MDT (multi-disciplinary team) guidance for managing prostate cancer
MDT (multi-disciplinary team) guidance for managing prostate cancer
MDT (multi-disciplinary team) guidance for managing prostate cancer

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>MDT</strong> (Multi-<strong>disciplinary</strong> Team)<br />
Guidance <strong>for</strong><br />
Managing Prostate Cancer<br />
Produced by:<br />
• British Uro-oncology Group (BUG)<br />
• British Association of Urological Surgeons (BAUS): Section of Oncology<br />
• British Prostate Group (BPG)<br />
This <strong>guidance</strong> has been supported by educational grants from Ferring Pharmaceuticals,<br />
Date of preparation: November 2009 GB.DOC.09.11.16<br />
2nd Edition (November 2009)<br />
Novartis and sanofi-aventis. The development and content of this <strong>guidance</strong><br />
has not been influenced in any way by the supporting companies.
Abbreviations<br />
3D-CRT: three-dimensional con<strong>for</strong>mal radiotherapy<br />
ADT: androgen deprivation therapy<br />
BPH: benign prostatic hyperplasia<br />
CAB: combined androgen blockade<br />
CHHiP: Conventional or Hypofractionated High Dose IMRT <strong>for</strong> Prostate Cancer<br />
CI: confidence interval<br />
CPA: cyproterone acetate<br />
CT: computed tomography<br />
DES: diethylstilbestrol<br />
DFS: disease-free survival<br />
DRE: digital rectal examination<br />
EBRT: external beam radiation therapy<br />
EPC: Early Prostate Cancer<br />
ERSPC: European Randomised Study of Screening <strong>for</strong> Prostate Cancer<br />
FFF: freedom from failure<br />
GnRH: gonadotrophin-releasing hormone<br />
HDR: high dose rate<br />
HIFU: high-intensity focused ultrasound<br />
HR: hazard ratio<br />
HRPC: hormone-refractory <strong>prostate</strong> <strong>cancer</strong><br />
IMRT: intensity modulated radiotherapy<br />
IPSS: International Prostate Symptom Score<br />
LDR: low dose rate<br />
LHRH: luteinising hormone releasing hormone<br />
LTAD: long-term androgen deprivation<br />
<strong>MDT</strong>: <strong>multi</strong>-<strong>disciplinary</strong> <strong>team</strong><br />
MRC: Medical Research Council<br />
MRI: magnetic resonance imaging<br />
MRS: magnetic resonance spectroscopy<br />
NCCN: National Comprehensive Cancer Network<br />
NICE: National Institute <strong>for</strong> Health and Clinical Excellence<br />
ONJ: osteonecrosis of the jaw<br />
OS: overall survival<br />
PFS: progression-free survival<br />
PLCO: Prostate, Lung, Colorectal and Ovarian<br />
ProtecT: Prostate Testing <strong>for</strong> Cancer and Treatment<br />
PSA: <strong>prostate</strong>-specific antigen<br />
RCT: randomised controlled trial<br />
SRE: skeletal-related events<br />
STAD: short-term androgen deprivation<br />
TRUS: transrectal ultrasound<br />
TURP: transurethral resection of the <strong>prostate</strong><br />
2
Integrated Care and the Multi-<strong>disciplinary</strong> Team (<strong>MDT</strong>)<br />
• The concept of integrated care is becoming increasingly accepted as a way to overcome<br />
fragmentation of patient management and to provide a consistent treatment strategy across<br />
the <strong>MDT</strong>. It also creates an optimal structure that facilitates audit and peer review.<br />
• Integration within the <strong>MDT</strong> is essential <strong>for</strong> patients with <strong>prostate</strong> <strong>cancer</strong> because the<br />
collaboration between <strong>MDT</strong> members (Table 1) is central to the treatment strategy, with ongoing<br />
support from the wider <strong>team</strong> to manage pain and the adverse effects of therapy. By being familiar<br />
with the complete spectrum of management strategies, the <strong>MDT</strong> can assist patients in making<br />
treatment decisions that are specific <strong>for</strong> their individual disease state, co-morbid conditions,<br />
age and lifestyle.<br />
Table 1: The make-up of the <strong>MDT</strong> in the <strong>prostate</strong> <strong>cancer</strong> setting<br />
Urological surgeons Oncology and urology nurse specialists<br />
Clinical and medical oncologists (Palliative care specialist)<br />
<strong>MDT</strong> co-ordinator and secretarial support (Oncology pharmacists)<br />
Radiologists (Social workers)<br />
Histopathologists (Dieticians)<br />
• According to the UK-based Integrated Care Network, the move to true integrated practice can<br />
add value in the following ways: 1<br />
o Changing the identity or branding of a service to create more positive user responses and<br />
staff allegiances, enabling a clear break with the past.<br />
o Securing organisational efficiencies, <strong>for</strong> example, in the shape of shared support services,<br />
integrated management, innovative administrative processes and emerging hybrid roles.<br />
o Defining a focus <strong>for</strong> action that includes clearer processes of accountability and is less prone<br />
to distraction by wider organisational concerns.<br />
o Introducing more robust arrangements <strong>for</strong> <strong>team</strong>-working and leadership-working in<br />
challenging times.<br />
o Creating new opportunities <strong>for</strong> investment, <strong>for</strong> example, in IT systems, and opening access to<br />
new sources of funding.<br />
• The algorithms presented in this <strong>guidance</strong> provide a single framework that is adapted <strong>for</strong> each<br />
major category of <strong>prostate</strong> <strong>cancer</strong>: localised, locally advanced and advanced (Figure 1).<br />
• The treatment algorithms presented in this document (Figures 2−4) represent a management<br />
structure that goes beyond a simple co-ordinated system and will work most efficiently when<br />
the <strong>MDT</strong> is functioning as a single integrated unit.<br />
3
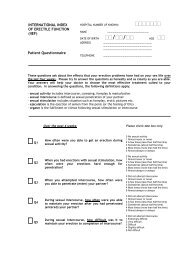
Figure 1: Summary of the definition of <strong>prostate</strong> <strong>cancer</strong> stages<br />
LOCALISED<br />
DISEASE<br />
T1/T2<br />
No/Mo<br />
Low Risk<br />
Gleason grade ≤6<br />
PSA ≤10<br />
Intermediate Risk<br />
Gleason grade 7<br />
and/or<br />
PSA (10-20)<br />
High Risk<br />
Gleason grade ≥8<br />
and/or<br />
PSA ≥20<br />
LOCALLY<br />
ADVANCED<br />
DISEASE<br />
(Non-metastatic)<br />
T1/T2 N+ Mo<br />
T3/T4 No/N+ Mo<br />
Failed local Rx<br />
with rising PSA<br />
and/or local<br />
recurrence+ Mo<br />
ADVANCED<br />
DISEASE<br />
(Metastatic)<br />
Proven M1<br />
4
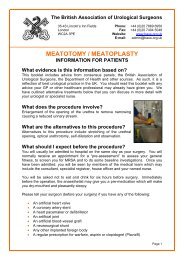
Figure 2: Treatment algorithm <strong>for</strong> localised disease<br />
Key Questions <strong>for</strong> the <strong>MDT</strong><br />
• TNM stage?<br />
• Gleason grade?<br />
• PSA/PSA Kinetics?<br />
• Age/co-morbidity/life<br />
expectancy?<br />
• Symptoms:<br />
– Bowel?<br />
– Urine IPSS score?<br />
• Sexual function?<br />
• Family history?<br />
Is this patient suitable <strong>for</strong> clinical trial?<br />
Low Risk<br />
Gleason grade ≤6<br />
PSA ≤10<br />
Active surveillance Radical <strong>prostate</strong>ctomy<br />
Radical <strong>prostate</strong>ctomy<br />
External beam radiotherapy<br />
(EBRT) +/– neo-adjuvant<br />
and concurrent hormone<br />
therapy<br />
Low dose rate (LDR)<br />
brachytherapy +/– neoadjuvant<br />
hormone therapy<br />
Watchful waiting<br />
Novel therapies<br />
<strong>MDT</strong><br />
Diagnostic Tests<br />
• Digital rectal exam (DRE)<br />
• PSA<br />
• Transrectal ultrasound<br />
(TRUS)/biopsy<br />
• MRI/CT pelvic scan*<br />
• Bone scan*<br />
(*Not mandatory <strong>for</strong> low-risk patients)<br />
MANAGEMENT OPTIONS<br />
Intermediate Risk<br />
Gleason grade 7<br />
and/or PSA (10-20)<br />
EBRT +/– neo-adjuvant,<br />
concurrent or adjuvant<br />
hormone therapy<br />
LDR brachytherapy<br />
+/– EBRT<br />
+/– hormone therapy<br />
Watchful waiting<br />
Novel therapies<br />
Ongoing Support<br />
Local patient support network<br />
Role of nurse/GP/healthcare professional <strong>team</strong><br />
Key Discussion Points<br />
with the Patient<br />
• Survival/prognosis?<br />
• Treatment options?<br />
• Treatment side-effects?<br />
• Impact on quality of life?<br />
• Importance of:<br />
– Psychological impact<br />
to patient and family?<br />
– Family history?<br />
– Clinical trials?<br />
– Sexual function?<br />
– Urinary function?<br />
– Bowel function?<br />
– Physical strength, energy?<br />
– Level of activity?<br />
– Accessibility to Rx?<br />
High Risk<br />
Gleason grade ≥8<br />
and/or PSA ≥20<br />
Selected Selected<br />
For treatment<br />
approach see<br />
locally advanced<br />
management<br />
5
Figure 3: Treatment algorithm <strong>for</strong> locally advanced (non-metastatic) disease<br />
Key Questions <strong>for</strong> the <strong>MDT</strong><br />
• TNM stage?<br />
• Gleason grade?<br />
• PSA/PSA Kinetics?<br />
• Age/co-morbidity/life<br />
expectancy?<br />
• Symptoms:<br />
– Bowel?<br />
– Urine IPSS score?<br />
• Sexual function?<br />
• Family history?<br />
• Bone pain?<br />
• Osteoporosis risk?<br />
Is this patient suitable <strong>for</strong> clinical trial?<br />
High-risk localised<br />
<strong>MDT</strong><br />
Diagnostic Tests<br />
• Digital rectal exam (DRE)<br />
• PSA<br />
• Transrectal ultrasound<br />
(TRUS)/biopsy<br />
• MRI/CT pelvic scan<br />
• Bone scan<br />
• Consider lymph node sampling<br />
(if this will determine changes<br />
in management approach)<br />
MANAGEMENT OPTIONS 1<br />
T1/T2 N+ Mo<br />
T3/T4 No/N+ Mo<br />
External beam radiotherapy (EBRT)<br />
+/- HDR brachytherapy boost<br />
+/-neo-adjuvant, concomitant<br />
and adjuvant hormone therapy<br />
Hormone therapy alone<br />
Watchful waiting<br />
Ongoing Support<br />
Local patient support network<br />
Role of nurse/GP/healthcare professional <strong>team</strong><br />
Key Discussion Points<br />
with the Patient<br />
• Survival/prognosis?<br />
• Treatment options?<br />
• Treatment side-effects?<br />
• Impact on quality of life?<br />
• Importance of:<br />
– Psychological impact<br />
to patient and family?<br />
– Family history?<br />
– Clinical trials?<br />
– Sexual function?<br />
– Urinary function?<br />
– Bowel function?<br />
– Physical strength, energy?<br />
– Level of activity?<br />
– Accessibility to Rx?<br />
6
Figure 3: Treatment algorithm <strong>for</strong> locally advanced (non-metastatic) disease (cont.)<br />
Is this patient suitable <strong>for</strong> clinical trial?<br />
Post-radical <strong>prostate</strong>ctomy<br />
MANAGEMENT OPTIONS 2<br />
Failed local Rx with rising PSA<br />
and/or local recurrence+ Mo<br />
Active surveillance/watchful waiting Active surveillance/watchful waiting<br />
Hormone therapy alone Hormone therapy alone<br />
External beam radiotherapy<br />
(EBRT) +/– concomitant +/–<br />
adjuvant hormone therapy<br />
Post-radical radiotherapy/<br />
brachytherapy<br />
Salvage <strong>prostate</strong>ctomy<br />
Novel local salvage therapy<br />
Ongoing Support<br />
Local patient support network<br />
Role of nurse/GP/healthcare professional <strong>team</strong><br />
7
Figure 4: Treatment algorithm <strong>for</strong> advanced (metastatic) disease<br />
Key Questions <strong>for</strong> the <strong>MDT</strong><br />
• TNM stage?<br />
• Gleason grade?<br />
• PSA/PSA Kinetics?<br />
• Age/co-morbidity/life<br />
expectancy?<br />
• Symptoms:<br />
– Bowel?<br />
– Urine IPSS score?<br />
• Sexual function?<br />
• Family history?<br />
• Bone pain?<br />
• Osteoporosis risk?<br />
• Palliative care referral?<br />
Is this patient suitable <strong>for</strong> clinical trial?<br />
Palliative Care<br />
• Pain control<br />
• Local radiotherapy<br />
Bone pain<br />
Spinal cord compression<br />
Nerve root compression<br />
• Continual assessment<br />
Second-/third-line if<br />
androgen sensitive?<br />
<strong>MDT</strong><br />
Diagnostic Tests<br />
• Digital rectal exam (DRE)<br />
• PSA<br />
• Transrectal ultrasound (TRUS)/<br />
biopsy (non mandatory if PSA<br />
>100 and radiological evidence<br />
of metastases)<br />
• Biochemistry screen<br />
• Full blood count<br />
• Bone scan<br />
• MRI/CT pelvic scan<br />
MANAGEMENT OPTIONS<br />
Proven M1/M2<br />
First line hormone therapy<br />
Significant rise in PSA Clinical/<br />
radiological progression<br />
Observation<br />
Second-/third-line hormone<br />
therapy<br />
Further progression<br />
Ongoing Support<br />
Local patient support network<br />
Role of nurse/GP/healthcare professional <strong>team</strong><br />
Key Discussion Points<br />
with the Patient<br />
• Survival/prognosis?<br />
• Treatment options?<br />
• Treatment side-effects?<br />
• Impact on quality of life?<br />
• Importance of:<br />
– Psychological impact<br />
to patient and family?<br />
– Family history?<br />
– Clinical trials?<br />
– Sexual function?<br />
– Urinary function?<br />
– Bowel function?<br />
– Physical strength, energy?<br />
– Level of activity?<br />
– Accessibility to Rx?<br />
HRPC<br />
Clinical trials<br />
Chemotherapy<br />
Strontium<br />
Bisphosphonate<br />
8
Integrated care and clinical governance<br />
• The effective functioning of the <strong>MDT</strong> and tailored care pathways <strong>for</strong> patients will support the<br />
(now routine) clinical governance procedures implemented throughout the NHS. Traditionally,<br />
clinical governance relates to a single organisation or service and this can raise challenges, with<br />
the recognition that patients require management across different organisations and services.<br />
There<strong>for</strong>e, it is appropriate to apply the principles of clinical governance to individual patients or<br />
groups of patients.<br />
• The focus should be on optimum patient satisfaction and care, rather than on per<strong>for</strong>mance of<br />
the NHS institution. The <strong>MDT</strong> and development of organised pathways (allowing <strong>for</strong> individual<br />
clinical discretion and patient involvement in decision-making) ensures that the patient’s journey<br />
is monitored and assessed as a single entity.<br />
9
Approach within the <strong>MDT</strong><br />
Key questions <strong>for</strong> the <strong>MDT</strong><br />
• TNM stage?<br />
• Gleason grade?<br />
• Prostate-specific antigen (PSA) concentration?<br />
• Risk group (according to National Comprehensive Cancer Network [NCCN] guidelines)?<br />
• Age/co-morbidity/life expectancy?<br />
• Symptoms:<br />
o International Prostate Symptom Score (IPSS), bowel, urinary?<br />
• Sexual function?<br />
• Bone pain?<br />
• Osteoporosis risk?<br />
• Family history?<br />
• Clinical trials?<br />
• The <strong>MDT</strong> is an essential part of <strong>cancer</strong> management. However, there are often difficulties in<br />
knowing which patients to discuss, ensuring that their details and diagnoses are available,<br />
and keeping a record of decisions made at the meetings.<br />
• <strong>MDT</strong>s have repeatedly been endorsed as the principal mechanism <strong>for</strong> ensuring that all relevant<br />
disciplines and professional groups contribute to, and participate in, decisions regarding the<br />
clinical management of patients. 2<br />
• <strong>MDT</strong>-working is positively related to a range of measures of effectiveness, including the quality<br />
of clinical care.<br />
• It is important to emphasise the distinction between management and administration.<br />
• A central concept of integrated care is to rein<strong>for</strong>ce the role of the <strong>MDT</strong> (working as a single unit),<br />
but with enough clinical freedom to tailor management strategies to the needs of individual<br />
patients.<br />
• Treatment strategies are influenced by the stage of disease and by an interaction between<br />
the risk of disease progression, survival and key patient characteristics, such as age, lifestyle<br />
and general health. The discussion of these factors is of crucial importance in determining the<br />
most appropriate way <strong>for</strong>ward. For example, age and the presence of co-morbidities may be a<br />
restrictive factor when considering surgery.<br />
• The case notes, pathology reports, test results and radiology <strong>for</strong> each patient must be available<br />
to be discussed at the meeting. The <strong>MDT</strong> must also ensure that the patient has the fullest possible<br />
role in determining treatment − the importance of this cannot be overstated. Patient preference<br />
should be discussed within the <strong>MDT</strong>. Although the majority of men with <strong>prostate</strong> <strong>cancer</strong> want to<br />
be involved in treatment decisions, an estimated one in five of all patients does not raise, or really<br />
understand, the potential issues and associated side-effects of treatments and alternatives that<br />
may be available to them. 3<br />
• The possibility of including a patient in a relevant clinical trial should not be <strong>for</strong>gotten.<br />
10
Approach to the Patient<br />
Key points <strong>for</strong> discussion with the patient<br />
• Survival prognosis?<br />
• Treatment options?<br />
• Treatment side-effects?<br />
• Impact on quality of life?<br />
• Importance of:<br />
o Sexual function?<br />
o Urinary function?<br />
o Bowel function?<br />
o Physical strength, energy?<br />
o Level of activity?<br />
o Accessibility to prescribed drugs?<br />
o Psychosocial impact on them and their family?<br />
• Family history?<br />
• Clinical trials?<br />
The patient’s expectations<br />
The patient should have the right to discuss their treatment with<br />
appropriately trained members of the <strong>MDT</strong><br />
• After a diagnosis of <strong>prostate</strong> <strong>cancer</strong>, most men will want to have some involvement in the<br />
decisions concerning their care. The following aspects have been found to be important: 4<br />
o Honesty about the severity of the <strong>cancer</strong> and their prognosis<br />
o Discussion of the best treatment options<br />
o The clinician being up-to-date on ongoing and recent research<br />
o Disclosing all treatment options<br />
o How <strong>cancer</strong> may affect their daily functioning<br />
• It is essential that the patient and healthcare professionals discuss the likelihood of adverse<br />
events associated with each treatment option and implications <strong>for</strong> their future lifestyle when<br />
determining management strategies.<br />
• The patient and his partner, family and/or other carers should be fully in<strong>for</strong>med about care and<br />
treatment options and there<strong>for</strong>e able to make appropriate decisions based upon the choices<br />
offered by their healthcare professionals. For example, the choice between radical treatment and<br />
active surveillance may be influenced by a patient’s desire to retain sexual activity, physical energy<br />
and quality of life.<br />
• Patients should be in<strong>for</strong>med and advised regarding the available treatment options and the<br />
potential effects of these on their lifestyle and quality of life.<br />
11
Discussing evidence with patients<br />
There is a lack of evidence to guide how healthcare professionals can most effectively share clinical<br />
data with those patients facing treatment decisions. However, basing recommendations largely on<br />
relevant clinical studies and expert opinion, it is possible to achieve five communication objectives<br />
when framing and communicating clinical evidence.<br />
1. Understand the patient’s experience, expectations and preferences<br />
2. Build partnerships with the patient and carer<br />
3. Provide evidence and discuss uncertainties and side-effects<br />
4. Present recommendations<br />
5. Check <strong>for</strong> understanding and agreement<br />
12
Assessment and Diagnosis<br />
Screening<br />
• PSA screening remains a relatively contentious subject in the field of <strong>prostate</strong> <strong>cancer</strong>. It is felt that<br />
robust evidence is lacking concerning whether screening results in a reduction in mortality from<br />
the disease.<br />
• Three ongoing large, randomised, controlled clinical trials are evaluating the value of PSA<br />
screening <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong>: the European Randomised Study of Screening <strong>for</strong> Prostate Cancer<br />
(ERSPC), 5 the Prostate, Lung, Colorectal and Ovarian (PLCO) <strong>cancer</strong> screening trial in the US6<br />
and the UK-based Prostate Testing <strong>for</strong> Cancer and Treatment (ProtecT) study. 7 The first reports<br />
from these trials have been published and have added further in<strong>for</strong>mation to the PSA screening<br />
debate:<br />
o The PLCO study reported no mortality benefit with the combination of PSA screening and<br />
digital rectal examination (DRE) during a median follow-up of 7 years. 6<br />
o In contrast, the ERSPC trial found that PSA screening was associated with a 20% relative<br />
reduction in <strong>prostate</strong> <strong>cancer</strong> mortality at a median follow-up of 9 years, equivalent to the<br />
prevention of approximately 7 <strong>prostate</strong> <strong>cancer</strong> deaths per 10,000 men screened. This mortality<br />
benefit was associated with a high risk of overdiagnosis, with nearly 76% of men who<br />
underwent a biopsy following an elevated PSA value having a false positive result. 5<br />
o ProtecT has demonstrated a benefit of repeat PSA testing in reducing the risk of high-grade<br />
<strong>prostate</strong> <strong>cancer</strong> in men with an initial PSA concentration of 3−20 ng/ml. 7<br />
• Quality of life and cost-effectiveness analyses from the ERSPC and PLCO trials, along with<br />
mortality results from ProtecT are needed to help resolve the ongoing PSA screening debate.<br />
Risk factors <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong><br />
The risk factors <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong> are generally well-documented, but are highlighted here <strong>for</strong><br />
completeness of the Guidance.<br />
• Age<br />
o Relatively rare in men under the age of 50 years.<br />
o Incidence increases in those over 60 years.<br />
• Race<br />
o A higher incidence of the disease is seen in African-Caribbean, African-American and West<br />
African races. The UK PROCESS study is compiling equivalent UK data. 8<br />
o Men of Chinese and Japanese origin have a low incidence of disease.<br />
• Geography<br />
o The highest incidence of <strong>prostate</strong> <strong>cancer</strong> is currently seen in North America and<br />
Northern Europe.<br />
• Family history<br />
o Men with a first-degree relative affected by <strong>prostate</strong> <strong>cancer</strong> have a relative risk of<br />
developing the disease themselves 2-fold greater than men with no relatives affected. 9<br />
o Those men with an affected second-degree relative have an increased relative risk<br />
of 1.7 of developing the disease.<br />
o Men with both a first- and second-degree relative affected have an increased relative<br />
risk of 8.8 of developing the disease.<br />
13
o There is also some evidence to show a link between an increased risk of <strong>prostate</strong> <strong>cancer</strong><br />
where there is a family history of breast, ovarian, bladder or kidney <strong>cancer</strong>. 10<br />
o The UK Familial Prostate Cancer Study is currently looking at the genetics of the disease<br />
with possible sites of interest lying on chromosomes 2, 5, Y and loss of heterozygosity at<br />
10q and 16q.<br />
Diagnostic tests<br />
DRE<br />
• The DRE remains valid as an initial method <strong>for</strong> assessing the <strong>prostate</strong>; however, DRE findings<br />
should not be regarded as a fail-safe test.<br />
PSA<br />
• As an independent variable, PSA concentrations are a better predictor of <strong>cancer</strong> than suspicious<br />
11, 12<br />
findings on DRE or transrectal ultrasound (TRUS).<br />
• Serum concentrations of PSA can be elevated in the presence of benign prostatic hyperplasia<br />
(BPH), prostatitis and other non-malignant conditions. Furthermore, there is, as yet, no<br />
recommendation <strong>for</strong> the optimal PSA threshold value that most effectively avoids the detection<br />
13, 14<br />
of insignificant <strong>cancer</strong>s that are unlikely to be life-threatening.<br />
• While PSA concentrations generally increase with advancing disease stage, the ability of PSA levels<br />
to accurately predict pathological stage in any one individual is low. 15−17<br />
• Asymptomatic patients who request a PSA test should be counselled be<strong>for</strong>e the procedure<br />
<strong>for</strong> the following reasons: 18<br />
o Although the test may detect a <strong>cancer</strong> at a stage where curative treatment can be offered,<br />
PSA will fail to detect some early tumours.<br />
o A PSA test may detect early <strong>prostate</strong> <strong>cancer</strong> in an estimated 5% of men aged 50−65 years.<br />
o Treatment of early <strong>prostate</strong> <strong>cancer</strong> can put the patient at some risk and may not necessarily<br />
improve life expectancy.<br />
Factors affecting PSA concentrations are summarised below.<br />
Age and race<br />
Table 2: Age-specific PSA (ng/ml) reference ranges, by race 19<br />
Age (years) White Black Latino Asian<br />
40−49 0−2.3 0−2.7 0−2.1 0−2.0<br />
50−59 0−3.8 0−4.4 0−4.3 0−4.5<br />
60−69 0−5.6 0−6.7 0−6.0 0−5.5<br />
70−79 0−6.9 0−7.7 0−6.6 0−6.8<br />
Biopsy/transurethral resection of the <strong>prostate</strong> (TURP) can cause an increase in PSA <strong>for</strong> a variable time<br />
period (4−12 weeks). 20<br />
Prostatitis can cause an increase in PSA concentration, which can be reduced to within a normal range<br />
21, 22<br />
with antibiotic treatment.<br />
14
Prostate size – a benignly enlarged gland can influence PSA concentrations.<br />
Infection – elevated PSA levels can be seen beyond 6 months in up to 50% of patients when associated<br />
with febrile urinary tract infections.<br />
Free and complexed PSA should be understood. Catalona et al. conclude that percentage free PSA<br />
is most useful in men with a PSA concentration in the range 2−15 ng/ml (Table 3); the higher the<br />
percentage of free PSA the lower the probability of <strong>cancer</strong>. 23<br />
Table 3: Probability of <strong>prostate</strong> <strong>cancer</strong> based on total and percentage free PSA 23<br />
Total PSA (ng/ml)<br />
PSA density i.e. PSA level (ng/ml)<br />
TRUS-determined <strong>prostate</strong> volume (ml)<br />
Probability of <strong>cancer</strong> (%)<br />
0−2 ~1<br />
2−4 15<br />
4−10 25<br />
>10 >50<br />
Free PSA (%)<br />
0−10 56<br />
10−15 28<br />
15−20 20<br />
20−25 16<br />
>25 8<br />
May be helpful in differentiating BPH from <strong>prostate</strong> <strong>cancer</strong> in patients who have a normal DRE with<br />
a PSA 4−10ng/ml. A PSA density >0.15 may suggest <strong>prostate</strong> <strong>cancer</strong>.<br />
PSA velocity can be valuable in the follow-up of men with a normal PSA but prior negative biopsies.<br />
Velocity is measured by a change in PSA concentration in three consecutive measurements taken at<br />
6-monthly intervals. A change in PSA concentration of >0.75 ng/ml per year is more likely to indicate<br />
<strong>prostate</strong> <strong>cancer</strong> than BPH. The usefulness of PSA velocity in those with a PSA concentration >10 ng/ml<br />
is unknown. 24<br />
TRUS<br />
• TRUS detects 50% more patients with <strong>prostate</strong> <strong>cancer</strong> than physical examination alone, 25, 26 but<br />
the ultrasonic appearance of <strong>prostate</strong> <strong>cancer</strong> is variable and only a very small number of <strong>cancer</strong>s<br />
are detected if a DRE and PSA test are normal. 26−28 There<strong>for</strong>e, TRUS is mainly used to aid biopsy.<br />
15
Biopsy and tumour grading<br />
• The National Institute <strong>for</strong> Health and Clinical Excellence (NICE) <strong>prostate</strong> <strong>cancer</strong> guideline<br />
recommends that the serum PSA level alone should not automatically lead to a <strong>prostate</strong> biopsy. 29<br />
It states that to help men decide whether to have a <strong>prostate</strong> biopsy, healthcare professionals<br />
should discuss with them their PSA level, DRE findings (including an estimate of <strong>prostate</strong> size)<br />
and co-morbidities, together with their risk factors (including increasing age and black African<br />
and black Caribbean ethnicity) and any history of a previous negative <strong>prostate</strong> biopsy.<br />
• NICE further highlights that men and their partners or carers should be given in<strong>for</strong>mation,<br />
support and adequate time to decide whether or not they wish to undergo <strong>prostate</strong> biopsy. 29<br />
Men will need to comprehend the potential risks (such as potentially living with a diagnosis of<br />
<strong>prostate</strong> <strong>cancer</strong> that is deemed clinically insignificant) and the benefits of <strong>prostate</strong> biopsy.<br />
• Where biopsy is indicated, a minimum of 10 biopsies should be obtained, according to the volume<br />
of the <strong>prostate</strong>. Biopsies should be per<strong>for</strong>med under local anaesthetic and antibiotic cover. 30<br />
• A European study has reported that a <strong>prostate</strong> <strong>cancer</strong> detection rate <strong>for</strong> the first set of biopsies<br />
is 24% and <strong>for</strong> the second set of biopsies after a negative initial set as 13%. 31<br />
Magnetic Resonance Imaging (MRI)<br />
• The classification used <strong>for</strong> staging <strong>prostate</strong> <strong>cancer</strong> is the internationally approved system<br />
recommended by the Union International Contra Cancer (available at: www.uicc.org).<br />
• TNM staging, Gleason score, and PSA concentration facilitate estimation of the risk of<br />
extracapsular disease and lymph node metastases. Pelvic staging is required <strong>for</strong> those of high<br />
or intermediate risk (according to NCCN classification). MRI is the preferred option to stage pelvic<br />
lesions and where MRI is contraindicated, computed tomography (CT) should be used. 29<br />
• Body coil MRI is sensitive and specific in identifying extracapsular extension of <strong>prostate</strong> <strong>cancer</strong><br />
in patients with high- or intermediate-risk disease. 32<br />
• NICE concludes: 29<br />
o MRI is now the most accurate and commonly-used imaging technique <strong>for</strong> tumour-staging<br />
men with <strong>prostate</strong> <strong>cancer</strong>. Many of the original publications used now outdated MRI<br />
technology, and the accuracy reported <strong>for</strong> MRI is improving, typically with endorectal coil<br />
imaging at 1.5 Tesla.<br />
o After transrectal <strong>prostate</strong> biopsy, intra-prostatic haematoma can affect image interpretation<br />
<strong>for</strong> at least 4 weeks.<br />
o Magnetic resonance spectroscopy (MRS) is an experimental technique based on the<br />
concentration of metabolites such as choline and citrate in the <strong>prostate</strong> gland. Prostate <strong>cancer</strong><br />
alters the concentrations of these metabolites and this may be used to find areas of tumour<br />
activity. MRS is not recommended <strong>for</strong> men with <strong>prostate</strong> <strong>cancer</strong> except in the context of a<br />
clinical trial.<br />
Bone scans and lymph node sampling<br />
• Bone scans (particularly in patients with PSA concentration >20 ng/ml) and lymph node biopsies<br />
are also important in the assessment process. A PSA concentration of
Key Questions <strong>for</strong> the <strong>MDT</strong><br />
• TNM stage?<br />
• Gleason grade?<br />
• PSA/PSA Kinetics?<br />
• Age/co-morbidity/life<br />
expectancy?<br />
• Symptoms:<br />
– Bowel?<br />
– Urine IPSS score?<br />
• Sexual function?<br />
• Family history?<br />
Is this patient suitable <strong>for</strong> clinical trial?<br />
Localised Disease: Management Options<br />
Figure 2: Treatment algorithm <strong>for</strong> localised disease<br />
Low Risk<br />
Gleason grade ≤6<br />
PSA ≤10<br />
Active surveillance Radical <strong>prostate</strong>ctomy<br />
Radical <strong>prostate</strong>ctomy<br />
External beam radiotherapy<br />
(EBRT) +/– neo-adjuvant<br />
and concurrent hormone<br />
therapy<br />
Low dose rate (LDR)<br />
brachytherapy +/– neoadjuvant<br />
hormone therapy<br />
Watchful waiting<br />
Novel therapies<br />
<strong>MDT</strong><br />
Diagnostic Tests<br />
• Digital rectal exam (DRE)<br />
• PSA<br />
• Transrectal ultrasound<br />
(TRUS)/biopsy<br />
• MRI/CT pelvic scan*<br />
• Bone scan*<br />
(*Not mandatory <strong>for</strong> low-risk patients)<br />
MANAGEMENT OPTIONS<br />
Intermediate Risk<br />
Gleason grade 7<br />
and/or PSA (10-20)<br />
EBRT +/– neo-adjuvant,<br />
concurrent or adjuvant<br />
hormone therapy<br />
LDR brachytherapy<br />
+/– EBRT<br />
+/– hormone therapy<br />
Watchful waiting<br />
Novel therapies<br />
Ongoing Support<br />
Local patient support network<br />
Role of nurse/GP/healthcare professional <strong>team</strong><br />
Key Discussion Points<br />
with the Patient<br />
• Survival/prognosis?<br />
• Treatment options?<br />
• Treatment side-effects?<br />
• Impact on quality of life?<br />
• Importance of:<br />
– Psychological impact<br />
to patient and family?<br />
– Family history?<br />
– Clinical trials?<br />
– Sexual function?<br />
– Urinary function?<br />
– Bowel function?<br />
– Physical strength, energy?<br />
– Level of activity?<br />
– Accessibility to Rx?<br />
High Risk<br />
Gleason grade ≥8<br />
and/or PSA ≥20<br />
Selected Selected<br />
For treatment<br />
approach see<br />
locally advanced<br />
management<br />
17
The following <strong>guidance</strong> <strong>for</strong> <strong>managing</strong> localised <strong>prostate</strong> <strong>cancer</strong> focuses on low- and intermediate-risk<br />
categories, defined here as: 34<br />
• Low risk (T1c/T2a; Gleason grade ≤6; PSA concentration ≤10 ng/ml)<br />
• Intermediate risk (T2b; Gleason grade 7 and/or PSA concentration: >10 and ≤20 ng/ml)<br />
In the proposed management algorithms, high-risk localised disease falls more naturally into<br />
management of locally advanced disease.<br />
Patient choice and the presence or absence of co-morbidities should be an essential component<br />
of management decisions in men with localised disease. Decisions concerning the choice of radical<br />
treatments need to be carefully balanced with the different options available and the impact of such<br />
treatments on a patient’s co-morbidities.<br />
In this section available evidence <strong>for</strong> the following management approaches is outlined:<br />
• Active surveillance<br />
• Watchful waiting<br />
• Radical <strong>prostate</strong>ctomy<br />
• External Beam Radiation Therapy (EBRT)<br />
• Low dose rate brachytherapy<br />
• Neoadjuvant/adjuvant hormone therapy<br />
• Novel therapies<br />
There is no consistent evidence <strong>for</strong> superiority of any of the three main radical treatments: radical<br />
<strong>prostate</strong>ctomy, EBRT or brachytherapy.<br />
18
Active surveillance<br />
Overview<br />
• Active surveillance is an approach to the management of early <strong>prostate</strong> <strong>cancer</strong> in which the choice<br />
between curative treatment and observation is based on evidence of disease progression (PSA<br />
kinetics or repeat biopsy findings) during a period of close monitoring. The aim is to reduce the<br />
burden of treatment side-effects without compromising survival.<br />
• Patients suitable <strong>for</strong> active surveillance are those with low-risk localised disease who are fit <strong>for</strong><br />
radical treatment. Ongoing prospective studies of active surveillance have shown that 60−80%<br />
of such men will avoid the need <strong>for</strong> treatment, and that 100% <strong>prostate</strong> <strong>cancer</strong>-specific survival<br />
35, 36<br />
at 10 years is achievable.<br />
• Active surveillance should be distinguished from watchful waiting. Traditional watchful waiting<br />
involves relatively lax observation with late, palliative treatment <strong>for</strong> those who develop symptoms<br />
of progressive disease. In contrast, active surveillance involves close monitoring with early, radical<br />
treatment in those with signs of disease progression.<br />
Patient selection<br />
• Low-risk, clinically localised <strong>prostate</strong> <strong>cancer</strong><br />
o Clinical stage T1c/2a<br />
o Gleason grade ≤3+4<br />
o PSA concentration
• Van As et al. reported the outcome of 326 men recruited to the Royal Marsden active surveillance<br />
study from 2002 to 2006, at a median follow-up of 22 months. 35 Median age was 67 years,<br />
and median initial PSA concentration 6.4 ng/ml. Sixty-five patients (20%) had deferred radical<br />
treatment, 16 (5%) changed to watchful waiting because of increasing co-morbidity, 7 (2%) died<br />
of other causes, and 238 (73%) remain on surveillance. There were no deaths from <strong>prostate</strong> <strong>cancer</strong><br />
and no men had developed metastatic disease.<br />
• It is possible that targeted radical treatment, based on an active surveillance strategy, will be as<br />
effective, and considerably less morbid, than radical treatment <strong>for</strong> all cases. The ProSTART phase III<br />
trial will compare the long term outcomes of active surveillance with those of immediate radical<br />
treatment, and aims to recruit approximately 2100 patients.<br />
20
Watchful waiting<br />
Overview<br />
• Watchful waiting is an approach to the management of localised <strong>prostate</strong> <strong>cancer</strong> that aims to<br />
avoid treatment, or delay it <strong>for</strong> as long as possible. Patients who eventually develop symptoms<br />
of progressive <strong>prostate</strong> <strong>cancer</strong> receive palliative treatment, usually with hormone therapy.<br />
• Watchful waiting is particularly suitable <strong>for</strong> patients aged over 75 years or younger men with<br />
significant co-morbidities.<br />
• Watchful waiting should be distinguished from active surveillance. Conventional watchful waiting<br />
involves relatively lax observation with late, palliative treatment <strong>for</strong> those who develop symptoms<br />
of progressive disease. In contrast, active surveillance involves close monitoring with early, radical<br />
treatment in those with signs of progression.<br />
Patient selection<br />
• Asymptomatic clinically localised <strong>prostate</strong> <strong>cancer</strong><br />
o Clinical stage T1−3<br />
o Gleason score ≤7<br />
o Any PSA concentration<br />
o Not suitable <strong>for</strong> radical treatment (usually by virtue of older age or co-morbidities)<br />
Side-effects<br />
• Uncertainty<br />
Clinical evidence<br />
• The NICE clinical guideline confirms a lack of evidence <strong>for</strong> watchful waiting and the Guideline<br />
Development Group reached a consensus that the recommendation from NICE would avoid<br />
unnecessary investigations: 29<br />
o Men with localised <strong>prostate</strong> <strong>cancer</strong> who have chosen a watchful waiting regimen and who<br />
have evidence of significant disease progression (that is, rapidly rising PSA level or bone pain)<br />
should be reviewed by a member of the urological <strong>cancer</strong> <strong>MDT</strong>.<br />
21
Radical treatments<br />
Radical <strong>prostate</strong>ctomy<br />
There are now four approaches to per<strong>for</strong>ming a radical <strong>prostate</strong>ctomy: retropubic, perineal, laparoscopic<br />
and robotic. The procedure involves removal of the whole <strong>prostate</strong> and the seminal vesicles. The most<br />
commonly used approaches are retropubic and perineal, but laparoscopic and robotic techniques are<br />
becoming more frequently adopted. The newer approaches have the advantage of reduced blood loss<br />
and shorter inpatient stays.<br />
Overview<br />
• In 1997, Selley et al. reviewed a total of 17 studies (two randomised controlled trials [RCTs] and<br />
15 observational studies involving a total of 5410 patients) to investigate the efficacy of radical<br />
<strong>prostate</strong>ctomy <strong>for</strong> men with localised <strong>prostate</strong> <strong>cancer</strong>. Cancer-specific survival after 10 years of followup<br />
ranged from 86% to 91%, with clinical disease-free survival (DFS) ranging from 57% to 83%. 38<br />
Patient selection<br />
• Anaesthetic fitness<br />
• At least 10 years’ life expectancy<br />
• Complications increase and benefits decrease in patients aged >70 years<br />
Side-effects of treatment<br />
• Based on the systematic review by Selley et al., the following side-effects should be considered: 38<br />
o Operative and post-operative mortality: 0.2−1.2%<br />
o Sexual dysfunction: 51−61%<br />
o Incontinence (mild stress): 4−21%<br />
o Incontinence (total): 0−7%<br />
Clinical evidence<br />
• One randomised trial has compared radical <strong>prostate</strong>ctomy with watchful waiting in localised<br />
<strong>prostate</strong> <strong>cancer</strong>. 39<br />
o The trial randomised 695 men with localised disease between radical <strong>prostate</strong>ctomy and<br />
watchful waiting.<br />
o At a median follow-up of 8.2 years, randomisation to radical <strong>prostate</strong>ctomy was associated with<br />
a benefit both in terms of disease-specific mortality (hazard ratio [HR] 0.56; 95% confidence<br />
interval [CI]: 0.36−0.88; p=0.01) and overall mortality (HR 0.74; 95%CI: 0.56−0.99; p=0.04).<br />
o This translated into 10-year OS of 73% versus 68% (p=0.04) <strong>for</strong> radical <strong>prostate</strong>ctomy versus<br />
watchful waiting.<br />
o In terms of 10-year freedom from distant metastases, the absolute benefit of surgery versus<br />
watchful waiting was 10% (84.8% versus 74.6%; p=0.004).<br />
o However, patients need to weigh these benefits against the risk of adverse consequences of<br />
treatment. The 5% absolute improvement in 10-year survival was achieved at the expense of a<br />
35% absolute increase in the risk of erectile dysfunction and a 28% absolute increase in the risk<br />
of urinary leakage.<br />
22
o Faced with these figures, some patients would choose surgery, but many would choose<br />
conservative management. 40<br />
• The above findings are now updated to incorporate a further 3 years of follow up. At 12 years: 41<br />
o 12.5% of the surgery group and 17.9% of the watchful waiting group had died of <strong>prostate</strong><br />
<strong>cancer</strong> (difference = 5.4%, 95%CI: 0.2−11.1).<br />
o 19.3% of men in the surgery group and 26% of men in the watchful waiting group had been<br />
diagnosed with distant metastases (difference = 6.7%, 95%CI: 0.2−13.2).<br />
o This follow-up analysis was consistent with the previous findings. Radical <strong>prostate</strong>ctomy can<br />
reduce <strong>prostate</strong> <strong>cancer</strong> mortality and risk of metastases but no further benefits were seen<br />
beyond 10 years of follow up in this study.<br />
Neoadjuvant and adjuvant hormone therapy with radical <strong>prostate</strong>ctomy<br />
• At present, evidence suggests that the down-staging achieved with neoadjuvant hormone<br />
therapy does not translate into improved DFS, and there<strong>for</strong>e cannot be recommended outside<br />
of clinical trials. 42−45<br />
• Similarly, there is currently no evidence that adjuvant hormone therapy provides a survival<br />
46, 47<br />
advantage <strong>for</strong> patients with pathologically proven localised disease.<br />
Adjuvant radiotherapy after radical <strong>prostate</strong>ctomy<br />
• The EORTC 22911 study was designed to investigate benefit <strong>for</strong> immediate postoperative<br />
radiotherapy in 502 patients with pT3 disease or positive surgical margins as opposed to<br />
radiotherapy offered <strong>for</strong> biochemical or clinical relapse. 48<br />
o After a median follow up of 5 years, biochemical progression-free survival (PFS) was<br />
significantly improved in the immediate radiotherapy group (74.0% versus 52.6%;<br />
p
External Beam Radiotherapy (EBRT)<br />
Overview<br />
• Selley et al. reviewed 21 observational studies and one RCT involving radiotherapy and found that<br />
survival and recurrence rates are associated with grade and stage of the disease. The 5-year DFS<br />
<strong>for</strong> those with T1–T2 stage disease averaged 70−80%. Local progression was observed in 10−20%<br />
of these patients, while distant metastases were observed in 20−40%. 38<br />
• Nilsson et al. per<strong>for</strong>med a systematic overview of radiotherapy in <strong>prostate</strong> <strong>cancer</strong>. Data from 26<br />
non-randomised trials of conventional EBRT showed a 10-year DFS of 100%, 69% and 57% <strong>for</strong><br />
T1a, T1b and T2 stage disease, respectively. 51<br />
• Long-term follow-up after EBRT continues to demonstrate an improvement in cause-specific<br />
survival. Improved selection and technical developments in radiotherapy leading to increased<br />
doses have shown better results.<br />
Three-dimensional con<strong>for</strong>mal radiotherapy (3D-CRT)<br />
• There is evidence that increased radiation dose is associated with increased <strong>cancer</strong> cell kill <strong>for</strong> men<br />
with localised <strong>prostate</strong> <strong>cancer</strong>. However, the traditional two-dimensional technique of treatment<br />
planning and delivery is limited by the normal tissue toxicity of the surrounding structures<br />
(bladder, rectum and bowel), such that the dose that can be safely delivered to the <strong>prostate</strong><br />
by EBRT is 65−70 Gy. Several technological advances over the last 20 years have enhanced the<br />
precision of EBRT, and have resulted in improved outcomes.<br />
• The three-dimensional con<strong>for</strong>mal radiotherapy (3D-CRT) approach reduces the dose-limiting late<br />
side-effect of proctitis 52 and has allowed <strong>for</strong> dose escalation to the whole <strong>prostate</strong> to 78 Gy.<br />
Intensity Modulated Radiotherapy (IMRT)<br />
• IMRT is an advanced technique of 3D-CRT. IMRT can modify the shape and intensity of the<br />
<strong>multi</strong>ple radiotherapy beams. It is very precise in targeting the treatment area, sparing<br />
surrounding tissue. IMRT is currently under evaluation, particularly <strong>for</strong> the irradiation of pelvic<br />
lymph nodes.<br />
• IMRT may result in reduced rectal toxicity when using doses greater than 80 Gy.<br />
Dose escalation<br />
• Evidence of the benefits of dose escalation has been demonstrated <strong>for</strong> T1−T3 <strong>prostate</strong> <strong>cancer</strong> by<br />
Pollack et al. in a phase III randomised study undertaken at the MD Anderson Hospital. 53<br />
o A total of 305 men were randomised between 1993 and 1998 to compare the efficacy of 70<br />
Gy versus 78 Gy with a median follow-up of 60 months. The primary endpoint was freedom<br />
from failure (FFF), including biochemical failure, which was defined as three rises in PSA level.<br />
o The FFF rates <strong>for</strong> the 70 Gy and 78 Gy arms at 6 years were 64% and 70%, respectively (p=0.03).<br />
Dose escalation to 78 Gy preferentially benefited those with a pre-treatment PSA concentration<br />
>10 ng/ml; the FFF rate was 62% <strong>for</strong> the 78 Gy arm versus 43% <strong>for</strong> those who received 70 Gy<br />
(p=0.01). For patients with a pre-treatment PSA concentration ≤10 ng/ml, no significant doseresponse<br />
relationship was found, with an average 6-year FFF rate of about 75%.<br />
o Although no difference in OS occurred, the freedom from distant metastasis rate was<br />
higher <strong>for</strong> those with PSA levels >10 ng/ml who were treated to 78 Gy (98% versus 88%<br />
at 6 years, p=0.056).<br />
24
• Dearnaley and colleagues have reported their findings from the MRC RT01 study. 54<br />
o In this 3D-CRT trial, 843 men were randomised to a standard dose of 64 Gy compared with<br />
an escalated dose of 74 Gy, with all men also receiving neoadjuvant hormone therapy.<br />
o Patients receiving the conventional dose had 5-year biochemical PFS rates of 60% compared<br />
to 71% in the dose-escalated arm. Advantages were also seen in terms of clinical PFS and the<br />
decreased use of androgen suppression.<br />
o Although these and other studies have shown benefits from dose escalation with 3D-CRT<br />
techniques, this has been offset to a degree by a reported increase in late rectal toxicity.<br />
• Prospective non-randomised studies conducted at the Memorial Sloan Kettering <strong>cancer</strong> centre<br />
have compared the outcomes of 1100 men who received doses in the range of 64−70 Gy and<br />
76−86 Gy using IMRT. 55<br />
o The results were evaluated within prognostic risk groups (using clinical stage, Gleason grade<br />
and presenting PSA concentration). They demonstrated that increasing the dose delivered<br />
beyond 70.2 Gy in men with intermediate- and high-risk disease improved the 5-year actuarial<br />
PSA relapse-free survival rate from 50% to 70% and 21% to 47%, respectively, in these two<br />
risk categories.<br />
• IMRT has the potential to reduce late rectal toxicity as shown in a further study that reports 3-year<br />
actuarial ≥grade 2 gastrointestinal toxicity at 4%. 56<br />
• A further development under investigation involves a change in the traditional fractionation<br />
schedules. Hypofractionation may improve <strong>cancer</strong> control <strong>for</strong> the same level of radiation-related<br />
toxicity and be a more effective treatment <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong> with a predicted low alpha/<br />
beta ratio. Phase II dose escalation studies using shortened schedules of hypofractionated IMRT<br />
regimens have indicated acceptable early toxicity. 57<br />
• The CHHiP (Conventional or Hypofractionated High Dose IMRT <strong>for</strong> Prostate Cancer) study is<br />
currently recruiting patients in the UK to compare standard fractionation IMRT (74 Gy in 37<br />
fractions) to two hypofractionated IMRT regimens (60 Gy in 20 fractions or 57 Gy in 19 fractions)<br />
in combination with neoadjuvant hormone therapy. 58<br />
Patient selection<br />
• EBRT can be unsuitable <strong>for</strong> patients with bilateral hip replacement, previous radiotherapy, severe<br />
proctitis or bowel morbidity.<br />
Side-effects<br />
• Acute complications include cystitis, faecal frequency and urgency, proctitis and rectal bleeding.<br />
• Late complications occurring 3 months or later after treatment include impotence, bleeding,<br />
proctitis and diarrhoea.<br />
EBRT plus neoadjuvant hormone therapy<br />
• Neoadjuvant hormone therapy reduces <strong>prostate</strong> volume by 30−40%. 59, 60 This can reduce the size of<br />
the treatment field and as a result the level of toxicity experienced.<br />
• There are also reports of an additive or synergistic effect on tumour cell kill with combined<br />
therapy. Theories as to the mechanism of this include improved oxygenation by reducing tumour<br />
bulk and movement of hormone-responsive cells into a resting phase, which could reduce<br />
repopulation rate and enhance tumour cell death (increased apoptosis). 61<br />
• The RTOG 86-10 trial randomised 471 men with T2−T4 <strong>prostate</strong> <strong>cancer</strong> to radiotherapy +/− 4<br />
months of androgen deprivation therapy (ADT) be<strong>for</strong>e and during EBRT or to radiotherapy alone. 62<br />
25
o At median follow-up of 8.7 years, there was a trend to improved survival (8-year survival<br />
53% versus 44%, p=0.1) <strong>for</strong> those treated by hormone therapy with radiotherapy, which was<br />
significant <strong>for</strong> the subgroup with Gleason grade 2−6 disease (70% versus 52%, p=0.015). 62<br />
o Ten-year OS estimates (43% versus 34%) and median survival times (8.7 versus 7.3 years)<br />
favoured combined therapy with hormones and radiation compared to radiation treatment<br />
alone; however, these differences did not reach statistical significance (p=0.12).<br />
o There was a statistically significant improvement in 10-year disease-specific mortality<br />
(23% versus 36%; p=0.01), distant metastases (35% versus 47%; p=0.006), DFS (11% versus<br />
3%; p
Low dose rate (LDR) brachytherapy<br />
Overview<br />
• In 2005, NICE reviewed the medical literature on LDR brachytherapy and concluded that, in the<br />
absence of randomised trials, the results of LDR brachytherapy are comparable to those achieved<br />
with surgery or EBRT in well-selected patients. 66<br />
• Suitable patients include those with localised disease (up to T2a) with a Gleason grade ≤6, and a<br />
PSA concentration ≤10 ng/ml. Patients with significant urinary symptoms or post-TURP may not be<br />
suitable.<br />
• Brachytherapy is as effective as radical <strong>prostate</strong>ctomy in patients with low-risk localised disease. 67<br />
• In intermediate-risk localised disease, the comparison is less clear, because many studies have<br />
added EBRT in combination. 68<br />
• Brachytherapy is a single-step procedure following a spinal or general anaesthetic.<br />
Brachytherapy plus EBRT<br />
• In a matched-pair analysis, the 5-year biochemical failure-free survival rate was 86% <strong>for</strong> patients<br />
treated with EBRT and LDR brachytherapy, and 72% <strong>for</strong> patients treated with EBRT alone (p=0.03).<br />
Both treatments were associated with comparable incidences of late genitourinary side-effects<br />
(18−19%). Late rectal toxicity decreased by 15% in patients treated with EBRT and brachytherapy<br />
(p=0.0003). 69<br />
Brachytherapy plus neoadjuvant hormone therapy<br />
• The role of neoadjuvant hormone therapy with brachytherapy is controversial. It is used to<br />
reduce the <strong>prostate</strong> volume when it exceeds 50 ml, in order to facilitate brachytherapy. Volume<br />
reduction decreases the total isotope activity required, potentially improves implant dosimetry<br />
and decreases pubic arch interference. 70<br />
Patient selection (exclusions)<br />
• Prostate size >50 ml<br />
• Recent TURP<br />
• Significant urinary outflow obstruction<br />
• Previous AP resection<br />
• Previous high dose pelvic radiotherapy<br />
27
Side-effects<br />
• A review of 16 studies by Crook et al. showed acute adverse events as: 67<br />
o Irritant urinary symptoms: 46−54%<br />
o Acute urinary retention: 1−14%<br />
o Acute proctitis: 1−2%<br />
o Chronic adverse events (rein<strong>for</strong>ced by Wills et al., 1999 71 ):<br />
• Incontinence: 5−6%<br />
• Haematuria: 1−2%<br />
• Strictures: 1−2%<br />
• Proctitis: 1−3%<br />
• Erectile dysfunction: 4−14% (or up to 38% in Wills et al., 1999 71 and up to 50% at 5 years<br />
in Merrick et al., 2001 68 ).<br />
Clinical evidence<br />
Table 4: Experience using trans-perineal implants as monotherapy (T1, T2 <strong>cancer</strong>s)<br />
Author Number of men Isotope<br />
*Series excluded Gleason grade >7, 38% with pre-treatment PSA ≤4.0 ng/ml<br />
Median follow-up PSA results<br />
(months) (months)<br />
Beyer & Priestley,<br />
79% with PSA<br />
489 I-125 35<br />
199772
Novel therapies<br />
Cryotherapy/High-intensity focused ultrasonography (HIFU)<br />
• The development of third-generation <strong>prostate</strong> cryotherapy has allowed the introduction of<br />
ultra-thin needles to deliver a minimally-invasive treatment <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong> patients in the<br />
primary and salvage setting<br />
79, 80<br />
o Early results established the low incidence of serious side-effects and good PSA control<br />
o Longer-term follow-up series show biochemical DFS at 10 years of 80.56% <strong>for</strong> low-risk,<br />
74.16% <strong>for</strong> moderate-risk and 45.54% <strong>for</strong> high-risk <strong>prostate</strong> <strong>cancer</strong> patients<br />
• This treatment has been approved by the American Urological Association and the European<br />
Association of Urology <strong>for</strong> treatment of patients with primary and radiation-failed <strong>prostate</strong><br />
<strong>cancer</strong><br />
• In the NICE guidelines, the minimally-invasive treatments of cryosurgery and HIFU were<br />
considered to be experimental and <strong>for</strong> use only within the clinical trial setting 29<br />
o After further clarification, it was agreed that these treatments would be funded by Primary<br />
Care Trusts provided patient data were collected in an approved way. Following consultation<br />
with the BAUS section of Oncology, a national database has been established to collect data<br />
from <strong>prostate</strong> <strong>cancer</strong> patients undergoing cryotherapy or HIFU <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong>. Inclusion<br />
of patients in this database is considered necessary to fulfil the NICE guidelines.<br />
• These treatments may be offered to patients with stage T1, T2 or T3 as a primary treatment or in<br />
salvage <strong>prostate</strong> <strong>cancer</strong> patients.<br />
o The staging requirements are a positive biopsy and MRI and bone scan showing no evidence<br />
of metastatic spread.<br />
29
Locally Advanced Disease (Non-metastatic):<br />
Management Options<br />
Figure 3: Treatment algorithm <strong>for</strong> locally advanced (non-metastatic) disease<br />
Key Questions <strong>for</strong> the <strong>MDT</strong><br />
• TNM stage?<br />
• Gleason grade?<br />
• PSA/PSA Kinetics?<br />
• Age/co-morbidity/life<br />
expectancy?<br />
• Symptoms:<br />
– Bowel?<br />
– Urine IPSS score?<br />
• Sexual function?<br />
• Family history?<br />
• Bone pain?<br />
• Osteoporosis risk?<br />
Is this patient suitable <strong>for</strong> clinical trial?<br />
High-risk localised<br />
<strong>MDT</strong><br />
Diagnostic Tests<br />
• Digital rectal exam (DRE)<br />
• PSA<br />
• Transrectal ultrasound<br />
(TRUS)/biopsy<br />
• MRI/CT pelvic scan<br />
• Bone scan<br />
• Consider lymph node sampling<br />
(if this will determine changes<br />
in management approach)<br />
MANAGEMENT OPTIONS 1<br />
T1/T2 N+ Mo<br />
T3/T4 No/N+ Mo<br />
External beam radiotherapy (EBRT)<br />
+/- HDR brachytherapy boost<br />
+/-neo-adjuvant, concomitant<br />
and adjuvant hormone therapy<br />
Hormone therapy alone<br />
Watchful waiting<br />
Ongoing Support<br />
Local patient support network<br />
Role of nurse/GP/healthcare professional <strong>team</strong><br />
Key Discussion Points<br />
with the Patient<br />
• Survival/prognosis?<br />
• Treatment options?<br />
• Treatment side-effects?<br />
• Impact on quality of life?<br />
• Importance of:<br />
– Psychological impact<br />
to patient and family?<br />
– Family history?<br />
– Clinical trials?<br />
– Sexual function?<br />
– Urinary function?<br />
– Bowel function?<br />
– Physical strength, energy?<br />
– Level of activity?<br />
– Accessibility to Rx?<br />
30
The term locally advanced <strong>prostate</strong> <strong>cancer</strong> can be used to encompass a spectrum of disease profiles<br />
that may include any of the following:<br />
• Clinical stage T3, T4 or N1 <strong>cancer</strong>s without evidence of distant metastases (M0)<br />
• Clinical stages T1 and T2 (‘localised’) at diagnosis, where ‘high-risk’ features (PSA concentration<br />
≥20 ng/ml or Gleason grade ≥8) indicate the likelihood of extraprostatic invasion or clinically<br />
undetectable metastatic disease<br />
• Pathological stage pT2 or pT3 disease with ‘high-risk’ features due to upstaging from additional<br />
pathological in<strong>for</strong>mation after radical <strong>prostate</strong>ctomy<br />
Men with locally advanced or high-risk <strong>prostate</strong> <strong>cancer</strong> generally have a significant risk of disease<br />
progression and <strong>cancer</strong>-related death if left untreated. These patients present two specific challenges.<br />
There is a need <strong>for</strong> local control and also a need to treat any microscopic metastases likely to be<br />
present but undetectable until disease progression. The optimal treatment approach will often<br />
there<strong>for</strong>e utilise <strong>multi</strong>ple modalities. The exact combinations, timing and intensity of treatment<br />
continue to be strongly debated. Management decisions should be made after all treatments have<br />
been discussed by the <strong>MDT</strong> and the balance of benefits and side-effects of each therapy modality have<br />
been considered by the patient with regard to their own individual circumstances.<br />
Watchful waiting<br />
Overview<br />
• Data on the use of watchful waiting in locally advanced disease is sparse.<br />
• Two non-randomised studies concluded that immediate orchidectomy was not associated with a<br />
81, 82<br />
survival advantage compared with therapy delayed until metastatic progression.<br />
• A pooled analysis of data from 2 RCTs involving 1036 men with locally advanced disease not<br />
suitable <strong>for</strong> curative treatment (T2−T4) suggested no survival benefit <strong>for</strong> immediate versus<br />
delayed hormone therapy at 1, 5 or 10 years. 83<br />
Clinical evidence<br />
• Adolfsson et al. prospectively followed 50 patients with locally advanced <strong>prostate</strong> <strong>cancer</strong> who<br />
were only treated upon patient request or when they became symptomatic. All patients were<br />
followed-up <strong>for</strong> more than 144 months, or had died be<strong>for</strong>e that point. OS and DFS at 5, 10 and 12<br />
years was 68% and 90%, 34% and 74%, and 26% and 70%, respectively. 84<br />
31
Hormone therapy<br />
Immediate versus deferred hormonal treatment<br />
• Immediate versus deferred treatment <strong>for</strong> advanced <strong>prostate</strong> <strong>cancer</strong> was investigated by the MRC<br />
Prostate Working Party Investigators Group. An RCT of 943 men with asymptomatic metastases or<br />
locally advanced disease, not suitable <strong>for</strong> curative treatment, was undertaken, with randomisation<br />
to immediate or deferred hormone therapy. 85<br />
o There was a significant advantage in the immediate treatment group in terms of distant<br />
progression. Mortality was only significantly changed by treating immediately in those with<br />
M0 disease (Table 5).<br />
o A modest but statistically significant increase in OS was seen in the immediate treatment<br />
group, but not significant difference in <strong>prostate</strong> <strong>cancer</strong> mortality or symptom-free survival<br />
was demonstrated.<br />
o Due consideration must there<strong>for</strong>e be given to potential effects of long-term ADT versus the<br />
potential avoidance of such effects in patients if hormone therapy is deferred. 86<br />
Table 5: Effect of immediate versus deferred hormonal treatment 85<br />
Immediate Deferred<br />
Distant progression 26% 45%<br />
Mortality due to <strong>prostate</strong> <strong>cancer</strong> M0 disease 31.6% 48.8%<br />
M1 disease No significant No significant<br />
difference difference<br />
Hormone therapy plus standard care<br />
• The <strong>multi</strong>centre, international Early Prostate Cancer (EPC) study evaluated the efficacy and<br />
tolerability of adding the non-steroidal anti-androgen bicalutamide 150 mg once-daily to<br />
standard care (<strong>prostate</strong>ctomy, radiotherapy or watchful waiting). 8113 patients with localised or<br />
locally advanced non-metastatic <strong>prostate</strong> <strong>cancer</strong> were included. 87<br />
o Objective PFS and OS were defined as the primary endpoints. At a third analysis, the median<br />
follow-up was 7.4 years. Exploratory analyses were also conducted to determine the efficacy<br />
of bicalutamide in clinically relevant subgroups.<br />
o A trend towards increased survival was seen <strong>for</strong> the subgroup treated with bicalutamide who<br />
would otherwise have undergone watchful waiting (HR 0.81; 95%CI: 0.66−1.01; p=0.06).<br />
o A significant improvement in objective PFS in favour of bicalutamide 150 mg <strong>for</strong> all locally<br />
advanced disease patients was demonstrated irrespective of standard care received (HR<br />
0.69; 95%CI: 0.58−0.83; p
Radiotherapy plus hormone therapy<br />
• A study by Widmark et al. has shown that the addition of radiotherapy to hormone therapy <strong>for</strong><br />
men with locally advanced or high-risk <strong>prostate</strong> <strong>cancer</strong> halves the 10-year <strong>prostate</strong> <strong>cancer</strong>-specific<br />
mortality and substantially decreases overall mortality. 88<br />
o This phase III study comparing endocrine therapy with and without local radiotherapy<br />
randomised 875 patients with locally advanced <strong>prostate</strong> <strong>cancer</strong> (T3; 78%; PSA concentration<br />
EBRT +/− neoadjuvant, concomitant and adjuvant hormone therapy<br />
Radiotherapy alone<br />
• In locally advanced disease, EBRT alone has been shown to have a poorer outcome than in<br />
localised <strong>prostate</strong> <strong>cancer</strong>. Consequently, combination therapy with radiotherapy and hormone<br />
therapy is rapidly being accepted as standard practice.<br />
• Although it has been widely used, there are still many uncertainties associated with radical<br />
radiotherapy with regard to the optimum dose and field size (particularly to what extent the<br />
treatment volume should try to include pelvic lymph nodes). These uncertainties are compounded<br />
by the availability of new approaches to the delivery of radiotherapy, such as IMRT. The latter is<br />
intended to shape the radiation field more precisely to the tumour volume, thereby reducing the<br />
side-effects of treatment and possibly allowing dose escalation that enhances its local efficacy.<br />
Radiotherapy target volume/lymph nodes<br />
• In high-risk patients the consensus is that the seminal vesicles should be included.<br />
• The RTOG 9413 trial was designed to determine whether there was an advantage in terms<br />
of PFS with total androgen suppression, whole pelvic radiotherapy followed by a <strong>prostate</strong><br />
boost compared with total androgen suppression and <strong>prostate</strong>-only radiotherapy. The trial<br />
also investigated the timing of hormone therapy with a further randomisation. One group<br />
received neoadjuvant hormone therapy followed by concurrent total androgen suppression and<br />
radiotherapy while the other group was treated with radiotherapy followed by adjuvant hormone<br />
therapy. Patients with non-metastatic disease but an estimated risk of lymph node involvement of<br />
>15% were randomised between the 4 arms. 89<br />
o The difference in OS <strong>for</strong> the 4 arms was statistically significant (p=0.027).<br />
o However, no statistically significant differences were found in PFS or OS between neoadjuvant<br />
versus adjuvant hormone therapy and whole pelvis radiotherapy compared with <strong>prostate</strong>only<br />
radiotherapy. A trend towards a difference was found in PFS (p=0.065) in favour of the<br />
whole pelvic radiotherapy + neoadjuvant hormone arm compared with the <strong>prostate</strong>-only<br />
radiotherapy + neoadjuvant hormones and whole pelvic radiotherapy + adjuvant hormone<br />
treatment arms.<br />
o These results have demonstrated that when neoadjuvant hormone therapy is used in<br />
conjunction with radiotherapy, whole pelvic treatment yields a better PFS than <strong>prostate</strong>-only<br />
radiotherapy. It also showed an improved OS when whole pelvic radiotherapy was combined<br />
with neoadjuvant rather than short-term adjuvant hormone therapy.<br />
Radiotherapy dose escalation<br />
• Evidence suggests that patients treated with radiotherapy to the <strong>prostate</strong> have a significantly<br />
better outcome, because the dose to the gland is increased. The benefit is greatest in those<br />
patients with high-risk features.<br />
• Debate remains over the best way of increasing the dose without significantly increasing normal<br />
tissue toxicity. 3D-CRT, IMRT and high dose rate (HDR) brachytherapy boost are methods currently<br />
under evaluation.<br />
34
• Evidence of the benefits of dose escalation has been demonstrated <strong>for</strong> T1−T3 <strong>prostate</strong> <strong>cancer</strong> by<br />
Pollack in a phase III randomised study at the MD Anderson Hospital. 53<br />
o A total of 305 men were randomised between 1993 and 1998 to compare the efficacy of<br />
70 Gy versus 78 Gy with a median follow-up of 60 months. The primary endpoint was FFF,<br />
including biochemical failure, which was defined as three rises in PSA level.<br />
o The FFF rates <strong>for</strong> the 70 Gy and 78 Gy arms at 6 years were 64% and 70%, respectively<br />
(p=0.03).<br />
o Dose escalation to 78 Gy preferentially benefited those with a pre-treatment PSA<br />
concentration >10 ng/ml; the FFF rate was 62% <strong>for</strong> the 78 Gy arm versus 43% <strong>for</strong> those who<br />
received 70 Gy (p=0.01). For patients with a pre-treatment PSA concentration ≤10 ng/ml, no<br />
significant dose response was found, with an average 6-year FFF rate of about 75%.<br />
o Although no difference in OS was observed, the freedom from distant metastasis rate was<br />
higher <strong>for</strong> those with PSA concentrations >10 ng/ml who were treated to 78 Gy (98% versus<br />
88% at 6 years; p=0.056).<br />
• Dearnaley and colleagues have reported their findings from the MRC RT01 study. 54<br />
o In this 3D-CRT trial 843 men were randomised to standard dose of 64 Gy compared to an<br />
escalated dose of 74 Gy with all men receiving neoadjuvant hormone therapy.<br />
o Patients receiving the conventional dose had 5-year biochemical PFS rates of 60% compared<br />
with 71% in the dose-escalated arm. Advantages were also seen in terms of PFS and the<br />
decreased use of androgen suppression.<br />
o Although these and other studies have shown benefits from dose escalation with 3D-CRT<br />
techniques, this has been offset to a degree by a reported increase in late rectal toxicity.<br />
• Prospective non-randomised studies at the Memorial Sloan Kettering <strong>cancer</strong> centre have<br />
compared the outcomes of 1100 men who received doses in the range of 64 to 70 Gy and 76 to<br />
86 Gy using IMRT. The results were evaluated within prognostic risk groups (using clinical stage,<br />
Gleason grade and presenting PSA). 55<br />
• They demonstrated that increasing the dose delivered beyond 70.2 Gy in men with intermediate-<br />
and high-risk disease improved the 5-year actuarial PSA relapse-free survivals from 50% to 70%<br />
and 21% to 47%, respectively, in these two risk categories.<br />
• These results confirmed the advantage of dose escalated radiotherapy with doses of over 80 Gy.<br />
IMRT has the potential to reduce late rectal toxicity as shown in a further study by Zelefsky which<br />
reports 3-year actuarial ≥ grade 2 gastrointestinal toxicity at 4%. 56<br />
• A further development under investigation involves a change in the traditional fractionation<br />
schedules. Hypofractionation may improve <strong>cancer</strong> control <strong>for</strong> the same level of radiation-related<br />
toxicity and be a more effective treatment <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong> with a predicted low alpha/<br />
beta ratio. Phase II dose escalation studies using shortened schedules of hypofractionated IMRT<br />
regimens have indicated acceptable early toxicity. 57<br />
• The CHHiP study is currently recruiting patients in the UK to compare standard fractionation IMRT<br />
(74 Gy in 37 fractions) to two hypofractionated IMRT regimens (60 Gy in 20 fractions or 57 Gy in<br />
19 fractions) in combination with neoadjuvant hormone therapy. 58<br />
35
HDR brachytherapy boost<br />
• HDR brachytherapy is a safe, reproducible and effective way of boosting conventional EBRT. There<br />
is published evidence <strong>for</strong> this approach demonstrating improved biochemical control and causespecific<br />
survival without a significant increase in toxicity.<br />
• Currently, HDR brachytherapy is used in combination with EBRT and is felt appropriate <strong>for</strong><br />
patients with high-risk localised or locally advanced <strong>prostate</strong> <strong>cancer</strong>. 90<br />
EBRT plus neoadjuvant hormone therapy<br />
• Neoadjuvant hormone therapy reduces <strong>prostate</strong> volume by 30−40%. 59, 60 This can reduce the size<br />
of the treatment field and as a result the level of toxicity experienced.<br />
• There are also reports of an additive or synergistic effect on tumour cell kill with combined<br />
therapy. Theories as to the mechanism of this include improved oxygenation by reducing tumour<br />
bulk and movement of hormone-responsive cells into a resting phase, which could reduce<br />
repopulation rate and enhance tumour cell death (increased apoptosis). 61<br />
• The RTOG 86-10 trial randomised 471 men with T2−T4 <strong>prostate</strong> <strong>cancer</strong> to radiotherapy +/− 4<br />
months of ADT (goserelin 3.6 mg depot once-monthly plus flutamide 250mg tid) be<strong>for</strong>e and<br />
during EBRT or to radiotherapy alone. The median follow-up was 6.7 years <strong>for</strong> all patients and 8.6<br />
years <strong>for</strong> surviving patients. 62<br />
o At median follow-up of 8.7 years <strong>for</strong> surviving patients, there was a trend to improved<br />
survival (8-year survival 53% versus 44%, p=0.1) <strong>for</strong> those treated by hormone therapy with<br />
radiotherapy, which was significant <strong>for</strong> the subgroup with Gleason grade 2−6 disease (70%<br />
versus 52%, p=0.015). 62<br />
o Ten-year OS estimates (43% versus 34%) and median survival times (8.7 versus 7.3 years)<br />
favoured combined therapy with hormones and radiation compared to radiation treatment<br />
alone; however, these differences did not reach statistical significance (p=0.12). 63<br />
o There was a statistically significant improvement in 10-year disease-specific mortality<br />
(23% versus 36%; p=0.01), distant metastases (35% versus 47%; p=0.006), DFS (11% versus<br />
3%; p
Clinical evidence<br />
• Adjuvant androgen suppression immediately after radical radiotherapy has been shown to<br />
significantly increase OS, PFS, and significantly reduce local progression, distant metastases and<br />
biochemical progression in several large randomised studies.<br />
• Bolla et al. (EORTC 22863) randomised 415 patients with locally advanced non-metastatic <strong>prostate</strong><br />
<strong>cancer</strong> (T1−4, Nx, M0) to receive either radiotherapy with immediate goserelin 3.6 mg therapy<br />
(every 4 weeks <strong>for</strong> 3 years) plus cyproterone acetate (CPA) during the first month of treatment <strong>for</strong><br />
disease flare (n=207) or radiotherapy alone (n=208). 91<br />
o After a mean follow-up of 66 months, the 5-year DFS rate was 74% versus 40% <strong>for</strong> the<br />
combined and EBRT alone groups, respectively (p=0.001).<br />
o Furthermore, the corresponding OS and <strong>cancer</strong>-specific survival rates at 5 years were 78% and<br />
62% (p=0.0002), while the <strong>cancer</strong>-specific survival rates were 94% versus 79%.<br />
o A further analysis of this study with a median follow-up of 9.1 years reported 192 deaths<br />
(112 in radiotherapy alone and 80 in the combined treatment arm). 92<br />
o The addition of 3 years of ADT increased the 10-year OS from 39.8% to 58.1% (HR 0.60;<br />
95%CI: 0.45−0.80; p=0.0004), clinical PFS from 22.7% to 47.7% (HR 0.42; 95%CI: 0.33−0.55;<br />
p
• Hanks et al. (RTOG 92-02) investigated the use of long-term androgen suppression following<br />
neoadjuvant hormonal cytoreduction and radiotherapy in locally advanced <strong>prostate</strong> <strong>cancer</strong><br />
(T2c to T4 with no extra pelvic lymph node involvement and PSA
Locally Advanced (Non-metastatic) Disease:<br />
Relapse after Primary Treatment<br />
Figure 3: Treatment algorithm <strong>for</strong> locally advanced (non-metastatic) disease (cont.)<br />
Is this patient suitable <strong>for</strong> clinical trial?<br />
Post-radical <strong>prostate</strong>ctomy<br />
MANAGEMENT OPTIONS 2<br />
Failed local Rx with rising PSA<br />
and/or local recurrence+ Mo<br />
Active surveillance/watchful waiting Active surveillance/watchful waiting<br />
Hormone therapy alone Hormone therapy alone<br />
External beam radiotherapy<br />
(EBRT) +/– concomitant +/–<br />
adjuvant hormone therapy<br />
Post-radical radiotherapy/<br />
brachytherapy<br />
Salvage <strong>prostate</strong>ctomy<br />
Novel local salvage therapy<br />
Ongoing Support<br />
Local patient support network<br />
Role of nurse/GP/healthcare professional <strong>team</strong><br />
Rising PSA levels<br />
• The PSA concentration at which to define treatment failure after <strong>prostate</strong>ctomy varies<br />
in the literature.<br />
Definitions of recurrence<br />
• The Phoenix definition of relapse after radiotherapy is nadir plus 2. 97<br />
• Patients whose PSA never falls to an undetectable level in the post-operative period are generally<br />
considered to have systemic disease. However, some may have local disease amenable to salvage<br />
radiotherapy, and so need to be assessed to determine the best management plan.<br />
• A PSA concentration that rises rapidly in the post-operative setting may be indicative of metastatic<br />
disease, while a PSA that remains undetectable over a long period then gradually rises may be<br />
more likely to indicate local recurrence.<br />
39
• Pound et al. carried out a retrospective review of 1997 men undergoing radical <strong>prostate</strong>ctomy<br />
by a single surgeon <strong>for</strong> clinically localised disease with no neoadjuvant or adjuvant treatment. 98<br />
A PSA ≥0.2 ng/ml was deemed evidence of recurrence.<br />
o At 15 years, 15% had PSA elevation and 34% of these had developed metastases.<br />
o The median time from PSA elevation to metastatic disease was 8 years.<br />
o After development of metastases, the median actuarial time to death was 5 years. In the<br />
survival analysis, time to biochemical progression, Gleason grade and PSA doubling time<br />
were predictive of the probability and time to the development of metastatic disease.<br />
• After completion of radiotherapy and hormonal treatment, testosterone recovery usually occurs.<br />
This may cause some PSA elevation that is related to normal <strong>prostate</strong> tissue recovery and not<br />
disease recurrence.<br />
• The definition of disease recurrence in the setting of combined therapy remains a matter<br />
of debate and consensus is awaited.<br />
• Benign PSA rises (PSA bounce) occur in approximately 12% of patients following EBRT<br />
and 30% following LDR brachytherapy in the absence of neoadjuvant hormonal treatment<br />
(starting between 18 months and 2 years after treatment).<br />
Local recurrence after radical <strong>prostate</strong>ctomy<br />
Overview<br />
• Overall, approximately 40% of patients who have a radical <strong>prostate</strong>ctomy have biochemical<br />
evidence of recurrence at some point.<br />
• Determining whether relapse is local or distant is important in determining optimal treatment.<br />
However, post-<strong>prostate</strong>ctomy imaging is unhelpful as this will always be negative, so there is<br />
no way of defining local versus distant disease categorically. Other factors that may aid this<br />
distinction include:<br />
o Timing and pattern of PSA relapse (rapid rise post-operatively indicates distant spread)<br />
o Involvement of seminal vesicles or lymph nodes<br />
o Margin status at surgery<br />
o Gleason grade<br />
• Radical salvage treatment is usually via radiotherapy to the <strong>prostate</strong> bed +/− hormone therapy.<br />
The optimal time of treatment, i.e. immediate adjuvant or early salvage EBRT, is currently<br />
uncertain. The timing and duration of hormone therapy is also unclear.<br />
• The RADICALS study is investigating the timing of radiotherapy (immediate versus early salvage)<br />
and hormone duration. 50<br />
40
Clinical evidence<br />
• The EORTC 22911 study was designed to investigate benefit <strong>for</strong> immediate post-operative<br />
radiotherapy in 502 patients with pT3 disease or positive surgical margins as opposed to<br />
radiotherapy offered <strong>for</strong> biochemical or clinical relapse. 48<br />
o After a median follow-up of 5 years, biochemical PFS was significantly improved in the<br />
immediate radiotherapy group (74.0% versus 52.6%; p
Recurrence after radical radiotherapy<br />
Overview<br />
• The therapeutic options <strong>for</strong> recurrence following radiotherapy include:<br />
o Salvage radical <strong>prostate</strong>ctomy: associated with 5-year biochemical DFS rates of 55−69%, but<br />
the technique is associated with a significant incidence of complications, such as rectal injury,<br />
anastamotic stricture and urinary incontinence.<br />
o Salvage cryotherapy: 5-year biochemical PFS ranges from 40% to 73%. The complications<br />
of salvage cryotherapy are erectile dysfunction, pelvic, rectal or perineal pain, recto-urethral<br />
fistula, bladder outlet obstruction and urethral stricture.<br />
o Salvage HIFU is currently under investigation.<br />
o Hormone therapy can be given in combination with local treatments or as monotherapy.<br />
Clinical evidence<br />
• Touma et al. reviewed the efficacy and safety of salvage radical <strong>prostate</strong>ctomy, cryotherapy and<br />
brachytherapy <strong>for</strong> recurrence following definitive radiotherapy. 100<br />
o Salvage radical <strong>prostate</strong>ctomy is associated with 5-year biochemical DFS rates of 55−69%, but<br />
the technique is associated with a significant incidence of complications, such as rectal injury,<br />
anastomotic stricture and urinary incontinence.<br />
o The four studies of salvage cryotherapy reviewed used varying definitions of recurrence.<br />
The 5-year biochemical PFS ranged from 40% when failure was defined as PSA 2 above<br />
nadir, to 62% and 73% when failure was defined as PSA greater than 2 and greater than 4,<br />
respectively.<br />
o The complications of salvage cryotherapy are erectile dysfunction, pelvic, rectal or perineal<br />
pain, rectourethral fistula, bladder outlet obstruction and urethral stricture.<br />
• In one trial of 49 patients reported by Grado et al., complications included lower urinary tract<br />
symptoms, especially in the first 3 months. TURP was necessary in 14% of patients due to bladder<br />
outlet obstruction, while haematuria occurred in 4% of cases, stricture in 6%, rectal ulcers in 4%<br />
and rectal bleeding necessitating colostomy in 2%. 101<br />
• In 71 patients with localised disease following EBRT, following HIFU, 80% demonstrated negative<br />
biopsies and 61% had a nadir PSA concentration
Advanced Prostate Cancer (Metastatic): Management Options<br />
Figure 4: Treatment algorithm <strong>for</strong> advanced (metastatic) disease<br />
Key Questions <strong>for</strong> the <strong>MDT</strong><br />
• TNM stage?<br />
• Gleason grade?<br />
• PSA/PSA Kinetics?<br />
• Age/co-morbidity/life<br />
expectancy?<br />
• Symptoms:<br />
– Bowel?<br />
– Urine IPSS score?<br />
• Sexual function?<br />
• Family history?<br />
• Bone pain?<br />
• Osteoporosis risk?<br />
• Palliative care referral?<br />
Is this patient suitable <strong>for</strong> clinical trial?<br />
Palliative Care<br />
• Pain control<br />
• Local radiotherapy<br />
Bone pain<br />
Spinal cord compression<br />
Nerve root compression<br />
• Continual assessment<br />
Second-/third-line if<br />
androgen sensitive?<br />
<strong>MDT</strong><br />
Diagnostic Tests<br />
• Digital rectal exam (DRE)<br />
• PSA<br />
• Transrectal ultrasound (TRUS)/<br />
biopsy (non mandatory if PSA<br />
>100 and radiological evidence<br />
of metastases)<br />
• Biochemistry screen<br />
• Full blood count<br />
• Bone scan<br />
• MRI/CT pelvic scan<br />
MANAGEMENT OPTIONS<br />
Proven M1/M2<br />
First line hormone therapy<br />
Significant rise in PSA Clinical/<br />
radiological progression<br />
Observation<br />
Second-/third-line hormone<br />
therapy<br />
Further progression<br />
Ongoing Support<br />
Local patient support network<br />
Role of nurse/GP/healthcare professional <strong>team</strong><br />
Key Discussion Points<br />
with the Patient<br />
• Survival/prognosis?<br />
• Treatment options?<br />
• Treatment side-effects?<br />
• Impact on quality of life?<br />
• Importance of:<br />
– Psychological impact<br />
to patient and family?<br />
– Family history?<br />
– Clinical trials?<br />
– Sexual function?<br />
– Urinary function?<br />
– Bowel function?<br />
– Physical strength, energy?<br />
– Level of activity?<br />
– Accessibility to Rx?<br />
HRPC<br />
Based on MRC evidence, the majority of patients with metastatic disease should be treated.<br />
Deferred treatment is acceptable only in highly selected, in<strong>for</strong>med patients.<br />
Clinical trials<br />
Chemotherapy<br />
Strontium<br />
Bisphosphonate<br />
43
Primary hormone therapy<br />
Overview<br />
• ADT is standard first-line treatment <strong>for</strong> the management of patients with metastatic disease.<br />
ADT can involve orchidectomy, LHRH agonists, anti-androgens and gonadotrophin-releasing<br />
hormone (GnRH) antagonists.<br />
• Orchidectomy remains the gold-standard ADT against which all other treatments are compared<br />
because of its rapid effects on total testosterone concentrations. 103<br />
104, 105<br />
• Survival appears equivalent with LHRH agonists and orchidectomy.<br />
• A meta-analysis has indicated that 2-year survival may be worse with medical treatment than<br />
with orchidectomy. 106<br />
• Patients, however, prefer medical treatment and in terms of usage, drug treatment represents<br />
the standard of care at all disease stages. 107−109<br />
• GnRH antagonists are clinically equivalent to LHRH agonists without causing the initial<br />
testosterone surge seen with LHRH agonists. Now licensed on the evidence of phase III clinical<br />
trial data, degarelix demonstrates reduced testosterone concentrations to below castrate levels<br />
in 3 days (90% decrease in median testosterone compared with leuprolide group experiencing<br />
a 65% increase in median testosterone levels; p
Table 6: Effect of immediate versus deferred hormonal treatment 85<br />
Combined (maximum) androgen blockade<br />
• There is debate over the use of combined androgen blockade (CAB). In 2000, the Prostate Cancer<br />
Trialists’ Collaborative Group published a meta-analysis of the available trials of CAB versus<br />
monotherapy. The analysis included 27 trials, which incorporated 8275 men, representing 98%<br />
111, 112<br />
of men ever randomised in trials of CAB versus monotherapy.<br />
o The 5-year survival <strong>for</strong> all patients receiving CAB was 25.4%, compared with 23.6% <strong>for</strong><br />
patients receiving monotherapy.<br />
o In subgroup analyses, patients treated with CPA seemed to fare slightly worse than those<br />
treated with flutamide or nilutamide, mostly secondary to non-<strong>prostate</strong> <strong>cancer</strong>-related<br />
deaths.<br />
• If the CPA studies were excluded, the results were as follows: 111<br />
Immediate Deferred<br />
Distant progression 26% 45%<br />
Mortality due to <strong>prostate</strong> <strong>cancer</strong> M0 disease 31.6% 48.8%<br />
M1 disease No significant No significant<br />
difference difference<br />
o CAB with flutamide alone was associated with an 8% reduction in the risk of death (95%CI:<br />
0.86−0.98; p=0.02), which translates to a small but significant improvement in 5-year survival<br />
over castration alone.<br />
o CAB with flutamide plus nilutamide was associated with an 8% reduction in the risk of death<br />
(95%CI: 1.00−1.27; p=0.005), which translates to a small but significant improvement in 5-year<br />
survival of 2.9% over castration alone.<br />
o Conversely, CAB with CPA is associated with an increased risk of death of 13% (95%CI:<br />
1.00−1.27; p=0.04), which translates to a small but significant reduction in 5-year survival<br />
of 2.8% over castration alone.<br />
• It can be concluded that the choice of anti-androgen used <strong>for</strong> CAB has an impact on outcome, and<br />
that CAB with a non-steroidal anti-androgen may offer a small but significant survival benefit.<br />
45
Second- or third-line hormone therapy<br />
• Some patients will respond to second-line hormone therapy (CAB with the addition of an antiandrogen,<br />
anti-androgen withdrawal, diethylstilboestrol [DES]). Anti-androgen withdrawal<br />
responses are seen in approximately 25% of cases who have been treated with first-line CAB<br />
or have had substantial (>1 year response) to second-line CAB.<br />
• A common second-line treatment is the addition of an anti-androgen. A retrospective analysis<br />
of 122 patients who received the addition of bicalutamide 50 mg to goserelin <strong>for</strong> PSA and clinical<br />
progression showed a >50% decrease in PSA concentration in 30% of patients (responders) and<br />
a reduction in PSA concentration in 75% of all patients. The median duration of response from<br />
start of bicalutamide 50 mg was 291 days <strong>for</strong> responders and 193 days <strong>for</strong> the population as a<br />
whole. Those patients with a short duration of response to goserelin monotherapy (
Chemotherapy, Strontium and Bisphosphonates<br />
Those patients who do not respond to hormone therapy are considered to have hormone-refractory<br />
<strong>prostate</strong> <strong>cancer</strong> (HRPC; i.e. unresponsive to all hormone therapies) or castrate-refractory <strong>prostate</strong><br />
<strong>cancer</strong> (unresponsive to treatment with LHRH agonists) and are candidates <strong>for</strong> chemotherapy, novel<br />
therapies and/or symptomatic local treatments.<br />
Chemotherapy<br />
• A prospective study by Tannock in 1996 compared the benefits of mitoxantrone 12 mg/m² every<br />
3 weeks plus prednisone 5 mg twice-daily with prednisone alone in 161 men with symptomatic<br />
HRPC. 116<br />
o The primary endpoint was palliative response defined as a 2-point decrease in pain as assessed<br />
by a 6-point pain scale.<br />
o There was a significant advantage to the chemotherapy combination with a 29% pain<br />
response compared to 12% with steroids alone.<br />
o The duration of palliation was 43 weeks versus 18 weeks (p
Side-effects<br />
• Side-effects of chemotherapy depend on the treatment, but usually include fatigue, nausea and<br />
vomiting, diarrhoea, hair loss and increased susceptibility to infection. Specific therapies to handle<br />
these side-effects may be necessary to improve the patient’s quality of life.<br />
Strontium<br />
• Metastatic pain can be palliated effectively with systemic radionuclide therapy with strontium<br />
chloride.<br />
• Relief of bone pain starts within 2 weeks. Possible initial bone pain flare may occur within 2 days,<br />
lasting 2−4 days.<br />
o Pain relief lasts 4−15 months.<br />
o 75−80% of patients experience significant palliation of pain.<br />
• A Canadian collaborative study showed significant improvement in quality of life, increased time<br />
to further metastases, significant reduction in the amount of additional radiotherapy needed,<br />
and significant falls in PSA and alkaline phosphatase. 120<br />
• Strontium is not associated with improvements in OS. 121<br />
• Four randomised clinical trials have reviewed the use of strontium. 122<br />
o One trial reported significant improvement in pain control, two trials reported fewer new<br />
sites of pain.<br />
o One trial showed no significant difference in pain control compared to a placebo but an<br />
improved 2-year survival rate.<br />
• A randomised clinical trial examining strontium versus placebo found a significant increase in<br />
median time to progression, but no significant effects on median OS or clinical response. 123<br />
Side-effects<br />
• The most notable side-effect of strontium is mild haematological suppression with a fall in<br />
circulating platelet and leukocyte counts recognised in most patients.<br />
o With usual therapeutic doses, platelets typically fall by 30% and leucocytes by 20%.<br />
o Clinically significant toxicity is rare, but its use is not recommended in patients with severely<br />
compromised bone marrow, platelet count
Bisphosphonates<br />
• The benefits of zoledronic acid, in combination with hormone therapy have been investigated<br />
in a study by Saad in men with HRPC and bone metastases. 124 This was a <strong>multi</strong>centre, randomised,<br />
placebo-controlled trial evaluating the efficacy of zoledronic acid 4 mg administered every<br />
3 weeks in 422 patients with HRPC <strong>for</strong> 15 months, with an option to continue <strong>for</strong> an additional<br />
9 months.<br />
o At the 2-year analysis, treatment with zoledronic acid was found to significantly reduce the<br />
percentage of patients with at least one skeletal-related event (SRE; defined as radiation <strong>for</strong><br />
bone pain or to prevent pathological fracture/spinal cord compression; pathological fracture;<br />
spinal cord compression; surgery to bone; change in antineoplastic therapy) compared with<br />
placebo (38% versus 49%; p=0.028). All SREs were delayed.<br />
o Zoledronic acid also significantly delayed the time to first SRE by around 6 months (median<br />
488 versus 321 days; p=0.009). Furthermore, patients in the zoledronic acid group had<br />
consistently lower incidences of all types of SRE than the placebo group. Pain scores were<br />
consistently lower in patients taking zoledronic acid 4mg than placebo, and significantly<br />
at 3, 9, 18, 21 and 24 months (p
Palliative Care<br />
Overview<br />
• Radiotherapy has been a mainstay in the palliation of painful metastatic bone lesions. Palliative<br />
radiotherapy can also aid other complications of metastatic disease, such as compression of the<br />
spinal cord or a nerve root, haematuria, ureteric obstruction, perineal discom<strong>for</strong>t caused by the<br />
local progression of <strong>prostate</strong> <strong>cancer</strong>, and symptomatic metastatic lymphadenopathy.<br />
Clinical evidence<br />
• Good evidence <strong>for</strong> the role of radiotherapy in palliation comes from McQuay et al. This systematic<br />
review covered 20 trials, which reported on 43 different radiotherapy fractionation schedules, and<br />
eight studies of radioisotopes. 128<br />
o Radiotherapy produced complete pain relief at 1 month in 395 out of 1580 (25%) patients,<br />
and at least 50% relief in 788 out of 1933 (41%) patients at some time during the trials.<br />
o In the largest trial, which included 759 patients, 52% achieved complete pain relief within<br />
4 weeks and the median duration of complete relief was 12 weeks.<br />
o The study found no difference between the use of radioisotopes (such as strontium) and<br />
EBRT <strong>for</strong> generalised disease, a finding supported by the work of Quilty et al.<br />
o In this latter study, 284 patients with <strong>prostate</strong> <strong>cancer</strong> and painful bone metastases were<br />
treated with local or hemi-body radiotherapy or strontium. Median survival was nonsignificantly<br />
different between groups (33 weeks with strontium versus 28 weeks with<br />
radiotherapy; p=0.1). 129<br />
o Both radiotherapy and strontium provided effective pain relief that was sustained <strong>for</strong><br />
3 months in 63.6% of patients after hemi-body radiotherapy compared with 66.1% of<br />
patients after strontium, and in 61% of patients after local radiotherapy compared with<br />
65.9% of patients in the comparable strontium group.<br />
o Fewer patients reported new pain sites after strontium than after local or hemi-body<br />
radiotherapy (p
Ongoing Support<br />
The <strong>MDT</strong> <strong>team</strong> should ensure regular communication with the primary care <strong>team</strong>.<br />
This may mean:<br />
• Timely provision of detailed discharge or outpatient summaries<br />
• Explanation of why a treatment route has been decided upon<br />
• The patient’s response to the chosen treatment<br />
• Sharing of protocols<br />
• Online educational resources<br />
• Agreement on prescribing policies<br />
• Provision of contact numbers <strong>for</strong> requests <strong>for</strong> in<strong>for</strong>mation<br />
The local patient support network, e.g. partner/family, must be included in the in<strong>for</strong>mation/education<br />
process through the use of:<br />
• Patient in<strong>for</strong>mation materials<br />
• Audio visual materials such as videos, DVDs and Web-based in<strong>for</strong>mation<br />
51
References<br />
1. Integrated Care Network. Integrated working: a guide. June, 2004. Available at: www.<br />
integratedcarenetwork.gov.uk/docs/publications/11/13.pdf.<br />
2. National Institute <strong>for</strong> Clinical Excellence. Guidance <strong>for</strong> commissioning <strong>cancer</strong> services. Improving<br />
outcomes in urological <strong>cancer</strong>s. The research evidence. London: NICE, 2002.<br />
3. House of Commons Committee of Public Accounts. The NHS Cancer Plan: a progress report.<br />
Twentieth report of session 2005−06. London: The Stationery Office, 2006.<br />
4. Davison BJ, Parker PA, Goldenberg SL. Patients’ preferences <strong>for</strong> communicating a <strong>prostate</strong> <strong>cancer</strong><br />
diagnosis and participating in medical decision-making. BJU Int 2004; 93: 47−51.<br />
5. Schroder FH, Hugosson Roobol MJ, et al. Screening and <strong>prostate</strong> <strong>cancer</strong> mortality in a randomized<br />
European study. N Engl J Med 2009; 360: 1320−1328.<br />
6. Andriole GL, Craw<strong>for</strong>d ED, Grubb RL 3rd, et al. Mortality results from a randomized <strong>prostate</strong><br />
<strong>cancer</strong> screening trial. N Engl J Med 2009; 360: 1310−1319.<br />
7. Rosario DJ, Lane JA, Metcalfe C, et al. Contribution of a single repeat PSA test to <strong>prostate</strong> cáncer<br />
risk assessment: experience from the ProtecT study. Eur Urol 2008; 53: 777−784.<br />
8. Ben-Shlomo Y, Evans S, Ibrahim F, et al. The risk of <strong>prostate</strong> <strong>cancer</strong> amongst black men in the<br />
United Kingdom: the PROCESS cohort study. Eur Urol 2008; 53: 99−105.<br />
9. Steinberg GD, Carter BS, Beaty TH, Childs B, Walsh PC. Family history and the risk of <strong>prostate</strong><br />
<strong>cancer</strong>. Prostate 1990; 17: 337−347.<br />
10. Negri E, Pelucchi C, Talamini R, et al. Family history of <strong>cancer</strong> and the risk of <strong>prostate</strong> <strong>cancer</strong> and<br />
benign prostatic hyperplasia. Int J Cancer 2005; 114: 648−652.<br />
11. Catalona WJ, Richie JP, DeKernion JB, et al. Comparison of <strong>prostate</strong> specific antigen concentration<br />
versus <strong>prostate</strong> specific antigen density in the early detection of <strong>prostate</strong> <strong>cancer</strong>: Receiver<br />
operating characteristic curves. J Urol 1994; 152 (6 Pt 1): 2031−2036.<br />
12. Elgamal A-AA, Cornillie FJ, Van Poppel HP, et al. Free-to-total <strong>prostate</strong> specific antigen ratio as a<br />
single test <strong>for</strong> detection of significant stage T1c <strong>prostate</strong> <strong>cancer</strong>. J Urol 1996; 156: 1042−1049.<br />
13. Aus G, Becker C, Lilja H, et al. Free-to-total <strong>prostate</strong>-specific antigen ratio as a predictor of nonorgan-confined<br />
<strong>prostate</strong> <strong>cancer</strong> (stage pT3). Scand J Urol Nephrol 2003; 37: 466−470.<br />
14. Aus G, Becker C, Franzen S, et al. Cumulative <strong>prostate</strong> <strong>cancer</strong> risk assessment with the aid of the<br />
free-to-total <strong>prostate</strong> specific antigen ratio. Eur Urol 2004; 45: 160−165.<br />
15. Hudson MA, Bahnson RR, Catalona WJ. Clinical use of <strong>prostate</strong> specific antigen in patients with<br />
<strong>prostate</strong> <strong>cancer</strong>. J Urol 1989; 142: 1011−1017.<br />
16. Brawer MK, Lange PH. Prostate-specific antigen in management of prostatic carcinoma. Urology<br />
1989; 33 (5 Suppl): 11−16.<br />
17. Partin AW, Carter HB, Chan DW, et al. Prostate specific antigen in the staging of localized <strong>prostate</strong><br />
<strong>cancer</strong>: influence of tumor differentiation, tumor volume and benign hyperplasia. J Urol 1990;<br />
143: 747−752.<br />
18. Dearnaley DP, Kirby RS, Kirk D, Malone P, Simpson RJ, Williams G. Diagnosis and management of<br />
early <strong>prostate</strong> <strong>cancer</strong>. Report of a British Association of Urological Surgeons working party. BJU Int<br />
1999; 83: 18−33.<br />
19. DeAntoni EP, Craw<strong>for</strong>d ED, Oesterling JE, et al. Age- and race-specific reference ranges <strong>for</strong><br />
<strong>prostate</strong>-specific antigen from a large community-based study. Urology 1996; 48: 234−239.<br />
20. Xu ZQ, Hua LX, Qian LX, Wu HF. Effect of transrectal prostatic biopsy on serum <strong>prostate</strong>-specific<br />
antigen levels. Zhonghua Nan Ke Xue 2002; 8: 341−342.<br />
52
21. Tchetgen MB, Oesterling JE. The effect of prostatitis, urinary retention, ejaculation and<br />
ambulation on the serum <strong>prostate</strong>-specific antigen concentration. Urol Clin North Am 1997; 24:<br />
283−291.<br />
22. Gamé X, Vincendeau S, Palascak R, Milcent S, Fournier R, Houlgatte A. Total and free <strong>prostate</strong>specific<br />
antigen levels during the first month of acute prostatitis. Eur Urol 2003; 43: 702−705.<br />
23. Catalona WJ, Partin AW, Slawin KM, et al. Use of the percentage of free <strong>prostate</strong>-specific antigen<br />
to enhance differentiation of <strong>prostate</strong> <strong>cancer</strong> from benign prostatic disease: A prospective<br />
<strong>multi</strong>center clinical trial. JAMA 1998; 279: 1542−1547.<br />
24. Smith DS, Catalona WJ. Rate of change of serum PSA levels as a method <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong><br />
detection: J Urol 1994; 152: 1163−1167.<br />
25. Gustafsson O, Norming U, Almgard LE, et al. Diagnostic methods in the detection of <strong>prostate</strong><br />
<strong>cancer</strong>: a study of a randomly selected population of 2,400 men. J Urol 1992; 148: 1827−1831.<br />
26. Mettlin C, Murphy GP, Babalan RJ, et al. The results of a five-year early <strong>prostate</strong> <strong>cancer</strong> detection<br />
intervention. Cancer 1996; 77: 150−159.<br />
27. Jones WT, Resnick MI. Prostate ultrasound in screening, diagnosis, and staging of <strong>prostate</strong> <strong>cancer</strong>.<br />
Prob Urol 1990; 4: 343−357.<br />
28. Ellis WJ, Chetner MP, Preston SD, Brawer MK. Diagnosis of prostatic carcinoma: The yield of serum<br />
<strong>prostate</strong> specific antigen, digital rectal examination and transrectal ultrasonography. J Urol 1994;<br />
152(5 I): 1520−1525.<br />
29. National Institute <strong>for</strong> Health and Clinical Excellence. Prostate <strong>cancer</strong>: diagnosis and treatment. Full<br />
guideline. London, NICE: 2008.<br />
30. Eskicorapci SY, Baydar DE, Akbal C, et al. An extended 10-core transrectal ultrasonography guided<br />
<strong>prostate</strong> biopsy protocol improves the detection of <strong>prostate</strong> <strong>cancer</strong>. Eur Urol 2004; 45: 444−448.<br />
31. Djavan B, Fong YK, Ravery V, et al. Are repeat biopsies required in men with PSA < or =4 ng/ml? A<br />
<strong>multi</strong>institutional prospective European study. Eur Urol 2005; 47: 38−44.<br />
32. Allen DJ, Hindley R, Clovis S, et al. Does body-coil magnetic-resonance imaging have a role in<br />
the preoperative staging of patients with clinically localized <strong>prostate</strong> <strong>cancer</strong>? BJU Int 2004; 94:<br />
534−538.<br />
33. Gerber G, Chodak GW. Assessment of value of routine bone scans in patients with newly<br />
diagnosed <strong>prostate</strong> <strong>cancer</strong>. Urology 1991; 37: 418−422.<br />
34. D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical <strong>prostate</strong>ctomy,<br />
external beam radiation therapy, or interstitial radiation therapy <strong>for</strong> clinically localized <strong>prostate</strong><br />
<strong>cancer</strong>. JAMA 1998; 280: 969−974.<br />
35. van As NJ, Norman AR, Thomas K, et al. Predicting the probability of deferred radical treatment<br />
<strong>for</strong> localised <strong>prostate</strong> <strong>cancer</strong> managed by active surveillance. Eur Urol 2008; 54: 1297−1305.<br />
36. van den Bergh RC, Roemeling S, Roobol MJ, et al. Outcomes of men with screen-detected <strong>prostate</strong><br />
<strong>cancer</strong> eligible <strong>for</strong> active surveillance who were managed expectantly. Eur Urol 2008; Sep 17<br />
[epub].<br />
37. Draisma G, Boer R, Otto SJ, et al. Lead times and overdetection due to <strong>prostate</strong>-specific antigen<br />
screening: estimates from the European Randomized Study of Screening <strong>for</strong> Prostate Cancer. J<br />
Natl Cancer Inst 2003; 95: 868−878.<br />
38. Selley S, Donovan J, Faulkner A, et al. Diagnosis, management and screening of early localised<br />
<strong>prostate</strong> <strong>cancer</strong>. Health Technol Assess 1997; 1: 1−96.<br />
53
39. Bill-Axelson A, Holmberg L, Ruutu M, et al. Radical <strong>prostate</strong>ctomy versus watchful waiting in early<br />
<strong>prostate</strong> <strong>cancer</strong>. N Engl J Med 2005; 352: 1977−1984.<br />
40. Singer PA, Tasch ES, Stocking C, et al. Sex or survival: trade-offs between quality and quantity of<br />
life. J Clin Oncol 1991; 9: 328−334.<br />
41. Bill-Axelson A, Holmberg L, Filen F, et al. Radical <strong>prostate</strong>ctomy versus watchful waiting in<br />
localized <strong>prostate</strong> <strong>cancer</strong>: the Scandinavian <strong>prostate</strong> <strong>cancer</strong> group-4 randomized trial. J Natl<br />
Cancer Inst 2008; 100: 1144−1154.<br />
42. Bonney WW, Schned AR, Timberlake DS. Neoadjuvant androgen ablation <strong>for</strong> localised prostatic<br />
<strong>cancer</strong>. Pathology methods, surgical end points and meta-analysis of randomised trials. J Urol<br />
1999; 160: 1754−1760.<br />
43. Paul R, Van Randenborgh H, Kubler H, et al. Significance of neoadjuvant therapy be<strong>for</strong>e radical<br />
<strong>prostate</strong>ctomy. Urologe A 2004; 43: 680−688.<br />
44. Selli C, Milesi C. Neoadjuvant androgen deprivation be<strong>for</strong>e radical <strong>prostate</strong>ctomy. A review.<br />
Minerva Urol Nefrol 2004; 56: 165−171.<br />
45. Witjes WPJ, Schulman CC, Debruyne FMJ. Preliminary results of a prospective randomised study<br />
comparing radical <strong>prostate</strong>ctomy versus radical <strong>prostate</strong>ctomy associated with neo-adjuvant<br />
hormonal combination therapy in T2-3 N0 M0 prostatic carcinoma. Urology 1997; 49 (3 Suppl):<br />
65−69.<br />
46. Hachiya T, Minei S, Hirano D, et al. Adjuvant hormone therapy in patients with positive surgical<br />
margins after radical <strong>prostate</strong>ctomy. Jpn J Urol 2002; 93: 469−475.<br />
47. Prayer-Galetti T, et al. Disease free survival in patients with pathological “C Stage” <strong>prostate</strong> <strong>cancer</strong><br />
at radical <strong>prostate</strong>ctomy submitted to adjuvant hormonal treatment. Eur Urol 2000; 38: 504, abs<br />
48.<br />
48. Bolla M, van Poppel H, Collette L, et al. Postoperative radiotherapy after radical <strong>prostate</strong>ctomy: a<br />
randomised controlled trial (EORTC trial 22911). Lancet 2005; 366: 572−578.<br />
49. Thompson Jr IM, Tangen CM, Paradelo J, et al. Adjuvant radiotherapy <strong>for</strong> pathologically advanced<br />
<strong>prostate</strong> <strong>cancer</strong>: a randomized clinical trial. JAMA 2006; 296: 2329−2335.<br />
50. Parker C, Sydes MR, Catton C, et al. Radiotherapy and androgen deprivation in combination after<br />
local surgery (RADICALS): A new Medical Research Council/National Cancer Institute of Canada<br />
phase III trial of adjuvant treatment after radical <strong>prostate</strong>ctomy. BJU Int 2007; 99: 1376−1379.<br />
51. Nilsson S, Norlen BJ, Widmark A. A systematic overview of radiation therapy effects in <strong>prostate</strong><br />
<strong>cancer</strong>. Acta Oncol 2004; 43: 316−381.<br />
52. Dearnaley DP, Khoo VS, Norman AR, et al. Comparison of radiation side-effects of con<strong>for</strong>mal and<br />
conventional radiotherapy in <strong>prostate</strong> <strong>cancer</strong>: a randomised trial. Lancet 1999; 353: 267−272.<br />
53. Pollack A, Zagars GK, Starkschall G, et al. Prostate <strong>cancer</strong> radiation dose response: results of the M.<br />
D. Anderson phase III randomized trial. Int J Radiat Oncol Biol Phys 2002; 53: 1097−1105.<br />
54. Dearnaley DP, Sydes MR, Graham JD, et al. Escalated-dose versus standard-dose con<strong>for</strong>mal<br />
radiotherapy in <strong>prostate</strong> <strong>cancer</strong>: first results from the MRC RT01 randomised controlled trial.<br />
Lancet Oncol 2007; 8: 475−487.<br />
55. Zelefsky MJ, Fuks Z, Lee HJ, et al. High dose radiation delivered by intensity modulated con<strong>for</strong>mal<br />
radiotherapy improves the outcome of localized <strong>prostate</strong> <strong>cancer</strong>. J Urol 2001; 166: 876−878.<br />
56. Zelefsky MJ, Fuks Z, Hunt M, et al. High-dose intensity modulated radiation therapy <strong>for</strong> <strong>prostate</strong><br />
<strong>cancer</strong>: early toxicity and biochemical outcome in 772 patients. Int J Radiat Oncol Biol Phys 2002;<br />
52: 1111−1116.<br />
54
57. Amer AM, Mott J, Mackay RI, et al. Prediction of the benefits from dose-escalated<br />
hypofractionated intensity-modulated radiotherapy <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong>. Int J Radiat Oncol Biol<br />
Phys 2003; 56: 199−207.<br />
58. South CP, Khoo VS, Naismith O, Norman A, Dearnaley DP. A comparison of treatment planning<br />
techniques used in two randomised UK external beam radiotherapy trials <strong>for</strong> localised <strong>prostate</strong><br />
<strong>cancer</strong>. Clin Oncol (R Coll Radiol) 2008; 20: 15−21.<br />
59. Shearer RJ, Davies JH, Gelister JS, Dearnaley DP. Hormonal cytoreduction and radiotherapy <strong>for</strong><br />
carcinoma of the <strong>prostate</strong>. Br J Urol 1992; 69: 521−524.<br />
60. Forman JD, Kumar R, Haas G, et al. Neoadjuvant hormonal downsizing of localized carcinoma of<br />
the <strong>prostate</strong>: effects on the volume of normal tissue irradiation. Cancer Invest 1995; 13: 8−15.<br />
61. Hara I, Miyake H, Yamada Y. Neoadjuvant androgen withdrawal prior to external radiotherapy <strong>for</strong><br />
locally advanced adenocarcinoma of the <strong>prostate</strong>. Int J Urol 2002; 9: 322−332.<br />
62. Pilepich MV, Winter K, John MJ, et al. Phase III RTOG trial 86-10 of androgen deprivation adjuvant<br />
to definitive radiotherapy in locally advanced carcinoma of the <strong>prostate</strong>. Int J Radiat Oncol Biol<br />
Phys 2001; 50: 1243−1252.<br />
63. Roach M 3rd, Bae K, Speight J, et al. Short-term neoadjuvant androgen deprivation therapy and<br />
external-beam radiotherapy <strong>for</strong> locally advanced <strong>prostate</strong> <strong>cancer</strong>: long-term results of RTOG 8610.<br />
J Clin Oncol 2008; 26: 585−591.<br />
64. Denham JW, Steigler A, Wilcox C, et al. Time to biochemical failure and <strong>prostate</strong>-specific antigen<br />
doubling time as surrogates <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong>-specific mortality: evidence from the TROG 96.01<br />
randomised controlled trial. Lancet Oncol 2008; 9: 1058−1068.<br />
65. D’Amico AV, Manola J, Loffredo M, Renshaw AA, DellaCroce A, Kantoff PW. 6-month androgen<br />
suppression plus radiation therapy vs radiation therapy alone <strong>for</strong> patients with clinically localized<br />
<strong>prostate</strong> <strong>cancer</strong>: a randomized controlled trial. JAMA 2004; 292: 821−827.<br />
66. National Institute <strong>for</strong> Health and Clinical Excellence. Low dose rate brachytherapy <strong>for</strong> localised<br />
<strong>prostate</strong> <strong>cancer</strong>. Interventional Procedure Guidance 132, July 2005.<br />
67. Crook J, Lukka H, Klotz L, et al. Systematic overview of the evidence <strong>for</strong> brachytherapy in clinically<br />
localised <strong>prostate</strong> <strong>cancer</strong>. CMAJ 2001; 164: 975−981.<br />
68. Merrick GS, Butler WM, Lief JH, Dorsey AT. Is brachytherapy comparable with radical<br />
<strong>prostate</strong>ctomy and external beam radiotherapy <strong>for</strong> clinically localised <strong>prostate</strong> <strong>cancer</strong>? Tech Urol<br />
2001; 7: 12−19.<br />
69. Singh AM, Gagnon G, Collins B, et al. Combined external beam radiotherapy and Pd-103<br />
brachytherapy boost improves biochemical failure free survival in patients with clinically localized<br />
<strong>prostate</strong> <strong>cancer</strong>: results of a matched pair analysis. Prostate 2005; 62: 54−60.<br />
70. Potters L, Morgenstern C, Calugaru E, et al. 12-year outcomes following permanent <strong>prostate</strong><br />
brachytherapy in patients with clinically localized <strong>prostate</strong> <strong>cancer</strong>. J Urol 2005; 173: 1562−1566.<br />
71. Wills F, Hailey D. Brachytherapy <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong>. Alberta Heritage Foundation <strong>for</strong> Medical<br />
Research, Alberta Canada. 1999, Dec. (http://www.ahfmr.ab.ca/publications).<br />
72. Beyer DC, Priestley JB Jr. Biochemical disease-free survival following 125I <strong>prostate</strong> implantation.<br />
Int J Radiat Oncol Biol Phys 1997; 37: 559−563.<br />
73. Blasko JC, Wallner K, Grimm PD, Ragde H. Prostate specific antigen based disease control<br />
following ultrasound guided 125iodine implantation <strong>for</strong> stage T1/T2 prostatic carcinoma. J Urol<br />
1995; 154: 1096−1099.<br />
74. Wallner K, Roy J, Zelefsky M, Harrison L. Short-term freedom from disease progression after I-125<br />
<strong>prostate</strong> implantation. Int J Radiat Oncol Biol Phys 1994; 30: 405−409.<br />
55
75. Stock RG, Stone NN, DeWyngaert JK, Lavagnini P, Unger PD. Prostate specific antigen findings and<br />
biopsy results following interactive ultrasound guided transperineal brachytherapy <strong>for</strong> early stage<br />
<strong>prostate</strong> carcinoma. Cancer 1996; 77: 2386−2392.<br />
76. Beyer DC, Brachman DG. Failure free survival following brachytherapy alone <strong>for</strong> <strong>prostate</strong> <strong>cancer</strong>:<br />
comparison with external beam radiotherapy. Radiother Oncol 2000; 57: 263−267.<br />
77. Ragde H, Korb LJ, Elgamal A-A, et al. Modern <strong>prostate</strong> brachytherapy. PSA results in 219 patients<br />
with up to 12 years of observational follow up. Cancer 2000; 89: 135−141.<br />
78. Kupelian PA, Potters L, Khuntia D, et al. Radical <strong>prostate</strong>ctomy, external beam radiotherapy or =72 Gy, permanent seed implantation, or combined seeds/<br />
external beam radiotherapy <strong>for</strong> stage T1-T2 <strong>prostate</strong> <strong>cancer</strong>. Int J Radiat Oncol Biol Phys 2004; 58:<br />
25−33.<br />
79. Han KR, Cohen JK, Miller RJ, et al. Treatment of organ confined <strong>prostate</strong> <strong>cancer</strong> with third<br />
generation cryosurgery: preliminary <strong>multi</strong>center experience. J Urol 2003; 170 (4 Pt 1): 1126−1130.<br />
80. Zisman A, Pantuck AJ, Cohen JK, Belldegrun AS. Prostate cryoablation using direct transperineal<br />
placement of ultrathin probes through a 17-gauge brachytherapy template-technique and<br />
preliminary results. Urology 2001; 58: 988−993.<br />
81. Parker MC, Cook A, Riddle PR, et al. Is delayed treatment justified in carcinoma of the <strong>prostate</strong>? Br<br />
J Urol 1985; 57: 724−728.<br />
82. Rana A, Chisholm GD, Khan M, et al. Conservative management with symptomatic treatment<br />
and delayed hormonal manipulation is justified in men with locally advanced carcinoma of the<br />
<strong>prostate</strong>. Br J Urol 1994; 74: 637−641.<br />
83. Wilt T, Nair B, MacDonald R, Rutks I. Early versus deferred androgen suppression in the treatment<br />
of advanced prostatic <strong>cancer</strong>. Cochrane Database Syst Rev 2001; CD003506.<br />
84. Adolfsson J, Steineck G, Hedlund PO. Deferred treatment of locally advanced nonmetastatic<br />
<strong>prostate</strong> <strong>cancer</strong>: a long-term followup. J Urol 1999; 161: 505−508.<br />
85. MRC Prostate Working Party Investigators Group. Immediate versus deferred treatment <strong>for</strong><br />
advanced <strong>prostate</strong> <strong>cancer</strong>. Initial results of the MRC trial. Br J Urol 1997; 79: 235−246.<br />
86. Studer UE, Whelan P, Albrecht W, et al. Immediate or deferred androgen deprivation <strong>for</strong> patients<br />
with <strong>prostate</strong> <strong>cancer</strong> not suitable <strong>for</strong> local treatment with curative intent: European Organisation<br />
<strong>for</strong> Research and Treatment of Cancer (EORTC) Trial 30891. J Clin Oncol 2006; 24: 1868−1876.<br />
87. McLeod DG, Iversen P, See WA, et al. Bicalutamide 150 mg plus standard care versus standard care<br />
alone <strong>for</strong> early <strong>prostate</strong> <strong>cancer</strong>. BJU Int 2006; 97: 247−254.<br />
88. Widmark A, Klepp O, Solberg A, et al. Endocrine treatment, with or without radiotherapy, in<br />
locally advanced <strong>prostate</strong> <strong>cancer</strong> (SPCG-7/SFUO-3): an open randomised phase III trial. Lancet 2009;<br />
373: 301−308.<br />
89. Lawton CA, DeSilvio M, Roach M 3rd, et al. An update of the phase III trial comparing whole pelvic<br />
to <strong>prostate</strong> only radiotherapy and neoadjuvant to adjuvant total androgen suppression: updated<br />
analysis of RTOG 94-13, with emphasis on unexpected hormone/radiation interactions. Int J Radiat<br />
Oncol Biol Phys 2007; 69: 646−655.<br />
90. Martinez AA, Gustafson G, Gonzalez J, et al. Dose escalation using con<strong>for</strong>mal high dose rate<br />
brachytherapy improves outcome in unfavorable <strong>prostate</strong> <strong>cancer</strong>. Int J Radiat Oncol Biol Phys<br />
2002; 53: 316−327.<br />
91. Bolla M, Collette L, Blank L, et al. Long-term results with immediate androgen suppression and<br />
external irradiation in patients with locally advanced <strong>prostate</strong> <strong>cancer</strong> (an EORTC study): a phase III<br />
randomised trial. Lancet 2002; 360: 103−106.<br />
56
92. Bolla M, Collette L, Van Tienhoven G, et al. Ten year results of long term adjuvant androgen<br />
deprivation with goserelin in patients with locally advanced <strong>prostate</strong> <strong>cancer</strong> treated with<br />
radiotherapy: A phase III EORTC study. Int J Radiat Oncol Biol Phys 2008; 72 (1 Suppl1): S30−S31.<br />
93. Bolla M, de Reijke TM, Van Tienhoven G, et al. Duration of androgen suppression in the treatment<br />
of <strong>prostate</strong> <strong>cancer</strong>. N Engl J Med 2009; 360: 2516−2527.<br />
94. Pilepich MV, Winter K, Lawton CA, et al. Androgen suppression adjuvant to definitive<br />
radiotherapy in <strong>prostate</strong> carcinoma − long-term results of phase III RTOG 85-31. Int J Radiat Oncol<br />
Biol Phys 2005; 61: 1285−1290.<br />
95. Hanks GE, Pajak TF, Porter A, et al. Phase III trial of long-term adjuvant androgen deprivation<br />
after neoadjuvant hormonal cytoreduction and radiotherapy in locally advanced carcinoma of the<br />
<strong>prostate</strong>: the Radiation Therapy Oncology Group Protocol 92-02. J Clin Oncol 2003; 21: 3972−3978.<br />
96. Horwitz EM, Bae K, Hanks GE, et al. Ten-year follow-up of radiation therapy oncology group<br />
protocol 92-02: a phase III trial of the duration of elective androgen deprivation in locally<br />
advanced <strong>prostate</strong> <strong>cancer</strong>. J Clin Oncol 2008; 26: 2497−2504.<br />
97. Roach M, Hanks G, Thames H, et al. Defining biochemical failure following radiotherapy with or<br />
without hormonal therapy in men with clinically localized <strong>prostate</strong> <strong>cancer</strong>: recommendations of<br />
the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys 2006; 65: 965−974.<br />
98. Pound CR, Partin AW, Eisenberger MA, et al. Natural history of progression after PSA elevation<br />
following radical <strong>prostate</strong>ctomy. JAMA 1999; 281: 1591−1597.<br />
99. Messing EM, Manola J, Yao J, et al. Immediate versus deferred androgen deprivation<br />
treatment in patients with node-positive <strong>prostate</strong> <strong>cancer</strong> after radical <strong>prostate</strong>ctomy and pelvic<br />
lymphadenectomy. Lancet Oncol 2006; 7: 472−479.<br />
100. Touma NJ, Izawa JI, Chin JL. Current status of local salvage therapies following radiation failure<br />
<strong>for</strong> <strong>prostate</strong> <strong>cancer</strong>. J Urol 2005; 173: 373−379.<br />
101. Grado GL, Collins JM, Kriegshauser, JS et al. Salvage brachytherapy <strong>for</strong> localized <strong>prostate</strong> <strong>cancer</strong><br />
after radiotherapy failure. Urology 1999; 53: 2−10.<br />
102. Gelet A, Chapelon JY, Poissonier L, et al. Local recurrence of <strong>prostate</strong> <strong>cancer</strong> after external beam<br />
radiotherapy: early experience of salvage therapy using high-intensity focused ultrasonography.<br />
Urology 2004; 63: 625−629.<br />
103. Tombal B. The importance of testosterone control in <strong>prostate</strong> <strong>cancer</strong>. Eur Urol Suppl 2007; 6:<br />
834−839.<br />
104. Vogelzang NJ, Chodak GW, Soloway MS, et al. Goserelin versus orchiectomy in the treatment<br />
of advanced <strong>prostate</strong> <strong>cancer</strong>: final results of a randomized trial. Zoladex Prostate Study Group.<br />
Urology 1995; 46: 220−226.<br />
105. Kaisary AV, Tyrrell CJ, Peeling WB, Griffiths K. Comparison of LHRH analogue (Zoladex) with<br />
orchiectomy in patients with metastatic prostatic carcinoma. Br J Urol 1991; 67: 502−508.<br />
106. Seidenfeld J, Samson DJ, Hasselblad V, et al. Single-therapy androgen suppression in men with<br />
advanced <strong>prostate</strong> <strong>cancer</strong>: a systematic review and meta-analysis. Ann Intern Med 2000; 132:<br />
566−577.<br />
107. Shahinian VB, Kuo YF, Freeman JL, Orihuela E, Goodwin JS. Increasing use of gonadotropinreleasing<br />
hormone agonists <strong>for</strong> the treatment of localized <strong>prostate</strong> carcinoma. Cancer 2005; 103:<br />
1615−2164.<br />
108. Kaku H, Saika T, Tsushima T, et al. Time course of serum testosterone and luteinizing hormone<br />
levels after cessation of long-term luteinizing hormone-releasing hormone agonist treatment in<br />
patients with <strong>prostate</strong> <strong>cancer</strong>. Prostate 2006; 66: 439−444.<br />
57
109. Cassileth BR, Soloway MS, Vogelzang NJ, et al. Quality of life and psychosocial status in stage D<br />
<strong>prostate</strong> <strong>cancer</strong>. Zoladex Prostate Cancer Study Group. Qual Life Res 1992; 1: 323−330.<br />
110. Klotz L, Boccon-Gibod L, Shore ND, et al. The efficacy and safety of degarelix: a 12-month<br />
comparative, randomized, open-label, parallel-group phase III study in patients with <strong>prostate</strong><br />
<strong>cancer</strong>. BJU Int 2008; 102: 1531−1538.<br />
111. Prostate Cancer Trialists’ Collaborative Group. Maximum androgen blockade in advanced <strong>prostate</strong><br />
<strong>cancer</strong>: an overview of the randomised trials. Lancet 2000; 355: 1491−1498.<br />
112. Klotz L. Combined androgen blockade in <strong>prostate</strong> <strong>cancer</strong>: Meta-analyses and associated issues.<br />
BJU Int 2001; 87: 806−813.<br />
113. Sartor AO, Tangen CM, Hussain MH, et al. Antiandrogen withdrawal in castrate-refractory<br />
<strong>prostate</strong> <strong>cancer</strong>: a Southwest Oncology Group trial (SWOG 9426). Cancer 2008; 112: 2393−2400.<br />
114. Byar DP. Treatment of prostatic <strong>cancer</strong>: studies by the Veterans Administration Cooperative<br />
Urological Research Group. Bull N Y Acad Med 1972; 48: 751−766.<br />
115. Robinson MR, Smith PH, Richards B, et al. The final analysis of the EORTC Genito-Urinary Tract<br />
Cancer Co-Operative Group phase III clinical trial (protocol 30805) comparing orchidectomy,<br />
orchidectomy plus cyproterone acetate and low dose stilboestrol in the management of<br />
metastatic carcinoma of the <strong>prostate</strong>. Eur Urol 1995; 28: 273−283.<br />
116. Tannock IF, Osoba D, Stockler MR, et al. Chemotherapy with mitoxantrone plus prednisone or<br />
prednisone alone <strong>for</strong> symptomatic hormone-resistant <strong>prostate</strong> <strong>cancer</strong>: a Canadian randomized<br />
trial with palliative end points. J Clin Oncol 1996; 14: 1756−1764.<br />
117. Small EJ, Halabi S, Dawson NA, et al. Antiandrogen withdrawal alone or in combination with<br />
ketoconazole in androgen-independent <strong>prostate</strong> <strong>cancer</strong> patients: a phase III trial (CALGB 9583).<br />
J Clin Oncol 2004; 22: 1025−1033.<br />
118. Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone<br />
<strong>for</strong> advanced <strong>prostate</strong> <strong>cancer</strong>. N Engl J Med 2004; 351: 1502−1512.<br />
119. Berthold DR, Pond GR, Soban F, de Wit R, Eisenberger M, Tannock I. Docetaxel plus prednisone<br />
or mitoxantrone plus prednisone <strong>for</strong> advanced <strong>prostate</strong> <strong>cancer</strong>: updated survival in the TAX 327<br />
study. J Clin Oncol 2008; 26: 242−245.<br />
120. Porter AT, McEwan AJ, Powe JE, et al. Results of a randomised phase III trial to evaluate the<br />
efficacy of strontium-89 adjuvant to local field EB-RT in the management of endocrine resistant<br />
metastatic <strong>prostate</strong> <strong>cancer</strong>. Int J Radiat Oncol Biol Phys 1993; 25: 805−813.<br />
121. Brundage MD, Crook JM, Lukka H, et al. Use of strontium-89 in endocrine refractory <strong>prostate</strong><br />
<strong>cancer</strong> metastatic to bone. Provincial genitourinary <strong>cancer</strong> disease group. Cancer Prev Control<br />
1998; 2: 79−87.<br />
122. Robinson RG, Preston DF, Schiefelbein M, Baxter KG. Strontium–89 therapy <strong>for</strong> the palliation of<br />
pain due to osseous metastases. JAMA 1995; 274: 420−424.<br />
123. Tu SM, Millikan RE, Mengistu B, et al. bone targeted therapy <strong>for</strong> advanced and androgen<br />
independent <strong>prostate</strong> <strong>cancer</strong>. A randomised phase II trial. Lancet 2001; 357: 336−341.<br />
124. Saad F, Gleason DM, Murray R, et al. A randomized, placebo-controlled trial of zoledronic acid<br />
in patients with hormone-refractory metastatic <strong>prostate</strong> carcinoma. J Natl Cancer Inst 2002; 94:<br />
1458−1468.<br />
125. Dearnaley DP, Mason MD, Parmar MK, Sanders K, Sydes MR. Adjuvant therapy with oral sodium<br />
clodronate in locally advanced and metastatic <strong>prostate</strong> <strong>cancer</strong>: long-term overall survival results<br />
from the MRC PR04 and PR05 randomised controlled trials. Lancet Oncol 2009; 10: 872−876.<br />
58
126. Marx RE, Sawatari Y, Fortin M, Broumand V. Bisphosphonate-induced exposed bone<br />
(osteonecrosis/osteopetrosis) of the jaws: risk factors, recognition, prevention and treatment.<br />
J Oral Maxillofac Surg 2005; 63: 1567−1575.<br />
127. Zometa (zoledronic acid). Summary of product characteristics, July 2008.<br />
128. McQuay HJ, Carroll D, Moore RA. Radiotherapy <strong>for</strong> painful bone metastases. A systematic review.<br />
Clin Oncol 1997; 9: 150−154.<br />
129. Quilty PM, Kirk D, Bolger JJ, et al. A comparison of the palliative effects of strontium-89 and<br />
external beam radiotherapy in metastatic <strong>prostate</strong> <strong>cancer</strong>. Radiother Oncol 1994; 31: 33−40.<br />
59