

Prenatal Screening for Fetal Aneuploidy in Singleton ... - SOGC
Prenatal Screening for Fetal Aneuploidy in Singleton ... - SOGC
Prenatal Screening for Fetal Aneuploidy in Singleton ... - SOGC

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
described an association between an <strong>in</strong>creased size of the<br />
nuchal translucency on the 11- to 14-week fetal ultrasound<br />
scan and an <strong>in</strong>creased risk of fetal Down syndrome. 18<br />
Several large studies have shown that NT has a DR <strong>for</strong><br />
Down syndrome rang<strong>in</strong>g from 69% to 75%, with an<br />
FPR of 5% to 8.1%. 5,10,19 This marker is associated with<br />
other numeric chromosome abnormalities, other fetal<br />
anomalies such as cardiac defects or diaphragmatic hernia,<br />
and a number of s<strong>in</strong>gle gene disorders, particularly those<br />
associated with decreased fetal movement. An NT above<br />
the 99th percentile has a sensitivity of 31% and specificity<br />
of 98.7% <strong>for</strong> major congenital heart defects when the<br />
fetal karyotype is normal. One <strong>in</strong> 33 fetuses with an NT<br />
above the 95th percentile (above 2.2 to 2.8 mm depend<strong>in</strong>g<br />
on gestational age) and 1 <strong>in</strong> 16 with an NT above the 99th<br />
percentile (≥ 3.5 mm regardless of gestational age) have a<br />
major cardiac defect detected. 20 F<strong>in</strong>d<strong>in</strong>g an <strong>in</strong>creased NT<br />
at 11 to 14 weeks’ gestation with a normal fetal karyotype<br />
warrants offer<strong>in</strong>g a detailed ultrasound exam<strong>in</strong>ation at<br />
<strong>Prenatal</strong> <strong>Screen<strong>in</strong>g</strong> <strong>for</strong> <strong>Fetal</strong> <strong>Aneuploidy</strong> <strong>in</strong> S<strong>in</strong>gleton Pregnancies<br />
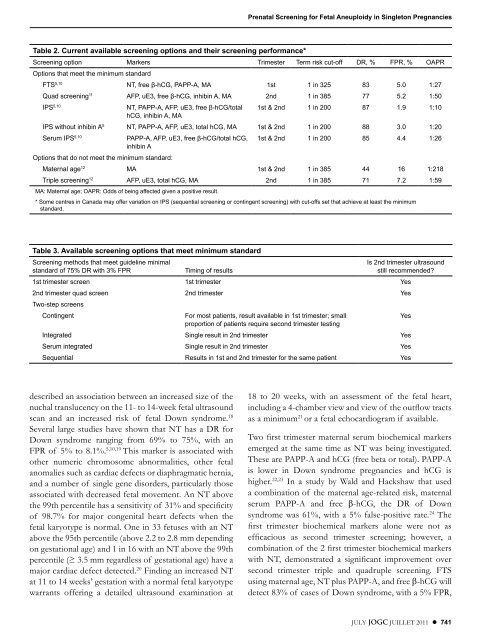
Table 2. Current available screen<strong>in</strong>g options and their screen<strong>in</strong>g per<strong>for</strong>mance*<br />
<strong>Screen<strong>in</strong>g</strong> option Markers Trimester Term risk cut-off DR, % FPR, % OAPR<br />
Options that meet the m<strong>in</strong>imum standard<br />
FTS5,10 NT, free β-hCG, PAPP-A, MA 1st 1 <strong>in</strong> 325 83 5 .0 1:27<br />
Quad screen<strong>in</strong>g11 AFP, uE3, free β-hCG, <strong>in</strong>hib<strong>in</strong> A, MA 2nd 1 <strong>in</strong> 385 77 5 .2 1:50<br />
IPS5,10 NT, PAPP-A, AFP, uE3, free β-hCG/total<br />
hCG, <strong>in</strong>hib<strong>in</strong> A, MA<br />
1st & 2nd 1 <strong>in</strong> 200 87 1 .9 1:10<br />
IPS without <strong>in</strong>hib<strong>in</strong> A5 NT, PAPP-A, AFP, uE3, total hCG, MA 1st & 2nd 1 <strong>in</strong> 200 88 3 .0 1:20<br />
Serum IPS5,10 PAPP-A, AFP, uE3, free β-hCG/total hCG,<br />
<strong>in</strong>hib<strong>in</strong> A<br />
1st & 2nd 1 <strong>in</strong> 200 85 4 .4 1:26<br />
Options that do not meet the m<strong>in</strong>imum standard:<br />
Maternal age12 MA 1st & 2nd 1 <strong>in</strong> 385 44 16 1:218<br />
Triple screen<strong>in</strong>g12 AFP, uE3, total hCG, MA 2nd 1 <strong>in</strong> 385 71 7 .2 1:59<br />
MA: Maternal age; OAPR: Odds of be<strong>in</strong>g affected given a positive result .<br />
* Some centres <strong>in</strong> Canada may offer variation on IPS (sequential screen<strong>in</strong>g or cont<strong>in</strong>gent screen<strong>in</strong>g) with cut-offs set that achieve at least the m<strong>in</strong>imum<br />
standard .<br />
Table 3. Available screen<strong>in</strong>g options that meet m<strong>in</strong>imum standard<br />
<strong>Screen<strong>in</strong>g</strong> methods that meet guidel<strong>in</strong>e m<strong>in</strong>imal<br />
Is 2nd trimester ultrasound<br />
standard of 75% DR with 3% FPR Tim<strong>in</strong>g of results<br />
still recommended?<br />
1st trimester screen 1st trimester Yes<br />
2nd trimester quad screen<br />
Two-step screens<br />
2nd trimester Yes<br />
Cont<strong>in</strong>gent For most patients, result available <strong>in</strong> 1st trimester; small<br />
proportion of patients require second trimester test<strong>in</strong>g<br />
Yes<br />
Integrated S<strong>in</strong>gle result <strong>in</strong> 2nd trimester Yes<br />
Serum <strong>in</strong>tegrated S<strong>in</strong>gle result <strong>in</strong> 2nd trimester Yes<br />
Sequential Results <strong>in</strong> 1st and 2nd trimester <strong>for</strong> the same patient Yes<br />
18 to 20 weeks, with an assessment of the fetal heart,<br />
<strong>in</strong>clud<strong>in</strong>g a 4-chamber view and view of the outflow tracts<br />
as a m<strong>in</strong>imum 21 or a fetal echocardiogram if available.<br />
Two first trimester maternal serum biochemical markers<br />
emerged at the same time as NT was be<strong>in</strong>g <strong>in</strong>vestigated.<br />
These are PAPP-A and hCG (free beta or total). PAPP-A<br />
is lower <strong>in</strong> Down syndrome pregnancies and hCG is<br />
higher. 22,23 In a study by Wald and Hackshaw that used<br />
a comb<strong>in</strong>ation of the maternal age-related risk, maternal<br />
serum PAPP-A and free β-hCG, the DR of Down<br />
syndrome was 61%, with a 5% false-positive rate. 24 The<br />
first trimester biochemical markers alone were not as<br />
efficacious as second trimester screen<strong>in</strong>g; however, a<br />
comb<strong>in</strong>ation of the 2 first trimester biochemical markers<br />
with NT, demonstrated a significant improvement over<br />
second trimester triple and quadruple screen<strong>in</strong>g. FTS<br />
us<strong>in</strong>g maternal age, NT plus PAPP-A, and free β-hCG will<br />
detect 83% of cases of Down syndrome, with a 5% FPR,<br />
JULY JOGC JUILLET 2011 l 741













