

CLIMBING WALL OPERATIONS MANUAL
CLIMBING WALL OPERATIONS MANUAL
CLIMBING WALL OPERATIONS MANUAL

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
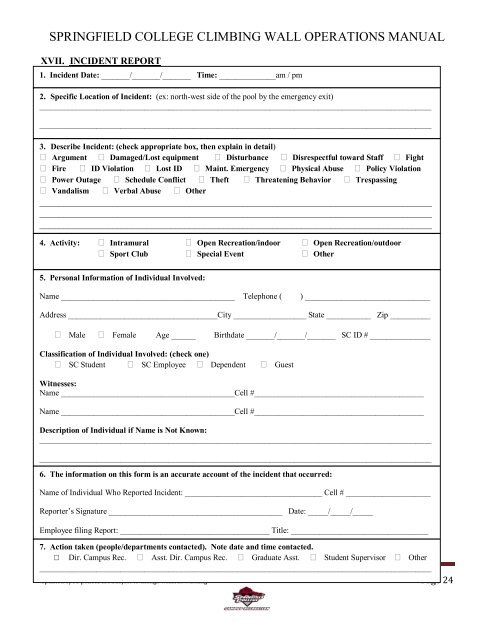
SPRINGFIELD COLLEGE <strong>CLIMBING</strong> <strong>WALL</strong> <strong>OPERATIONS</strong> <strong>MANUAL</strong><br />
XVII. INCIDENT REPORT<br />
1. Incident Date: _______/_______/_______ Time: ______________am / pm<br />
INCIDENT REPORT<br />
2. Specific Location of Incident: (ex: northwest side of the pool by the emergency exit)<br />
_________________________________________________________________________________________________<br />
_________________________________________________________________________________________________<br />
3. Describe Incident: (check appropriate box, then explain in detail)<br />
Argument Damaged/Lost equipment Disturbance Disrespectful toward Staff Fight<br />
Fire ID Violation Lost ID Maint. Emergency Physical Abuse Policy Violation<br />
Power Outage Schedule Conflict Theft Threatening Behavior Trespassing<br />
Vandalism Verbal Abuse Other<br />
_________________________________________________________________________________<br />
_________________________________________________________________________________<br />
_________________________________________________________________________________<br />
4. Activity: Intramural Open Recreation/indoor Open Recreation/outdoor<br />
Sport Club Special Event Other<br />
5. Personal Information of Individual Involved:<br />
Name ___________________________________________ Telephone ( ) _______________________________<br />
Address _____________________________________City __________________ State ___________ Zip __________<br />
Male Female Age ______ Birthdate _______/_______/_______ SC ID # _______________<br />
Classification of Individual Involved: (check one)<br />
SC Student SC Employee Dependent Guest<br />
Witnesses:<br />
Name ___________________________________________Cell #__________________________________________<br />
Name ___________________________________________Cell #__________________________________________<br />
Description of Individual if Name is Not Known:<br />
_________________________________________________________________________________________________<br />
_________________________________________________________________________________________________<br />
6. The information on this form is an accurate account of the incident that occurred:<br />
Name of Individual Who Reported Incident: __________________________________ Cell # _____________________<br />
Reporter’s Signature ___________________________________________ Date: _____/_____/_____<br />
Employee filing Report: _____________________________________ Title: __________________________________<br />
7. Action taken (people/departments contacted). Note date and time contacted.<br />
□ Dir. Campus Rec. Asst. Dir. Campus Rec. Graduate Asst. Student Supervisor Other<br />
_________________________________________________________________________________________________<br />
Updated 8/08 polices are subject to change without warning Page 24


