Baby Friendly Community Initiative - MEDiCAM
Baby Friendly Community Initiative - MEDiCAM
Baby Friendly Community Initiative - MEDiCAM

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Baby</strong> <strong>Friendly</strong><br />
<strong>Community</strong> y <strong>Initiative</strong><br />
(BFCI) ( (BFCI) )<br />
CHEA Mary, MD, MHID<br />
National National Nutrition Programme<br />
National Maternal & Child Health Center<br />
Mt Maternal l&Child & Child<br />
Health<br />
O Outline tli<br />
Maternal & Child Health in Cambodia<br />
Infant and Young Child Feeding (IYCF)<br />
<strong>Baby</strong> <strong>Baby</strong> <strong>Friendly</strong> <strong>Friendly</strong> <strong>Community</strong> <strong>Community</strong> <strong>Initiative</strong> <strong>Initiative</strong> (BFCI)<br />
(BFCI)<br />
140<br />
120<br />
Current IYCF <strong>Community</strong> <strong>Community</strong>-based based activities<br />
What is <strong>Baby</strong> <strong>Baby</strong>-<strong>Friendly</strong> <strong>Friendly</strong> <strong>Community</strong> <strong>Initiative</strong>?<br />
(BFCI)<br />
BFCI Implementation Package<br />
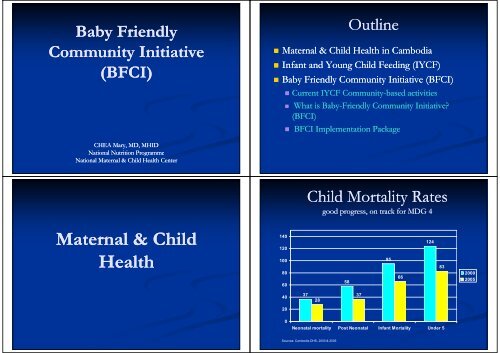
Child Mortality Rates<br />
good progress, on track for MDG 4<br />
100<br />
95<br />
83<br />
80<br />
60<br />
58<br />
66<br />
2000<br />
2005<br />
40<br />
20<br />
0<br />
37<br />
28<br />
37<br />
124<br />
Neonatal mortality Post Neonatal Infant Mortality Under 5<br />
Sources: Cambodia DHS, 2000 & 2005
120<br />
100<br />
80<br />
60<br />
40<br />
20<br />
0<br />
Child Mortality Rates<br />
106<br />
Myyanmar<br />
83 83<br />
Cammbodia<br />
still ill among the h hi highest h i in the h region i<br />
Laao<br />
PDR<br />
38<br />
Indoonesia<br />
Number of under five deaths per 1,000 live births<br />
34 31<br />
Philipppines<br />
China<br />
23 21<br />
‐ 40,000 children under 5 die every year in Cambodia, out of them 10,000 die in the<br />
first month of life<br />
Bb <strong>Baby</strong> If Infant and dY Young<br />
Child Child F Feeding di (IYCF)<br />
Vieet<br />
Nam<br />
Thhailand<br />
12<br />
Maalaysia<br />
3<br />
Singgapore<br />
Undernutrition in Young g Children<br />
some improvements, but still unacceptably high<br />
Trends in the Prevalence of Child Malnutrition<br />
Cambodia 1996-2008<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
59<br />
49<br />
44<br />
40<br />
13 17<br />
8 9<br />
43<br />
40<br />
28 29<br />
Stuntingg Wastingg Underweight g<br />
1996 2000 2005 2008<br />
Source: WHO Global Database on Child Growth and Malnutrition 2007<br />
Wasting & underweight are the most responsive to short-term changes.<br />
This suggests gg that the decline in child malnutrition has now stagnated g<br />
and possibly started to reverse.<br />
Infant and Young Child Feeding Program<br />
Goal<br />
To Improve the survival and well being of infants and young<br />
children by improving their nutritional status, growth, and<br />
development through optimal feeding
Infant and Young Child Feeding Program<br />
Objectives<br />
1. To increase early initiation of brestfeeding within 1 hour of delivery<br />
2. To increase exclusive breastfeeding of infants < 6 months old<br />
3. To Improve appropriate complementary feeding starting at 6 months of age<br />
with continued breastfeeding for at least two years or beyond<br />
4. To support the provision of appropriate care for sick and malnourished<br />
children<br />
80<br />
70<br />
60<br />
50<br />
30<br />
Breastfeeding g Practices<br />
Significant increase in early and exclusive breastfeeding<br />
Trends in early breastfeeding rates, 2000-2005<br />
35 35.1 1<br />
24.4<br />
68.3<br />
40 CDHS 2000<br />
20<br />
10<br />
0<br />
11 11<br />
Early breastfeeding - Early Breastfeeding - Exclusive<br />
within 1 hour within 1 day Breastfeeding<br />
60<br />
CDHS 2005<br />
Source: CDHS 2000 & 2005<br />
Infant and Young g Child Feeding g<br />
Approaches and Strategies<br />
Policy Policy and and legal environment: Sub Sub-decree Sub Sub-decree decree on on Marketing Marketing of Products for IYCF<br />
and National Policy on IYCF<br />
Facility Facility-based based provision of quality IYCF services: Changes in hospital<br />
policies/actions through the the establishment establishment of of <strong>Baby</strong> <strong>Baby</strong> <strong>Friendly</strong> <strong>Friendly</strong> Hospital Hospital <strong>Initiative</strong><br />
<strong>Initiative</strong><br />
(BFHI), management of severe malnutrition and IYCF counseling at health<br />
facilities through in-service in service and pre pre-service service training<br />
<strong>Community</strong><br />
<strong>Community</strong>-based y based activities: <strong>Community</strong> ommunity y nutrition interventions and the<br />
establishment of <strong>Baby</strong> <strong>Friendly</strong> <strong>Community</strong> <strong>Initiative</strong> (BFCI)<br />
Advocacy and communication strategy strategy: Use se of communication strategy,<br />
including g mass media and behavior change g communications (e.g. ( g World<br />
Breastfeeding Week celebration)<br />
Exclusive Breastfeeding for Infants 00-5<br />
5 months<br />
100<br />
90<br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
11<br />
60<br />
CDHS 2000 CDHS 2005 CAS 2008<br />
49<br />
62<br />
66<br />
40<br />
71<br />
All<br />
Urban<br />
RRural l<br />
Exclusive breastfeeding rate increases from 60% in 2005 to 66% in 2008. But decreases in urban areas.
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
Breastfeeding Competitors<br />
Competitors<br />
57 57.2 2 55 55.7 7<br />
existing and emerging issues<br />
36 3.6 52 5.2<br />
1.7 36 3.6<br />
Prelacteal Breastfeeding No<br />
feeding and breastmilk<br />
substitutes<br />
breastfeeding<br />
CDHS 2000 CDHS 2005<br />
Bb <strong>Baby</strong> Fi <strong>Friendly</strong> dl<br />
C <strong>Community</strong> i I <strong>Initiative</strong> i i i<br />
(BFCI)<br />
months<br />
Age in<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
Complementary p y Feeding g<br />
inadequate complementary feeding<br />
33<br />
44<br />
61.7<br />
46.8<br />
6-8 9-11 12-17 18-23<br />
Percent of infants/children<br />
Currently breastfed, fed 3 or more food groups daily, and daily feeding frequency appropriate for age<br />
C Current tIYCF IYCF <strong>Community</strong> <strong>Community</strong>-based C it b bbased d activities ti iti<br />
Source: Cambodia DHS 2005<br />
World Breastfeeding Week: since 2001, conducted at all levels<br />
<strong>Community</strong> nutrition nutrition and and IYCF IYCF education education conducted conducted by by HC<br />
HC<br />
staff, NGOs and village volunteers<br />
Establishment of of <strong>Baby</strong> <strong>Baby</strong> <strong>Friendly</strong> <strong>Friendly</strong> <strong>Community</strong> <strong>Community</strong> <strong>Initiative</strong> <strong>Initiative</strong> (BFCI)<br />
(BFCI)<br />
Cooking Demonstration World Breastfeeding Week
What is <strong>Baby</strong> <strong>Baby</strong>-<strong>Friendly</strong> <strong>Baby</strong> <strong>Baby</strong>-<strong>Friendly</strong> <strong>Friendly</strong> <strong>Community</strong> <strong>Initiative</strong>?<br />
<strong>Initiative</strong>?<br />
(BFCI)<br />
<strong>Community</strong> <strong>Community</strong>-based based initiative to<br />
support, promote, and d protect<br />
breastfeeding and to promote<br />
appropriate appropriate complementary complementary feeding<br />
feeding<br />
Main components: Breastfeeding,<br />
Adequate Complementary Complementary Feeding, Feeding<br />
Maternal nutrition, Early Childhood<br />
and Development, Development, p and hygiene yg<br />
Works through formation and<br />
training of “Mother Mother Support Group Group”<br />
at the village level<br />
Close links to Health Centers<br />
BFCI Implementation Package<br />
BFCI Implementation I l t ti Guidelines G id li Communication C CCommunication i ti & &Ad Advocacy<br />
BFCI Training Modules<br />
1. Introduction<br />
2. How to Establish & Maintain<br />
<strong>Baby</strong> <strong>Baby</strong>-<strong>Friendly</strong> <strong>Friendly</strong> <strong>Community</strong><br />
3P 3. Partners<br />
4. Roles & Responsibilities<br />
5. Monitoring & Evaluation<br />
Curricula for training all<br />
partners, staff, and<br />
volunteers involved with<br />
BFCI<br />
1. BFCI Flipchart<br />
2. Advocacy Materials<br />
<strong>Baby</strong> <strong>Baby</strong>-<strong>Friendly</strong> <strong>Friendly</strong> <strong>Community</strong> <strong>Initiative</strong> (BFCI)<br />
2000 2000-2007 2007<br />
IYCF promotion at<br />
community level began in<br />
2000<br />
“BFCI BFCI” began in 2004<br />
By end of 2007, over 3,360<br />
villages “<strong>Baby</strong> <strong>Baby</strong>-<strong>Friendly</strong> <strong>Friendly</strong>”<br />
villages ill (or ( about b t 20% 20% of f all ll<br />
villages in Cambodia) in 12<br />
provinces<br />
Implemented with support<br />
from o UN UNICEF, C F,C CARE, ,<br />
RACHA, and others<br />
Mother Support Group and health officials<br />
in Kampong Thom Province, Province 2007<br />
o UN C F,C ,<br />
Results achieved (BFCI ( monitoring g data, , UNICEF Jan-Aug g 2007): )<br />
- Early Breastfeeding in <strong>Baby</strong> <strong>Friendly</strong> Villages: 72%<br />
- Exclusive Breastfeeding rate in <strong>Baby</strong> <strong>Friendly</strong> Villages: 79%<br />
Steps for Establishing <strong>Baby</strong> <strong>Baby</strong>-<strong>Friendly</strong> <strong>Friendly</strong> Communities<br />
Select Health Centers, build partnerships with Commune<br />
St Step 1: 1 CCouncils, il and d train i HC and d CWCFP<br />
Step 2:<br />
Step 3:<br />
Step 4:<br />
Select BFCI villages<br />
Orient community leaders (village chiefs) to BFCI<br />
Orient existing VHSG members to BFCI<br />
Step 5:<br />
Select and train BFCI volunteers ol nteers
Criteria for maintaining BFCI<br />
Criteria 1: Participation of Commune Council<br />
- At least 2 supervision visits per year to each BFCI village<br />
- Participation in annual planning and review meetings with HC staff<br />
- Comm Commune ne Council Co ncil ffunding nding or tangible ssupport pport<br />
Criteria 2: Regular meetings for BFCI volunteers and follow-up after training<br />
- All BFCI FC volunteers vo u tee s meet eet at the t e health ea t center ce te at least east 2 times t es per pe year yea<br />
- Follow-up from the BFCI training is incorporated into all regular meetings at the health center<br />
that involve BFCI volunteers (VHSG, TBA, BFCI, etc). Follow-up topics may include (but are<br />
not limited to) review of technical information and recommendations, recommendations feedback from volunteers<br />
and problem solving, supervision for reporting forms as needed, etc.<br />
Criteria 3: Monitoring and Supervision<br />
Two reports per year from the village to the health center<br />
At least two supervision visits per year from the Health Center staff to each BFCI village<br />
Cit Criteria i 44: Regular R l Trainings T i i for f BFCI volunteers l t<br />
Existing BFCI volunteers are re-trained every 2 years.Once a year, the complete training is<br />
offered to replacement volunteers (new volunteers that replace drop-out volunteers).<br />
Criteria 5: Targeted home visits and monthly “<strong>Baby</strong>-<strong>Friendly</strong> Gatherings”<br />
Mother Support Group (MSG) completes the monthly monitoring forms (Form 1) for all<br />
children under 1 year of age, age every month. month<br />
Supervision reports/checklists from HC staff and CWCFP confirm that the MSG has organized<br />
at least 4 “<strong>Baby</strong> <strong>Friendly</strong> Gatherings” in the community in one year.<br />
Monitoring g and Evaluation of BFCI<br />
All partners implementing BFCI should report every six six-months months (April<br />
and October) to the BFCI Coordinator at the National Nutrition<br />
Program<br />
The key “<strong>Baby</strong> “<strong>Baby</strong>-<strong>Friendly</strong>” <strong>Friendly</strong>” indicators include:<br />
1. Proportion of infants who are put to the breast within 1 hour after<br />
delivery (early initiation of breastfeeding) (0 (0-11.9 11.9 months of age)<br />
2P 2. Proportion i of fif infants that h are exclusively l i l breastfed b fdi in the h first fi 6 6 months h<br />
of life (0 (0-5.9 5.9 months of age)<br />
3 3. Proportion P i of f children hild who h receive i any pre pre-lacteal l llacteal lf feeds d<br />
4. Proportion of children aged 66-9<br />
9 months who receive complementary<br />
f food d( (semi (semi-solid i solid lid or solid) lid) in i addition dditi to t breastmilk. b t ilk<br />
5. Proportion of children aged 66-12<br />
12 months of age who ate any animal<br />
products in the last 24 24 hours. hours<br />
Roles and Responsibilities p of Key y<br />
Players in BFCI<br />
Responsibilities p of Mother Support pp Group p<br />
Commune Council, Committee for Women and Children<br />
Focal Point Point (CWCFP)<br />
(CWCFP)<br />
Health Center staff<br />
Operational District<br />
Provincial Provincial Health Department<br />
National National- BFCI Coordinator at National Nutrition Program<br />
M Monitoring i i and dE Evaluation l i of f BFCI(C BFCI (Con’t) ’ )<br />
NNP will also collect programmatic indicators every six<br />
months (April and October) on the following:<br />
1. Number of BFCI villages g<br />
2. Number of Health Centers trained in BFCI<br />
3. Number of Operational Districts implementing BFCI<br />
4. Number Number of of BFCI BFCI trainings trainings conducted conducted in in the the last last 6<br />
6<br />
months<br />
5 5. Number N b of f BFCI BFCI volunteers l trained i d in i the h last l 6<br />
6<br />
months
Evaluation E EEvaluation l ti of f BFCI<br />
BFCI<br />
Evaluation of BFCI should be conducted by an<br />
external evaluation team.<br />
This should be done every two to three years.<br />
The method method of of the the evaluation evaluation should should be to to survey survey a<br />
a<br />
random selection of BFCI and non non-BFCI BFCI villages, with<br />
a sample p size that will y yield meaningful g comparisons p of<br />
the key indicators in BFCI and non non-BFCI BFCI areas.<br />
This is also an opportunity pp y to collect more detailed<br />
information on child feeding practices, food availability,<br />
household economic status, access to health services,<br />
and other related factors according to the UNICEF<br />
conceptual framework of child health and nutrition.<br />
T Trainings i i for f BFCI<br />
BFCI<br />
BFCI Training of Trainers to<br />
PHD/OD: 6 6 day. day<br />
The optimal number of participants<br />
for a a TOT TOT is is 8 8 to to 12 12 participants. participants<br />
All 27 Lessons are used in the BFCI<br />
TOT<br />
BFCI Training of Trainers to HC<br />
& CCWC staff: staff: 6 6 day<br />
day<br />
BFCI Training to Mother Support<br />
Gro Group: p: 5 day<br />
Flow of Trainings for BFCI<br />
Master Trainers (NNP)<br />
(TOT)<br />
National level MOH<br />
and NGO staff<br />
(TOT)<br />
PHD and OD <strong>Community</strong> Leaders<br />
(1-day orientation)<br />
(TOT)<br />
Health Center Staff<br />
(MSG Training)<br />
Mother Support Group (MSG)<br />
Advocacy yMaterials &BFCI Flipchart p<br />
Flipchart messages developed based on key messages<br />
agreed g to by y IYCF Technical Working g Group p (NNP ( and<br />
partners)<br />
BFCI Advocacy Ad<br />
materials, including g cost<br />
estimates for establishing<br />
and maintaining BFCI<br />
(brief presentation and 1-<br />
page flyer will be<br />
included in in Section 3, 3<br />
“Partnerships”)
S Sample l of fB Budgeting d ti<br />
BBBudgeting Budgeting dd ii should should hh ldb ldbbe be covered covered ddto to the the hh<br />
following following gg activities: activities:<br />
Orient community leaders (CCWC, village chiefs) to BFCI<br />
Sl Select BFCI BFCI villages ill<br />
Train BFCI volunteers<br />
Supervision visits to community (HC, CCWC(?), OD,<br />
PHD PHD, etc) t )<br />
Annual BFCI review meeting (several HC together)<br />
Th Thank k you f for your attention<br />
tt ti<br />
Allocate Allocate funds funds for for ––<br />
What NGOs can help?<br />
p<br />
training for Mother Support Group volunteers on breastfeeding and<br />
complementary feeding,<br />
buying local foods foods- such as oil, vegetables, meat, iodized salt- salt for monthly<br />
mother’s meetings/cooking demonstration (no milk donations please! Mother’s<br />
milk is best)<br />
scales l f for weighing i hi children hild<br />
operational costs for MOH staff (PHD, OD, HC) and Commune Councils to<br />
supervise <strong>Baby</strong> <strong>Baby</strong>-<strong>Friendly</strong> <strong>Friendly</strong> <strong>Community</strong> activities<br />
Refer new mothers leaving hospitals to BFCI volunteers (Mother Support<br />
Group) in their communities (for (for BFHI BFHI hospital hospital staff) staff)<br />
Give supplementary training to BFCI volunteers on how to appropriately<br />
support s ppo HIV V positive pos ve women wo e in infant a feeding eed g in the e community co y (for (for ((<br />
PMTCT PMTCT staff) staff)