“Cath Lab Catastrophes: Management and Prevention” “Cath Lab ...
“Cath Lab Catastrophes: Management and Prevention” “Cath Lab ...
“Cath Lab Catastrophes: Management and Prevention” “Cath Lab ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
China Interventional Therapeutics (CIT) 2008<br />
March 20 -- 23, 2008<br />
Beijing, China<br />
<strong>“Cath</strong> <strong>Lab</strong> <strong>Catastrophes</strong>:<br />
<strong>Management</strong> <strong>and</strong> <strong>Prevention”</strong><br />
Fayaz Shawl, M.D., F.A.C.C.<br />
Clinical Professor of Medicine<br />
Director of Interventional Cardiovascular Medicine<br />
George Washington University - Washington, D.C.<br />
Director Interventional Cardiology<br />
Washington Adventist Hospital - Takoma Park, Maryl<strong>and</strong>
Faculty Disclosure<br />
Fayaz Shawl, M.D., F.A.C.C.<br />
Research/Grant Support:<br />
Cordis Corporation
Defensive Angioplasty<br />
Knowledge of clinical <strong>and</strong> morphologic factors<br />
relating to mortality <strong>and</strong> complications<br />
Do not overextend your capability<br />
Knowledge of complications relating to different<br />
devices<br />
Plan offensive strategy to h<strong>and</strong>le various anatomic<br />
subsets, plan defensive strategy if failure occurs<br />
Anticipate failure<br />
Review each complication (may prevent the next!)<br />
Record <strong>and</strong> monitor your results, review at frequent<br />
intervals
THE MORTAL RISK OF<br />
INTERVENTION IS MORE<br />
CLOSELY ASSOCIATED WITH<br />
COMPLEX PATIENTS<br />
THAN WITH<br />
COMPLEX LESIONS
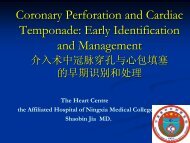
Complications of of Percutaneous Intervention: Elective Stenting<br />
Mortality<br />
20<br />
15<br />
10<br />
5<br />
0<br />
Risk Factors<br />
1. EF < 40<br />
Multivariate Correlates of In-Hospital Mortality<br />
2. Creatinine > 1.5<br />
3. Age > 70<br />
4. Triple Vessel Disease<br />
5. Unstable Angina<br />
0.35 0.16 0.52<br />
4.82<br />
3.57<br />
0 1 2 3 4 5<br />
No. of Risk Factors<br />
17.39<br />
N N = = 283 641 574 311 84 84 23 23<br />
(Number of of vessels dilated & & lesion morphology not significant)
Mayo Clinic Risk Risk Score Variables: Predictors of of<br />
Death, Q Q Wave MI, MI, Emergent or or Urgent CABG, CVA CVA<br />
Clinical Variables<br />
Age<br />
Cardiogenic shock<br />
S. creatinine > 265 µml/l (>3.5 mg/dl) or<br />
history of chronic or end stage renal disease<br />
Urgent or emergent procedure<br />
NYHA > 3 heart failure<br />
Angiographic Variables<br />
Thrombus<br />
Left main disease<br />
Multi-vessel disease<br />
Developed from learning set of 5,463 procedures, January 1996-December 1999.<br />
Validated in 1,781 procedures in 2000. Validated in 3,264 pts in NHLBI Dynamic Registry.<br />
Singh M. et al. JACC 2002;40:387-93<br />
Singh M. et al. JACC 2003;42:722-8
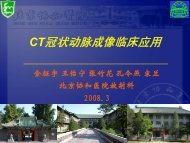
Major Complication Rate (%)<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
Risk:<br />
Risk Score:<br />
Mayo Clinic Risk Risk Score for for PCI PCI<br />
≤ 2<br />
Very Low<br />
0-5<br />
2-5<br />
Low<br />
6-8<br />
5-10<br />
Moderate<br />
9-11<br />
10-15<br />
High<br />
12-15<br />
JACC 2002;40:387<br />
≥ 25<br />
Very High<br />
>15<br />
Risk Factor:<br />
Age 90-99: 6<br />
Shock: 5<br />
Left main: 5<br />
Age 80-89: 5<br />
Age 70-79: 4<br />
Renal disease: 3<br />
Age 60-69: 3<br />
Non-elective<br />
procedure: 2<br />
MV Disease: 2<br />
NHYA > 3: 2<br />
Thrombus: 2<br />
Age 50-59: 2<br />
Age 40-49: 1
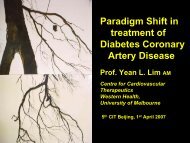
Lower Pre-Procedural Hemoglobin Level is Associated<br />
with Increased Risk of In-Hospital Mortality<br />
26,313 consecutive PCI, 9 hospitals, University of Michigan<br />
Hgb Level<br />
6.6-12.3<br />
12.3-13.5<br />
13.5-14.4<br />
14.4-15.4<br />
15.4-20.1<br />
All PCI Patients<br />
N = 24,554<br />
2.9%*<br />
1.6%<br />
1.1%<br />
0.9%<br />
1.1%<br />
Mortality, In-Hospital<br />
S. Beinart et al. Circ 2002;19:3700<br />
PCI with AMI (
Cath Cath <strong>Lab</strong> <strong>Lab</strong> Complications<br />
Prophylactic use of IABP <strong>and</strong> Integrilin
Cath Cath <strong>Lab</strong> <strong>Lab</strong> Complications
Cath Cath <strong>Lab</strong> <strong>Lab</strong> Complications<br />
Result
Cath Cath <strong>Lab</strong> <strong>Lab</strong> Complications
Cath Cath <strong>Lab</strong> <strong>Lab</strong> Complications<br />
Error of Omission - Post IVUS Evaluation
Coronary Dissection Following PCI PCI<br />
Causes<br />
Guide Catheter:<br />
L Amplatz Guide<br />
# 6 Fr. JR4 Guide!!<br />
Balloon/Stent Oversizing<br />
Overexpansion<br />
particularly on angle ><br />
45°<br />
Calcified Vessel<br />
Chronic Total Occlusion
Edge Edge Dissection Following Stenting<br />
Non-flowing limiting. Arc of dissection <<br />
90°<br />
STRUT Trial<br />
Incidence 17%; no in-hospital complications<br />
Hong, et al. - 327 pts<br />
Incidence 20.4%; no in-hospital complications<br />
6-month TLR 23.9 vs 22.3%<br />
SHERIS Trial - 150 pts<br />
Incidence 10.7%; 6-month TLR 25% vs 27%<br />
All tears healed by IVUS
Cath Cath <strong>Lab</strong> <strong>Lab</strong> Complications
Cath Cath <strong>Lab</strong> <strong>Lab</strong> Complications<br />
Recurrent Chest pain 6 hrs. post-PCI
Dissections Following Elective Coronary Stent<br />
Placement: Acute <strong>and</strong> <strong>and</strong> Long-Term Outcomes<br />
No<br />
Dissection<br />
Dissection<br />
A-B<br />
Dissection<br />
C-F<br />
No. 1426 101 52<br />
Pvalue<br />
30 Day: Death (%) 0 0 2 0.11<br />
Q AMI (%) 1 0 4 0.03<br />
Non Q AMI (%) 5 4 13 0.007<br />
9 Month: Death (%) 1 2 2 0.18<br />
Q AMI (%) 1 1 4 0.01<br />
Non Q AMI (%) 5 4 15 0.005<br />
TLR (%) 10 8 19 NS<br />
J. Saucedo et al. Circ 2000;102:1155
Stent Thrombosis<br />
<strong>Management</strong><br />
Mechanical opening of stent<br />
<strong>Management</strong> of thrombus<br />
IIbIIIa inhibitor<br />
Angiojet<br />
X-SIZER (Endicor)<br />
Aspiration Thrombectomy<br />
Identify the Cause<br />
IVUS evaluation<br />
Check medications
Coronary Perforation<br />
Perforation Classification<br />
TYPE I: Extraluminal crater without<br />
extravasation<br />
Type II: Pericardial or myocardial blush<br />
without contrast jet extravasation<br />
Type III: Extravasation through frank (> 1<br />
mm) perforation<br />
Type III (Cavity Spilling): Perforation into<br />
anatomic cavity (e.g. Coronary Sinus)<br />
S.G. Ellis et al. Circ 1994;90:2725-30
Coronary Perforation<br />
Clinical Outcome 62/2900 Procedures<br />
(0.5%)<br />
Death Em-CABG Q-AMI Tamponade<br />
Type N (%) (%) (%) (%)<br />
I 13 0 15 0 8<br />
II 31 0 10 0 13<br />
III CS 2 0 0 0 0<br />
III 16 19 63 15 63<br />
S.G. Ellis et al. Circ 1994;90:2725-30
Cath Cath <strong>Lab</strong> <strong>Lab</strong> Complications<br />
Chronic<br />
Total<br />
Occlusion
Coronary Perforations:<br />
Incidence, Predictors <strong>and</strong> <strong>and</strong> Outcome<br />
5728 pts; 10,000 lesions; 4/93-11/01 Milan Italy<br />
Incidence 84 pts (1.5%)<br />
POBA 45 (53.6%)<br />
DCA 8 (9.5%)<br />
Rota 3 (3.6%)<br />
Cutting balloon 2 (2.4%)<br />
Guidewire 23 (27.4%)<br />
Other devices 3 (3.6%)<br />
Atheroablative procedure 2.4% vs. 1.3%<br />
Complex lesions 1.9% vs. 0.5%<br />
Higher B/A ratio 1.3 vs. 1.2<br />
G. Stankovic et al. Circ 2002;19:2210
Coronary Perforations:<br />
Incidence, Predictors <strong>and</strong> <strong>and</strong> Outcome (cont.)<br />
5728 pts; 10,000 lesions; 4/93-11/01 Milan Italy<br />
Outcomes<br />
In-hospital In-hospital MACE 34.5%<br />
AMI 17.8%<br />
Em-CABG 13.1%<br />
Death 8.3%<br />
G. Stankovic et al. Circ 2002;19:2210
Vessel Perforation: <strong>Management</strong><br />
Don’t panic<br />
Prolonged balloon inflation<br />
Reverse heparin<br />
Platelet infusion, FFP<br />
Echocardiogram<br />
Pigtail catheter to pericardium<br />
Covered stent (if deliverable)<br />
Gelfoam or thrombus occlusion of vessel<br />
Surgery rarely required<br />
Follow-up echocardiogram very important
Air Embolus<br />
Often from manifold injections<br />
(contrast or flush)<br />
Prevention<br />
Avoid pressurized flush<br />
Back bleed before injecting<br />
Small amounts are well tolerated<br />
Large amounts cause “Air Lock”<br />
Chest Pain<br />
Bradycardia<br />
Hypotension
Air Lock: <strong>Management</strong><br />
Don’t Panic<br />
100% O2<br />
Morphine, Atropine<br />
Neosynephrine 0.1 mg. IV<br />
I/C Epinephrine 1:10,000 dil.<br />
Turn patient<br />
Suction / Flushing<br />
IABP<br />
CPS (for refractory hemodynamic<br />
collapse)
Death<br />
Risks Risks of of PCI PCI<br />
Myocardial infarction<br />
Acute closure<br />
Vascular perforation<br />
Embolus of clot or air or plaque debris<br />
Side branch occlusion<br />
Hematoma <strong>and</strong> Hemorrhage<br />
Others: SAT<br />
Renal failure
Cerebrovascular Complications<br />
Rare (0.07%), mostly embolic in<br />
origin, careful management of<br />
wires, guide catheter, <strong>and</strong> flush<br />
Endocarditis patient: LV thrombus -<br />
avoid LV gram<br />
Majority from plaques on aorta<br />
Check ACT - keep > 250 sec.
Myocardial Infarction<br />
Mechanism Dissection, Abrupt closure,<br />
Side branch closure, No<br />
reflow, Thrombosis, Distal<br />
embolism<br />
Recent trials Q-wave at 1 - 2%<br />
Non-Q MI 5 - 10%<br />
CPK/MB 1 - 3x elevation: little<br />
consequences<br />
> 5x elevation: adverse<br />
long term effects
Acute Closure<br />
Abrupt closure: 2 - 9% (TIMI 0-II<br />
Flow)<br />
Threatened closure: Dissection or<br />
Thrombus with TIMI III Flow<br />
Prevention:<br />
Antiplatelets<br />
IIb/IIIa inhibitors<br />
Treat thrombus before stenting
Factors Associated with with Abrupt Abrupt Closure<br />
Clinical: unstable angina, female,<br />
AMI, chronic renal failure<br />
Angiographic: Intraluminal thrombus,<br />
long lesion, > 45 degree<br />
angulation, branch points,<br />
proximal tortuosity, ostial<br />
RCA, SVG, prestenosis ><br />
90%, intimal dissection
Predictors of of Mortality after after Abrupt Abrupt<br />
Closure<br />
% myocardium at risk<br />
LM & MV disease<br />
CHF, UA<br />
Target vessel supplies collaterals<br />
Age > 65<br />
Chronic Renal Failure<br />
Female gender<br />
Diabetes
Stent vs. Conventional Techniques for the Treatment of<br />
Abrupt Vessel Closure or Symptomatic Dissections<br />
100 pts with abrupt vessel closure / symptomatic<br />
dissection<br />
R<strong>and</strong>omized to Stent (n = 51) vs. Prolonged<br />
dilation/Emergency CABG<br />
In-Hospital<br />
Events<br />
Stent<br />
(n = 51)<br />
St<strong>and</strong>ard<br />
(n=49)<br />
Death 2% 2%<br />
QMI 16% 8%<br />
Emerg CABG 4% 0
Think: dissection, embolus, air,<br />
hypotension as well as microemboli<br />
High risk with SVG, Thrombus, Rota,<br />
Diffuse disease<br />
Prevent: ?IIbIIIa, CA ++ Prevent: ?IIbIIIa, CA antagonists,<br />
++ antagonists,<br />
Adenosine, DPD<br />
Slow Slow or or No No Flow<br />
Flow<br />
Treat: Support B/P with pressors, IABP<br />
Administer: distal Nitroprusside,<br />
Adenosine, CA ++ Administer: distal Nitroprusside,<br />
Adenosine, CA antagonists, Epinephrine<br />
++ antagonists, Epinephrine
Coronary Perforation<br />
PTCA 0.1%, Roto/DCA 0.5 - 2.0%. Stent<br />
0.5%<br />
Wire perforation (3/7000) rare, but may be<br />
slow to be recognized. Often with stiff wire,<br />
hydrophilic wire<br />
If device doesn’t follow, usually benign<br />
Device perforation can be rapidly fatal<br />
May occur hours later<br />
Clinical signs are variable<br />
Treatment: reverse A/C, perfusion balloon,<br />
centesis, covered stents, coils, RH Cath,<br />
serial ECHOs
Perforation Risk Risk<br />
Wire - Vessel Tortuosity (Esp.<br />
Hydrophilic Wire Use)<br />
Ablative Techniques - With Vessel<br />
Tortuosity<br />
Stents - Small Calcified Vessels / High<br />
B/A Ratio<br />
Interaction with IIbIIIa inhibitors<br />
???
Coronary Perforation in in the the Era Era of of Abciximab<br />
36 perforations<br />
6,214 PCI (0.58%)<br />
73.7<br />
Abciximab use<br />
57.1<br />
21.2<br />
Portamine<br />
64.3<br />
15.8<br />
Platelet TX<br />
50<br />
erfusion balloon<br />
26<br />
85.7<br />
5.3<br />
Tamponade<br />
42.9<br />
5.3<br />
Pericardiocentesis<br />
E Dippel et al., CCI 2001<br />
Perforation class by Ellis et al.<br />
50<br />
0<br />
Urgent CABG<br />
Class II<br />
Class III<br />
50<br />
Death<br />
21.4<br />
0
Coronary Perforation in in the the Era Era of of Abciximab<br />
N = 6,999 consecutive PCI from 1994 thru 1996<br />
Overall tamponade incidence 0.2% (15 pts)<br />
Perforation Causes:<br />
Target Lesion Site (n=5)<br />
Tip of Guidewire (n=3)<br />
Temporary Pacemaker Wire (n=7)<br />
0.3<br />
2.3<br />
3.2<br />
10.8<br />
PTC Stent DC/TEC ROTA<br />
Incidence by device<br />
Von Sohsten et al, Am Heart J 2000<br />
# per 1000 pts
Subacute Stent Thrombosis<br />
Increased risk with small vessels, multiple<br />
stents, uncovered dissection, low EF<br />
DES: multiple stents, long stents, small<br />
vessels, risk even higher - up to 1 year<br />
after stopping antiplatelets<br />
Risk for Q-wave MI: 60%<br />
Mortality: up to 25%
Allergic Reactions<br />
Local anesthetic (rare), contrast, protamine<br />
Anaphalactoid (no IgE)<br />
Increased risk with atopic disorder, seafood (?),<br />
prior contrast reaction<br />
Prevent: Prednisone (13 hrs+), H1 <strong>and</strong> H2<br />
blockers, Premedications<br />
Treat: One ml of Epi 1:10:000 in 10 ml, give 1 ml<br />
every minute, steroids,<br />
volume, volume, volume<br />
Protamine (cross reaction with NPH insulin)<br />
give test dose
Hypotension<br />
Think Think of hypovolemia (bleed <strong>and</strong><br />
dehydration), tamponade (esp.<br />
with TTVP)<br />
Vasovagal Vasovagal reaction, anaphylaxis,<br />
occlusion<br />
Treat Treat per diagnosis
Retroperitoneal Hematoma<br />
Uncontrolled free bleeding usually means<br />
laceration of the artery: change sheath,<br />
remove sheath <strong>and</strong> compress<br />
Puncture above the inguinal ligament may<br />
lead to retroperitoneal hematoma<br />
(Puncture using Fluoro)<br />
Rx: CT scan, transfusion, occasional surgical<br />
decompression, reverse IIbIIIa & heparin
Pseudoaneurysm <strong>and</strong> <strong>and</strong> AV AV Fistula Fistula<br />
Frequency 1 - 2%<br />
< 2 cm. Usually close spontaneously<br />
90% close with compression<br />
Thrombin injections<br />
Surgery rarely needed<br />
Prevention: Accurate puncture <strong>and</strong> initial<br />
control of the bleeding with sheath upsize<br />
<strong>and</strong> early removal
Iliac Iliac Dissection or or Perforation<br />
Generally occurs during retrograde passing of<br />
wires <strong>and</strong> catheters through tortuous or stenotic<br />
arteries<br />
If these dissections are retrograde <strong>and</strong> small,<br />
usually the forward blood flow will tag down the<br />
dissection flap<br />
If persists or flow limiting, can be treated by<br />
stenting<br />
Perforation: seal with PTA balloon, then operate<br />
or put covered stent
What What are are the the Steps Steps that that can can be be taken taken to to<br />
Minimize Complications?<br />
Ischemia:<br />
Embolism:<br />
Slow Flow:<br />
IABP with LM, Decreased EF<br />
Diffuse calcium with Roto<br />
Embolectomy Catheters<br />
IIbIIIa inhibitors<br />
ADP inhibitors<br />
IIbIIIa inhibitors<br />
Distal Protection<br />
Thrombectomy<br />
Prophylactic Ca ++ Prophylactic Ca blockers, Nipride,<br />
++ blockers, Nipride,<br />
or adenosine preloaded on<br />
delivery catheters
What What are are the the Steps Steps that that can can be be taken taken to to<br />
Minimize Complications Cont...?<br />
Side Branch Occlusion:<br />
Perforations:<br />
Renal Failure:<br />
Debulking<br />
Dual Stents<br />
Avoid Stenting<br />
Coils<br />
Covered Stents<br />
Contrast agents<br />
Small guides<br />
Hydration <strong>and</strong> diuresis
Preprocedural Risk Risk Assessment<br />
Conceptual Framework<br />
Should I Perform the Procedure?<br />
Absolute<br />
1. Risk to the Patient<br />
Rate of Death or MACE per 100<br />
Rate of “Minor” Complications<br />
Long Term Risk of Death, MI, & TLR
Preprocedural Risk Risk Assessment<br />
2. Risk to the Patient -<br />
Relative Risk<br />
Risk of PTCA vs. Alternative Therapies<br />
(Surgery or Medical Rx) for Short <strong>and</strong><br />
Long Term Complications
Preprocedural Risk Risk Assessment<br />
3. Risk to the Operator<br />
Adverse Outcomes on Physician<br />
Profile for Hospital Privileges, Payor<br />
Contracts, <strong>and</strong> Public Relations
What What are are Procedural Complications?<br />
Ischemia<br />
Acute Closure<br />
Embolism<br />
Side Branch Occlusion<br />
Slow / No Flow<br />
Perforation<br />
Other<br />
SAT<br />
Renal Failure
What What are are Procedural Complications?<br />
Wire Crossing<br />
Thrombosis<br />
Severe/Angulated Stenosis<br />
Poor Visualization<br />
After Wire Crossing<br />
Dissection, thrombus, major stroke,<br />
branch closure<br />
Can we deliver a stent?<br />
Calcium<br />
Tortuosity<br />
Poor guide support<br />
}Potential Potential for getting<br />
caught with your<br />
pants down! (i.e.<br />
closure without<br />
distal protection)
Correlates of of Adverse Outcomes<br />
Old<br />
Small / large<br />
USA<br />
Female<br />
Low LVEF<br />
SVG<br />
Thrombus<br />
Clinical<br />
CHF<br />
Angiographic<br />
Emergency<br />
PVD<br />
RF<br />
Calcification<br />
Bifurcation<br />
Tortuosity
Summary<br />
Intra-procedural complications can be prevented<br />
<strong>and</strong> minimized (but not eliminated) with today’s<br />
technology <strong>and</strong> careful planning.<br />
Acute <strong>and</strong> long term mortality are determined<br />
primarily by clinical factors not controlled by the<br />
operator.<br />
Consideration of short <strong>and</strong> long term risks to<br />
patients must be assessed taking both these facts<br />
into consideration.<br />
These risks, when compared to therapeutic<br />
alternatives, will lead to optimal outcome for<br />
patients.