

Assessing the impact of PRSPs on Child Poverty: The Case of Bolivia
Assessing the impact of PRSPs on Child Poverty: The Case of Bolivia
Assessing the impact of PRSPs on Child Poverty: The Case of Bolivia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
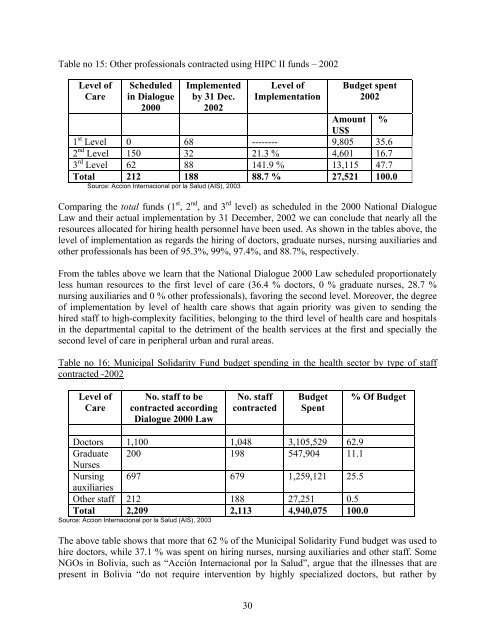
Table no 15: O<str<strong>on</strong>g>the</str<strong>on</strong>g>r pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>als c<strong>on</strong>tracted using HIPC II funds – 2002<br />
Level <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
Care<br />
Scheduled<br />
in Dialogue<br />
2000<br />
Implemented<br />
by 31 Dec.<br />
2002<br />
30<br />
Level <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
Implementati<strong>on</strong><br />
Budget spent<br />
2002<br />
Amount<br />
US$<br />
%<br />
1 st Level 0 68 -------- 9,805 35.6<br />
2 nd Level 150 32 21.3 % 4,601 16.7<br />
3 rd Level 62 88 141.9 % 13,115 47.7<br />
Total 212 188 88.7 % 27,521 100.0<br />
Source: Acci<strong>on</strong> Internaci<strong>on</strong>al por la Salud (AIS), 2003<br />
Comparing <str<strong>on</strong>g>the</str<strong>on</strong>g> total funds (1 st , 2 nd , and 3 rd level) as scheduled in <str<strong>on</strong>g>the</str<strong>on</strong>g> 2000 Nati<strong>on</strong>al Dialogue<br />
Law and <str<strong>on</strong>g>the</str<strong>on</strong>g>ir actual implementati<strong>on</strong> by 31 December, 2002 we can c<strong>on</strong>clude that nearly all <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
resources allocated for hiring health pers<strong>on</strong>nel have been used. As shown in <str<strong>on</strong>g>the</str<strong>on</strong>g> tables above, <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
level <str<strong>on</strong>g>of</str<strong>on</strong>g> implementati<strong>on</strong> as regards <str<strong>on</strong>g>the</str<strong>on</strong>g> hiring <str<strong>on</strong>g>of</str<strong>on</strong>g> doctors, graduate nurses, nursing auxiliaries and<br />
o<str<strong>on</strong>g>the</str<strong>on</strong>g>r pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>als has been <str<strong>on</strong>g>of</str<strong>on</strong>g> 95.3%, 99%, 97.4%, and 88.7%, respectively.<br />
From <str<strong>on</strong>g>the</str<strong>on</strong>g> tables above we learn that <str<strong>on</strong>g>the</str<strong>on</strong>g> Nati<strong>on</strong>al Dialogue 2000 Law scheduled proporti<strong>on</strong>ately<br />
less human resources to <str<strong>on</strong>g>the</str<strong>on</strong>g> first level <str<strong>on</strong>g>of</str<strong>on</strong>g> care (36.4 % doctors, 0 % graduate nurses, 28.7 %<br />
nursing auxiliaries and 0 % o<str<strong>on</strong>g>the</str<strong>on</strong>g>r pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essi<strong>on</strong>als), favoring <str<strong>on</strong>g>the</str<strong>on</strong>g> sec<strong>on</strong>d level. Moreover, <str<strong>on</strong>g>the</str<strong>on</strong>g> degree<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> implementati<strong>on</strong> by level <str<strong>on</strong>g>of</str<strong>on</strong>g> health care shows that again priority was given to sending <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
hired staff to high-complexity facilities, bel<strong>on</strong>ging to <str<strong>on</strong>g>the</str<strong>on</strong>g> third level <str<strong>on</strong>g>of</str<strong>on</strong>g> health care and hospitals<br />
in <str<strong>on</strong>g>the</str<strong>on</strong>g> departmental capital to <str<strong>on</strong>g>the</str<strong>on</strong>g> detriment <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> health services at <str<strong>on</strong>g>the</str<strong>on</strong>g> first and specially <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
sec<strong>on</strong>d level <str<strong>on</strong>g>of</str<strong>on</strong>g> care in peripheral urban and rural areas.<br />
Table no 16: Municipal Solidarity Fund budget spending in <str<strong>on</strong>g>the</str<strong>on</strong>g> health sector by type <str<strong>on</strong>g>of</str<strong>on</strong>g> staff<br />
c<strong>on</strong>tracted -2002<br />
Level <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
Care<br />
No. staff to be<br />
c<strong>on</strong>tracted according<br />
Dialogue 2000 Law<br />
No. staff<br />
c<strong>on</strong>tracted<br />
Budget<br />
Spent<br />
Doctors 1,100 1,048 3,105,529 62.9<br />
Graduate<br />
Nurses<br />
200 198 547,904 11.1<br />
Nursing<br />
auxiliaries<br />
697 679 1,259,121 25.5<br />
O<str<strong>on</strong>g>the</str<strong>on</strong>g>r staff 212 188 27,251 0.5<br />
Total 2,209 2,113 4,940,075 100.0<br />
Source: Acci<strong>on</strong> Internaci<strong>on</strong>al por la Salud (AIS), 2003<br />
% Of Budget<br />
<strong>The</strong> above table shows that more that 62 % <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> Municipal Solidarity Fund budget was used to<br />
hire doctors, while 37.1 % was spent <strong>on</strong> hiring nurses, nursing auxiliaries and o<str<strong>on</strong>g>the</str<strong>on</strong>g>r staff. Some<br />
NGOs in <strong>Bolivia</strong>, such as “Acción Internaci<strong>on</strong>al por la Salud”, argue that <str<strong>on</strong>g>the</str<strong>on</strong>g> illnesses that are<br />
present in <strong>Bolivia</strong> “do not require interventi<strong>on</strong> by highly specialized doctors, but ra<str<strong>on</strong>g>the</str<strong>on</strong>g>r by
