Diagnosis and Treatment of Suspected Deep Vein Thrombosis
Diagnosis and Treatment of Suspected Deep Vein Thrombosis
Diagnosis and Treatment of Suspected Deep Vein Thrombosis

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
CLINICAL POLICY<br />
<strong>Diagnosis</strong> <strong>and</strong> <strong>Treatment</strong> <strong>of</strong> Patients with a <strong>Suspected</strong> <strong>Deep</strong> <strong>Vein</strong><br />
<strong>Thrombosis</strong> Policy<br />
For use in: PCT-wide<br />
Target Audience: All Trust Clinical Staff<br />
Purpose Policy for the diagnosis <strong>and</strong> treatment <strong>of</strong><br />
patients with a suspected <strong>Deep</strong> <strong>Vein</strong><br />
<strong>Thrombosis</strong><br />
Document Author: Jenny Murphy<br />
Approved by: Clinical Guidelines Group or Equivalent<br />
Ratified by: Policy Sub-Committee (PSC)<br />
Policy Indexed: HStHCL218<br />
Version Number: 2.0<br />
Effective From: February 2010<br />
Review Date: February 2013<br />
Statutory <strong>and</strong> legal requirements Policy based on recommendations from the<br />
NHS Litigation Authority<br />
Implementation Lead Jenny Murphy<br />
Implementation Process Refer to attached dissemination plan<br />
The Trust is committed to creating an environment that promotes equality <strong>and</strong> embraces<br />
diversity, both within our workforce <strong>and</strong> in service delivery. This document should be<br />
implemented with due regard to this commitment<br />
This document seeks to uphold the duties <strong>and</strong> principles contained within the Human Rights<br />
Act. All Staff within the PCT should be aware <strong>of</strong> its implications<br />
This policy is due for review by February 2013. After this date, this policy <strong>and</strong> associated<br />
process documents may become invalid. All users should ensure that they are consulting the<br />
current version <strong>of</strong> this document.
Key individuals involved in developing the document (Internal Staff Only)<br />
Name(s)<br />
Designation<br />
Jenny Murphy Advanced Practitioner<br />
Elaine McDowell Clinical Service Manager<br />
Distributed to the following for approvals <strong>and</strong> comments<br />
Committee(s)<br />
Members <strong>of</strong> the Policy Sub Committee (PSC)<br />
Members <strong>of</strong> the Clinical Policies Guidelines<br />
Group (CPG)<br />
Individual(s)<br />
Designation<br />
Chris Turner Head <strong>of</strong> Urgent Care<br />
Phillip Chalmers Divisional Manager<br />
Linda Spooner Pr<strong>of</strong>essional Development Manager<br />
Page 2 <strong>of</strong> 40
Table <strong>of</strong> Contents<br />
Introduction ..................................................................................................................................4<br />
Purpose........................................................................................................................................4<br />
Scope...........................................................................................................................................5<br />
Policy ...........................................................................................................................................5<br />
Training Requirements.................................................................................................................7<br />
Duties <strong>and</strong> Responsibilities ..........................................................................................................7<br />
Document Storage <strong>and</strong> Filing.......................................................................................................8<br />
References...................................................................................................................................9<br />
Appendix 1 .................................................................................................................................10<br />
Appendix 2 .................................................................................................................................12<br />
Appendix 3 .................................................................................................................................14<br />
Appendix 4 .................................................................................................................................23<br />
Appendix 5 .................................................................................................................................24<br />
Appendix 6 .................................................................................................................................25<br />
Appendix 7 .................................................................................................................................26<br />
Appendix 8 .................................................................................................................................27<br />
Appendix 9 .................................................................................................................................28<br />
Appendix 10 ...............................................................................................................................29<br />
Appendix 11 ...............................................................................................................................30<br />
Appendix 12 ...............................................................................................................................31<br />
Appendix 13 ...............................................................................................................................32<br />
Appendix 14 ...............................................................................................................................33<br />
Appendix 15 ...............................................................................................................................35<br />
Appendix 16 ...............................................................................................................................37<br />
Appendix 17 ...............................................................................................................................38<br />
Appendix 18 ...............................................................................................................................39<br />
Appendix 19 ...............................................................................................................................40<br />
Page 3 <strong>of</strong> 40
INTRODUCTION<br />
To comply with the requirements <strong>of</strong> the Clinical Negligence Scheme for Trusts, Risk Pooling<br />
Schemes for Trusts, best practice <strong>and</strong> NHS guidance, the Trust has implemented an effective<br />
community diagnostic <strong>and</strong> treatment service for the treatment <strong>of</strong> deep vein thrombosis in non -<br />
complex patients in a nurse led environment.<br />
An effective community diagnostic <strong>and</strong> treatment service promotes quality <strong>of</strong> life <strong>and</strong> reduces<br />
the necessity for attendance at the Emergency Department. This document describes the<br />
clinical pathway for patients who are referred by their GP or who self refer to the Widnes Walkin<br />
Centre or the St Helens Minor injuries / Walk-In Centre with a suspected DVT.<br />
Administration <strong>of</strong> Enoxaparin carries potential risks <strong>and</strong> should only be given if the benefits<br />
outweigh these risks. Stringent guidelines must be followed to ensure that the correct drug <strong>and</strong><br />
dose is given to the correct patient at the correct time <strong>and</strong> that any adverse reactions are dealt<br />
with promptly <strong>and</strong> efficiently in accordance with hospital/PCT policies.<br />
This policy is supported by Nursing <strong>and</strong> Midwifery Council guidelines St<strong>and</strong>ards for Medicines<br />
Management.<br />
PURPOSE<br />
The purpose <strong>of</strong> this policy is designed to provide comprehensive guidance to all qualified nurses<br />
within the Walk-In Centres who have undergone appropriate training in delivering a community<br />
DVT service <strong>and</strong> must be read in conjunction with the Enoxaparin PGD. This policy will enable<br />
the organisation to fulfil its obligations under the NHS plan.<br />
Objectives<br />
To sustain a stream line <strong>and</strong> non – fragmented deep vein thrombosis service across<br />
NHS Halton <strong>and</strong> St Helens Primary Care trust<br />
To <strong>of</strong>fer the patient a safe <strong>and</strong> effective diagnostic <strong>and</strong> treatment service <strong>and</strong> promoting<br />
quality <strong>of</strong> life<br />
To reduce the necessity to attend Emergency Department <strong>and</strong> GP assessment unit<br />
therefore reducing hospital admission<br />
Outcome<br />
To reduce the patient journey<br />
Prevent unnecessary medical referrals<br />
Effective use <strong>of</strong> resources within the NHS<br />
More effective treatment <strong>of</strong> patients with suspected non – complex <strong>Deep</strong> <strong>Vein</strong><br />
<strong>Thrombosis</strong><br />
Page 4 <strong>of</strong> 40
SCOPE<br />
This policy applies to all qualified nurses within the Walk-In Centre teams who have received<br />
training <strong>and</strong> met competencies both practically <strong>and</strong> theoretically.<br />
POLICY<br />
This policy acknowledges St Helens <strong>and</strong> Knowsley Acute NHS Trust in their support in assisting<br />
in the delivery <strong>of</strong> the community DVT Service.<br />
This process describes the clinical pathway for patients with suspected DVT either self<br />
referring or referred by their GP (see appendix 6)<br />
If the patient is deemed suitable for community diagnosis <strong>and</strong> treatment, the patient will<br />
then be commenced on the DVT pathway (Appendix 3).<br />
Following a holistic assessment, which will include the Wells score, the Nurse Practitioner<br />
will fully discuss the process with the patient. If the patient is happy to proceed with the<br />
pathway, verbal informed consent, to be treated at the WIC by a nurse practitioner, will be<br />
given <strong>and</strong> recorded.<br />
Bloods will be taken for D-dimer, LTF,s, U+E’s, FBC <strong>and</strong> where patient is a diabetic blood<br />
will also be taken for glucose levels.<br />
the result <strong>of</strong> the D Dimer <strong>and</strong> Wells score will determine if the patient commences the<br />
relevant DVT pathway <strong>and</strong> Enoxaparin via PGD ( appendix 4) administered<br />
This process describes the clinical pathway for patients with suspected DVT either self<br />
referring or referred by their GP when the near/ on site patient testing machine is out <strong>of</strong><br />
order.<br />
If the patient is deemed suitable for community diagnosis <strong>and</strong> treatment, the patient will<br />
then be commenced on the DVT pathway (Appendix 7).<br />
Following a holistic assessment, which will include the Wells score, the Nurse Practitioner<br />
will fully discuss the process with the patient. If the patient is happy to proceed with the<br />
pathway, verbal informed consent, to be treated at the WIC by a nurse practitioner, will be<br />
given <strong>and</strong> recorded.<br />
Bloods will be taken for D-dimer, LFT’s, U+E’s, FBC <strong>and</strong> where patient is a diabetic blood<br />
will also be taken for glucose levels.<br />
Bloods will be transported either via normal collection ( twice a day) or taxi. Staff at<br />
Whiston Pathology lab haematology department will be contacted via telephone re<br />
request.<br />
Page 5 <strong>of</strong> 40
Once a D Dimer result has been received this <strong>and</strong> the Wells score will determine if the<br />
patient commences the relevant DVT pathway <strong>and</strong> Enoxaparin via PGD ( appendix 4)<br />
administered<br />
The Nurse Practitioner in the Walk-in Centre will be responsible for -:<br />
Taking referrals from General Practitioners in Halton <strong>and</strong> St Helens PCT.<br />
Assessing <strong>and</strong> treating patients who self refer.<br />
Advising GP’s <strong>and</strong> other referring clinicians regarding suitability for treatment in the<br />
community.<br />
Providing advice <strong>and</strong> information to patients concerning their condition, treatment <strong>and</strong><br />
follow up.<br />
Ensuring bloods drawn <strong>and</strong> transported in the agreed manner.<br />
Commencement <strong>of</strong> relevant DVT pathway on receipt <strong>of</strong> D-dimer results, if appropriate.<br />
Administering Enoxaparin as per PGD. ( Appendix 4)<br />
Referral to anticoagulant nurse.(appendix 2)<br />
Referral to Ultrasound. .(appendix 2)<br />
Discussing blood results with the anti coagulant nurse prior to the administration <strong>of</strong> the<br />
second dose <strong>of</strong> Enoxaparin.<br />
Referral to GP or other service as required.<br />
Maintaining accurate records.<br />
Planning education, training <strong>and</strong> continuing pr<strong>of</strong>essional development.<br />
Ensuring that all staff using this policy act within The NMC Code <strong>and</strong> in accordance with<br />
the St<strong>and</strong>ards for Medicines management.<br />
Liaising with the Clinical Governance team for the purpose <strong>of</strong> research <strong>and</strong> audit.<br />
Page 6 <strong>of</strong> 40
Haematology Consultants will be responsible for:<br />
The medical care <strong>of</strong> the patients once they have commenced the DVT pathway.<br />
Informing <strong>and</strong> developing appropriate treatment <strong>and</strong> care pathways in collaboration with<br />
nursing staff.<br />
TRAINING REQUIREMENTS<br />
The PCT will ensure that all members <strong>of</strong> the Walk-In Centre staff providing this service will<br />
receive the necessary level <strong>of</strong> training for them to fulfil their individual responsibilities as<br />
identified in this policy. Training for the team regarding Wells assessment <strong>and</strong> the management<br />
<strong>of</strong> the patient on a care pathway is provided in house. Only those members <strong>of</strong> staff detailed in<br />
this Policy who have had specific training to deliver this service can undertake an assessment<br />
<strong>of</strong> patients presenting with a suspected DVT.<br />
DUTIES AND RESPONSIBILITIES<br />
Duties within the Organisation<br />
Duties <strong>and</strong> accountabilities <strong>of</strong> directors, committees, specialist staff, <strong>and</strong> authors with<br />
responsibility for procedural documents must be included within the document.<br />
Chief Executive<br />
The Chief Executive is responsible for ensuring compliance with the Hospital/PCT Policies <strong>and</strong><br />
Guidelines, legislation, NHS guidance <strong>and</strong> for ensuring the policy is effective.<br />
Trust Board<br />
The Trust board is responsible for has overall responsibility for ensuring the provision <strong>of</strong><br />
effective clinical services within the organisation, <strong>and</strong> to ensure that the Trust complies with its<br />
statutory obligations.<br />
All Halton & St Helens Staff<br />
All Staff are responsible for adhering to <strong>and</strong> complying with the requirements <strong>of</strong> the policies,<br />
guidelines, protocols <strong>and</strong> st<strong>and</strong>ard operating procedures (SOPs) contained within <strong>and</strong><br />
applicable to their area <strong>of</strong> operation.<br />
Temporary <strong>and</strong> Agency Staff, Contractors <strong>and</strong> Subcontractors<br />
All Staff are responsible for adhering to <strong>and</strong> complying with the requirements <strong>of</strong> the policies,<br />
guidelines, protocols <strong>and</strong> st<strong>and</strong>ard operating procedures (SOPs) contained within <strong>and</strong><br />
applicable to their area <strong>of</strong> operation.<br />
Page 7 <strong>of</strong> 40
DOCUMENT STORAGE AND FILING<br />
The approved <strong>and</strong> ratified policy document will be uploaded to the document portal. Follow the<br />
link below to view the policy document <strong>and</strong> its related pages:<br />
http://sharepointcompliance/default.aspx<br />
Page 8 <strong>of</strong> 40
REFERENCES<br />
Reference<br />
Michiels JJ, Gadisseur, Van der Planken M,<br />
Schroynes W, Berneman Z et al<br />
<strong>Diagnosis</strong> <strong>of</strong> <strong>Deep</strong> <strong>Vein</strong> <strong>Thrombosis</strong>: How many tests<br />
Do We Need?<br />
Acta chir belg 2005, 105, 16-25<br />
Patient Group Direction :Enoxaparin 2009; Halton <strong>and</strong><br />
St Helens PCT, NHS Minor Injuries Walk in Centre.<br />
Wells PS Anderson DR, Rodger M, et al. Evaluation <strong>of</strong><br />
d-Dimer in the diagnosis <strong>of</strong> suspected deep-vein<br />
thrombosis. N Engl J Med 2003; 349:1227 - 1235<br />
Wells PS Anderson DR, Rodger M, et al. Excluding<br />
pulmonary embolism at the bedside without diagnostic<br />
imaging: management <strong>of</strong> patients with suspected<br />
pulmonary embolism presenting to the emergency<br />
department by using a simple clinical model <strong>and</strong> d –<br />
dimmer . Ann Intern med. 2001;135: 98-107.<br />
Wells PS Anderson DR, Rodger M, et al. Wells score<br />
for <strong>Deep</strong> <strong>Vein</strong> <strong>Thrombosis</strong>. Lancet 1997; 350: 1795 -<br />
1798<br />
Page 9 <strong>of</strong> 40<br />
Relevance (whole<br />
document or<br />
section, please<br />
state)<br />
Whole 1a<br />
Whole 1v<br />
Whole 1b<br />
Whole 11b<br />
Whole 1b<br />
Evidence<br />
Grade
APPENDIX 1<br />
Glossary <strong>of</strong> Terms<br />
St Helens Minor injuries/Walk-In Centre – refers to the Millennium Centre where patients can<br />
self present or be referred without appointment for treatment <strong>of</strong> minor ailments <strong>and</strong> injuries.<br />
Widnes Walk-in Centre – refers to the Health Care Resource Centre where patients can self<br />
present or be referred without appointment for treatment <strong>of</strong> minor ailments <strong>and</strong> injuries.<br />
WIC- refers to St Helens Minor injuries / walk in centre or Widnes walk in centre<br />
DVT – refers to deep vein thrombosis.<br />
D-Dimer test – refers to the test carried out in the laboratory (or an onsite near patient testing<br />
machine) to confirm or exclude DVT. D-Dimer is a fibrin degradation product generated during<br />
fibrinolysis. D-Dimer concentrations are raised in the setting <strong>of</strong> acute deep vein thrombosis, <strong>and</strong><br />
normal concentrations are expected in the absence <strong>of</strong> acute venous thrombosis unless other,<br />
coexistent conditions that activate the coagulant system are present.<br />
Wells score – refers to a clinical probability tool developed by Wells et al, (1995) which uses a<br />
structured assessment <strong>of</strong> explicit historical <strong>and</strong> physical assessment to stratify patients into low,<br />
moderate <strong>and</strong> high risk <strong>of</strong> deep vein thrombosis.<br />
Nurse Practitioner - refers to a nurse at the Walk-In Centre who have undergone specific<br />
training to assess patients <strong>and</strong> administer where appropriate Enoxaparin via a Patient Group<br />
Direction.<br />
Operational Policy – refers to the document, which guides the clinical pr<strong>of</strong>essional through the<br />
DVT pathway (Appendix B).<br />
Patient Group Direction (PGD) is a written instruction to enable a healthcare pr<strong>of</strong>essional to<br />
supply <strong>and</strong> / or administer a licensed medicine to groups <strong>of</strong> patients how may not be individually<br />
identified before presentation for treatment.( the majority <strong>of</strong> clinical care should be provided on<br />
an individual, patient-specific basis).This must be approved by a team, which includes, a<br />
Director, a Senior Doctor, a Senior Pharmacist<br />
PCT- refers to NHS Halton <strong>and</strong> St Helens Primary Care Trust<br />
ED – refers to Emergency Department Whiston Hospital<br />
GP- refers to General practitioner<br />
Page 10 <strong>of</strong> 40
GPAU- refers to the GP assessment unit at Whiston hospital<br />
Single point access refers to out <strong>of</strong> hours GP that covers Halton <strong>and</strong> St Helens<br />
LFT,s refers to Liver Function Tests<br />
U+E,s refers to Urea <strong>and</strong> Electrolytes<br />
FBC refers to Full Blood Count<br />
Page 11 <strong>of</strong> 40
APPENDIX 2<br />
REFERRAL FORM TO ANTICOAGULANT NURSES<br />
WHISTON HOSPITAL FROM THE WALK-IN CENTRES<br />
NAME…………………………………………….<br />
ADDRESS………………………………………...<br />
…………………………………………………….<br />
…………………………………………………….<br />
POST CODE……………………………………...<br />
DATE OF BIRTH ….../……../……..<br />
TEL NO…………………………………………...<br />
NEXT OF KIN<br />
TEL NO…………………………………………...<br />
DATE OF REFERAL …../……/……….<br />
GP…………………………………………………<br />
ADDRESS………………………………………..<br />
……………………………………………………<br />
…………………………………………………….<br />
TEL NO…………………………………………...<br />
PATIENT’S WEIGHT………………Kgs<br />
PREVIOUS DVT YES/NO<br />
FAMILY HISTORY YES/NO<br />
EXCLUSION CRITERIA FOR WALK-IN CENTRE TREATMENT<br />
PATIENTS UNDER 16 YEARS OF AGE<br />
KNOWN ACTIVE CANCER<br />
SUSPECTED OR PREVIOUS PULMONARY EMBOLUS<br />
SOCIAL REASONS eg NOT INDEPENDENT, NO SUITABLE CARER<br />
NO ACCESS TO A TELEPHONE<br />
IV DRUG USER<br />
ALCOHOL DEPENDENT<br />
PREGNANCY & PATIENTS LESS THAN 6/52 POST PARTUM<br />
HISTORY AND RECORD OF BLOODS TAKEN<br />
D-DIMER RESULT……………………………………<br />
CLINICAL STRATIFICATION LOW RISK MED RISK HIGH RISK<br />
Page 12 <strong>of</strong> 40<br />
YES/NO<br />
YES/NO<br />
YES/NO<br />
YES/NO<br />
YES/NO<br />
YES/NO<br />
YES/NO<br />
YES/NO
ENOXAPARIN (CLEXANE)<br />
DATE DOSE PRESCRIBED BY TIME GIVEN GIVEN BY<br />
DOPPLER REQUEST RIGHT LEG LEFT LEG<br />
DATE AND TIME ……………………………………………………………………..<br />
SIGNATURE………………………………… PRINT NAME……………………………………..<br />
Page 13 <strong>of</strong> 40
APPENDIX 3<br />
Click here to view <strong>and</strong> print the document<br />
Page 14 <strong>of</strong> 40
Page 15 <strong>of</strong> 40
Page 16 <strong>of</strong> 40
Page 17 <strong>of</strong> 40
Page 18 <strong>of</strong> 40
Page 19 <strong>of</strong> 40
Page 20 <strong>of</strong> 40
Page 21 <strong>of</strong> 40
Page 22 <strong>of</strong> 40
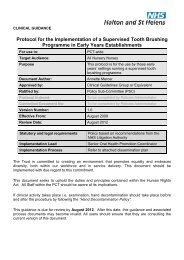
APPENDIX 4<br />
GP<br />
Referral with letter <strong>and</strong><br />
phone call<br />
Low *<br />
Clinical assessment<br />
inc. Wells criteria<br />
Risk<br />
stratification<br />
Medium *<br />
Halton <strong>and</strong> St Helens<br />
St. Helens NHS Minor Injuries/ Walk in Centre<br />
Widnes Walk in Centre<br />
Pathway for patients presenting with<br />
<strong>Deep</strong> <strong>Vein</strong> <strong>Thrombosis</strong><br />
At the Walk-in Centre<br />
High *<br />
*Refer to separate pathways overleaf<br />
Page 23 <strong>of</strong> 40<br />
? DVT<br />
Self referral<br />
Clinical assessment<br />
Differential<br />
diagnosis<br />
Discharge
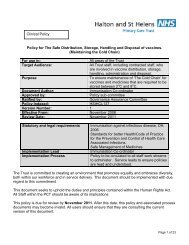
APPENDIX 5<br />
Negative D Dimer<br />
500 ng/ml<br />
Give 1 st dose Enoxaparin<br />
Prior to 2 nd dose<br />
Enoxaparin ensure:<br />
Refer to Anti Coagulation<br />
Nurse (ACN) for follow<br />
up.<br />
Blood results have been<br />
checked by practitioner
APPENDIX 6<br />
Negative D Dimer<br />
500ng/ml<br />
Give 1 st dose Enoxaparin<br />
Prior to 2 nd dose Enoxaparin ensure:<br />
Refer to Anti Coagulation Nurse (ACN)<br />
for follow up.<br />
Blood results have been checked by<br />
practitioner<br />
Arrange Doppler<br />
Page 25 <strong>of</strong> 40
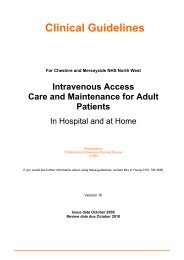
APPENDIX 7<br />
Negative D Dimer<br />
< 500 ng/ml<br />
Arrange:<br />
Referral to Anti Coagulation<br />
nurse (ACN) for follow up.<br />
Doppler<br />
Halton <strong>and</strong> St Helens<br />
St. Helens NHS Minor injuries / Walk-in Centre<br />
Widnes Walk in Centre<br />
Medium Risk<br />
Well’s score 1-2<br />
D-Dimer FBC, U&E, LFT, Coagulation<br />
screen, Glucose (if diabetic).<br />
D Dimer result<br />
Page 26 <strong>of</strong> 40<br />
Positive D Dimer<br />
>500 ng/ml<br />
Recall patient for 1 st dose<br />
Enoxaparin<br />
Prior to 2 nd dose Enoxaparin ensure:<br />
Referral to Anti Coagulation<br />
Nurse (ACN) for follow up.<br />
Blood results have been checked<br />
by practitioner
APPENDIX 8<br />
Negative D Dimer<br />
< 500ng/ml<br />
Arrange:<br />
Referral to Anti<br />
Coagulation nurse<br />
(ACN) for follow<br />
up.<br />
Halton <strong>and</strong> St Helens<br />
St. Helens NHS Minor injuries / Walk-in Centre<br />
Widnes Walk in Centre<br />
Medium Risk<br />
Well’s score 1-2<br />
D-Dimer<br />
FBC, U&E, LFT, Coagulation<br />
screen, Glucose (if diabetic).<br />
Send to Whiston<br />
Lab<br />
Results within 2 hrs<br />
Positive D Dimer<br />
>500ng/ml<br />
Recall patient for 1 st<br />
dose Enoxaparin<br />
Prior to 2 nd dose Enoxaparin ensure:<br />
Referral to Anti Coagulation Nurse<br />
(ACN) for follow up.<br />
Blood results have been checked<br />
by practitioner<br />
Doppler arranged<br />
Page 27 <strong>of</strong> 40
APPENDIX 9<br />
Negative D-Dimer<br />
500ng/ml<br />
Halton <strong>and</strong> St Helens<br />
St. Helens NHS Walk-in Centre<br />
Widnes Walk in Centre<br />
Prior to 2 nd dose Enoxaparin ensure:<br />
Refer to Anti Coagulation Nurse<br />
(ACN) for follow up.<br />
Blood results have been<br />
checked by ACN<br />
Arrange Doppler<br />
Page 28 <strong>of</strong> 40
APPENDIX 10<br />
Negative D-Dimer<br />
190ng/ml<br />
Halton <strong>and</strong> St Helens<br />
St. Helens NHS Walk-in Centre<br />
Widnes Walk in Centre<br />
Prior to 2 nd dose Enoxaparin<br />
ensure:<br />
Refer to Anti Coagulation<br />
Nurse (ACN) for follow up.<br />
Blood results have been<br />
checked by ACN<br />
Arrange Doppler
APPENDIX 11<br />
Halton <strong>and</strong> St Helens<br />
St. Helens NHS Minor injuries /Walk-in Centre<br />
Widnes Walk in Centre<br />
High Risk<br />
Well’s score >3<br />
D- Dimer<br />
FBC, U&E, LFT, Coagulation<br />
screen, Glucose (if diabetic).<br />
Administer 1 st dose Enoxaparin<br />
Arrange:<br />
Referral to Anti Coagulation<br />
nurse (ACN) for follow up.<br />
Doppler<br />
Prior to 2 nd dose Enoxaparin<br />
ensure:<br />
Blood results have been<br />
checked by practitioner<br />
Page 30 <strong>of</strong> 40
APPENDIX 12<br />
Halton <strong>and</strong> St Helens<br />
St. Helens NHS Minor injuries /Walk-in Centre<br />
Widnes Walk in Centre<br />
High Risk<br />
Well’s score >3<br />
D- Dimer FBC, U&E, LFT,<br />
Coagulation screen, Glucose (if<br />
diabetic).<br />
Administer 1 st dose Enoxaparin<br />
Arrange:<br />
Referral to Anti Coagulation<br />
nurse (ACN) for follow up.<br />
Doppler<br />
Prior to 2<br />
Blood results have been<br />
checked by practitioner<br />
nd dose Enoxaparin<br />
ensure:<br />
Page 31 <strong>of</strong> 40
APPENDIX 13<br />
Information for patients attending with<br />
<strong>Suspected</strong> <strong>Deep</strong> <strong>Vein</strong> <strong>Thrombosis</strong><br />
Halton <strong>and</strong> St Helens<br />
St Helens MIU/WIC <strong>and</strong> Widnes WIC<br />
Your Doctor has referred you to the Walk-In centre because there is the possibility that you<br />
may have a blood clot in your leg. To find out if this is the case we will discuss with you how to<br />
diagnose your condition. This may include a physical examination, a blood test <strong>and</strong> possibly a<br />
scan <strong>of</strong> your leg at Whiston hospital.<br />
If we believe a blood clot is a strong possibility you may be <strong>of</strong>fered an injection <strong>of</strong> a “blood<br />
thinning” drug called Enoxaparin. If a clot is present this helps to stop it from getting any larger.<br />
If you receive a scan <strong>of</strong> your leg, but we do not find a clot, an anticoagulant nurse will discuss<br />
with you your risk factors <strong>of</strong> having a clot. If you are felt to have risk factors the scan would<br />
usually be repeated in one week.<br />
If the scan finds a clot you would usually be started on Warfarin, another type <strong>of</strong> “blood<br />
thinning” drug. You would be <strong>of</strong>fered education <strong>and</strong> information through the Anticoagulation<br />
Nurse at Whiston Hospital, <strong>and</strong> provide follow up by a consultant regarding your care <strong>and</strong> drug<br />
treatment.<br />
The risk factors <strong>of</strong> having a clot are:<br />
Previous clots<br />
Recent long haul flights<br />
Recent surgery<br />
Immobility<br />
Family history <strong>of</strong> clots<br />
Pregnancy (If you have a positive scan Warfarin will not be started, you will remain on<br />
Clexane).<br />
Please note that it is advised you do not drive until we have a diagnosis or you are pain free.<br />
We recommend you elevate your legs whilst sitting <strong>and</strong> gently mobilise – but if pain increases<br />
on exercise please rest. You are advised to refrain from sporting activities <strong>and</strong> may find it<br />
necessary to take time <strong>of</strong>f work.<br />
Contact numbers for:<br />
Anticoagulant nurse, Whiston 0151 430 1845<br />
St Helen’s Minor injuries/ Walk-In Centre 01744 627400<br />
Widnes Walk in Centre Reception 0151 495 5000<br />
Page 32 <strong>of</strong> 40
APPENDIX 14<br />
Halton <strong>and</strong> St Helens<br />
St. Helens Minor Injuries Unit/NHS Walk-in Centre<br />
Widnes Walk in Centre<br />
Information for patients receiving Enoxoparin (Clexane)<br />
What is Enoxoparin?<br />
Enoxoparin belongs to a group <strong>of</strong> medicines called Low Molecular Weight Heparins.<br />
What is Enoxoparin used for?<br />
Enoxoparin is used to prevent unwanted blood clots from forming in veins <strong>and</strong> to break up blood<br />
clots that have already developed in veins.<br />
How is Enoxoparin given?<br />
Enoxoparin is injected under your skin. The nurse in the Walk-In Centre will administer<br />
your injection.<br />
The nurse will tell you when to attend for your next injection.<br />
It is important that you attend on the time <strong>and</strong> date arranged for any follow-up injections.<br />
Does Enoxoparin have side-effects?<br />
As well as benefits, a medicine may occasionally cause some unwanted effects in some<br />
patients. These are called side-effects.<br />
Side effects <strong>of</strong> Enoxoparin may include:<br />
Pain, bruising <strong>and</strong> mild local irritation at the site <strong>of</strong> injection.<br />
Rarely, hard nodules or lumps at the site <strong>of</strong> the injection, these usually resolve after a<br />
few days.<br />
Skin rashes<br />
Itching<br />
Bleeding disorders, bruising, pain or tenderness in your abdomen, joint pains.<br />
Rarely, hair loss.<br />
If you experience any unusual bleeding, develop any abdominal pain or feel unwell with any<br />
allergic skin rashes or difficulty breathing, attend Accident <strong>and</strong> Emergency immediately. If<br />
you have any questions or concerns regarding your treatment with Enoxoparin please ask<br />
the nurse at the St Helens Minor Injuries Unit/ NHS Walk-In Centre.<br />
OR<br />
Page 33 <strong>of</strong> 40
Telephone:<br />
Anti-Coagulant Nurses on 0151 430 1845 (9am-5pm Mon-Fri)<br />
St Helens Minor Injuries Unit/NHS Walk-In Centre 01744 627400<br />
Widnes Walk in Centre 0151 495 500<br />
NHS Direct 08454647<br />
Page 34 <strong>of</strong> 40
APPENDIX 15<br />
Click here to view <strong>and</strong> print the form<br />
NEW REFERRAL FORM<br />
FOR DIRECT ACCESS OF PATIENT WITH SUSPECTED DEEP VEIN THROMBOSIS<br />
St Helens MIU/WIC <strong>and</strong> Widnes WIC<br />
This form is an integral part <strong>of</strong> the DVT pathway <strong>and</strong> therefore should be completed in full.<br />
Failure to do so may result in the patient being referred back to original source depending on<br />
patient’s clinical need.<br />
PATIENTS DETAILS<br />
SURNAME FIRST NAME<br />
………………………………………. ……………………………………<br />
ADDRESS<br />
………………………………………………………………………………………………………………<br />
………………………………………………………………………………………………………………<br />
…………………………………………………………<br />
TEL NUMBER DATE OF BIRTH<br />
…………………………………… ………………………………….<br />
GP NAME / PRACTICE<br />
………………………………………………………………………………………………………………<br />
………………………………………………………………………………………………………………<br />
…………………………………………………………<br />
TEL NUMBER ………………………………………<br />
Brief history <strong>of</strong> presenting complaint /problem<br />
………………………………………………………………………………………………………………<br />
………………………………………………………………………………………………………………<br />
………………………………………………………………………………………………………………<br />
…………………………<br />
Are there any social factors that would prevent the patients frequent return ie mobility or<br />
transport<br />
issues………………………………………………………………………………………………………<br />
Page 35 <strong>of</strong> 40
………………………………………………………………………………………………………………<br />
…………………………………………………………<br />
WELLS SCORE = …………..<br />
Paralysis/paresis/plaster immobilisation <strong>of</strong> lower limbs +1<br />
Bedridden >3 days, major surgery in 4 hrs +1<br />
Active cancer – treatment in previous 6/12 or on palliative treatment +1<br />
Entire leg swollen +1<br />
Calf swollen >3cm (measure 10cm below tibial tuberoscity) +1<br />
L= ……….cm R = ………..cm<br />
Tenderness along deep veins +1<br />
Pitting oedema worse in symptomatic leg +1<br />
Collateral superficial vein ( non varicose) +1<br />
Alternative diagnosis more likely than DVT -2<br />
If a DVT is excluded, what management plan would you advise<br />
Home care Own Analgesia Review with GP in 24hrs<br />
Review with GP in 48 hrs ---------------------please circle<br />
Page 36 <strong>of</strong> 40
APPENDIX 16<br />
Patients excluded from this service<br />
Surgery within the last 4 weeks yes<br />
Children under 16 years old yes<br />
Currently suspected <strong>of</strong> / previous pulmonary embolus yes<br />
Intravenous Drug user yes<br />
Alcohol Dependence yes<br />
Known diagnoses <strong>of</strong> malignant disease yes<br />
Pregnant <strong>and</strong> < 6 weeks post partum yes<br />
Known renal impairment yes<br />
Known hepatic impairment/ severe liver disease yes<br />
known bleeding disorder<br />
(haemophilia/thrombocytopenia)<br />
yes<br />
Pt who have had any type <strong>of</strong> stroke in the last 12 mths yes<br />
Pt who have had neuro or ophthalmic surgery after<br />
major trauma within the past 12 mths<br />
yes<br />
Pt who have diabetic retinopathy yes<br />
Pt with prosthetic heart valves yes<br />
Pt who have had an active oesophageal , gastric,<br />
duodenal ulceration in the last 12 mths<br />
Patients taking the following drugs area also excluded from the PGD <strong>and</strong> should be<br />
referred through usual channels (single point access/GPAU).<br />
Dipyridamole<br />
Dextran<br />
Thrombolytics<br />
Anti coagulation<br />
Drotrecogin alfa<br />
Iioprost<br />
Sibutramine<br />
Systemic glucocorticoids<br />
If you are unsure <strong>of</strong> whether the patient meets the criteria, please ring <strong>and</strong> speak to a member<br />
<strong>of</strong> MIU/WIC Team 01744 627403/627426<br />
Page 37 <strong>of</strong> 40<br />
yes
APPENDIX 17<br />
Patients excluded from community DVT service<br />
to be used in conjunction with PGD<br />
Surgery within the last 4 weeks yes<br />
Children under 16 years old yes<br />
Currently suspected <strong>of</strong> / previous pulmonary embolus yes<br />
Intravenous Drug user yes<br />
Alcohol Dependence yes<br />
Known diagnoses <strong>of</strong> malignant disease yes<br />
Pregnant <strong>and</strong> < 6 weeks post partum yes<br />
Known renal impairment yes<br />
Known hepatic impairment/ severe liver disease yes<br />
known bleeding disorder<br />
(haemophilia/thrombocytopenia)<br />
yes<br />
Pt who have had any type <strong>of</strong> stroke in the last 12 mths yes<br />
Pt who have had neuro or ophthalmic surgery after<br />
major trauma within the past 12 mths<br />
yes<br />
Pt who have diabetic retinopathy yes<br />
Pt with prosthetic heart valves yes<br />
Pt who have had an active oesophageal , gastric,<br />
duodenal ulceration in the last 12 mths<br />
yes<br />
Halton <strong>and</strong> St Helens<br />
Patients taking the following drugs area also excluded from the PGD <strong>and</strong> should be<br />
referred through usual channels (single point access/GPAU).<br />
Dipyridamole<br />
Dextran<br />
Thrombolytics<br />
Anti coagulation<br />
Drotrecogin alfa<br />
Iioprost<br />
Sibutramine<br />
Systemic glucocorticoids<br />
Page 38 <strong>of</strong> 40
APPENDIX 18<br />
EQUALITY IMPACT ASSESSMENT TOOL<br />
To be completed with the policy document when submitted to the appropriate committee for<br />
consideration, approval <strong>and</strong> ratification.<br />
1. Does the policy/guidance affect one group less or<br />
more favourably than another on the basis <strong>of</strong>:<br />
Race NO<br />
Ethnic origins (including gypsies <strong>and</strong> travellers) NO<br />
Nationality NO<br />
Gender NO<br />
Culture NO<br />
Religion or belief NO<br />
Sexual orientation including lesbian, gay <strong>and</strong><br />
bisexual people<br />
Yes/No Comments<br />
NO<br />
Age NO<br />
Disability - learning disabilities, physical disability,<br />
sensory impairment <strong>and</strong> mental health problems<br />
2. Is there any evidence that some groups are<br />
affected differently?<br />
3. If you have identified potential discrimination, are<br />
there any exceptions valid, legal <strong>and</strong>/or<br />
justifiable?<br />
4. Is the impact <strong>of</strong> the policy/guidance likely to be<br />
negative?<br />
5. If so can the impact be avoided? NA<br />
6. What alternative are there to achieving the<br />
policy/guidance without the impact?<br />
7. Can we reduce the impact by taking different<br />
action?<br />
If you have identified a potential discriminatory impact <strong>of</strong> this policy document, please refer it to<br />
Jenny Murphy, together with any suggestions as to the action required to avoid/reduce this<br />
impact. For advice in respect <strong>of</strong> answering the above questions, please contact Jenny Murphy.<br />
Page 39 <strong>of</strong> 40<br />
NO<br />
NO<br />
NA<br />
NA<br />
NA<br />
NA
APPENDIX 19<br />
DISSEMINATION AND TRAINING PLAN<br />
To be completed with the policy document when submitted to the appropriate committee for<br />
consideration, approval <strong>and</strong> ratification.<br />
The status column must be given a Red, Amber or Green rating with evidence to demonstrate<br />
an action has been completed.<br />
DISSEMINATION PLAN<br />
Title <strong>of</strong> document:<br />
<strong>Diagnosis</strong> <strong>and</strong> <strong>Treatment</strong> <strong>of</strong> Patients with<br />
a <strong>Suspected</strong> <strong>Deep</strong> <strong>Vein</strong> <strong>Thrombosis</strong><br />
Policy<br />
Dissemination Lead: (Print name <strong>and</strong><br />
contact details)<br />
Jenny Murphy<br />
Proposed action to retrieve out-<strong>of</strong>-date<br />
copies <strong>of</strong> the document:<br />
Date finalised:<br />
February 2010<br />
To be disseminated to: Disseminated<br />
by whom?<br />
TRAINING PLAN<br />
Previous document already being used? Yes (Please delete as<br />
appropriate)<br />
If yes, in what format <strong>and</strong> where?<br />
Paper Copy St Helens MIU/WIC<br />
Jenny<br />
Murphy<br />
Event (Please provide details <strong>of</strong> available training venues/dates to<br />
educate staff about this policy document)<br />
Page 40 <strong>of</strong> 40<br />
Timescale<br />
(Date)<br />
Within a<br />
month<br />
Training for staff will be provided in the MIU/WIC ( St Helens <strong>and</strong> Widnes )<br />
in scheduled sessions<br />
Training Plan Lead (Please provide details <strong>of</strong> staff who will be<br />
responsible for overseeing this training)<br />
Jenny Murphy Advanced Practitioner<br />
Elaine McDowell Clinical Service Manager<br />
Additional information (Please provide details <strong>of</strong> any processes in place<br />
to support implementation)<br />
Status<br />
R A G<br />
Paper<br />
or<br />
Electronic<br />
Comments<br />
Timescale Owner Status<br />
R A G<br />
Denotes: Action not yet taken or deadline for action not met. Action plan to address this must be provided.<br />
Denotes: Action partially implemented.<br />
Denotes: Action complete.