTICE: Application, Review, and<br />
Reporting Process for Waives for<br />
State Innovation Under Sec. 1332<br />
AGENCY: CMS/Treasury<br />
Delegation of Authority to CMS<br />
ACTION: Notice / Effective<br />
Immediately<br />
NOTICE: Office of the Secretary:<br />
Delegation of Authority; CMS<br />
AGENCY: HHS<br />
Risk Adjustment Standards in<br />
ACA<br />
ACTION: Proposed Final Rule<br />
NOTICE: ACA; Standards Related<br />
to Reinsurance, Risk Corridors and<br />
Risk Adjustment<br />
AGENCY: HHS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
OCIIO-9983-P<br />
F<br />
CMS-9987-PF<br />
RIN 0938-<br />
AQ75<br />
FR 13553-01<br />
76 FR 13618<br />
DOCID:<br />
fr14mr11-74<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 7/20/2011<br />
Due Date: 5:00pm, 9/16/2011<br />
NIHB File Date: 9/16/2011<br />
Date of Subsequent Agency<br />
Action, if any: 12/13/2011<br />
Issue Date: 3/14/2011<br />
Due Date: 5/13/2011<br />
NIHB File Date: 5/13/2011<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
2/27/2012<br />
Issue Date: 3/14/2011<br />
Due Date: None<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-9975-PF Issue Date: 7/15/2011<br />
Due Date: 10/31/2011 (revised)<br />
NIHB File Date: 9/27/2011<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
3/23/2012; issued correction<br />
5/17/2012<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: No response<br />
provided.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of<br />
Subsequent Agency<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: √<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: To be<br />
entered.<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: √<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 27 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
29.<br />
31.a.<br />
31.b.<br />
31.c.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Premium Subsidies and Tax<br />
Credits<br />
ACTION: Proposed Final Rule<br />
NOTICE: <strong>Health</strong> Insurance<br />
Premium Tax Credit<br />
AGENCY: IRS, Treasury<br />
Essential <strong>Health</strong> Benefits Bulletin<br />
ACTION: Request for comment<br />
NOTICE: Essential <strong>Health</strong> Benefits,<br />
HHS Informational Bulletin<br />
AGENCY: HHS<br />
Preventive <strong>Health</strong> Services<br />
ACTION: Interim Final Rule<br />
NOTICE: Group <strong>Health</strong> Plans and<br />
<strong>Health</strong> Insurance Issuers Relating<br />
to Coverage of Preventive Services<br />
AGENCY: HHS/IRS/DoL<br />
Certain Preventive Services<br />
ACTION: Advanced Notice of<br />
Proposed Rule Making<br />
NOTICE: Certain Preventive <strong>Health</strong><br />
Services under the ACA<br />
AGENCY: HHS/ IRS/DoL<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
IRS REG-<br />
131491<br />
No reference<br />
number<br />
CMS-9992-<br />
IFC2<br />
CMS-9968-<br />
ANPRM<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 8/12/2011<br />
Due Date: 10/31/2011<br />
NIHB File Date: 10/31/2011<br />
Date of Subsequent Agency<br />
Action, if any: 5/23/2012<br />
Issue Date: 12/16/2011<br />
Due Date: 1/31/2012<br />
NIHB File Date: 1/31/2012<br />
Date of Subsequent Agency<br />
Action, if any: CMS issued FAQ<br />
on EHB 2/17/2012<br />
Issue Date: 7/19/2010; 8/3/2011<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Bulletin<br />
2/10/2012<br />
Issue Date: 3/21/2012<br />
Due Date: 6/19/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √<br />
Analysis of Agency action: To be<br />
prepared and entered.<br />
NIHB recommendations included: √<br />
Subsequent Agency action: √ (partial)<br />
Analysis of Agency action: To be<br />
entered.<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 28 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
31.d.<br />
33.<br />
37.<br />
38.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Standards Related to Essential<br />
<strong>Health</strong> Benefits<br />
ACTION: Proposed Rule<br />
NOTICE: Exchanges Part II—<br />
Standards Related to Essential<br />
<strong>Health</strong> Benefits; <strong>Health</strong> Insurance<br />
Issuer and Exchange<br />
Responsibilities<br />
AGENCY: CMS<br />
Citizenship Documentation<br />
ACTION:<br />
NOTICE:<br />
AGENCY: CMS<br />
Performance Metrics for<br />
Medicaid and Exchange<br />
Eligibility & Enrollment<br />
ACTION:<br />
NOTICE:<br />
AGENCY: CMS<br />
Appeals<br />
ACTION:<br />
NOTICE:<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-9980-P<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: [Pending at OMB as<br />
of 11/8/2012]<br />
Due Date:<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-[TBD] Issue Date: [TBD]<br />
Due Date: [TBD]<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-[TBD] Issue Date: [TBD]<br />
Due Date: [TBD]<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-[TBD] Issue Date: [TBD]<br />
Due Date: [TBD]<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 29 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
39.<br />
42.<br />
45.<br />
47.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Basic <strong>Health</strong> Program<br />
ACTION: Request for Information<br />
NOTICE: State Flexibility to<br />
Establish a Basic <strong>Health</strong> Program<br />
under the ACA<br />
AGENCY: CMS<br />
Employer Minimum Value<br />
Standard<br />
ACTION:<br />
NOTICE:<br />
AGENCY: CMS/DoL<br />
Actuarial Value and Cost-Sharing<br />
ACTION: Pre-Rule Bulletin<br />
NOTICE: Draft Actuarial Value and<br />
Cost-Sharing Reductions Bulletin<br />
AGENCY: CMS<br />
HSA Eligibility and IHS<br />
Beneficiaries<br />
ACTION: Proposed Rule<br />
NOTICE: <strong>Health</strong> Savings Accounts<br />
Eligibility and IHS Beneficiaries<br />
AGENCY: Treasury/IHS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-9980-NC Issue Date: 9/14/2011<br />
Due Date: 5:00 pm, 10/31/2011<br />
NIHB File Date: 10/31/2011<br />
Date of Subsequent Agency<br />
Action, if any: None as of<br />
4/30/2012<br />
CMS<br />
RIN-0938-<br />
ZB08<br />
Notice 2012-14<br />
Issue Date: [TBD]<br />
Due Date: [TBD]<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: Post-2/24/2012<br />
Due Date: None<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 2/2012<br />
Due Date: 4/30/2012<br />
NIHB File Date: 4/30/2012<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: √<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: √<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 30 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
48.<br />
50.b.<br />
51.<br />
53.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Medical Loss Ratio<br />
Requirements<br />
ACTION: Final Rule<br />
NOTICE: Medical Loss Ratio<br />
Requirements under the Affordable<br />
Care Act--Notice Requirements<br />
AGENCY: CMS<br />
EHB and QHP Standards<br />
ACTION: Proposed Final Rule<br />
NOTICE: Data Collection to Support<br />
Standards Related to Essential<br />
<strong>Health</strong> Benefits; Recognition of<br />
Entities for the Accreditation of<br />
Qualified <strong>Health</strong> Plans<br />
AGENCY: CMS<br />
Student Insurance Coverage<br />
ACTION: Final Rule<br />
NOTICE: Student <strong>Health</strong> Insurance<br />
AGENCY: CMS<br />
Certificates of Exemption<br />
ACTION:<br />
NOTICE:<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-9998-F Issue Date: 5/16/2012<br />
Due Date: None<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued correction<br />
5/17/2012<br />
CMS-9965-PF Issue Date: 6/5/2012<br />
Due Date: 7/5/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued Final Rule<br />
7/20/2012<br />
CMS-9981-F Issue Date: 3/21/2012<br />
Due Date:<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Future<br />
issuance<br />
referenced in<br />
CMS-9989-F<br />
Action, if any:<br />
Issue Date: [TBD]<br />
Due Date:<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Subsequent Agency<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 31 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
54.<br />
56.<br />
63.<br />
64.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
ESI Coverage Verification<br />
ACTION: Notice<br />
NOTICE: Employer-Sponsored<br />
Coverage Verification: Preliminary<br />
Informational Statement<br />
AGENCY: CMS<br />
Stop-Loss Insurance<br />
ACTION: Request for Information<br />
NOTICE: Request for Information<br />
AGENCY: CMS/IRS/DoL<br />
<strong>Health</strong> Care EFT Standards<br />
ACTION: Interim Final Rule with<br />
Request for Comment<br />
NOTICE: Administrative<br />
Simplification: Adoption of<br />
Operating Rules for <strong>Health</strong> Care<br />
Electronic Funds Transfers (EFT)<br />
and Remittance Advice Trans.<br />
AGENCY: HHS<br />
Policy on Conferring with Urban<br />
<strong>Indian</strong> Organizations<br />
ACTION: Request for comment<br />
NOTICE: Draft Policy on Conferring<br />
With Urban <strong>Indian</strong> Organizations<br />
AGENCY: IHS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS<br />
RIN: 0938-<br />
ZB09<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: [OMB approved<br />
4/26/2012]<br />
Due Date:<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-9967-NC Issue Date: 5/1/2012<br />
Due Date: 7/2/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
HHS<br />
RIN 0938-<br />
AR01<br />
No reference<br />
number<br />
Action, if any:<br />
Issue Date: 8/10/2012<br />
Due Date: 10/9/2012<br />
NIHB File Date: None.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 7/16/2012<br />
Due Date: 9/10/2012<br />
NIHB File Date: None.<br />
Comments filed by NCUIH and<br />
ANTHC.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
ANTHC and NCUIH<br />
analysis of action: [To<br />
be entered.]<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included: [To<br />
be entered.]<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 32 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
65.<br />
67.<br />
68.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
<strong>Health</strong> Care Reform Insurance<br />
Web Portal Requirements<br />
ACTION: Request for comment<br />
NOTICE: <strong>Health</strong> Care Reform<br />
Insurance Web Portal<br />
Requirements<br />
AGENCY: CMS<br />
State Consumer Assistance<br />
Grants<br />
ACTION: Request for Information<br />
NOTICE: Revision of a currently<br />
approved collection; Consumer<br />
Assistance Program Grants<br />
AGENCY: CMS<br />
Security of Electronic <strong>Health</strong><br />
Information<br />
ACTION: Request for comment<br />
NOTICE: <strong>Health</strong> Insurance Reform:<br />
Electronic Security Standards<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-10320 Issue Date: 8/15/2012<br />
Due Date: 9/13/2012<br />
NIHB File Date: 9/13/2012<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10333 Issue Date: 7/27/2012<br />
Due Date: 9/25/2012<br />
NIHB File Date: None.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10149 Issue Date: 8/31/2012<br />
Due Date: 10/30/2012<br />
NIHB File Date: None.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: [To<br />
be entered.]<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 33 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
69.<br />
77.<br />
88.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Data Elements for Exchange<br />
Application<br />
ACTION: Request for Information<br />
NOTICE: Data Collection to<br />
Support Eligibility Determinations<br />
for Insurance Affordability<br />
Programs and Enrollment through<br />
Affordable Insurance Exchanges,<br />
Medicaid and Children’s <strong>Health</strong><br />
Insurance Program Agencies<br />
AGENCY: CMS<br />
Unique Plan Identifiers<br />
ACTION: Final Rule<br />
NOTICE: Adoption of a Standard<br />
for a Unique <strong>Health</strong> Plan Identifier;<br />
Addition to the <strong>National</strong> Provider<br />
Identifier Requirements; and a<br />
Change to the Compliance Date for<br />
the ICD-10 Medical Data Code Sets<br />
AGENCY: CMS<br />
Early Retiree Reinsurance<br />
Program Survey<br />
ACTION: Request for Comment<br />
NOTICE: Early Retiree<br />
Reinsurance Program Survey of<br />
Plan Sponsors<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
CMS-10440<br />
and CMS-<br />
10438<br />
CMS-0040-F<br />
CMS-0040-CN<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 7/6/2012<br />
Due Date: 9/4/2012<br />
NIHB File Date: 9/4/2012<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 9/5/2012<br />
Due Date: None<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any: Issued correction<br />
10/4/2012<br />
CMS-10408 Issue Date: 9/28/2012<br />
Due Date: 11/27/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: √<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included: √<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 34 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
89.<br />
90.<br />
91.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Notice of Benefit and Payment<br />
Parameters for 2014<br />
ACTION: Proposed Rule<br />
NOTICE: Patient Protection and<br />
Affordable Care Act Notice of<br />
Benefit and Payment Parameters<br />
for 2014<br />
AGENCY: CMS<br />
Adverse Benefit Determinations<br />
ACTION: Guidance<br />
NOTICE: Adverse Benefit<br />
Determinations and Final Internal<br />
Adverse Benefit Determinations for<br />
Beneficiaries in Non-Federal<br />
Governmental <strong>Health</strong> Plans<br />
AGENCY: CCIIO<br />
Waiting Period Limitation Under<br />
Public <strong>Health</strong> Service Act<br />
ACTION: Guidance<br />
NOTICE: Guidance on 90-Day<br />
Waiting Period Limitation under<br />
Public <strong>Health</strong> Service Act<br />
AGENCY: CCIIO<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-9964-P Issue Date: TBD<br />
Due Date:<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CCIIO (no<br />
reference<br />
number)<br />
CCIIO (no<br />
reference<br />
number)<br />
Issue Date: 8/17/2012<br />
Due Date: None<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 8/31/2012<br />
Due Date: 9/30/2012<br />
NIHB File Date: None.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 35 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
92.<br />
35.<br />
36.<br />
74.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
<strong>Health</strong> Insurance Market Rules<br />
ACTION: Proposed Rule<br />
NOTICE: Patient Protection and<br />
Affordable Care Act <strong>Health</strong><br />
Insurance Market Rules<br />
AGENCY: CMS<br />
Medical Child Support<br />
ACTION:<br />
NOTICE:<br />
AGENCY: CMS<br />
Transitional Medical Assistance<br />
ACTION:<br />
NOTICE:<br />
AGENCY: CMS<br />
Beat Down Blood Pressure<br />
Challenge<br />
ACTION: Notice<br />
NOTICE: Announcement of<br />
Requirements and Registration for<br />
Beat Down Blood Pressure<br />
Challenge<br />
AGENCY: ONC, HHS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
CMS-9972-P Issue Date: [Pending at OMB as<br />
of 11/8/2012]<br />
Due Date:<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Section IV: Other<br />
CMS-[TBD] Issue Date: [TBD]<br />
Due Date: [TBD]<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-[TBD] Issue Date: [TBD]<br />
Due Date: [TBD]<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
ONC (no Issue Date: 3/23/2012<br />
reference Due Date: None<br />
number) NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 36 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
75.<br />
76.<br />
82.<br />
93.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
<strong>Indian</strong> Tribal Government Plan<br />
ACTION: Request for comment<br />
NOTICE: Determination of<br />
Governmental Plan Status<br />
AGENCY: IRS<br />
Tribal Self-Governance Program<br />
ACTION: New-Limited<br />
Competition<br />
NOTICE: Funding Opportunity:<br />
Tribal Self-Governance Program;<br />
Planning Cooperative Agreement<br />
AGENCY: IHS<br />
HIPAA Rules<br />
ACTION: Final Rule<br />
NOTICE: Modifications to the<br />
HIPAA Privacy, Security,<br />
Enforcement, and Breach<br />
Notification Rules<br />
AGENCY: Office of Civil Rights,<br />
HHS<br />
New Freedom Initiative<br />
ACTION: Request for Comment<br />
NOTICE: New Freedom Initiative—<br />
Web-based Reporting System for<br />
Grantees<br />
AGENCY: CMS<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
IRS REG-<br />
133223-08<br />
HHS-2012-<br />
IHS-TSGP-<br />
0001<br />
HHS<br />
RIN 0945-<br />
AA03<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 3/8/2012<br />
Due Date: 6/2012<br />
NIHB File Date: None<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 8/8/2012<br />
Due Date: 9/9/2012<br />
NIHB File Date: None.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: [Pending at OMB<br />
since 3/24/2012]<br />
Due Date:<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
CMS-10161 Issue Date: 9/28/2012<br />
Due Date: 10/29/2012<br />
NIHB File Date: None.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action: √<br />
NIHB analysis of<br />
action: None.<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action: [To be<br />
entered.]<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 37 of 38 11/12/2012
RRIAR<br />
Ref.<br />
#<br />
94.<br />
95.<br />
96.<br />
97.<br />
Short Title/<br />
Current Status of Regulation/<br />
Title/<br />
Agency<br />
Methodology for Designation of<br />
Frontier and Remote Areas<br />
ACTION: Request for Comment<br />
NOTICE: Methodology for Design.<br />
of Frontier and Remote Areas<br />
AGENCY: HRSA<br />
<strong>Indian</strong> <strong>Health</strong> Service Forms to<br />
Implement the Privacy Rule<br />
ACTION: Request for Comment<br />
NOTICE: IHS Forms to Implement<br />
Privacy Rule (45 CFR Parts 160;<br />
164)<br />
AGENCY: IHS<br />
IHS New System of Records<br />
ACTION: Notice<br />
NOTICE: Privacy Act of 1974<br />
System of Records<br />
AGENCY: IHS<br />
Federal Employees <strong>Health</strong><br />
Benefits Program Coverage<br />
ACTION: Interim Final Rule<br />
NOTICE: Federal Employees<br />
<strong>Health</strong> Benefits Program Coverage<br />
for Certain Intermittent Employees<br />
AGENCY: OPM<br />
TABLE A: REGULATIONS INCLUDED TO DATE IN RRIAR TABLES B AND C<br />
UPDATED THROUGH 11/9/2012<br />
File Code<br />
HRSA (no<br />
reference<br />
number)<br />
IHS-810, 912-<br />
1, 912-2, 913,<br />
and 917<br />
IHS (no<br />
reference<br />
number)<br />
OPM<br />
RIN 3206-<br />
AM74<br />
Dates (Issue, Due, File,<br />
Subsequent Action)<br />
Issue Date: 11/5/2012<br />
Due Date: 1/4/2013<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 10/2/2012<br />
Due Date: 60 days (approx.<br />
11/30/2012)<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: 10/29/2012<br />
Due Date: 12/13/2012<br />
NIHB File Date: Under review.<br />
Date of Subsequent Agency<br />
Action, if any:<br />
Issue Date: [Approved by OMB<br />
as of 11/6/2012]<br />
Due Date:<br />
NIHB File Date:<br />
Date of Subsequent Agency<br />
Action, if any:<br />
In Table B--<br />
Is the summary of<br />
Agency action<br />
included?<br />
Is the NIHB analysis<br />
included?<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
Summary of Agency<br />
action:<br />
NIHB analysis of<br />
action:<br />
In Table C--<br />
Is the list of NIHB<br />
recommendations included?<br />
Has the Agency taken subsequent<br />
action?<br />
Is an analysis of subsequent<br />
Agency action included?<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
NIHB recommendations included:<br />
Subsequent Agency action:<br />
Analysis of Agency action:<br />
: regulation review complete : regulation currently under review : regulation release pending<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>, Regulation Review and Impact Analysis Report Page 38 of 38 11/12/2012
Mr. John n J. O'Brien<br />
Director, , <strong>Health</strong>care and Insuran nce<br />
U.S. Offi ice of Person nnel Manage ement<br />
1900 E Street, S NW, Room R 5532B B<br />
Washing gton, DC 204 415-0001<br />
Re: NIHB N Comm ments on Draf ft Multi-Stat te Plan Proggram<br />
Applicaation<br />
Dear Mr. . O'Brien:<br />
On behal lf of the <strong>National</strong><br />
<strong>Indian</strong> n <strong>Health</strong> Bo oard<br />
Office of f Personnel Managemen M t (OPM) Dra<br />
comment ts are provid ded below as s well as in th<br />
1 , I am wwriting<br />
to suubmit<br />
commments<br />
on thee<br />
U.S.<br />
aft 2014 Muulti-State<br />
Plaan<br />
Program AApplication.<br />
. Our<br />
he attached ccomment<br />
temmplate.<br />
The Mul lti-State Plan n Program (Program) ( will w be criticcally<br />
importtant<br />
to ensurre<br />
that Ameerican<br />
<strong>Indian</strong>s and a Alaska Natives N (AI/ /ANs) are ab ble to accesss<br />
affordable health insurrance<br />
througgh<br />
the<br />
Affordab ble Insurance e Exchanges s (Exchanges s). As discuussed<br />
below, , AI/ANs haave<br />
a federal right<br />
to health care at no cost c to them through the e <strong>Indian</strong> Heaalth<br />
Service, Tribes and Tribal progrrams,<br />
and urban<br />
<strong>Indian</strong> org ganizations (collectively<br />
( , the I/T/U oof<br />
the <strong>Indian</strong>n<br />
health systtem).<br />
Becauuse<br />
of<br />
this, they y are unlikely y to purchas se insurance products onn<br />
the Exchannges<br />
unless tthey<br />
can conntinue<br />
to receive<br />
care at no cost to them m, and do so at the Indiaan<br />
health carre<br />
provider oof<br />
their choicce.<br />
If<br />
they do not particip pate in the Exchanges, E AI/ANs willl<br />
not be abble<br />
to take aadvantage<br />
oof<br />
the<br />
1 Establish<br />
Del livered via electronic e traansmission<br />
Octo ober 22, 20122<br />
hed 40 years ag go, NIHB is an n inter-Tribal organization o thaat<br />
advocates onn<br />
behalf of Triibal<br />
governmennts<br />
for<br />
the provisi ion of quality health h care to all American <strong>Indian</strong>s and AAlaska<br />
Natives. . NIHB is govverned<br />
by a Booard<br />
of<br />
Directors consisting c of a representative<br />
from each of<br />
the twelve Inndian<br />
<strong>Health</strong> SService<br />
(“IHS” ”) Areas. Eachh<br />
Area<br />
<strong>Health</strong> Boa ard elects a rep presentative to o sit on the NIH HB <strong>Board</strong> of DDirectors.<br />
In arreas<br />
where theere<br />
is no Area H<strong>Health</strong><br />
<strong>Board</strong>, Tri ibal governme ents choose a representative who communnicates<br />
policy information aand<br />
concerns of the<br />
Tribes in that area with h NIHB. Whe ether Tribes op perate their enntire<br />
health caare<br />
program tthrough<br />
contraacts<br />
or<br />
compacts with IHS und der Public La aw 93-638, th he <strong>Indian</strong> Selff-Determinatioon<br />
and Educattion<br />
Assistancce<br />
Act<br />
(“ISDEAA A”), or continue e to also rely on o IHS for deli ivery of some, or even most, of their healthh<br />
care, NIHB iis<br />
their<br />
advocate
premium tax credit assistance and cost-sharing exemptions Congress intended would be made<br />
available to improve health care outcomes for AI/AN people.<br />
To overcome this financial barrier to meaningful AI/AN access to the Exchanges, Tribal entities<br />
may choose to pay all or part of the premiums on behalf of designated AI/AN individuals.<br />
Tribes and Tribal organizations will be hesitant to do so unless the plans on the Exchanges are<br />
open to allowing them to make aggregated premium payments on behalf of their members, and<br />
the plans offer to include <strong>Indian</strong> health care providers in their provider networks. In addition,<br />
based on the successful experience under the Medicare Part D Program, we have found the use<br />
of a standard contract addendum that addresses <strong>Indian</strong>-specific issues to be critical to successful<br />
contracting by health plans with <strong>Indian</strong> health care providers. Our comments focus on designing<br />
the Program application criteria to ensure that the Multi-State Plans (MSPs) selected by OPM<br />
will allow Tribal entities to implement this solution for AI/AN people.<br />
Our comments request that the application criteria OPM establishes for the Program encourage<br />
MSP applicants to (1) demonstrate how they will offer to include <strong>Indian</strong> healthcare providers in<br />
their provider networks, (2) agree to use a standard contract addendum when contracting with<br />
<strong>Indian</strong> health care providers, and (3) allow Tribes, Tribal organizations and urban <strong>Indian</strong><br />
organizations to make aggregated group payments of premiums on behalf designated individuals<br />
to the MSPs. These requests are consistent with the guidance provided by CMS in its Final<br />
Exchange Establishment Rule, “Patient Protection and Affordable Care Act; Establishment of<br />
Exchanges and Qualified <strong>Health</strong> Plans,” 77 Fed. Reg. 18346 (March 27, 2012), and with ongoing<br />
efforts by the CMS Center for Consumer Information and Insurance Oversight (CCIIO) to<br />
draft and issue a standard <strong>Indian</strong> addendum, thereby facilitating and encouraging Qualified<br />
<strong>Health</strong> Plans (QHPs) to contract with <strong>Indian</strong> health care providers. For OPM to foster these<br />
three measures (i.e., MSP contracting with <strong>Indian</strong> health care providers, use of a standard <strong>Indian</strong><br />
addendum, and group payment of premiums on behalf of AI/ANs) is also fully consistent with<br />
advancing the Federal trust responsibility.<br />
OPM Has a Continuing Federal Trust Responsibility to Enable Meaningful AI/AN Access to<br />
the Federal <strong>Health</strong> Care Programs It is Charged with Administering<br />
The Federal government’s trust responsibility to provide health care services to Tribes originates<br />
in treaties and other agreements between Tribes and the United States, and has been consistently<br />
reaffirmed in numerous Acts of Congress, Executive Orders, regulations, and the ongoing course<br />
of dealings between the Federal government and <strong>Indian</strong> Tribal governments. The most recent<br />
reaffirmation of the unique responsibility was included in the 2010 amendments to the <strong>Indian</strong><br />
<strong>Health</strong> Care Improvement Act in which Congress declared:<br />
“Congress declares that it is the policy of this Nation, in fulfillment<br />
of its special trust responsibilities and legal obligations to <strong>Indian</strong>s--<br />
(a) to ensure the highest possible health status for <strong>Indian</strong>s<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 2 of 7 October 22, 2012
and urban <strong>Indian</strong>s and to provide all resources necessary to effect<br />
that policy . . .” 2 .<br />
Although the Federal trust responsibility to provide health care to AI/ANs has been carried out in<br />
recent years by the <strong>Indian</strong> <strong>Health</strong> Service (as well as Tribes and Tribal organizations, operating<br />
under the <strong>Indian</strong> Self-Determination and Education Assistance Act (ISDEAA)), this<br />
responsibility is not limited to the <strong>Indian</strong> <strong>Health</strong> Service. Rather, it applies to the Federal<br />
government as a whole, and to each agency charged with administering federal health care<br />
programs.<br />
OPM has demonstrated itself as a model agency in administering the Federal trust responsibility<br />
in its implementation of the Federal Employees <strong>Health</strong> Benefits (FEHB) program option for<br />
Tribes. OPM's commitment to Tribal consultation and the resources required to getting the<br />
program up and running and available to Tribes across the country is to be commended. We<br />
hope that OPM will continue to administer the Federal trust responsibility in the Program with<br />
the same level of commitment, Tribal consultation and collaboration it has demonstrated with the<br />
FEHB program.<br />
The Unique Nature of the <strong>Indian</strong> <strong>Health</strong> System Creates Barriers to Accessing Exchange<br />
Benefits for American <strong>Indian</strong>s and Alaska Natives<br />
American <strong>Indian</strong>s and Alaska Natives have a right to health care at no cost to them, and AI/ANs<br />
who seek services from IHS and Tribal providers do not pay for those services directly.<br />
Consistent with the Federal trust responsibility, Congress has enacted laws that ensure that<br />
AI/ANs are not charged for participating in other federal health care programs. In Medicaid,<br />
CHIP and the Exchanges 3 , for example, there are no deductibles or co-pays for AI/ANs.<br />
Similarly, the ACA provides that AI/ANs are not subject to the penalties for failing to obtain<br />
insurance.<br />
Because AI/ANs can obtain care at no cost to themselves through the I/T/U, AI/ANs will be<br />
hesitant to purchase health insurance through the Exchanges. Yet Congress clearly intended<br />
Exchange coverage to be an additional vehicle for providing additional resources to the <strong>Indian</strong><br />
health care system, and Congress encouraged AI/ANs to participate in the Exchange program<br />
when it exempted most AI/ANs from cost-sharing in the Exchanges.<br />
The Congressional Budget Office (CBO) estimates that the premium exchange subsidies for<br />
qualified individuals will total $1,017 billion over the 2012-2022 period. We estimate as many<br />
as 510,000 AI/ANs will qualify for exchange subsidies as their family income falls between 138<br />
and 400 percent of the Federal Poverty Level (FPL). These tax credits are only available through<br />
the Exchanges.<br />
2 25 U.S.C. § 1602.<br />
3 All AI/AN who receive their care through an I/T/U or contract health services are not subject to cost-sharing<br />
through the Exchanges. AI/AN with incomes below 300 percent of the Federal Poverty Level who receive care<br />
from any other provider are similarly exempt from cost-sharing in the Exchanges.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 3 of 7 October 22, 2012
Access to this benefit is critically important to the <strong>Indian</strong> health system, as it will provide access<br />
to the private insurance market that many AI/ANs could not otherwise afford, and create new<br />
third party sources of revenues for I/T/U, which are chronically underfunded with federal<br />
appropriated funds at only 55 percent of need. Without action by OPM and its sister agencies to<br />
remove barriers to access Exchanges by AI/ANs, however, these benefits will likely remain<br />
unclaimed by AI/AN people, and provide no relief to the chronic health care disparities between<br />
AI/ANs and the general population.<br />
OPM Has an Opportunity to Implement the Program to Reduce Barriers to AI/AN Access to<br />
the Exchanges<br />
OPM has a unique opportunity to further reduce impediments to AI/ANs’ timely access to<br />
comprehensive health care services by lowering barriers to Exchange coverage by AI/ANs and in<br />
the process create positive and lasting change in the health care of AI/AN people. As outlined<br />
above, there are three critical steps for achieving this goal: (1) encourage MSPs to contract with<br />
I/T/U; (2) facilitate the use of a standard <strong>Indian</strong> addendum when contracting with I/T/U; and (3)<br />
require MSPs to accept aggregate payment of premiums on behalf of AI/ANs.<br />
Tribal Sponsorship<br />
Because AI/ANs have little incentive to purchase insurance products on the Exchanges when<br />
they otherwise have a right to free care through the I/T/U system, many Tribes and Tribal<br />
organizations may choose to pay all or part of the unsubsidized portion of the premium payment<br />
on behalf of their members. In the final rule on Exchange establishment, CMS confirmed that an<br />
“Exchange may permit <strong>Indian</strong> Tribes, Tribal organizations and urban <strong>Indian</strong> organizations to pay<br />
aggregated QHP [Qualified <strong>Health</strong> Plan] premiums on behalf of qualified individuals…” 45<br />
C.F.R. § 155.240(b). Similarly, in the Preamble to the Final Rule, CMS stated that “[w]e<br />
encourage Exchanges to include this [Tribal Sponsorship] option as part of its consultation with<br />
Tribal governments.” 77 Fed. Reg. 18310, 18338 (Mar. 27, 2012).<br />
We understand that the MSPs selected by OPM will operate in accordance with the rules of the<br />
Exchange in which they participate. For example, some Exchanges may permit premium<br />
payments from plan enrollees to be made through the Exchange, while others (such as those<br />
operated as Federally-facilitated Exchanges) will require payments to be made directly to the<br />
QHPs themselves. But, as provided for the Affordable Care Act, all Exchange enrollees have the<br />
right to make direct payments to QHPs. Likewise, OPM should ensure that any MSP selected<br />
be willing to permit Tribal entities to make aggregate payments for sponsored AI/ANs in each<br />
Exchange they operate.<br />
Inclusion of I/T/U in MSP Provider Networks<br />
Tribal entities are unlikely to make such premium payments on behalf of their members unless<br />
their Tribal health facilities can fully participate as in-network providers in the MSP provider<br />
networks. Although Section 206 of the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act (IHCIA) allows<br />
I/T/U providers to bill health plans for services provided to the plan’s enrollees whether or not<br />
the I/T/U provider is in the plan’s network, it is preferable that the I/T/U be part of a plan’s<br />
network. Section 408 of the IHCIA provides that Federal health care programs like the Multi-<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 4 of 7 October 22, 2012
State Plan Program must accept I/T/Us as in-network providers on the same basis as any other<br />
provider. Including I/T/U in MSP networks will facilitate coordination of care, minimize<br />
duplication of services, and provide greater certainty to the I/T/U providers in the timeliness and<br />
amount of payments. It will also significantly reduce the transaction costs that would be<br />
involved for each I/T/U to enforce its right to payment under Section 206 of the IHCIA.<br />
Accordingly, we request that OPM encourage plans that seek qualification as an MSP to offer to<br />
contract with I/T/U providers in their service areas. Inclusion of I/T/U providers should be<br />
central to demonstrating network adequacy for AI/AN people who are likely to have longstanding<br />
relationships with these providers who provide culturally competent care.<br />
The Draft 2014 Multi-State Plan Program Application (Application) requires MSPs to<br />
“Describe provisions for adequate choice for enrollees who are American<br />
<strong>Indian</strong>s and for ensuring covered services from the <strong>Indian</strong> <strong>Health</strong> Service,<br />
as applicable”<br />
in demonstrating the adequacy of their provider networks. The Application also requires MSPs<br />
to<br />
“Describe your approach to ensuring compliance with 45 CFR 156.235,<br />
regarding Essential Community Providers in your network.”<br />
We are encouraged that OPM has proposed to ask potential MSPs to demonstrate their networks<br />
will provide adequate choice for AI/AN enrollees and to ensure continued coverage of services<br />
from the IHS. However, we believe this section of the application must be strengthened and<br />
made more precise if it is to have the desired effect. First, we note that it should cover American<br />
<strong>Indian</strong>s and Alaska Natives, not just American <strong>Indian</strong>s. Second, we note that health care services<br />
to AI/ANs are not only provided by the IHS, but also by Tribes, Tribal organizations and urban<br />
<strong>Indian</strong> organizations. Third, the only adequate choice for most AI/AN people is their local I/T/U<br />
provider. In many cases in <strong>Indian</strong> country, the only alternative health care option for AI/AN<br />
people is located hundreds of miles from Tribal population centers, leaving the I/T/U as the only<br />
practical option available. Even in more densely populated areas of the country, the I/T/U offers<br />
the only health care facility providing culturally competent care. Accordingly, because<br />
"adequate choice" for AI/AN people means the I/T/U of their choice, this requirement should be<br />
revised to explicitly require MSP applicants to describe provisions to offer to include I/T/U<br />
providers in their provider networks.<br />
To address these concerns, we recommend that the first of the two provisions above from the<br />
Application be amended, as follows:<br />
Describe provisions for adequate choice for enrollees who are American<br />
<strong>Indian</strong>s or Alaska Natives and for ensuring these enrollees have access to<br />
covered services from the <strong>Indian</strong> <strong>Health</strong> Service, Tribal health programs,<br />
and urban <strong>Indian</strong> health programs, as applicable.<br />
We also note with approval that the draft application would require a plan to demonstrate<br />
compliance with 45 CFR 156.235 regarding essential community providers. I/T/Us are essential<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 5 of 7 October 22, 2012
community providers for purposes of the final Exchange rule, and a “sufficient number and<br />
geographic distribution of essential community providers” must be included in any provider<br />
network for that reason as well.<br />
Use of a Standard <strong>Indian</strong> Addendum<br />
One impediment for I/T/U providers may be the standard contract language an MSP requires.<br />
Often, the standard contract language offered by health plans contains provisions that are<br />
inconsistent with federal Tribal rights. For example, many such contracts will impose a<br />
requirement that the provider demonstrate it has obtained sufficient insurance. I/T/Us are<br />
generally covered by the Federal Tort Claims Act, however, and should not be required to spend<br />
significant and unnecessary dollars purchasing private insurance that is duplicative of FTCA<br />
coverage simply to enter into a provider contract. Likewise, when health plans are informed of<br />
the applicability of various <strong>Indian</strong>-specific federal laws, their concerns are often addressed.<br />
The attached Addendum for <strong>Indian</strong> <strong>Health</strong> Care Providers has been developed to preemptively<br />
address these issues. It sets out federal laws that apply to provider contracts between I/T/Us and<br />
QHPs. We believe that use of this <strong>Indian</strong> Addendum will benefit both the plans and the <strong>Indian</strong><br />
<strong>Health</strong> Care Providers by lowering perceived barriers to contracting, assuring compliance by the<br />
MSPs with key federal laws protecting I/T/Us, and minimizing potential disputes.<br />
HHS has recognized the merits of the use of such an <strong>Indian</strong> Addendum. In the preamble to the<br />
Final Rule on Exchange Establishment, HHS stated that:<br />
We recognize that furnishing QHP issuers with a standard <strong>Indian</strong> Addendum to a<br />
provider contract may make it easier for QHP issuers to contract with <strong>Indian</strong><br />
providers. We note that QHP issuers may not be aware of the various Federal<br />
authorities that govern contracting with <strong>Indian</strong> health providers, and such an<br />
Addendum may lower the perceived barrier of contracting with <strong>Indian</strong> providers.<br />
We plan to develop a template for contracting between QHP issuers and Tribal<br />
health care providers. While we do not uniformly mandate that QHP issuers use<br />
the template, we believe that QHP issuers will find it in their interest to adopt<br />
such a template when contracting with <strong>Indian</strong> providers. We also note that<br />
Exchanges may elect to direct QHP issuers to use the <strong>Indian</strong> Addendum when<br />
contracting with <strong>Indian</strong> providers. 77 Fed. Reg. at 18423.<br />
CCIIO, the agency tasked with developing guidance and regulations on the Exchanges, is<br />
currently developing a standard <strong>Indian</strong> Addendum template. We further understand that CCIIO<br />
is preparing additional guidance that would encourage health plans to offer to contract with I/T/U<br />
using the <strong>Indian</strong> Addendum. We understand that this guidance may be released soon. We<br />
encourage OPM to ensure that the evaluation criteria OPM sets for the MSPs require or at the<br />
very least encourage plans in the strongest possible terms to offer to contract with I/T/U using<br />
the <strong>Indian</strong> Addendum. For your reference, we have attached a copy of a guide to the <strong>Indian</strong><br />
Addendum we previously provided to CCIIO. Again, we strongly encourage OPM to make the<br />
attached <strong>Indian</strong> Addendum a part of OPM's 2014 Multi-State Plan Program Application along<br />
with the explanatory guide.<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 6 of 7 October 22, 2012
The MSPs will be of particular importance to AI/ANs and I/T/Us across the country. Ultimately,<br />
the MSPs will be available in every state, regardless of how a state implements their Exchange<br />
and regardless of whether an Exchange is operated by a state or HHS. Consistent with that<br />
Federal trust responsibility, we urge OPM to ensure that any plan that seeks MSP designation be<br />
required to demonstrate how it will offer to contract with the I/T/U using the Addendum as a<br />
condition for participation as an MSP.<br />
Conclusion<br />
The Multi-State Plan Program provides an important opportunity to ensure that AI/AN people<br />
will be able to meaningfully participate in Exchange coverage options and take advantage of the<br />
federal health care funding offered only through the Exchanges. As discussed above and in the<br />
specific recommendations we have made in the attached comments template, we urge OPM to<br />
administer this federal health care program in a way that incentivizes AI/AN participation in the<br />
Exchanges while still allowing them to receiving culturally competent care at the I/T/U provider<br />
of their choice. OPM can accomplish this by requiring the MSPs to offer to enter into network<br />
provider contracts with I/T/Us using the attached <strong>Indian</strong> addendum, and to allow aggregate<br />
payment of premiums by Tribal entities on behalf of qualified AI/AN individuals.<br />
We appreciate the opportunity to provide comments on OPM's Draft 2014 Multi-State Plan<br />
Program Application. We would like to have further consultation with OPM on the issues raised<br />
in our comments and are available to provide additional information as may be necessary. You<br />
may contact Jennifer Cooper, NIHB Legislative Director at jcooper@nihb.org for further<br />
questions.<br />
cc: Yvette Roubideaux, IHS<br />
Stacy A. Bohlen, NIHB<br />
Susan McNally, OPM<br />
John Cutler, OPM<br />
Gary Cohen, CMS<br />
Peter Nakahata CCIIO<br />
Sincerely Yours,<br />
Cathy Abramson<br />
Chairperson, <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Page 7 of 7 October 22, 2012
November 12, 2012<br />
Centers for Medicare and Medicaid Services<br />
Office of Strategic Operations and Regulatory Affairs<br />
Division of Regulation Development<br />
Department of <strong>Health</strong> and Human Services<br />
Attention CMS-10445 / OCN: 0938-New<br />
Room C4-26-05<br />
7500 Security Boulevard<br />
Baltimore, MD 21244-1850<br />
Submitted via regulations.gov<br />
RE: Comments of CMS-10445; Survey regarding the Medicare Advantage Quality Bonus Payment<br />
Demonstration<br />
I write on behalf of the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NIHB) 1 , to the Centers for Medicare and Medicaid<br />
Services (CMS) regarding the request for comments on CMS-10445 / OCN 0938-New pertaining to the<br />
Paperwork Reduction Act (PRA) Notice on the survey of Medicare Advantage plans regarding the<br />
Medicare Advantage Bonus Payment Demonstration published in the Federal Register on September 17,<br />
2012 (Request for Comments). 2 We appreciate the opportunity to comment on the proposed survey.<br />
We provide below a limited set of recommended additions to the survey.<br />
Background<br />
CMS-10445 requests comments on the survey to be conducted of Medicare Advantage Organizations<br />
(MAOs) as part of an assessment of the MA Bonus Payment Demonstration.<br />
Under the Affordable Care Act (ACA), beginning in 2012, all plans earning four or five stars in Medicare’s<br />
Star Rating program will receive quality bonus payments (QBPs). As an extension of this legislation, CMS<br />
launched the Medicare Advantage Quality Bonus Payment Demonstration, which accelerates the phasein<br />
of QBPs by extending bonus payments to three-star plans and eliminating the cap on blended county<br />
1 Established 40 years ago, NIHB is an inter-Tribal organization that advocates on behalf of Tribal governments for the provision<br />
of quality health care to all American <strong>Indian</strong>s and Alaska Natives. NIHB is governed by a <strong>Board</strong> of Directors consisting of a<br />
representative from each of the twelve <strong>Indian</strong> <strong>Health</strong> Service (“IHS”) Areas. Each Area <strong>Health</strong> <strong>Board</strong> elects a representative to<br />
sit on the NIHB <strong>Board</strong> of Directors. In areas where there is no Area <strong>Health</strong> <strong>Board</strong>, Tribal governments choose a representative<br />
who communicates policy information and concerns of the Tribes in that area with NIHB. Whether Tribes operate their entire<br />
health care program through contracts or compacts with IHS under Public Law 93-638, the <strong>Indian</strong> Self-Determination and<br />
Education Assistance Act (“ISDEAA”), or continue to also rely on IHS for delivery of some, or even most, of their health care,<br />
NIHB is their advocate<br />
2 77 Federal Register 57090, Comment Request, Medicare Advantage Quality Bonus Payment Demonstration, CMS-10445,<br />
September 17, 2012 (http://www.gpo.gov/fdsys/pkg/FR-2012-09-17/html/2012-22726.htm)<br />
Draft NIHB Comments on CMS-10445 Page 1 of 3
enchmarks that otherwise would limit QBPs. Through this demonstration, CMS seeks to understand<br />
how incentive payments impact plan quality across a broader spectrum of plans.<br />
Through a contractor, CMS will conduct a survey of MAOs and as many as 10 case studies of MAOs to<br />
supplement analyses of administrative and financial data for MAOs and environmental and literature<br />
scans. CMS requires this information collection to evaluate the QBP demonstration and better<br />
understand what impact the demonstration has had on MAO operations and their efforts to improve<br />
quality. Researchers will use a survey questionnaire designed to capture information on how MAOs<br />
perceive the demonstration and are planning for or implementing changes in quality initiatives and to<br />
identify factors that help or hinder the capacity to achieve quality improvement and that influence the<br />
decision calculus to make changes. For the case studies, researchers will hold a series of open-ended<br />
discussions with MAO staff guided by a discussion protocol. The case studies will supplement the<br />
information gathered from the survey and data analysis, providing context and details about successful<br />
quality improvement activities.<br />
Analysis<br />
The CMS survey is required of MAOs and will guide CMS in designing quality improvement efforts and<br />
requirements. The survey includes a question about the “main challenges to improving star ratings for<br />
your contract”, and the survey includes a question as to whether quality improvement efforts are<br />
focused on a particular population. The survey does not, though, explicitly query about the efforts<br />
undertaken by MAOs to meet the needs of these particular populations. For instance, and a particular<br />
concern for American <strong>Indian</strong>s and Alaska Natives (AI/ANs), is whether MAOs seek to include culturally<br />
and linguistically competent providers in their networks in order to meet the needs of AI/ANs.<br />
Despite the remote locations of many AI/ANs, and compounded by the relatively low number of AI/ANs<br />
in most MAO service areas, there is typically not a great deal of attention paid to addressing the access<br />
needs of AI/ANs. Including a question in the survey seeking information on whether MAOs focus quality<br />
improvement efforts on particular beneficiary populations should produce useful information, as the<br />
survey currently does. But, the survey should also include a question soliciting information on what<br />
efforts are undertaken to address the needs of these beneficiary populations. Doing so – gathering<br />
information on whether MAOs make efforts to conduct quality improvement efforts with particular<br />
populations as well as identifying what those efforts are – should: 1) provide useful information for<br />
evaluating the Medicare Advantage Quality Bonus Payment Demonstration and 2) stimulate the MAOs<br />
to pay greater attention to these beneficiary populations. Combined, the information will indicate<br />
whether MAOs focus quality improvement efforts on AI/ANs and, if so, what those efforts are.<br />
Recommendations<br />
The proposed survey does seek information (in questions A2. and A2a.) on whether the MAOs focus<br />
quality improvement efforts on particular beneficiary populations.<br />
Recommendation: In question A2a. add the following two options –<br />
Draft NIHB Comments on CMS-10445 Page 2 of 3
_________ American <strong>Indian</strong> or Alaska Native<br />
_________ Persons with English as a second language<br />
The proposed survey, though, does not include a question or provide an opportunity for survey<br />
respondents to include information on efforts to match particular beneficiary populations with<br />
particular providers that may be most responsive to these beneficiaries’ needs.<br />
Recommendation: Re-label A3 as A4, and adjust all subsequent numbering. Insert the following<br />
new questions as “A3.” and “A3a.”.<br />
A3. Have you worked to contract with providers that have cultural and linguistic competencies<br />
for the particular beneficiary populations you are targeting? _____ Yes ______ No<br />
A3a. If yes, which ones?<br />
_______ Federally-Qualified <strong>Health</strong> Centers<br />
_______ <strong>Indian</strong> <strong>Health</strong> Services or other <strong>Indian</strong> health care providers<br />
________ [ ]<br />
_______ Other: ________________________________________<br />
Thank you for your attention to these recommendations. We appreciate the opportunity to provide<br />
comment on CMS-10445. We are available to provide additional information as may be necessary to<br />
fully consider our recommendations.<br />
Sincerely Yours,<br />
Cathy Abramson<br />
Chairman, <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
Cc: Marilyn Tavenner, Acting Administrator, CMS<br />
Kitty Marx, Director of Tribal Affairs, CMS<br />
Dr. Yvette Roubideaux, Director, IHS<br />
Stacy Bohlen, Executive Director, NIHB<br />
H. Sally Smith, Chairwomen, MMPC<br />
Draft NIHB Comments on CMS-10445 Page 3 of 3
Dear Governor:<br />
THE SECRETARY OF HEALTH AND HUMAN SERVICES<br />
WASHINGTON, D.C. 20201<br />
November 9,2012<br />
Over the past two years, we have worked together as many of you began building your new<br />
health insurance marketplaces. The hard work you have engaged in has laid the foundation for<br />
providing access to quality affordable coverage for millions of Americans. Consumers in all<br />
fifty states and the District of Columbia will have access to insurance through these new<br />
marketplaces on January 1, 2014, as scheduled, with no delays.<br />
This Administration is committed to providing significant flexibility for building a marketplace<br />
that best meets your state's needs. We intend to issue further guidance to assist you in the very<br />
near future. Funding is now available to you no matter where you are in the process of<br />
establishing an Exchange and no matter whether you plan to run your own Exchange, partner<br />
with another state, or work with the federal government. In response to your request, we<br />
previously announced that states have until the end of2014 to apply for these federal funds and<br />
have the flexibility to use such funds both for building Exchanges and for associated start-up<br />
costs provided that a state's Exchange is not yet self-sustaining. The next application deadline<br />
for Levelland Level 2 Exchange establishment grants is November 15,2012. I encourage you<br />
to take advantage of these additional resources.<br />
As the date approaches for submission of your Blueprint for Approval of State-based and State<br />
Partnership Exchanges, we have heard from many states that additional time would allow you to<br />
submit a more comprehensive, complete Blueprint application for your Exchange.<br />
The deadline for a Declaration Letter for a State-based Exchange remains Friday, November 16,<br />
2012. However, today, in order to continue to provide you with appropriate technical support if<br />
you are pursuing a State-based Exchange, HHS is extending the deadline for State-based<br />
Exchange Blueprint application submissions to Friday, December 14,2012. HHS will approve<br />
or conditionally approve the State-based Exchanges for 2014 by the statutory deadline of January<br />
1,2013.<br />
Additionally, if you are pursuing a State Partnership Exchange, we will accept Declaration<br />
Letters and Blueprint Applications and make approval determinations for State Partnership<br />
Exchanges on a rolling basis. The final deadline for both the Declaration Letter and Blueprint<br />
Application for State Partnership Exchanges that would be effective for 2014 has been extended<br />
to Friday, February 15,2013. And states will be able to apply to run Exchanges in subsequent<br />
years.
November 9, 2012<br />
Page 2<br />
We are committed to providing you with the flexibility, resources, and technical assistance<br />
necessary to help you achieve successful implementation of your state's Exchange and look<br />
forward to continuing to work with you as we implement the health care law.<br />
Sincerely,<br />
Kathleen Sebelius
Tribal Consultation for <strong>Health</strong> Insurance Exchanges<br />
Survey Questions<br />
Please take a few minutes to fill out this questionnaire for the Tribal Self Governance<br />
Advisory Committee (TSAGC). In December 2012, States will submit their applications,<br />
or “blueprints,” to create a State <strong>Health</strong> Insurance Exchange or to become partners with<br />
the federal government in operating an Exchange. The federal government will ask<br />
States to explain how they consulted with Tribes in their planning process. We want to<br />
hear the perception of Tribes in every State, so we can compare it with what States are<br />
reporting. If your Tribe is in more than one State, please fill out a separate<br />
questionnaire for each State. We would like your response no later than December 20.<br />
Thank you for assisting us.<br />
1. Name of Tribe: __________________<br />
2. Name of Person Responding to Survey: _______________________<br />
3. Title of Person responding to survey: __________________________<br />
4. E-mail address of person responding to survey: ___________________<br />
5. State where Tribe is located: ___________________<br />
If your Tribe is in more than one State, please fill out a separate questionnaire for<br />
each State.<br />
6. Which kind of <strong>Health</strong> Insurance Exchange are you expecting to have in your State:<br />
a. State Exchange<br />
b. Federally Exchange<br />
c. Partnership (Federally-Facilitated Exchange with State taking on some<br />
functions)<br />
d. Don’t know<br />
7. Has your Tribe been involved in Tribal Consultation on Exchanges?<br />
a. Yes at the State level<br />
b. Yes at federal level<br />
c. Not involved at either the State or federal level
Tribal Consultation for <strong>Health</strong> Insurance Exchanges<br />
Survey Questions Page 2<br />
Follow up: What is the main reason you have not been involved?<br />
8. If you wanted to be involved at the State level, do you have the name of a person<br />
working for the State who you could contact?<br />
a. Yes. Please give name: _______________________<br />
b. No.<br />
9. Please check any of the following which describe your State’s Tribal consultation<br />
policy for health insurance exchanges:<br />
a. State has a Tribal consultation policy for the <strong>Health</strong> Insurance Exchange and<br />
Tribes helped to formulate the policy.<br />
b. State does not have a Tribal consultation policy specifically for <strong>Health</strong><br />
Insurance Exchanges, but they have other policies for State government that<br />
require Tribal consultation for planning Exchanges.<br />
c. State is working on a Tribal consultation policy for the Exchange, but it has not<br />
been finalized.<br />
c. State does not have any Tribal consultation policies that cover Exchanges.<br />
d. Don’t know.<br />
10. Has your Tribe been invited to participate in any of the following:<br />
a. Meetings to discuss <strong>Health</strong> Insurance Exchange planning with Tribes Y/N<br />
b. Meetings to discuss Medicaid Expansion with Tribes. Y/N<br />
c. Individual discussions with <strong>Health</strong> Insurance Commissioner. Y/N<br />
d. Individual discussions with State planners for Exchange. Y/N<br />
e. State workgroups set up to plan <strong>Health</strong> Insurance Exchanges. Y/N<br />
f. Membership on the planning or governing body for Exchange. Y/N<br />
11. Has your Tribe been involved in discussions with the State on any of the following<br />
issues related to <strong>Health</strong> Insurance Exchanges:<br />
a. Essential <strong>Health</strong> Benefits Y/N
Tribal Consultation for <strong>Health</strong> Insurance Exchanges<br />
Survey Questions Page 3<br />
b. <strong>Indian</strong> Addendum and Qualified <strong>Health</strong> Plan (QHP) networks Y/N<br />
c. Eligibility and enrollment, including identification of American <strong>Indian</strong>s and<br />
Alaska Natives Y/N<br />
d. Tribal sponsorship of premiums for individuals in Exchange Y/N<br />
e. Payment to I/T/U for services provided to enrolled individuals Y/N<br />
f. Design of website Y/N<br />
g. Navigators and in-person assisters Y/N<br />
h. Call centers Y/N<br />
12. How much do you agree with the following Statements:<br />
a. Our State interacts with Tribes as full partners during the design and<br />
implementation of the <strong>Health</strong> Insurance Exchange.<br />
Strongly agree/Agree/Disagree/Strongly Disagree/ No Answer<br />
b. Tribal consultation on Exchanges has ensured that the <strong>Health</strong> Insurance<br />
Exchange will meet the needs of Tribes in our State.<br />
13. Other comments:<br />
Strongly agree/Agree/Disagree/Strongly Disagree/ No Answer<br />
Thank you.
Background<br />
Analysis of Tribal Consultation Policies<br />
For <strong>Health</strong> Insurance Exchanges<br />
Mim Dixon<br />
November 11, 2012<br />
On September 14, 2011, Secretary of <strong>Health</strong> and Human Services (HHS) Kathleen<br />
Sebelius sent a letter to each State governor regarding Tribal consultation on all health<br />
and human services programs that are supported with federal funding, including Tribal<br />
consultation in the development of health insurance exchange under the Affordable<br />
Care Act (see Attachment A). The Secretary cited the Executive Order on Tribal<br />
Consultation signed by President Obama in 2009, and the HHS Tribal Consultation<br />
Policy. The letter states,<br />
States must consult with Tribes to ensure the programs that they administer with<br />
federal funding meet the needs of the Tribes in that state. Tribes should be<br />
considered full partners by states during the design and implementation of<br />
programs that are administered by states with HHS funding. The requirement of<br />
states to consult with Tribes in the development of the Affordable Insurance<br />
Exchanges is an example of how states can proactively include and partner with<br />
Tribes during the planning stages of a program that has the potential to benefit<br />
Tribal members greatly.<br />
While this letter requires States with federal funding to consult with Tribes on the<br />
development of <strong>Health</strong> Insurance Exchanges, it does not actually require that States<br />
adopt a Tribal consultation policy for their Exchanges. At an HHS Tribal Consultation<br />
on Federally-Facilitated Exchanges held in Washington, DC, on July 26, 2012, a Center<br />
for Consumer Information and Insurance Oversight (CCIIO) representative stated that<br />
the requirement for Tribal consultation would be considered in the certification process<br />
in 2013 when CCIIO decides whether States have the readiness to implement<br />
Exchanges.<br />
Federal Funding for Exchange Planning<br />
Every State except Alaska applied for and received an initial planning grant to consider<br />
whether or not they would create an Exchange, with the understanding that the federal<br />
government would create exchanges for States that did not create their own<br />
Exchanges. States were then able to apply for Establishment Grants to do the work of<br />
designing Exchanges. Level 1 and Level 2 Establishment Grants were available to<br />
States.
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
Tribes understood from the HHS Secretary’s letter to Governors that States with<br />
federally-funded Planning Grants and Establishment Grants would be consulting with<br />
Tribes in their respective States during the planning and implementation process.<br />
Establishment Grant funding could be used for this purpose. However, this has not<br />
happened in every State that received this federal funding.<br />
Partnership Exchanges<br />
CCIIO issued Blueprint for Approval of Affordable State-Based and State Partnership<br />
Insurance Exchanges on August 14, 2012. It outlines ways that States that decide not<br />
to operate their own Exchanges can assume some of the responsibilities for the<br />
Federally-facilitated Exchange (FFE). States may take on functions related to plan<br />
management, or consumer assistance, or both. States that want to take on these<br />
functions must submit a “blueprint” to CCIIO by February 15, 2013. 1 CCIIO is expected<br />
to make decisions in early 2013 2 , about the readiness of States to operate their own<br />
Exchanges or to take on responsibilities in a Partnership Exchange.<br />
Within the Partnership Exchanges, States could take responsibility for a number of<br />
functions that have great interest for Tribes and Urban <strong>Indian</strong> programs, such as<br />
certifying Qualified <strong>Health</strong> Plans with regard to network adequacy and essential health<br />
benefits (EHB), as well as administration of the navigator program and in-person<br />
assister program. Furthermore, States must be involved in the coordination of other<br />
programs that they manage with federal funding -- Medicaid, Medicaid Expansion and<br />
Child <strong>Health</strong> Insurance Programs (CHIP) — with the FFE for purposes of a single,<br />
streamlined application, determination of eligibility, and enrollment. States are also<br />
encouraged to run the re-insurance program that is required under the Affordable Care<br />
Act (ACA) through 2016.<br />
Tribal Consultation Approaches<br />
The <strong>Indian</strong> <strong>Health</strong> Service (IHS), Tribes, and Urban <strong>Indian</strong> clinics (collectively called the<br />
“I/T/U” or “<strong>Indian</strong> health programs”) have the experience and perspective to advise both<br />
the federal government and state governments about how to structure policies and<br />
procedures to be workable in the unique context of <strong>Indian</strong> health programs. <strong>Indian</strong><br />
health programs have a strong interest in making sure that all of the activities of both<br />
state and federal Exchanges are carried out in a way that preserves the protections for<br />
American <strong>Indian</strong>s and Alaska Natives (AI/AN) and makes it easy for the <strong>Indian</strong> health<br />
1 Original deadline of November 16 was extended by HHS on November 9 to February 15, 2012.<br />
2 Originally, the federal government was to decide by January 1, 2013, whether states were ready to operate their<br />
own Exchanges or participate in partnership arrangements. However, the deadline for states to submit their<br />
blueprints was extended from November 15 until December 14. Therefore, it is assumed that HHS may not be able<br />
to assess readiness by January 1, 2013, as originally intended.<br />
2
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
facilities to bill for services that they provide to people who are enrolled in Exchange<br />
plans.<br />
Some States have a better history of working with Tribes than other States where there<br />
may be hostility over a variety of issues that may be unrelated to health care. In States<br />
with good relations with Tribes, there may be state law that requires Tribal consultation<br />
and provides the infrastructure to make it happen. In those States, there may also be a<br />
state policy for Tribal consultation in the Medicaid program and cooperative efforts at<br />
planning. However, in most States – even those with a history of good relationships<br />
with Tribes-- the Exchange planning process is being conducted in the Department of<br />
Insurance or by an off-shoot of that type of agency, which has had very little experience<br />
working with <strong>Indian</strong> health programs. State <strong>Health</strong> Insurance Commissioners typically<br />
are ignorant about <strong>Indian</strong> health programs and federal <strong>Indian</strong> law. Their focus is on<br />
regulating insurance companies so that they do not lose money and fail to live up to<br />
their contractual obligations.<br />
Survey of State Exchange Consultation Policies and Approaches<br />
In 2011, CCIIO provided to Tribes and to the Tribal Technical Advisory Group (TTAG),<br />
an advisory group to the Centers for Medicare and Medicaid (CMS), a list of contact<br />
people in each State that would serve as liaisons with the I/T/U. Starting in July 2012,<br />
Tribal representative began contacting people on that list by e-mail to inquire about<br />
whether or not their Exchange had a Tribal Consultation Policy. By that time, many<br />
people had moved to other jobs, their e-mails were not working, and Tribal<br />
representatives were referred as often as four different times to other people. In some<br />
cases, there was no response to Tribal e-mails and no further names in State<br />
government to pursue. Tribal representatives tried again to contact people in August,<br />
September and October and were unable to make contact with anyone in the following<br />
states: Alaska, Florida, Idaho, Kansas, North Dakota, Texas, and Wisconsin. One can<br />
only assume that if this survey failed to make contact, then the I/T/U also could not use<br />
the list provided by CCIIO to contact anyone involved in Exchange planning in those<br />
States. Tribal representatives asked for an updated list of contacts from CCIIO in<br />
September 2012, but have not yet received it at the time this report is written.<br />
A summary of the findings from the States that responded to this survey is provided as<br />
Attachment B. Only 3 of the 34 states with Tribes had a final, signed Exchange Tribal<br />
Consultation Policy: Colorado, Minnesota, and Oregon. In addition, 6 States reported<br />
that they were working with Tribes on an Exchange Tribal Consultation Policy that they<br />
expected to have signed and completed by the November 16, 2012 deadline for the<br />
State Exchange and Blueprint applications. These are: Arizona, California,<br />
Connecticut, Mississippi, New York, and Washington.<br />
3
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
In a New Mexico and Utah, there are State Tribal consultation policies that cover a<br />
broad range of health topics, including Medicaid. These are being used to guide State<br />
Exchange planning activities. Utah has been consulting with Tribes about updating their<br />
policies, but this process has not been finalized. Nebraska State officials report that<br />
they are using the New Mexico policies as a template and adapting them for Nebraska.<br />
While Oklahoma has returned its Establishment Grant funding is not planning an<br />
Exchange, they note that the Oklahoma <strong>Health</strong> Care Authority, which runs the Medicaid<br />
and CHIP program, has a Tribal Consultation Policy. As long as an Exchange or<br />
Partnership is within State government and a separate quasi-governmental organization<br />
has not been established to operate an Exchange, these States believe that their<br />
existing policies apply to Exchange planning.<br />
Another approach is being used by Rhode Island, which has one federally-recognized<br />
Tribe. Instead of developing a formal Tribal Consultation Policy, they have chosen to<br />
include the Tribal <strong>Health</strong> Director in a variety of State health advisory committees that<br />
have already been established. They have documentation to submit to CCIIO that<br />
describes discussions with the Tribal <strong>Health</strong> Director about Exchange planning issues.<br />
Alabama is another State with one federally-recognized Tribe that seems to think a<br />
formal Tribal Consultation Policy is unnecessary; however, they have put their<br />
Exchange planning on hold until after the elections.<br />
An additional 3 states responded to the survey saying that they are not establishing a<br />
state Exchange and therefore not working on a Tribal Consultation policy: Louisiana,<br />
Montana, and Wyoming. The survey response from Montana reported that the state<br />
was advised by CCIIO that they would be handling Tribal Consultation for the FFE.<br />
Timing of Tribal Consultation<br />
Many States that have received Establishment Grants believe that they do not need to<br />
have a Tribal Consultation Policy until they have state legislation or executive orders to<br />
establish an Exchange, or until they apply to CCIIO for certification to operate an<br />
Exchange or to assume Partnership functions in the FFE. Meanwhile they are going<br />
forward with planning many details that are important to tribes.<br />
For example, according to Reforum website (http://www.statereforum.org/stateprogress-on-essential-health-benefits)<br />
by the end of July 2012, 7 states with Tribes had<br />
formed workgroups on essential health benefits (EHB) (Alabama, Colorado,<br />
Connecticut, Massachusetts, Minnesota, Mississippi, Nebraska, Nevada, and New<br />
York). In addition, 3 States with Tribes had already enacted benchmark plan type<br />
(Arizona, California, and Nevada). Other States with Tribes had conducted<br />
assessments of benchmark plan options (Maine, Michigan, Mississippi, North Carolina<br />
and New York.) Tribes need to be involved with these discussions and decisions<br />
4
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
because significant issues are at stake, including mental health parity, limitation in<br />
number of visits, and having a separate plan for pediatric oral and vision services.<br />
Consultation for Partnerships in FFE<br />
In summary, 13 of the 34 states with Tribes have an approach to Tribal Consultation for<br />
Exchange planning. Among the other 21 states, 10 did not receive Establishment<br />
Grants and are, therefore, not likely to have state Exchanges or Partnerships in the FFE<br />
(including 6 that did not respond to the survey).<br />
Both the I/T/U and the federal government should be most concerned about the States<br />
that received Establishment Grants with the clear direction to engage in Tribal<br />
consultation and for which there is no evidence that this has been done. These include:<br />
Iowa, Massachusetts, Maine, Michigan, North Carolina, Nevada, and South Dakota.<br />
Idaho also received an Establishment Grant, but did not respond to the survey.<br />
A number of these States indicated that they are still evaluating their options and have<br />
not made a decision about what they will be doing, in most cases waiting until after the<br />
election. This seems to be a rationale for not engaging Tribes in the planning process<br />
and not developing policies, such as a Tribal Consultation policy. However, if they have<br />
been using their Establishment Grant funding to do planning, they are likely to submit a<br />
Blueprint for partnership in the FFE. These States may assume FFE functions related<br />
to plan management, or consumer assistance, or both. If the federal government<br />
approves their Partnership applications, these States will be making decisions that<br />
affect the I/T/U without necessary consultation.<br />
Attachments:<br />
A. Letter to Governors from Kathleen Sebelius, HHS Secretary, September 14, 2011<br />
B. Status of Tribal Consultation Policies<br />
C. Issues for Tribal Consultation<br />
5
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
Attachment A<br />
Dear Governor:<br />
THE SECRETARY OF HEALTH AND HUMAN SERVICES WASHINGTON, D.C. 20201<br />
September 14, 2011<br />
Over the last two years, the Department of <strong>Health</strong> and Human Services (HHS) has taken a number<br />
of steps to strengthen our partnership with American <strong>Indian</strong> and Alaska Native Tribal Nations. We<br />
take seriously the federal government's obligation to help improve the health of American <strong>Indian</strong>s<br />
and Alaska Natives through the various health and human services programs administered by the<br />
Department.<br />
However, improving the health and well-being of Tribal nations is contingent upon understanding the<br />
specific needs of Tribal communities. Tribal consultation is an essential tool in understanding these<br />
unique needs and ensuring government to government relations. I am writing to you today to<br />
encourage you to consult with Tribes as you administer health and human services programs that are<br />
supported with federal funding.<br />
HHS has made significant progress in strengthening our partnership with Tribes, and Tribal<br />
consultation is one piece of our efforts to fulfill our responsibility to represent the best interests of<br />
Tribes. Since President Obama signed an Executive Order on Tribal Consultation in 2009, HHS has<br />
also updated its formal Tribal consultation policy. The updated policy includes the responsibility of<br />
states to consult with Tribes when HHS has transferred the authority and funding for programs to<br />
states that are intended to benefit Tribes. States must consult with Tribes to ensure the programs that<br />
they administer with federal funding meet the needs of the Tribes in that state. Tribes should be<br />
considered full partners by states during the design and implementation of programs that are<br />
administered by states with HHS funding. The requirement of states to consult with Tribes in the<br />
development of the Affordable Insurance Exchanges is an example of how states can proactively<br />
include and partner with Tribes during the planning stages of a program that has the potential to<br />
benefit Tribal members greatly. Consultations can identify strengths and barriers to Tribes accessing<br />
these services and ensure that Tribes have the opportunity for greater health care coverage for their<br />
members and employees.<br />
I believe we share a vision of the future where our nation is strong and where every individual and<br />
every community has the opportunity to reach their full potential. We can continue to strengthen<br />
our partnership with Tribes and improve health and human service opportunities for all. Together,<br />
we have the opportunity to build something great.<br />
Kathleen Sebelius<br />
6
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
Attachment B<br />
State <strong>Health</strong> Insurance Exchanges, Status of Tribal Consultation Policies, 10-18-12<br />
Stat<br />
e<br />
Contact Polic<br />
y?<br />
7<br />
Status<br />
(latest status<br />
report date)<br />
Establishm<br />
ent<br />
Grant?<br />
Type<br />
Exchan<br />
ge<br />
Expecte<br />
d<br />
AK No FFE<br />
AL Kathleen Healy<br />
HIX<br />
No FFE<br />
Kathleen.healey@myalabama.gov establishme<br />
nt on hold<br />
until after<br />
elections.<br />
Only one<br />
federallyrecognized<br />
tribe seems<br />
to be reason<br />
for State not<br />
to have<br />
formal<br />
policy.<br />
(7/20/12)<br />
AZ Donald Hughes<br />
Expected to Yes<br />
dhughes@az.gov (602-542-1334) be<br />
completed in<br />
October.<br />
CA Jessica Abernethy<br />
Working on Yes State<br />
Jessica.abernethy@hbex.ca.gov<br />
it. Check in<br />
November<br />
CO Myung Kim<br />
yes CO <strong>Health</strong> Yes State<br />
mkim@cohbe.org<br />
Benefit<br />
Exchange<br />
Policy<br />
Regarding<br />
Consultation<br />
with<br />
Colorado’s<br />
American<br />
<strong>Indian</strong><br />
Tribes was<br />
signed in<br />
December<br />
2011.<br />
CT Julie Lyons Finalize Yes State
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
Julie.Lyons@ct.gov (860-418-<br />
6267)<br />
Sept 27<br />
FL No FFE<br />
IA Angela Doyle Scar<br />
Angela.DouyleScar@idph.iowa.go<br />
v<br />
no (9/18/12) Yes<br />
ID Yes<br />
KS No FFE<br />
LA Carol Steckel<br />
No LA is not No FFE<br />
Carol.Steckel@LA.gov (337-233-<br />
establishing<br />
9627)<br />
a state<br />
based<br />
exchange<br />
and is<br />
therefore not<br />
working on a<br />
Tribal<br />
Consultation<br />
Policy.<br />
(7/9/12)<br />
MA Kaitlyn Kenny<br />
Kaitlyn.kenney@state.ma.us<br />
(617-933-3030)<br />
Yes State<br />
ME Katrin P. Teel<br />
No ME is<br />
Yes<br />
Katrin.Teel@maine.gov<br />
reviewing its<br />
(207-287-3531<br />
options and<br />
has not<br />
developed<br />
any policies<br />
such as<br />
Tribal<br />
Consultation<br />
Policies.<br />
(10/19/12)<br />
MI Chris Priest<br />
No MI is waiting Yes<br />
PriestC1@michigan.gov (517-335- until after<br />
5178)<br />
they have<br />
established<br />
legal<br />
authority for<br />
a statebased<br />
exchange to<br />
work on a<br />
Tribal<br />
Consultation<br />
8
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
MN April Todd-Malmlov<br />
April.todd-malmlov@state.mn.us<br />
(651-296-6025)<br />
MS Liz Barnett<br />
Liz.Barnett@mid.state.ms.us<br />
MT Christa McClure<br />
cmcclure@mt.gov (406-444-2041)<br />
Policy.<br />
(7/10/12)<br />
Yes MN <strong>Health</strong><br />
Insurance<br />
Exchange<br />
Tribal<br />
Consultation<br />
Policy<br />
signed<br />
9/25/12<br />
Working on<br />
it (9/14/12)<br />
No MT was<br />
advised by<br />
CCIIO that<br />
they would<br />
be handling<br />
Tribal<br />
Consultation<br />
for FFE<br />
(7/9/12).<br />
9<br />
Yes<br />
Yes<br />
No<br />
FFE
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
NB John Paul (JP) Sabby<br />
JP.Sabby@nebraska.gov<br />
(402-471-0344)<br />
NC Jean Holliday<br />
Jean.holliday@ncdoi.gov<br />
10<br />
Nebraska is<br />
using NM<br />
Tribal<br />
Consultation<br />
Policy as a<br />
template<br />
and<br />
adapting it.<br />
No decision<br />
on<br />
Exchange<br />
until after<br />
election. If<br />
there is a<br />
State<br />
Exchange, it<br />
will be<br />
located<br />
inside state<br />
government<br />
in Division of<br />
Insurance.<br />
Check back<br />
in<br />
November.<br />
(10-18-12)<br />
No NC has not<br />
established<br />
legal<br />
authority<br />
and<br />
therefore no<br />
legal entity<br />
exists to<br />
execute<br />
Tribal<br />
Consultation<br />
Policy.<br />
There is only<br />
one<br />
federallyrecognized<br />
tribe (EBC)<br />
and they<br />
have been in<br />
discussions<br />
Yes<br />
Yes
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
ND<br />
bout<br />
Exchange.<br />
(7/12/12).<br />
No FFE<br />
NM Priscilla Caverly<br />
State HSD Yes<br />
Priscilla.Caverly@ state.nm.us<br />
has tribal<br />
consultation<br />
policy<br />
signed<br />
7/29/11.<br />
State-Tribal<br />
Collaboratio<br />
n Act ,<br />
SB196,<br />
requires all<br />
departments<br />
of state<br />
government<br />
to have a<br />
tribal<br />
consultation<br />
policy.<br />
(7/10/12)<br />
NV Jon Hager<br />
jhager@exchange.nv.gov (775-<br />
687-9926)<br />
Yes<br />
NY Lisa Sbrana<br />
Tribal<br />
Yes state<br />
Lbs05@health.state.ny.us<br />
consultation<br />
(212-417-5293)<br />
meeting<br />
scheduled<br />
for 10/30/12<br />
OK Buffy Heater<br />
No OK<br />
No FFE<br />
Buffy.heater@okhca.org<br />
exchange<br />
planning on<br />
hiatus and<br />
there is no<br />
Tribal<br />
Consultation<br />
Policy,<br />
although<br />
Medicaid<br />
(OHCA)<br />
does have<br />
one.<br />
(7/13/12)<br />
OR Rachel Oh Yes OR <strong>Health</strong> Yes state<br />
11
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
Rachel.oh@orhix.org Insurance<br />
Exchange<br />
Corporation<br />
Tribal<br />
Consultation<br />
Policy<br />
signed<br />
RI Megan Hall<br />
Megan.hall@faulknerconsultinggr<br />
oup.com<br />
12<br />
4/2/12.<br />
An<br />
unsigned<br />
Tribal<br />
Consultation<br />
Document<br />
dated May<br />
11, 2012,<br />
outlines<br />
processes<br />
for tribalstate<br />
communicati<br />
on. State<br />
has one<br />
federallyrecognized<br />
tribe<br />
(Narraganse<br />
tt). Tribal<br />
health<br />
director<br />
serves on<br />
Medicaid<br />
Advisory<br />
Committee.<br />
Tribe is<br />
invited to<br />
attend public<br />
meetings.<br />
(7/15/12)<br />
Yes state
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
SD Eric Matt<br />
Eric.matt@state.sd.us<br />
No SD has not<br />
yet decided<br />
whether they<br />
will have a<br />
state<br />
exchange.<br />
No formal<br />
Tribal<br />
Consultation<br />
Policy.<br />
Convened<br />
workgroup in<br />
2011 with<br />
tribal<br />
representati<br />
on.<br />
Medicaid<br />
Tribal<br />
Consultation<br />
group meets<br />
quarterly<br />
and they are<br />
updated on<br />
health<br />
reform.<br />
(7/11/12)<br />
TX No FFE<br />
UT Melissa Zito<br />
Dept of<br />
No FFE<br />
mzito@utah.gov (801-712-9346)<br />
<strong>Health</strong> Tribal<br />
Consultation<br />
Policy<br />
signed<br />
11/2/06.<br />
Exchange<br />
uses Utah<br />
<strong>Indian</strong><br />
<strong>Health</strong><br />
Advisory<br />
<strong>Board</strong>.<br />
WA Brad Finnegan<br />
Working on Yes State<br />
Brad.finnegan@hca.wa.gov<br />
it. Check in<br />
November<br />
WI No FFE<br />
WY Tom Hirsig<br />
No No state No FFE<br />
Tom.hirsig@wyo.gov<br />
exchange<br />
and<br />
13<br />
Yes
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
14<br />
therefore no<br />
work on<br />
Tribal<br />
Consultation<br />
Policy.<br />
(7/9/12)
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
Attachment C<br />
Issues for Tribal Consultation in Exchange Planning<br />
Version 10/25/12<br />
A. Qualified <strong>Health</strong> Plan (QHP) Networks and Essential <strong>Health</strong> Benefits<br />
1. Require all QHPs to offer contracts to all I/T/U providers with an <strong>Indian</strong><br />
Addendum<br />
2. Develop rules and processes to assure that AI/AN who are enrolled in a<br />
QHP and referred through an I/T/U CHS program (and/or are below 300<br />
percent FPL) are not charged a co-pay or deductible for services they receive<br />
outside the I/T/U.<br />
3. Essential <strong>Health</strong> Benefits<br />
a. Review the scope and duration of services<br />
b. Providers covered<br />
B. Payment for Services Provided by I/T/U<br />
c. Substitution of benefit categories from benchmark plan<br />
d. Offering pediatric oral and vision services in the QHP versus<br />
a separate plan<br />
e. Compliance with Mental <strong>Health</strong> Parity and Addiction Equity<br />
Act (MHPAEA)<br />
1. Enforcement of Section 206 of the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act<br />
(IHCIA)<br />
a. Assure that the I/T/U is paid in a sufficient and timely way for services<br />
delivered to individuals who are enrolled in QHPs if the I/T/U is not a<br />
network provider.<br />
b. Create single point of contact for I/T/U facilities that have problems<br />
collecting from QHPs, and a process for dealing with those issues.<br />
2. Reimbursement for Waived Cost Sharing<br />
a. Develop a process to assure that the I/T/U receives payment for the<br />
co-pays and deductibles that are waived for AI/AN.<br />
15
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
b. Develop process to reimburse other QHP providers for waived cost<br />
sharing for AI/AN.<br />
C. Eligibility and Enrollment and Tribal Sponsorship<br />
1. Eligibility<br />
a. Identification of individuals who are eligible for special protections and<br />
provisions as AI/AN in the eligibility process and at the provider level to<br />
assure that deductibles and co-pays are waived.<br />
b. Utilization of existing databases or development of new databases to<br />
expedite eligibility determinations.<br />
c. Deciding how additional documentation will be requested, submitted,<br />
reviewed, and stored and how eligibility determinations will be made when<br />
individuals are not included in approved data systems.<br />
d. Develop the system to assure waiver of penalties for AI/AN without<br />
Insurance and to communicate who is covered by this provision in the law.<br />
2. Enrollment process<br />
a. Enrollment process must accommodate special provision for AI/ANs in<br />
Exchanges (monthly enrollment, waiver of cost sharing, exclusion of<br />
certain sources of income).<br />
b. As single point of enrollment, Exchanges must be able to identify<br />
AI/AN for benefits and protections in Medicaid, Medicaid Expansion,<br />
Child <strong>Health</strong> Insurance Programs, and Basic <strong>Health</strong> Plans, if there are<br />
any in the State.<br />
3. Tribal Sponsorship<br />
4. Website<br />
a. Allow tribes to decide which individuals they want to sponsor and<br />
provide opportunity for aggregate payment of premiums.<br />
b. Decide the terms and conditions of Tribal Sponsorship.<br />
c. Allow I/T/U clinic addresses to be used for QHP mailing to enrolled<br />
individuals.<br />
16
D. FFE Data<br />
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
a. Design the website to include information specific to AI/ANs and the<br />
I/T/U.<br />
b. Test the website in <strong>Indian</strong> Country and in urban <strong>Indian</strong> clinics to make<br />
sure it is culturally appropriate, easy to navigate to <strong>Indian</strong> health<br />
information, and the information is presented in a way that is accurate and<br />
easy accessible to consumers, as well as those assisting with enrollment.<br />
5. Enrollment Assistance<br />
a. Carve outs for navigator contracts for the I/T/Us, including an <strong>Indian</strong><br />
Addendum.<br />
b. Provide other enrollment assistance funding, such as Medicaid<br />
Administrative Match (MAM).<br />
6. Call Centers<br />
a. Decide whether it is most appropriate to have an <strong>Indian</strong> desk to handle<br />
questions and resolve problems regarding AI/AN and I/T/Us, or whether<br />
everyone who works at a call center should receive training about Tribes<br />
in the State, the <strong>Indian</strong> health care delivery system and special provisions<br />
in the law, regulations and systems for AI/AN.<br />
b. Review scripts that are used in call centers to assure their accuracy for<br />
AI/ANs and I/T/Us.<br />
c. Provide appropriate back up for call center employees who are unable<br />
to answer questions about AI/ANs and I/T/U and standards for timely<br />
response.<br />
d. Keep FAQs and review answers for accuracy.<br />
1. Enrollment data<br />
2. Federal data hub<br />
a.IHS registration data<br />
b. Other AI/AN data sets<br />
3. Identifying AI/AN in FFE data and reports<br />
a. For benefits and protections for AI/AN<br />
b. For reimbursing cost sharing<br />
17
Analysis of Tribal Consultation Policies For <strong>Health</strong> Insurance Exchanges<br />
c. Performance metrics<br />
d. Measuring effectiveness/barriers to enrollment of AI/AN<br />
E. Outreach and Education<br />
1. Provide outreach and education that is culturally appropriate.<br />
2. Assure that AI/ANs know which QHPs have I/T/U providers in their<br />
networks.<br />
3. Inform consumers and providers about the special protections and<br />
provisions for AI/AN.<br />
18
John O'Brien<br />
Director, <strong>Health</strong>care & Insurance<br />
Office of Personnel Management (OPM)<br />
John O'Brien is the Director of <strong>Health</strong> Care and Insurance at the Office of Personnel Management. In this position he<br />
oversees the insurance programs for federal employees including the Federal Employees <strong>Health</strong> Benefit (FEHB)<br />
program, which provides health insurance to over 8 million federal employees, retirees, and their dependents. In<br />
addition, he leads the team implementing OPM's responsibilities under the Affordable Care Act (ACA). These include<br />
the development of multi-state plans for state exchanges and allowing employees of tribes and tribal organizations to<br />
purchase health and life insurance through the federal system.<br />
From 2007 to 2009 he helped oversee the State of Maryland's unique all-payer hospital rate setting system as the<br />
Deputy Director for Research and Methodology at the Maryland <strong>Health</strong> Services Cost Review Commission (HSCRC).<br />
From 1997 to 2007 he was the Director of Acute Care Policy at the University of Maryland, Baltimore County (UMBC)<br />
Hilltop Institute where his work focused on the management and oversight of Medicaid managed care plans. Mr.<br />
O'Brien was a 2005 recipient of an Ian Axford Fellowship in Public Policy under which he studied health system<br />
performance measurement in New Zealand. He has a Master Degree in Public Administration from Syracuse<br />
University.
Centers for Medicare & Medicaid Services’ Tribal<br />
Technical Advisory Group<br />
American <strong>Indian</strong> and Alaska Native<br />
Strategic Plan<br />
2013 - 2018<br />
This draft plan is being circulated for Tribal Leader and health director comments and<br />
recommendations. An electronic copy is available at: www.nihb.org. Please submit<br />
your comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong><br />
<strong>Board</strong> at EHeintzman@nihb.org. Thank you!<br />
The 2013-2018 CMS-TTAG AI/AN Strategic Plan covers the time period from Fiscal Year 2013 to Fiscal Year<br />
2017(FY2013-FY2017), which spans from October 1, 2013 to September 30, 2018. Recommendations contained in<br />
the plan will also be used to inform budget requests for Fiscal Year 2012.
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
CMS Tribal Technical Advisory Group<br />
W. Ron Allen<br />
Chairman, Jamestown S’Klallam Tribe<br />
Tribal Self Governance Advisory Committee<br />
Representative<br />
Pearl Capoeman-Baller<br />
Quinault <strong>Indian</strong> Nation<br />
Portland Area Representative<br />
James Crouch<br />
Executive Director, California Rural <strong>Indian</strong> <strong>Health</strong><br />
<strong>Board</strong>, Inc.<br />
California Area Representative<br />
Valerie Davidson<br />
Senior Director of Legal and Intergovernmental<br />
Affairs, Alaska Native <strong>Health</strong> Consortium<br />
Alaska Area Representative<br />
Juana Majel-Dixon<br />
Secretary, NCAI Executive Committee<br />
<strong>National</strong> Congress of American <strong>Indian</strong>s<br />
Representative<br />
Judy Goforth Parker, PhD<br />
Administrator, Chickasaw Nation Division of <strong>Health</strong><br />
Oklahoma Area Representative<br />
Carl Harper<br />
Director, Office of Resource Access & Partnerships<br />
<strong>Indian</strong> <strong>Health</strong> Service Representative<br />
Rex Lee Jim<br />
Vice-President, Navajo Nation<br />
Navajo Area Representative<br />
Grace Manuel<br />
Legislative Council Member, Tohono O’odham<br />
Nation<br />
Tucson Area Representative<br />
2<br />
Richard Narcia<br />
President, <strong>Board</strong> of Directors, Gila River <strong>Indian</strong><br />
Community<br />
Phoenix Area Representative<br />
Marlene Redneck<br />
Northern Cheyenne Tribal Council<br />
Billings Area Representative<br />
H. Sally Smith<br />
Chairman, Bristol Bay <strong>Health</strong> Area <strong>Health</strong><br />
Corporation<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> Representative<br />
Carmelita Skeeter<br />
Chief Executive Officer, <strong>Indian</strong> <strong>Health</strong> Care Resource<br />
Center of Tulsa<br />
<strong>National</strong> Council on Urban <strong>Indian</strong> <strong>Health</strong><br />
Representative<br />
Donita Stephens<br />
Finance Director, Choctaw <strong>Health</strong> Center<br />
Nashville Representative<br />
Alec Thundercloud, MD<br />
Executive Director of <strong>Health</strong>, Ho-Chunk Nation<br />
Bemidji Representative<br />
Donald Warne, MD, MPH<br />
Senior Policy Analyst, Great Plains Tribal Chairmen’s<br />
<strong>Health</strong> <strong>Board</strong><br />
Aberdeen Representative<br />
Albuquerque Representative<br />
Vacant
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Table of Contents<br />
TABLE OF CONTENTS ..........................................................................................................1<br />
DEDICATION .....................................................................................................................2<br />
EXECUTIVE SUMMARY ............................................................................................... 3<br />
INTRODUCTION..................................................................................................................4<br />
GOALS AND OBJECTIVES FOR 2013-2018<br />
Goal 1. Tribal Consultation ...........................................................................................................12<br />
Goal 2. Policy Development and Implementation ......................................................................15<br />
Goal 3. Long Term Services and Support ......................................................................................19<br />
Goal 4. Outreach and Education ...................................................................................................22<br />
Goal 5. Data for Evaluation ...........................................................................................................25<br />
APPENDIX A: PLAN SUMMARY AND BUDGET ..........................................................................28<br />
APPENDIX B: LEGAL BASIS FOR SPECIAL CMS PROVISIONS FOR AI/ANS .....................................40<br />
APPENDIX C: CMS ORGANIZATION CHART .............................................................................62<br />
APPENDIX D: COMMON TERMS & ACRONYMS .......................................................................63<br />
ACKNOWLEDGEMENTS ........................................................................................................64<br />
1
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Dedication<br />
This CMS American <strong>Indian</strong> and Alaska Native Strategic Plan<br />
is dedicated to three colleagues whose contributions made the Tribal Technical<br />
Advisory Group (TTAG) stronger and more effective.<br />
Robert Dean Moore, Rosebud Sioux (1963 - 2010)<br />
Tribal Council member for the Rosebud Sioux Tribe, Robert Moore was<br />
the Aberdeen Area representative to the TTAG. Earlier in his career, as the<br />
<strong>Indian</strong> Affairs staff member for former US Senator Tom Daschle, Robert<br />
raised awareness of health disparities and the need for long-term care for<br />
Tribal elders. He was a friend and warrior for all throughout <strong>Indian</strong><br />
communities.<br />
Kristine Anne Locke (1950 - 2012)<br />
Technical Advisor to the Tribal Self Governance Advisory Committee<br />
(TSGAC) representative on the TTAG, Kris Locke brought technical<br />
expertise, wisdom and experience to the process of defining values and<br />
core principles, fostering team work among all participants, and providing<br />
technical and program support for TTAG subcommittees. She worked<br />
tirelessly on behalf of Tribes and American <strong>Indian</strong> and Alaska Native<br />
people.<br />
Elmer Brewster, MSW, MPH, Paiute (1949 - 2012)<br />
A friend to all who knew him, Elmer Brewster was engaged with the TTAG<br />
from its beginning, shared data and information about the costs of <strong>Indian</strong><br />
health care, advocated for payment systems that were inclusive, and<br />
represented the <strong>Indian</strong> <strong>Health</strong> Service and the <strong>Indian</strong> health system<br />
honorably.<br />
2
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Executive Summary<br />
This is the third American <strong>Indian</strong> and Alaska Native (AI/AN) Strategic Plan for the Centers for<br />
Medicare and Medicaid Services (CMS) by the Tribal Technical Advisory Group (TTAG). Update of<br />
AI/AN Strategic Plan is urgently needed to address new opportunities and challenges of<br />
implementing legislation passed since the last Plan was written, including:<br />
American Recovery and Reinvestment Act of 2009 (ARRA)<br />
Patient Protection and Affordable Care Act (ACA), which also amended and<br />
permanently authorized the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act (IHCIA)<br />
AI/AN Strategic Plan has five goals that apply to all CMS programs, including Medicare, Medicaid,<br />
CHIP, and <strong>Health</strong> Insurance Exchanges:<br />
1. CMS engages in meaningful consultation with Tribes and works closely with the TTAG.<br />
(Page 12)<br />
2. CMS enacts and implements policy through regulation, guidance, review and<br />
enforcement to align CMS programs to serve AI/ANs by improving enrollment processes,<br />
assuring access to care, having efficient payment systems, and increasing the I/T/U capacity<br />
to deliver integrated, comprehensive programs. (Page 15)<br />
3. CMS improves and expands opportunities for development and delivery of Long Term<br />
Services and Support throughout <strong>Indian</strong> communities. (Page 19)<br />
4. Through outreach and enrollment activities, all I/T/U programs are fully informed about<br />
CMS programs and AI/ANs know about benefits to which they are entitled. (Page 22)<br />
5. Develop and improve CMS data systems to evaluate and expand the capacity of CMS to<br />
serve American <strong>Indian</strong>s and Alaska Natives. (Page 25)<br />
Annual Plan budget is $5.5 million in 2013, $7.3 million in 2014, $7.4 million in 2015, and $4.5<br />
million in the following 3 years. The higher amounts are needed in the next three years to prepare<br />
for 2014 and on-going implementation to assure that AI/ANs benefit from ACA. Budget summary is<br />
provided in Appendix A (Page 28).<br />
AI/AN Strategic Plan serves as an important reference document through the inclusion of Appendix<br />
B: Legal Basis for Special CMS Provisions for American <strong>Indian</strong>s and Alaska Natives. (Page 39)<br />
3
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Introduction<br />
New developments require strategic response<br />
This is the third American <strong>Indian</strong> and Alaska Native Strategic Plan that the Tribal Technical Advisory<br />
Group (TTAG) to the Centers for Medicare and Medicaid Services (CMS) has prepared to help guide<br />
Centers for Medicare & Medicaid Services (CMS). The first one was issued for the period of 2005-2010,<br />
and the second for the period of 2010-2015. There have been significant changes in the law and in CMS<br />
since the most recent strategic plan was issued in 2009, including:<br />
American Recovery and Reinvestment Act of 2009 (ARRA), P.L. 111-5, February 17, 2009.<br />
Patient Protection and Affordable Care Act (ACA), P.L. 111-148, March 23, 2010, which also<br />
permanently authorized the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act (IHCIA) by Section 10221.<br />
CMS Tribal Consultation Policy, signed Nov 17, 2011.<br />
The Supreme Court of the United States decision on June 28, 2012, that upheld the ACA, but<br />
created new challenges in the event that some states choose not to implement Medicaid<br />
Expansion.<br />
A prolonged period of an economic recession that has created pressures on State budgets<br />
that affect Medicaid program funding and services.<br />
Changes in direction by CMS to create a greater emphasis on payment related to quality,<br />
integration of services, utilization of electronic methods for enrollment and care<br />
management, and greater accountability.<br />
This new American <strong>Indian</strong> and Alaska Native Strategic Plan for 2013-2018 is urgently needed to:<br />
Get ready for 2014 when people will be able to enroll in the new Medicaid Expansion and<br />
<strong>Health</strong> Insurance Exchanges.<br />
Strengthen primary care networks to prepare for the managed care approaches across all<br />
CMS programs by facilitating the integration of <strong>Indian</strong> health providers, utilizing them as<br />
medical homes, acknowledging new provider types and services, and providing adequate<br />
payment for services.<br />
Build capacity for long term care through community based services and support in Tribal<br />
communities.<br />
Implement protections in the law for American <strong>Indian</strong>s and Alaska Natives who enroll in<br />
federally-funded health programs.<br />
4
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Create a partnership between CMS and Tribal governments that provides early discussions<br />
of policy development and planning to assure the integration of CMS programs and <strong>Indian</strong><br />
health programs to create effective processes for enrollment, access to care, care<br />
coordination, quality care, and adequate payment for services.<br />
Reduce health disparities for American <strong>Indian</strong>s and Alaska Natives which are among the<br />
worst of any racial or ethnic group in our nation, a condition that can be improved through<br />
better integration of the <strong>Indian</strong> health care system and CMS programs.<br />
CMS programs must reduce health disparities<br />
Federal funding for Medicaid, Medicaid Expansion, CHIP, Medicare, and <strong>Health</strong> Insurance Exchanges<br />
is intended to reduce health disparities in our society. At every stage of their lifespan, American<br />
<strong>Indian</strong>s and Alaska Natives (AI/AN) have significantly worse health status than the rest of the nation.<br />
A recent analysis of Medicaid data in one state 1 shows that infant mortality among AI/ANs was<br />
twice the rate for the Medicaid population as a whole. Compared to the rest of the world, the<br />
AI/AN infant mortality rate was higher in that State than such countries as Poland, Slovakia, Estonia,<br />
Malaysia, Thailand, and Sri Lanka. Contributing factors included deaths due to Sudden Infant Death<br />
Syndrome (SIDS) at a rate 3 times higher among <strong>Indian</strong>s compared to the total Medicaid population,<br />
deaths due to injuries at a rate 5 times higher among <strong>Indian</strong>s, and a rate of deaths from<br />
complications of pregnancy and delivery 50 percent higher than the total Medicaid population.<br />
Medicaid data from the same state also provided an analysis of the risk factors that lead to poor<br />
pregnancy outcomes. Compared to all pregnant women on Medicaid, <strong>Indian</strong> pregnant women were<br />
2.7 times more likely to have a mental health diagnosis, 3.3 times the rate of alcohol and substance<br />
abuse, a 70 percent higher rate of smoking, and a 30 percent higher rate of obesity.<br />
CMS must assure that AI/ANs and <strong>Indian</strong> <strong>Health</strong> Service (IHS)/Tribal/and Urban <strong>Indian</strong> Organization<br />
(I/T/U) users are accurately identified in records for Medicaid, Medicare and <strong>Health</strong> Insurance<br />
Exchanges that can be used to calculate health disparities, as well as provide utilization data and<br />
performance metrics. In the past IHS provided health status and health disparity information on a<br />
nationwide basis for AI/ANs who are I/T/U users; however, that effort was discontinued in 2007.<br />
According to the most recent reports from IHS, AI/ANs die at higher rates than other Americans<br />
from tuberculosis (500 percent higher), alcoholism (514 percent higher), diabetes (177 percent<br />
higher), unintentional injuries (140 percent higher), homicide (92 percent higher) and suicide (82<br />
1 American <strong>Indian</strong> <strong>Health</strong> Commission for Washington State, Tribal Maternal and Infant <strong>Health</strong> Strategic Plan, 2010.<br />
Analysis based on 8 years of data by Laurie Cawthon, MD, MPH, Manager of First Steps Data Base in Washington<br />
State Department of Social and <strong>Health</strong> Services.<br />
5
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
percent higher). 2 Current data are needed to know whether interventions, such as enrollment in<br />
CMS programs, are effective in changing health outcomes.<br />
A number of factors contribute to persistent disparities in AI/AN health status. American <strong>Indian</strong>s and<br />
Alaska Natives have the highest rates of poverty in America, accompanied by high unemployment<br />
rates, lower education levels, poor housing, lack of transportation and geographic isolation. All of<br />
these factors contribute to insufficient access to health services. American <strong>Indian</strong>s and Alaska<br />
Natives continue to experience historical trauma from damaging federal policies, including those of<br />
forced removal, boarding schools, and taking of tribal lands, and continuing threats to culture,<br />
language, and access to traditional foods.<br />
Historic and persistent under-funding of the <strong>Indian</strong> healthcare system has resulted in problems with<br />
access to care, and has limited the ability of the <strong>Indian</strong> healthcare system to provide the full range of<br />
medications and services that could help prevent or reduce the complications of chronic diseases.<br />
CMS, IHS and Tribes must work together to help eliminate existing health inequalities. Together we<br />
can and must strengthen the ability of <strong>Indian</strong> health programs to serve as the medical home for<br />
AI/ANs, offering culturally competent care with a public health focus, while fulfilling their important<br />
role as essential providers for Medicaid, Medicare, and Children <strong>Health</strong> Insurance programs and the<br />
prospective <strong>Health</strong> Insurance Exchange plans. This plan offers CMS and TTAG a roadmap for making<br />
that happen.<br />
The <strong>Indian</strong> health care system is unique<br />
The United States has acknowledged its special trust responsibility to provide health services to AI/ANs.<br />
This responsibility is the direct result of treaties between the United States and <strong>Indian</strong> Tribes and of<br />
executive orders, and has been reaffirmed by judicial decisions, executive orders, and Acts of Congress<br />
(see Appendix B, p. 39).<br />
The IHS was created in 1955 to assist the United States to fulfill its obligation to provide health care to<br />
AI/ANs. Twenty years later, Congress enacted the <strong>Indian</strong> Self-Determination and Education Assistance<br />
Act of 1975 (P.L. 93-638) to enable Tribes and Tribal Organizations to directly operate health programs<br />
that would otherwise be operated by IHS, thereby empowering Tribes too design and operate health<br />
programs that are responsive to community needs. Title V of the <strong>Indian</strong> <strong>Health</strong> Care Improvement Act<br />
of 1976 (P.L. 94-437) (IHCIA) authorized federal funding for urban <strong>Indian</strong> organizations to provide health<br />
services to AI/ANs, many of whom had been relocated to urban areas by federal relocation programs.<br />
2 Website http://www.ihs.gov/Public Affairs/IHSBrochure/Disparities.asp. AI/AN data from 2004-2006 are<br />
compared with U.S. All Races data for 2005.<br />
6
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Taken together, this complex healthcare delivery system is often referred to as the “I/T/U”<br />
(IHS/Tribal/Urban) or <strong>Indian</strong> healthcare system. A year later, the Congress authorized IHS and tribal<br />
health programs to bill Medicare and Medicaid, which expanded the resources available to them to<br />
carry out the federal trust responsibility.<br />
Today the <strong>Indian</strong> healthcare system includes 46 <strong>Indian</strong> hospitals (1/3 of which are tribally operated) and<br />
nearly 630 <strong>Indian</strong> health centers, clinics, and health stations (80 percent of which are tribally operated).<br />
When specialized services are not available at these sites, health services are purchased from public and<br />
private providers through the IHS-funded Contract <strong>Health</strong> Services (CHS) program. Additionally, 34<br />
urban programs offer services ranging from community health to comprehensive primary care.<br />
The I/T/U utilizes a community-based public health model with many approaches that are not found in<br />
typical American medical delivery systems. For example, the <strong>Indian</strong> health programs include public<br />
health nursing, outreach workers, prevention services, and even building community water and<br />
sanitation services. <strong>Indian</strong> health programs have pioneered new types of providers, such as community<br />
health aides and dental health therapists, as well as new approaches to delivering services in remote<br />
rural areas, including telehealth. Tribal governments manage a wide range of services, such as<br />
substance abuse treatment, the U.S.D.A. nutrition programs for pregnant women, infants and children<br />
(WIC), Senior Centers and elder nutrition sites, rabies vaccinations for dogs, and injury prevention<br />
programs, to name just a few. Tribal programs tend to take a more holistic view and utilize indigenous<br />
people who speak the local language and live in remote Tribal communities.<br />
Not only does the <strong>Indian</strong> health system have to deal with health disparities, it’s important to note that<br />
the system is also challenged with funding disparities. The IHS Federal Disparity Index (FDI) is used to<br />
determine the level of funding for the <strong>Indian</strong> health system relative to its total need. The FDI compares<br />
actual health care costs for an IHS beneficiary to those costs of a beneficiary served in mainstream<br />
America. The FDI uses actuarial methods that control for age, sex, and health status to price health<br />
benefits for <strong>Indian</strong> people using the Federal Employee <strong>Health</strong> Benefits (FEHB) plan, which is then used to<br />
make per capita health expenditure comparisons. Based on this model it is estimated that Congress<br />
provides direct appropriations to the <strong>Indian</strong> health system, on average, at approximately 60 percent of<br />
its level of need. 3 It is these health and funding disparities that exacerbate the challenges in providing<br />
health care for AI/AN people.<br />
3 The IHS calculates funding needs for IHS and tribal health programs by “comparing [IHS] funding to the cost of<br />
providing medical insurance for [AI/AN] users in a mainstream health insurance plan such as the Federal<br />
Employees <strong>Health</strong> Plan (FEHP).” <strong>Indian</strong> <strong>Health</strong> Manual, Part 6, Chapter 4, Manual Exhibit 6-4-A. This methodology<br />
is commonly referred to as the Federal Disparity Index (FDI). Available at:<br />
http://www.ihs.gov/NonMedicalPrograms/lnf/<br />
7
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
The federal government reimburses States 100 percent for Medicaid services delivered to AI/ANs<br />
through IHS and Tribal health programs. States are reimbursed for payments made to Urban <strong>Indian</strong><br />
<strong>Health</strong> Programs for Medicaid services provided to AI/ANs on the basis of the state-specific Federal<br />
Medical Assistance Percentage (FMAP), which in 2013 varies from a minimum of 50 percent up to 73.43<br />
percent. Many programs operated by the IHS and Tribes use a bundled rate approved by the Office of<br />
Management and Budget (OMB) on an annual basis, called the “IHS Reimbursement Rate“ or the ”IHS<br />
encounter rate.” These and other unique circumstances and billing practices are generally not well<br />
understood outside the <strong>Indian</strong> health system. A summary of the legal basis for special CMS provisions<br />
for American <strong>Indian</strong>s and Alaska Natives has been updated and presented in Appendix B (page 39). The<br />
lack of 100 percent FMAP to States for services provided in Urban <strong>Indian</strong> <strong>Health</strong> Programs has precluded<br />
these programs from inclusion in the “IHS encounter rate” reimbursement methodology, and hinders<br />
the recognition by States of the special obligations owed to urban <strong>Indian</strong>s and Urban <strong>Indian</strong> <strong>Health</strong><br />
Programs under Federal law. There is much more work to be done to align the policies, programs, and<br />
systems for billing for CMS services in order to ensure that AI/ANs have the health care coverage they<br />
are entitled to receive.<br />
Tribal consultation is required for CMS programs<br />
The United States government has a unique legal and political relationship with American <strong>Indian</strong> and<br />
Alaska Native Tribes. This special relationship recognizes Tribes as sovereign nations that retain the<br />
inherent right to self-govern, and that interact with the United States on a government-to-government<br />
basis. These rights are grounded in the U.S. Constitution and treaties, and are reinforced by judicial<br />
precedent and Presidential Executive Orders that direct federal agencies to consult with Tribes on a<br />
government-to-government basis. Tribal consultation is an open and continuous exchange of<br />
information that leads to mutual understanding and informed decision making between federal<br />
agencies and tribal governments. Tribal consultation should occur at the earliest possible point in the<br />
policy formulation process, particularly whenever decisions would significantly impact Tribes, would<br />
have a substantial compliance cost, or would result in new or changed policies. Both the Department of<br />
<strong>Health</strong> and Human Services (HHS) and CMS have Tribal consultation policies, and CMS is developing<br />
procedures to operate those policies. The CMS Tribal Consultation policy calls for an annual review and<br />
revisions to update the policy.<br />
The purpose of the first goal of this Strategic Plan is to ensure meaningful consultation with <strong>Indian</strong><br />
Tribes on policy and programmatic issues including, but not limited to eliminating health disparities of<br />
<strong>Indian</strong>s and ensuring access to critical health services, including those made available through Medicare,<br />
Medicaid, CHIP, and Exchange Plans administered by CMS. The involvement of Tribes and the TTAG in<br />
the development of CMS policy allows for culturally appropriate approaches resulting in greater access<br />
8
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
to CMS programs and positive outcomes for <strong>Indian</strong> people and the health programs operated by the<br />
<strong>Indian</strong> <strong>Health</strong> Service, Tribes and Tribal Organizations, and urban <strong>Indian</strong> organizations.<br />
Tribal Technical Advisory Group advises CMS<br />
The Tribal Technical Advisory Group (TTAG) was started by CMS in 2004 as a policy advisory body. In<br />
2009 ARRA Section 5006(e)(l), P.L. 111-5 established the TTAG in law, added new categories of<br />
members, and reaffirmed its status as exempt from the Federal Advisory Committee Act (FACA), 5 U.S.C.<br />
App. 2<br />
TTAG has 18 members: elected tribal leaders (or their designated employees) selected from the 12<br />
Areas of the IHS, as well as representatives from the <strong>National</strong> Congress of American <strong>Indian</strong>s (NCAI), the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NIHB), the Tribal Self-Governance Advisory Committee (TSGAC), the<br />
<strong>Indian</strong> <strong>Health</strong> Service, and the <strong>National</strong> Council of Urban <strong>Indian</strong> <strong>Health</strong> (NCUIH). TTAG meetings,<br />
subcommittees, and workgroups facilitate the exchange of information and perspectives on the<br />
administration of CMS programs and their efficacy in <strong>Indian</strong> communities. TTAG meetings complement,<br />
but do not supplant, tribal consultation processes that take place between CMS and individual Tribes.<br />
Some of the recommendations from the TTAG have been implemented as CMS regulation and policy,<br />
and later reaffirmed in federal law. While the TTAG has offered their advice to CMS on a wide range of<br />
issues, the following are some of the significant achievements:<br />
CMS Tribal Consultation Policy is adopted and training is provided for CMS employees to<br />
implement it.<br />
Native American Contacts (NACs) are designated for each Regional Office of CMS.<br />
Medicaid Administrative Match may be made available by State Medicaid programs to Tribal<br />
health programs to provide enrollment assistance.<br />
<strong>Indian</strong> Addendum 4 developed for Medicare Part D to assure participation by I/T/U pharmacies<br />
on terms appropriate to their governmental status and statutory protections.<br />
Successful campaign is initiated to increase AI/AN enrollment in CHIP.<br />
4 “<strong>Indian</strong> Addendum” refers to contract terms that are specific to IHS and tribal health programs that was<br />
approved by CMS and that Medicare Part D pharmacy plans must include in preferred provider arrangements with<br />
IHS and tribal health programs.<br />
9
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
On April 6, 2012, CMS approved Arizona’s request to amend its 1115 demonstration known as<br />
the Arizona <strong>Health</strong> Care Cost Containment System (AHCCCS), which allows the State to offer<br />
uncompensated care payments to <strong>Indian</strong> <strong>Health</strong> Service and tribal 638 facilities. Under the<br />
amended demonstration, IHS and Tribal 638 facilities can begin to claim payments for<br />
uncompensated care costs associated with services furnished to individuals with income up to<br />
100 percent of the FPL.<br />
CMS training is provided to I/T/U in each Area on an annual basis, supplemented by Medicine<br />
Dish programs, All Tribes calls, a CMS Day at the NIHB Annual Consumer Conference, CMS<br />
sponsorship of a Long Term Care Conference and a website.<br />
Meaningful use of electronic health records rules are defined and promote I/T/U participation.<br />
States are required to consult with Tribes and Tribal Organizations on Medicaid State Plans,<br />
waivers and the development of health insurance exchanges.<br />
Regulation tracking process is implemented for AI/AN and I/T/U issues.<br />
CMS Tribal Affairs Group added staff to address issues.<br />
Medicaid, CHIP, and Medicare enrollment, service and payment data for AI/AN have been<br />
identified and reported .<br />
Collaborative policymaking processes such as those demonstrated by TTAG improve the quality of<br />
resultant decisions.<br />
Organization of CMS AI/AN Strategic Plan<br />
This plan is organized to provide a focus on the goals and objectives. Supporting documentation and<br />
budget summaries are provided in appendices. There are five overarching goals in this plan that apply<br />
to all CMS programs, including Medicare, Medicaid, CHIP, and <strong>Health</strong> Insurance Exchanges. These are:<br />
Goal 1: CMS engages in meaningful consultation with Tribes and works closely with the TTAG.<br />
Goal 2: CMS enacts and implements policy through regulation, guidance, review and<br />
enforcement to align CMS programs to serve AI/ANs by improving enrollment processes,<br />
assuring access to care, having efficient payment systems, and increasing the I/T/U capacity to<br />
deliver integrated, comprehensive programs.<br />
10
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Goal 3: CMS improves and expands opportunities for development and delivery of Long Term<br />
Services and Support (LTSS) throughout <strong>Indian</strong> communities.<br />
Goal 4: All I/T/U programs are fully informed about CMS programs and AI/ANs know about<br />
benefits to which they are entitled.<br />
Goal 5: Develop and improve CMS data systems to evaluate and expand the capacity of CMS to<br />
serve American <strong>Indian</strong>s and Alaska Natives.<br />
For each goal, a number of objectives are listed with tasks identified that are necessary to achieve each<br />
objective.<br />
Budgets for each of the tasks are estimates based on experience and have not been calculated based on<br />
actual or projected costs. For items related to policy development, it is assumed that CMS staff is<br />
already funded. It should be noted that the budgets do not consider the time and expenses of TTAG<br />
members, alternates and their technical advisors who participate in TTAG meetings, subcommittee<br />
meetings, teleconferences, and other activities.<br />
11
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Goal 1: CMS will execute its federal trust responsibility to engage in meaningful consultation<br />
with Tribes and work closely with the Tribal Technical Advisory Group.<br />
Objective 1a – On an annual basis, CMS will engage the TTAG to evaluate and revise the CMS Tribal Consultation<br />
Policy<br />
Task 1: Evaluate and revise existing CMS Tribal Consultation Policy, in collaboration with the<br />
TTAG and CMS Tribal Affairs Group (TAG), and provide an opportunity for Tribal consultation on<br />
the policy.<br />
Task 2: CMS will conduct an annual Tribal Consultation session separate and distinct from the<br />
HHS Department-wide and Regional Tribal Consultation session.<br />
Budget request: $75,000 per year<br />
Task 3: In partnership with TTAG and IHS, CMS will develop a written annual report documenting<br />
and evaluating consultation activities, which will be disseminated to partners in the first quarter<br />
of each fiscal year. The report will assess both consultation processes and outcomes. This<br />
detailed report will be used by TTAG to monitor and evaluate consultation processes and their<br />
impact.<br />
Budget request: $40,000 per year. These funds will be used to support tracking activities by<br />
CMS and process evaluations carried out by a qualified tribal consultant/organization, and<br />
review of the report with relevant stakeholders.<br />
Objective 1b – In collaboration with the TTAG, CMS will develop mechanisms to involve Tribes in states that<br />
have federally-facilitated exchanges and partnership exchanges to assure that I/T/U issues are<br />
addressed in the planning, policies, structure, and operations of those exchanges.<br />
Task 1: Beginning in 2012, CMS and TTAG will agree on a list of issues that could affect AI/AN<br />
participation in health insurance exchanges and create workgroups that meet regularly to resolve<br />
those issues prior to July 2013.<br />
Objective 1c – Each year, CMS will provide financial and administrative support to facilitate the ongoing<br />
activities of TTAG, and a sufficient budget to support TTAG activities included in the 2013-2018<br />
Strategic Plan.<br />
12
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 1: CMS will fully fund the Tribal Technical Advisory Group, including TTAG travel, per diem,<br />
communication needs, basic staffing, and other related expenses for face-to-face meetings up to<br />
three times per year. TTAG serves as a policy advisory body to CMS, providing expertise on<br />
policies, guidelines, and programmatic issues affecting the delivery of health care for AI/ANs.<br />
Budget request: $280,000 per year. Funds will be used to support the travel and per diem<br />
expenses of TTAG members three times per year, occasional subcommittee meetings, and<br />
the ongoing communication and professional technical assistance needed to support TTAG<br />
meetings and activities.<br />
Task 2: CMS will actively seek to recruit AI/ANs for key policy positions, particularly with regard<br />
to <strong>Indian</strong> health care. CMS will develop a personnel succession plan to ensure consistent and<br />
competent TAG staffing with expertise in the <strong>Indian</strong> healthcare system. The personnel succession<br />
plan should include recruitment, training, and promotion strategies, particularly for AI/ANs,<br />
including internships, cross-training opportunities for IHS employees, recruitment of AI/ANs to<br />
serve as Native American Contacts (NACs) in regional offices, and/or providing executive<br />
leadership training for AI/ANs in CMS.<br />
Budget request: $25,000 per year for succession planning and recruiting as needed.<br />
Task 3: The Tribal Affairs Group at CMS will report quarterly to TTAG activities and funding for<br />
implementation of this Strategic Plan.<br />
Task 4: CMS will retain at least 7 FTE personnel in their Tribal Affairs Group (TAG) who will<br />
provide policy and administrative support to TTAG. CMS will hire and retain Native American<br />
Contacts in each of its Regional Office locations.<br />
Objective 1d – CMS personnel with the authority to make binding decisions will regularly participate in TTAG<br />
meetings, the Annual DHHS Budget Consultation session, and DHHS regional tribal consultation<br />
meetings and listening sessions.<br />
Task 1: On an annual basis, the CMS Administrator, and/or CMS Center and Office Directors, will<br />
participate in at least three face-to-face meetings with TTAG, along with other CMS officials with<br />
pertinent expertise in the subject matter at hand.<br />
Task 2: Key leadership from CMS Headquarters will attend annual DHHS regional tribal<br />
consultation meetings and listening sessions.<br />
Objective 1e – CMS will develop a set of standard operating procedures that will be used by the agency to guide<br />
administrative decisions regarding <strong>Indian</strong> health policy.<br />
Task 1: In recognition of the United States trust responsibility described in Appendix B (p. 39),<br />
TTAG and the CMS Office of External Affairs will work collaboratively to develop a set of standard<br />
13
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
operating procedures that can be used by CMS to guide policy formation and Tribal consultation.<br />
Such procedures should be based on values and principles that promote the federal trust<br />
responsibility for health care and Tribal consultation.<br />
Budget request: $40,000 for the first year to develop the standard operating procedures.<br />
Funds will be used to support the completion of this task by a qualified consultant or Tribal<br />
Organization, and any partner meetings needed to develop mutually agreed upon standard<br />
operating procedures. An additional $15,000 per year is requested to monitor compliance<br />
and evaluate the effectiveness of the standard operating procedures.<br />
Examples of such values and principles include:<br />
CMS recognizes that the tribal healthcare delivery system is politically, legally, and culturally<br />
unique and that policies developed specifically for <strong>Indian</strong> healthcare can be designed to apply<br />
only to <strong>Indian</strong> health programs, and will not be considered to set precedent for other types of<br />
healthcare delivery system.<br />
It is a well-settled canon of construction that federal laws enacted for the benefit of <strong>Indian</strong> Tribes<br />
are to be given a liberal interpretation, and that doubtful expressions are to be resolved in favor<br />
of <strong>Indian</strong> interests.<br />
Absent express statutory prohibition, CMS shall engage in Tribal consultation and implement<br />
Tribal recommendations made during such consultations, regarding any CMS policies and actions<br />
that:<br />
1. Have Tribal implications, or<br />
2. Have substantial direct effects on<br />
a. one or more <strong>Indian</strong> Tribes, or<br />
b. the relationship between the Federal Government and <strong>Indian</strong> Tribes, or<br />
c. the distribution of power and responsibilities between the Federal<br />
Government and <strong>Indian</strong> Tribes.<br />
CMS will develop enrollment strategies that maximize AI/AN participation in Medicaid, Medicare,<br />
and CHIP, and health insurance exchanges, and will work collaboratively with I/T/Us to carry out<br />
identified strategies.<br />
14
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Goal 2: CMS enacts policy through regulation, guidance, review and enforcement to align<br />
CMS programs to serve American <strong>Indian</strong>s and Alaska Natives by improving enrollment<br />
processes, assuring access to care, having efficient payment systems, and increasing the I/T/U<br />
capacity to deliver integrated, comprehensive programs.<br />
Objective 2a – CMS will work with the TTAG to develop a global approach to funding enrollment assistance<br />
provided by the I/T/U and eligibility determinations for all CMS supported programs.<br />
Task 1: Evaluate the number of States that are using Medicaid Administrative Match (MAM) to<br />
fund enrollment assistance at I/T/Us and the number of I/T/U programs that are receiving this<br />
funding, and the best approaches to provide financial support (including expansion of MAM to<br />
other I/T/Us and broadening the programs for which its funding can be used) for assisting AI/ANs<br />
who use I/T/U programs to enroll in Medicaid, Medicaid Expansion, CHIP, qualified health plans<br />
through the health insurance exchange, and other insurance and benefits (including those<br />
provided by the Department of Veterans Affairs (VA), and other new approaches for simplifying<br />
applications and approvals for enrollment within control of CMS.<br />
Task 2: Develop mechanisms for the I/T/U to receive Navigator or other funding from the<br />
federally-facilitated Exchanges, partnership exchanges and state exchanges.<br />
Task 3: Consider alternative sources of funding for the I/T/U to assist AI/ANs to enroll in CMS<br />
funded programs, including Medicaid, Medicare, CHIP, and qualified health plans offered through<br />
exchanges, including special enrollments that may be offered to eligibles.<br />
Task 4: Streamline systems to offer aggregate payment options and remove any barriers to<br />
Tribes and others paying premiums for enrollment in federally-funded programs, including<br />
Medicare, Basic <strong>Health</strong> Plans, and <strong>Health</strong> Insurance Exchanges.<br />
Objective 2b – To maximize access to care and coordination of services for AI/ANs, CMS will work with the TTAG<br />
to develop processes to assure that I/T/Us can choose to be network providers for managed care<br />
organizations that deliver services with funding from Medicare, Medicaid, CHIP and <strong>Health</strong><br />
Insurance Exchanges.<br />
Task 1: CMS will work with the TTAG to develop a prototype <strong>Indian</strong> Addendum that can be used<br />
with managed care provider contracts in all programs of CMS to acknowledge the federal laws<br />
that are specific to the I/T/U and that can affect provider contracts.<br />
Task 2: CMS will adopt standards of network adequacy for managed care organizations that are<br />
federally-funded (in whole or part) that require inclusion of I/T/Us as sources of care that are<br />
geographically accessible and culturally appropriate.<br />
15
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 3: CMS will review programs, policies, and payment mechanisms and provide training and<br />
technical assistance to assure that each I/T/U can be the medical home for the AI/ANs who use<br />
its services.<br />
Task 4: CMS will assure that all AI/ANs who are enrolled in a managed care organization through<br />
Medicare, Medicaid, CHIP or <strong>Health</strong> Insurance Exchanges can be referred to specialty care by<br />
I/T/U providers and that the laws and protections regarding deductibles and co-pays for AI/AN<br />
are followed.<br />
Objective 2c – CMS will assure that I/T/Us are paid for all services that are covered by CMS supported<br />
programs and provided to any AI/AN who is enrolled in Medicaid, Medicaid Expansion, Basic<br />
<strong>Health</strong> Plans, Medicare, and <strong>Health</strong> Insurance Exchanges.<br />
Task 1: CMS will enforce the laws that assure that I/T/Us are paid for off-plan services delivered<br />
by it or an I/T/U provider to an AI/AN enrolled in a federally funded program by<br />
assuring that this requirement is included in contracts with managed care organizations<br />
and preferred provider arrangements,<br />
providing a point of contact for I/T/U programs that are not able to receive payment for<br />
services that have been billed,<br />
informing the managed care or preferred provider organization of its obligation to pay<br />
for these services, and<br />
cancelling or not renewing contracts with managed care or preferred provider<br />
organizations or qualified health plans that do not abide by the applicable statutory and<br />
contractual and requirements.<br />
Task 2. CMS will sponsor a conference to engage Tribal technical advisors and others in a better<br />
understanding of emerging payment approaches in Medicare and Medicaid, analyze how those<br />
approaches may affect I/T/U participation and revenues, and share that information with I/T/U<br />
management.<br />
Budget: $120,000 in 2013.<br />
Task 3: All CMS programs will review their payment policies for telehealth services and work<br />
with the TTAG to update those policies to assure that I/T/Us can be paid for telehealth services.<br />
Task 4: CMS will resolve the problem of paying for Medicaid serves for AI/AN youth who are<br />
receiving treatment and/or enrolled in boarding schools in a state other than where their parents<br />
are resident (A/K/A Across State Borders).<br />
Task 5: CMS will create a workgroup across all CMS programs and with the TTAG to develop<br />
criteria for I/T/U providers as distinct provider types for enrollment in Medicare and in State<br />
16
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Medicaid programs in order to achieve greater flexibility for services and distinct payment<br />
methodologies.<br />
Objective 2d – The CMS Office for Dual Eligibles will work with a subcommittee of the TTAG to assure that<br />
I/T/Us can participate in new approaches for coordinating services to and associated payments<br />
for people who are dually eligible for Medicaid and Medicare, and in some cases also eligible for<br />
services from the VA.<br />
Task 1: TTAG will form a subcommittee to work with the Office for Dual Eligibles on planning<br />
new programs, enrollment policies, and payment approaches appropriate for I/T/Us.<br />
Objective 2e – CMS and the TTAG will work together to assure that AI/AN continue to receive needed services<br />
and the I/T/U continues to receive payment for those services In the context of States reforming<br />
their Medicaid programs, creating new types of waivers, choosing whether to implement<br />
Medicaid Expansion, and eliminating CHIP programs.<br />
Task 1: CMS will provide information and technical assistance to Tribes and States to allow them<br />
to adopt the principles and approaches used in the Arizona Medicaid waiver that preserves<br />
services for AI/ANs.<br />
Task 2: CMS will notify Tribes affected by State reforms to their Medicaid programs and consult<br />
with Tribes as soon as practicable on State Medicaid reform proposals.<br />
Task 3: CMS will, as a condition of approving any State reform proposal, require the State to<br />
design its proposal to ensure continued AI/AN access to existing covered services and I/T/U<br />
payment for those services.<br />
Objective 2f – Offices within CMS that are responsible for enforcement and compliance will work with the TTAG<br />
to develop approaches for assisting I/T/Us adhere to applicable laws and regulations, to develop<br />
adequate compliance systems, and to resolve compliance issues.<br />
Task 1: The CMS TAG will provide training on <strong>Indian</strong> health care delivery systems to offices<br />
responsible for enforcement. Such training will include material regarding the unique legal and<br />
regulatory environment in which I/T/Us carry out their programs.<br />
Task 2: CMS will expedite consideration of recommendations regarding Safe Harbors submitted<br />
by Tribes and Tribal Organizations to assure that there is appropriate coordination between<br />
health care delivery systems without violations of the law.<br />
Task 3: CMS will work with the TTAG to develop appropriate policies for compliance that<br />
consider the budgets, size, location, and staffing of I/T/U programs and to develop tiered<br />
standards that do not unreasonably take resources from direct patient care to comply with CMS<br />
requirements for accountability.<br />
17
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 4: CMS will provide training, technical assistance, and funding for systems’ improvements<br />
to I/T/Us to assist them to comply with policies with regard to disclosure and auditing.<br />
Objective 2g– CMS will facilitate implementation of ARRA Section 5006 that authorizes American <strong>Indian</strong><br />
Medicaid Managed Care Entities.<br />
Task 1: CMS will sponsor a meeting with Tribes, Tribal Organizations, urban <strong>Indian</strong><br />
organizations, and others to share information, provide technical assistance, and identify next<br />
steps for implementing the creation of American <strong>Indian</strong> Medicaid Managed Care Entities under<br />
Section 5006 of ARRA.<br />
Budget request: $150,000 per year in 2014 and 2015.<br />
Objective 2h – CMS will create internal processes and funding to facilitate partnerships with Tribes, Tribal<br />
Organizations, and urban <strong>Indian</strong> organizations to work together on new policies and approaches<br />
to better align CMS and I/T/U programs.<br />
Task 1: CMS will substantively involve TTAG in administrative, regulatory, and legislative policy<br />
questions before the notice of proposed rule-making (NPRM) and provide funding for a policy<br />
analyst to track NPRMs, determine whether proposed rules are relevant to <strong>Indian</strong> health care,<br />
provide information to the TTAG about the potential impacts of regulations, track TTAG<br />
comments on NPRMs, and track final regulations to see if they have been responsive to TTAG<br />
recommendations.<br />
Budget request: $250,000 per year<br />
Task 2. CMS will create better mechanisms to fund cooperative agreements with Tribes, Tribal<br />
Organizations, and urban <strong>Indian</strong> organizations to provide policy analysis, outreach and education<br />
to assist CMS to carry out its mission to improve the health status of AI/ANs through better<br />
access to care and quality of care.<br />
Task 3. The CMS Office of Legislation will work with Tribes, Tribal Organizations, and urban<br />
<strong>Indian</strong> organizations on mutually beneficial legislation, including revisions to the Affordable Care<br />
Act to clarify the definition of <strong>Indian</strong> and to address issues related to Medicaid Expansion that<br />
were created by the Supreme Court decision.<br />
Task 4. CMS will move the Tribal Affairs Group from the Office of Public Engagement to the<br />
Office of the Administrator to more accurately reflect its role in policy development across all<br />
CMS agencies.<br />
18
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Goal 3: Improve and expand the development and delivery of Long Term Services and<br />
Support throughout <strong>Indian</strong> communities.<br />
Objective 3a - Develop and maintain an interactive data base of current Long Term Services and Supports (LTSS)<br />
provided by the <strong>Indian</strong> <strong>Health</strong> Service, tribal health programs, and urban <strong>Indian</strong> organizations<br />
with contact information for the providers. Develop toolkits to assist other health programs to<br />
evaluate options and develop similar programs. In addition, CMS working with IHS and the<br />
Administration for Community Living (ACL) in HHS will provide technical assistance to I/T/Us<br />
developing and taking advantage of these LTSS programs<br />
Task 1: Working with ACL and IHS, CMS will develop and maintain a website that will serve as an<br />
AI/AN LTSS portal to:<br />
1. Facilitate a learning community for the sharing of knowledge and expertise among<br />
I/T/U health programs by:<br />
a. Posting lists of existing programs and contacts for each;<br />
b. Posting technical assistance resources, information, and links;<br />
c. Hosting web-based seminars and conference calls;<br />
d. Posting inventory of State Medicaid Plans and waivers that address LTSS in<br />
states where I/T/U programs are located and updating the inventory at least<br />
annually;<br />
e. Research and post “best practices” and models for successful LTSS programs,<br />
including an analysis and description of prior Elder Care Initiative projects;<br />
f. Providing information to I/T/Us about training and technical assistance<br />
resources and potential funding opportunities.<br />
2. Provide an actively moderated listserv that will make available:<br />
a. A forum for communication among CMS, IHS, and ACL with I/T/Us as they<br />
develop LTSS; and<br />
b. A forum for communication and sharing among I/T/U programs<br />
Budget request: $125,000 in 2013 and $100,000 per year in 2014 and 2015.<br />
The website will identify current opportunities and barriers for operation and development of<br />
LTSS communities where I/T/U programs operate, and present “best practices” or models of<br />
successful LTSS programs in such locations and information about how I/T/U programs<br />
participate in these LTSS programs.<br />
19
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Note: In 2011 AoA, IHS and CMS signed a Memorandum of Understanding (MOU) to establish a<br />
coordinated effort between the agencies to develop methods and means for providing technical<br />
support to I/T/Us in order to expand development and delivery of LTSS in <strong>Indian</strong> communities.<br />
Task 2: CMS will work with the TTAG, IHS, and the Administration for Community Living to<br />
develop technical assistance materials for I/T/Us that want to develop and take advantage of<br />
these LTSS programs.<br />
Objective 3b - CMS will develop an AI/AN LTSS Delivery Plan and a LTSS Roadmap (formerly Toolkit) for I/T/Us<br />
to provide information and guidance to I/T/Us wishing to research the possibilities of<br />
implementing LTSS programs in their communities.<br />
Task 1: CMS will work with TTAG and IHS to<br />
Assist I/T/Us to assess their current LTSSs and to identify internal and external barriers<br />
to optimal operation and expansion;<br />
Develop an AI/AN LTSS Service Delivery Plan containing strategies to overcome existing<br />
administrative or regulatory policy barriers for the implementation of LTSS in <strong>Indian</strong><br />
communities, including practical guidance from I/T/Us that have already developed<br />
certain services; and<br />
Develop recommendations on how to engage States and CMS for financing LTSS in<br />
<strong>Indian</strong> communities.<br />
Task 2: Working with TTAG, IHS, and ACL, CMS will develop a searchable web tool (LTSS<br />
Roadmap) as a part of the website development in Objective 3a for use by I/T/Us in the<br />
development of LTSS programs. The Roadmap will include information on LTSS that are<br />
accessible and/or covered under State Plans and waivers, and will include options available to<br />
I/T/Us to overcome barriers and improve access to LTSS and financing.<br />
Budget request: $150,000 per year in 2013, 2014, and 2015.<br />
Objective 3c - Throughout the next five years, CMS and TTAG will work collaboratively to educate tribal leaders<br />
about long term care program planning and implementation, particularly regarding services that<br />
address the needs of elders, veterans, and persons with disabilities.<br />
Task 1: CMS and TTAG will review annually documents that describe overarching principles and<br />
talking‐points, regarding the importance of LTSS for AI/ANs in <strong>Indian</strong> communities and other<br />
communities where I/T/Us are located and delivery by I/T/U programs, controlling the cost and<br />
improving the quality of LTSS programs supported with Federal funds, including Medicare and<br />
Medicaid.<br />
Task 2: On a quarterly basis, CMS and TTAG will develop audience‐specific educational<br />
materials for I/T/U leadership and staff that describe strategies to achieve increased access to<br />
20
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
LTSS in <strong>Indian</strong> communities and other communities in which I/T/U programs are located and<br />
will disseminate these materials to tribal leaders and I/T/U staff.<br />
Budget request: $100,000 per year. These funds will cover formative research, media<br />
design, printing, and dissemination.<br />
Task 3: On an annual basis, CMS will work with TTAG and IHS to identify existing meetings or<br />
conferences that are attended by I/T/U leaders and staff, at which workshops or<br />
presentations could be provided on LTSS services in <strong>Indian</strong> communities and other<br />
communities in which I/T/U programs are located. When appropriate, experts in this field<br />
will provide workshops or presentations.<br />
Budget request: $100,000 per year. These funds will cover travel, per diem, and<br />
registration expenses for CMS, Tribal and/or expert presentations at five or more national<br />
meetings/conferences.<br />
Task 4: ACL, IHS, and CMS will jointly develop and support an annual AI/AN LTSS Conference for<br />
experts to provide education on LTSS and allow I/T/U LTSS programs to share their experiences,<br />
showcase best practices, and enhance the LTSS’ learning network.<br />
Budget request: $200,000 per year in 2013, 2014, and 2015. These funds will cover<br />
conference planning, facility costs, speaker fees, travel, and registration expenses for a<br />
national AI/AN LTSS conference.<br />
Task 5: From 2013-2017, CMS will fund a resource center to build capacity for LTSS for 15<br />
Tribes, by assisting them with planning and development grants, and providing teams of experts<br />
to evaluate their existing LTSS, developing specific steps to integrate and expand necessary<br />
LTSS, and providing program specific assistance in overcoming barriers to accomplishing the<br />
steps.<br />
Budget request: $300,000 in 2013; $1.5 million per year in 2014 and 2015<br />
21
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Goal 4: Every <strong>Indian</strong> <strong>Health</strong> Service, tribal and urban <strong>Indian</strong> health program is fully informed<br />
about CMS programs and every American <strong>Indian</strong> and Alaska Native knows about the benefits<br />
to which they are entitled.<br />
Objective 4a – Maintain effective communications between CMS and Tribes and I/T/U health programs.<br />
Task 1: CMS will work with the TTAG and its Outreach & Education subcommittee to design and<br />
implement a communications plan each year that facilitates a better understanding of CMS<br />
programs among I/T/U providers.<br />
Budget request: $25,000 per year<br />
Task 2: CMS will use national <strong>Indian</strong> organizations such as the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
(NIHB), the <strong>National</strong> Congress of American <strong>Indian</strong>s (NCAI), <strong>National</strong> Council of Urban <strong>Indian</strong><br />
<strong>Health</strong> (NCUIH), and the Tribal Self-Governance Advisory Committee (TSGAC) to share CMS<br />
information with Tribal governments and I/T/U health programs via established communication<br />
channels, such as newsletters, websites, e-mails, and meetings.<br />
Budget request: $150,000 per year. Funds will be used to sponsor national and regional<br />
Tribal Organizations to disseminate CMS information via established communication<br />
channels.<br />
Task 3: At the request of area and national <strong>Indian</strong> organizations, CMS will participate in tribal<br />
meetings, such as: the CMS Day at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>’s Annual Consumer<br />
Conference; the annual meetings for the <strong>National</strong> Congress of American <strong>Indian</strong>s, Tribal Self<br />
Governance, Direct Service Tribes, and Urban <strong>Indian</strong> Clinics; meetings of Area <strong>Indian</strong> <strong>Health</strong><br />
<strong>Board</strong>s; and tribal consultation meetings.<br />
Budget request: $150,000 in 2013, $175,000 in 2014, $175,000 in 2015. Funds will be used<br />
for sponsorship and to support registration, exhibit costs, and travel expenses.<br />
Task 4: CMS should contract with Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong>s and other organizations of I/T/U<br />
programs to publicize CMS trainings and provide travel assistance for tribal participation in<br />
regional trainings.<br />
Budget request: $240,000 in 2013, $240,000 in 2014, $250,000 in 2015. Funds will be used<br />
by regional and national tribal organizations to publicize CMS meetings and facilitate tribal<br />
participation in regional trainings.<br />
22
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Objective 4b – Provide information, training, and capacity building assistance to the I/T/U regarding CMS<br />
programs.<br />
Task 1: In collaboration with TTAG, CMS will develop and implement an annual training plan for<br />
I/T/U providers using appropriate Information Technology (IT) communication systems, such as<br />
webinars, Medicine Dish programs, YouTube videos, and other social media.<br />
Budget request: $100,000 in 2013, $150,000 in 2014, $200,000 in 2015.<br />
Task 2: CMS will hold 20 training meetings per year to provide information about Medicare,<br />
Medicaid, CHIP, and <strong>Health</strong> Insurance Exchanges to I/T/U employees to improve their provision<br />
of CMS services and increase enrollment of AI/AN beneficiaries.<br />
Budget request: $750,000 per year. These funds will be used to contract with Area <strong>Health</strong><br />
<strong>Board</strong>s to hold annual trainings and meetings for I/T/U employees.<br />
Task 3: CMS will develop, maintain, and update web based manual of CMS policies and guidance<br />
that are specifically related to AI/AN and the I/T/U.<br />
Budget request: $100,000 in 2013, $125,000 in 2014, and $150,000 in 2015.<br />
Task 4: All Tribes Calls will be scheduled specifically for issues related to <strong>Indian</strong> healthcare at<br />
least 6 times per year, with TTAG assisting in developing topics for the calls.<br />
Budget request: $100,000 per year.<br />
Task 5: CMS and its contractors will provide tribal-specific ICD-10 training in each of the 12 Areas<br />
of the <strong>Indian</strong> <strong>Health</strong> Service, and other coding training as needed.<br />
Budget request: $200,000 in 2013, $750,000 in 2014, $850,000 in 2015.<br />
Objective 4c – Provide training and technical assistance for I/T/U programs to maximize enrollment of eligible<br />
AI/ANs in Medicaid, Medicaid Expansion, Medicare, CHIP, and <strong>Health</strong> Insurance Exchanges.<br />
Task 1: CMS will provide training and technical assistance to I/T/Us and States to improve access<br />
to sustainable sources of compensation for I/T/Us to provide enrollment assistance to AI/ANs for<br />
CMS programs, such as Medicaid Administrative Match (MAM), and Navigator funding for<br />
Exchange enrollment.<br />
Budget request: $100,000 per year.<br />
Task 2: CMS will provide training and technical assistance to I/T/Us and States to increase<br />
utilization by I/T/Us of electronic enrollment applications and determinations, and new<br />
approaches to simplification of enrollment processes.<br />
Budget request: $500,000 per year.<br />
23
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 3: CMS, in collaboration with TTAG, will develop a simple and practical handout for use by<br />
I/T/U personnel, States, and other entities providing enrollment assistance to AI/ANs that<br />
explains the special provisions they qualify for because of their status as AI/ANs in CMS<br />
programs.<br />
Budget request: $125,000 in 2013, $200,000 in 2014, $125,000 in 2015.<br />
Objective 4d – Provide materials and marketing designed to inform American <strong>Indian</strong>s and Alaska Natives about<br />
CMS programs for which they may be eligible.<br />
Task 1: CMS will develop, design, produce, and disseminate materials that are culturally<br />
appropriate and effective in AI/AN communities, with an emphasis on the new Medicaid<br />
Expansion and <strong>Health</strong> Insurance Exchanges, by:<br />
Hiring graphic artists who are AI/AN<br />
Developing a television campaign with AI/AN images and messages that are<br />
appropriate for people using <strong>Indian</strong> health programs<br />
Developing radio programs for tribal radio stations<br />
Placing materials in effective communication channels<br />
Translating materials as needed<br />
Budget request: $500,000 per year.<br />
24
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Goal 5: Develop and Improve CMS data systems to evaluate and expand the capacity<br />
of CMS to serve American <strong>Indian</strong>s and Alaska Natives.<br />
Objective 5a – CMS will create data systems that identify AI/AN appropriately to assure that they are provided<br />
the benefits and protections under laws and regulations (such as waiver of co-payments and<br />
deductibles) under Medicaid, CHIP, Basic <strong>Health</strong> Plans, and <strong>Health</strong> Insurance Exchanges.<br />
Task 1: CMS and TTAG will create a joint workgroup on Data and Policy to assure that AI/AN<br />
provisions of ARRA and ACA, as well as other laws and regulations, are implemented in<br />
the eligibility and enrollment processes, including designating and implementing the<br />
federal data hub for eligibility; to assure that computer systems used by providers flag<br />
AI/AN cost sharing protections; and to appropriately designate AI/ANs for reporting and<br />
performance metrics, including assessing levels of enrollment.<br />
Task 2: Twice a year CMS will hold a day of meetings at CMS central offices in Baltimore for<br />
TTAG Data and Policy Subcommittee members to exchange information with key CMS<br />
staff in policy implementation, data systems, and innovations to understand the<br />
changes that are occurring with the implementation of health care legislation and how<br />
they could affect AI/AN enrollment and I/T/U provider participation in CMS programs.<br />
Task 3: The attendees will make recommendations to the CMS TTAG regarding approaches<br />
needed to change CMS and other data collection systems for implementation of health<br />
care legislation and suggest topics on the effects on AI/AN and I/T/U for follow-up.<br />
Task 4: Make the CMS data and any findings from the data systems available online, in<br />
presentations at AI/AN and CMS conferences, and in reports, so that AIAN stakeholders<br />
can use the data and findings.<br />
Budget request: $150,000 per year for Objective 5a.<br />
Objective 5b – Develop and improve data for AI/AN populations within and outside of the IHS healthcare<br />
delivery system that can be used to evaluate CMS program enrollment, health care delivery,<br />
outcomes, and payments across states and IHS Areas during the implementation of ACA, CHIPRA,<br />
ARRA, and any subsequent health care policy changes.<br />
Task 1: Establish baseline enrollment rates in CMS programs and federally facilitated <strong>Health</strong><br />
Insurance Exchanges for AI/ANs and monitor changes in the rates.<br />
25
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 2: Establish baseline usage indicators for CMS program health care services used by AI/ANs<br />
and monitor changes in the usage.<br />
Task 3: Determine health outcomes in CMS programs of care for AI/ANs.<br />
Task 4: Establish baseline CMS program payments for health care for AI/ANs and monitor<br />
changes in the payments.<br />
Task 5: Make the evaluation data sets and findings available online, in presentations at AI/AN<br />
and CMS conferences, and in reports, so that AIAN stakeholders can use the data and<br />
findings.<br />
Budget request: $300,000 per year for Objective 5b.<br />
Objective 5c – Produce an AI/AN CMS Data Symposium on the impact of the implementation of ACA, CHIPRA,<br />
ARRA, and any subsequent health care policy changes on AI/AN and I/T/U providers.<br />
Task 1: CMS will sponsor a one-day Data and Policy Conference bringing together experts in<br />
demographic, services ,and policy analysis from outside CMS to better understand the<br />
impacts of the legislative health care reforms relevant to AI/AN and I/T/U providers.<br />
Task 2: Conduct conference planning sessions with CMS staff, and secure the necessary<br />
personnel, materials, facilities, and equipment to accomplish the tasks needed to plan,<br />
prepare, and execute the Conference including making site arrangements for the event<br />
and travel arrangements for speakers.<br />
Task 3: Provide brief descriptions of three research projects that could be carried out using the<br />
American <strong>Indian</strong> specific data developed to date that might have utility to Tribes, IHS<br />
funded health providers, state Medicaid programs or <strong>Health</strong> Benefit Exchanges.<br />
Task 4: Provide a technical writer for the symposium who shall prepare a draft Data Symposium<br />
Summary report within 4 weeks after the event.<br />
Task 5: Make summaries of the presentations available online and in a report, so that AI/AN and<br />
CMS stakeholders can benefit from the data and findings.<br />
Budget request: $50,000 for one conference.<br />
26
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Objective 5d – CMS and TTAG annually will update and review its AI/AN research and evaluation plan to better<br />
track and evaluate CMS program services and policy impacts on AI/ANs and ITUs.<br />
Task 1: CMS will work with the TTAG and its subcommittees, Tribal Epidemiology Centers, and<br />
the HHS <strong>Health</strong> Research Advisory Committee for AI/ANs (HRAC) to update the plan to<br />
identify additional data development and analysis work.<br />
Task 2: Carry out additional data development and analysis activities that are of high impact or<br />
of a time sensitive nature.<br />
Budget request: $75,000 per year for objective 5d.<br />
27
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
APPENDIX A: PLAN SUMMARY AND BUDGET<br />
Goal 1: CMS engages in meaningful consultation with Tribes and work closely with the Tribal Technical Advisory Group (TTAG).<br />
Objectives & Tasks FY 2013 FY 2014 FY 2015 FY 2016 FY 2017 FY 2018<br />
Objective 1a – On an annual basis, CMS will engage the TTAG to evaluate and revise the CMS Tribal Consultation Policy<br />
Task 1: Evaluate and revise existing CMS Tribal Consultation<br />
Policy, in collaboration with the TTAG and CMS Tribal Affairs<br />
Group (TAG), and provide an opportunity for Tribal<br />
consultation on the policy.<br />
<br />
Task 2: Conduct an annual Tribal Consultation session. 75,000 75,000 75,000 75,000 75,000 75,000<br />
Task 3: Written annual report documenting and evaluating<br />
consultation activities disseminated to partners in the first<br />
quarter of each fiscal year to assess both consultation<br />
processes and outcomes.<br />
40,000 40,000 40,000 40,000 40,000 40,000<br />
Objective 1b – In collaboration with the TTAG, CMS will develop mechanisms to involve tribes in states that have federal-facilitated exchanges and partnership<br />
exchanges to assure that I/T/U issues are addressed in the planning, policies, structure, and operations of those exchanges.<br />
Task 1: Beginning in 2012, health insurance exchanges<br />
workgroups that meet regularly to resolve issues.<br />
<br />
Objective 1c – Each year, CMS will provide financial and administrative support to facilitate the ongoing activities of TTAG, and a sufficient budget to support TTAG<br />
activities included in the 2013-2018 Strategic Plan.<br />
Task 1: CMS will fully fund the Tribal Technical Advisory Group. 280,000 280,000 280,000 280,000 280,000 280,000<br />
Task 2: CMS will actively seek American <strong>Indian</strong>s and Alaska<br />
Natives to hire for key policy positions.<br />
25,000 25,000 25,000 25,000 25,000 25,000<br />
28
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 3: The Tribal Affairs Group at CMS will report quarterly to<br />
TTAG<br />
activities and funding for implementation of this Strategic Plan<br />
Task 4: CMS will retain at least 7 FTE personnel in the Tribal Affairs<br />
Group.<br />
<br />
<br />
Objective 1d – CMS personnel with the authority to make binding decisions will regularly participate in TTAG meetings, the Annual DHHS Budget Consultation session,<br />
and DHHS regional tribal consultation meetings and listening sessions.<br />
Task 1: On an annual basis, the CMS Administrator, the CPC<br />
Director, the CMM Director, and the CMSO Director will<br />
participate in at least 3 face-to-face meetings with TTAG, along<br />
with other CMS officials.<br />
Task 2: Key leadership from CMS Headquarters will attend<br />
annual DHHS regional tribal consultation meetings and<br />
listening sessions.<br />
<br />
<br />
Objective 1e – By fiscal year 2013, CMS will develop a set of standard operating procedures that will be used by the agency to guide administrative decisions regarding<br />
<strong>Indian</strong> health policy<br />
Task 1: TTAG and the CMS Office of External Affairs will<br />
develop standard operating procedures that can be used by<br />
CMS to guide policy formation and Tribal consultation.<br />
40,000 15,000 15,000 15,000 15,000 15,000<br />
SUBTOTAL 460,000 435,000 435,000 435,000 435,000 435,000<br />
29
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Goal 2: CMS enacts and implements policy through regulation, guidance, review and enforcement to align CMS programs to serve AI/AN by<br />
improving enrollment processes, assuring access to care, having efficient payment systems, and increasing the I/T/U capacity to deliver integrated,<br />
comprehensive programs.<br />
Objective 2a – CMS will work with the TTAG to develop a global approach to funding enrollment assistance provided by the I/T/U and eligibility determinations for all<br />
CMS programs.<br />
Task 1: Evaluate the number of States and Tribes using<br />
MAM to fund enrollment assistance and other<br />
approaches for assisting AI/AN who use I/T/U facilities<br />
to enroll in CMS programs through the health insurance<br />
exchange websites, and ways to simplifying<br />
applications and approvals for enrollment.<br />
Task 2: Develop mechanisms for the I/T/U to receive<br />
Navigator or other funding from the Federallyfacilitated<br />
Exchanges, the partnership exchanges and<br />
the state exchanges.<br />
Task 3: Consider alternative sources of funding for the<br />
I/T/U to assist AI/AN to enroll in CMS funded programs,<br />
including Medicaid, Medicare and dual eligibles.<br />
Task 4: Streamline systems to offer aggregate payment<br />
options and<br />
remove any barriers to Tribes and others paying<br />
premiums for enrollment in CMS programs.<br />
<br />
<br />
<br />
<br />
Objective 2b – To maximize access to care and coordination of services for AI/ANs, CMS will work with the TTAG to develop processes to assure that the I/T/U can<br />
choose to be network providers for managed care organizations that deliver services with funding from Medicare, Medicaid, CHIP and <strong>Health</strong> Insurance Exchanges.<br />
Task 1: Develop a prototype <strong>Indian</strong> Addendum that<br />
can be used with managed care provider contracts in all<br />
CMS programs.<br />
<br />
30
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 2: Adopt network adequacy standards to include<br />
I/T/U for managed care organizations funded through<br />
CMS programs.<br />
Task 3: Review programs, policies, payment<br />
mechanisms and provide training and technical<br />
assistance to assure that the I/T/U can be the medical<br />
home for AI/AN who use their services.<br />
Task 4: Assure that AI/AN who are enrolled in<br />
managed care organization through CMS programs can<br />
be referred to specialty care by I/T/U providers and<br />
that the laws and protections regarding deductibles<br />
and co-pays for AI/AN are followed.<br />
<br />
<br />
<br />
Objective 2c – CMS will assure that the I/T/U is paid for all services provided that are covered by CMS programs for all AI/AN who are enrolled in Medicaid, Medicaid<br />
Expansion, Basic <strong>Health</strong> Plans, Medicare, and <strong>Health</strong> Insurance Exchanges.<br />
Task 1: CMS enforces the law that assures that the<br />
I/T/U is paid for off-plan services by managed care<br />
organizations with CMS funding.<br />
Task 2: CMS will sponsor a conference to engage Tribal<br />
technical advisors and others on emerging payment<br />
approaches, analyze how those approaches may affect<br />
I/T/U, and share that information.<br />
Task 3: All CMS programs will review their payment<br />
policies to assure that the I/T/U can be paid for<br />
telehealth services delivered to AI/AN.<br />
Task 4: CMS will pay for Medicaid serves for AI/AN<br />
youth who are<br />
receiving treatment and/or enrolled in boarding<br />
schools in a different state from their parents (A/K/A<br />
Across State Borders).<br />
Task 5: CMS will create a workgroup across all agencies<br />
and with the TTAG to develop criteria for I/T/U<br />
providers as distinct provider types for enrollment in<br />
Medicare and Medicaid.<br />
<br />
120,000 0 0 0 0 0<br />
<br />
<br />
<br />
31
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Objective 2d – The Office for Dual Eligibles will work with a subcommittee of the TTAG to assure that there is integration of the <strong>Indian</strong> health system in new<br />
approaches for coordinating services and payments for people who are eligible for Medicaid and Medicare, and in some cases also eligible for services from the VA.<br />
Task 1: Workgroup on policy and data to implement<br />
AI/AN provisions of ARRA and ACA on eligibility and<br />
enrollment, federal data hub, and computer systems<br />
used by providers to flag AI/AN cost sharing<br />
protections, and performance metrics.<br />
<br />
Objective 2e – CMS and the TTAG will work together to assure that AI/AN continue to receive needed services and the I/T/U continues to receive payment for those<br />
services In the context of States reforming their Medicaid programs, creating new types of waivers, choosing whether to implement Medicaid Expansion, and<br />
eliminating CHIP programs.<br />
Task 1: Information and technical assistance to Tribes<br />
and States to adopt principles and approaches used in<br />
Arizona Medicaid waiver to preserve services for AI/AN.<br />
Task 2: Notify Tribes about State Medicaid reforms and<br />
consult with them.<br />
Task 3: State Medicaid reform proposals approval<br />
contingent on continued services for AI/AN from I/T/U,<br />
and payment for those services.<br />
<br />
120,000 0 0 0 0 0<br />
<br />
Objective 2f – Offices within CMS that are responsible for enforcement and compliance will work with the TTAG to develop reasonable approaches for assuring that<br />
I/T/U adheres to laws and regulations.<br />
Task 1: Training on <strong>Indian</strong> health care delivery systems<br />
to CMS offices responsible for enforcement.<br />
Task 2: Expedite consideration of recommendations<br />
regarding Safe<br />
Harbors submitted by Tribes and Tribal Organizations.<br />
Task 3: Develop appropriate policies for compliance<br />
with tiered standards that consider the budgets, size,<br />
location and staffing of I/T/U facilities.<br />
<br />
<br />
<br />
32
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 4: Training, technical assistance, and funding for<br />
systems<br />
improvement to the I/T/U to comply with policies on<br />
disclosure and<br />
auditing.<br />
<br />
Objective 2g– CMS will facilitate ARRA Section 5006 that authorizes American <strong>Indian</strong> Medicaid Managed Care Entities.<br />
Task 1: Sponsor a meeting on the creation of<br />
American <strong>Indian</strong> Medicaid Managed Care Entities under<br />
Section 5006 of ARRA.<br />
0 150,000 150,000 0 0 0<br />
Objective 2h – CMS will create internal processes and funding to facilitate partnerships with Tribes and Tribal organizations to work together on new policies and<br />
approaches to better align CMS and I/T/U programs.<br />
Task 1: Maintain funding for regulation review. 250,000 250,000 250,000 250,000 250,000 250,000<br />
Task 2: Create better mechanisms to fund cooperative<br />
agreements with Tribes and Tribal Organizations.<br />
Task 3: The CMS Office of Legislation will work with<br />
Tribes on mutually beneficial legislation, including<br />
revisions to ACA to clarify the definition of <strong>Indian</strong> and<br />
to address issues related to Medicaid Expansion.<br />
Task 4: Move the CMS Tribal Affairs Group from the<br />
Office of Public Engagement to the Office of the<br />
Administrator.<br />
<br />
<br />
<br />
SUBTOTAL 490,000 400,000 400,000 250,000 250,000 250,000<br />
33
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Goal 3: CMS Improves and expands the development and delivery of Long Term Services and Support (LTSS) throughout <strong>Indian</strong> communities.<br />
Objective 3a - Develop and maintain an interactive data base of current Long Term Services and Supports (LTSS) provided by the <strong>Indian</strong> <strong>Health</strong> Service (IHS), tribal<br />
health programs, and urban <strong>Indian</strong> health programs (I/T/U) with contact information for the providers. Develop tool kits to assist other health programs to evaluate<br />
options and develop similar programs. In addition, CMS working with IHS and the Administration for Community Living (ACL) in HHS will provide technical assistance<br />
to I/T/Us developing and taking advantage of these LTSS programs<br />
Task 1: Working with ACL and IHS, CMS will develop<br />
and maintain a<br />
website that will serve as an AI/AN LTSS portal.<br />
Task 2: CMS will work with the TTAG, IHS and ACL to<br />
develop technical assistance materials for I/T/U.<br />
125,000 100,000 100,000 0 0 0<br />
<br />
Objective 3b - CMS will develop an AI/AN LTSS Delivery Plan and a LTSS Roadmap (formerly Toolkit) for <strong>Indian</strong> communities to provide information and guidance to<br />
I/T/Us wishing to research the possibilities of implementing LTSS programs in their communities.<br />
Task 1: Assist I/T/Us to assess their current LTSSs,<br />
develop an AI/AN LTSS Service Delivery Plan, and<br />
develop recommendations to engage States and CMS<br />
for financing LTSS in <strong>Indian</strong> communities.<br />
Task 2: Develop a searchable web tool (LTSS<br />
Roadmap) as a part of the website development.<br />
<br />
150,000 150,000 150,000 0 0 0<br />
Objective 3c- Throughout the next five years, CMS and TTAG will work collaboratively to educate tribal leaders about long term care program planning and<br />
implementation, particularly regarding services that address the needs of elders, veterans, and persons with disabilities.<br />
Task 1: Annually review documents for I/T/U that<br />
describe principles and talking‐points about the<br />
importance of LTSS, controlling costs, and improving<br />
quality.<br />
<br />
34
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 2: Quarterly development and dissemination of<br />
audience‐specific educational materials for I/T/U<br />
leadership and staff that describe strategies to achieve<br />
increased access to LTSS in <strong>Indian</strong> communities.<br />
Task 3: Annually identify existing meetings or<br />
conferences attended by I/T/U leaders and provide<br />
presentations there on LTSS services in <strong>Indian</strong><br />
communities.<br />
100,000 100,000 100,000 100,000 100,000 100,000<br />
100,000 100,000 100,000 100,000 100,000 100,000<br />
Task 4: Support annual AI/AN LTSS Conference. 200,000 200,000 200,000 0 0 0<br />
Task 5: Fund a resource center to build capacity for<br />
LTSS for 15 Tribes.<br />
300,000 1,500,000 1,500,000 0 0 0<br />
SUBTOTAL 975,000 2,150,000 2,150,000 200,000 200,000 200,000<br />
Goal 4: Every I/T/U facility is fully informed about CMS programs and every AI/AN knows about benefits to which they are entitled.<br />
Objective 4a – Maintain effective communications between CMS and Tribes.<br />
Task 1: Design and implement annual communications<br />
plan that facilitates a better understanding of CMS<br />
programs among I/T/U providers.<br />
Task 2: CMS will use tribal organizations to share CMS<br />
information with Tribes via established communication<br />
channels.<br />
Task 3: At the request of tribal organizations, CMS will<br />
participate in tribal meetings.<br />
Task 4: CMS should contract with Area <strong>Indian</strong> <strong>Health</strong><br />
<strong>Board</strong>s and other Tribal organizations to publicize CMS<br />
trainings and provide travel assistance for Tribal<br />
participation in regional trainings.<br />
Objective 4b – Provide information, training and capacity building assistance to the I/T/U regarding CMS programs.<br />
25,000 25,000 25,000 25,000 25,000 25,000<br />
150,000 150,000 150,000 150,000 150,000 150,000<br />
150,000 175,000 175,000 175,000 175,000 175,000<br />
240,000 240,000 250,000 250,000 250,000 250,000<br />
35
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 1: Develop and implement annual training plan<br />
for I/T/U providers using appropriate Information<br />
Technology (IT) communication systems.<br />
Task 2: Hold 20 training meetings per year to provide<br />
information about CMS programs to I/T/U employees.<br />
Task 3: Develop, maintain and update web based<br />
manual of CMS policies and guidance specifically<br />
related to AI/AN and the I/T/U.<br />
Task 4: All Tribes Calls related to <strong>Indian</strong> healthcare at<br />
least 6 times per year.<br />
Task 5: Tribal-specific ICD-10 training in each of the 12<br />
Areas of the IHS.<br />
100,000 150,000 200,000 200,000 200,000 200,000<br />
750,000 750,000 750,000 750,000 750,000 750,000<br />
100,000 125,000 150,000 100,000 100,000 100,000<br />
100,000 100,000 100,000 100,000 100,000 100,000<br />
200,000 750,000 850,000 200,000 200,000 200,000<br />
Objective 4c – Provide training and technical assistance for I/T/U facilities to maximize enrollment of eligible AI/AN in Medicaid, Medicaid Expansion, Medicare, CHIP<br />
and <strong>Health</strong> Insurance Exchanges.<br />
Task 1: Training and technical assistance to I/T/U and<br />
States to identify enrollment assistance funding for<br />
CMS programs.<br />
Task 2: Training and technical assistance to I/T/U and<br />
States to increase use of electronic enrollment<br />
applications and determinations, and simplification of<br />
enrollment processes.<br />
Task 3: Develop a simple and practical handout for<br />
enrollment assistance that explains the special<br />
provisions for AI/ANs in CMS programs.<br />
100,000 100,000 100,000 100,000 100,000 100,000<br />
500,000 500,000 500,000 500,000 500,000 500,000<br />
125,000 200,000 125,000 0 0 0<br />
Objective 4d – Provide materials and marketing designed to inform AI/AN consumers about CMS programs for which they may be eligible.<br />
36
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 1: CMS will develop, design, produce and<br />
disseminate create materials that are culturally<br />
appropriate and effective in AI/AN communities, with<br />
an emphasis on the new Medicaid Expansion and<br />
<strong>Health</strong> Insurance Exchanges.<br />
500,000 500,000 500,000 500,000 500,000 500,000<br />
SUBTOTAL 3,040,000 3,765,000 3,875,000 3,050,000 3,050,000 3,050,000<br />
Goal 5: Develop and improve CMS data systems to evaluate and expand the capacity of CMS to serve American <strong>Indian</strong>s and Alaska Natives.<br />
Objective 5a – CMS will create data systems that identify AI/AN appropriately to assure that they are provided the benefits and protections under law and regulations<br />
(such as waiver of co-payments and deductibles) under Medicaid, Basic <strong>Health</strong> Plans, and <strong>Health</strong> Insurance Exchanges.<br />
Task 1: Workgroup on policy and data to implement<br />
AI/AN provisions of ARRA and ACA on eligibility and<br />
enrollment, federal data hub, and computer systems<br />
used by providers to flag AI/AN cost sharing protections,<br />
and performance metrics.<br />
Task 2: Twice a year CMS will hold a day of meetings at<br />
CMS for TTAG Data and Policy Committee members to<br />
exchange information with key CMS staff. Attendees will<br />
make recommendations to the CMS TTAG and suggest<br />
topics for follow-up. Presentations at AI/AN and CMS<br />
conferences, and in reports.<br />
<br />
150,000 150,000 150,000 150,000 150,000 150,000<br />
Objective 5b – Develop and improve data for the AI/AN populations within and outside of the IHS healthcare delivery system that can be used to evaluate CMS<br />
program enrollment, health care delivery, outcomes and payments across states and IHS Areas during the implementation of ACA, CHIPRA, ARRA and any subsequent<br />
health care policy changes.<br />
Task 1: Establish baseline enrollment rates for AI/ANs<br />
and monitor<br />
changes.<br />
Task 2: Establish baseline usage indicators for AI/ANs<br />
and monitor<br />
changes.<br />
<br />
<br />
37
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 3: Determine health outcomes for AI/ANs in CMS<br />
programs.<br />
Task 4: Establish baseline CMS program payments for<br />
health care for AI/AN and monitor changes.<br />
Task 5: Make evaluation data sets and findings available<br />
online, in presentations at AI/AN and CMS conferences,<br />
and in reports.<br />
<br />
<br />
300,000 300,000 300,000 300,000 300,000 300,000<br />
Objective 5c – Produce an AI/AN CMS Data Symposium on the impact of the implementation of ACA, CHIPRA ARRA and any subsequent health care policy changes on<br />
AI/AN and I/T/U providers.<br />
Task 1: Sponsor AI/AN Data and Policy Conference. <br />
Task 2: Conduct conference planning sessions with CMS<br />
staff, and secure the necessary personnel, materials,<br />
facilities and equipment to accomplish the tasks needed<br />
to plan, prepare and execute the Conference including<br />
making site arrangements for the event and travel<br />
arrangements for speakers.<br />
Task 3: Provide brief descriptions of three research<br />
projects that could be carried out using AI/AN specific<br />
data.<br />
Task 4: Technical writer for the symposium shall prepare<br />
Data Symposium Summary.<br />
Task 5: Make summaries of the presentations available<br />
online, and in a report.<br />
<br />
<br />
<br />
50,000 0 0 0 0 0<br />
Objective 5d – CMS and TTAG annually will update and review its AI/AN research and evaluation plan to better track and evaluate CMS program services and policy<br />
impacts on AI/AN’s and ITU’s.<br />
38
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Task 1: CMS will work with the TTAG and its Sub<br />
Committees, Tribal<br />
Epidemiology Centers, and the DHHS <strong>Health</strong> Research<br />
Advisory Committee<br />
for AI/AN (HRAC) to update the plan to identify additional<br />
data<br />
development and analysis work.<br />
Task 2: Carry out additional data development and<br />
analysis activities that are of high impact or of a time<br />
sensitive nature.<br />
TOTAL<br />
S<br />
<br />
75,000 75,000 75,000 75,000 75,000 75,000<br />
575,000 525,000 525,000 525,000 525,000 525,000<br />
TOTALS 5,540,000 7,275,000 7,385,000 4,460,000 4,460,000 4,460,000<br />
39
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Appendix B: Legal Basis for Special CMS Provisions for American <strong>Indian</strong>s and Alaska Natives<br />
I. Introduction<br />
Carol Barbero, Esq. 5<br />
Elliott Milhollin, Esq.<br />
Hobbs, Straus, Dean and Walker, LLP<br />
November 2012<br />
There is a special relationship between the United States and <strong>Indian</strong> Tribes that creates a trust<br />
responsibility toward <strong>Indian</strong> people regarding health care. The existence of this truly unique obligation<br />
supplies the legal justification and moral foundation for health policy making specific to American<br />
<strong>Indian</strong>s and Alaska Natives (AI/ANs) – with the objectives of enhancing their access to health care and<br />
overcoming the chronic health status disparities of this segment of the American population.<br />
It is beyond question that the obligation to carry out the trust responsibility to <strong>Indian</strong>s applies to all<br />
agencies of the federal government – including the Centers for Medicare & Medicaid Services (CMS) –<br />
as evidenced by Presidential Executive Orders and Special Memoranda. 6 Furthermore, with regard to<br />
health care for AI/ANs, federal law assigns comprehensive duties to the Secretary of the Department of<br />
<strong>Health</strong> and Human Services (HHS) in order to achieve the goals and objectives established by Congress<br />
for <strong>Indian</strong> health. The trust responsibility, and laws enacted pursuant thereto, provides ample<br />
authority for the Secretary – whether acting through the <strong>Indian</strong> <strong>Health</strong> Service (IHS), CMS, or other<br />
agency of HHS – to take pro-active efforts to achieve the <strong>Indian</strong> health objectives Congress has<br />
articulated.<br />
5 The initial version of this Appendix D appeared in the first Strategic Plan submitted to CMS in 2005 by the CMS Tribal<br />
Technical Advisory Group. In that submission, the author acknowledged the Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
(NPAIHB) and its member tribes for their generous support of the author’s earlier work which provided foundation for that<br />
paper. That earlier paper, titled "The Federal Trust Responsibility: Justification for <strong>Indian</strong>-Specific <strong>Health</strong> Policy," was<br />
presented at the <strong>National</strong> Roundtable on the <strong>Indian</strong> <strong>Health</strong> System and Medicaid Reform sponsored by the NPAIHB at the<br />
Urban Institute on August 31, 2005. This Appendix D has been updated to reflect significant <strong>Indian</strong>-specific health policy<br />
legislative and administrative actions that have occurred since it was originally drafted. The authors would like to thank the<br />
United South and Eastern Tribes, Inc. for its generous support in updating this Appendix D.<br />
6 See, e.g., Exec. Order No. 13175, 65 Fed. Reg. 67249 (Nov. 6, 2000) reprinted in 2000 U.S.C.C.A.N. at B77; White House<br />
Memorandum for Heads of Executive Departments and Agencies, Nov. 5, 2009; Dep't of <strong>Health</strong> and Human Services Tribal<br />
Consultation Policy (Dec. 14, 2010); Centers for Medicare and Medicaid Services Tribal Consultation Policy (Nov. 17, 2011);<br />
Cramer v. United States, 261 U.S. 219 (1923).<br />
40
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
HHS and CMS both recognize this authority in their tribal consultation policy:<br />
Since the formation of the Union, the United States (U.S.) has recognized<br />
<strong>Indian</strong> Tribes as sovereign nations. A unique government-to-government<br />
relationship exists between <strong>Indian</strong> Tribes and the Federal Government<br />
and this relationship is grounded in the U.S. Constitution, numerous<br />
treaties, statutes, Federal case law, regulations, and executive orders that<br />
establish and define a trust relationship with <strong>Indian</strong> Tribes. This<br />
relationship is derived from the political and legal relationship that <strong>Indian</strong><br />
Tribes have with the Federal Government and is not based upon race.<br />
This special relationship is affirmed in statutes and various Presidential<br />
Executive Orders … 7<br />
While CMS often looks to the Social Security Act for authority, the historic and complex body of federal<br />
<strong>Indian</strong> law and case law applies throughout the federal government to all agencies, including CMS. The<br />
intent of this paper is to provide a brief summary of federal <strong>Indian</strong> law that is most relevant to current<br />
and future regulations and guidance regarding participation of <strong>Indian</strong>s and the <strong>Indian</strong> health system in<br />
Medicare, Medicaid, Child <strong>Health</strong> Insurance Programs, and health insurance exchanges.<br />
II. The United States has a Trust Responsibility to <strong>Indian</strong>s<br />
A. Origins of the trust responsibility to <strong>Indian</strong>s<br />
The federal trust responsibility to <strong>Indian</strong>s, and the related power to exercise control over <strong>Indian</strong> affairs<br />
in aid of that responsibility, is rooted in the United States Constitution – most significantly the <strong>Indian</strong><br />
Commerce Clause, the Treaty Clause, and the exercise of the Supremacy Clause. 8 The Constitution<br />
contains no explicit language that defines the trust relationship. Rather, the parameters of the trust<br />
responsibility have evolved over time through judicial pronouncements, treaties, Acts of Congress,<br />
Executive Orders, regulations, and the ongoing course of dealings between the federal government<br />
and <strong>Indian</strong> tribal governments.<br />
7 Dep't of <strong>Health</strong> and Human Services Tribal Consultation Policy (Dec. 14, 2010), at 1; Centers for Medicare and Medicaid<br />
Services Tribal Consultation Policy (Nov. 17, 2011), at 1.<br />
8 Morton v. Mancari, 417 U.S. 535, 551-552 (1974) ("The plenary power of Congress to deal with the special problems of<br />
<strong>Indian</strong>s is drawn both explicitly and implicitly from the Constitution itself."); McClanahan v. Arizona State Tax Comm’n, 411<br />
U.S. 164, 172, n.7 (1973); see also TASK FORCE No. 9, VOL. 1, AMERICAN INDIAN POLICY REVIEW COMM’N 31 (1976)<br />
(explaining the origins of Constitutional power to regulate <strong>Indian</strong> affairs as flowing from Congress’s treaty making powers,<br />
powers to regulate commerce with <strong>Indian</strong> tribes, and its authority to withhold appropriations); FELIX S. COHEN, HANDBOOK<br />
OF FEDERAL INDIAN LAW 418-423 (2005); Reid Payton Chambers, Judicial Enforcement of the Federal Trust Responsibility to<br />
<strong>Indian</strong>s, 27 STAN. L. REV. 1213, 1215-1220 (1975).<br />
41
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
The earliest formal dealings between the federal government and <strong>Indian</strong> Tribes were undertaken<br />
through treaty-making. From the United States’ perspective, treaty objectives were essentially twofold:<br />
cessation of hostilities to achieve and maintain public peace, and acquisition of land occupied by<br />
tribal members. Tribes doubtless had a peace-making motive as well, but in return for the vast tracts<br />
of land they relinquished to the more powerful federal government, Tribes also obtained the promise –<br />
expressed or implied – of support for the social, educational, and welfare needs of their people,<br />
including health care. These treaties/promises were the first expression of the federal government’s<br />
obligation to <strong>Indian</strong> tribes.<br />
The initial express recognition that a trust responsibility existed came from the courts. In the landmark<br />
case of Cherokee Nation v. Georgia, 30 U.S, 1 (1831), Chief Justice John Marshall established the legal<br />
foundation for the trust responsibility by describing <strong>Indian</strong> Tribes as “domestic dependent nations”<br />
whose relationship with the United States “resembles that of a ward to his guardian.” Id. At 17. That<br />
theme – and the duty of the federal sovereign to <strong>Indian</strong> Tribes – carried forward some 50 years later<br />
when, in United States v. Kagama, 118 U.S. 375, 384 (1886), the Supreme Court acknowledged that<br />
Tribes are under the protection and care of the United States:<br />
From their very weakness and helplessness, so largely due to the course<br />
of dealing of the federal government with them, and the treaties in which<br />
it has been promised, there arises the duty of protection, and with it the<br />
power [of protection]. 9<br />
Through nearly two centuries of case law, the courts have extensively examined the parameters of the<br />
trust responsibility to <strong>Indian</strong>s, frequently in the context of whether the federal government has the<br />
authority to perform an action and whether there are limitations on the exercise of Congressional<br />
power over <strong>Indian</strong> affairs. While Congress has plenary authority over <strong>Indian</strong> matters through the<br />
Constitution, the “guardian-ward” relationship articulated by Chief Justice Marshall requires that<br />
federal actions be beneficial, or at least not harmful, to <strong>Indian</strong> welfare. This is not to say, however,<br />
that the United States has always acted honorably toward <strong>Indian</strong>s throughout its history. 10<br />
Nonetheless, the fact that our government has failed in some instances to act in an honorable manner<br />
9 See also <strong>Board</strong> of County Commissioners of Creek County v. Seber, 318 U.S. 705, 715 (1943) ("Of necessity the United<br />
States assumed the duty of furnishing . . . protection [to <strong>Indian</strong> tribes] and with it the authority to do all that was required<br />
to perform that obligation . . . .").<br />
10 An example is unilateral abrogation of <strong>Indian</strong> treaties by Congress. See, e.g., Lone Wolf v. Hitchcock, 187 U.S. 553<br />
(1903).<br />
42
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
toward <strong>Indian</strong>s does not and should not absolve the more powerful sovereign from its responsibility to<br />
carry out its obligations honorably.<br />
B. “<strong>Indian</strong>” as a political rather than a racial classification: <strong>Indian</strong>-specific lawmaking and<br />
the “rationally related” standard of review<br />
In pursuit of its authority under the Constitution and the trust responsibility, Congress has enacted<br />
<strong>Indian</strong>-specific laws on a wide variety of topics 11 as well as included <strong>Indian</strong>-specific provisions in<br />
general laws to address <strong>Indian</strong> participation in federal programs. 12 In the landmark case of Morton v.<br />
Mancari, 417 U.S. 535 (1974), the Supreme Court set out the standard of review for such laws – the<br />
“rational basis” test. In Mancari, the Court reviewed an assertion by non-<strong>Indian</strong>s that the application<br />
of <strong>Indian</strong> preference in employment at the Bureau of <strong>Indian</strong> Affairs (as ordered in the <strong>Indian</strong><br />
Reorganization Act 13 ) was racially discriminatory under the then-recently amended civil rights law<br />
which prohibited racial discrimination in most areas of federal employment.<br />
11 See, e.g., <strong>Indian</strong> <strong>Health</strong> Care Improvement Act, 25 U.S.C. § 1601, et seq.; <strong>Indian</strong> Self-Determination and Education<br />
Assistance Act, 25 U.S.C. §450, et seq.; <strong>Indian</strong> Education Act, 20 U.S.C. §7401, et seq.; Tribally Controlled Schools Act, 25<br />
U.S.C. §2501, et seq.; Tribally Controlled College or University Assistance Act, 25 U.S.C. §1801, et seq.; Native American<br />
Housing Assistance and Self-Determination Act, 25 U.S.C. §4101, et seq.; <strong>Indian</strong> Child Welfare Act, 25 U.S.C. §1901, et seq.;<br />
<strong>Indian</strong> Child Protection and Family Violence Prevention Act, 25 U.S.C. §3201, et seq.; <strong>Indian</strong> Employment, Training, and<br />
Related Services Demonstration Act, 25 U.S.C. §3401, et seq.<br />
12 See, e.g., 42 U.S.C. §1395qq (eligibility of IHS/tribal facilities for Medicare payments); 42 U.S.C. §1396j (eligibility of<br />
IHS/tribal facilities for Medicaid payments); 42 U.S.C. §1397bb(b)(3)(D) (assurance of CHIP services to eligible low-income<br />
<strong>Indian</strong> children); Elementary and Secondary Education Act, as amended, 20 U.S.C. §6301, et seq. (funding set-asides<br />
throughout this law for the benefit of children enrolled in the Bureau of <strong>Indian</strong> Affairs school system); Impact Aid Program,<br />
20 U.S.C. §7701, et seq. (federal aid to public school districts for <strong>Indian</strong> children living on <strong>Indian</strong> lands); Carl D. Perkins<br />
Vocational and Applied Technology Education Act, 20 U.S.C. §§2326 and 2327 (funding set-aside for <strong>Indian</strong> vocational<br />
education programs and tribal vocational Institutions); Higher Education Act, 20 U.S.C. §1059c (funding for triballycontrolled<br />
higher education institutions); Individuals with Disabilities Education Act, 20 U.S.C. §1411(c) (funding set-aside<br />
for Bureau of <strong>Indian</strong> Affairs schools); Head Start Act, 42 U.S.C. §9801, et seq. (includes funding allocation for <strong>Indian</strong> tribal<br />
programs and special criteria for program eligibility); Federal Highway Act, 23 U.S.C. §101, et seq. (1998, 2005, 2008 and<br />
2012 amendments include funding set-asides for <strong>Indian</strong> reservation roads programs and direct development of regulations<br />
through Negotiated Rulemaking with tribes); American Recovery and Reinvestment Act of 2009, P.L. 111-5 (Feb. 17, 2009)<br />
(§5006 making amendments to the Social Security Act to provide various protections for <strong>Indian</strong>s under Medicaid and CHIP,<br />
discussed below); Patient Protection and Affordable Care Act, P.L. 111-148 (Mar. 23, 2010) (various <strong>Indian</strong> specific<br />
provisions, discussed below).<br />
13 25 U.S.C. §461, et seq. The <strong>Indian</strong> hiring preference appears at 25 U.S.C. §472.<br />
43
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
While the Supreme Court’s civil rights jurisprudence has generally applied strict scrutiny when<br />
reviewing classifications based on race, color, or national origin, 14 in Mancari the Court determined<br />
that this test was not appropriate when reviewing an <strong>Indian</strong> employment preference law. Indeed, the<br />
Court declared that the practice under review was not even a “racial” preference. Rather, in view of<br />
the unique historic and political relationship between the United States and <strong>Indian</strong> Tribes, the Court<br />
characterized the preference law as political rather than racial, and said that “[a]s long as the special<br />
treatment [for <strong>Indian</strong>s] can be tied rationally to the fulfillment of Congress’ unique obligation toward<br />
the <strong>Indian</strong>s, such legislative judgments will not be disturbed.” Id. At 555. The Court found that hiring<br />
preferences in the federal government’s <strong>Indian</strong> service were intended “to further the Government’s<br />
trust obligation toward the <strong>Indian</strong> tribes,” to provide greater participation in their own selfgovernment,<br />
and “to reduce the negative effect of having non-<strong>Indian</strong>s administer matters that affect<br />
<strong>Indian</strong> tribal life” in agencies, such as the BIA, which administer federal programs for <strong>Indian</strong>s. Id. At<br />
541-542 (emphasis added). 15<br />
Once the link between special treatment for <strong>Indian</strong>s as a political class and the federal government’s<br />
unique obligation to <strong>Indian</strong>s is established, “ordinary rational basis scrutiny applies to <strong>Indian</strong><br />
classifications just as it does to other non-suspect classifications under equal protection analysis.”<br />
Narragansett <strong>Indian</strong> Tribe v. <strong>National</strong> <strong>Indian</strong> Gaming Comm’n., 158 F.3d 1335, 1340 (D.C. Cir. 1998).<br />
The <strong>Indian</strong> hiring preference sanctioned by the Court in Mancari is only one of the many activities the<br />
Court has held are rationally related to the United States’ unique obligation toward <strong>Indian</strong>s. The Court<br />
14 The Supreme Court has interpreted Title VI to allow racial and ethnic classifications only if those classifications are<br />
permissible under the Equal Protection Clause. Regents of Univ. of Cal. v. Bakke, 438 U.S. 265, 287 (1978). In this regard,<br />
the Court has also stated that "all racial classifications, imposed by whatever federal, state, or local governmental actor,<br />
must be analyzed by a reviewing court under strict scrutiny. In other words, such classifications are constitutional only if<br />
they are narrowly tailored measures that further compelling governmental Interests." Adarand Constructors, Inc. v. Pena,<br />
515 U.S. 200, 227 (1995).<br />
15<br />
<strong>Indian</strong> Preference provisions are not limited to the BIA, and have been applied in a variety of federal programs for the<br />
benefit of <strong>Indian</strong>s. Section 7 of the <strong>Indian</strong> Self Determination Act, for example, establishes a broad federal policy of<br />
providing hiring, training, and contracting preferences for <strong>Indian</strong>s in contracts or grants with <strong>Indian</strong> organizations across all<br />
federal agencies. 25 U.S.C. § 450e(b). <strong>Indian</strong> preference provisions are also found in other statutes. See, e.g., 42 U.S.C. §<br />
9839(h) (establishing an <strong>Indian</strong> hiring preference at American <strong>Indian</strong> Programs Branch of Head Start Bureau); 20 U.S.C. §<br />
3423c(c) (establishing an <strong>Indian</strong> employment preference in the Office of <strong>Indian</strong> Education in the Department of Education).<br />
See also Preston v. Heckler, 734 F.2d 1359 (9th Cir. 1984) (<strong>Indian</strong> Preference Act requires Secretary of HHS to adopt<br />
standards for evaluating qualifications of <strong>Indian</strong>s for employment in the <strong>Indian</strong> <strong>Health</strong> Service that are separate and<br />
independent from general civil service standards).<br />
44
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
has upheld a number of other activities singling out <strong>Indian</strong>s for special or preferential treatment, e.g.,<br />
the right of for-profit <strong>Indian</strong> businesses to be exempt from state taxation, Moe v. Confederated Salish<br />
& Kootenai Tribes, 425 U.S. 463, 479-80 (1976); fishing rights, Washington v. Washington State<br />
Commercial Passenger Fishing Vessel Ass’n, 443 U.S. 658, 673 n.20 (1979); and the authority to apply<br />
federal law instead of state law to <strong>Indian</strong>s charged with on-reservation crimes, United States v.<br />
Antelope, 430 U.S. 641, 645-47 (1977). The Court in Antelope explained its decisions in the following<br />
way:<br />
The decisions of this Court leave no doubt that federal legislation with<br />
respect to <strong>Indian</strong> tribes, although relating to <strong>Indian</strong>s as such, is not based<br />
upon impermissible racial classifications. Quite the contrary,<br />
classifications singling out <strong>Indian</strong> tribes as subjects of legislation are<br />
expressly provided for in the Constitution and supported by the ensuing<br />
history of the Federal Government’s relations with <strong>Indian</strong>s.<br />
Antelope, 430 U.S. at 645 (emphasis added).<br />
The courts continue to acknowledge the special political status of <strong>Indian</strong>s and to uphold legislation<br />
singling out <strong>Indian</strong>s on that basis. See, e.g., Am. Fed’n of Gov’t Employees, AFL-CIO v. United States,<br />
330 F.3d 513, 522-23 (D.C. Cir. 2003) (finding outsourcing preference for <strong>Indian</strong>-owned firms was<br />
rationally related to the legitimate legislative purpose of promoting the economic development of<br />
federally recognized Tribes and their members); United States v. Wilgus, 638 F.3d 1274, 1287-88 (10 th<br />
Cir. 2011) (upholding exception to the Bald Eagle Protection Act for <strong>Indian</strong> tribal members to possess<br />
eagle feathers).<br />
III. Congress’s Recognition of the Federal Trust Responsibility in <strong>Health</strong> Laws<br />
Since the early part of the 20 th century, Congress has enacted a number of laws that authorize, direct,<br />
and fund the provision of health care services to <strong>Indian</strong> people. 16 Here we focus on the most<br />
significant legislative enactments intended to ensure access of <strong>Indian</strong> people to federally-assisted<br />
health care programs and to enhance the viability of <strong>Indian</strong> <strong>Health</strong> Service and tribal programs that<br />
serve the <strong>Indian</strong> population.<br />
A. The <strong>Indian</strong> <strong>Health</strong> Care Improvement Act<br />
16 See, e.g., Snyder Act, 25 U.S.C. § 13; Johnson-O'Malley Act, 25 U.S.C. § 452; Transfer Act, 42 U.S.C. § 2001, et seq.<br />
(transferred responsibility for <strong>Indian</strong> health to Public <strong>Health</strong> Service); annual appropriations to the <strong>Indian</strong> <strong>Health</strong> Service<br />
included in the Interior and Related Agencies Appropriations Acts.<br />
45
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
The <strong>Indian</strong> <strong>Health</strong> Care Improvement Act (IHCIA) 17 was originally enacted in 1976 as Public Law 94-437.<br />
It brought statutory order and direction to the delivery of federal health services to <strong>Indian</strong> people. Its<br />
legislative history catalogued the deplorable conditions of <strong>Indian</strong> health that demanded legislative<br />
attention: inadequate and under-staffed health facilities; improper or non-existent sanitation facilities;<br />
prevalence of disease; poor health status; inadequate funding; 18 low enrollment of <strong>Indian</strong>s in<br />
Medicare, Medicaid, and Social Security; serious shortage of health professionals, including <strong>Indian</strong><br />
health professionals; and the need for health care for <strong>Indian</strong> people who had moved from reservations<br />
to urban areas. The legislation addressed each of these deficiencies through focused titles: Manpower;<br />
<strong>Health</strong> Services; <strong>Health</strong> Facilities (including sanitation facilities); Access to Medicare and Medicaid;<br />
Urban <strong>Indian</strong> <strong>Health</strong>; and a feasibility study for establishing an American <strong>Indian</strong> School of Medicine. 19<br />
The IHCIA has been periodically reauthorized and amended since 1976. In 2010, the law was<br />
comprehensively amended and authorized as a permanent law of the United States. 20<br />
Throughout its history, the IHCIA has contained an unequivocal recognition of the United States’<br />
responsibility to improve the health of <strong>Indian</strong> people, to provide federal health services to this<br />
population, and to foster maximum <strong>Indian</strong> participation in health care program management. The<br />
2010 amendments reiterated and reinforced these federal commitments through the following<br />
provisions:<br />
Congressional Findings<br />
The Congress finds the following:<br />
(1) Federal health services to maintain and improve the health of the <strong>Indian</strong>s are consonant with and<br />
required by the Federal Government’s historical and unique legal relationship with, and resulting<br />
responsibility to, the American <strong>Indian</strong> people.<br />
(2) A major national goal of the United States is to provide the resources, processes, and structure that will<br />
enable <strong>Indian</strong> tribes and tribal members to obtain the quantity and quality of health care services and<br />
17 25 U.S.C. §1601, et seq. The <strong>Indian</strong> <strong>Health</strong> Care Improvement Act was amended and permanently reauthorized by<br />
Section 10221 of the Patient Protection and Affordable Care Act, P.L. 111-148 (Mar. 23, 2010).<br />
18 The House Interior and Insular Affairs Committee noted that per capita spending on <strong>Indian</strong> health in 1976 was 25<br />
percent less than the average American per capita amount. H.R. REP. No. 94-1026, pt. I, at 16 (1976), reprinted in 1976<br />
U.S.C.C.A.N. 2652, 2655. According to the U.S. Commission on Civil Rights, IHS per capita spending for <strong>Indian</strong> medical care<br />
in 2003 was 62 percent lower than the U.S. per capita amount. U.S. Commission on Civil Rights, Broken Promises:<br />
Evaluating the Native American <strong>Health</strong> Care System (Sept. 2004), at 98.<br />
19 The IHCIA was later amended to include formal establishment of the <strong>Indian</strong> <strong>Health</strong> Service as an agency of DHHS. Pub.<br />
L. No. 100-713 (1988). The IHS establishment is codified at 25 U.S.C. § 1661.<br />
20 Sec. 10221 of the Patient Protection and Affordable Care Act, P.L. 111-148 (Mar. 23, 2010).<br />
46
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
opportunities that will eradicate the health disparities between <strong>Indian</strong>s and the general population of the<br />
United States.<br />
(3) A major national goal of the United States is to provide the quantity and quality of health services which<br />
will permit the health status of <strong>Indian</strong>s to be raised to the highest possible level and to encourage the<br />
maximum participation of <strong>Indian</strong>s in the planning and management of those services.<br />
(4) Federal health services to <strong>Indian</strong>s have resulted in a reduction in the prevalence and incidence of<br />
preventable illnesses among, and unnecessary and premature deaths of, <strong>Indian</strong>s.<br />
(5) Despite such services, the unmet health needs of American <strong>Indian</strong> people are severe and the health status<br />
of the <strong>Indian</strong>s is far below that of the general population of the United States. 21<br />
Declaration of <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> Policy<br />
Congress declares that it is the policy of this Nation, in fulfillment of its special trust responsibilities and legal<br />
obligations to <strong>Indian</strong>s –<br />
(1) to ensure the highest possible health status for <strong>Indian</strong>s and urban <strong>Indian</strong>s and to provide all resources<br />
necessary to effect that policy;<br />
(2) to raise the health status of <strong>Indian</strong>s and urban <strong>Indian</strong>s to at least the levels set forth in the goals contained<br />
within the <strong>Health</strong>y People 2010 initiative or successor objectives;<br />
(3) to ensure maximum <strong>Indian</strong> participation in the direction of health care services so as to render the<br />
persons administering such services and the services themselves more responsive to the needs and<br />
desires of <strong>Indian</strong> communities;<br />
(4) to increase the proportion of all degrees in the health professions and allied and associated health<br />
professions awarded to <strong>Indian</strong>s so that the proportion of <strong>Indian</strong> health professions in each Service are is<br />
raised to at least the level of that of the general population;<br />
(5) to require that all actions under this chapter shall be carried out with active and meaningful consultation<br />
with <strong>Indian</strong> tribes and tribal organizations, and conference with urban <strong>Indian</strong> organizations, to implement<br />
this chapter and the national policy of <strong>Indian</strong> self-determination;<br />
(6) to ensure that the United States and <strong>Indian</strong> tribes work in a government-to-government relationship to<br />
ensure quality health care for all tribal members; and<br />
(7) to provide funding for programs and facilities operated by <strong>Indian</strong> tribes and tribal organizations in<br />
amounts that are not less than the amounts provided to programs and facilities operated directly by the<br />
Service. 22<br />
It is important to note that these expressions of policy, obligation, and objectives apply to the federal<br />
government as a whole. The Act reposes responsibility for their implementation in the Secretary of<br />
<strong>Health</strong> and Human Services. While the <strong>Indian</strong> <strong>Health</strong> Service has first-line responsibility for<br />
administering the <strong>Indian</strong> health system, the Secretary of HHS remains the official with ultimate<br />
responsibility to see that programs are performed as directed and the objectives established by<br />
Congress are achieved. Thus, the obligation to exercise the trust responsibility for <strong>Indian</strong> health, to<br />
implement the expressed policies, and to achieve the stated goals extend to the Centers for Medicare<br />
& Medicaid Services, as an agency of HHS.<br />
B. Statutory Authority for Participation in Medicare and Medicaid<br />
21 25 U.S.C. §1601.<br />
22 25 U.S.C. §1602.<br />
47
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
In the 1976 IHCIA, Congress amended the Social Security Act to extend to <strong>Indian</strong> health facilities the<br />
authority to collect Medicare and Medicaid reimbursements. Prior to these amendments, the IHS, as a<br />
federal agency, was not permitted to claim reimbursements from Medicare and Medicaid.<br />
• Sec. 1880 23 made IHS hospitals (including those operated by <strong>Indian</strong> Tribes 24 ) eligible to collect<br />
Medicare reimbursement.<br />
• Sec. 1911 25 made IHS and tribal facilities eligible to collect reimbursements from Medicaid<br />
• An amendment to Sec. 1905(b) 26 applied a 100 percent federal medical assistance percentage<br />
(FMAP) to Medicaid services provided to an <strong>Indian</strong> by an IHS or tribally-operated facility.<br />
Sections 1880 and 1911 were intended to bring additional revenue into the <strong>Indian</strong> health system in<br />
order to address the deplorable condition of <strong>Indian</strong> health facilities, many of which were in such a poor<br />
state they were unable to achieve accreditation. The application of a 100 percent FMAP to the<br />
Medicaid-covered services provided by these facilities was made in express recognition of the federal<br />
government’s treaty obligations for <strong>Indian</strong> health. The Committee of jurisdiction observed that since<br />
the United States already had an obligation to pay for health services to <strong>Indian</strong>s as IHS beneficiaries, it<br />
was appropriate for the U.S. to pay the full cost of their care as Medicaid beneficiaries. 27 This action is<br />
consistent with the status of AI/ANs as a political designation.<br />
Through amendments to Sec. 1880 made in 2000, 2003 and 2010, IHS and tribal hospitals and clinics<br />
are authorized to collect reimbursements for all Medicare Part A and Part B services. As health care<br />
providers, IHS and tribal health programs are authorized to collect reimbursements under Medicare<br />
Parts C and D, as well. 28<br />
23 42 U.S.C. §1395qq.<br />
24 Tribes and tribal organizations are authorized to operate IHS-funded hospitals and clinics through contracts and<br />
compacts issued pursuant to the <strong>Indian</strong> Self-Determination and Education Assistance Act, 25 U.S.C. § 450, et seq.<br />
25 42 U.S.C. §1396j.<br />
26 42 U.S.C. §1396d(b).<br />
27 H.R. REP. No. 94-1026, pt. III, at 21 (1976), as reprinted in 1976 U.S.C.C.A.N. 2782, 2796.<br />
28<br />
In fact, Congress expressly authorized the Secretary of HHS to issue standards to assure access by pharmacies operated<br />
by the IHS, tribes and urban <strong>Indian</strong> organizations to the Medicare Part D prescription drug benefit (42 U.S.C. §1395w-<br />
104(b)(1)(C)(iv)), and required the Secretary to establish procedures (including authority to waive requirements) to assure<br />
participation by these pharmacies in the transitional assistance feature of the temporary discount drug program. 42 U.S.C.<br />
48
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
C. Statutory Authority for Participation in CHIP<br />
IHS and tribal health providers are authorized to collect payments when providing services to<br />
individuals enrolled in the Children’s <strong>Health</strong> Insurance Program (CHIP). 29 To assure that low-income<br />
<strong>Indian</strong> children who are CHIP-eligible are not overlooked, Congress, when creating the program in<br />
1997, expressly required States to describe in their State plans the procedures they will use to assure<br />
access for these children. 30<br />
D. <strong>Indian</strong>-Specific Provisions Designed to Ensure <strong>Indian</strong> Access to Medicaid, Medicare and<br />
CHIP<br />
Since early 2009, Congress has added several significant provisions to Titles XIX and XXI of the Social<br />
Security Act that give voice to the federal government’s unique responsibility to <strong>Indian</strong> people and the<br />
need to remove barriers to their participation in Medicaid and CHIP, especially when AI/ANs eligible for<br />
those programs receive services from <strong>Indian</strong> health providers. We highlight these actions below.<br />
Proof of Citizenship for Medicaid Enrollment. In the Deficit Reduction Act of 2005 (DRA),<br />
Congress directed that on and after July 1, 2006, persons who apply to enroll or renew<br />
enrollment in Medicaid must provide documentary proof of identity and U.S. citizenship, and<br />
identified the types of documents that would be acceptable proof. <strong>Indian</strong> health advocates<br />
feared – correctly, as it turns out – that many AI/ANs would not possess sanctioned<br />
documentation of their status as U.S. citizens. Recognizing the barrier this presented for <strong>Indian</strong><br />
access to Medicaid and CHIP, in 2009 Congress amended these requirements to designate<br />
documents issued by a federally-recognized <strong>Indian</strong> Tribe evidencing an individual’s<br />
membership, enrollment in, or affiliation with such Tribe as satisfactory evidence of U.S.<br />
citizenship. 31 Significantly, Congress gave tribal documentation “tier I” status – the same as a<br />
U.S. passport. Individuals presenting tribal affiliation documentation would not be required to<br />
present any additional identity documentation.<br />
§1395w-141(g)(5)(B). Congress added language in the Affordable Care Act to allow <strong>Indian</strong> patients to qualify for the<br />
catastrophic coverage phase of the Part D program. 42 U.S.C. §1395w–102(b)(4)(C).<br />
29 42 U.S.C. §2105(c)(6)(B); see also 25 U.S.C. §1647a.<br />
30 42 U.S.C. §2103(a)(3)(D).<br />
31 42 U.S.C. §1396b(x)(3)(B), as added by Sec. 211 of the Children’s <strong>Health</strong> Insurance Program Reauthorization Act of 2009<br />
(P.L. 111-3) (Feb. 4, 2009).<br />
49
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
This legislative action recognizes not only the historic reality that <strong>Indian</strong> people were the<br />
original occupants of the North American continent, it also implements in the clearest possible<br />
way the policy of maintaining a government-to-government relationship with <strong>Indian</strong> Tribes. It<br />
also demonstrates respect for the sovereignty of Tribes both to determine tribal membership<br />
and to issue legal documents. As a practical matter, amending the law to order acceptance of<br />
tribal documentation underscores Congress’s recognition of its continued responsibility to<br />
enact <strong>Indian</strong>-specific legislation when needed to assure full access to federal programs.<br />
Medicaid Premium and Cost-Sharing Protections. Pursuant to an amendment to Medicaid<br />
made in 2009, States are prohibited from imposing any premium or cost-sharing on an <strong>Indian</strong><br />
for a covered service provided by the IHS, a health program operated by an <strong>Indian</strong> Tribe, Tribal<br />
Organization or urban <strong>Indian</strong> organization, or through referral under contract health services. 32<br />
Disregard of Certain <strong>Indian</strong> Property from Resources for Medicaid and CHIP Eligibility. In 2009,<br />
Congress amended the Medicaid and CHIP laws to exempt from the resources calculation<br />
certain enumerated types of <strong>Indian</strong> property. Primarily, the excluded property is of a type that<br />
flows to an individual <strong>Indian</strong> by virtue of his/her membership in a Tribe. 33<br />
Medicaid Estate Recovery Protections. In an express endorsement of a provision in the CMS<br />
State Medicaid Manual, in 2009 Congress statutorily exempted certain <strong>Indian</strong>-related income,<br />
resources and property held by a deceased <strong>Indian</strong> from the Medicaid estate recovery<br />
requirement. 34 The objective of the Manual and statutory protection was to remove a<br />
disincentive to enrollment for <strong>Indian</strong> people eligible for Medicaid.<br />
Special <strong>Indian</strong>-specific Rules for Medicaid Managed Care. In 2009, Congress removed several<br />
barriers to full and fair participation of <strong>Indian</strong> people and <strong>Indian</strong> health providers in Medicaid<br />
programs operated through managed care entities. This gave an <strong>Indian</strong> Medicaid enrollee the<br />
option to select an <strong>Indian</strong> health program as his/her primary care provider, and directed that<br />
32 42 U.S.C. §§1396o(j) and 1396o-1(b)(3)(vii), as added by Sec. 5006(a) of the American Recovery and Reinvestment Act<br />
of 2009 (P.L. 111-5) (Feb. 17, 2009). In recognition of the trust responsibility, <strong>Indian</strong> children have been exempt from costsharing<br />
in the CHIP program pursuant to regulation at 42 C.F.R. §457.535.<br />
33 42 U.S.C. §§1396a(ff) and 1397gg(e)(1)(H), as added by Sec. 5006(b) of the American Recovery and Reinvestment Act of<br />
2009 (P.L. 111-5) (Feb. 17, 2009).<br />
34 42 U.S.C. §1396p(b)(3)(B), as added by Sec. 5006(c) of the American Recovery and Reinvestment Act of 2009 (P.L. 111-5)<br />
(Feb. 17, 2009).<br />
50
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
<strong>Indian</strong> health providers (IHS, tribal, and urban <strong>Indian</strong> organization programs) be paid at a rate<br />
not less than that of the managed care entity’s network provider. 35 These changes were<br />
needed to overcome the reluctance of managed care entities to admit <strong>Indian</strong> health providers<br />
to their networks and to reimburse them for services provided to <strong>Indian</strong> Medicaid enrollees.<br />
Authority for Tribal Medicaid Administrative Match. Federal funds may not be used to meet<br />
State matching requirements, except as authorized by Federal law. In 2005, CMS issued a State<br />
Medicaid Director letter that permits <strong>Indian</strong> Tribes and Tribal Organizations to certify funds<br />
received under the <strong>Indian</strong> Self-Determination and Education Assistance Act as public<br />
expenditures to be used as the non-Federal share of expenditures to fulfill State matching<br />
requirements for administrative claiming activities under the Medicaid program. These<br />
activities include, among other things, outreach and application assistance for Medicaid<br />
enrollment and activities that ensure appropriate utilization of Medicaid services by Medicaid<br />
beneficiaries.<br />
E. Solicitation of Input from <strong>Indian</strong> <strong>Health</strong> Programs.<br />
In recognition of the need to assure that impacts on the unique <strong>Indian</strong> health system by proposed<br />
changes in Medicare, Medicaid, and CHIP are fully evaluated, Congress placed in the Social Security Act<br />
a requirement for prior notice to and solicitation of input from IHS, tribal health programs, and urban<br />
<strong>Indian</strong> organizations. On the federal level, this requirement is to be carried out by CMS through<br />
maintenance of the Tribal Technical Advisory Group originally chartered by the agency in 2003. 36<br />
States are required to solicit advice from IHS and tribal health programs and urban <strong>Indian</strong> organizations<br />
within their borders prior to submission of any state plan amendments, waiver requests, and<br />
demonstration projects to CMS. 37<br />
35 42 U.S.C. §1396u-2(h), as added by Sec. 5006(d) of the American Recovery and Reinvestment Act (P.L. 111-5) (Feb. 17,<br />
2009).<br />
36 42 U.S.C. §1320b-24, as added by Sec. 5006(e)(1) of the American Recovery and Reinvestment Act (P.L. 111-5) (Feb. 17,<br />
2009). The maintenance of the Tribal Technical Advisory Group does not substitute for government-to-government<br />
consultation with tribes.<br />
37 42 U.S.C. §§1396a(a)(73) and 1397gg(e)(1)(C), as added by Sec. 5006(e)(2) of the American Recovery and Reinvestment<br />
Act (P.L. 111-5) (Feb. 17, 2009).<br />
51
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
F. Cap on Rates Charged for Contract <strong>Health</strong> Services.<br />
Modeling on the Medicare Provider Agreement provision that caps the amount a hospital can charge<br />
for services purchased by the Department of Veterans Affairs, in 2003 Congress enacted a similar<br />
limitation on the amount a Medicare participating hospital may charge for services purchased by<br />
<strong>Indian</strong> health programs operated by the IHS, Tribes, and Tribal Organizations, and urban <strong>Indian</strong><br />
organizations (I/T/Us). As a condition for participation in Medicare, such hospitals must accept<br />
patients referred by I/T/Us in accordance with the admission practices, payment methodology, and<br />
payment rates set forth in Secretarial regulations, and may accept no more than the payment rates set<br />
by the Secretary. 38 This statutory rate cap is often referred to by the shorthand “Medicare-like rates.”<br />
In regulations issued by IHS and CMS in 2007, the maximum amount a Medicare hospital is permitted<br />
to accept for a service purchased by an I/T/U is the applicable Medicare rate. 39<br />
These statutory and regulatory actions are intended to enable I/T/Us to achieve greater economies for<br />
the services they must purchase for their <strong>Indian</strong> patients with funds appropriated for contract health<br />
services.<br />
G. <strong>Indian</strong>-Specific Provisions Designed to Ensure <strong>Indian</strong> Access to the <strong>Health</strong> Insurance<br />
Exchanges<br />
The Patient Protection and Affordable Care Act (ACA) was enacted by Congress in 2010 in order to<br />
reform the health insurance market and make health insurance more accessible and affordable for all<br />
Americans. It imposes a responsibility on most Americans to acquire or maintain health insurance<br />
coverage, and contains a number of provisions intended to strengthen health insurance consumer<br />
protections and enhance the health care workforce. Congress included a number of provisions<br />
designed to ensure that <strong>Indian</strong>s could take advantage of the new reforms. We highlight several of<br />
these below.<br />
Exemption from Penalty for Failure to Comply with the Individual Mandate. Although Congress<br />
designed the law to make nearly all Americans responsible for acquiring or maintaining<br />
acceptable levels of health insurance coverage, Congress specifically exempted members of<br />
<strong>Indian</strong> Tribes from the tax penalty for failure to obtain acceptable coverage. 40 This provision is<br />
38 42 U.S.C. §1395cc(a)(1)(U), as added by the Medicare Modernization Act of 2003 (P.L. 108-173).<br />
39 72 Fed. Reg. 30706 (June 4, 2007), adding Subpt. D to 42 C.F.R. Part 136, and adding §489.29 to 42 C.F.R. Part 489.<br />
These regulations became effective on July 5, 2007.<br />
40 26 U.S.C. §5000A(e)(3).<br />
52
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
based on the theory that the United States is responsible for providing health care to <strong>Indian</strong>s,<br />
but it has failed to supply an acceptable package of benefits through the <strong>Indian</strong> <strong>Health</strong> Service.<br />
Having failed in that responsibility, it would violate the trust responsibility to require <strong>Indian</strong>s to<br />
pay for non-IHS coverage or be assessed a tax penalty for failing to do so.<br />
Cost-Sharing Protections for <strong>Indian</strong>s Enrolled in a <strong>Health</strong> Insurance Exchange Plan. The<br />
Affordable Care Act prohibits assessment of any cost-sharing for any service provided by an<br />
<strong>Indian</strong> health provider to an AI/AN enrolled in an Exchange plan. Furthermore, no cost sharing<br />
may be assessed by non-<strong>Indian</strong> health providers to an AI/AN enrolled in such a plan if the<br />
individual receives services through an <strong>Indian</strong> health provider or through contract health<br />
services. <strong>Indian</strong>s with income below 300 percent of the Federal Poverty Level do not have cost<br />
sharing in the private sector even if they do not have a referral from an <strong>Indian</strong> health provider.<br />
The Secretary of HHS is responsible for paying the Exchange plan the additional actuarial cost<br />
that results from these cost-sharing protections. 41<br />
Special enrollment periods for AI/AN. The ACA provides special enrollment periods for AI/ANs<br />
for health insurance exchanges. This is another measure to provide access to this important<br />
source of funding for the I/T/U.<br />
These provisions are designed to reduce the costs for AI/ANs to access the Exchange plans and to<br />
provide incentives for them to do so, as well as to increase the likelihood that I/T/Us will receive<br />
payments from health insurance exchange plans for services they provide to AI/Ans.<br />
IV. Executive Branch Recognition of the Federal Trust Responsibility in Administering Federal<br />
<strong>Health</strong> Programs<br />
A. Executive Branch Administration of the Trust Responsibility<br />
The Executive Branch is responsible for carrying out the federal trust responsibility to provide health<br />
care to <strong>Indian</strong>s. The federal government’s general trust duty to provide social services and its duty as a<br />
trustee to protect and manage <strong>Indian</strong> trust property are different types of duties and thus are treated<br />
differently by the courts. 42 Courts have generally been reluctant to impose liability for the federal<br />
government’s failure to provide social services under the general trust relationship. 43 One notable<br />
41 42 U.S.C. §18071(d).<br />
42 Seminole Nation v. United States, 316 U.S. 286, 297 (1942).<br />
43 See, e.g., Gila River Pima-Maricopa <strong>Indian</strong> Community v. U.S., 427 F.2d 1194 (Ct.CI. 1970), cert. denied. 400 U.S. 819<br />
(1970).<br />
53
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
exception is the case of Morton v. Ruiz 44 where the Supreme Court said the Bureau of <strong>Indian</strong> Affairs<br />
erred in refusing to provide welfare benefits to unemployed <strong>Indian</strong>s who lived off, but near, their<br />
reservation. The Court reiterated that the “overriding duty of our Federal Government [is] to deal<br />
fairly with <strong>Indian</strong>s wherever located”, and that BIA’s failure to publish eligibility criteria through<br />
Administrative Procedure Act regulations was not consistent with the “distinctive obligation of trust<br />
incumbent upon the Government in its dealings” with <strong>Indian</strong>s. 45<br />
The IHCIA policy statements quoted above expressly recognize a trust responsibility to maintain and<br />
improve the health of <strong>Indian</strong>s, and establish a national policy to assure the highest possible health<br />
status to <strong>Indian</strong>s, as well as to provide all resources necessary to effect that policy. While currently<br />
there may be no available mechanism to enforce these policies judicially, this does not make them<br />
meaningless. They establish the goals, which the Executive Branch – particularly the Department of<br />
<strong>Health</strong> and Human Services – must strive to achieve as it implements federal law. In fact, they justify –<br />
indeed, require – the Executive Branch to be proactive and use its resources “to assure the highest<br />
possible health status for <strong>Indian</strong>s and urban <strong>Indian</strong>s and to provide all resources necessary to effect<br />
that policy.” 25 U.S.C. §1602(1). The Executive Branch has a dual duty – to carry out the policy<br />
established by Congress in federal law, and to perform the United States’ trust responsibility to <strong>Indian</strong>s<br />
in accord with the Congressionally-established standard.<br />
<strong>Indian</strong> people take the United States at its word when reading the policy statement in the IHCIA, and<br />
have a right to expect its trustee to achieve the goal of assuring them the highest possible health<br />
status. As stated by Justice Black in his lament over the U.S. breaking faith with <strong>Indian</strong>s, “Great<br />
nations, like great men, should keep their word.” 46<br />
B. CMS Administration of the Trust Responsibility<br />
As part of DHHS, and as an agency required to implement statutory provisions intended to benefit<br />
<strong>Indian</strong> health, CMS should affirmatively advance policy objectives as set out by Congress in the IHCIA<br />
when making <strong>Indian</strong>-related decisions in the Medicare and Medicaid programs. The trust responsibility<br />
and the federal laws enacted to carry it out not only permit CMS to treat AI/ANs served by the <strong>Indian</strong><br />
44 415 U.S. 199 (1974).<br />
45 Id. at 236. See also Chambers, note 2, supra, at 1245-46 (arguing that courts should apply the trust responsibility as a<br />
"fairness doctrine" in suits against the United States for breach of a duty to provide social services).<br />
46 Federal Power Comm'n v. Tuscarora <strong>Indian</strong> Nation, 362 U.S. 99, 142 (1960) (Black, J., dissenting),<br />
54
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
health system as unique Medicare and Medicaid consumers entitled to special treatment, they require<br />
it.<br />
CMS shares the responsibility to carry out the policy goals established by Congress in the IHCIA. Both<br />
the HHS and CMS tribal consultation policies recognize “the unique government to government”<br />
relationship between the United States and Tribes, as well as the trust responsibility “defined and<br />
established” by “the U.S. Constitution, numerous treaties, statutes, Federal case law, regulations, and<br />
executive orders.” 47 One manifestation of this trust responsibility is CMS’s recognition that “CMS and<br />
<strong>Indian</strong> Tribes share the goals of eliminating health disparities for American <strong>Indian</strong>s and Alaska Natives<br />
(AI/AN) and of ensuring that access to Medicare, Medicaid, the Children’s <strong>Health</strong> Insurance Program<br />
(CHIP), and Exchanges is maximized.” 48 Through its consultation policy, CMS has committed to<br />
consulting with <strong>Indian</strong> Tribes when developing policy that may affect <strong>Indian</strong>s.<br />
CMS has exercised its authority to administer federal health care programs and interpret the statutes<br />
within its jurisdiction in a manner that assures access by <strong>Indian</strong> people and participation by the unique<br />
<strong>Indian</strong> health delivery system. In recent decades, CMS (previously HCFA) has taken steps to carry out<br />
the trust responsibility to <strong>Indian</strong>s in its administration of the Medicare, Medicaid, and CHIP programs.<br />
Each was a rational exercise of the agency’s authority and fully justified by the United States’ special<br />
obligations to <strong>Indian</strong> Tribes.<br />
A summary of these actions follows:<br />
Authority for Tribal Facilities to Bill Medicaid at the Same Rate as IHS Facilities. In 1996,<br />
through a Memorandum of Agreement with IHS, HCFA re-interpreted the term “facility of the<br />
<strong>Indian</strong> <strong>Health</strong> Service” in Section 1911 (Medicaid) to allow a tribally-owned facility operated<br />
under an ISDEAA agreement to elect designation as a “facility of the <strong>Indian</strong> <strong>Health</strong> Service.”<br />
Previously, HCFA had interpreted the term “facility of the <strong>Indian</strong> <strong>Health</strong> Service” to include only<br />
facilities actually owned or leased by IHS. The MOA enabled these tribally-owned facilities to<br />
bill Medicaid at the annually-established Medicaid billing rates for IHS facilities and applied the<br />
100 percent FMAP to Medicaid services provided by such facilities.<br />
Exemption of IHS and Tribal Clinics from the Outpatient Prospective Payment System. In 2002,<br />
the Director of the Center for Medicare agreed to continue the exemption of IHS and tribal<br />
clinics from the Outpatient Prospective Payment System.<br />
47 Centers for Medicare & Medicaid Services Tribal Consultation Policy (Nov. 17, 2011), at 1; U.S. Dep't of <strong>Health</strong> and<br />
Human Services Tribal Consultation Policy (Dec. 14, 2010), at 1.<br />
48 Centers for Medicare & Medicaid Services Tribal Consultation Policy (Nov. 17, 2011), at 2.<br />
55
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
CMS has Broadly Defined the Hospital Services that are Subject to the Medicare-like Rates Cap.<br />
In 2007, CMS issued regulations implementing Section 506 of the Medicare Modernization Act<br />
to require all Medicare-participating hospitals to accept Medicare-like rates when providing<br />
services to I/T/U beneficiaries. The final regulations broadly defined hospital and critical access<br />
hospital services subject to the rule to include inpatient, outpatient, skilled nursing facilities,<br />
and any other service or component of a hospital. 42 C.F.R. §136.30; 42 C.F.R. §489.29.<br />
IHS and Tribal Facility Participation in Medicaid. The 1996 IHS/HCFA MOA incorporated the<br />
regulatory policy that states must accept as Medicaid providers IHS facilities that meet state<br />
requirements, but these facilities are not required to obtain a state license. 42 C.F.R. §431.110.<br />
Thus, it applied this regulatory policy to tribally-owned facilities. Congress converted this policy<br />
into law for all federally-funded health programs serving AI/AN in the 2010 amendments to the<br />
<strong>Indian</strong> <strong>Health</strong> Care Improvement Act. 49<br />
Cost-Sharing Protections for <strong>Indian</strong> Children in CHIP. In 1999, HCFA issued guidance, followed<br />
by a proposed rule, that prohibits states from imposing any cost-sharing on AI/AN children<br />
under CHIP, citing the unique federal relationship with <strong>Indian</strong> Tribes. This rule was<br />
subsequently promulgated in final form. 42 C.F.R. §457.535. This HCFA regulation reflects the<br />
agency’s interpretation of how best to carry out the statutory provision requiring states to<br />
demonstrate how they will assure CHIP access for eligible <strong>Indian</strong> children. 42 U.S.C.<br />
§1397bb(b)(3)(D). In 2000, HCFA announced that the policy prohibiting cost sharing for <strong>Indian</strong><br />
children under CHIP would be extended to Section 1115 Medicaid demonstration projects and<br />
stated the agency would no longer approve Section 1115 projects that impose such costsharing.<br />
66 Fed. Reg. 2490, 2526 (Jan. 11, 2001).<br />
State-Tribal Consultation on Medicaid Programs. In 2001, CMS issued a policy statement that<br />
requires states to consult with Tribes within their borders on Medicaid waiver proposals and<br />
waiver renewals before submitting them to CMS. 50 Congress subsequently made this<br />
consultation requirement statutory, adding State Plan Amendments and demonstration<br />
49 25 U.S.C. §1647a.<br />
50 Letter from <strong>Health</strong> Care Fin. Admin. To State Medicaid Directors (July 17, 2001)<br />
http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/smd071701.pdf.<br />
56
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
projects as requisite subjects of tribal consultation. 51 CMS informed the States of this<br />
consultation requirement on several occasions and codified the 2001 policy statement. 52 In<br />
May of 2012, CMS announced that it would not accept the waiver applications submitted by<br />
New Mexico and Kansas until they met the tribal consultation requirements.<br />
CMS Tribal Technical Advisory Group. In 2003, CMS chartered a Tribal Technical Advisory Group<br />
comprised of tribal officials and tribal employees to advise the agency on Medicare, Medicaid,<br />
and CHIP issues that impact <strong>Indian</strong> health programs. CMS’s foresight was met with approval by<br />
Congress, which granted the TTAG explicit statutory status in 2009 and added representatives<br />
of the IHS and urban <strong>Indian</strong> organizations to the TTAG’s membership. 42 U.S.C. §1320b-24.<br />
<strong>Indian</strong> <strong>Health</strong> Addendum Required for Medicare Part D Pharmacy Contracts. When<br />
implementing the Medicare Part D drug benefit, CMS recognized that special terms and<br />
conditions in pharmacy contracts would be needed to assure that IHS, tribal, and urban <strong>Indian</strong><br />
organization pharmacies would be able to participate in the Part D program. The agency<br />
requires Part D plans to include the CMS-approved text of an <strong>Indian</strong> <strong>Health</strong> addendum in<br />
contracts offered to those pharmacies. 42 C.F.R. §423.120(a)(6). The addendum addresses<br />
several aspects of federal law and regulations applicable to those pharmacies, such as Federal<br />
Tort Claims Act coverage (obviating the need for privately-purchased professional liability<br />
insurance). 53<br />
Approval of <strong>Indian</strong>-specific State Medicaid Plan Provision. In April of 2012, CMS approved an<br />
Arizona Medicaid waiver request through which several optional Medicaid services can<br />
continue to be covered at IHS and tribal facilities, although they are otherwise discontinued<br />
from coverage in the State’s plan. When these services are provided to <strong>Indian</strong> patients at IHS<br />
and tribal facilities, the 100 percent FMAP continues to apply. This action is a significant<br />
acknowledgement by CMS that it has the authority and the obligation to carry out its trust<br />
responsibility for <strong>Indian</strong> health.<br />
51 42 U.S.C. §§1396a(a)(73) and 1397gg(e)(1)(C), as added by Sec. 5006(e)(2) of the American Recovery and Reinvestment<br />
Act (P.L. 111-5) (Feb. 17, 2009).<br />
52 CMS SMD #09-003 (June 17, 2009); CMS SMDL #10-001 (Jan. 22, 2010); 77 Fed. Reg. 11678 (Feb. 27, 2012).<br />
53<br />
The text of the Addendum is included in the Medicare program's solicitation for applications for new cost plan<br />
sponsors. See, e.g., "Medicare Prescription Drug Benefit, Solicitation for Applications for New Cost Plan Sponsors, 2012<br />
Contract Year," at 131.<br />
57
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Carrying out the trust responsibility to <strong>Indian</strong>s in these and other ways coincides with and compliments<br />
CMS’s stated program objectives.<br />
V. The Unique Nature of the <strong>Indian</strong> <strong>Health</strong> System<br />
The IHS-funded system for providing health services to AI/ANs is one-of-a kind; it is unlike any other<br />
mainstream health delivery system. In fact, the federal government created and designed the system<br />
in use today for the specific purpose of serving <strong>Indian</strong> people in the communities in which they live.<br />
Overall, the <strong>Indian</strong> health programs have a community-based approach and seek to provide culturallyappropriate<br />
services. As demonstrated in this Plan, the IHS system was created for <strong>Indian</strong> people as a<br />
political class, not as a racial group. These circumstances require unique rules and policies from CMS<br />
to enable IHS-funded programs to fully access Medicare, Medicaid, and CHIP and to achieve the<br />
agency’s health disparities elimination objective.<br />
We outline below some of the unique circumstances of this health system and of <strong>Indian</strong> Tribes that<br />
have been established or recognized by federal law and regulations:<br />
Limited service population. The IHS health care system is not open to the public. It is<br />
established to serve AI/AN beneficiaries who fall within the eligibility criteria established by the<br />
IHS. See 42 C.F.R. §136.12. 54 The IHS estimates the service population served by IHS and<br />
tribally-operated programs in more than 30 states is approximately 2.1 million AI/Ans.<br />
No cost assessed to patients. IHS serves AI/AN beneficiaries without cost. For several years,<br />
Congress reinforced this policy with language in the annual IHS appropriations act that<br />
prohibited the agency to charge for services without Congressional consent. 55 IHS services at<br />
no cost to the <strong>Indian</strong> patient remains IHS policy today. Some members of Congress have<br />
described the IHS as a pre-paid health plan – pre-paid with land ceded by Tribes to the U.S.<br />
government.<br />
54 Under certain circumstances non-<strong>Indian</strong>s connected with an <strong>Indian</strong> beneficiary (such as minor children and spouses)<br />
can receive services as beneficiaries. Other non-<strong>Indian</strong>s may receive services in carefully defined circumstances, but are<br />
liable for payment. See 25 U.S.C. §1680c.<br />
55 See, e.g., Pub. L. No. 104-134, 110 Stat. 1321-190 (April 26, 1996).<br />
58
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
<strong>Indian</strong> preference in employment. <strong>Indian</strong> preference in hiring applies to the <strong>Indian</strong> <strong>Health</strong><br />
Service. 42 C.F.R. §136.41-.43. 56 Such preference also applies to tribally-operated programs<br />
through the requirement that, to the greatest extent feasible, preference for training and<br />
employment must be given to <strong>Indian</strong>s in connection with administration of any contract or<br />
grant authorized by any federal law to <strong>Indian</strong> organizations or for the benefit of <strong>Indian</strong>s. 25<br />
U.S.C. §450e(b).<br />
Only Tribes have rights under ISDEAA. <strong>Indian</strong> Tribes (and Tribal Organizations sanctioned by<br />
one/more Tribes) – and only those entities – can elect to directly operate an IHS-funded<br />
program through a contract or compact from the <strong>Indian</strong> <strong>Health</strong> Service issued pursuant to the<br />
<strong>Indian</strong> Self-Determination and Education Assistance Act (ISDEAA). 25 U.S.C. §450 et seq. The<br />
tribal operator receives the program funds the IHS would have used and additional funding for<br />
administrative costs. A tribal operator directly hires its staff and has the authority to re-design<br />
the program(s) it offers.<br />
Federal Tort Claims Act coverage. Pursuant to federal law, tribal health programs and their<br />
employees are covered by the Federal Tort Claims Act (FTCA). 25 U.S.C. §450f, note. For this<br />
reason, it is often unnecessary for Tribes to purchase liability insurance for the health services<br />
they operate with federal funding.<br />
Use of HHS personnel. To help staff their programs, Tribes and Tribal Organizations are<br />
authorized by law to utilize employees of HHS under Intergovernmental Personnel Act<br />
assignments and commissioned officers of HHS under Memoranda of Agreement. 25 U.S.C,<br />
§450i.<br />
Creation of specific health care providers. Federal law has created health care delivery<br />
providers found only in the <strong>Indian</strong> health care system. See Community <strong>Health</strong> Representative<br />
Program, 25 U.S.C. §1616; Community <strong>Health</strong> Aide Program (CHAP) for Alaska, 25 U.S.C. §1616l.<br />
The Alaska Medicaid Plan reimburses <strong>Indian</strong> health programs for covered services provided by<br />
CHAPs in Alaska. Through a 2010 amendment to the IHCIA, the Secretary is authorized to<br />
implement a CHAP program for Tribes in the lower 48 states.<br />
56 See also Preston v. Heckler, 734 F.2d 1359 (9th Cir. 1984) (upholding the <strong>Indian</strong> <strong>Health</strong> Service's <strong>Indian</strong> employment<br />
preference).<br />
59
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
IHS as payer of last resort. A longstanding IHS regulation makes IHS programs the payer of last<br />
resort for eligible <strong>Indian</strong> beneficiaries, notwithstanding any state or local law to the contrary.<br />
42 C.F.R. §136.61. Congress has made this payer of last resort status a statutory requirement<br />
for IHS, tribal, and urban <strong>Indian</strong> organization programs. 57<br />
IHS-specific Medicare and Medicaid reimbursement rates. On an annual basis, the IHS (in<br />
consultation with CMS) establishes the rates at which Medicare outpatient and Medicaid<br />
inpatient and outpatient services provided to eligible <strong>Indian</strong>s shall be reimbursed to IHS<br />
facilities. See, e.g.,77 Fed. Reg. 33470 (June 6, 2012). This is an all-inclusive encounter rate<br />
which is unique to <strong>Indian</strong> health care. Tribal clinics may instead elect to bill for services as a<br />
Federally Qualified <strong>Health</strong> Center (FQHC).<br />
100 Percent Federal Medical Assistance Percentage. The cost of Medicaid covered services<br />
provided to AI/ANs in IHS and tribal facilities are reimbursed to the States at 100 percent FMAP<br />
in recognition that the responsibility for <strong>Indian</strong> health care is a federal obligation. Sec. 1905(b)<br />
of SSA; 42 U.S.C. §1396d(b).<br />
No U.S. right of recovery from Tribes. If an <strong>Indian</strong> Tribe (or a Tribal Organization sanctioned by<br />
one/more Tribes) has a self-insured health plan for its employees, the United States is<br />
prohibited by law from recovering from that plan the cost of services provided unless the<br />
sponsoring Tribe/Tribal Organization expressly authorizes such recovery. 25 U.S.C. §1621e(f).<br />
<strong>Indian</strong> Tribes are governments. Upon achieving federal recognition, an <strong>Indian</strong> Tribe is<br />
acknowledged to be and is treated as a government by the United States. The U.S. deals with<br />
<strong>Indian</strong> Tribes on a government-to-government basis that is recognized in Executive Orders and<br />
consultation policies adopted by federal agencies. 58 <strong>Indian</strong> Tribes determine their own<br />
governmental structure. They are not required to follow the U.S. model of separate legislative,<br />
executive, and judicial branches.<br />
57 25 U.S.C. §1623(b), as added by Sec. 2901(b) of the Affordable Care Act (P.L. 111-148) (Mar. 23, 2010).<br />
58<br />
See, e.g., Exec. Order No. 13175, "Consultation and Coordination with <strong>Indian</strong> Tribal Governments (Nov. 9, 2000) (issued<br />
by President Clinton and subsequently endorsed by Presidents George W. Bush and Barack Obama); White House<br />
Memorandum for Heads of Executive Departments and Agencies, Nov. 5, 2009 (President Obama endorsement); Dep't of<br />
<strong>Health</strong> and Human Services Tribal Consultation Policy (Dec. 14, 2010); Centers for Medicare and Medicaid Services Tribal<br />
Consultation Policy (Nov. 17, 2011).<br />
60
Draft Report: Currently being circulated for Tribal leader and health director review and<br />
comment. Please provide comments by October 30, 2012 to Liz Heintzman at the<br />
<strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
State law does not apply. By virtue of the Supremacy Clause, state laws generally do not apply<br />
to the IHS system. 59 The Supreme Court has recognized that <strong>Indian</strong> tribal governments are not<br />
subject to state laws, including tax laws, unless those laws are made expressly applicable by<br />
federal law. See, e.g., McClanahan v. Arizona State Tax Comm’n, 411 U.S. 1641 (1973). <strong>Indian</strong><br />
tribal governments are not political subdivisions of states. Tribal facilities and their employees<br />
may not be required to have state licensure to perform their duties.<br />
Federal trust responsibility. The United States has a trust responsibility to <strong>Indian</strong> Tribes<br />
(described above).<br />
Tribal sovereign immunity. <strong>Indian</strong> tribal governments enjoy sovereign immunity except vis-à-vis<br />
the United States government, the superior sovereign. See, e.g., United States v. United States<br />
Fidelity & Guaranty Co., 309 U.S. 506 (1940).<br />
In sum, an <strong>Indian</strong> Tribe that has elected to directly operate its health care program can simultaneously<br />
serve in several capacities: as a sovereign government; as beneficiary of IHS-funded health care; as a<br />
direct provider of health care (including the right of recovery from third party payers); as administrator<br />
of a health program with responsibilities for advising its patients about eligibility for Medicare,<br />
Medicaid, and CHIP; and as a sponsor of a health insurance plan for its employees (and the payor<br />
under such a plan if it is a self-insured plan). CMS must take these multiple roles into account and<br />
fashion special policies to effectively implement Medicare, Medicaid, and CHIP in <strong>Indian</strong> communities<br />
in ways that assure full access by <strong>Indian</strong> beneficiaries and IHS/tribal providers.<br />
59 For example, Section 408 of the IHCIA provides that an entity operated by IHS, an <strong>Indian</strong> tribe, tribal organization or<br />
urban <strong>Indian</strong> organization that meets state requirements for licensure must be accepted as a provider but is not required to<br />
obtain a state license. 25 U.S.C. §1647a.<br />
61
Draft Report: Currently being circulated for Tribal leader and health director review and comment. Please provide<br />
comments by October 30, 2012 to Liz Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
APPENDIX C: CMS ORGANIZATION CHART<br />
62
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Appendix D: Common Terms & Acronyms<br />
All agencies are in CMS unless otherwise indicated.<br />
ACA Patient Protection and Affordable Care<br />
Act (P.L. 111-148)<br />
AI/AN American <strong>Indian</strong>s and Alaska Natives<br />
ACL Administration for Community Living (in<br />
HHS)<br />
ARRA American Recovery and Reinvestment Act<br />
of 2009 (P.L. 111-5)<br />
CCIIO Center for Consumer Information and<br />
Insurance Oversight<br />
CHS Contract <strong>Health</strong> Services, (IHS program to<br />
purchase services)<br />
CHIP Child <strong>Health</strong> Insurance Program<br />
CHIPRA Children’s <strong>Health</strong> Insurance Program<br />
Reauthorization Act of 2009 (P.L. 111-3)<br />
CMCS Center for Medicaid and CHIP Service<br />
CMM Center for Medicare Management<br />
CMMI Center for Medicare and Medicaid<br />
Innovation<br />
CMS Centers for Medicare & Medicaid Services<br />
CMSO Center for Medicaid and State Operations<br />
DHHS Department of <strong>Health</strong> and Human<br />
Services<br />
FFE Federally-facilitated Exchange<br />
FMAP Federal Medical Assistance Percentage<br />
(for Medicaid)<br />
FQHC Federally Qualified <strong>Health</strong> Centers<br />
HHS Department of <strong>Health</strong> and Human<br />
Services<br />
63<br />
I/T/U <strong>Health</strong> care services operated by the IHS,<br />
Tribes and urban <strong>Indian</strong> clinics<br />
IHCIA <strong>Indian</strong> <strong>Health</strong> Care Improvement Act (P.L.<br />
94-437)<br />
IHS <strong>Indian</strong> <strong>Health</strong> Service (federal agency in<br />
DHHS)<br />
LTSS Long Term Services and Support<br />
MA Medicare Advantage (managed care plan)<br />
MAM Medicaid Administrative Match<br />
MOA Memorandum of Agreement<br />
NAC Native American Contact in CMS Regional<br />
Offices<br />
NIHB <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
OGC Office of General Counsel<br />
Part A Medicare inpatient coverage<br />
Part B Medicare outpatient coverage<br />
Part C Medicare managed care plans, also called<br />
Medicare Advantage<br />
Part D Medicare prescription drug benefit<br />
TAG Tribal Affairs Group<br />
TTAG Tribal Technical Advisory Group<br />
Title XVIII Medicare, Social Security Act<br />
Title XIX Medicaid, Social Security Act<br />
Title XXI Children’s <strong>Health</strong> Insurance<br />
Program , Social Security Act
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Acknowledgements<br />
This American <strong>Indian</strong> and Alaska Native Strategic Plan, 2013-2018 was developed by the CMS Tribal<br />
Technical Advisory Group (TTAG) with assistance from the Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
(NPAIHB). Funding for this project was provided by CMS through an Interagency Agreement with the<br />
<strong>Indian</strong> <strong>Health</strong> Service and a subcontract from the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> (NIHB).<br />
This plan was developed over a period of six months, beginning in June 2012. The TTAG Strategic Plan<br />
Subcommittee met in-person and by conference call to develop new goals, objectives, and tasks. TTAG’s<br />
subcommittees for Tribal Consultation, Long Term Care, Data, and Outreach & Education provided<br />
essential input related to their visions for future activities and outcomes. TTAG approved the plan for<br />
nationwide tribal comment and review in September 2012.<br />
This is the third AI/AN Strategic Plan developed by TTAG. Each plan has built on the work of the<br />
preceding plan, although much of the background information in previous plans has been dropped from<br />
this version to make it shorter. The first plan, for the period 2005-2010, was developed under the TTAG<br />
Strategic Plan Chairmanship of Margaret Terrance, Nashville Area Representative to TTAG, and was<br />
staffed by Mim Dixon, consultant. The second plan, for the period from 2010- 2015, was developed<br />
under the TTAG Strategic Plan Subcommittee, chaired by the Honorable W. Ron Allen, Chair of the<br />
Jamestown S’Klallam Tribe, and Tribal Self-Governance Advisory Committee representative to the TTAG.<br />
The staff for the second plan included Craig Carter and Stephanie Craig Rushing from NPAIHB, as well as<br />
Kitty Marx and Caitlin Wesaw who were then at NIHB.<br />
TTAG would like to thank the many people in CMS who participated in interviews and provided their<br />
insights for the development of this plan. While we are keeping their names and comments<br />
confidential, we hope they will see the wisdom they shared reflected on these pages. Mim Dixon and<br />
Jim Roberts staffed this plan, with assistance from Lisa Griggs (NPAIHB), Tyra Baer (NIHB), and Liz<br />
Heintzman (NIHB).<br />
Strategic Plan Subcommittee<br />
W. Ron Allen, Tribal Chairman, Jamestown S’Klallam Tribe, Strategic Plan Subcommittee Chair<br />
Jennifer Cooper, JD, <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
Jim Crouch, MPH, California Rural <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
Valerie Davidson, JD, Alaska Native Tribal <strong>Health</strong> Consortium<br />
64
Draft Report: Currently being circulated for Tribal leader and health director<br />
review and comment. Please provide comments by October 30, 2012 to Liz<br />
Heintzman at the <strong>National</strong> <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong> at EHeintzman@nihb.org.<br />
Carol Korenbrot , PhD, California Rural <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
Jim Lamb, Alaska Native Tribal <strong>Health</strong> Consortium<br />
Liz Malerba, United South and Eastern Tribes<br />
Elliott Milhollin, JD, Hobbs, Strauss Dean and Walker<br />
Myra Munson, JD, MSW, Sonosky, Chambers, Miller and Munson<br />
Raho Ortiz, <strong>Indian</strong> <strong>Health</strong> Service<br />
Judy Goforth Parker, PhD, Chickasaw Nation<br />
Jim Roberts, Northwest Portland Area <strong>Indian</strong> <strong>Health</strong> <strong>Board</strong><br />
Jay Steiner, JD, <strong>National</strong> Council for Urban <strong>Indian</strong> <strong>Health</strong><br />
Alec Thurdercloud, MD, Ho-Chunk Nation<br />
65