

CLIMBING WALL OPERATIONS MANUAL
CLIMBING WALL OPERATIONS MANUAL
CLIMBING WALL OPERATIONS MANUAL

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
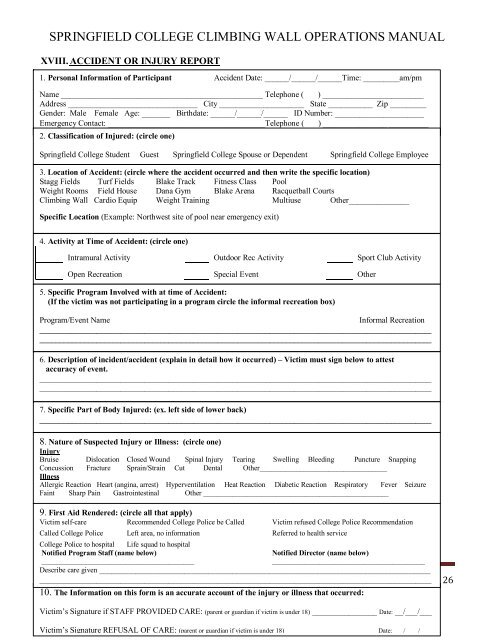
SPRINGFIELD COLLEGE <strong>CLIMBING</strong> <strong>WALL</strong> <strong>OPERATIONS</strong> <strong>MANUAL</strong><br />
XVIII. ACCIDENT OR INJURY REPORT<br />
1. Personal Information of Participant Accident Date: ______/______/______Time: _________am/pm<br />
XIX.<br />
Name XX. __________________________________________________ Telephone ( ) _________________________<br />
Address ________________________________ City _____________________ State ___________ Zip _________<br />
Gender:<br />
XXI.<br />
Male Female Age: _______ Birthdate: ______/______/______ ID Number: ______________________<br />
Emergency XXII. Contact: _______________________________________Telephone ( ) _________________________<br />
XXIII.<br />
2. Classification of Injured: (circle one)<br />
XXIV.<br />
Springfield XXV. College Student Guest Springfield College Spouse or Dependent Springfield College Employee<br />
XXVI.<br />
3.<br />
XXVII.<br />
Location of Accident: (circle where the accident occurred and then write the specific location)<br />
Stagg Fields Turf Fields Blake Track Fitness Class Pool<br />
Weight XXVIII. Rooms Field House Dana Gym Blake Arena Racquetball Courts<br />
Climbing XXIX. Wall Cardio Equip Weight Training Multiuse Other_______________<br />
XXX.<br />
Specific<br />
XXXI.<br />
Location (Example: Northwest site of pool near emergency exit)<br />
_________________________________________________________________________________________________<br />
4. Activity at Time of Accident: (circle one)<br />
Intramural Activity<br />
XXXII.<br />
XXXIII. Open Recreation<br />
Outdoor Rec Activity<br />
Special Event<br />
Sport Club Activity<br />
Other<br />
XXXIV.<br />
5. Specific Program Involved with at time of Accident:<br />
XXXV. (If the victim was not participating in a program circle the informal recreation box)<br />
XXXVI.<br />
Program/Event XXXVII. Name Informal Recreation<br />
_________________________________________________________________________________________________<br />
XXXVIII.<br />
_________________________________________________________________________________________________<br />
XXXIX.<br />
_________________________________________________________________________________________________<br />
XL.<br />
6. Description of incident/accident (explain in detail how it occurred) – Victim must sign below to attest<br />
XLI.<br />
accuracy of event.<br />
_________________________________________________________________________________________________<br />
XLII.<br />
_________________________________________________________________________________________________<br />
XLIII.<br />
_________________________________________________________________________________________________<br />
XLIV.<br />
7. XLV. Specific Part of Body Injured: (ex. left side of lower back)<br />
_________________________________________________________________________________________________<br />
XLVI.<br />
_________________________________________________________________________________________________<br />
XLVII.<br />
8. XLVIII. Nature of Suspected Injury or Illness: (circle one)<br />
Injury XLIX.<br />
Bruise Dislocation Closed Wound Spinal Injury Tearing Swelling Bleeding Puncture Snapping<br />
Concussion L. Fracture Sprain/Strain Cut Dental Other___________________________________<br />
Illness LI.<br />
Allergic LII. Reaction Heart (angina, arrest) Hyperventilation Heat Reaction Diabetic Reaction Respiratory Fever Seizure<br />
Faint Sharp Pain Gastrointestinal Other ___________________________________________________<br />
LIII.<br />
9. LIV. First Aid Rendered: (circle all that apply)<br />
Victim LV. selfcare Recommended College Police be Called Victim refused College Police Recommendation<br />
Called LVI. College Police Left area, no information Referred to health service<br />
College LVII. Police to hospital Life squad to hospital<br />
LVIII. Notified Program Staff (name below) Notified Director (name below)<br />
__________________________________________ __________________________________________<br />
Describe care given __________________________________________________________________________________<br />
_________________________________________________________________________________________________<br />
Updated 8/08 polices are subject to change without warning Page 26<br />
10. The Information on this form is an accurate account of the injury or illness that occurred:<br />
Victim’s Signature if STAFF PROVIDED CARE: (parent or guardian if victim is under 18) ________________ Date: __/___/___<br />
Victim’s Signature REFUSAL OF CARE: (parent or guardian if victim is under 18) ________________________ ____Date: ___/____/____


