Mitanin Program - Nipccd
Mitanin Program - Nipccd
Mitanin Program - Nipccd

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Project Name:<br />
Efficiency Criteria<br />
Human Resource<br />
Efficiency<br />
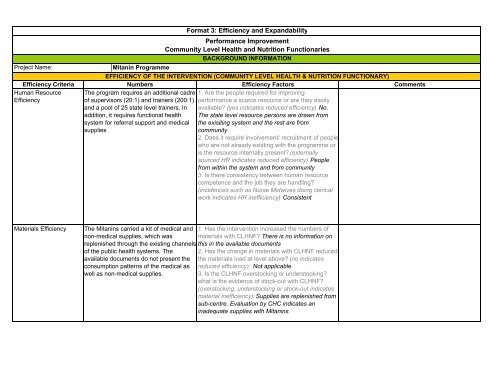
<strong>Mitanin</strong> <strong>Program</strong>me<br />
Format 3: Efficiency and Expandability<br />
Performance Improvement<br />
Community Level Health and Nutrition Functionaries<br />
BACKGROUND INFORMATION<br />
EFFICIENCY OF THE INTERVENTION (COMMUNITY LEVEL HEALTH & NUTRITION FUNCTIONARY)<br />
Numbers Efficiency Factors<br />
The program requires an additional cadre 1. Are the people required for improving<br />
of supervisors (20:1) and trainers (200:1). performance a scarce resource or are they easily<br />
and a pool of 25 state level trainers. In available? (yes indicates reduced efficiency) No.<br />
addition, it requires functional health The state level resource persons are drawn from<br />
system for referral support and medical the exisiting system and the rest are from<br />
supplies<br />
community<br />
2. Does it require involvement/ recruitment of people<br />
who are not already existing with the programme or<br />
is the resource internally present? (externally<br />
sourced HR indicates reduced efficiency) People<br />
from within the system and from community<br />
3. Is there consistency between human resource<br />
competence and the job they are handling?<br />
(incidences such as Nurse Midwives doing clerical<br />
work indicates HR inefficiency) Consistent<br />
Materials Efficiency The <strong>Mitanin</strong>s carried a kit of medical and 1. Has the intervention increased the numbers of<br />
non-medical supplies, which was materials with CLHNF? There is no information on<br />
replenished through the existing channels this in the available documents<br />
of the public health systems. The 2. Has the change in materials with CLHNF reduced<br />
available documents do not present the the materials load at level above? (no indicates<br />
consumption patterns of the medical as reduced efficiency): Not applicable<br />
well as non-medical supplies.<br />
3. Is the CLHNF overstocking or understocking?<br />
what is the evidence of stock-out with CLHNF?<br />
(overstocking, understocking or stock-out indicates<br />
material inefficiency): Supplies are replenished from<br />
sub-centre. Evaluation by CHC indicates an<br />
inadequate supplies with <strong>Mitanin</strong>s<br />
Comments
Time Efficiency <strong>Mitanin</strong> initiative was planned as a 60<br />
months programme. 18 months for pilot<br />
phase (selection, training and deployment<br />
of <strong>Mitanin</strong>) and the remaining 42 months<br />
for intervention and their work in<br />
community<br />
Technology Efficiency There is no information on this in the<br />
available document<br />
Financial Efficiency Annual programme cost per <strong>Mitanin</strong> (over<br />
60,000 mitanins) is Rs. 3750. Annual<br />
drug cost per <strong>Mitanin</strong> (over 60,000<br />
mitanins) is Rs. 2300<br />
1. Is it a quick action intervention for performance<br />
improvement? The Intervention takes 1.5 years as<br />
start-up time.<br />
2. Does bringing in this performance improvement<br />
take longer time out of CLHNF's routine work time?<br />
In other words, did participation in integrating<br />
performance improvement techniques hamper<br />
CLHNF's work? Since the performance<br />
improvement is done on the job review process, it<br />
does not reduce the working hours. However, there<br />
is no evidence to assess this<br />
1. Does the intervention use easily available<br />
gadgets and technology? (yes indicates improved<br />
efficiency): NA<br />
2. Are the gadgets and technology user-friendly to<br />
CLHNFs? (yes indicates improved efficiency)NA<br />
3. Are the gadgets portable? (yes indicates<br />
improved efficiency) NA<br />
4. Is the technology universally compatible with<br />
other gadgets? (yes indicates improved<br />
efficiency) NA<br />
5. Are the gadgets energy efficient? Less use of nonrenewable<br />
fuels and scarcely available energy<br />
sources (yes indicates imrpoved efficiency) NA<br />
1. Have DALYs and QALYs been calculated?: There<br />
is no information on this in the available documents<br />
2. If yes, does it show an improved cost per DALY/<br />
QALY?: N.A<br />
Sources of Information<br />
1. Human Resource Efficiency: Outcome Evaluation of <strong>Mitanin</strong>, SHRC<br />
2. Materials Efficiency: Outcome Evaluation of <strong>Mitanin</strong>, SHRC<br />
3. Time Efficiency: Mishra JP, <strong>Mitanin</strong> <strong>Program</strong>me, Available at:http://www.cbhi-hsprod.nic.in/prin.asp?SF=25&KI=5&OT=1<br />
4. Technology Efficiency: All available documents<br />
5. Financial Efficiency: Mishra JP, <strong>Mitanin</strong> <strong>Program</strong>me, Available at:http://www.cbhi-hsprod.nic.in/prin.asp?SF=25&KI=5&OT=1<br />
EXPANDABILITY (COMMUNITY LEVEL HEALTH & NUTRITION FUNCTIONARY)<br />
EXPANDABILITY FACTORS EXPERT GROUP'S COMMENTS SOURCE
Relevance to the existing problem<br />
Is this aspect of performance an issue of concern at national and state<br />
levels?<br />
Relevance of the performance improvement component in current<br />
programs?<br />
Transferability 1. Consistency (profile, job responsibilities) between the CLHNF under<br />
study and those with health systems and WCD Department?<br />
2. Is the solution consistent to existing infrastructure and human<br />
resources?<br />
3. Does the solution have multiple and complex components? How easy<br />
is it to transfer?<br />
4. Did the implementation of the model face resistance (from the<br />
community, from the health workers', from the workers' union or the<br />
health systems)?<br />
5. What are the groups that are most likely to resist the integration of this<br />
technique? Who are most likely to support it?<br />
Robustness<br />
Comment of the Expert Group:<br />
Date of Review<br />
1. Has this performance improvement technique been tried over a wide<br />
range of population? Was it successful?<br />
2. Has this technique been tried in EAG States? What was the success of<br />
it?<br />
3. How dependable is this technique on political support from highest<br />
offices? Is it sustainable despite political change and change of office<br />
bearers?<br />
4. Are there funds available to initiate it on a larger scale? Are there<br />
financial, technological, material and human resources available to<br />
sustain it at scale?<br />
Expert Group Member's Names: