Craniofacial Anomalies, Part 2 - Plastic Surgery Internal
Craniofacial Anomalies, Part 2 - Plastic Surgery Internal
Craniofacial Anomalies, Part 2 - Plastic Surgery Internal

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
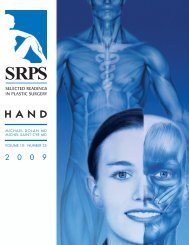
Fig 8. Left, child with asymmetrical nasoethmoidal, nasoorbital<br />
encephalocele. Right, same child at age 5, after removal of the<br />
encephalocele and correction of the trigonocephaly, orbital<br />
dystopia, and hypertelorism in one procedure at 8 months of age.<br />
(Reprinted with permission from Holmes AD, Meara JG, Kolker<br />
AR, et al: Frontoethmoidal encephaloceles: reconstruction and<br />
refinements. J Craniofac Surg 12:6, 2001.)<br />
foramen cecum. In a frontoethmoidal encephalocele<br />
the diverticulum does not recede and the bone<br />
does not close. The etiology of encephalocele is<br />
unknown but includes racial, genetic, environmental,<br />
and paternal factors. 122<br />
Encephaloceles occur with a number of craniofacial<br />
syndromes. 123 The world wide incidence of<br />
encephalocele is 1/5000. 124 In Western Europe, North<br />
America, Australia, and Japan, occipital encephaloceles<br />
predominate. In Southeast Asia and Russia,<br />
anterior encephaloceles outnumber posterior ones<br />
by a 9.5:1 ratio. 124,125 The reason for this discrepancy<br />
is unknown.<br />
The principles of treatment are incision of the sac,<br />
amputation of excess tissue to the level of the surrounding<br />
skull, closure of the dura, and closure of<br />
the skin. 126 David, 127 Forcada et al, 128 and Smit and<br />
colleagues129 review the spectrum of cranial and<br />
cerebral malformations that may be present in<br />
frontoethmoidal encephaloceles and discuss the<br />
diagnosis and management of these deformities.<br />
David127 analyzed the experience with frontoethmoidal<br />
encephaloceles by the Australian <strong>Craniofacial</strong><br />
Unit from 1975 to 1993 and reached the following<br />
conclusions:<br />
• Early complete surgery is indicated to allow the<br />
developing brain and eyes to remodel the facial<br />
deformity.<br />
• Intracranial abnormalities are common.<br />
SRPS Volume 10, Number 17, <strong>Part</strong> 2<br />
• Frontoethmoidal encephaloceles differ from other<br />
neural tube defects in their lack of a familial pattern<br />
and peculiar geographic distribution.<br />
• Treatment by craniofacial technique is best.<br />
• The established deformity can be effectively managed<br />
by craniofacial osteotomies.<br />
• Most patients have abnormal intercanthal distances<br />
but normal interpupillary and lateral canthal<br />
measurements.<br />
• The frontal sinus region often needs repeat bone<br />
grafting, and nasal bone grafts commonly need<br />
to be replaced as patients age.<br />
• Treatment for craniofacial clefts should be postponed<br />
until after growth is complete.<br />
• Early treatment of patients with basal encephaloceles<br />
is indicated to prevent further damage and<br />
infection.<br />
• <strong>Surgery</strong> for extensive basal encephaloceles is complex<br />
and probably should be done through a<br />
facial hemisection approach.<br />
Holmes et al130 offer their experience with 35<br />
cases of frontoethmoidal encephalocele. The goals<br />
of treatment are as follows (Fig 9):<br />
• urgent closure of open skin defects to prevent<br />
infection and desiccation of brain<br />
• removal or invagination of nonfunctional extracranial<br />
tissue<br />
• watertight dural closure<br />
• total craniofacial reconstruction with special care<br />
to avoid the “long nose deformity”<br />
To correct the deformity caused by hypertelorism<br />
and a long midface, Holmes and coworkers130 lower<br />
the supraorbital bar by rotating it medially, posteriorly<br />
and downward in the midline, while laterally it is<br />
widened to correct the trigonocephalic deformity.<br />
Successful correction depends on an understanding<br />
of the pathologic anatomy; careful planning of<br />
osteotomies and bone movements to correct the<br />
whole deformity, including trigonocephaly and the<br />
long nose deformity; nasal reconstruction with cantilever<br />
graft to avoid the long nose deformity; skin<br />
closure removing abnormal skin and careful placing<br />
of scars; transnasal canthoplasty to reposition the<br />
11