insanity.pdf
insanity.pdf
insanity.pdf

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
8 INSANITY AND DIMINISHED CAPACITY<br />
BEFORE THE COURT<br />
Adelene Africa<br />
After reading this chapter you should be able to<br />
∗ Distinguish between ‘<strong>insanity</strong>’ and ‘mental disorder’<br />
∗ Understand the legal test for criminal responsibility<br />
∗ Distinguish between pathological and non-pathological criminal incapacity<br />
* Understand the role which psychological knowledge plays in determining mental state<br />
* Be familiar with the controversies surrounding expert psychological testimony in cases of<br />
criminal responsibility<br />
Importance of this chapter<br />
Mental illness is one of several factors recognised by South African law as<br />
negating criminal responsibility. Statutory provision in the form of the<br />
<strong>insanity</strong> defence has been made for people who suffer from mental illness, and<br />
they cannot be held responsible for their actions. Consequently, the law<br />
acknowledges that mentally ill offenders cannot be sanctioned in the same<br />
way as sane offenders (Snyman, 2002). Thus, where mental illness and<br />
criminal responsibility are concerned, the law is clear as to the legal test which<br />
has to be applied, the nature of expert testimony which has to be adduced, and<br />
the disposition of such offenders. Psychologists (and psychiatrists) 1 play an<br />
important role in assisting the court with expert testimony regarding the<br />
mental state of the offender. In some instances, this role may be problematic<br />
because the nature of psychological evidence adduced in cases concerned with<br />
questions of ‘sanity’ can be contentious.<br />
Developments in the last twenty years have resulted in judicial recognition<br />
of the role of psychological factors, other than mental illness, in the negation<br />
of criminal responsibility. This recognition is typically expressed in the<br />
defence of non-pathological criminal incapacity and encompasses the idea that<br />
transient mental states are grounds for exculpation. The acceptance of this<br />
defence into South African law widened the scope of expert psychological and<br />
psychiatric testimony to include psychological evidence.<br />
Lawyers and mental health professionals often cross swords in cases where<br />
a defence of non-pathological criminal incapacity is mounted., The differences<br />
in interpretation and application have sparked controversy both within and<br />
between these professions. For example, mental health professionals differ in<br />
the way that they construe the defence, resulting in a myriad of diagnostic<br />
categories which are ostensibly ‘temporary mental conditions’ (Gillmer,<br />
1996). The defence has received much attention from legal commentators,<br />
1 A Psychologist has a Masters degree in Psychology . For the purposes of this chapter,<br />
the term will refer to those practitioners who have postgraduate training in Clinical<br />
Psychology. A Psychiatrist is a medical doctor who has specialised in Psychiatry.
Insanity and diminished capacity 2<br />
who have focussed largely on its form and content, as well as the factors<br />
which the courts have taken into account in passing judgement. These<br />
discussions have also focussed on the content of expert psychological<br />
testimony in cases where it has been adduced, specifically in relation to<br />
reasons why courts have either accepted or rejected such testimony (Snyman,<br />
1989; 1991; 1995; Rumpff, 1990; Burchell, 1995; Boister, 1996).<br />
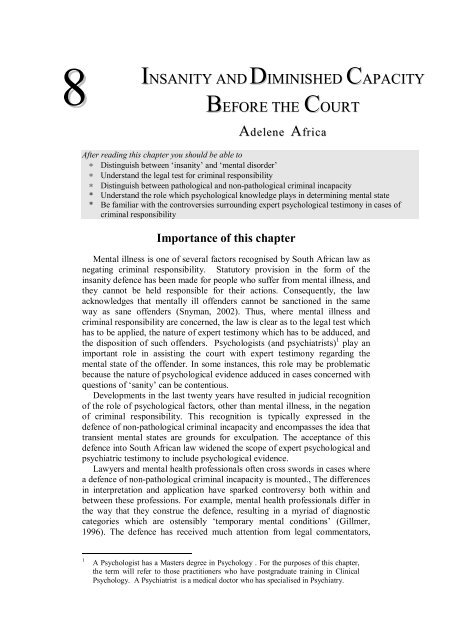
This chapter explores the role which psychological knowledge plays in<br />
assisting the court in determining criminal responsibility where the accused’s<br />
mental state is in question. In order to achieve this aim, the chapter provides<br />
an overview of the statutory provisions for defences which negate criminal<br />
responsibility. These include the <strong>insanity</strong> defence, the defence of diminished<br />
responsibility, and the defence of non-pathological incapacity. This provides a<br />
platform to explore some of the difficulties which arise when psychological<br />
conceptions of mental illness (or disorder) intersect with legal notions of<br />
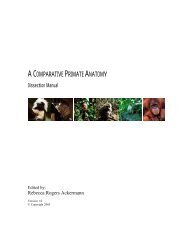
<strong>insanity</strong>. Figure 8.1 provides a flowchart summary that the reader may wish to<br />
refer to during the course of the chapter.<br />
Yes<br />
Was X able to act in accordance with an<br />
appreciation of wrongfulness?<br />
Yes<br />
Trial proceeds<br />
Verdict: Guilty<br />
or not guilty<br />
Disposition:<br />
Imprisonment<br />
X is charged with an offence<br />
Did X appreciate the wrongfulness of the act?<br />
No<br />
What was X’s mental state at the time of the<br />
offence?<br />
Pathological condition? Non-pathological condition?<br />
Mental<br />
disorder<br />
Mental defect Temporary<br />
emotional<br />
states<br />
Verdict: Not<br />
guilty by<br />
reason of<br />
mental illness<br />
Disposition:<br />
Indefinite<br />
hospitalisation<br />
Verdict: Not<br />
guilty<br />
Figure 8.1 Flowchart of the possible routes through the criminal justice<br />
system when criminal responsibility is at stake<br />
Free
Africa 3<br />
Insanity is a<br />
legally defined<br />
state of mind and<br />
does not refer to<br />
a mental<br />
disorder<br />
Mental illness<br />
refers to a<br />
behavioural or<br />
psychological<br />
pattern which<br />
causes personal<br />
distress and<br />
impairment<br />
The Insanity Defence (Pathological Criminal Incapacity)<br />
The term ‘<strong>insanity</strong>’ refers to a legally defined state of mind and does not<br />
refer to a particular psychological disorder or state. In fact, as will be shown,<br />
legal conceptions of <strong>insanity</strong> may be far removed from psychiatric or<br />
psychological conceptions of mental illness.<br />
Fitness to stand trial<br />
In terms of criminal procedure, every person is presumed to be sane until<br />
the contrary is proven. However in the case of mental illness or defect, when<br />
an accused’s capacity to follow court proceedings is compromised, he or she<br />
cannot be tried in a court of law. Section 77 of the Criminal Procedure Act 51<br />
of 1977 (CPA) therefore makes provision for an inquiry and report on the<br />
accused’s fitness to stand trial. Further statutory provision is made for expert<br />
testimony to establish the presence of mental illness or defect and the extent to<br />
which it impacts on the accused’s ability to follow proceedings. Where the<br />
offence has been violent, as in the case of murder, rape or culpable homicide,<br />
Section 79 of the CPA provides for the inquiry to be conducted by a panel of<br />
psychiatrists at a psychiatric hospital. Psychiatric evidence regarding the<br />
presence of mental illness and its impact on the capacity of the accused to<br />
understand proceedings is contained within the report presented to the court.<br />
However, the court may also require psychological evidence - for example,<br />
evidence pertaining to the accused person’s level of intellectual functioning.<br />
This inquiry is conducted and reported on by a psychologist 2 . If the findings of<br />
the psychiatrists and psychologist conclude that the accused is not fit to stand<br />
trial, he or she will be admitted to a state psychiatric hospital for an indefinite<br />
period of time.<br />
Where fitness to stand trial is concerned, the<br />
psychologist may play a role at the court’s request.<br />
Psychological knowledge regarding factors such as<br />
intellectual functioning, personality functioning and<br />
emotional functioning may therefore be admitted as<br />
testimony so that the court is put in a position to make a<br />
finding regarding the accused person’s capacity to<br />
follow proceedings.<br />
The impact which the accused person’s mental state has on his or her<br />
functioning is relevant to both the capacity to understand and to follow court<br />
proceedings, as well as his or her criminal responsibility. However, as will see,<br />
an inquiry into an accused’s fitness to stand trial has no bearing on the inquiry<br />
into his or her responsibility.<br />
The Legal Test for Insanity in South Africa<br />
When the <strong>insanity</strong> defence is raised, the court is concerned as to whether<br />
the accused can be held criminally responsible in light of the purported mental<br />
2 In terms of Section 6 of the Criminal Matters Amendment Act 68 of 1998 (which amends Section 79<br />
(1) of Act 51 of 1977), clinical psychologists are also empowered to conduct and report on forensic<br />
assessments concerning pathological mental states. Prior to this, only psychiatrists were legally<br />
allowed to perform this duty.<br />
Activity 8.1.<br />
X is accused of murdering his neighbour.<br />
In court he babbles incoherently and laughs<br />
inappropriately when the judge addresses<br />
him. Is he fit to stand trial? Explain your<br />
answer.
Affective<br />
functioning<br />
refers to<br />
emotional<br />
functioning.<br />
Conative<br />
functioning<br />
refers to<br />
volitional<br />
functioning<br />
Insanity and diminished capacity 4<br />
illness or defect (Reed and Seago, 1999). There are various legal tests which<br />
must be applied when this defence is raised, and while there are differences in<br />
various jurisdictions, these tests, and the defence in general, have their roots in<br />
English law.<br />
The legal test for <strong>insanity</strong> in South Africa is rooted in the McNaughton<br />
Rules of 1843 which stemmed from a murder trial where the accused was<br />
found ‘not guilty on the ground of <strong>insanity</strong>’. This right-from-wrong test is<br />
concerned with the accused’s legal responsibility at the time of the alleged<br />
offence and Card (1992, p.127) summarises it as follows:<br />
(a) Everyone is presumed sane until the contrary is proved.<br />
(b) It is a defence to a criminal prosecution for the accused to show<br />
that he was labouring under such a defect of reason, due to disease<br />
of the mind, as either not to know the nature and quality of his act<br />
or, if he did know this, not to know that he was<br />
doing wrong.<br />
Activity 8.3<br />
Discuss the difference between affective,<br />
conative and cognitive functioning.<br />
The McNaughton test relies heavily on the accused’s<br />
cognitive capacity (intellectual capacity) which may<br />
have compromised his or her insight and judgment. ‘Defect of reason due to<br />
disease of mind’ is central to the defence and does not consider other aspects<br />
Affective<br />
functioning<br />
refers to<br />
Activity 8.2<br />
emotional What is the legal test for <strong>insanity</strong> in South<br />
functioning. Africa?<br />
Conative<br />
functioning<br />
refers to<br />
volitional<br />
functioning<br />
of psychological functioning namely,<br />
affective (emotional) and conative (volitional)<br />
functioning, which are integral to human<br />
nature.. As a result, in English law, the<br />
defence cannot be raised if the offence was committed because of emotional<br />
upheaval caused by emotions such as rage, jealousy or stress. Equally, it is not<br />
possible to raise the defence of <strong>insanity</strong> where the accused has committed an<br />
alleged offence because of poor self-control as would be in the case of an<br />
‘irresistible impulse’. Card (1992) criticises the McNaughton Rules as being<br />
too restrictive because they do not allow for a defence of ‘irresistible impulse’.<br />
He says that the narrow focus on impaired cognitive capacities ignores the<br />
reality that mental illness can impair conative functioning.<br />
English law therefore explicitly requires biological evidence of mental<br />
illness and its concomitant effects, with the result that psychiatrists generally<br />
serve as expert witnesses in cases where ‘sanity’ is contested. This may<br />
explain why affective and volitional factors are not recognised in this defence,<br />
as they can be better understood within a psychological framework as opposed<br />
to a strictly medical or biological model.<br />
Box 8.1 Who was Daniel McNaughton?<br />
Mental defect<br />
refers to<br />
significantly<br />
below average<br />
intellectual<br />
functioning<br />
The McNaughton Rules of 1843 have their roots in the trial of Daniel McNaughton who was accused<br />
of murdering Edward Drummond. McNaughton, a wood-turner from Glasgow was in his early thirties<br />
and suffered from persistent delusions of persecution by the Tories. He was plagued by these delusions<br />
for several years prior to the murder and he tried to evade the ‘spies who were following him by going to<br />
England and to France. He claimed that they continued to follow him and that he was compelled to kill<br />
the British Prime Minister, Sir Robert Peel but mistakenly shot Edward Drummond who was Prime<br />
Minister’s Private Secretary. At his trial eight medical witnesses testified that his psychosis resulted in an<br />
inability to distinguish right from wrong. Today McNaughton’s symptoms would probably qualify for a<br />
diagnosis of schizophrenia, however as the diagnosis has not been developed at that time, records show<br />
that he was diagnosed with ‘chronic mania and dementia’.
Africa 5<br />
The jury found McNaughton ‘not guilty by reason of <strong>insanity</strong>’and he was remanded to a psychiatric<br />
institution for the rest of his life. (Rollin,1977).<br />
In the late nineteenth century, the scope of the McNaughton Rules was<br />
broadened in South Africa [CT3]so as to include the ‘irresistible impulse’ rule.<br />
The courts acknowledged that mental illness or defect could impair conative<br />
functioning and therefore negate responsibility (Kruger, 1980). In R v Koortz<br />
1953 (1) SA 371 (A), the re-formulated McNaughton Rules were accepted by<br />
the court:<br />
A person is not punishable for conduct which would in ordinary<br />
circumstances have been criminal if, at the time, through disease of mind<br />
or mental defect -<br />
(a) he was prevented from knowing the nature and quality of the<br />
conduct, or that it was wrong; or<br />
(b) he was the subject of an irresistible impulse which prevented him<br />
from controlling such conduct<br />
(Gardiner and Lansdown, cited in Kruger, 1980, p.156).<br />
Where the <strong>insanity</strong> defence was raised, most cases were decided under the<br />
‘irresistible impulse’ rule but several difficulties arose in its application. These<br />
centred around establishing whether in fact the impulse derived from mental<br />
illness and not from emotional factors such as jealousy, greed or revenge. In<br />
addition, it was difficult to establish whether the impulse was indeed<br />
irresistible and whether the accused genuinely had no control over it. These<br />
problems and perceived loopholes within the law were addressed by the<br />
Rumpff Commission of Inquiry into the Responsibility of Mentally Deranged<br />
Persons and Related Matters (RP 69/1967), which was established following<br />
the assassination of the South African Prime Minister, Hendrik Verwoerd, by<br />
a mentally ill offender. The Rumpff Commission concluded that a person’s<br />
responsibility for his or her actions is based on the ability to exercise free<br />
choice and the ability to distinguish between right and wrong (Kruger, 1980).<br />
The recommendations of the Commission subsequently gave rise to the<br />
provisions in Section 78(1) of the CPA which states that:<br />
A person who commits an act which constitutes an offence and who at<br />
the time of such commission suffers from a mental illness or mental<br />
defect which makes him incapable<br />
(a) of appreciating the wrongfulness of his act; or<br />
(b) of acting in accordance with an appreciation of the wrongfulness of<br />
his act,<br />
shall not be criminally responsible for such act.3<br />
3 This section of the Act has subsequently been amended as follows:<br />
A person who commits an act or makes an omission which constitutes an offence and<br />
who at the time of such commission suffers from a mental illness or mental defect<br />
which makes him or her incapable<br />
(a) of appreciating the wrongfulness of his or her act or omission; or<br />
(b) of acting in accordance with an appreciation of the wrongfulness of his or her act<br />
or omission.shall not be criminally responsible for such act or omission<br />
Section 5 of the Criminal Matters Amendment Act 68 of 1998<br />
The clinical<br />
assessment<br />
process includes<br />
the clinical<br />
interview,<br />
psychological<br />
testing and<br />
collateral<br />
information
Insanity and diminished capacity 6<br />
Diagnosing Mental Illness<br />
The criteria which courts apply with respect to responsibility embody a<br />
right-from-wrong-test, which assesses the capacity to act according to the<br />
appropriate insight. The test has biological (i.e. presence<br />
of mental illness) and psychological components (i.e.<br />
impairment of cognitive and/or conative functions) and<br />
a successful defence requires the presence of both.<br />
Case example 8.1 : Depression, murder and criminal responsiblity<br />
Activity 8.5<br />
Discuss the difference between mental<br />
illness and mental defect.<br />
In S v Kavin 1978 (2) SA 731 (W), the accused was charged with murdering his wife, daughter and son. He was<br />
also charged with the attempted murder of another daughter. His defence was that he was suffering from a mental<br />
illness which rendered him non-responsible. He was examined by three psychiatrists who concurred with a<br />
diagnosis of ‘severe reactive depression superimposed on a type of personality disorder displaying immature and<br />
unreflective behaviour’ (p. 734). Two psychiatrists opined that he was able to appreciate the wrongfulness of his<br />
act while a third was uncertain. However, all three concurred that his depressive state rendered him incapable of<br />
acting in accordance with an appreciation of wrongfulness. In this case the accused’s conative functioning was<br />
impaired by a depressive disorder.<br />
Case Exercise<br />
Read the case, along with S v Mahlinza 1967 1 SA 408 (A) (both can be accessed in the collections of law reports<br />
held by most academic libraries). Compare the arguments regarding what constitutes mental illness by focussing<br />
on the expert evidence which was led.<br />
The DSM-IV TR<br />
is a taxonomy of<br />
mental disorders<br />
The law does not provide a definition of mental illness or mental defect<br />
and therefore makes provision for expert testimony to establish this (Van<br />
Oosten, 1990). In order to make a diagnosis of mental illness, the psychologist<br />
uses a variety of tools as part of the clinical assessment process. The clinical<br />
interview provides the psychologist with the opportunity to gather salient<br />
aspects of the accused’s psychosocial history. This history-taking includes<br />
information such as the nature of the symptoms, the level of distress which is<br />
experienced, family history and occupational functioning. In addition the<br />
clinician (psychologist) may make use of measures such as psychological tests<br />
which provide objective information about the accused’s functioning. For<br />
example, personality tests will yield information regarding personality style<br />
and functioning while intelligence tests assess cognitive<br />
functioning. Collateral information (third party<br />
information) may be gathered from significant others so<br />
as to provide additional insight into the accused’s<br />
functioning in various spheres. This information may<br />
be provided by family members, work colleagues or other professionals (such<br />
as general practitioners, psychiatrists and psychologists) whom the accused<br />
has consulted.<br />
An important diagnostic tool which psychologists in South Africa use to<br />
make diagnoses, is the Diagnostic and Statistical Manual of Mental Disorders<br />
(DSM-IV TR) 8(APA, 2000). This system classifies mental disorders in terms<br />
of their diagnostic criteria (symptoms) and provides clinicians with the<br />
information necessary to make diagnoses. For example, to make a diagnosis of<br />
Schizophrenia 4 , the clinician has to establish the presence of psychotic<br />
symptoms, the duration of these symptoms and the degree to which the<br />
4 Schizophrenia is a psychotic disorder characterised by delusions, hallucinations, disorganised speech<br />
and disorganised or catatonic behaviour. (DSM-IV-TR, APA, 2000).<br />
Activity 8.4<br />
What are the various tools which the<br />
psychologist may use to make a diagnosis?<br />
Psychologists<br />
diagnose mental<br />
illness and do<br />
not determine<br />
criminal<br />
responsibility
Africa 7<br />
person’s functioning has been impaired. The DSM-IV TR (APA, 2000)<br />
provides guidelines which assist the clinician in this process. The evidence<br />
which the psychologist presents in court will therefore allude to the presence<br />
of mental illness (for example, Schizophrenia) and how this impacts on the<br />
accused’s functioning.<br />
It is important to note that the psychologist, in providing a diagnosis, is not<br />
required or able to offer an opinion on the accused’s criminal responsibility.<br />
This is a matter to be decided by the courts. As Ogilivie Thompson J A in R v<br />
Harris 1965 (2) SA 340 (A) at 365 B-C states,<br />
... it must be borne in mind that...in the ultimate analysis, the crucial<br />
issue of the appellant’s criminal responsibility for his actions at the<br />
relevant time is a matter to be determined not by psychiatrists but by the<br />
Court itself. In determining that issue - initially the trial Court and on<br />
appeal this Court - must of necessity have regard not only to expert<br />
medical evidence but also to all the other facts of the case, including the<br />
reliability of the appellant as a witness and the nature of his proved<br />
actions throughout the relevant period’. This dictum highlights that the<br />
issue of determining criminal responsibility is a legal question while the<br />
diagnosis of mental illness is a psychological question.<br />
A diagnosis of mental illness does not automatically imply that an accused<br />
is non-responsible. Snyman (2002) says that the fact that a person has been<br />
declared mentally ill in terms of the Mental Health Act 18 of 1973, does not<br />
imply that he or she is also mentally ill in terms of s78(1) of the CPA. This is<br />
because the latter is chiefly concerned with how mental illness negates<br />
responsibility, and not with the nature of mental illness itself. For example, if a Mentally ill<br />
person is diagnosed with Schizophrenia and certified in terms of the Mental offenders are<br />
Health Act 18 of 1973, this does not automatically negate responsibility. In hospitalised for<br />
order for a successful defence to be raised, it has to be<br />
indefinite<br />
Activity 8.6 periods of time<br />
proven that the symptoms of Schizophrenia impaired What kind of psychological knowledge can<br />
the person’s cognitive and/or conative functioning. assist the court in making findings<br />
regarding mental state?<br />
Disposition of Mentally Ill Offenders<br />
Where the court accepts the defence of <strong>insanity</strong>, the accused is found not<br />
guilty and will be remanded into the care of a state psychiatric hospital for an<br />
indefinite period of time (Kruger 1999). For example, in S v Kavin 1978 (2)<br />
SA 731 (W), the court accepted the evidence that the accused’s depression<br />
impaired his conative functioning and therefore he was found not guilty of<br />
murder and attempted murder. He was remanded into the care of a state<br />
psychiatric hospital for an indefinite period, and was declared unfit to possess<br />
a firearm. In cases such as this, provision is made for the review of the<br />
patient’s progress and the hospital may recommend a discharge based on the<br />
prognosis of the illness and the danger which the patient poses to him or<br />
herself and society. This process has to be ratified by the courts, particularly<br />
where the offence has been violent (Kruger, 1980).<br />
The Insanity Defence – Controversies and Challenges<br />
The <strong>insanity</strong> defence in South Africa has not evoked the same kind of<br />
controversy as in the case of American jurisdictions. For this reason it is useful<br />
to explore some of the debates which have plagued legal and psychological
Insanity and diminished capacity 8<br />
The legal test for<br />
pathological<br />
incapacity is<br />
identical to that<br />
for nonpathological<br />
incapacity<br />
practitioners in the U.S. American conceptions of <strong>insanity</strong> are much broader<br />
than those found in South African law. Consequently, a wide range of<br />
psychological states, which do not necessarily have a biological basis, are<br />
considered to be instances of <strong>insanity</strong> (Slovenko, 1995). The inclusion of an<br />
array of diagnoses as grounds for exculpation has been viewed as problematic<br />
by various legal commentators. Dershowitz (1994), for example, is sceptical<br />
of the mitigating function of syndrome evidence involving allegations of<br />
abuse. He views such evidence as an ‘abuse excuse’ which purely functions as<br />
a means of evading responsibility. He comments on psychiatry and<br />
psychology’s complicity in helping offenders to evade appropriate punishment<br />
by providing them with ‘cop-outs’ and ‘sob stories’ couched in psychological<br />
jargon. He feels that this kind of evidence threatens the foundations of the<br />
American legal system as it expands the parameters of excusable behaviour.<br />
This kind of thinking, along with the public outcry subsequent to the acquittal<br />
of John Hinckley 5 , has resulted in the re-evaluation of the <strong>insanity</strong> defence at<br />
both state and federal levels in the US. Consequently, some American<br />
jurisdictions have abolished the defence while in others the McNaughton rules<br />
have been modified (Steadman, McGreevy, Morrissey, Callahan, Robbins and<br />
Cirincione, 1993).<br />
Slovenko (1995) argues that it is difficult to establish the current status of<br />
the <strong>insanity</strong> defence in America, given the many changes which it has<br />
undergone in various states. Current debate has centred on whether or not the<br />
defence should be abolished completely, particularly because it is seen as a<br />
loophole for those who should be subject to the full force of the law. Some<br />
proponents of abolition argue that criminal responsibility is a matter of law<br />
and should be left to juries for deliberation and not to the assessment of<br />
psychiatric experts. Slovenko says that these critics argue that ‘psychiatry is<br />
corrupting the criminal justice system by expanding the concept of mental<br />
illness, always at the expense of the concept of responsibility’ (1995, p.34).<br />
While South African law has not been plagued with the same conundrums,<br />
there is some controversy regarding the legal test which is applied. The debate<br />
centres on the fact that the tests for pathological and non-pathological<br />
incapacity are identical. The defence of non-pathological incapacity<br />
acknowledges that psychological states such as anger, fear, shock and<br />
emotional stress may render a person non-responsible for his or her actions.<br />
Consequently, the circumstances within which an accused may be exculpated<br />
are substantially broadened. Unlike a successful <strong>insanity</strong> plea, a verdict of not<br />
guilty does not imply indefinite hospitalisation. Instead the accused is free to<br />
resume his or her life.<br />
Petty (1998) argues that the application of the provisions within s78 (1) of<br />
the CPA to what are in fact two distinct mental states, is problematic. The<br />
dilemma which this poses is exacerbated by the fact that because the law<br />
construes mental illness in terms of the degree of criminal responsibility, no<br />
diagnostic parameters have been set. From a psychological perspective, there<br />
is a clear distinction between distress and impairment caused by pathology and<br />
that which is caused by a temporary emotional state. However, these kinds of<br />
5 Public outcry followed the 1982 <strong>insanity</strong> acquittal of John Hinckley following the<br />
assassination attempt on President Reagan (Steadman, McGreevy, Morrissey,<br />
Callahan, Robbins and Cirincione, 1993).
Africa 9<br />
distinctions are not central to legal deliberations because the court is<br />
concerned with whether the accused met the criteria for the legal test and not<br />
with the nature of the mental state. Petty (1998) feels that the lack of<br />
conceptual clarity and the fact that the defences can be raised in the<br />
alternative, present challenges for the psychologist. Consequently, the<br />
boundaries between the defences are blurred, resulting in ‘an anomalous,<br />
circuitous process whereby the court applies the test for criminal capacity...’<br />
(Petty, 1998, p. 4).<br />
Diminished Responsibility<br />
South African law, in line with Anglo-American jurisdictions,<br />
acknowledges that there are varying degrees of criminal responsibility. As a<br />
result, Section 78(7) of the Criminal Procedure Act (51 of 1977) states that:<br />
If the court finds that the accused at the time of the commission of the<br />
act in question was criminally responsible for the act but that his<br />
capacity to appreciate the wrongfulness of the act or to act in accordance<br />
with an appreciation of wrongfulness of the act was diminished by<br />
reason of mental illness or mental defect, the court may take the fact of<br />
such diminished responsibility into account when sentencing the<br />
accused.<br />
In terms of this provision, the accused may be suffering from some form of<br />
mental illness but the level of impairment experienced does not fulfil the<br />
requirements for the legal test of <strong>insanity</strong>. The pathology is then considered to<br />
be a mitigating factor in the degree of responsibility. A defence of diminished<br />
responsibility does not afford the accused complete exculpation, but may<br />
result in a reduced sentence instead of indefinite confinement to a state<br />
psychiatric hospital (Snyman, 2002).<br />
Controversy<br />
It stands to reason that expert testimony is required to establish that an<br />
abnormality of the mind existed at the time of the offence. However some<br />
English legal commentators have questioned the role which psychiatrists and<br />
psychologists play in assessing diminished responsibility. In a report by the<br />
Butler Committee on Mentally Abnormal Offenders (cited in Clarkson and<br />
Keating, 1990), the proficiency of such experts in<br />
assessing degrees of mental responsibility was<br />
questioned, since this is a concept of law and morality<br />
and not of psychiatry or psychology. The Committee<br />
questioned whether the accused’s ability to conform to<br />
the law could be measured clinically given that the law requires a substantial<br />
impairment of mental responsibility. Allen argues that ‘ the question of<br />
substantial impairment is inappropriate for medical witnesses as it is one of<br />
degree and whether it exists depends not only on the medical evidence but on<br />
all the evidence of the case relating to the facts and circumstances of the<br />
killing’ (1995, p. 128). He argues that the courts have allowed expert opinion<br />
in these matters so as to produce a greater range of exemptions from murder.<br />
Activity 8.78.<br />
Discuss the elements of the defence of<br />
diminished responsibility
Insanity and diminished capacity 10<br />
The defence of<br />
automatism<br />
questions the<br />
voluntariness of<br />
the act<br />
Sane automatism<br />
is caused by a<br />
psychological<br />
blow resulting in<br />
an altered state<br />
of consciousness<br />
Dissociative<br />
amnesia is<br />
characterised by<br />
gaps in memory<br />
caused by<br />
traumatic events<br />
Other Defences Related to Capacity/voluntariness of the act – Sane and<br />
Insane Automatism<br />
The provisions within s78 (1) of the CPA are chiefly concerned with the<br />
extent to which mental illness affects criminal capacity. Thus while the court<br />
acknowledges that an offence has been committed, its chief concern is whether<br />
the accused can be held criminally responsible. However, there are instances<br />
where the court questions whether the act itself was voluntary, and in these<br />
cases the defence of automatism is raised. In this defence, an altered state of<br />
consciousness is presumed to result in a person committing an offence in an<br />
automaton state. When the voluntariness of the act is in question, it does not<br />
constitute an act in law and therefore the accused cannot be held criminally<br />
responsible (Kruger, 1999).<br />
South African courts, in line with Anglo-American<br />
jurisdictions, distinguish between sane and insane<br />
automatism. While the voluntariness of the act is central<br />
to both of these defences, a successful outcome has<br />
Activity 8.89.<br />
Explain how the defence of diminished<br />
responsibility differs from the <strong>insanity</strong><br />
defence<br />
differing implications for the accused. In cases of sane automatism, an<br />
acquittal means that the accused is free, while in instances of insane<br />
automatism, the accused is remanded to a psychiatric hospital for an indefinite<br />
period of time.<br />
Sane Automatism<br />
Sane automatism occurs when a person involuntarily performs an action<br />
while experiencing a change in his or her state of consciousness. This altered<br />
state does not have a pathological basis which can be linked to some inherent<br />
biological cause. Instead, the automatism is presumed to arise from severe<br />
psychological stress caused by life events, and results in ‘dissociation’. This<br />
complete splitting between mental and physical activity renders the person<br />
incapable of controlling his or her actions and consequently the act which is<br />
performed cannot be recognised as an act in law (Schopp, 1995).<br />
Dissociation is a psychological state which involves ‘a disruption in the<br />
usually integrated functions of consciousness, memory, identity or perception<br />
of the environment’ (Barnard, 1998, p. 28). The impairment in the integration<br />
of functions is caused by a ‘psychological blow’ which causes the person to<br />
dissociate. In the same way that a physical blow to the head can result in an<br />
altered state of consciousness, so too can traumatic experiences impair<br />
functioning. For example, if a person experiences a horrific attack, he or she<br />
may dissociate from that experience and experience amnesia for the event.<br />
Consequently, the person will be unable to recall details of the event while not<br />
experiencing any other difficulties in memory. This dissociation and the<br />
resultant amnesia occur, ostensibly because the psychological effects of the<br />
event are too traumatic for the conscious mind to deal with.<br />
Dissociative amnesia is an example of a dissociative disorder which has<br />
been forwarded as a diagnosis in the defence of sane automatism. The<br />
diagnostic features (symptoms) which are reported relate to gaps in memory,<br />
and these in turn are linked to traumatic or stressful events. In essence, a<br />
person suffering from dissociative amnesia will not suffer any other memory<br />
impairment and the amnesia is limited to the traumatic experience itself<br />
(DSM-IV TR, APA, 2000). For example, a person may report amnesia for<br />
Dissociation is a<br />
complete<br />
splitting between<br />
mental and<br />
physical activity
Africa 11<br />
episodes of sexual abuse at the hands of another. The physical and<br />
psychological trauma which characterises sexual abuse triggers the<br />
dissociative episode resulting in an altered state of consciousness. He or she<br />
‘blocks out’ the painful episodes and experiences<br />
amnesia for these events. Consequently the person is<br />
unable to relate any of these experiences as they are<br />
inaccessible to conscious memory. Mounting a defence<br />
of sane automatism<br />
In order to mount a defence of sane automatism it must be proven that the<br />
there has been an antecedent build-up such as a period of conflict or dispute<br />
which the person has experienced. The dissociative episode which the person<br />
undergoes must have been caused by some external trigger mechanism For<br />
example, a person a who has been experiencing marital difficulties may be so<br />
overwhelmed by the news that his or her is spouse is filing for divorce that he<br />
or she reacts violently and murders the spouse. Consequently, he or she may<br />
have no conscious memory of this action because of the extreme nature of the<br />
emotional reaction (in this example, rage), which completely overwhelms the<br />
conscious mind and renders him or her incapable of goal-directed action.<br />
Where such a claim is made, the psychologist has to assess whether the<br />
accused experienced a discrete dissociative episode at the time of the murder.<br />
An integral part of this diagnosis is whether the person has amnesia for the<br />
event. This diagnosis is15 difficult to make in that the psychologist relies on<br />
the accused’s version of events, which may not always be reliable. The<br />
assessment as to whether the person has a true absence of memory for that<br />
discrete period is also problematic, given that the clinician again relies on the<br />
accused’s account. On one hand, it may be more plausible that a person<br />
‘blocks out’ memories of situations in which they have<br />
been victimised, while on the other, it is more difficult<br />
to accept such claims made by a person who is the<br />
victimiser. While the question of the veracity of such<br />
claims falls within the ambit of the court, the<br />
psychologist is to a certain extent placed in the position of assessing the<br />
accused’s truthfulness. In essence one has to ask whether it is plausible that<br />
someone who commits a crime triggered by an external stressor is so<br />
overwhelmed by emotion, that he or she has no memory of it.<br />
For example, in S v Pederson [1998] 3 All SA 321, the appellant appealed<br />
against his conviction for the murder of his estranged wife. The appellant<br />
claimed that he had not acted consciously and voluntarily in killing his wife<br />
and that even if the act was voluntary, he had no intention of murdering her.<br />
He claimed that he was under the influence of alcohol and had been angry and<br />
aggressive because his wife was leaving him. There was a history of domestic<br />
violence which culminated in the stabbing of the wife. The appellant claimed<br />
to have no recollection of the incident as he had experienced an acute<br />
catathymic crisis at the time of the murder. The psychological evidence<br />
defined this crisis as a ‘mental storm’ which overwhelmed his mental capacity<br />
such that he was unable to exert control over actions. The Court questioned<br />
whether the Appellant had experienced a true absence of memory for the<br />
incident or whether the amnesia served the purpose of repressing the trauma<br />
caused by the incident. The Court held that for the defence of sane automatism<br />
to succeed, the Appellant had to prove that he had experienced true amnesia<br />
Activity 8.910.<br />
Explain what is meant by the voluntariness<br />
of an act.<br />
Activity 8.1011<br />
Give three examples of psychological<br />
blows which may result in sane automatism
Insanity and diminished capacity 12<br />
for the event and that there was an absence of control by the mind over his<br />
actions. The Court upheld the conviction the basis of the evidence that the<br />
accused had not acted in an automaton state and that his actions were<br />
sufficiently goal-directed.<br />
Case example 8.2 : How do we assess the truthfulness of an accused claiming sane automatism?<br />
In S v Potgieter 1994 (1) SACR 61 (A) the appellant appealed against the conviction and sentence which was<br />
imposed for the murder of her partner. At the trial, the defence argued that the appellant acted in a state of sane<br />
automatism and therefore was not criminally liable. The evidence which was led, indicated that she has been in a<br />
abusive relationship with her partner for six years. She had endured physical, verbal, emotional and financial<br />
abuse and also witnessed the maltreatment of her children from a previous marriage. The appellant testified that<br />
on the day in question, the deceased had once again assaulted her and ordered her to leave the house with her<br />
children. He left the house and she called a locksmith to open the safe so that she could retrieve the pistol which<br />
was kept there. She inserted a magazine and left the holstered pistol on the vanity slab in the bathroom. She<br />
testified that that night, she had woken up when she heard the baby crying. She found the deceased sitting in the<br />
lounge and asked him to turn down the volume on the television. She gave the baby his bottle and when she<br />
returned to her room, the deceased stood in the doorway, grabbed her and threw her against the wall. Her last<br />
memory was of him shouting at her and she saw his blurred image moving away from her. She then heard a loud<br />
bang after which she realised that she had a pistol in her hand and that he must have shot the deceased who was<br />
lying on the bed. Based on her account of events, the defence argued that the appellant had acted in an automaton<br />
state. The psychological evidence to support this highlighted her emotional reaction subsequent to the shooting as<br />
well as the fact that she did not have a history of violence. The state however questioned her account and her<br />
truthfulness as a witness. There were several inconsistencies in her testimony which did not accord with the facts<br />
of the case. Consequently, the state argued that her actions were not consistent with automatism as she had<br />
performed several goal-directed actions which resulted in the death of her partner. The court accepted the state’s<br />
evidence and found that the accused’s version of the events did not accord with the factual evidence. On appeal,<br />
the court upheld the conviction and supported the findings of the trial court. However in considering the sentence<br />
imposed, the court found that the trial court had erred in imposing a sentence of imprisonment. The court held that<br />
the abusive conditions which the appellant had endured, had resulted adversely affected her and that murder was<br />
committed when she was emotionally distraught and unable to exercise the requisite self-control. Consequently,<br />
the sentence was set aside and the matter was remitted to the trial court for consideration of a sentence of<br />
correctional supervision.<br />
Case Exercise<br />
Read the full case (in the law reports). Consider the argument advanced by the defence counsel. Construct your<br />
own argument in support of the defence’s contention that the trial judge had misdirected himself in finding that the<br />
appellant had acted in a goal-directed manner.<br />
Insane Automatism<br />
While sane automatism is brought about by external factors, insane<br />
automatism arises from a change in consciousness which is caused by mental<br />
illness (Reed and Seago, 1999). In this sense it can be seen as a variant of the<br />
<strong>insanity</strong> 16 defence in that it also requires the ‘disease of mind’ criterion. For<br />
example, the psychotic symptoms associated with schizophrenia can impair<br />
cognitive and volitional functioning to such an extent that the person is unable<br />
to act in a goal-directed manner. Consquently, the law acknowledges that an<br />
accused who suffers from a biological condition which may induce an<br />
automaton state, cannot be held criminally responsible as the act occurred<br />
outside of conscious awareness. A successful defence of insane automatism<br />
results in a verdict of ‘not guilty by reason of <strong>insanity</strong>’ which requires<br />
mandatory commitment to a psychiatric hospital for an indefinite period of<br />
time. The conditions governing commitment are therefore the same as for
Africa 13<br />
those who have been found not guilty under the <strong>insanity</strong> plea (Reed and<br />
Seago, 1999).<br />
Automatism : controversies and challenges<br />
While English courts have clear-cut guidelines as to the interpretation of<br />
sane automatism, American courts have failed to develop any clarity as to<br />
their interpretations. Schopp (1995), in reflecting on the stance in American<br />
jurisdictions, says that some courts have viewed automatism as a variation of<br />
the <strong>insanity</strong> plea while others have expressly rejected this notion and<br />
considered it a separate defence. Finkel (1988) refers to the sane automatism<br />
defence as an ‘atypical’ <strong>insanity</strong> defence because the jury rules on whether<br />
there was an act and does not concern itself with the existence of disease of<br />
mind or the issue of intent. Thus the mental state of the accused is not central<br />
to ascertaining responsibility. Finkel (1988) argues that psychiatric testimony<br />
provides ‘the room, shadings, and interpretative leeway’ (p. 291) which<br />
enables lawyers to employ the defence if other avenues have failed.<br />
The legal debates as to the interpretation of the defence are paralleled by<br />
psychological debates regarding the clinical veracity of acute periods of<br />
dissociative amnesia. Schopp (1999) argues that the incidence of the complete<br />
splitting between mental and physical activity is a clinical rarity. In fact, the<br />
DSM-IV TR (APA, 2000) states that an acute form of dissociative amnesia<br />
which is characterised by a sudden onset is less common than dissociation<br />
arising from protracted periods of trauma.<br />
As in Anglo-American jurisdictions, claims of sane automatism are viewed<br />
with caution by South African courts because a diagnosis of dissociation relies<br />
heavily on the accused’s account of the event. There are no objective<br />
psychological measures for assessing whether he or she experienced a discrete<br />
dissociative episode or the concomitant amnesia. While the factual evidence is<br />
central to the court’s deliberations, the psychologist’s diagnosis hinges on the<br />
accused’s account. The difficulty which arises is that expert psychological<br />
evidence is based on a claim of a discrete period of dissociation which<br />
occurred some time before the assessment. Kruger (1999) says that the<br />
reliability and truthfulness of the accused are crucial factors in laying a factual<br />
basis for the defence. This raises the question as to whether the expert is<br />
placed in the position of assessing the reliability of the accused or whether<br />
such claims are accepted on the face of what the accused has said. It is<br />
therefore an ethical and professional dilemma - does the expert have to assume<br />
the role of moral judge when asked to adduce evidence of such a nature? In<br />
addition, if the accused’s truthfulness is questioned by the court, how is the<br />
expert’s testimony viewed, based as it is on the accused’s account?<br />
Non-pathological Criminal Incapacity<br />
In the last twenty years South African courts have come to recognise the<br />
importance of psychological factors in the assessment of criminal<br />
responsibility. The provisions within s78(1) of the CPA have been interpreted<br />
in such a way that factors other than mental illness have been considered in the<br />
issue of non-responsibility (Strauss, 1995). Thus the biological component<br />
(i.e. mental illness) of this test is not the sole negating factor, and emotional<br />
factors have been held to affect criminal capacity.
Insanity and diminished capacity 14<br />
Non-pathological states refer to a wide range of temporary emotional<br />
reactions17 which may affect the accused’s ability to distinguish between right<br />
and wrong or the ability to act in accordance with an appreciation of<br />
wrongfulness (Snyman, 1989). As with the concept of <strong>insanity</strong>, nonpathological<br />
incapacity is not a psychological construct and merely refers to<br />
non-responsibility which does not arise from mental illness. Several landmark<br />
cases (such as S v Arnold 1985 (3) SA 256 (C) and S v Campher 1987 (1) SA<br />
940 (A) introduced the notion of non-pathological states<br />
such as emotional stress, personality disintegration,<br />
shock or anger, which can impair cognitive and/or<br />
conative functioning. In S v Laubscher 1988 (1) SA 163<br />
(A) for example, the accused appealed against his<br />
Activity 8.1112.<br />
Identify the elements of the defence of<br />
provocation<br />
conviction for the murder of his father-in-law. The shooting occurred as result<br />
of a confrontation with his parents-in-law regarding their efforts to dissolve<br />
his marriage and to deny him access to his son. The accused confronted his<br />
father-in-law, whereupon he fired twenty-one rounds into various rooms, some<br />
of which hit and killed the deceased. The defence led psychological and<br />
psychiatric evidence at the trial and the accused was said to have suffered<br />
from a ‘total personality disintegration’ which resulted in an impairment of<br />
functioning. However, both the trial and appeal court held that the expert<br />
testimony did not accord with the facts of the case. These facts showed that<br />
the accused demonstrated insight into what he was doing and that his actions<br />
were goal-directed and voluntary. The Laubscher judgement also commented<br />
that expert testimony is not indispensable in this defence and that the court is<br />
in a position to make a decision based on the facts of the case.<br />
Given that commonly accepted textbook diagnoses for temporary<br />
impairment do not exist, the defence has been interpreted by experts in various<br />
ways. Consequently, various psychological terms have been bandied about in<br />
an attempt to explain phenomena which do not fall within the parameters of<br />
psychopathology. Gillmer (1996) describes the defence as a ‘many-headed<br />
creature’ which can embody anything from a ‘total psychological<br />
disintegration’ to a ‘narrowing of consciousness’, ‘a separation of intellect and<br />
emotion’, ‘annihilator rage’, ‘dissociation’ or ‘good old-fashioned<br />
automatism’ (p. 20). It would seem as if psychology has attempted to provide<br />
the language and understanding to describe those non-pathological states<br />
which do not fit into the law’s conception of human nature. However, Gillmer<br />
(1996) questions whether psychology has not been complicit in assisting the<br />
law with diagnoses to support claims of temporary impairment, in order that<br />
courts view these as more credible and therefore acceptable as grounds for<br />
non-responsibility.<br />
Provocation<br />
The defence of provocation also falls within the ambit of non-pathological<br />
incapacity because it focuses on words or behaviour or a combination of the<br />
two which incite a person to react violently (Snyman, 2002). The emotional<br />
state induced by the provocation is temporary but may be so intense that the<br />
person’s cognitive and or conative functioning is impaired. The law is<br />
concerned with the effect of provocation on the accused, taking into account<br />
personal characteristics such as temperament which may explain the violent<br />
behaviour (Theron du Toit, 1993).
Africa 15<br />
An example of the way in which expert testimony has been adduced in this<br />
defence, is that of spousal homicide. Theron du Toit draws on the work of<br />
Hoffman and Zeffert (1988) by saying that ‘[t]he opinion of expert witnesses<br />
is admissible whenever, by reason of their special knowledge or skill, they are<br />
better qualified to draw inferences than the court. The admissibility of the<br />
evidence of expert witnesses is furthermore governed by the relevance of that<br />
evidence’ (1993, p. 247). She says that developments within case law<br />
regarding spousal homicide have pointed to the need for psychiatric or<br />
psychological evidence in ascertaining criminal responsibility. In the case of S<br />
v Campher 1987 (1) SA 940 (A), the court acknowledged this need and<br />
consequently expert testimony regarding battered woman syndrome was<br />
considered to be relevant and admissible. However, as cases such as S v Wiid<br />
1990 (1) SACR 561 (A) have shown, expert testimony is not indispensable,<br />
particularly when a factual foundation for non-responsibility has been laid in<br />
evidence. The result is that the onus is on the State to prove that the accused<br />
was criminally responsible. When a factual foundation has been laid, expert<br />
testimony may serve the purpose of facilitating this process but in the final<br />
analysis, it may well be superfluous (Theron du Toit, 1993). This antithetical<br />
situation highlights the difficulties which arise in defences which fall within<br />
the ambit of non-pathological incapacity. On one hand, expert testimony<br />
serves the purpose of outlining the psychological factors which lead to nonresponsibility.<br />
On the other, expert testimony is not required by law because<br />
the court may be in a position to make a finding based solely on the factual<br />
evidence (Van Oosten, 1993).<br />
Case example 8.3: Can rage impair conative functioning?<br />
In S v Moses 1996 (1) SACR 701 (C), the accused was charged with the murder of his lover. On the day<br />
in question, the accused and the deceased had unprotected intercourse after which the deceased declared<br />
that he had AIDS. The accused testified that he became enraged at hearing this and went to find an<br />
ornament with which he struck the deceased twice on his head. He then went to the kitchen to get a<br />
small knife and stabbed the deceased in the side. He returned to the kitchen to find a big knife with which<br />
he slit the deceased’s throat and wrists. The accused testified that he was overwhelmed with hatred for<br />
the deceased and he felt that his trust had been abused. It also reminded him of the sexual abuse which he<br />
had suffered at the hands of his father. His mind was flooded with thoughts as to how he would break the<br />
news of being HIV positive to his family and he also feared dying a horrible death. He testified that he<br />
was aware of what he was doing but was unable to control his actions because he was so enraged. In<br />
support of the defence of non-pathological incapacity resulting from extreme provocation, the defence<br />
led psychiatric and psychological evidence. This evidence focused on the accused’s psychosocial history<br />
which included sexual abuse, domestic violence and depression. He was diagnosed with borderline<br />
personality disorder and it was argued that he had manifested various neurotic behaviours such as head<br />
banging, bedwetting and fear of the dark, in childhood. This psychiatric ‘picture’ of the accused was<br />
coupled with a psychological ‘picture’ which traced a pattern of poor impulse control. It was argued that<br />
he was prone to anger and outbursts of violence and that he had exhibited rage reactions whenever he<br />
was provoked. The defence argued that given the accused’s personality structure and poor impulse<br />
control, his conative ability was impaired. He was therefore unable to control himself even though he<br />
was cognitively aware of his actions. In contrast, the state led rebuttal evidence in which the psychiatrist<br />
argued that a person’s conative functioning can only be impaired in sane automatism or other<br />
pathological states. It was argued that the accused did not act in an involuntary or automatic manner and<br />
that his actions were goal-directed and guided by conscious thought. He therefore had the cognitive<br />
capacity to distinguish right from wrong. The accused did not exhibit any signs of dissociative amnesia
Insanity and diminished capacity 16<br />
and therefore did not fulfil the criteria for sane automatism. The court found that the state’s evidence was<br />
problematic as it focussed on the accused’s cognitive capacity – which was never in dispute. The defence<br />
had argued that the accused had the cognitive capacity to appreciate wrongfulness but was unable to<br />
control his actions because of extreme provocation. In weighing up the evidence, the court found the<br />
accused’s ability to control his actions was significantly impaired and he was therefore acquitted.<br />
Case Exercise<br />
Read the case in the law reports. Provide a coherent argument as to why the accused should not have<br />
been acquitted.<br />
Non-pathological incapacity : controversies and challenges<br />
There are several problematic issues regarding the defence of nonpathological<br />
incapacity which are highlighted by legal commentators.<br />
The first issue relates to the onus of proof. Unlike the <strong>insanity</strong> defence, the<br />
accused does not bear the onus of proof, instead the State is required to prove<br />
beyond reasonable doubt that that s/he had criminal capacity at the time of the<br />
offence. However, the accused has to lay a foundation in evidence which the<br />
State then has to rebut (Boister, 1997). Burchell (1995) argues that there is an<br />
‘inherent injustice’ in placing the burden of proof on the accused claiming<br />
<strong>insanity</strong> while a plea of non-pathological incapacity places the onus of proof<br />
on the state. This ‘injustice’ is extended to the successful outcomes of these<br />
defences - in the former, it means confinement to a psychiatric hospital while<br />
the latter provides for complete acquittal. Burchell (1995) feels that a complete<br />
revision of legislation and burden of proof standards may address these<br />
problems but he is not optimistic about this occurring. It would seem that the<br />
courts are intent on applying the subjective test of criminal capacity<br />
particularly in the case of non-pathological incapacity.<br />
Following on from this, Burchell (1997) questions<br />
whether South African law is correct in applying a 19<br />
subjective test of criminal capacity and argues that it<br />
may be more useful to have some kind of objective test<br />
by which to measure the accused’s behaviour. He<br />
Activity 8.1213<br />
Identify three non-pathological states<br />
which may be used as grounds for<br />
exculpation.<br />
views the normative yardstick used in Anglo-American jurisdictions as being<br />
more useful and argues that a partial excuse as opposed to complete<br />
exculpation is more appropriate. .<br />
A third issue centres around a concern that the defence may be abused by<br />
those who have exhausted all other avenues in attempt to escape punishment.<br />
Snyman (1991) says that the courts have therefore treated such defences with<br />
great caution because they can be easily raised. In the same way that courts are<br />
circumspect with regards to the defence of sane automatism, so too do they<br />
view the defence of non-pathological incapacity. Snyman (2002) says that in<br />
those cases in which the defence has been considered seriously, the accused<br />
had shown a cumulative build-up of stress and/or provocation which then<br />
resulted in a temporary impairment of cognitive and/or conative functioning.<br />
Fourthly, while the notion of temporary emotional reactions suggests an<br />
interplay of psychological phenomena, there is no statutory requirement for<br />
expert evidence in such cases. It would appear that while a significant number<br />
of reported cases have relied on expert testimony, it is unclear whether the<br />
courts consider this evidence as indispensable for the defence to succeed.<br />
Kruger (1999) argues that psychiatric and psychological evidence do not play
Africa 17<br />
an indispensable role because the court itself is in a good position to make a<br />
decision based on the facts of the case. Burchell (1995) views the indecision<br />
regarding the importance of this testimony as problematic. There are instances<br />
when courts do not receive a balanced view of the accused’s actions because<br />
the state has not adduced psychiatric or psychological evidence. He suggests<br />
that judges should require the state to lead such evidence so as to mitigate<br />
against a one-sided view of the accused’s actions.<br />
The ambivalent attitude which courts have towards expert testimony is further<br />
fuelled by the courts’ concern as to the accused’s reliability and truthfulness<br />
since this defence hinges on the accused’s account of events. Burchell (1995)<br />
says that this defence by its very nature, is viewed with caution and if the<br />
accused’s reliability and truthfulness are questionable then the expert<br />
testimony will also be viewed in the same light (see, for example, S v<br />
Potgieter 1994 (1) SACR 61 (A). Burchell (1995) argues that one of the<br />
problems which arises in the forensic assessment of an accused, is that it<br />
occurs before the evidence has been heard in court. Therefore in pursuit of the<br />
truth, it would be advisable to allow the expert to re-evaluate his/her opinion<br />
after the factual evidence has been led. In this way greater weight may be<br />
given to such evidence after it has been established that the accused has<br />
provided the court with a convincing account of events.<br />
Finally, while the defence has been the focus of legal debate, it has also<br />
received some attention from mental health professionals, albeit to a lesser<br />
extent. The focus of discussion in these circles has been on the nature of<br />
expert evidence which is adduced (Van Rensburg & Verschoor, 1989; Strauss,<br />
1995; Van der Merwe, 1997). However the role of expert testimony in these<br />
cases has raised particular challenges for experts, and Zabow (1990) says that<br />
they ‘have been less than successful in attempting to adapt theory, diagnosis<br />
and clinical method to the framework of existing legal standards’ (p.5). In<br />
addition, in these cases experts do not have recourse to textbook diagnoses<br />
which can describe temporary cognitive or conative impairment (Strauss,<br />
1995).<br />
The discussion has shown that South African courts have been more accepting<br />
of the role of psychological factors in negating criminal responsibility but it<br />
would seem that a rather ambivalent attitude towards expert testimony<br />
prevails. As Boister concludes ‘[t]his indicates clearly that the crucial aspect<br />
of the defence of non-pathological criminal incapacity is not its psychological<br />
validity but its legal validity’ (1996, p. 373).<br />
Summary<br />
1. The legal test for <strong>insanity</strong> in South Africa has a biological component<br />
(ie the presence of mental illness) and a psychological component (the<br />
impairment of cognitive and/or conative functioning).<br />
2. The diagnosis of mental illness falls within the domain of psychiatrists<br />
and psychologists while the assessment of criminal responsibility falls<br />
within the domain of the court.<br />
3. In the defence of automatism the voluntariness of the act is in question.<br />
The person cannot be held criminally liable because the act is
Insanity and diminished capacity 18<br />
committed while he or she is an altered state of consciousness and is<br />
unable to perform goal-directed actions.<br />
4. The defence of non-pathological incapacity allows for temporary<br />
emotional states to be used as grounds for exculpation.<br />
Recommended reading<br />
Boland, F (1999). Anglo-American <strong>insanity</strong> defence reform: The war between<br />
law and medicine. Aldershot: Ashgate/Dartmouth.<br />
Burchell, J. M. (1997). South African Criminal Law and Procedure vol 1:<br />
General principles of Criminal Law. (Third edition) Cape Town: Juta.<br />
Reznek, L. (1997). Evil or ill? Justifying the <strong>insanity</strong> defence. London:<br />
Routledge.<br />
Snyman, C. R. ( 2002). Criminal Law. (Fourth edition). Durban: Butterworths.<br />
Slovenko, R. (1995) Psychiatry and criminal culpability. New York: John<br />
Wiley and Sons.<br />
Exercises<br />
1. How does the assessment of fitness to stand trial differ from an assessment<br />
of criminal responsibility. Use two examples to illustrate your answer.<br />
2. The defence of non-pathological incapacity provides a loophole in the law<br />
for those accused who want to evade criminal responsibility. Discuss this<br />
statement .<br />
3. Psychological evidence is superfluous in assisting the court in determining<br />
criminal responsibility. Argue in favour or against this statement by<br />
drawing on case law to support your argument.<br />
4. John is charged with the murder of his mother and his attorney raises<br />
queries regarding his mental state at the time of the offence. Collateral<br />
information from his sister indicates that John had been ‘acting strangely’<br />
for a few weeks prior to the offence. She reports that he was agitated,<br />
unable to sleep at night and would pace around restlessly. He also had an<br />
insatiable appetite which was quite out of character. On the day of the<br />
murder, John’s mother told him to do some gardening. He seemed very<br />
upset and agitated and was mumbling incoherently. He became enraged<br />
and bludgeoned his mother with a spade. Using a diagram, illustrate the<br />
process which should be followed to ascertain whether John can be held<br />
criminally responsible.<br />
5. Emma is charged with the murder of her lover but claims to have no<br />
memory of the incident when questioned by the police. She recalls that<br />
they had an argument about her partner’s infidelity and that she had been<br />
very upset by this. She has no memory of shooting her partner and says<br />
that it feels as if she ‘blacked out’ for a while. Her first memory<br />
subsequent to the shooting is of seeing her partner lying on the floor with<br />
the gun next to her. When Emma was questioned by the police, she<br />
appeared confused, disoriented and tearful. As her attorney, you will be
Africa 19<br />
arguing that Emma cannot be held criminally responsible on nonpathological<br />
grounds. Construct an argument to support your claim that<br />
she was unable to exercise volitional control because she was<br />
overwhelmed by rage. Draw on case law to support your argument and<br />
suggest how psychological evidence may assist your case.<br />
References<br />
Allen, M. J. (1995). Textbook on Criminal Law. London : Blackstone Press Limited.<br />
American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental<br />
Disorders-TR (Fourth edition Revised).<br />
Barnard, P. G. (1998). Diminished capacity and automatism as a defence. American<br />
Journal of Forensic Psychology, 16(2), 27- 62.<br />
Boister, N. (1996). Recent cases : general principles of liability. South African Journal of<br />
Criminal Justice, 9(3), 371-374.<br />
Burchell, J. (1995). Non-pathological incapacity: evaluation of psychiatric testimony. South<br />
African Journal of Criminal Justice, 8(1), 37-42.<br />
Burchell, J. M. (1997). South African Criminal Law and Procedure Vol 1: General Principles<br />
of Criminal Law. (Third edition) Cape Town: Juta.<br />
Card, R. (1992). Criminal Law. London : Butterworths.<br />
Clarkson, C. M.. V. and Keating, H. M. (1990). Criminal Law : Texts and materials. London<br />
: Sweet and Maxwell.<br />
Criminal Procedure Act, 51 of 1977.<br />
Criminal Matters Amendment Act 68 of 1998.<br />
Dershowitz, A (1994). The Abuse Excuse and other cop–outs, sob-stories and evasions of<br />
responsibility. New York : Free Press.<br />
Finkel, N. J. (1988). Insanity on trial. New York: Plenum Press.<br />
Gillmer, B. (1996). Psycho-legal incoherence. Paper presented to the National Congress of the<br />
South African Psychological Society. Johannesburg, September 1996.<br />
Kruger, A. (1980). Mental health law in South Africa. Durban: Butterworths.<br />
Kruger, A. (1999). Accused: Capacity to understand proceedings: Mental illness and criminal<br />
responsibility. In E. Du Toit, F. De Jager, A. Paizes, A. Skeen& S. van der Merwe(eds.).<br />
Commentary on the Criminal Procedure Act (Service 22). Cape Town: Juta.<br />
Rollin, H (1977). ‘McNaughton’s madness’. In D. West and A.Walk (eds). Daniel<br />
McNaughton: His trial and the aftermath. Kent: Gaskell Books.<br />
Petty, C. (1998). The psychopathology of self-control. Unpublished MA thesis, University of<br />
Stellenbosch.<br />
Reed, A. and Seago, P. (1999). Criminal Law. London: Sweet and Maxwell.<br />
Rumpff, (1990). Feite of woorde. Consultus, 3 (1), 19-22.<br />
R v Harris 1965 (2) SA 340 (A)<br />
S v Arnold 1985 (3) SA 256 (C)<br />
S v Campher 1987 (1) SA 940 (A)<br />
S v Kavin 1978 (2) SA 731 (W)<br />
S v Laubscher 1988 (1) S A 163 (A)<br />
S v Mahlinza 1967 (1) SA 408 (A)<br />
S v Moses 1996 (1) SACR 701 (C)<br />
S v Pederson 1998 3 All SA 321<br />
S v Potgieter 1994 (1) SACR 61 (A)<br />
S v Wiid 1990 (1) SACR 561 (A)<br />
Schopp, R. F. (1991). Automatism, <strong>insanity</strong> and the psychology of criminal responsibility: A<br />
philosophical enquiry. Cambridge: Cambridge University Press.<br />
Slovenko, R. (1995) Psychiatry and criminal culpability. New York: John Wiley and Sons.<br />
Snyman, C. R. (1989). Die verweer van nie-patologiese ontoerekeningsvatbaarheid in<br />
die strafreg. Tydskrif vir Regswetenskap, 14(1), 1-15.<br />
Snyman, C. R. (1991). Provokasie as volkome verweer in die Strafreg. Consultus, 4(1),35-38.<br />
Snyman, C. R. ( 2002). Criminal Law. (Fourth edition). Durban: Butterworths.<br />
Steadman H., McGreevy, M., Callahan, L., Robbins, P. and Cirincone, C. (1993). Before and<br />
after Hinckley: evaluating <strong>insanity</strong> defence reform. New York: Guilford Press.
Insanity and diminished capacity 20<br />
Strauss, S. A. (1995). Nie-patologiese ontoerekeningsvatbaarheid as verweer in die<br />
strafreg. South African Practice Management, 16(4), 14-34.<br />
Theron Du Toit, R. (1993). Provocation to killing in domestic relationships. Responsa<br />
Meridiana, 6, (3), 230-252.<br />
Van der Merwe, R. (1997). Sielkundige perspektiewe op tydelike nie-patologiese<br />
ontoerekeningsvatbaarheid. Obiter, 18(1), 138-144.<br />
Van Oosten, F. F.W. (1990). The <strong>insanity</strong> defence : its place and role in criminal law. South<br />
African Journal of Criminal Justice, 3(1), 1-9.<br />
Van Oosten, F. F.W. (1993). Non-pathological criminal incapacity versus pathological<br />
criminal incapacity. South African Journal of Criminal Justice, 6(2), 127-147.<br />
Van Rensburg, P. and Verschoor, T. (1989) Medies-geregtelike aspekte van amnesie.<br />
Tydskrif vir Regswetenskap,14(2), 40-54.<br />
Zabow, T. (1990). Conditions other than mental illness or mental disorder in ‘criminal’ and<br />
‘diminished responsibility’ (the meaning of psychiatric disorder in criminal responsibility).<br />
Psychiatric Insight, 7 (1), 4-5.